Embed Size (px)
Citation preview

WINTHROPInstitute for Heart Care
Managing Mitral
Regurgitation in HF Patients:
Is it the Chicken or the Egg?
Srihari S. Naidu, MD, FACC, FSCAI, FAHAAssociate Professor of Medicine, SUNY – Stony Brook
Director, Cardiac Catheterization Laboratory,
Winthrop University Hospital, Mineola, NY
Past Trustee, SCAI ; Trustee, Brown University

WINTHROPInstitute for Heart Care
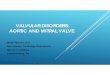
Classification of MR
Incompetent mitral
valve closure
Systolic retrograde blood flow
from the LV into the LA
Mayo Clinic (www.mayoclinic.com)
Primary
(Degenerative):Anatomic abnormality
of the mitral valve
• Leaflets
• Subvalvular
apparatus
• Chordae and
papillary muscles
Secondary
(Functional):LV dilation; often
secondary to ischemic
heart disease
• Leads to mitral
annular dilation
• Incomplete coaptation
of the mitral valve

WINTHROPInstitute for Heart Care
Classification of MR
Srihari S. Naidu, MD, MitraClip Program, Winthrop University Hospital
“The Valve” “The Ventricle”
Usually myxomatous Ischemic or not

WINTHROPInstitute for Heart Care
Chicken (LV) or Egg (MV)? How we’ve thought of things so far …
Primary MR LV Dysfx Mixed MR and
Worsening EF/HF
LV Dysfx Sec MR Worsening EF/HF
Fix the MR prior to LV dysfunction/AF/pHTN to avoid progression
If EF already reduced, probably still worthwhile to fix until EF < 20-25
Improve heart function to minimize MR and progression
-Revascularization
-Bi-V pacemaker/ICD
-Medications for Remodeling
Continued
3-4+ MR ?

WINTHROPInstitute for Heart Care
MR and LV Dysfunction
Increasing Mitral
Regurgitation
Increase
Load/Stress
Muscle
Damage/Loss
Dysfunction
of Left Ventricle
Dilation of
Left Ventricle1 year
mortality
up to
57%1
1 Cioffi G, et al. Functional mitral regurgitation predicts 1-year mortality in elderly patients with systolic chronic heart failure.
European Journal of Heart Failure 2005 Dec;7(7):1112-7
Both MR and LV Dysfunction
Contribute to Progressive
Heart failure and Secondary
Worsening of Each Other

WINTHROPInstitute for Heart Care
6
Prevalence of Valve Disease
According to Age
Nkomo et al. Burden of Valvular Heart Diseases: A Population-based Study,
Lancet, 2006; 368: 1005-11.
> 9.3% for ≥75 year olds
14
12
10
8
6
4
2
0
Pre
vale
nce (
%)
of m
odera
te
to s
evere
valv
e d
isease
Aortic valve disease
Age (years)
<45 45-54 55-64 65-74 >75
Mitral valve disease
All valve disease

WINTHROPInstitute for Heart Care
7
MR and Heart FailurePrevalence in CHF
Moderate or
severe MR
present in
40%
Heart Failure and significant MR are inseparable
Patel JB, et al. J Card Fail 2004;10:285-291; Go AS, et al. Circulation 2013;127:e6.
0
10
20
30
40
50
60
70
%
None
Moderate
Mod-Severe
Severe
Advanced Heart Failure

WINTHROPInstitute for Heart Care
The Egg: Degenerative
(Primary) MR

WINTHROPInstitute for Heart Care
9
Asymptomatic Primary MRNatural History
Avierinos JF, et al. Circulation 2002;106:1355
100
90
80
70
60
50
Surv
ival %
0 2 4 6 8 10
2 RF
1 RF
95 ±2
70 ±5
55 ±9
Risk Factors:
Age 50 yrs
Atrial fibrillation
LA enlargement
Flail
Mild MR
MR 3
or
EF <50%
Years after diagnosis

WINTHROPInstitute for Heart Care
10
Asymptomatic Primary MRSeverity and Survival
Enriquez-Sarano M et al. NEJM 2005;352:875-83
Worse Survival
100
90
80
70
60
50
0
Su
rviv
al (%
)
Years
0 1 2 3 4 5
P<0.01
ERO <20mm2 (91 ±3%)
ERO 40mm2 (58 ±9%)
ERO 20-39mm2
(66 ±6%)
More CV Events
70
60
50
40
30
20
10
0
Ra
te o
f C
ard
iac E
ve
nts
%
Years
0 1 2 3 4 5
P<0.01
ERO <20mm2 (15 ±4%)
ERO 20-39mm2
(40 ±7%)
ERO 40mm2 (62 ±8%)

