Embed Size (px)
Citation preview

Women and MigraineWomen and MigraineThe Hormonal LinkThe Hormonal Link
Womens Health in Primary CareWomens Health in Primary CareOrlando Florida March 2011Orlando Florida March 2011
Norma Jo Waxman MDNorma Jo Waxman MD
Associate Professor of Family and Community MedicineAssociate Professor of Family and Community MedicineFaculty in the Bixby Center for Global Reproductive HealthFaculty in the Bixby Center for Global Reproductive HealthUniversity of California San FranciscoUniversity of California San Francisconjwaxmanfcmucsfedunjwaxmanfcmucsfedu
Learning ObjectivesLearning ObjectivesAt the end of this talk participants will be able to At the end of this talk participants will be able to
Define migraine with and without aura menstrually Define migraine with and without aura menstrually related migraine and true menstrual migrainerelated migraine and true menstrual migraine
Utilize pharmacologic and behavioral options for acute Utilize pharmacologic and behavioral options for acute and prophylactic management of migraineand prophylactic management of migraine
Understand when hormonal medication is helpful and Understand when hormonal medication is helpful and safe for women with migrainesafe for women with migraine
Recognize and decrease incidence of chronic daily Recognize and decrease incidence of chronic daily headache in your practiceheadache in your practice
No pharmaceutical No pharmaceutical support or commercial support or commercial disclosuresdisclosures
Member of ARHP Member of ARHP expert advisory expert advisory committee on committee on Hormonal Migraines Hormonal Migraines and developed slide and developed slide set Many used in this set Many used in this presentationpresentation
Faculty DisclosureFaculty Disclosure
ldquoDespite the fact that it is so common and has so much impact on society migraine is one of the most misunderstood misdiagnosed and undertreated diseases on earthrdquo
Carolyn Bernstein MD The Migraine Brain
Why Care About MigraineWhy Care About Migraine Very Common neurologic Very Common neurologic
disorderdisorderbull UnderrecognizedUnderrecognizedbull UndertreatedUndertreated
Produces severe disability Produces severe disability 1212
Overuse of any drug may lead Overuse of any drug may lead
to chronic daily HAsto chronic daily HAs3434
IHS Headache Classification Subcommittee of the International Headache Society (IHS) The International Classification of Headache Disorders 2nd ed Cephalalgia 200424(Suppl1)139-41 1 Lipton RB et al Headache 200141646ndash657 2 Bigal ME et al Cephalalgia 2006 2643ndash49 3 Scher AI et al Pain 20031681ndash89 4 Bigal ME Lipton RB Headache 2006461334ndash1343 5 Kruit MC et al JAMA 2004291427ndash434 6 Kurth T et al JAMA 2006296283ndash291
Migraine in USAMigraine in USA
30 million migraine sufferers30 million migraine sufferers 1 in 10 persons a migraineur1 in 10 persons a migraineur 1 of 4 households include a migraineur1 of 4 households include a migraineur 99thth leading disability more common than diabetes leading disability more common than diabetes
or asthmaor asthmabull 30 of migraineurs have 3+ attacksmo30 of migraineurs have 3+ attacksmobull 75 have reduced ability to function75 have reduced ability to functionbull 50 are severely impaired50 are severely impaired
Lipton RB et al Headache 200141646ndash657
Migraine Co-morbiditiesMigraine Co-morbiditiesbull PMSPMSbull DepressionDepressionbull Anxiety disorders (generalized panic Anxiety disorders (generalized panic
bipolar OCD)bipolar OCD)bull AbusePTSDAbusePTSDbull StrokeStrokebull Irritable bowel syndromeIrritable bowel syndromebull EpilepsyEpilepsybull FibromyalgiaFibromyalgia
Epidemiology of Migraine in Epidemiology of Migraine in WomenWomen
Women are affected 3x more than menWomen are affected 3x more than men 20 million women in USA 20 million women in USA 40 of women in their lifetime40 of women in their lifetime
bull Before puberty equally prevalent in both sexes Before puberty equally prevalent in both sexes bull After puberty 3x more women than menAfter puberty 3x more women than menbull Peaks in midlifePeaks in midlifebull darrdarr after menopauseafter menopause
Lipton RB Headache 2001 Lipton RB Neurology 2007 Stewart Cephalalgia 2008
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine Without AuraMigraine Without Aura
At least 5 attacks with At least 5 attacks with Headache lasts 4ndash72 hours wo treatment or Headache lasts 4ndash72 hours wo treatment or
without successful treatmentwithout successful treatmentAt least 2 of the following four symptomsAt least 2 of the following four symptoms
bull Unilateral pain (60)Unilateral pain (60)bull Throbbing (70)Throbbing (70)bull Aggravation by movement Aggravation by movement bull Moderate to severe painModerate to severe pain
ICHD = International Classification of Hreadache DisordersAdapted from Cephalalgia 20048(suppl 1)S24-26
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine Without AuraMigraine Without Aura (contrsquod) (contrsquod)
And at least 1 of the following 2 symptomsAnd at least 1 of the following 2 symptoms
bull Nausea andor vomitingNausea andor vomitingbull Photophobia andor phonophobiaPhotophobia andor phonophobia
Not attributed to organic diseaseNot attributed to organic disease
Adapted from IHS Cephalalgia 2004
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine with AuraMigraine with Aura
At least 2 attacks withAt least 1 fully reversible symptom wo motor
Visual (flickering lights zigzags spots or lines andor loss of vision) + andor
Sensory (ldquopins and needlesrdquo andor numbness) + andor Dysphasic speech
Adapted from IHS Cephalalgia 2004
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
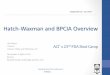
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Learning ObjectivesLearning ObjectivesAt the end of this talk participants will be able to At the end of this talk participants will be able to
Define migraine with and without aura menstrually Define migraine with and without aura menstrually related migraine and true menstrual migrainerelated migraine and true menstrual migraine
Utilize pharmacologic and behavioral options for acute Utilize pharmacologic and behavioral options for acute and prophylactic management of migraineand prophylactic management of migraine
Understand when hormonal medication is helpful and Understand when hormonal medication is helpful and safe for women with migrainesafe for women with migraine
Recognize and decrease incidence of chronic daily Recognize and decrease incidence of chronic daily headache in your practiceheadache in your practice
No pharmaceutical No pharmaceutical support or commercial support or commercial disclosuresdisclosures
Member of ARHP Member of ARHP expert advisory expert advisory committee on committee on Hormonal Migraines Hormonal Migraines and developed slide and developed slide set Many used in this set Many used in this presentationpresentation
Faculty DisclosureFaculty Disclosure
