Embed Size (px)
DESCRIPTION
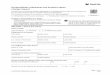
Withdrawal request form for campus use.
Citation preview

Signator of fund Date
Second Signature Date
Name
Senior campus Administrator (if required)
City
State ZIP
Mail to Payee Hold for pickup
Mail to: YES NO
Name
City YES NO
State ZIP
Invoice # Acct # Fund GL Acct Function
Project
Program Amount
TOTAL: $0.00 $0.00
Payee Social Security Number
REQUEST FOR WITHDRAWAL OF FUNDS (rev 2009-07)
AUTHORIZED BY:
7. IS THIS A REQUEST FOR AN HONORARIUM, CONSULTING
FEE OR CONTRACTED SERVICE PAYMENT? (If yes, attach contract
or service agreement.)
1. NAME OF FUND
2. AMOUNT OF PAYMENT
3. PURPOSE OF WITHDRAWAL (attach original documentation)
FUND #
Address
Same as Above
PROJECT #
5. SEND CHECK TO (check one): 6. IS THIS A REQUEST FOR AN ADVANCE? (If yes, original
documentation is required within 30 days of the advance being issued.)
4. MAKE CHECK PAYABLE TO:
Address
This total MUST equal the amount listed on step 2, above:
8. Complete (non-shaded) columns below, as needed.
Memos/additional information

![Separation from Employment Withdrawal Request 401(k) Plan · Separation from Employment Withdrawal Request 401(k) Plan STD FSPSRV ][04/18/18)(934512-02 WITHDRAWALNO_GRPG 283098/][GU19][KAGUDOC](https://img.pdfslide.us/doc/110x75/5ebd1f2c8cc9fa349b1e6072/separation-from-employment-withdrawal-request-401k-plan-separation-from-employment.jpg)




















![Disability Withdrawal Request 401(k) Plan · Disability Withdrawal Request 401(k) Plan STD FDSTDB ][04/07/17)(98960-01 WITHDRAWAL NO_GRPG 421/][GU22)(/][GP22 DOC ID: 477279085 Page](https://img.pdfslide.us/doc/110x75/5b646e127f8b9a3c5e8d4320/disability-withdrawal-request-401k-plan-disability-withdrawal-request-401k.jpg)


![In-Service Withdrawal Request Governmental 457(b) PlanIn-Service Withdrawal Request Governmental 457(b) Plan STD FINSRV ][06/03/19)(98953-01 WITHDRAWAL NO_GRPG 57617/][GU22)(/][JMCG](https://img.pdfslide.us/doc/110x75/5f42755aaa9b9419f36df629/in-service-withdrawal-request-governmental-457b-plan-in-service-withdrawal-request.jpg)