WINTHROPInstitute for Heart Care
11
Flail Mitral LeafletNatural History
Ling L, et al. N Engl J Med 1996; 335:1417-1423
100
80
60
40
20
0
Surv
ival %
Years After Diagnosis
0 1 2 3 4 5 6 7 8 9 10
P<0.001
Class I or II
Class III or IV
Mortality4% per year
34% per year

WINTHROPInstitute for Heart Care
EF and Surgical Outcome
100
80
60
40
20
0
Surv
ival %
Years
0 1 2 3 4 5 6 7 8 9 10
EF 60%
EF 50-60%
EF <50%
P=0.0001
72 ±4%
53 ±9%
EF <60% is Abnormal in MR
32 ±12%
Enriquez-Sarano M, et al., Circulation 1994;90:830-837

WINTHROPInstitute for Heart Care
13
Symptoms and SurgeryOutcome with Primary MR
100
80
60
40
20
0
Surv
ival %
Years
0 1 2 3 4 5 6 7 8 9 10
NYHA I-II
NYHA III-IV
P<0.0001
90 ±2
76 ±5
73 ±3
48 ±4
Tribouilly CM et al., Circulation 1999;99:400-5

WINTHROPInstitute for Heart Care
14
Early Surgery Is BetterPatients without Class I Indications
100
80
60
40
20
0
Surv
ival %
Follow-up, y
0 5 10 15 20
Suri R et al., JAMA 2013;310:609-16
Early surgery
Medical management
Log-rank P<.001

WINTHROPInstitute for Heart Care
Summary for Primary MR
• Prognosis governed by:
– Number of related risk factors
– Severity (ERO or MR grade)
– Ejection Fraction
– NYHA Class
• Outcome governed by:
– Surgical repair/replacement once indicated
– Early consideration

WINTHROPInstitute for Heart Care
The Chicken: Secondary
(Functional) MR

WINTHROPInstitute for Heart Care
17
• Papillary muscle
displacement
Trichon BH, et al. Am J Cardiol 2003;91:538-43
Secondary Mitral RegurgitationA Ventricular Problem
Regional or
Global Dysfunction
• Annular flattening
• Leaflet tethering

WINTHROPInstitute for Heart Care
18
Secondary Mitral RegurgitationA Harbinger of Poor Outcome
Two-fold Increase Risk of DeathGrigioni F, et al. Circulation 2001;103:1759-64;
Basket JF, et al. Can J Cardiol 2007;23:797-800
1.0
0.8
0.6
0.4
0.2
0.0
Su
rviv
al (%
)
Years
0 1 2 3 4 5
P<0.001
50
40
30
20
10
0D
ea
th o
r h
ea
rt fa
ilure
ho
sp
ita
liza
tio
n %
Follow-up time (days)
0 365 730 1095
P=0.0006
MI w/o MR
MI with MR
61 ±6
38 ±5
Mitral
Regurgitation
No Mitral
Regurgitation
Post-MI SOLVD (EF >35%)

WINTHROPInstitute for Heart Care
19
Hospitalization-free survival decreased with
increased MR severity1
100
80
60
40
20
0
Ho
sp
ita
liza
tio
n-f
ree
Su
rviv
al (%
)
Years
0 1 2 3 4 5 6 7
P<0.01
No MR(40%)
Severe MR
7%)
Mild/mod MR
(25%)
Transplant-free survival decreased with
increased MR severity2
100
90
80
70
60
50
40
Tra
nsp
lant-
fre
e S
urv
iva
l (%
)
Days
0 500 1000 1500 2000
Grade IV
(46.5 ±6.7%)
Grade III
(68.5 ±4.6%)
Secondary Mitral RegurgitationIncreased Severity = Increased Morbidity
1. Rossi A, Dini FL, Faggiano P, et al. Independent prognostic value of functional mitral regurgitation in patients with heart failure: a quantitative analysis of 1256 patients with ischemic and non-ischaemic dilated cardiomyopathy. Heart. 2011;97(20):1675-1680.
2. Bursi F, Barbieri A, Grigioni F, et al. Prognostic implications of functional mitral regurgitation according to the severity of the underlying chronic heart failure: a long-term outcome study. Eur J Heart Fail. 2010;12(4):382-388.
Grade II
(64.4 ±4.9%)
No MR & Grade I
(82.7 ±3.1%)

WINTHROPInstitute for Heart Care
Surgery for Secondary MR
Wu AH, et al. J Am Coll Cardiol 2005;45:381-87No Mortality Benefit
1.0
0.8
0.6
0.4
0.2
0.0
Event-
fre
e S
urv
ival
Time (Days)
0 500 1000 1500 2000