ldquoDespite the fact that it is so common and has so much impact on society migraine is one of the most misunderstood misdiagnosed and undertreated diseases on earthrdquo
Carolyn Bernstein MD The Migraine Brain
Why Care About MigraineWhy Care About Migraine Very Common neurologic Very Common neurologic
disorderdisorderbull UnderrecognizedUnderrecognizedbull UndertreatedUndertreated
Produces severe disability Produces severe disability 1212
Overuse of any drug may lead Overuse of any drug may lead
to chronic daily HAsto chronic daily HAs3434
IHS Headache Classification Subcommittee of the International Headache Society (IHS) The International Classification of Headache Disorders 2nd ed Cephalalgia 200424(Suppl1)139-41 1 Lipton RB et al Headache 200141646ndash657 2 Bigal ME et al Cephalalgia 2006 2643ndash49 3 Scher AI et al Pain 20031681ndash89 4 Bigal ME Lipton RB Headache 2006461334ndash1343 5 Kruit MC et al JAMA 2004291427ndash434 6 Kurth T et al JAMA 2006296283ndash291
Migraine in USAMigraine in USA
30 million migraine sufferers30 million migraine sufferers 1 in 10 persons a migraineur1 in 10 persons a migraineur 1 of 4 households include a migraineur1 of 4 households include a migraineur 99thth leading disability more common than diabetes leading disability more common than diabetes
or asthmaor asthmabull 30 of migraineurs have 3+ attacksmo30 of migraineurs have 3+ attacksmobull 75 have reduced ability to function75 have reduced ability to functionbull 50 are severely impaired50 are severely impaired
Lipton RB et al Headache 200141646ndash657
Migraine Co-morbiditiesMigraine Co-morbiditiesbull PMSPMSbull DepressionDepressionbull Anxiety disorders (generalized panic Anxiety disorders (generalized panic
bipolar OCD)bipolar OCD)bull AbusePTSDAbusePTSDbull StrokeStrokebull Irritable bowel syndromeIrritable bowel syndromebull EpilepsyEpilepsybull FibromyalgiaFibromyalgia
Epidemiology of Migraine in Epidemiology of Migraine in WomenWomen
Women are affected 3x more than menWomen are affected 3x more than men 20 million women in USA 20 million women in USA 40 of women in their lifetime40 of women in their lifetime
bull Before puberty equally prevalent in both sexes Before puberty equally prevalent in both sexes bull After puberty 3x more women than menAfter puberty 3x more women than menbull Peaks in midlifePeaks in midlifebull darrdarr after menopauseafter menopause
Lipton RB Headache 2001 Lipton RB Neurology 2007 Stewart Cephalalgia 2008
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine Without AuraMigraine Without Aura
At least 5 attacks with At least 5 attacks with Headache lasts 4ndash72 hours wo treatment or Headache lasts 4ndash72 hours wo treatment or
without successful treatmentwithout successful treatmentAt least 2 of the following four symptomsAt least 2 of the following four symptoms
bull Unilateral pain (60)Unilateral pain (60)bull Throbbing (70)Throbbing (70)bull Aggravation by movement Aggravation by movement bull Moderate to severe painModerate to severe pain
ICHD = International Classification of Hreadache DisordersAdapted from Cephalalgia 20048(suppl 1)S24-26
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine Without AuraMigraine Without Aura (contrsquod) (contrsquod)
And at least 1 of the following 2 symptomsAnd at least 1 of the following 2 symptoms
bull Nausea andor vomitingNausea andor vomitingbull Photophobia andor phonophobiaPhotophobia andor phonophobia
Not attributed to organic diseaseNot attributed to organic disease
Adapted from IHS Cephalalgia 2004
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine with AuraMigraine with Aura
At least 2 attacks withAt least 1 fully reversible symptom wo motor
Visual (flickering lights zigzags spots or lines andor loss of vision) + andor
Sensory (ldquopins and needlesrdquo andor numbness) + andor Dysphasic speech
Adapted from IHS Cephalalgia 2004
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

No pharmaceutical No pharmaceutical support or commercial support or commercial disclosuresdisclosures
Member of ARHP Member of ARHP expert advisory expert advisory committee on committee on Hormonal Migraines Hormonal Migraines and developed slide and developed slide set Many used in this set Many used in this presentationpresentation
Faculty DisclosureFaculty Disclosure
ldquoDespite the fact that it is so common and has so much impact on society migraine is one of the most misunderstood misdiagnosed and undertreated diseases on earthrdquo
Carolyn Bernstein MD The Migraine Brain
Why Care About MigraineWhy Care About Migraine Very Common neurologic Very Common neurologic
disorderdisorderbull UnderrecognizedUnderrecognizedbull UndertreatedUndertreated
Produces severe disability Produces severe disability 1212
Overuse of any drug may lead Overuse of any drug may lead
to chronic daily HAsto chronic daily HAs3434
IHS Headache Classification Subcommittee of the International Headache Society (IHS) The International Classification of Headache Disorders 2nd ed Cephalalgia 200424(Suppl1)139-41 1 Lipton RB et al Headache 200141646ndash657 2 Bigal ME et al Cephalalgia 2006 2643ndash49 3 Scher AI et al Pain 20031681ndash89 4 Bigal ME Lipton RB Headache 2006461334ndash1343 5 Kruit MC et al JAMA 2004291427ndash434 6 Kurth T et al JAMA 2006296283ndash291
Migraine in USAMigraine in USA
30 million migraine sufferers30 million migraine sufferers 1 in 10 persons a migraineur1 in 10 persons a migraineur 1 of 4 households include a migraineur1 of 4 households include a migraineur 99thth leading disability more common than diabetes leading disability more common than diabetes
or asthmaor asthmabull 30 of migraineurs have 3+ attacksmo30 of migraineurs have 3+ attacksmobull 75 have reduced ability to function75 have reduced ability to functionbull 50 are severely impaired50 are severely impaired
Lipton RB et al Headache 200141646ndash657
Migraine Co-morbiditiesMigraine Co-morbiditiesbull PMSPMSbull DepressionDepressionbull Anxiety disorders (generalized panic Anxiety disorders (generalized panic
bipolar OCD)bipolar OCD)bull AbusePTSDAbusePTSDbull StrokeStrokebull Irritable bowel syndromeIrritable bowel syndromebull EpilepsyEpilepsybull FibromyalgiaFibromyalgia
Epidemiology of Migraine in Epidemiology of Migraine in WomenWomen
Women are affected 3x more than menWomen are affected 3x more than men 20 million women in USA 20 million women in USA 40 of women in their lifetime40 of women in their lifetime
bull Before puberty equally prevalent in both sexes Before puberty equally prevalent in both sexes bull After puberty 3x more women than menAfter puberty 3x more women than menbull Peaks in midlifePeaks in midlifebull darrdarr after menopauseafter menopause
Lipton RB Headache 2001 Lipton RB Neurology 2007 Stewart Cephalalgia 2008
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine Without AuraMigraine Without Aura
At least 5 attacks with At least 5 attacks with Headache lasts 4ndash72 hours wo treatment or Headache lasts 4ndash72 hours wo treatment or
without successful treatmentwithout successful treatmentAt least 2 of the following four symptomsAt least 2 of the following four symptoms
