Embed Size (px)
DESCRIPTION
The Magazine of the Sport Medicine Council of Alberta
Citation preview

The Magazine of The Sport Medicine Council of Alberta
Special Issue:
Sport Science
Winter 2006
pulse

2 SMCA Pulse Winter 2006
Winter 2006 Vol. 19 No. 1
SMCA SMCA Board of DirectorsBoard of Directors
President . . . . . .Dr. Gordon Bell, Ph.D.
Past -President . .Koralee Samaroden, BPE, PFLC
Vice-President . .Dwayne Laing, BPE, CAT (c)
Treasurer . . . . . . .Darren Turchansky, CA
Secretary . . . . . . .Jennifer Hanon
ASSM Rep . . . . . . .Position Currently Vacant
SPC Rep . . . . . . . . .Gabrielle Cave, BSc., P.T., MCPA
AATA Rep . . . . . . .Dwayne Laing, BPE, CAT (c)
SSAA Rep . . . . . .Dr. Gordon Bell, Ph.D.
SNS Rep . . . . . . . .Jane Dawson-Edwards, R.D.
Member at Large .Ray Kardas
SMCA SMCA E m p l o y e e sE m p l o y e e s
Executive Director . . . . . Ryan Petersen, BPE
Account Manager . . . . . . Janice Peters, BCom
Director of Programs
Services & Fundraising . Michael Pugh, BPE
Special Projects
Coordinator . . . . . . . . . . . . . Jennifer Johnson, BPE
Pulse Magazine Published by:Sport Medicine Council of Alberta
11759 - Groat RoadEdmonton, Alberta, Canada
T5M 3K6Phone: (780) 415 - 0812
Fax (780) 422 - 3093Website: www.sportmedab.ca
Email: [email protected]
Contents copyright 2005 by SMCA. Articles may not be reprintedwithout permission. The opinions are those of the respective
authors are not necessarily those of the SMCA.ISSN: 1181-9812
Publication agreement no. 40038086Subscriptions: 1 year $14.99 plus GST
Send subscription request and changes via email to:[email protected]
We gratefully acknowledge the financial support of AlbertaCommunity Development and the Alberta Sport, Recreation, Parks
and Wildlilfe Foundation, towards our editorial costs.
ppuullssee TT aa bb ll ee oo ff CC oo nn tt ee nn tt ssLatest News from the SMCA............................................................Page 3
Featured Articles:Female Athlete Issues: The Varsity Athlete at theUniversity of Alberta
Written By: V. Harber & J. Matthews-White
Pages 4 & 5
How Do You Spin It? An Examination of theBiomechanical Factors that Produce Spin on aVolleyball in the Skill of Spiking.
Written By: J. Pierre Baudin, P. Gervais & T. Wu
Pages 6 & 7
Breath In, Breath Out...The Effect of Off-SeasonTraining Programming for Edmonton Rowers: AComparison of Inspiratory to Expiratory BreathingMuscle Training on Pulmonary Measures andRowing Performance.
Written By: G. Bell, D. Syrotuik, A. & R. Jones
Pages 8 & 9
A Method for Increasing Cardiac Output in HighlyTrained Athletes.
Written By: D.J. Smith & M. A. McGillivray
Page 10
Modeling Maximal Instep Kick in Soccer
Written By: G. Shan
Page 11
How Will Moye Make You Move? BiomechanicalAnalysis of Moye Starting Blocks.
Written By: P. Gervais & J. S. Leblanc
Pages 12 & 13
Perfectionism, Perceptions of Physical Self, SkatingSelf-Efficacy & Imagery Use in CompetitiveSynchronized Skaters.
Written By: J. G. H. Dunn, C. C. Loitz, W. M. Rogers &C. Hall
Pages 14 & 15

3 SMCA Pulse Winter 2006
L a t e s t N e w s F r o mT h e S M C A
~The SMCA Online Shopping Page is currently beingreconstructed to make printing and faxing your medicalsupply order a thing of the past. Most notably, our newonline shopping system will feature a summary order page,listing only the items you have selected to purchase, andour shopping page is now capable of being submittedelectronically via email. We hope to have the new onlineshopping page in place by mid- November, but keepchecking our website at http://www.sportmedab.ca for thelatest updates.
~ As a non-profit organization, the SMCA relies ongovernment funding and lotteries to help us run ourprograms and services. On February 14 & 15 at theBaccarat Casino in downtown Edmonton, the SMCA will behosting our biannual Casino Fundraiser. Currently, we arein need of volunteers to help us work the casino. If anyoneis interested in working any shifts, the SMCA would begreatly appreciative. Please contact our office via phone oremail for a list of available shifts.
~ The SMCA Sport Medicine Page has been featured inthe Edmonton Sports Scene Magazine for the months ofSeptember, October and November now. Topics we havediscussed so far include soccer injuries and concussions,pre- and post-exercise nutrition and how to treat, preventand rehabilitate athletic injuries. The Sport Medicine Councilof Alberta would like to thank Charlotte Varem-Sandersand Lisa Linner for submitting their article on pre- and post-exercise nutrition and encourage other sport medicineprofessionals to publish their sport medicine findings on theSport Medicine Page. Pick up your copy of the EdmontonSports Scene Magazine today at any of their locations, listedon their website at http://www.sportscene.ca/edmonton. Topublish your article in the Sport Medicine Page, pleasecontact Jennifer at the SMCA office.
~ The official end to the SMCA MembershipRenewal/Application Period was September 30, but if youhaven’t renewed your SMCA membership yet, pleasecontact our office. We have restructured our categories toextend free SMCA memberships to members of our sixprovider groups. All others will either fall into our Subscriberor Corporate membership categories.
~ The SMCA is very excited about our ongoing partnershipwith Willis Insurance and we continue to encourage ourmembers to take advantage of their no-obligation quote forhome and auto insurance. Every three months, the SMCAwill be mailing our members a Wilis Insurance Package foryour review. You never know...Willis may be able to saveyou money on your insurance premiums. For moreinformation, please see their advertisement on the backcover.
