Embed Size (px)
Citation preview
Neuromyelitis Optica
Dean M. Wingerchuk, MD, MSc, FRCPCMayo Clinic College of Medicine
NMO: Outline• Historical concept• Definitions and diagnosis• Pathology• NMO-IgG• Use of NMO-IgG
• New diagnostic criteria• Prognosis
• Management• acute attacks• attack prevention
Neuromyelitis Optica (NMO)“Devic’s Syndrome/Disease”
• “Historical definition” – 19th century• Monophasic disorder• Fulminant bilateral optic neuritis
(ON) and myelitis occurring in close temporal association
Neuromyelitis Optica: History
• Case series• 1914-1990s• “Traditional” definition:
• Simultaneous bilateral ON and ATM• Variants:
• Unilateral ON• Relapsing course
• Similarity to Japanese optic-spinal MS• Debate: Is NMO a disease or severe
and topographically restricted MS?
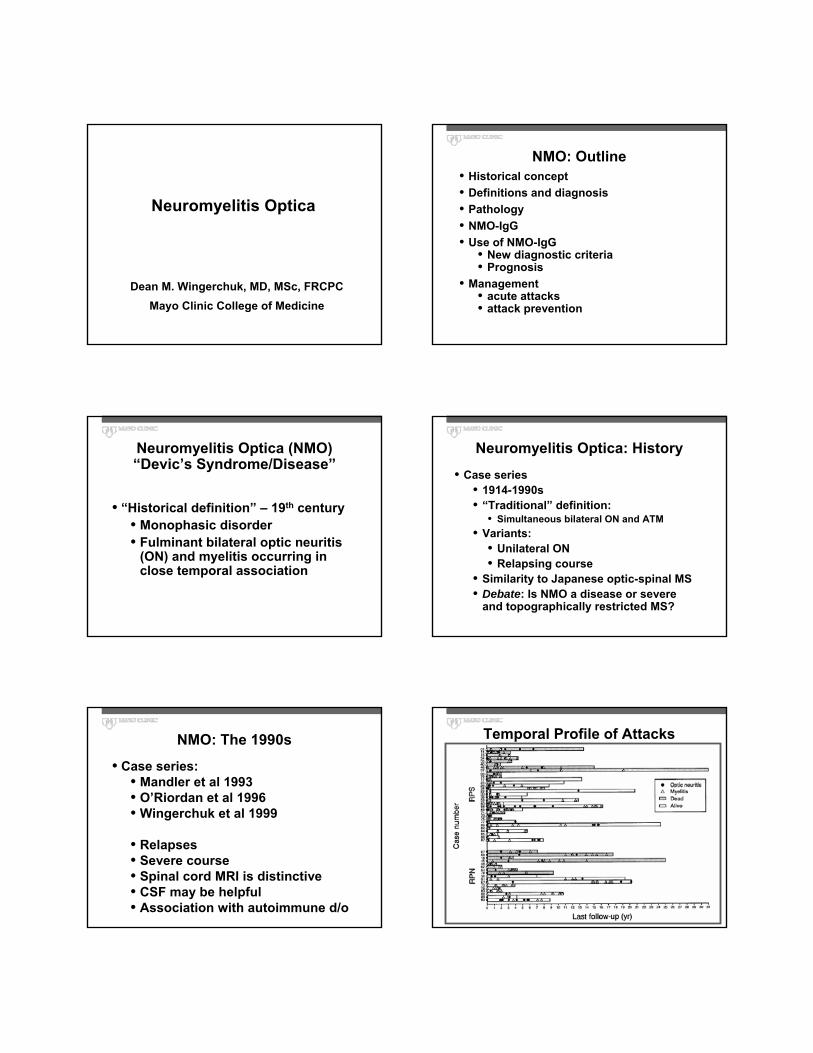
NMO: The 1990s
• Case series:• Mandler et al 1993• O’Riordan et al 1996• Wingerchuk et al 1999
• Relapses• Severe course• Spinal cord MRI is distinctive• CSF may be helpful• Association with autoimmune d/o
Temporal Profile of Attacks
CSF Results
• > 50 WBC : 35%• > 5 neutrophils : 25%• Either : 39%
…within 4 weeks of myelitis
NMO: DefinitionsOld (Traditional)