WINTHROPInstitute for Heart Care
Summary for Secondary MR
• Prognosis governed by:
– Severity of MR
– Underlying degree of LV dysfunction, NYHA
class, and comorbidities
• Outcome not apparently improved by
surgical repair or replacement

WINTHROPInstitute for Heart Care
What are our options?
Untreated severe MR (degenerative OR functional) is associated with increased morbidity and mortality
Natural History Summary
For DMR and FMR

WINTHROPInstitute for Heart Care
23
Timing of SurgeryACC/AHA Guidelines – Primary MR
Consider surgery whenSymptoms
or
LV dysfunction (EF<60%, ESD≥40 mm)
Repair preferred over replacement
Nishimura R, et al., J Am Coll Cardiol 2014;63:2438-88

WINTHROPInstitute for Heart Care
24
Timing of SurgeryACC/AHA Guidelines – Primary MR
For patients without symptoms:
likelihood of repair success >95%
and
mortality rate <1%
Can be done if
Nishimura R, et al., J Am Coll Cardiol 2014;63:2438-88

WINTHROPInstitute for Heart Care
25
Surgical InterventionACC/AHA Guidelines – Secondary MR
Surgery may be considered for severe
symptoms despite optimal GDMT (IIb)
Also while undergoing other CV
surgery, if severe (IIa) or moderate (IIb)
Nishimura R, et al., J Am Coll Cardiol 2014;63:2438-88

WINTHROPInstitute for Heart Care
General Principles: The
World Prior to MitraClip
Primary
Surgery for symptoms or
LV dysfunction
Secondary
Asymptomatic pts
if repairable
and low risk
Revascularization and
Medical
therapy first
No medical
option for valve
Consider CRT
Surgery only in highly
selected patients with HF

WINTHROPInstitute for Heart Care
An Untreated Population
Total MR Patients1,2
Eligible for Treatment3,4
(MR Grade ≥3+)
4,100,000
1,700,000
Annual MV Surgery5
Annual Incidence3
(MR Grade ≥3+)250,000
30,000Only 2% Treated Surgically
14% Newly Diagnosed
Each Year
1,670,000
Untreated Large
and Growing Clinical
Unmet Need
1. US Census Bureau. Statistical Abstract of the US: 2006, Table 12.
2. Nkomo et al. Burden of Valvular Heart Diseases: A Population-based Study, Lancet, 2006; 368: 1005-11.
3. Patel et al. Mitral Regurgitation in Patients with Advanced Systolic Heart Failure, J of Cardiac Failure, 2004.
4. ACC/AHA 2008 Guidelines for the Management of Patients with Valvular Heart Disease, Circulation: 2008
5. Gammie, J et al, Trends in Mitral Valve Surgery in the United States: Results from the STS Adult Cardiac Database, Annals of Thoracic Surgery 2010.
Mitral Regurgitation 2009 U.S. Prevalence

WINTHROPInstitute for Heart Care
Would New Options Change
the Paradigm and Outcome?
Medical Therapy
Less Invasive
Increased MR Reduction
MV SurgeryMitraClip®

WINTHROPInstitute for Heart Care
MitraClip System

WINTHROPInstitute for Heart Care
Severe Myopathy and Severe MR:
Is The Clip an Option?
In DMR: Too Late, EF severely reduced,
surgery becomes risky
In FMR: Myopathy continues to progress,
there is an acute LV insult at surgery on an
already diseased heart, and/or complete
elimination of MR increases afterload

WINTHROPInstitute for Heart Care
279 Patients enrolled at 37 sites
Randomized 2:1
Echocardiography Core Lab and Clinical Follow-Up:
Baseline, 30 days, 6 months, 1 year, 18 months, and
annually through 5 years
Control GroupSurgical Repair or Replacement
N=95
Significant MR (3+-4+)Specific Anatomical Criteria
Device GroupMitraClip System
N=184
EVEREST II Randomized

WINTHROPInstitute for Heart Care
Primary Endpoints
Safety
• Major Adverse Event Rate at 30 days
• Per protocol cohort
• Superiority hypothesis
Effectiveness
• Clinical Success Rate– Freedom from the combined outcome of
• Death
• MV surgery or re-operation for MV dysfunction
• MR >2+ at 12 months
• Per protocol cohort
• Non-inferiority hypothesis
Pre-Specified MAEs
Death
Major Stroke
Re-operation of Mitral Valve
Urgent / Emergent CV Surgery
Myocardial Infarction
Renal Failure
Deep Wound Infection
Ventilation >48 hrs
New Onset Permanent Atrial Fib
Septicemia
GI Complication Requiring
Surgery
All Transfusions ≥2 units