~ The SMCA is currently working on a grant proposal toacquire funding to purchase new resources for our SportMedicine Resource Library. The resource library boasts acomplimentary borrowing policy and houses a variety ofmaterials on topics such as sport nutrition, athletic training,injury prevention and rehabilitation, drug education andsport medicine research. For a listing of the materials in ourresource library, visit our website athttp://www.sportmedab.ca/library.html. If you would like tosee any resources in the library that currently are not,please contact our office or send us an email.
The Sport Medicine Council of Alberta Would Like to Thank our Partners
for their Ongoing Support:
The Sport Medicine Council ofAlberta would like to thank the:
And its Sport Science Researchersfor contributing their Articles to this
issue of the Pulse Magazine.
4 SMCA Pulse Winter 2006
FF eemmaa ll eeAA tt hh ll ee tt eeII ss ss uu ee ss ::
The VarsityAthlete at the University of
Alberta

5 SMCA Pulse Winter 2006
IntroductionWomen's health in the area of sports medicine has changed dramatically.Thirty years ago, physicians and therapists had little experience intreating female athletes and other active women. It is known that rates ofcertain musculoskeletal injuries and medical problems resulting fromand/or impacting athletic activity are greater in female athletes comparedto their male counterparts (Mees, 2003). Researchers, physicians andtherapists are beginning to understand the origins of these differences aswell as the gender-specific implications of these injuries and conditions.Most recently, a collaboration of professional associations developed aconsensus statement regarding select musculoskeletal and medicalissues of interest to team physicians who are responsible for the medicalcare of female athletes (American College of Sports Medicine ConsensusStatement, 2003). Areas identified include anterior cruciate ligament(ACL) injuries, stress fractures, osteoporosis and osteopenia, disorderedeating, menstrual dysfunction, and pregnancy and contraception. Withexception of ACL injuries, the other targeted areas are conditions that, ifoccurring together, are known as the Female Athlete Triad. Eachcondition alone is cause for concern but when combined can beextremely dangerous to the health of the athlete. Presently, there is nodatabase or on going injury reporting system available to analyze sportsinjuries or medical issues of female athletes at the University of Alberta.Establishing a database to collect this kind of information is essential formonitoring varsity musculoskeletal and medical issues for female athletesacross all sports. Understanding the magnitude and nature of theseconditions will permit effective prevention and treatment strategies.
ObjectiveThe purpose of this study is to document the clinical sports medicineissues and related risk factors of female varsity athletes at the Universityof Alberta. From these data, a sports medical profile will be developed forthe entire varsity group. In addition, this inventory will help createsport-specific profiles.
DesignRetrospective design.
SettingUniversity of Alberta, Edmonton.
SubjectsA total of 131 rostered athletes (mean age=22 yr, range=17-29) from 7sports (basketball, field hockey, ice hockey, rugby, soccer, cross-countryrunning, volleyball) volunteered to participate in this study.
Intervention/Main Outcome Measures The study protocol was approved by the Faculty's Research Ethics Board.Participation in this study required completion of the "University of AlbertaFemale Varsity Athlete Medical Form" and consent for its use in research.All varsity athletes are required to complete a standardized medical formprior to participating in their specific sport. This questionnaire asks aboutthe athlete's health status and injury experience within the last year. Keyrisk factors such as early age at onset of training, late age of menarche,reduced number of menses/year, treatment of anemia, calciumsupplement use, weight reduction diets, eating disorders and stressfractures are addressed. This information often helps identify athletes atrisk for sport-related injury or conditions that impair performance.Participants from 7 different women's varsity sport teams providedconsent for use of this information in the proposed study. Answers were
coded and individual data from each question were entered into aspreadsheet program and analyzed descriptively.
Main ResultsThe majority of athletes began training for sport between the ages of10-15 years of age (62%). Another 30% of athletes began training at ayounger age (4-9 yr). The average age of menarche was 12.9+1.3 yrwith the majority (86%) of athletes having their first menstrual cyclebetween the ages of 10-15 yr. Four (4) athletes were 16-17 yr atmenarche. From the athlete group, 3 reported 0 menses/yr (amenorrhea)and 2 reported 3-4 menses/yr (oligomenorrhea). Approximately 12% ofthe athletes (16/131) have been treated for anemia while another 8%(11/131) take calcium supplements. Diets to reduce body weight havebeen employed by 16% (21/131). Most athletes (80%, 105/131) aresatisfied with their current body weight and there were no reported casesof eating disorders. Stress fractures were reported by 8% (11/131) of theathlete group of which 9 of the 11 reports were for a lower body fracture(ie spine, tibia, metatarsal).
ConclusionsOur data suggest that most athletes are free of established risk factorsassociated with the Female Athlete Triad. Approximately 10% showedthe presence of several risk factors and may need some additionalassistance or attention. The profile of our database shows that 30% ofathletes have started training at an early age, while lower numbers ofmenstrual irregularities, anemia, weight reduction diets and stressfractures were reported. No eating disorders were reported by anyathlete. Self-report measures are known to lack accuracy, particularlywhen dealing with potentially sensitive and personal issues.Opportunities to educate the athlete and improve self-awareness aboutthese issues may contribute to improved health status and reduction ofrisk factors.
Source of Funding:Sport Science Association of Alberta (SSAA) through the Alberta Sport,Recreation, Parks & Wildlife Foundation ( ASRPWF.)
For More Information, Contact:Dr. Vicki Harber
Faculty of Physical Education and RecreationE424 Van Vliet CenterUniversity of Alberta
Edmonton, AB, T6G 2H9.