• Bilateral ON• Myelitis• Short interattack interval• Monophasic
New (Evolving)• Unilateral or bilateral ON• Long. extensive myelitis• Monophasic or relapsing • Any interattack interval• MRI head normal• Autoimmunity
Diagnostic Criteria (1999)• Absolute criteria (all required):
1. Optic neuritis2. Acute myelitis3. Clinically restricted to optic nerve and spinal cord
• Supportive criteria:Either 1 Major
• MRI: brain negative at onset (25/58)• MRI: cord T2 lesion >3 segments (21/23)• CSF: >50 WBC/uL OR >5 PMN/uL (20/54)
Or 2 Minor• Bilateral optic neuritis (59/71)• Severe ON (VA <20/200 in 1 eye) (31/69)• Fixed, attack-related weakness (MRC<2) in >1 limb
(32/71)
Exceptions to NMO Diagnostic Criteria (we expected this…)
• Extra-optic-spinal symptoms/signs• Brain MRI lesions• Milder attacks
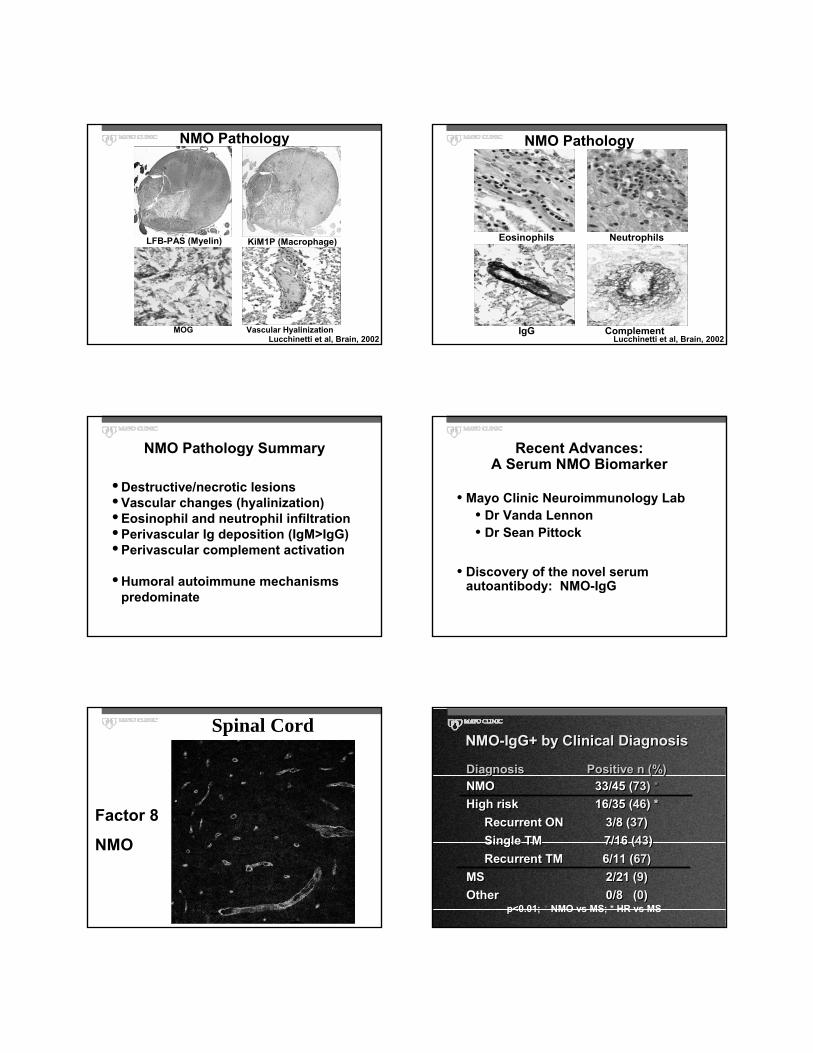
NMO Pathology
LFB-PAS (Myelin) KiM1P (Macrophage)
MOG Vascular HyalinizationLucchinetti et al, Brain, 2002
NMO Pathology
Eosinophils
ComplementIgG
Neutrophils
Lucchinetti et al, Brain, 2002
NMO Pathology Summary
• Destructive/necrotic lesions• Vascular changes (hyalinization)• Eosinophil and neutrophil infiltration• Perivascular Ig deposition (IgM>IgG) • Perivascular complement activation