bull Unilateral pain (60)Unilateral pain (60)bull Throbbing (70)Throbbing (70)bull Aggravation by movement Aggravation by movement bull Moderate to severe painModerate to severe pain
ICHD = International Classification of Hreadache DisordersAdapted from Cephalalgia 20048(suppl 1)S24-26
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine Without AuraMigraine Without Aura (contrsquod) (contrsquod)
And at least 1 of the following 2 symptomsAnd at least 1 of the following 2 symptoms
bull Nausea andor vomitingNausea andor vomitingbull Photophobia andor phonophobiaPhotophobia andor phonophobia
Not attributed to organic diseaseNot attributed to organic disease
Adapted from IHS Cephalalgia 2004
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine with AuraMigraine with Aura
At least 2 attacks withAt least 1 fully reversible symptom wo motor
Visual (flickering lights zigzags spots or lines andor loss of vision) + andor
Sensory (ldquopins and needlesrdquo andor numbness) + andor Dysphasic speech
Adapted from IHS Cephalalgia 2004
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

ldquoDespite the fact that it is so common and has so much impact on society migraine is one of the most misunderstood misdiagnosed and undertreated diseases on earthrdquo
Carolyn Bernstein MD The Migraine Brain
Why Care About MigraineWhy Care About Migraine Very Common neurologic Very Common neurologic
disorderdisorderbull UnderrecognizedUnderrecognizedbull UndertreatedUndertreated
Produces severe disability Produces severe disability 1212
Overuse of any drug may lead Overuse of any drug may lead
to chronic daily HAsto chronic daily HAs3434
IHS Headache Classification Subcommittee of the International Headache Society (IHS) The International Classification of Headache Disorders 2nd ed Cephalalgia 200424(Suppl1)139-41 1 Lipton RB et al Headache 200141646ndash657 2 Bigal ME et al Cephalalgia 2006 2643ndash49 3 Scher AI et al Pain 20031681ndash89 4 Bigal ME Lipton RB Headache 2006461334ndash1343 5 Kruit MC et al JAMA 2004291427ndash434 6 Kurth T et al JAMA 2006296283ndash291
Migraine in USAMigraine in USA
30 million migraine sufferers30 million migraine sufferers 1 in 10 persons a migraineur1 in 10 persons a migraineur 1 of 4 households include a migraineur1 of 4 households include a migraineur 99thth leading disability more common than diabetes leading disability more common than diabetes
or asthmaor asthmabull 30 of migraineurs have 3+ attacksmo30 of migraineurs have 3+ attacksmobull 75 have reduced ability to function75 have reduced ability to functionbull 50 are severely impaired50 are severely impaired
Lipton RB et al Headache 200141646ndash657
Migraine Co-morbiditiesMigraine Co-morbiditiesbull PMSPMSbull DepressionDepressionbull Anxiety disorders (generalized panic Anxiety disorders (generalized panic
bipolar OCD)bipolar OCD)bull AbusePTSDAbusePTSDbull StrokeStrokebull Irritable bowel syndromeIrritable bowel syndromebull EpilepsyEpilepsybull FibromyalgiaFibromyalgia
Epidemiology of Migraine in Epidemiology of Migraine in WomenWomen
Women are affected 3x more than menWomen are affected 3x more than men 20 million women in USA 20 million women in USA 40 of women in their lifetime40 of women in their lifetime
bull Before puberty equally prevalent in both sexes Before puberty equally prevalent in both sexes bull After puberty 3x more women than menAfter puberty 3x more women than menbull Peaks in midlifePeaks in midlifebull darrdarr after menopauseafter menopause
Lipton RB Headache 2001 Lipton RB Neurology 2007 Stewart Cephalalgia 2008
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine Without AuraMigraine Without Aura
At least 5 attacks with At least 5 attacks with Headache lasts 4ndash72 hours wo treatment or Headache lasts 4ndash72 hours wo treatment or
without successful treatmentwithout successful treatmentAt least 2 of the following four symptomsAt least 2 of the following four symptoms
bull Unilateral pain (60)Unilateral pain (60)bull Throbbing (70)Throbbing (70)bull Aggravation by movement Aggravation by movement bull Moderate to severe painModerate to severe pain
ICHD = International Classification of Hreadache DisordersAdapted from Cephalalgia 20048(suppl 1)S24-26
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine Without AuraMigraine Without Aura (contrsquod) (contrsquod)
And at least 1 of the following 2 symptomsAnd at least 1 of the following 2 symptoms
bull Nausea andor vomitingNausea andor vomitingbull Photophobia andor phonophobiaPhotophobia andor phonophobia
Not attributed to organic diseaseNot attributed to organic disease
Adapted from IHS Cephalalgia 2004
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine with AuraMigraine with Aura
At least 2 attacks withAt least 1 fully reversible symptom wo motor
Visual (flickering lights zigzags spots or lines andor loss of vision) + andor
Sensory (ldquopins and needlesrdquo andor numbness) + andor Dysphasic speech
Adapted from IHS Cephalalgia 2004
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Why Care About MigraineWhy Care About Migraine Very Common neurologic Very Common neurologic
disorderdisorderbull UnderrecognizedUnderrecognizedbull UndertreatedUndertreated
Produces severe disability Produces severe disability 1212
Overuse of any drug may lead Overuse of any drug may lead
to chronic daily HAsto chronic daily HAs3434
IHS Headache Classification Subcommittee of the International Headache Society (IHS) The International Classification of Headache Disorders 2nd ed Cephalalgia 200424(Suppl1)139-41 1 Lipton RB et al Headache 200141646ndash657 2 Bigal ME et al Cephalalgia 2006 2643ndash49 3 Scher AI et al Pain 20031681ndash89 4 Bigal ME Lipton RB Headache 2006461334ndash1343 5 Kruit MC et al JAMA 2004291427ndash434 6 Kurth T et al JAMA 2006296283ndash291
Migraine in USAMigraine in USA
30 million migraine sufferers30 million migraine sufferers 1 in 10 persons a migraineur1 in 10 persons a migraineur 1 of 4 households include a migraineur1 of 4 households include a migraineur 99thth leading disability more common than diabetes leading disability more common than diabetes
or asthmaor asthmabull 30 of migraineurs have 3+ attacksmo30 of migraineurs have 3+ attacksmobull 75 have reduced ability to function75 have reduced ability to functionbull 50 are severely impaired50 are severely impaired
Lipton RB et al Headache 200141646ndash657
Migraine Co-morbiditiesMigraine Co-morbiditiesbull PMSPMSbull DepressionDepressionbull Anxiety disorders (generalized panic Anxiety disorders (generalized panic
bipolar OCD)bipolar OCD)bull AbusePTSDAbusePTSDbull StrokeStrokebull Irritable bowel syndromeIrritable bowel syndromebull EpilepsyEpilepsybull FibromyalgiaFibromyalgia
Epidemiology of Migraine in Epidemiology of Migraine in WomenWomen
Women are affected 3x more than menWomen are affected 3x more than men 20 million women in USA 20 million women in USA 40 of women in their lifetime40 of women in their lifetime