CommentaryFemale athletes experience specific injuries and medical conditions inexcess of their male counterparts and, as a result, activity andperformance may be impaired (Mees, 2003; Consensus Statement,2003). The University of Alberta does not keep a database or ongoingreporting system that is dedicated to sports injury analysis or medicalissues. Interruptions to an athlete's training can best be avoided witheffective prevention programs. In the event of such a disruption, rapidreturn to sport can be supported by successful rehabilitation treatments.Creating and maintaining optimal sport performance requires an ongoingreporting system. Approximately 10% of the athlete group investigated inthis study demonstrated the presence of several risk factors. Educationalprograms aimed at awareness and prevention may help reduce the risk ofindividual athletes and teams experiencing poor performance.
Written By:V. Harber and J. Matthews-WhiteFaculty of Physical Education and RecreationUniversity of AlbertaEdmonton, Alberta, Canada
FFeemmaallee AAtthhlleettee IIssssuueess......From page 4

6 SMCA Pulse Winter 2006
An
Examination
of the
Biomechanical
Factors that
Produce Spin
on a Volleyball
in the Skill of
SpikingWritten By:J. Pierre Baudin, P. Gervais & T. WuFaculty of Physical Educationand RecreationUniversity of AlbertaEdmonton, Alberta, Canada
IntroductionSpiking is the most important attacking skill in the sport of volleyball andits effectiveness is in large part determined by the amount of topspin ithas after leaving the attacker's hand. A spinning volleyball has theadvantage of being able to be hit with greater velocity, higher above thenet, and at flatter angles over the net than balls with little or no spin andstill land in the court on the opposite side. This is possible because of thelift forces produced on the spinning ball as a result of the Magnus Effectand Bernoulli's principle. The importance of this spin is demonstrated bythe emphasis that is placed on it in the volleyball instructional literature(Howard, 1996, Baudin, 1994, Scates, 1993, Prsala, 1982). For spin to be produced on the volleyball a torque must be applied bysome external force not acting through the axis of rotation found at itscenter of mass. The technique that produces this in a volleyball spikeseems to be agreed upon in the instructional literature. It is described asbeing produced by the heel or palm of the hand contacting first and thenthe fingers wrapping over top. Prsala (1982) concludes, "It is only duringthe wrapping action that the force applied to the ball becomes eccentric togive the ball a spin". While there is agreement in the instructionalliterature there is no actual research data to support these claims.Alexander and Seaborn (1980) describe the hand contact only as "wristflexion" while Maxwell (1982) states "The hand is further accelerated byangular acceleration at the wrist creating a 'snapping' action." Clearly, theactual mechanical factors creating the spin of the volleyball during thespiking action are not known.
ObjectiveIt was the purpose of this study to determine the biomechanical factorsthat produce the spin on a volleyball during a spiking action. It washypothesized that spin is produced by the eccentric application of forcesto the ball by the pads of the fingers striking the ball before the heel orpalm of the hand contacts the ball.
DesignQuasi-experimental design.
SettingUniversity of Alberta, Edmonton.
SubjectsParticipants for the study were 7 men and 11 women, members of university volleyball teams with many years of training and experience.
Intervention/Main Outcome Measures First, reflective markers were placed on the forearm, wrist, distal end ofthe 5th metatarsal, and the finger tip of the middle finger of each subject.They then warmed up by doing 25 repetitions of a standing spike againsta wall. Finally, they performed 5 standing spikes, each of a volleyball thatthey themselves tossed into the air and hit into a net.
Article Continued on Next Page...
Ho
w Do You Spin It?
7 SMCA Pulse Winter 2006
HHooww DDoo YYoouu SSppiinn IItt??From page 6
High-speed video of the subjects was collected using standardtwo-dimensional videography methods using a high-speed digital videocamera operating at 500 Hz. The camera was positioned to allow a closesagittal view of the forearm and hand of each subject and the ball as itwas struck. The video record of each of the 90 spikes was analyzed withthe APASTM motion analysis system. A 4 point, three-segment model wasused to represent the arm and hand and 2 points visible on the ball wereused to calculate angular kinematics on the ball. Spatial data smoothedwith a second-order Butterworth digital filter was then used in thekinematic analysis of hand segments and the ball.
Main ResultsThe study reveals that two different hand contacts produce spin on thevolleyball by a spiker's hand. The first technique, agrees with theliterature, showing that the spin is produced by the palm of the hand firstcontacting the middle of the ball followed by a wrapping action of thefingers over top creating the torque. This study found that the entire palmof the hand contacts first and then the fingers wrap over top of the ball.As a result, the "wrapping action", although present, is quite limitedespecially with some trials where palm and finger contact was almostsimultaneous.
A second technique, not previously reported, was also seen in which thefingers of the hand contact first at a point high on the ball to createtorque. This was then followed by the palm of the hand striking the middleof the ball.
Of the 90 trials analyzed, 47 were found to have palm first contact and 43had finger first contact. Interestingly of the 18 subjects, only 3 exhibitedthe same hand strike pattern for all of their trials, with two subjects usingthe finger first technique and one using the palm first method. Theremainder of the subjects used both techniques during the course of the 5trials.
ConclusionsThe results of this study indicate that experienced volleyball players use
two different techniques of hand contact to produce spin in a spikedvolleyball. One method, that has been previously discussed, has thepalm of the hand contacting the ball first and then the fingers wrappingover top to produce torque and thus spin on the ball. The secondtechnique revealed for the first time in this study is that of a finger firstcontact higher up on the ball that produced an eccentric force on the balland therefore the torque required to produce spin. This then leads to thequestion, "Which produces more spin on the ball?" The palm first contacttechnique produced a mean ball angular velocity of 39.02 rad/s that wasnot significantly different from the finger first technique that produced amean ball angular velocity of 41.42 rad/s. This seems to indicate that thetechniques are equal in producing spin on the volleyball during spiking.
Source of funding:Sport Science Association of Alberta (SSAA) through the Alberta Sport,Recreation, Parks & Wildlife Foundation (ASRPWF.)