• Humoral autoimmune mechanisms predominate
Recent Advances:A Serum NMO Biomarker
• Mayo Clinic Neuroimmunology Lab• Dr Vanda Lennon• Dr Sean Pittock
• Discovery of the novel serum autoantibody: NMO-IgG
Spinal CordSpinal Cord
Factor 8Factor 8
NMONMO
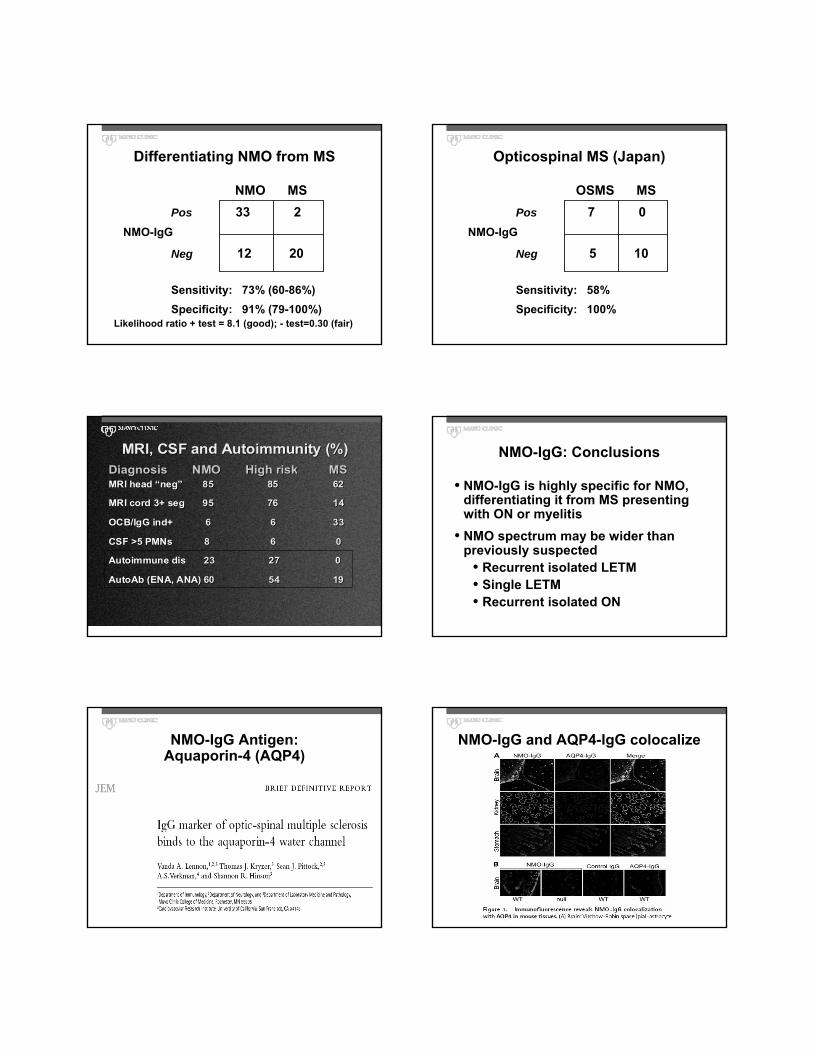
NMO-IgG+ by Clinical DiagnosisNMO-IgG+ by Clinical Diagnosis
Diagnosis Positive n (%)NMO 33/45 (73) *High risk 16/35 (46) *
Recurrent ON 3/8 (37)Single TM 7/16 (43)Recurrent TM 6/11 (67)
MS 2/21 (9)Other 0/8 (0)
Diagnosis Positive n (%)NMO 33/45 (73) *High risk 16/35 (46) *
Recurrent ON 3/8 (37)Single TM 7/16 (43)Recurrent TM 6/11 (67)
MS 2/21 (9)Other 0/8 (0)
p<0.01; * NMO vs MS; * HR vs MS
Differentiating NMO from MS
Pos 3333 22NMO-IgG
Neg 1212 2020
Sensitivity: 73% (60-86%)Specificity: 91% (79-100%)
NMO MS
Likelihood ratio + test = 8.1 (good); - test=0.30 (fair)
Opticospinal MS (Japan)
Pos 77 00NMO-IgG
Neg 55 1010
Sensitivity: 58%Specificity: 100%
OSMS MS
MRI, CSF and Autoimmunity (%)MRI, CSF and Autoimmunity (%)Diagnosis NMO High risk MSMRI head “neg” 85 85 62
MRI cord 3+ seg 95 76 14
OCB/IgG ind+ 6 6 33
