Embed Size (px)
Citation preview

12/10/2018
1
WisPQC
Eat, Sleep, Console
Webinar for NAS/NOWS
Initiative
December 6, 2018
12:00-1:00 p.m.
GoToWebinar®
ESC Development
• Developed by a collaborative effort between faculty at
Yale, Children’s Hospital at Dartmouth-Hitchcock and
Boston Medical Center
Key Elements of Eat, Sleep, Console Care Tool
• First treatment should be non-pharmacologic
• All opioid-exposed infants should be monitored in the
hospital for 4-7 days for signs of withdrawal – per
AAP
• Some infants may require pharmacologic treatment
(replacement opioids)
Rationale for Pharmacologic Treatment
• Finnegan Scale: most commonly used to foNAS symptoms
• Typically, Finnegan scores consecutively of 8 or greater are used
to initiate and titrate pharmacologic treatment
• Rationale for using a score of 8 for medication has never been
scientifically established or validated
• Recent studies: Finnegan scoring poor psychometric properties
• New research suggests pharmacologic treatment should be
based on function-based assessments (how well the infant is
eating, sleeping, and infant comfort).
Pharmacologic Treatment
• If non-pharmacologic care has been optimized and the infant
continues to have poor eating, sleeping, or consoling, then
pharmacologic treatment should be considered
–After a team huddle and
–After maximal optimization of non-pharmacologic care
• 10 – 40 % of infants will require pharmacologic treatment:
–Usually initiating treatment at 3 – 4 days of life for
methadone and buprenorphine-exposed infants
–Usual rate of 50 – 80 % pharmacologic treatment when
using a numerical, score based approach
ESC Primary Focus
• The ESC method’s sole principle is that treatment of
infant (both non-pharmacologic and pharmacologic
treatment) should be based on infant function and
comfort, rather than reducing signs and symptoms of
withdrawal.
• Focus on the parent as primary caregiver.

12/10/2018
2
Timing and Location of ESC Assessments
• Assessments should be initiated within 4-6 hours of birth
• Assessments should continue for 4-7 days for infants exposed to long-acting
opioids (i.e. Buprenorphine, Methadone)
• Assessments should continue for a minimum of 48 hours for shorter-acting
opioids (i.e. Oxycodone, Codeine)
• Assessments should be performed every 3-4 hours at the time of other
routine infant care (i.e. feeding, assessment of vital signs)
• Should incorporate input from all infant caregivers who interacted with infant
during the time period assessed (i.e. mother, other parent, nurse, cuddler)
• Do not need to remove infant from mother/other parent/caregiver if being
held
Implementation Expertise
• Copyrighted material that we had to get
written permission to use and add to Epic.
• We will also need to share data with the
authors as part of copyright permission.
• Grossman, M. et al., Hospital Pediatrics. 2018;8(1):1-6
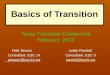
The Eat, Sleep and Console (ESC)
Approach
Grossman, M. et al., Hospital Pediatrics.
Outcomes Using the ESC Approach
Predicted Outcomes Using the Finnegan’s
Approach
p - value
Infants with NAS receiving morphine, n (%)
Hospital Days, n (%)No MorphineIncreased Morphine DoseDecreased Morphine Dose
Same Morphine Dose
6 (12)
258 (87.2)8 (2.7)
21 (7.1)
9 (3.0)
31 (62)
156 (52.7)76 (25.7)35 (11.8)
29(9.8)
< 0.001
< 0.001< 0.001< 0.001
< 0.001
Outcomes
Grossman, M. et al., Hospital Pediatrics. 2018;8(1):1-6
The ESC approach limits pharmacologic treatment (98% to 12%) and may lead to reductions in length of stay (22.5 days to 5.9 days).
Decrease the LOS of Infants
with NAS
Nonpharmacologic Interventions
Standardized non pharmacologic care
Prenatal counseling of parents
Parental/Volunteer presenceSimplified
assessment of infants
Implementation of the ESC Approach
Decreased use of
Morphine
Rapid Morphine weans
Education of Caregivers
Empowering messaging to
parents
Train Nurses and Pediatricians in ESC
Approach
Key Drivers Interventions
Primary Aim
30-day readmission rates
adverse clinical events/NICU
transfers
weight change during readmission
Balancing/Safety Measures
Overall Goal
Improve the
family-centered
care of Infants
with NAS