bull Before puberty equally prevalent in both sexes Before puberty equally prevalent in both sexes bull After puberty 3x more women than menAfter puberty 3x more women than menbull Peaks in midlifePeaks in midlifebull darrdarr after menopauseafter menopause
Lipton RB Headache 2001 Lipton RB Neurology 2007 Stewart Cephalalgia 2008
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine Without AuraMigraine Without Aura
At least 5 attacks with At least 5 attacks with Headache lasts 4ndash72 hours wo treatment or Headache lasts 4ndash72 hours wo treatment or
without successful treatmentwithout successful treatmentAt least 2 of the following four symptomsAt least 2 of the following four symptoms
bull Unilateral pain (60)Unilateral pain (60)bull Throbbing (70)Throbbing (70)bull Aggravation by movement Aggravation by movement bull Moderate to severe painModerate to severe pain
ICHD = International Classification of Hreadache DisordersAdapted from Cephalalgia 20048(suppl 1)S24-26
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine Without AuraMigraine Without Aura (contrsquod) (contrsquod)
And at least 1 of the following 2 symptomsAnd at least 1 of the following 2 symptoms
bull Nausea andor vomitingNausea andor vomitingbull Photophobia andor phonophobiaPhotophobia andor phonophobia
Not attributed to organic diseaseNot attributed to organic disease
Adapted from IHS Cephalalgia 2004
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine with AuraMigraine with Aura
At least 2 attacks withAt least 1 fully reversible symptom wo motor
Visual (flickering lights zigzags spots or lines andor loss of vision) + andor
Sensory (ldquopins and needlesrdquo andor numbness) + andor Dysphasic speech
Adapted from IHS Cephalalgia 2004
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Migraine in USAMigraine in USA
30 million migraine sufferers30 million migraine sufferers 1 in 10 persons a migraineur1 in 10 persons a migraineur 1 of 4 households include a migraineur1 of 4 households include a migraineur 99thth leading disability more common than diabetes leading disability more common than diabetes
or asthmaor asthmabull 30 of migraineurs have 3+ attacksmo30 of migraineurs have 3+ attacksmobull 75 have reduced ability to function75 have reduced ability to functionbull 50 are severely impaired50 are severely impaired
Lipton RB et al Headache 200141646ndash657
Migraine Co-morbiditiesMigraine Co-morbiditiesbull PMSPMSbull DepressionDepressionbull Anxiety disorders (generalized panic Anxiety disorders (generalized panic
bipolar OCD)bipolar OCD)bull AbusePTSDAbusePTSDbull StrokeStrokebull Irritable bowel syndromeIrritable bowel syndromebull EpilepsyEpilepsybull FibromyalgiaFibromyalgia
Epidemiology of Migraine in Epidemiology of Migraine in WomenWomen
Women are affected 3x more than menWomen are affected 3x more than men 20 million women in USA 20 million women in USA 40 of women in their lifetime40 of women in their lifetime
bull Before puberty equally prevalent in both sexes Before puberty equally prevalent in both sexes bull After puberty 3x more women than menAfter puberty 3x more women than menbull Peaks in midlifePeaks in midlifebull darrdarr after menopauseafter menopause
Lipton RB Headache 2001 Lipton RB Neurology 2007 Stewart Cephalalgia 2008
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine Without AuraMigraine Without Aura
At least 5 attacks with At least 5 attacks with Headache lasts 4ndash72 hours wo treatment or Headache lasts 4ndash72 hours wo treatment or
without successful treatmentwithout successful treatmentAt least 2 of the following four symptomsAt least 2 of the following four symptoms
bull Unilateral pain (60)Unilateral pain (60)bull Throbbing (70)Throbbing (70)bull Aggravation by movement Aggravation by movement bull Moderate to severe painModerate to severe pain
ICHD = International Classification of Hreadache DisordersAdapted from Cephalalgia 20048(suppl 1)S24-26
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine Without AuraMigraine Without Aura (contrsquod) (contrsquod)
And at least 1 of the following 2 symptomsAnd at least 1 of the following 2 symptoms
bull Nausea andor vomitingNausea andor vomitingbull Photophobia andor phonophobiaPhotophobia andor phonophobia
Not attributed to organic diseaseNot attributed to organic disease
Adapted from IHS Cephalalgia 2004
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine with AuraMigraine with Aura
At least 2 attacks withAt least 1 fully reversible symptom wo motor
Visual (flickering lights zigzags spots or lines andor loss of vision) + andor
Sensory (ldquopins and needlesrdquo andor numbness) + andor Dysphasic speech
Adapted from IHS Cephalalgia 2004
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Migraine Co-morbiditiesMigraine Co-morbiditiesbull PMSPMSbull DepressionDepressionbull Anxiety disorders (generalized panic Anxiety disorders (generalized panic
bipolar OCD)bipolar OCD)bull AbusePTSDAbusePTSDbull StrokeStrokebull Irritable bowel syndromeIrritable bowel syndromebull EpilepsyEpilepsybull FibromyalgiaFibromyalgia
Epidemiology of Migraine in Epidemiology of Migraine in WomenWomen
Women are affected 3x more than menWomen are affected 3x more than men 20 million women in USA 20 million women in USA 40 of women in their lifetime40 of women in their lifetime
bull Before puberty equally prevalent in both sexes Before puberty equally prevalent in both sexes bull After puberty 3x more women than menAfter puberty 3x more women than menbull Peaks in midlifePeaks in midlifebull darrdarr after menopauseafter menopause
Lipton RB Headache 2001 Lipton RB Neurology 2007 Stewart Cephalalgia 2008
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine Without AuraMigraine Without Aura
At least 5 attacks with At least 5 attacks with Headache lasts 4ndash72 hours wo treatment or Headache lasts 4ndash72 hours wo treatment or
without successful treatmentwithout successful treatmentAt least 2 of the following four symptomsAt least 2 of the following four symptoms
bull Unilateral pain (60)Unilateral pain (60)bull Throbbing (70)Throbbing (70)bull Aggravation by movement Aggravation by movement bull Moderate to severe painModerate to severe pain
ICHD = International Classification of Hreadache DisordersAdapted from Cephalalgia 20048(suppl 1)S24-26
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine Without AuraMigraine Without Aura (contrsquod) (contrsquod)
And at least 1 of the following 2 symptomsAnd at least 1 of the following 2 symptoms
bull Nausea andor vomitingNausea andor vomitingbull Photophobia andor phonophobiaPhotophobia andor phonophobia
Not attributed to organic diseaseNot attributed to organic disease
Adapted from IHS Cephalalgia 2004
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine with AuraMigraine with Aura
At least 2 attacks withAt least 1 fully reversible symptom wo motor
Visual (flickering lights zigzags spots or lines andor loss of vision) + andor
Sensory (ldquopins and needlesrdquo andor numbness) + andor Dysphasic speech
Adapted from IHS Cephalalgia 2004
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Epidemiology of Migraine in Epidemiology of Migraine in WomenWomen