CSF >5 PMNs 8 6 0
Autoimmune dis 23 27 0
AutoAb (ENA, ANA) 60 54 19
Diagnosis NMO High risk MSMRI head “neg” 85 85 62
MRI cord 3+ seg 95 76 14
OCB/IgG ind+ 6 6 33
CSF >5 PMNs 8 6 0
Autoimmune dis 23 27 0
AutoAb (ENA, ANA) 60 54 19
NMO-IgG: Conclusions
• NMO-IgG is highly specific for NMO, differentiating it from MS presenting with ON or myelitis
• NMO spectrum may be wider than previously suspected
• Recurrent isolated LETM• Single LETM• Recurrent isolated ON
NMO-IgG Antigen:Aquaporin-4 (AQP4)
NMO-IgG and AQP4-IgG colocalize
Evidence for Humoral Autoimmune Mechanisms
• Co-existing autoimmune disorders• Clinical disease or serologies
• Cord lesions:• Ig deposition• Complement activation
• Discovery of NMO-specific IgG autoantibody
• NMO = aquaporin channelopathy?
Diagnosis of NMO:
Incorporation of NMO-IgG
NMO-IgG Diagnostic Utility
• NMO-IgG alone• 75% sensitive• 90% specific• …when trying to differentiate NMO
from MS with ON/cord predominance
• Virtually never seen in ‘garden variety’ MS
NMO-IgG Diagnostic Utility
• Normal brain MRI plus NMO-IgG +• >94% sensitive• >90% specific• …for clinical diagnosis of NMO
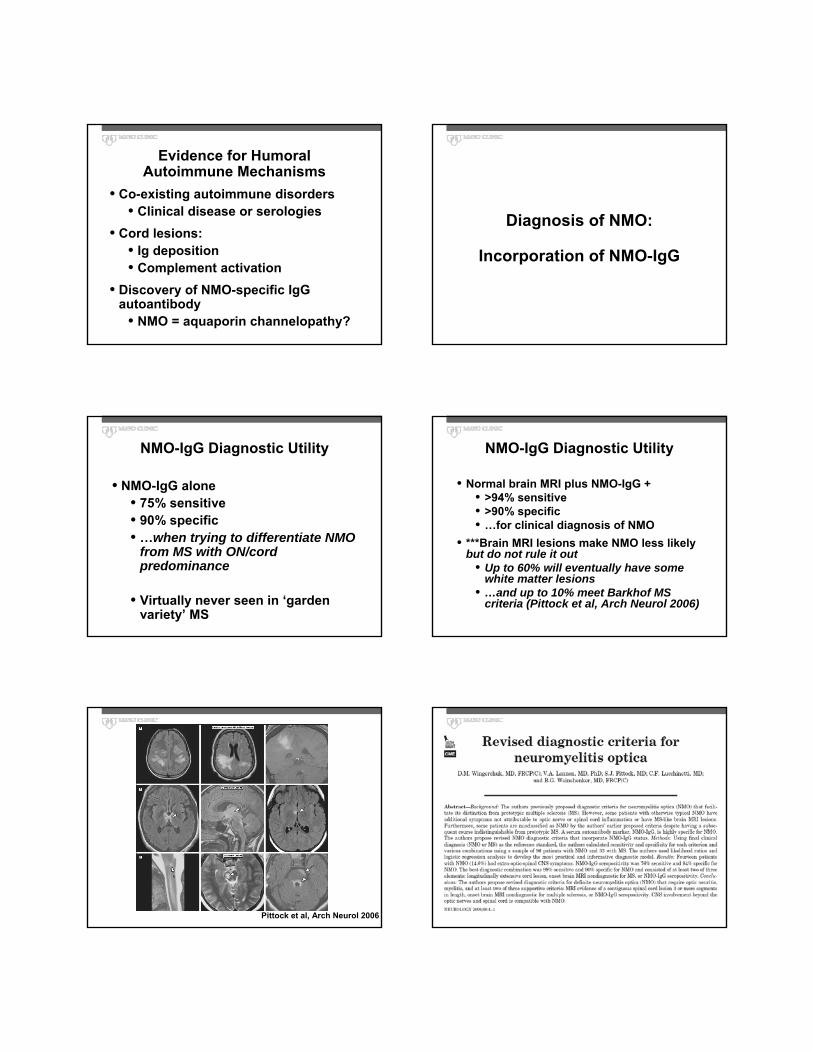