12/10/2018
3
Key Interventions:
Education of Nurses and Physicians on recent NAS literature and ESC Approach
Revised Scoring System for NAS using the ESC Approach
Revised Pharmacotherapy Guideline for NAS
Revised EPIC NAS order set including workflow sheet for ESC approach
Who is Scored?
• All Infants suspected of Prenatal Exposure to Narcotics
(Positive drug screen for mother or baby, H/O substance
use during pregnancy, inadequate prenatal care) will be
screened.
• Screening to be completed using the ESC Scoring with the
Finnegan tool every 2-4 hours and only when patient is
awake.
When/Where/How is Infant Scored?
• ESC assessments should be performed every 2-4 hours at the
time of routine cares or feedings.
• Initial assessment should be completed within 2 hours of birth
and continues based on the length of time required for the
type of infant exposure. (See Neonatal Abstinence Policy)
• All assessments should reflect the interval timeframe since last
ESC assessment.
• Assessments should be completed in their own room and
remain with their mother (or visiting caregiver) as much as
possible.
When/Where/How is Infant Scored?
• ESC assessments are documented in the EMR ESC flow
sheet until discontinued by physician.
• Continue to use ESC & Finnegan Scoring when
receiving pharmacological treatment in SCN.
• If receiving pharmacologic treatment, should continue
ESC assessments for 24 hours following treatment
discontinued.
Documentation in Epic
MUST ADD:
ESC found under Neuro
in the NB PCS Body
System Flowsheet

12/10/2018
4
Define Newborn: EAT……
• Breast feeding or Bottle feeding well
– Breast: latches deeply with comfortable latch for mother and sustains active suckling with only brief pauses
– Bottle: effectively coordinates suck and swallow without gagging or excessive spitting up
• Eating 10 ml of finger or bottle feeding each feeding
• Indicated if clearly a non- NAS related issue (prematurity, spittiness or sleepy first 24 hours, or inability to latch/suck due to infant/maternal anatomical factors)
• If unclear if poor feeding is due to NAS, continue to monitor infant while using non-pharm interventions
• No • Poor feeding due NAS symptoms
(fussiness, tremors, uncoordinated or excessive suck)
• Unable to coordinate feeding within 10 minutes of hunger cues
• Unable to sustain suck/latch within 10 minutes of initiating feeding
• Any excessive spitting up or emesis with feeding
Yes
Define Newborn: Sleep ……
• Yes
• Able to sleep for 1 hour or longer after feeding
• Indicate if sleeps <1 hour is clearly related to non-NAS factors (cluster feeding, interruptions for routine newborn care, symptoms in first day likely due to nicotine or SSRI withdrawal)
• If unclear if sleep < 1 hour is due to NAS, continue to monitor infant while using non-pharm interventions
• No
• Sleeps < 1 hour due to NAS symptoms ( fussiness, restlessness, increased startle reflex, tremors)
This image cannot currently be displayed.
Define Newborn: Console ……
Yes
• Infant consoles easily with 10 minutes using CSIs.
CSIs: (Consoling Support Interventions)
• Caregiver begins softly & slowly talking to infant and uses his/her voice to calm infant.
• Caregiver looks for hand-to-mouth movements and facilitates by gently bringing infant’s hand to mouth.
• Caregiver continues talking to infant while placing hand firmly but gently on infant’s abdomen.
• Caregiver continues softly talking to infant while bringing arms & legs to the center of their body.
• Caregiver picks up infant, holds skin-to-skin or swaddled, and gently rocks or sways infant.
• Caregiver offers a finger or pacifier for infant to suck, or a feeding if infant is showing hunger cues.
• Indicate if inconsolable due to hunger, difficulty feeding, or non-NAS source of discomfort.
• If unclear if the inability to console is due to NAS, continue to monitor infant while using non-pharm interventions
No
• Infant inconsolable within 10 minutes of caregivers providing comfort & supporting interventions
• Excessive crying and restlessness for over 10 minutes with interventions provided