Women are affected 3x more than menWomen are affected 3x more than men 20 million women in USA 20 million women in USA 40 of women in their lifetime40 of women in their lifetime
bull Before puberty equally prevalent in both sexes Before puberty equally prevalent in both sexes bull After puberty 3x more women than menAfter puberty 3x more women than menbull Peaks in midlifePeaks in midlifebull darrdarr after menopauseafter menopause
Lipton RB Headache 2001 Lipton RB Neurology 2007 Stewart Cephalalgia 2008
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine Without AuraMigraine Without Aura
At least 5 attacks with At least 5 attacks with Headache lasts 4ndash72 hours wo treatment or Headache lasts 4ndash72 hours wo treatment or
without successful treatmentwithout successful treatmentAt least 2 of the following four symptomsAt least 2 of the following four symptoms
bull Unilateral pain (60)Unilateral pain (60)bull Throbbing (70)Throbbing (70)bull Aggravation by movement Aggravation by movement bull Moderate to severe painModerate to severe pain
ICHD = International Classification of Hreadache DisordersAdapted from Cephalalgia 20048(suppl 1)S24-26
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine Without AuraMigraine Without Aura (contrsquod) (contrsquod)
And at least 1 of the following 2 symptomsAnd at least 1 of the following 2 symptoms
bull Nausea andor vomitingNausea andor vomitingbull Photophobia andor phonophobiaPhotophobia andor phonophobia
Not attributed to organic diseaseNot attributed to organic disease
Adapted from IHS Cephalalgia 2004
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine with AuraMigraine with Aura
At least 2 attacks withAt least 1 fully reversible symptom wo motor
Visual (flickering lights zigzags spots or lines andor loss of vision) + andor
Sensory (ldquopins and needlesrdquo andor numbness) + andor Dysphasic speech
Adapted from IHS Cephalalgia 2004
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine Without AuraMigraine Without Aura
At least 5 attacks with At least 5 attacks with Headache lasts 4ndash72 hours wo treatment or Headache lasts 4ndash72 hours wo treatment or
without successful treatmentwithout successful treatmentAt least 2 of the following four symptomsAt least 2 of the following four symptoms
bull Unilateral pain (60)Unilateral pain (60)bull Throbbing (70)Throbbing (70)bull Aggravation by movement Aggravation by movement bull Moderate to severe painModerate to severe pain
ICHD = International Classification of Hreadache DisordersAdapted from Cephalalgia 20048(suppl 1)S24-26
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine Without AuraMigraine Without Aura (contrsquod) (contrsquod)
And at least 1 of the following 2 symptomsAnd at least 1 of the following 2 symptoms
bull Nausea andor vomitingNausea andor vomitingbull Photophobia andor phonophobiaPhotophobia andor phonophobia
Not attributed to organic diseaseNot attributed to organic disease
Adapted from IHS Cephalalgia 2004
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine with AuraMigraine with Aura
At least 2 attacks withAt least 1 fully reversible symptom wo motor
Visual (flickering lights zigzags spots or lines andor loss of vision) + andor
Sensory (ldquopins and needlesrdquo andor numbness) + andor Dysphasic speech
Adapted from IHS Cephalalgia 2004
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine Without AuraMigraine Without Aura (contrsquod) (contrsquod)
And at least 1 of the following 2 symptomsAnd at least 1 of the following 2 symptoms
bull Nausea andor vomitingNausea andor vomitingbull Photophobia andor phonophobiaPhotophobia andor phonophobia
Not attributed to organic diseaseNot attributed to organic disease
Adapted from IHS Cephalalgia 2004
ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine with AuraMigraine with Aura
At least 2 attacks withAt least 1 fully reversible symptom wo motor
Visual (flickering lights zigzags spots or lines andor loss of vision) + andor
Sensory (ldquopins and needlesrdquo andor numbness) + andor Dysphasic speech
Adapted from IHS Cephalalgia 2004
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

ICHD Diagnostic Criteria for ICHD Diagnostic Criteria for Migraine with AuraMigraine with Aura
At least 2 attacks withAt least 1 fully reversible symptom wo motor
Visual (flickering lights zigzags spots or lines andor loss of vision) + andor
Sensory (ldquopins and needlesrdquo andor numbness) + andor Dysphasic speech
Adapted from IHS Cephalalgia 2004
morehellip
IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

IHS Diagnostic Criteria for IHS Diagnostic Criteria for Migraine with AuraMigraine with Aura (contrsquod)(contrsquod)
bull Symptoms of aura develop gradually over Symptoms of aura develop gradually over gt5min or gt5min or different symptoms occur in different symptoms occur in succession over gt5 min succession over gt5 min
bull Each symptom last gt5 and lt60 min Each symptom last gt5 and lt60 min
bull Migraine begins with aura or within lt60 min Migraine begins with aura or within lt60 min
bull Symptoms are fully reversibleSymptoms are fully reversible
bull No organic diseaseNo organic disease
Adapted from IHS Cephalalgia 2004
Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Prevalence of MigrainePrevalence of Migraineby Age and Sexby Age and Sex
FemalesMales
Age (years)
20 30 40 50 60 70 80 1000
5
10
15
20
25
30
Migraine Prevalence
()
Lipton RB et al Headache 2001
Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Headaches and the Menstrual Headaches and the Menstrual CycleCycle
Adapted from Stewart WF et al Neurology 2000
12
10
8
6
4
2
0
Day of Menstrual Cycle
Pa
tie
nts
wit
h H
A (
)
Migraine without aura
Tension type
Migraine with aura
minus16 minus14 minus12 minus10 12 14 161086420minus8 minus6 minus4 minus2
HA = headache
Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Menstrual Migraines SubtypesMenstrual Migraines Subtypes(ICHD-2)(ICHD-2)
Menstrually Related Migraine (MRM)Menstrually Related Migraine (MRM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 2 out of 3 menstrual cycles and menstruation in at least 2 out of 3 menstrual cycles and additionally at other times of the cycleadditionally at other times of the cycle
~46 of women with migraine~46 of women with migraine
Pure Menstrual Migraine (MM)Pure Menstrual Migraine (MM)Attacks fulfill criteria for Attacks fulfill criteria for 11 Migraine without aura11 Migraine without auraAttacks occur days 1 Attacks occur days 1 plusmn 2 (ie days -2 to +3) of plusmn 2 (ie days -2 to +3) of
menstruation in at least 23 cycles and at no other time of menstruation in at least 23 cycles and at no other time of the cyclethe cycle
~14 of women with migraine ~14 of women with migraine
IHS Cephalalgia 2004
Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Distribution of Migraine Types in Distribution of Migraine Types in WomenWomen
bull 40 non-menstrual migraine
bull 60 menstrual migraine ndash MRM comprises the
majority of MM (46 of 60)
Female MigraineursMRM = menstrually related migraine MM = menstrual migraine