• ***Brain MRI lesions make NMO less likely but do not rule it out
• Up to 60% will eventually have some white matter lesions
• …and up to 10% meet Barkhof MS criteria (Pittock et al, Arch Neurol 2006)
Pittock et al, Arch Neurol 2006
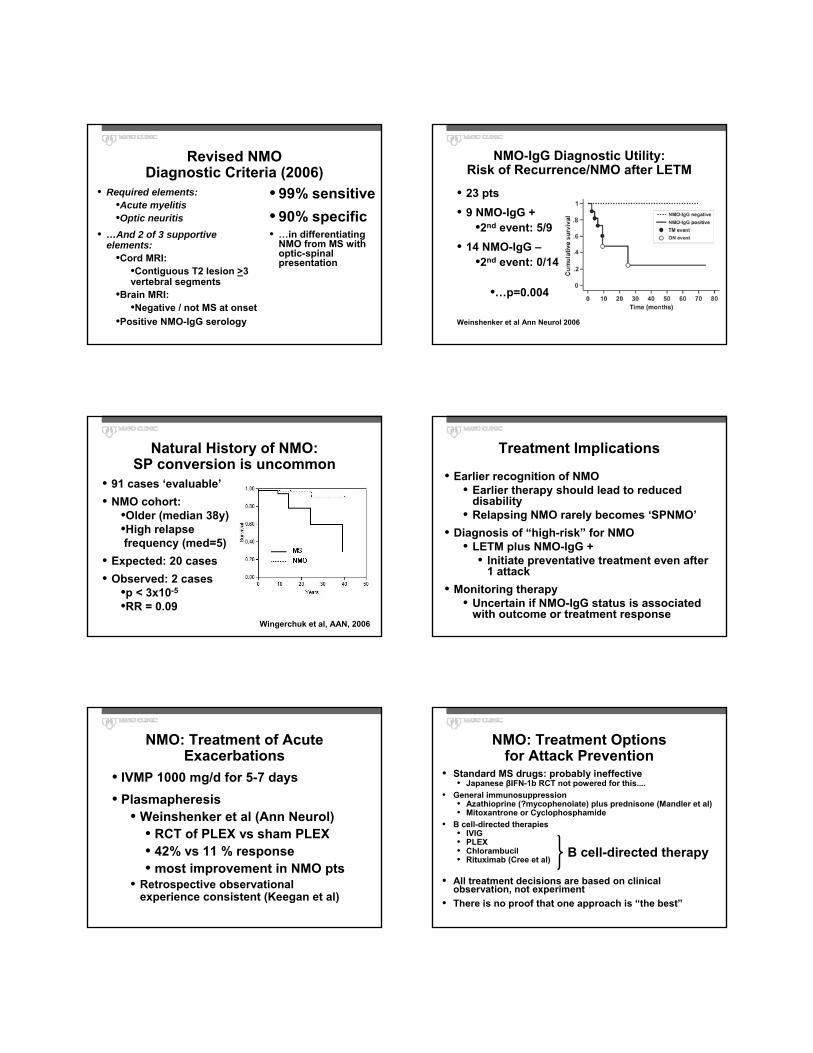
Revised NMO Diagnostic Criteria (2006)
• 99% sensitive• 90% specific• …in differentiating
NMO from MS with optic-spinal presentation
• Required elements:•Acute myelitis•Optic neuritis
• …And 2 of 3 supportive elements:
•Cord MRI: •Contiguous T2 lesion >3 vertebral segments
•Brain MRI: •Negative / not MS at onset
•Positive NMO-IgG serology
NMO-IgG Diagnostic Utility:Risk of Recurrence/NMO after LETM
• 23 pts• 9 NMO-IgG +
•2nd event: 5/9• 14 NMO-IgG –
•2nd event: 0/14
•…p=0.004
Weinshenker et al Ann Neurol 2006
Natural History of NMO:SP conversion is uncommon
• 91 cases ‘evaluable’• NMO cohort:
•Older (median 38y)•High relapsefrequency (med=5)
• Expected: 20 cases• Observed: 2 cases
•p < 3x10-5
•RR = 0.09Wingerchuk et al, AAN, 2006
Treatment Implications
• Earlier recognition of NMO• Earlier therapy should lead to reduced
disability• Relapsing NMO rarely becomes ‘SPNMO’