For more information, Contact: Dr. J. Pierre Baudin
Faculty of Physical Education and RecreationP319 Van Vliet CenterUniversity of Alberta
Edmonton, AB T6G 2H9
CommentaryThis first study of hand contact of the ball when spiking found that therewere two techniques that are equally effective at producing spin on thevolleyball however; more studies should be done to confirm this. All of thesubjects were originally taught to use the wrapping action and it ispossible that if taught the finger first method they may be more effectiveat producing spin. Volleyball coaches need to be informed of fingers-firstcontact technique and methods should be developed to effectively teach itto volleyball players.
Services:~ Functional Ability Evaluations ~ Onsite Job Demands Analysis
~ On Site Athletic Event Coverage ~ Home Exercise Programs
~ Footmaxx Computerized Orthotics ~ Massage Therapy
~ Acute & Chronic Orthopedic & SportInjuries
~ Personal Training Services ~ Work Related & Motor Vehicle
Accident Injury Programs
So, you need to attend Physical Therapy... Ermineskin Physical Therapy was established in 1985 with the aim of serving theambulatory Physical Therapy needs of the citizens of Edmonton and area. In 2003 wechanged our name to South Edmonton Physical Therapy & Sport Rehab Inc. tobetter reflect our location and services.
Our team of Physical Therapists are all graduates of a recognized university programand are members of the College of Physical Therapists of Alberta.
We treat many different problems from back and neck pain to joint replacementsurgery and motor vehicle accident injuries, as well as many other problemsassociated with keeping the human body moving.
We are accredited by the Rehabilitation Accreditation Commission (CARF).
3010-106 St.Edmonton 780-438-0001
Thank you South Edmonton PT & SR Inc.
for your Longtime Support as an SMCA Corporate Member!
South EdmontonPhysical Therapy &
Sport Rehab Inc.
8 SMCA Pulse Winter 2006
The Effect of Off-Season TrainingProgramming for EdmontonRowers: A Comparison ofInspiratory to Expiratory BreathingMuscle Training on PulmonaryMeasures and Rowing Performance.
IntroductionResistance to breathing at the mouth can be controlled by devices thatresist airflow during inspiration and/or expiration. These chest muscletrainers can be effective in improving various aspects of forceful breathing(Sheel et al. Sports Med. 32: 567-581, 2002), reduce fatigue (Bell et al.CJAP, 28, S32) and possibly aid performance in certain sporting events.With respect to the sport of rowing, Volianitis et al. (Med. Sci. SportsExerc., 33: 803-809, 2001) has shown that inspiratory (only) chest muscletraining can produce significant increases in inspiratory mouth pressure,less inspiratory muscle fatigue and improved rowing performance inlightweight oarswomen. Our previous research (Bell et al. CJAP, 28, S32)found an improved inspiratory and expiratory mouth pressure withcombined inspiratory/expiratory chest muscle training and no effect onrowing performance.
ObjectiveThe purpose of this study was to compare inspiratory only to expiratoryonly chest muscle training adaptations in conjunction with off-seasonconcurrent strength and endurance training in rowers. It washypothesized that the adaptations to maximal inspiratory pressuremeasured at the mouth will be greatest with inspiratory chest muscletraining and vice versa with little effect on performance.
DesignQuasi-experimental design.
SettingUniversity of Alberta, Edmonton.
SubjectsThe subjects (n = 13 male and 16 females) were a combination ofon-water and indoor-only rowers from the local rowing community.Attrition rate was 5 subjects. This study was approved by a UniversityResearch Ethics Board.
Intervention/Main Outcome MeasuresEach subject completed a maximal oxygen consumption test (VO2max),mRM strength test, a 2000 m rowing performance test, and maximalexpiratory and inspiratory mouth pressure tests (PEmax, PImax). Afterinitial testing, all subjects were matched on 2000 m performance time bygender and randomly assigned to either an inspiratory (INS) or expiratory(EXP) chest muscle training group.
Article Continued on Next Page...
Written By:G. Bell, D. Syrotuik, A. & R. JonesFaculty of Physical Education & Pulmonary MedicineUniversity of AlbertaEdmonton, Alberta, Canada
Breath In,Breath Out...

BBrreeaatthh IInn,, BBrreeaatthh OOuutt......From page 8
9 SMCA Pulse Winter 2006
Inspiration and expiration force was controlled at the mouth usingPowerLung® training devices. Training began at 3 sets of 10 maximalbreathing repetitions, 1x/day and increased to 2x/day, 6 d/wk. The level ofresistance to inspiration and expiration was also progressively increased.In addition to the chest muscle training, a concurrent endurance andstrength training was followed, 6 days a week for 10 weeks: 3 days ofcontinuous and interval aerobic endurance training on Concept II rowingmachines and 3 alternate days of strength training consisting of 10exercises (4 lower and 6 upper body). All testing was repeated after the10-week program.
Main ResultsThere were similar increases in VO2max, bench and leg press mRMstrength levels, as well as similar significant decreases in 2000 m rowingtime after training for both genders. Men had a significant greater resting
PEmax and PImax pressurecompared to
women. PImax at rest was significantly increased to the same extentafter inspiratory and expiratory chest muscle training but PEmax was onlysignificantly improved with expiratory muscle training.
ConclusionsOur results suggest that 10 weeks of chest muscle training using devicesdesigned to provide variable resistance to inspiration and expirationcombined with a concurrent strength and endurance training program waseffective in enhancing resting maximal inspiratory and expiratorybreathing pressure depending on the type of chest muscle training used.Our findings showed that expiratory chest muscle training significantlyincreased PImax (~14%) and PEmax (~12%) but inspiratory chest muscletraining was only effective at enhancing PImax (~26%, p<0.05) and notPEmax (~8%, n.s.). Our conclusion is that expiratory chest muscle
training showed the greatest overall improvement in both inspiratory andexpiratory resting maximal mouth pressures.
Source of funding:Sport Science Association of Alberta (SSAA) through the Alberta Sport,Recreation, Parks & Wildlife Foundation (ASRPWF.)