MRM 46
Non-menstrual Migraine
40
Pure MM 14
Mannix LK Calhoun AH Curr Treat Options Neurol 2004
Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Menstrual MigrainesMenstrual Migraines
Compared with attacks at other times of Compared with attacks at other times of the cycle menstrual attacks arethe cycle menstrual attacks are
bull More disablingMore disablingbull Longer in durationLonger in durationbull Less responsive to acute treatmentLess responsive to acute treatmentbull More likely to relapseMore likely to relapse
MacGregor EA Hackshaw A Neurology 2004 Dowson AJ et al Headache 2005
Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Non-HormonalNon-HormonalMigraine Triggers Migraine Triggers
bull HungerHungerbull Certain FoodsCertain Foodsbull DehydrationDehydrationbull SleepSleepbull Head and neck Head and neck
painspains
bull EmotionalEmotionalbull Environmental smoke Environmental smoke
bright lights change in bright lights change in weather weather
bull Concomitant diseaseConcomitant diseasebull SexSex
Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Hormonal Migraine Triggers Hormonal Migraine Triggers
bull Estrogen withdrawal or change in level Estrogen withdrawal or change in level MenstruationMenstruationPlacebo days with combined hormonal Placebo days with combined hormonal
contraceptivescontraceptivesPregnancyPregnancyPeri-menopausePeri-menopauseHormone replacement therapyHormone replacement therapy
Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 1 SarahCase 1 SarahNew Patient VisitNew Patient Visit
24-year-old non-smoker 24-year-old non-smoker Sexually activeSexually activeOn intake checks off On intake checks off
ldquoheadachesrdquo which she ldquoheadachesrdquo which she says are worse with her says are worse with her periodsperiods
Presents for Presents for contraceptioncontraception
Does Sarah have migraine
Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Use ldquoPINrdquo for Diagnosis of Use ldquoPINrdquo for Diagnosis of MigraineMigraine
Impairment Do your headaches limit you
Nausea Do you feel nauseated
Photophobia Does light bother you
Based on Lipton RB et al Neurology 2003
Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 1 SarahCase 1 Sarah
Accurate diagnosis of migraine aura is Accurate diagnosis of migraine aura is essential for the safe prescribing of essential for the safe prescribing of estrogen-containing contraceptionestrogen-containing contraception
Sarah has migraine Sarah has migraine without without aura She has no aura She has no other risk factors for strokeother risk factors for stroke
Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 1 SarahCase 1 Sarah Is Sarah eligible for estrogen-Is Sarah eligible for estrogen-
containing contraceptioncontaining contraception
A) A) YesYes
B) B) NoNo
Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 1 SarahCase 1 Sarah
bull Is Sarah eligible for estrogen-containing contraceptives Might she opt for a patch or ring
A) Yes Low-dose estrogen contraception can be used in women under age 35 who have migraine without aura and no other risk factors for stroke
B) No OCPs should never be used in women who have migraine
MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

MEC Headaches and CHCMEC Headaches and CHC
InitiateInitiate ContinueContinueNon-migrainous (mild or severe)Non-migrainous (mild or severe) 11 2 2MigraineMigraine
(i) without focal neurologic symptoms(i) without focal neurologic symptomsAge lt 35Age lt 35 22 3 3
Age gt 35Age gt 35 33 4 4(ii) with focal neurologic symptoms(ii) with focal neurologic symptoms 44 4 4 (at any age)(at any age)
photophonophobia NV are not focal symptomsphotophonophobia NV are not focal symptoms
Focal symptoms = vision changes numbness parasthesiasFocal symptoms = vision changes numbness parasthesiashttpwwwwhointreproductive-healthpublicationsRHR_00_2_medical_eligibility_criteria_3rd
Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Treatment of MigrainesTreatment of Migraines Education and behavior modificationEducation and behavior modification
Identify and avoid or modify triggersIdentify and avoid or modify triggers
Acute treatmentAcute treatment
Prophylactic treatment Prophylactic treatment bull Short-termShort-termbull Long-termLong-term
Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Treatment of MigrainesTreatment of Migraines TriptansTriptans more effective than NSAIDs and more effective than NSAIDs and
combination analgesics- warn about SEscombination analgesics- warn about SEs
NSAIDS can act synergistically with TriptansNSAIDS can act synergistically with Triptans
Phenothiazines PO or PR great for nausea amp Phenothiazines PO or PR great for nausea amp painpain
Think non-oral meds with nausea amp vomiting Think non-oral meds with nausea amp vomiting
Sleep can abolishes headache Sleep can abolishes headache
Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Options for Acute TherapyOptions for Acute Therapy AspirinAspirin IbuprofenIbuprofen Naproxen sodiumNaproxen sodium
Combination AnalgesicsCombination Analgesics Acetaminophen aspirin and caffeineAcetaminophen aspirin and caffeine
TriptansTriptans PhenothiazinesPhenothiazines
Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Rescue or Emergency Rescue or Emergency Treatment of MigraineTreatment of Migraine
When acute tx failsWhen acute tx fails
When HA returns in lt24 hrs or continues When HA returns in lt24 hrs or continues for daysfor days
IVIM phenothiazines in addition to DHE or IVIM phenothiazines in addition to DHE or a triptan work better than narcotics- a triptan work better than narcotics-
Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Prophylaxis of MigrainesProphylaxis of Migraines Consider prophylaxis if acute meds used Consider prophylaxis if acute meds used
gt 4xmo rescue meds gt 1xmo or gt 4xmo rescue meds gt 1xmo or headaches are functionally limitingheadaches are functionally limiting
Start prophylaxis at low dose and titrate Start prophylaxis at low dose and titrate up over 2-3 monthsup over 2-3 months
TCAs are effective independent of their TCAs are effective independent of their antidepressant effectantidepressant effect
Limited studies show biofeedback relaxation Limited studies show biofeedback relaxation training spinal manipulation and physical training spinal manipulation and physical therapy may be helpful therapy may be helpful
Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Medications for ProphylaxisMedications for ProphylaxisConsider hx co-morbidities and hormonal stateConsider hx co-morbidities and hormonal state TCAs- Amitrip best studied but most side effectsTCAs- Amitrip best studied but most side effects SNRIs (more effective then SSRIs)SNRIs (more effective then SSRIs) Beta- blockers- Beta- blockers-
Propranolol most studied and successful- Nadolol and Propranolol most studied and successful- Nadolol and Timolol tooTimolol too
Valproate Topiramate Gabapentin and other ldquoanti-Valproate Topiramate Gabapentin and other ldquoanti-convulsantsrdquo and ldquomood stabilizersrdquoconvulsantsrdquo and ldquomood stabilizersrdquo