• Diagnosis of “high-risk” for NMO• LETM plus NMO-IgG +
• Initiate preventative treatment even after 1 attack
• Monitoring therapy• Uncertain if NMO-IgG status is associated
with outcome or treatment response
NMO: Treatment of Acute Exacerbations
• IVMP 1000 mg/d for 5-7 days• Plasmapheresis
• Weinshenker et al (Ann Neurol)• RCT of PLEX vs sham PLEX• 42% vs 11 % response• most improvement in NMO pts
• Retrospective observational experience consistent (Keegan et al)
NMO: Treatment Options for Attack Prevention
• Standard MS drugs: probably ineffective• Japanese βIFN-1b RCT not powered for this....
• General immunosuppression• Azathioprine (?mycophenolate) plus prednisone (Mandler et al)• Mitoxantrone or Cyclophosphamide
• B cell-directed therapies• IVIG• PLEX• Chlorambucil• Rituximab (Cree et al)
• All treatment decisions are based on clinical observation, not experiment
• There is no proof that one approach is “the best”
B cell-directed therapy

Summary• NMO can be distinguished from classical MS• NMO spectrum disorders include:
• (some) recurrent TM/LETM• (some) recurrent ON• (some) Japanese opticospinal MS
• NMO-IgG is a highly specific biomarker• Treatment: target humoral mechanisms