For more information, Contact:Dr. Gordon Bell
Faculty of Physical Education and Recreation E424 Van Vliet Center
University of Alberta Edmonton, AB T6G 2H9
CommentaryRowing in a 2000 m competition is
performed at an intensity that requiresforceful breathing that is
coordinated with the row-ing stroke. Thus, boththe inspiratory and
expiratory breathingcomponents of rowingare stressed during
the high ventilationrates required for
rowers to perform.
Previously, we showed that a program that combined both inspiratory andexpiratory chest muscle training was able to improve forceful breathingbut did not improve 2000 m simulated rowing performance beyond thatwhich occurs with a regular off-season program consisting of strength andendurance training. This study was performed to determine whetherinspiratory only or expiratory only chest muscle training was moreeffective. The present findings suggest that the expiratory chest muscletraining was able to improve both inspiratory and expiratory forcefulbreathing whereas inspiratory chest muscle training was only able toimprove inspiratory breathing force and was unable to significantlyimprove expiratory muscle training. Once again, our findings suggest thatchest muscle training improvements do not seem to transfer to simulated2000m rowing performance changes.
10 SMCA Pulse Winter 2006
ObjectiveTo compare the effects of two training protocols, high intensity training(HIT) and low intensity training (LIT) on changes in maximal strokevolume (SVmax), plasma volume (PV), VO2 max, and enduranceperformance variables.
DesignExploratory parallel cohort.
SettingHuman Performance Laboratory, U. of C., AB.
ParticipantsTwelve trained male cyclists (25 6yrs; 74.6 3.8 kg; 61.7 3.6 ml·kg-1min-1) volunteered to participate in 10 weeks of testing and training.
MethodologyThere were four test weeks separated by high volume training (HVT) (4days - 3 hrs per day), high or low intensity training (2 weeks), and finally ataper (2weeks). During each test week, the cyclists performed: 1) aprogressive cycle test to measure VO2 max, cardiac output (Q), maximumheart rate (HRmax), and peak aerobic power output (PAPO); 2) a lactateminimum test; 3) a 20 km time trial (TT); 4) progressive exerciseechocardiography test to PAPO; and 5) an endurance ride at 110%lactate minimum power output (LMPO). In addition, hemoglobin andhematocrit were measured. Cardiovascular measures were determined byopen-circuit acetylene breathing. After the initial HVT block, the group wasrandomly assigned to HIT (n = 6) or LIT (n = 6). All subjects (SS)completed the same total volume of work 6 days per week, the HIT groupcompleted 8 x 2.5 min at PAPO with rest to 65% HRmax twice per week,the rest of the training for both groups was done at aerobic thresholdintensity.
VO2 Max DeterminationSS performed a standard incremental test to exhaustion on a treadmill.Expired air was collected and analyzed using a metabolic measurementcart (Parvo-Med True Max). PAPO was determined as the last poweroutput completed for 1 minute during the incremental test.
Cardiac OutputSS performed open-circuit acetylene breathing at selected intervalsduring the incremental treadmill tests. This technique involved breathing
trace amounts of acetylene gas while inspired andexpired air was continuously monitored by a massspectrometer. Stroke Volume was calculated formthe Fick equation where VO2 = SV x HR x a-vO2difference.
20 km Time TrialSS performed a 20 km time trial on roller on theirown bicycle with a PowerTap wheel substituted fortheir own rear wheel and their front forks mountedon a stand for stability.
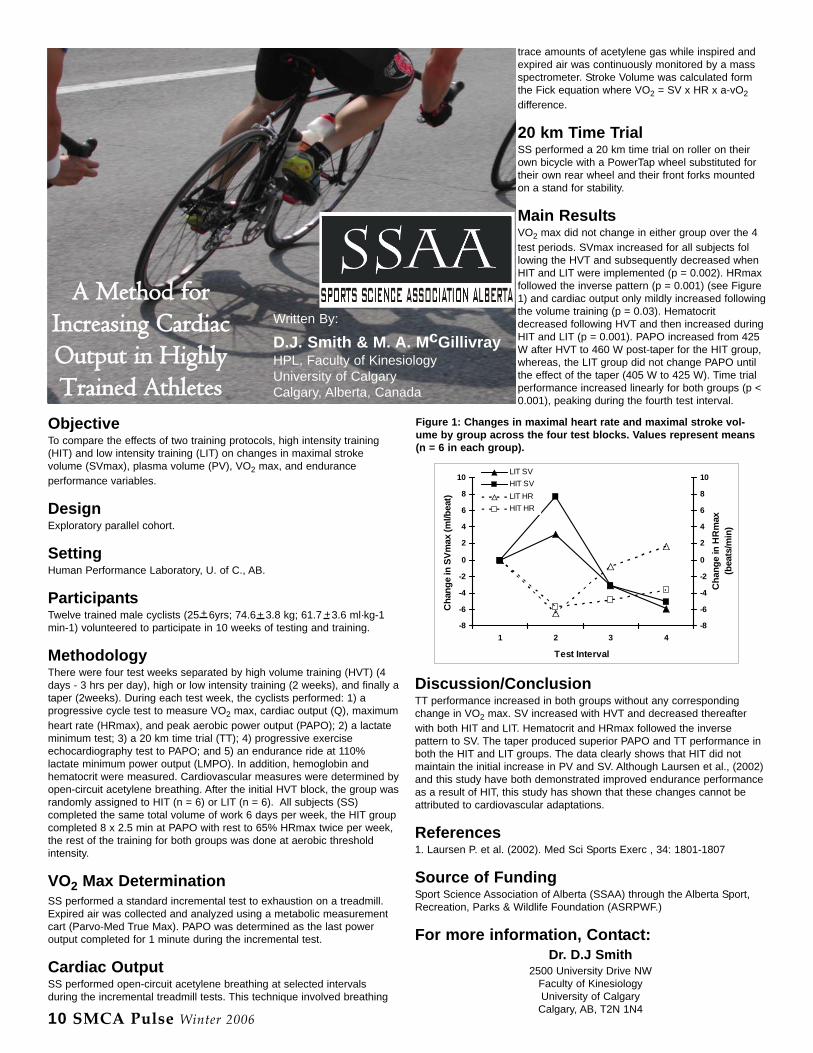
Main ResultsVO2 max did not change in either group over the 4test periods. SVmax increased for all subjects following the HVT and subsequently decreased whenHIT and LIT were implemented (p = 0.002). HRmaxfollowed the inverse pattern (p = 0.001) (see Figure1) and cardiac output only mildly increased followingthe volume training (p = 0.03). Hematocritdecreased following HVT and then increased duringHIT and LIT (p = 0.001). PAPO increased from 425W after HVT to 460 W post-taper for the HIT group,whereas, the LIT group did not change PAPO untilthe effect of the taper (405 W to 425 W). Time trialperformance increased linearly for both groups (p <0.001), peaking during the fourth test interval.