BotoxBotox Verapamil and CCB- less effectiveVerapamil and CCB- less effective Hormonal Tx Hormonal Tx
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
SupplementsMagnesiumVitamin B2- riboflavinFeverfewButterbur (Petadolex)Coenzyme Q10 Omega-3 Fatty Acids Isoflavones
chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best chelated magnesium at 400-600 mgd for 3-4 months works as prophylaxis (best in pt w aura or perimenstrual migraine and those not responding to triptans) in pt w aura or perimenstrual migraine and those not responding to triptans) Riboflavin 400mgd for 3 months decrease migraine frequencyRiboflavin 400mgd for 3 months decrease migraine frequency
Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Preventive Options with Preventive Options with Non-pharmacologic ModalitiesNon-pharmacologic Modalities
Cognitivebehavioral ModalitiesCognitivebehavioral Modalities 1048707 1048707 MeditationMeditation Recognize and Avoid TriggersRecognize and Avoid Triggers Headache DiaryHeadache Diary
Physical ModalitiesPhysical Modalities Massage Massage Yoga Yoga AcupunctureAcupuncture 1048707 1048707 Osteopathic manipulationOsteopathic manipulation Peppermint oil ( Helpful for acute)Peppermint oil ( Helpful for acute)
Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Evaluating MigraineEvaluating Migraine Lab testsLab tests
Hormone Hormone TestsTests
Cat ScanCat Scan
Headache Headache DiaryDiary
Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Red FlagsRed Flags Headaches begin after age 50Headaches begin after age 50 Very sudden onset of HeadacheVery sudden onset of Headache First or worstFirst or worst Change in frequency or severityChange in frequency or severity ImmunosuppressionImmunosuppression Fever stiff neck rash traumaFever stiff neck rash trauma Focal neurologic symptoms or signsFocal neurologic symptoms or signs PapilledemaPapilledema
Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 1 SarahCase 1 SarahRecommended ApproachRecommended Approach
Migraine diaryMigraine diary
Counseling about migraine triggers and Counseling about migraine triggers and non-pharmacologic treatment optionsnon-pharmacologic treatment options
Her choice of hormonal non-hormonal Her choice of hormonal non-hormonal contraceptioncontraception
Acute treatment with triptanAcute treatment with triptan
Schedule 2-3 mo fu to review diarySchedule 2-3 mo fu to review diary
Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 1 SarahCase 1 SarahReturn VisitReturn Visit
Headache diary confirms menstrual related migraine 2ndash3 attacksmo without aura Severe attack during pill-free week
What do you do next
Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Options for Pharmacologic Options for Pharmacologic Treatment for MRMTreatment for MRM
RescueEmergency treatmentsIMIV phenothiazines or DHE
Prophylactic perimenstrual treatmentsNSAIDsSupplemental estrogenTriptansExtended cycle combined hormonal
contraceptives
Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Prophylactic Treatments for MM and Prophylactic Treatments for MM and MRM with Continuous hormonal therapyMRM with Continuous hormonal therapy
Continuous combined contraceptives Dedicated product Monophasic product throw away placebo Continuous cycling with ring
Estrogen back in hormone-free interval Mircette Yaz Supplemental estrogen
Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Migraine OCPs and StrokeMigraine OCPs and Stroke 6 per 100000 6 per 100000 year ndash healthy year ndash healthy 12 per 100000 12 per 100000 year ndash migraine year ndash migraine 18 per 100000 18 per 100000 year ndash migraine with aura year ndash migraine with aura
12 per 100000 12 per 100000 year ndash healthy and COC year ndash healthy and COC 19 per 100000 19 per 100000 year ndash migraine and COC year ndash migraine and COC 30 per 100000 30 per 100000 year ndash migraine with aura and COC year ndash migraine with aura and COC
34 per 100000 34 per 100000 year ndash stroke in pregnancy year ndash stroke in pregnancy
Attributable risk 7-19 per 100000 women per yearAttributable risk 7-19 per 100000 women per year ~ ~ 4000 year4000 year
So What about estrogen containing contraception in women with MigraineSo What about estrogen containing contraception in women with Migrainebull IHS low-dose estrogen in women with simple visual auraIHS low-dose estrogen in women with simple visual aura
bull ACOG progestin only intrauterine or barrier contraceptionACOG progestin only intrauterine or barrier contraception
bull WHO absolute contraindication in all women with auraWHO absolute contraindication in all women with aura
Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Prescribing Contraception in Prescribing Contraception in Women with MigrainesWomen with Migraines
Use a Progesterone Only method with auraUse a Progesterone Only method with aura
Lowest estrogen levels with ring Lowest estrogen levels with ring
Consider 20 or 25 mcg pillsConsider 20 or 25 mcg pills
Consider eliminating the placebo week Consider eliminating the placebo week
Follow-up in 1-3 months after initial RxFollow-up in 1-3 months after initial Rx
Stress need to discontinue method if Stress need to discontinue method if Migraines worsenMigraines worsen
Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 1 SarahCase 1 SarahTreatment and OutcomeTreatment and Outcome
Change 21-day OCPs to continuous hormonal therapy
For symptomatic treatment of migraine continue therapy with nsaids and triptans
Lifestyle modificationsMore regular mealsMore sleep and exerciseStress-reduction techniques
Follow up in 1-3 months
Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 2 PamCase 2 Pam
35-year-old woman6th week of pregnancyMenstrual migraine diagnosed 10 years agoMigraine more frequent and severe since
she became pregnant
Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Migraine and MRM in PregnancyMigraine and MRM in Pregnancy60 ndash 70 of migraineurs improve 60 ndash 70 of migraineurs improve
during pregnancy during pregnancy
Non-pharmacologic treatment is Non-pharmacologic treatment is preferredpreferred
BiofeedbackBiofeedbackRelaxation therapyRelaxation therapyCognitive-behavioral therapyCognitive-behavioral therapyMagnesiumMagnesium
MacGregor EA MacGregor EA J Fam Plann Reprod Health Care J Fam Plann Reprod Health Care 20072007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AcetaminophenAcetaminophen YY YY YY YY
CodeineCodeine (Y)(Y) (Y)(Y) (Y)(Y) YY
AspirinAspirin (Y)(Y) (Y)(Y) AvoidAvoid AvoidAvoid
DiclofenacDiclofenacIbuprofenIbuprofenNaproxenNaproxen
(Y)(Y) (Y)(Y) AvoidAvoid YY
DihydroergotamineDihydroergotamineErgotamineErgotamine
CICI CICI CICI CICI
Migraine Drug Use During Pregnancy and Lactation (Analgesics and Ergots)
YY = no evidence of harm = no evidence of harm(Y) (Y) == data suggest unlikely to cause harmdata suggest unlikely to cause harm(Y) (Y) = limited data but probably safe= limited data but probably safeCICI = contraindicated = contraindicated IDID = insufficient data = insufficient data = for emergency treatment of migraine = for emergency treatment of migraine not responding to standard measuresnot responding to standard measures