12/10/2018
5
Non-Pharm Interventions include…
• Rooming-in with parent throughout the hospital stay
• Ensuring parental presence at the bedside as often as possible during the hospital stay
• Encouraging skin-to-skin contact
• Swaddling/flexed positioning
• Ensuring optimal feeding quality including encouraging breastfeeding for mother without
concerns for continued concerning substance use or other medical contraindication
• Non-nutritive sucking with pacifier or finger (ensuring baby is well fed first)
• Ensuring a quiet environment with low light stimulation in the room.
• Limiting visitors to one at a time (and to those that will be quiet/supportive)
• Providing uninterrupted periods of sleep/clustering infant’s care
• May use noise machine at infant bedside not within infant’s crib.
• Use of swing only during daytime and when caregiver is awake. Caregiver must be continuously
observing infant while in swing. (Swing must be removed when not in use or at night time.)
NAS Rooming-In and Visiting Caregiver
Guidelines/Expectations
• Infants exposed/withdrawing require close
observation and some special care. A great way to
help them is to room-in with them as much as
possible and provide them loving care and support.
We understand that there may be a times, you may
need to step away from your infant for
appointments or other childcare responsibilities.
The follow are the guidelines to establish a visiting
caregivers list in your absence.
• Rooming-in strongly encouraged at all times.
• All caregivers will use safe sleep practices.
NAS Rooming-In and Visiting Caregiver
Guidelines/Expectations
• Rooming-in strongly encouraged at all times.
• All caregivers will use safe sleep practices.
• All caregivers will use good hand hygiene.
• Banded parents may only be gone for 4 hours per
day unless medically indicated.
• ONLY banded parents may room in overnight with
infant.
NAS Rooming-In and Visiting Caregiver
Guidelines/Expectations
• A banded parents or Verified visiting caregiver should be present with infant at all times. Visiting caregiver is responsible to attend to infant’s needs until parents return.
• Banded parent MUST notified RN when leaving unit for visiting caregiver to be verified and given proper badge. Visiting caregiver must have photo ID to assume cares. Once banded parent returns RN to be notified.
• Visiting caregivers list will be established once mother is medically discharged. Maximum of 4 adults can be on the list.
Nursing Workflow1. Identify NAS Infant.
2. Initiate NAS protocol.
3. Educate Parents on ESC & Finnegan Scoring Tools.
4. Begin Scoring at 2 hours of age. Then every 2-4 hours to follow while infant is awake until discontinued or discharged home.
5. Follow ESC Algorithm for appropriate interventions and when to notify Healthcare provider. (ESC Algorithm to follow and laminated in all baby charts)
6. RN should accompany physician when rounding for accurate continuity of infant’s care with parents.
7. RN should write a progress note after two scoring assessment with ESC with answers of “no” or when any update of physician is completed.
8. Rounding: Should be done minimally of every hour by RN, more frequent check ins and observations of feeds and cares required for NAS support and education of caregivers. ( would be great to have NAS patient placed in rooms 2506,2507, or 2509 for better observation and workflow)
9. Initiate Substance exposed/Neonatal abstinence care plan.