Discussion/ConclusionTT performance increased in both groups without any correspondingchange in VO2 max. SV increased with HVT and decreased thereafterwith both HIT and LIT. Hematocrit and HRmax followed the inversepattern to SV. The taper produced superior PAPO and TT performance inboth the HIT and LIT groups. The data clearly shows that HIT did notmaintain the initial increase in PV and SV. Although Laursen et al., (2002)and this study have both demonstrated improved endurance performanceas a result of HIT, this study has shown that these changes cannot beattributed to cardiovascular adaptations.
References1. Laursen P. et al. (2002). Med Sci Sports Exerc , 34: 1801-1807
Source of FundingSport Science Association of Alberta (SSAA) through the Alberta Sport,Recreation, Parks & Wildlife Foundation (ASRPWF.)
For more information, Contact:Dr. D.J Smith
2500 University Drive NWFaculty of Kinesiology University of Calgary Calgary, AB, T2N 1N4
-8
-6
-4
-2
0
2
4
6
8
10
1 2 3 4
Test Interval
Cha
nge
in S
Vmax
(ml/b
eat)
-8
-6
-4
-2
0
2
4
6
8
10
Cha
nge
in H
Rm
ax
(bea
ts/m
in)
LIT SVHIT SVLIT HR HIT HR
Figure 1: Changes in maximal heart rate and maximal stroke vol-ume by group across the four test blocks. Values represent means(n = 6 in each group).
Written By:
D.J. Smith & M. A. McGillivrayHPL, Faculty of KinesiologyUniversity of CalgaryCalgary, Alberta, Canada
+ + +
A Method forIncreasing CardiacOutput in HighlyTrained Athletes
11 SMCA Pulse Winter 2006
IntroductionSoccer is the most popular sport in the world with hundreds of millions ofparticipants (Ekstrand, 1994). Because of its popularity, a considerableamount of studies has been conducted to understand the skills involved,especially the kick (David et al. 2000). Yet, due to test constraints,difficulty in multi-signal exploration and the complexity of total body con-trol, a full view of an optimal kick remains uncharted. Hence, the pur-pose of this study was to reveal the holistic view by the link between mus-cle activities and joints control through full-body biomechanical model-ling.
ObjectiveThe project targeted three goals:1. Establish a 15-segmental full body model to reveal the 3Dcharacteristics of kick2. Utilize the model to synchronize leg muscle EMGs with 3D kinematicsto explore the joint coordination and control patterns3. Explore possible new parameters for a quantitative evaluation.
SettingThe measurements were conducted in PE240 (Biomechanics Lab),University of Lethbridge.
SubjectsTwenty novice subjects (21.5 y 2.2) were recruited from an introductoryKinesiology class at the University of Lethbridge and an equal number ofelite soccer players (20.4 y 3.5) volunteered from the varsity soccerteam. Half of the participators were females.
Intervention/Main Outcome MeasuresFrom motion capture, we can obtain anatomical positions that allow themodeling of the skeletal structure, which enables the calculation of joints'flexion/extension, abd-/adduction and rotation as well as joints' moment.In addition, muscles can be attached to the skeletal frame usinganatomical knowledge. Thus, muscle lengthening can be determined inconnection with skeletal movement. From these, when correlated withEMG signals, muscular work patterns (eccentric etc) can be determined.
Main ResultsResults show: 1) effective upper-body movement to be a key factor increating better initial conditions for a more explosive muscle contractionduring kicking. It permits a more powerful quasi whip-like movement ofthe kicking leg; 2) the timely change of distance between the kick-side hipand the non-kick-side shoulder provides a quantitative means ofmeasuring kick quality.
Source of Funding:Sport Science Association of Alberta (SSAA) through the Alberta Sport,Recreation, Parks & Wildlife Foundation (ASRPWF.)
For more information, Contact:Dr. Gongbing Shan Dept of Kinesiology, UofL
4401 University Dr, Lethbridge, AB, T1K 3M4e-mail: [email protected]
Modeling Maximal
Instep Kick in
Soccer
Written By:Dr. G. ShanDepartment of KinesiologyUniversity of LethbridgeLethbridge, Alberta, Canada
+
+

IntroductionIn track and field athletics, all athletes competing in races of 400m or lessmust, by rule, use starting blocks. Since the commencement of themodern Olympic Games in 1896, there has been little overall change inthe starting technique of elite sprinters (Mach, 1985, T & F Quart Rev,85(2):11-14). Early sprinters used to dig holes in the track in which toplace their feet when starting. With the innovation of synthetic tracksurfaces, starting blocks were invented to replace the start holes. Whilethere have been some modifications over the years, the overall design ofthe standard starting block has not changed much, nor has the techniqueof starting. Numerous studies have been carried out on the biomechanicsof starting from blocks in attempts to identify the optimal start parameters(e.g., Henry, 1952, Res Quart, 23(3):301-318; Turner & Henson, 1985, T& F Quart Rev, 85(2):29-32; Schot & Knutzen, 1992, Res Quart Ex Sp,63(2): 137-147), including some recent research examining newconfigurations for starting blocks (i.e., Parry et al., 2003, NSA, 18(1):13-22).In recent years, a different type of starting block has gained some supportin the coaching community (McFarlane, 1993, Mod Ath & Coach,31(2):13-15), but it has received little or no attention in the researchliterature. The Moye block uses a large steep back pedal and a small lowfront pedal. The athlete places the full foot on the back pedal but only theheel of the foot goes on the front pedal with the forefoot resting on thetrack. The athlete is supposed to assume a taller hip stance than in
traditional blocks, and the block pedals are placed closer to the start line.Those who have argued for the use of the Moye technique state that itresults in faster start times and requires less muscular effort thanstandard start techniques (McFarlane, 1993). To date, no publishedresearch has investigated the Moye starting technique.