MacGregor EA J Fam Reprod Health Care 2007
DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

DrugDrug 1st Trimester1st Trimester 2nd Trimester2nd Trimester 3rd Trimester3rd Trimester LactationLactation
AlmotriptanAlmotriptanFrovatriptanFrovatriptan
IDID IDID IDID IDID
EletriptanEletriptan IDID IDID IDID YY
NaratriptanNaratriptanRizatriptanRizatriptan
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
SumatriptanSumatriptan (Y)(Y) (Y)(Y) (Y) (Y) YY
ZolmatriptanZolmatriptan IDID IDID IDID (Y)(Y)
Magnesium Magnesium sulphatesulphate
(Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
PrednisolonePrednisolone (Y)(Y) (Y)(Y) (Y)(Y) (Y)(Y)
Drug use during pregnancy and lactation (Triptans magnesium prednisolone)
MacGregor EA J Fam Reprod Health Care 2007
Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 2 PamTreatment and Outcome ReassuranceReassurance
bull Migraine may improve by the 2Migraine may improve by the 2ndnd trimester trimester particularly in women w history of menstrual particularly in women w history of menstrual migraine migraine
bull No evidence migraine will affect pregnancy outcomeNo evidence migraine will affect pregnancy outcome
AcuteAcutebull Acetaminophen NSAIDS Acetaminophen NSAIDS
bull Triptans (1-2nd trimester- may be safe- need Triptans (1-2nd trimester- may be safe- need more studies)more studies)
ProphylacticProphylacticbull If possible delay treatment until 2If possible delay treatment until 2ndnd trimester trimester
Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 2 Pam Case 2 Pam Treatment and OutcomeTreatment and Outcome (contrsquod) (contrsquod)
Propranolol Propranolol safe and effective and can be used safe and effective and can be used postpartum and during lactation (FDA C)postpartum and during lactation (FDA C)
bull Use lowest effective dose Use lowest effective dose bull Stop 2 to 3 days before deliveryStop 2 to 3 days before deliverybull Manage with neurologist or headacheManage with neurologist or headache
specialistspecialist
AmitriptylineAmitriptyline is another option is another option (FDA C)(FDA C)
Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 3 HannahCase 3 Hannah52-year-old womanPresents with headache5-year history of menstrual
migraine and occasional attacks of migraine with aura
Hot flashes mood swingsAsks about hormone therapy
Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Menstrual Migraine and Menstrual Migraine and Hormone Therapy (HT)Hormone Therapy (HT)
Lowest and Non oral routes are best
Evaluate risk factors for stroke and CAD
Migraine with aura is not a contraindication to HT in low risk women (no RCTs expert opinion)
If aura 1st appears after start of HT reduce estrogen and consider work up for TIA
Macgregor EA Migraine the menopause and hormone replacement therapy a clinical review J Fam Plann Reprod Health Care 200733(4)245-9 Macgregor EA Estrogen replacement and Migraine Maturitas Volume 63 Issue 1 20 May 2009 Pages 51-55
Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Case 3 HannahCase 3 HannahTreatment and OutcomeTreatment and Outcome
Acute treatment with NSAIDS amp triptansAcute treatment with NSAIDS amp triptans
Low-dose non-oral estradiol AND continuous progestin (if Low-dose non-oral estradiol AND continuous progestin (if needed)needed)
Hannahrsquos migraine attacks increase when HT is initiated Hannahrsquos migraine attacks increase when HT is initiated but improve with continued usebut improve with continued use
Fluoxetine amp venlafaxime useful migraine prophylaxis and Fluoxetine amp venlafaxime useful migraine prophylaxis and treat hot flashestreat hot flashes
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Diagnostic CriteriaDiagnostic Criteria Headache 15 or Headache 15 or more daysmonth for at least 6 monthsmore daysmonth for at least 6 months
Preventable with accurate medication Preventable with accurate medication history history
Speaks to early use of prophylaxisSpeaks to early use of prophylaxis
Depression anxiety and drug abuse may Depression anxiety and drug abuse may complicate presentationcomplicate presentation1 Cephalalgia 20048 (suppl 1)S24ndash26 2 Bigal ME et al Cephalalgia 200727568
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Chronic Daily Headache (CDH)Chronic Daily Headache (CDH) AKA rebound headacheAKA rebound headache chronic tension- chronic tension-
type medication induced transformed type medication induced transformed migrainemigraine
CDH caused by CDH caused by overuse of acuteoveruse of acute meds meds
Unrecognized epidemicUnrecognized epidemic majority of majority of referrals to headache clinicsreferrals to headache clinics
Disabling and expensive Disabling and expensive
Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Chronic Daily Headache (CDH)Chronic Daily Headache (CDH)
Taper off acute medications Taper off acute medications Overuse of NSAIDs tylenol narcotics Overuse of NSAIDs tylenol narcotics
typicaltypical May require hospitalization May require hospitalization 6 RCTs showed sig improvement w 6 RCTs showed sig improvement w
AmitriptylineAmitriptyline The longer one has CDH the harder it is The longer one has CDH the harder it is
to treatto treat Steroids may be helpful during taper Steroids may be helpful during taper
Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Creating a Supportive Office Creating a Supportive Office EnvironmentEnvironment
Educate patients Educate patients and entire and entire healthcare teamhealthcare team
Make adjustments Make adjustments in your officein your office
bull LightLightbull OdorsmellsOdorsmellsbull NoiseNoisebull ChemicalChemical
Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Summary Behavioral and Summary Behavioral and Lifestyle Modifications Lifestyle Modifications
Avoid dietary emotional and Avoid dietary emotional and environmental triggersenvironmental triggers
Eat regular healthful mealsEat regular healthful mealsGet the right amount of sleepGet the right amount of sleepGet regular exerciseGet regular exerciseLearn stress management techniquesLearn stress management techniques
Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

Summary Pharmacologic TxSummary Pharmacologic TxAcute treatment (NSAIDs triptans) Rescue Tx- DHE phenothiazinesProphylactic treatmentPerimenstrual (NSAIDs estrogen triptan) if
Response to acute tx inadequateRegular predictable periods
Continuous (extended cycle contraception) ifPatient needs contraceptionPatient has irregular periodsOther strategies fail
A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses

A range of behavioral and drug options exist for the management of severe migraine
Take-Home PointsTake-Home PointsMigraine is a neurological illness caused by abnormality in
brain chemistry
A substantial proportion of women with migraine experience increased incidence around onset of menses
Short-term prevention is the best approach for these women if they have regular menses