12/10/2018
6
Start ESC Scoring together with Finnegan Scoring every 2-4 hours and only when
patient is awake
ESC Scoring involves documenting an answer of “YES” or “NO” to the following
questions:•Can an infant breastfeed well or eat > 10ml per feeding (finger or bottlefeeding)•Can an infant sleep > 1 hour?•Can an infant be consoled within 10 minutes?
Continue to monitor ESC Scoring together with Finnegan Scoring
every 2-4 hours and only when patient is wake until physician discontinues the order
Start the nonpharmacologicintervention that may include the
following: •Feeding on demand•Swaddling and holding•Low stimulation environment•Parental/Volunteer presence
“YES” to all three questions
“NO” to any question
“NO” to any question
“YES” to all three
questions
Two consecutive ESC scoring
documentations of any “NO”
Call Healthcare provider
or Pediatrician On-Call
for increase in
pharmacotherapy
EAT, SLEEP AND CONSOLE (ESC) ALGORITHM FOR NURSES
Discontinue scoring 24 hours after pharmacotherapy is discontinued
Continue to monitor ESC Scoring together with Finnegan Scoring
every 2-4 hours and only when patient is wake until physician discontinues the order
Discontinue CR monitor and pulse oximeter once off
pharmacotherapy
“YES” to all three questions
Call Healthcare provider
or Pediatrician On-Call
for pharmacotherapy
Any two consecutive ESC scoring
documentations of any “NO”
Once on pharmacotherapy, admit to SCN, place on CR monitor and
pulse oximeter
If Patient falls outside of the algorithm, questions, or concerns, consult Healthcare
Provider or On-Call Pediatrician for further care instructions.
EAT, SLEEP AND CONSOLE (ESC) ALGORITHM FOR NURSES (continued)
EAT, SLEEP AND CONSOLE PARENT EDUCATION
Eat, sleep and console is a way to watch your baby for signs of substance withdrawal. The nurse watches your baby closely for the
recommended stay advised by your doctor. The nurse will score your baby every 2 to 4 hours while baby is awake. The nurse scores
“yes” or “no” for eat, sleep and console. The nurse is watching baby for the following signs of withdrawal.
EAT
Baby will be scored for poor eating if:
• Baby can’t eat within 10 minutes of acting hungry
• Baby can’t eat at the breast well AND/OR with a bottle/syringe/finger of 10 mL because baby is fussy, shaking, or is sucking extra
GOOD FEEDINGS:
• Baby eating early with hunger signs without any limit on how long baby eats or the amount
• Breastfeeding: Baby can latch deep and with a comfortable latch for mother. Baby is actively sucking only taking small breaks. If
you need help with breastfeeding please ask for help from lactation or nurses.
• Bottle Feeding: Baby can eat without gagging, drooling or spitting up. If you need help with bottle feeding please ask for help
from the nurses. Nurses can help and see if baby needs a different bottle position or type of nipple.
SLEEP
Baby will be scored for poor sleeping if:
• Baby sleeps less than 1 hour after eating because baby is fussy, shaking and uneasy or is easily scared
• The nurses can help provide hints for helping baby sleep safely
CONSOLE
Baby will be scored if they are not able to be comforted if:
• Baby continues to cry and be fussy for 10 minutes or more and can’t be comforted by the person caring for the baby
• A great way to help your baby be comfortable in its new world is to have baby in the room with you as much as possible and give
them loving care and support.
Parental EducationESC Scoring:
• We are scoring based on infant’s ability to function. Is the infant able to eat, sleep, and be comforted?
• Infant is scored every 2-4 hours while awake only. Do not wake infant to score.
• Infant will be scored using ESC and Finnegan scoring tools.
• Infant will be treated based off the ESC scoring tool.
– If infant scores a “no” for two consecutive ESC scoring assessments then Healthcare Provider is contacted to discuss pharmacotherapy treatment.
– If pharmacotherapy treatment is ordered, infant is admitted into SCN.
• Non-pharmacologic interventions should be initiated, taught, and reinforced with parents/caregivers.
Rooming In:• Parental involvement is strongly recommend
to provide the best comfort & support for the infant.
• Once mother is discharged, a Visiting Caregivers list can be established and utilized in times when a parent can not be present.
– Parents can not be absent for more than 4 hours in a day.
– Only 4 adults (greater than 18 years old) can be placed on Visiting Caregivers list.
– Visiting Caregiver must have a ID with them and be validated by Birth Center RN prior to assuming cares and parent leaving.
• Must obtain a badge identifying them as the Visiting Caregiver.
– Visiting Caregiver must remain in patient room caring for infant at all times. May call RN for assistance as needed or if needs to leave before parents return.
– NO Visiting Caregivers allowed to overnight stay. Only Parents!!
– Parents must keep Identification bracelets on until infant is discharged.
• Reinforce Safe Sleep Practices & Guidelines for parents/caregivers to follow.
WAYS TO HELP COMFORT BABY
Page 1
• Picks up baby
• Holds baby skin-to-skin or swaddled in blanket
• Gently rocks baby
• Talking softly and slow to calm baby down
• Keep talking calmly to infant and place hand firm but softly on baby’s belly
• Gives pacifier or finger for baby to suck on
• Person caring for baby looks for hunger signs and helps bring infant’s hand to mouth to help calm baby
• Feeding baby if they are acting hungry
• Sound machine in room
• Hospital swing use in room only during the day when baby is being watched
• If your baby can not eat, sleep and console easily for more than one scoring the nurse will contact your baby’s doctor to talk about possible changes in care.
NAS Rooming-In and Visiting Caregiver
Guidelines/ExpectationsInfants that are exposed and withdrawing from drugs require close observation and some special care. A great way to help them is to room-in with them as much as possible and provide them loving care and support. We understand that there may be a times, you may need to step away from your infant for appointments or other childcare responsibilities. The follow are the guidelines to establish a visiting caregivers list in your absence.
• Rooming-in strongly encouraged at all times.
• All caregivers will use safe sleep practices.
• All caregivers will use good hand hygiene.
• Banded parents may only be gone for 4 hours per day unless medically indicated.
• ONLY banded parents may room in overnight with infant.
• A banded parent or a verified visiting caregiver should be present with infant at all times. Visiting caregiver is responsible to attend to infant’s needs until parents return.
• Banded parent MUST notified RN when leaving unit for visiting caregiver to be verified and given proper badge. Visiting caregiver must have photo ID to assume cares. Once banded parent returns RN to be notified.
• Visiting caregivers list will be established once mother is medically discharged. Maximum of 4 adults can be on the list.
Infant’s Name___________________________
Parents (Banded Caregivers)
1.______________________
2.______________________
Visiting Caregivers:1.____________________________
2.____________________________
3.____________________________
4.____________________________
**** Found in SCN drawer ****

12/10/2018
7
• How to educate patients/families on the process
• How to accommodate mom’s longer stays
• Will ESC replace the Finnagen tool?
• How do we focus on ESC while keeping safe sleep
ChallengesUpcoming
WebinarMeetings:Invite your team of opioid project
champions to gather together
Nursing
Weekday Date Time Topic
Wed Dec 12 12:00– 1:00 pm Learning Collaborative Sessions: Schedule &
Format
Thank you.
For additional information,
contact Sue Kannenberg at
608-285-5858 ext. 205