WINTHROPInstitute for Heart Care
EVEREST 4 Year Results
Percutaneous
(n = 161)
Surgical
(n = 73)
P Value
Composite
Efficacy
Endpoint
39.8% 53.4% 0.070
Death 17.4% 17.8% 0.914
Surgery or Re-
operation for
Mitral Valve
Dysfunction
24.8% 5.5% < 0.001
MR 3+ or 4+ 21.7% 24.7% 0.745
Roughly 75% were DMR

WINTHROPInstitute for Heart Care

WINTHROPInstitute for Heart Care

WINTHROPInstitute for Heart Care
Age: 82 ±9 years
Prior MI: 24%
Prior stroke: 10%
Diabetes: 30%
COPD: 32%
Renal disease: 28%
Mean STS Risk
13.2%
Lim et al. Improved functional status and quality of life in prohibitive surgical risk
patients with degenerative mitral regurgitation after transcatheter mitral valve repair,
JACC 2014;64:182-192.
Prohibitive Surgical Risk
DMR Cohort (n=127)

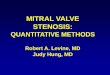
WINTHROPInstitute for Heart Care
Prohibitive Surgical Risk
DMR Cohort (n=127)
Left Ventricular Volumes
Hospitalizations for Heart Failure
Left Ventricular End Diastolic Volume Left Ventricular End Systolic Volume
(N = 69)Paired
Data(N=69)
0.67
0.18
0.0
0.2
0.4
0.6
0.8
1.0
1 Year Prior… 1 Year Post…
HF
Ho
spit
aliz
atio
n R
ate
pe
r P
atie
nt Y
ear
73% Reduction
125
109
60
70
80
90
100
110
120
130
140
Baseline 1 Year
Vo
lum
em
L
-16 mL
0
49
46
30
35
40
45
50
55
60
Baseline 1 Year
0
-3 mL
4+
4+
3+
3+
2+
2+
1+
1+
0%
20%
40%
60%
80%
100%
Baseline 12 Months
Patien
ts (%
)
Mitral Regurgitation Grade
0
1+
3+
4+
2+
I
II
IV
III

WINTHROPInstitute for Heart Care
The MitraClip Clip Delivery System is indicated for the
percutaneous reduction of significant symptomatic
mitral regurgitation (MR ≥ 3+) due to primary
abnormality of the mitral apparatus [degenerative
MR] in patients who have been determined to be at
prohibitive risk for mitral valve surgery by a heart
team, which includes a cardiac surgeon experienced
in mitral valve surgery and a cardiologist experienced
in mitral valve disease, and in whom existing
comorbidities would not preclude the expected
benefit from reduction of the mitral regurgitation.
MitraClip Indications

WINTHROPInstitute for Heart Care
Transcatheter Mitral Repair
May be considered for prohibitive risk patients
with primary MR and severe symptoms despite
GDMT (class IIb)
Why not functional MR??
ACC/AHA Guidelines – Primary MR

WINTHROPInstitute for Heart Care
Interaction of Age and MR Type

WINTHROPInstitute for Heart Care
41
Randomize 1:1
Clinical and TTE follow-up:
Baseline, Treatment, 1-week (phone)
1, 6, 12, 18, 24, 36, 48, 60 months
Control group
Standard of care
N=215
Symptomatic heart failure subjects who are treated per standard of care
Determined by the site’s local heart team as not appropriate for mitral valve surgery
Specific valve anatomic criteria
MitraClip
N=215
Significant FMR (≥3+ by core lab)
Trial DesignGoals: 430 patients at 75 US sites
Clinical Investigational Plan 11-512:
Version 5.1, November 11, 2013. COAPT
protocol approved by FDA July 27, 2012

WINTHROPInstitute for Heart Care
Summary of MitraClip
MitraClip therapy safely reduces DMR in patients at
prohibitive risk for MV surgery
In this group of prohibitive risk DMR patients, MitraClip
therapy provides meaningful clinical improvements
Reduction of LV volumes
Improvements in NYHA Functional Class
Improvements in Quality of Life
Reduction in Hospitalizations for Heart Failure
Results in FMR may be even better but await COAPT

WINTHROPInstitute for Heart Care
43
Is it the Chicken or the Egg?
Yes! But it doesn’t matter ….
as significant MR is always
contributory to worse prognosis
Managing MR in HF

WINTHROPInstitute for Heart Care
Thank You