ObjectiveThe purpose of this research project was to examine the biomechanics ofa sprint start from Moye blocks as compared to standard starting blocks.
DesignQuasi-experimental design.
SettingUniversity of Alberta, Edmonton.
SubjectsThe subjects (n = 5) were members of the University of Alberta varsitytrack and field team (2 female, 3 male) who volunteered to take part. Allhad extensive experience with standard starting blocks but minimal or noexperience using Moye starting blocks.
Article Continued on Next Page...
12 SMCA Pulse Winter 2006
BiomechanicalAnalysis of
Moye StartingBlocks
Written By:P. Gervais & J. S. LeblancFaculty of Physical Education & RecreationUniversity of AlbertaEdmonton, Alberta, Canada
How Will Moye...
Make You Move?

Intervention/Main Outcome Measures Each subject completed one day of practice and two days of testing.During the practice session, athletes were instructed on the use of theMoye block and received practise on them. On each of the two testingdays, subjects performed two sets of five starts, one set from each type ofblock. The order in which the types of blocks were tested wasrandomised by subject on the first day, and the order was then reversedon the second day to reduce any order effect in the testing protocol.Each sprint start was 25m in distance, and subjects were given aminimum of 3 minutes between trials and five minutes between sets oftrials. The distances of the block pedals from the start line werestandardised based on a measure of foot length: two and three footlengths for the standard blocks; and one and two and a half foot lengthsfor the Moye blocks.
The start commands consisted of an automated voice ("on your marks"and "set") and a simulated gun sound; these were generated by aReacTime unit (Lynx Systems Developers, USA) attached to the startingblocks. Reaction times (RT) to the millisecond were recorded from theReacTime units. A Laveg-Sport laser (JENOPTIK, Germany) was used torecord linear displacement of the body; the laser was targeted on thelow-back of the subject and recorded position to the nearest millimetre at50 Hz. Subjects were also filmed in the sagittal plane by two JVC high-speed digital video cameras (120 Hz) with over-lapping fields of view.The APAS system was used to carry out a 2D kinematic analysis.A total of 94 trials were analysed from the ReacTime and laser data.Performance measures included: RT; split times to 5m, 10m, 15m, 20mand 25m; and, instantaneous velocity at 5m, 10m, 15m, 20m and 25m.Average values were calculated for each subject from each type of block.These values were then assessed by paired t-tests (alpha = 0.05) todetect differences in group means between the standard and Moyestarting blocks. Subsequently, trials were selected from one male andone female subject to examine the total-body centre of mass (CM)location in the "set" position and the length of the first and second stepfrom the blocks.
Main ResultsReaction times were 190 ms (41) from the standard blocks and 153 ms(31) from the Moye blocks, which was a significantly (p<0.022) fasteraverage RT. The split times to reach 5m (1.02s vs. 1.05s, p<0.003), 10m(1.74s vs. 1.77s, p<0.005), 15m (2.49s vs. 2.52s, p<0.033), and 20m(2.99s vs. 3.02s, p<0.046) were found to be significantly faster for thestarts from the standard blocks, but not at 25m (3.47s vs. 3.50s,p<0.062). However, there were no significant differences ininstantaneous running velocity at any of the interval distances (p-valuesfrom 0.101-0.919). The location of the CM in the "set" position wasdetermined from video for two of the subjects. While the height of the CMdid not seem to be different between the standard and Moye blocks, theMoye put the CM horizontally closer to the start line by 5-10cm. Thelength of the first step was longer from the Moye block by 25-35cm, butthe length of the second step was approximately the same, so anyadvantage in step length seemed to be restricted to the first step.
ConclusionsThe faster RT recorded on the Moye block starts did not seem to translateinto faster sprint times to any of the interval distances. It may be that thefaster RT were caused by some artefact of the interaction of the Moyeblock and the ReacTime units. In fact, only 3 out of 94 recorded trialswere deemed to be false starts by the ReacTime units (and subsequentlynot included in calculations of average RT), and all three of these wereduring trials on the Moye blocks. It may be that something in the blockconfiguration makes it result in faster recorded RT - this may haveimplications for athletes using the Moye block in competition since majorcompetitions typically make use of false start detection equipment, likethe ReacTime units used in this study. Further research will be requiredto clarify this point.
Source of Funding:Sport Science Association of Alberta (SSAA) through the Alberta Sport,Recreation, Parks & Wildlife Foundation (ASRPWF.)
For more information, Contact:Dr. Pierre Gervais
Faculty of Physical Education and RecreationE424 Van Vliet CenterUniversity of Alberta
Edmonton, AB, T6G 2H9.
CommentaryThis study represent a preliminary assessment of the biomechanics of theMoye starting blocks, and further analysis will be necessary to moreclearly identify differences as compared to traditional starting blocks - thiswill include the use of non-sprint trained subjects to remove the effects ofprevious training on the standard blocks.
What Do you Get When you Cross...
The Sport Medicine Page in The Edmonton Sports Scene
Magazine!Articles. Advice. Answers.
Pick Up Your Copy Today!13 SMCA Pulse Winter 2006
HHooww WWiillll MMooyyee MMaakkee YYoouu MMoovvee......From page 12
with
14 SMCA Pulse Winter 2006
IntroductionTo date there have only been a few studies in the sport and exercisepsychology literature that have examined the personality trait ofperfectionism and its relationship to cognition, affect, and behaviouramong athletes. Nevertheless, these few studies have consistently shownthat perfectionism is an important personality construct to examinebecause it has been related to anger (Dunn et al, in press), burnout(Gould et al., 1997), self-esteem (Gotwals et al., 2003), anxiety (Hall etal., 1998), and motivational orientations (Dunn et al., 2002) in a variety ofcompetitive sport settings. The defining feature of a perfectionist is theindividual's tendency to set exactingly high personal standards. Althoughathletes may set high personal standards, with respect to theirperformances (whether in training or competition), these standards mayalso extend to other aspects of their lives including physical appearance.Aesthetic sports (such as figure skating and gymnastics) put a great dealof emphasis not only upon physical performance, but also on physicalappearance. Thus, in these aesthetic-based sports, a premium is placedupon a lean and attractive appearance. Previous research by Dunham(2002) that was conducted with figure skaters in Canada revealed thatathletes with a maladaptive or unhealthy profile of perfectionism tended tohave negative attitudes towards their bodies, whereas athletes whodemonstrated a more adaptive or healthy profile of perfectionism tendedto have more positive attitudes towards their bodies. Given that negativeattitudes towards one's body have been linked with eating disorders, it isimportant to understand the factors that may lead to such negative bodyimage tendencies. By studying the relationship between perfectionistorientations and self-efficacy (i.e., the self-belief that one can successfully
complete a specific task),physical self-perceptions,and imagery use, weattempted to further ourunderstanding of factorsthat may influence howathletes in aestheticsports come to viewthemselves (in terms ofability) and their bodies.
ObjectivesPerfectionism is amultidimensional construct.Consequently, the specificpurposes of this study were toexamine the relationshipbetween the various dimensions ofperfectionism and (1) physical self-perceptions, (2) self-efficacy, and (3)skating-related imagery in competitivesynchronized skaters. It is our hope that the results will point to potentiallyconstructive and destructive correlates of perfectionism amongsynchronized skaters and ultimately help improve performance incompetition and training for aesthetic-sport athletes.
DesignCorrelational.
SettingSkate Canada Synchronized Skating Competition in Camrose, Alberta.
ParticipantsOne hundred and eight female synchronized skaters from WesternCanada (M age = 23.3 years; SD = 8.9) participated in the study.
Measures/InstrumentsParticipants completed questionnaires to measure demographiccharacteristics, perfectionist orientations, physical self-concept, skatingself-efficacy, and imagery use. The specific instruments were (1) a skatingversion of the Sport-Multidimensional Perfectionism Scale (Sport-MPS;Dunn et al., 2002), (2) the Adult Body Satisfaction Scale (ABSS)(Reboussin et al., 2000), (3) a sport modified version of the ExerciseSelf-Efficacy Scale (Rodgers & Sullivan, 2000) and (4) a sport-modifiedversion of the Exer-cise Imagery Questionnaire (Hausenblas et al., 1999).
Article Continued on Next Page...
Perfectionism, Perceptions of PhysicalSelf, Skating Self-Efficacy & Imagery Use in
Competitive Synchronized SkatersWritten By:J. G. H. Dunn, C. C. Loitz, W. M. Rogers & C. HallFaculty of Physical Education and RecreationUniversity of AlbertaEdmonton, Alberta, Canada
15 SMCA Pulse Winter 2006
Main ResultsWe performed bivariate correlation analyses to examine the relationshipsbetween (a) perfectionism and physical satisfaction, (b) perfectionism andskating self-efficacy, and (c) perfectionism and skating imagery use.Bivariate correlations (r) revealed that concern over mistakes (COM) wasthe only Sport-MPS subscale that was related to satisfaction with physicalappearance (r = -.26). In other words, as athletes' levels of COMincreased, they tended to become less satisfied with their physicalappearance.
Bivariate correlations (r) revealed that COM (r = -.44), perceived parentalpressure (PPP) (r = -.23), and perceived coach pressure (PCP) (r = -.25)were negatively correlated with task self-efficacy. The direction of thesecorrelations indicates that increases in COM, PPP and PCP areassociated with lowered task self-efficacy (i.e., lowered belief in one'sability to successfully complete the skating task). All three of theseSport-MPS subscales are generally deemed to reflect maladaptive orunhealthy aspects of perfectionism (Dunn et al., 2002).
Bivariate correlations (r) revealed that skaters' personal standards (PS)were positively correlated to skating technique imagery (r = .20). In otherwords, as skaters' personal standards increase, so does their likelihood ofusing imagery as a mental skill to improve skating technique. All of theaforementioned correlations were significant at p < .05 or lower.
ConclusionsOverall, the results indicate that skaters who are concerned about makingmistakes tend to be less satisfied with their physical appearance.Perfectionism theory suggests that people high in COM tend to view
mistakes as being unacceptable, so it appears that high COM athletesare more critical about flaws in their physical appearance. Skaters withhigher maladaptive perfectionist tendencies (high COM, high PPP andhigh PCP) also tended to possess lower task self-efficacy, indicating thatthey tended to have less confidence in their ability to skate the program.We speculate that combining the effects of lowered self-efficacy andlowered satisfaction with one's appearance may result in dysfunctionalbehaviours among aesthetic sport athletes (e.g., disordered eating orobsessive exercising/practicing to obtain the skater's ideal performancelevel or appearance).
The personal standards (PS) dimension of perfectionism has been shownto have adaptive qualities in previous perfectionism research. This waspartly confirmed in this study given that athletes with higher PS scorestended to employ skating-technique imagery as a potentially adaptivestrategy to improve performance.
Source of funding:Sport Science Association of Alberta (SSAA) through the Alberta Sport,Recreation, Parks & Wildlife Foundation (ASRPWF.)
For more information, Contact: Dr. John Dunn
Faculty of Physical Education and RecreationE-424 Van Vliet Center
University of AlbertaEdmonton, AB T6G 2H9
SSyynncchhrroonniizzeedd SSkkaatteerrss CCoonntt’’dd......From page 14
Exclusive Benefit for SMCA Members!!