Embed Size (px)
Citation preview

William P. Nash, M.D.Captain, Medical Corps, United States NavyCombat/Operational Stress Control Coordinator Headquarters, Marine Corps
Combat Stress Injuries

Operational Deployment Affects Everyone
• Everyone deployed to a combat zone is affected by that experience, mentally and physically
• Some are affected in positive, growth-enhancing ways• Some find new meaning in their lives and a stronger
spiritual connection• But others are injured by their operational
experiences, superficially or deeply• Most heal from their operational stress injuries, just
as most physical injuries also heal in time• But a few stress injuries persist long after
deployments have ended

The Challenge of Operational Stress Management in the Military and VA
• Discriminating between normal, adaptive responses to combat or operational stress, and those that are pathological
• Identifying pathological stress reactions early, but without adding the insult of stigma to the injury of stress and trauma
• Treating stress problems early and effectively, but without promoting disability

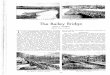
Most Operational Stress Symptoms Are Transient
50.0%
20.0%
1.6%7.8% 9.8%
0%
10%
20%
30%
40%
50%
60%
Marines in Iraqwith StressSymptoms*
Marines in Iraqwith Stress
Disorders*
Marines WhoReceived Psych
Tx in Iraq**
Marines Treatedin Garrison***
Marine OIFVeterans
Treated at VA***
* In two heavily-engaged infantry companies in an urban area** During OIF-II, Feb 2004 through March 2005*** Mental Health diagnoses only, FY-02 through FY-05

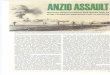
Combat/Operational Stress Trajectories Over Time
SYM
PTO
M B
UR
DEN
Diagram courtesy of Bret Litz, PhD, NCPTSD, Boston
Hig
hM
od
er a
t eLo
wG
row
t h PRE-DEPLOYMENT
DEPLOYMENT
RETURN
3 MOS. POST
6 MOS. POST
CHRONIC COURSE
RECOVERY COURSE
INNOCULATION COURSE
RESILIENT COURSE
GROWTH COURSE
DELAYED COURSE

Stigma Prevents Some Service Members From Getting Needed Help
• Walter Reed Army Institute of Research study: 1709 soldiers and Marines surveyed 3-4 months after OIF-I
– 17% had symptoms of PTSD, depression, or anxiety– 86% of those with symptoms realized they had a problem– 45% said they wanted help– 29% had received mental health help in the past year
• Biggest reasons for not asking for help:– 65% “I would be seen as weak.”– 63% “My leaders might treat me differently.”– 59% “My unit might have less confidence in me.”– 55% “I couldn’t get time off of work to get treatment.”– 51% “My leaders would blame me for the problem.”– 50% “It would harm my career.”

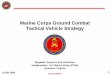
Greek Warrior Ideal: Arete
• Ancient Greek ideal of the aristocrat warrior
• Features of arete:– Strength– Valor– Courage– Fortitude
• Has continued unchanged in the militaries of the world
• The foundation of all military core values and identity
• For a warrior to develop stress symptoms of any kind is to fail to live up to the warrior ideal!
Brad Pitt as Achilles in “Troy”

The Warrior Ideal and Identity Must Always Be Respected
• Warriors and veterans with stress symptoms must be helped to preserve their honor, not be encouraged to abandon it
• Health and pastoral care personnel must be mindful of military cultures
• Use language that minimizes shame without trivializing potentially disabling problems
• U.S. Marine Corps solution: stress reactions are either:– Normal, reversible adaptations, or– Irreversible (but usually self-limiting) stress injuries– Like physical injuries, stress injuries are never the sole fault of the individual

Some of the “Manageable” Hardships of Operational Deployment
PHYSICALPHYSICAL• HeatHeat • • DehydrationDehydration • • IllnessIllness• ColdCold • • Sleep deprivationSleep deprivation • • InjuryInjury
COGNITIVECOGNITIVE• BoredomBoredom • • Being hyper-focusedBeing hyper-focused• Lack of information Lack of information •• Information overloadInformation overload
EMOTIONALEMOTIONAL• Fear of death/injuryFear of death/injury • • Fear of failureFear of failure• Feeling devaluedFeeling devalued • • Loyalty conflictsLoyalty conflicts
SOCIALSOCIAL• Being away from loved ones and friendsBeing away from loved ones and friends• Loss of personal spaceLoss of personal space • • IsolationIsolation
SPIRITUALSPIRITUAL• Loss of clarity about life’s purposeLoss of clarity about life’s purpose• Loss of innocenceLoss of innocence • • Loss of trustLoss of trust

Some of the “Manageable” Hardships of Homecoming
PHYSICALPHYSICAL• TrafficTraffic • • CrowdsCrowds • • Being unarmedBeing unarmed• Access to alcohol and drugsAccess to alcohol and drugs
COGNITIVECOGNITIVE• Not knowing how much to tell family, friendsNot knowing how much to tell family, friends• Loyalty conflictsLoyalty conflicts • • BoredomBoredom
EMOTIONALEMOTIONAL• Withdrawal from the rush of battleWithdrawal from the rush of battle
• • Feeling unsafe Feeling unsafe • • HelplessnessHelplessness
SOCIALSOCIAL• Being separated from buddies and leadersBeing separated from buddies and leaders• Being overwhelmed/misunderstood by familyBeing overwhelmed/misunderstood by family
SPIRITUALSPIRITUAL• Difficulty making sense of what happenedDifficulty making sense of what happened• Guilt Guilt • • Conflicting valuesConflicting values

Three Tactics for Normal, Reversible Adaptation to Stress
ACCOMMODATEACCOMMODATE NEUTRALIZENEUTRALIZE DISENGAGEDISENGAGE
• Change yourself to better suit the stressor
• This makes you more tolerant to that particular stressor
• This is the goal of all training and education
• Eliminate or reduce the stressor
• This lessens the force and impact of that particular stressor
• A fast way to adapt, but often not possible
• Detach mentally from the environment, yourself, or both
• Examples: denial, withdrawal, numbness
• Stores up stress for later processing

Three Phases of Normal Adaptation
-80%
-40%
0%
40%
80%
“In the Groove”
Fatigue, Rebound
Dread, Alarm
Str
ess L
evel
Time
This time scale could be mere seconds (e.g., an all-out sprint), minutes (a single fire-fight), or months (an entire deployment)

Common “Rebound” Changes in Service Members After Deployment
• Aggressiveness– De-sensitized to aggression– Angry, irritable, agitated because of stress– May even crave violence as excitement
• Relative numbness– Numb to their own and others’ suffering– Numb to their own and others’ joy
• Becoming easily frustrated or overwhelmed• Feeling alienated from family and friends
at home• Having a hard time getting back into home/garrison
routines

Stress Injuries Occur When Stress Is Too Intense or Lasts Too Long
• Injury– May be more abrupt– A derailment, change in self– Individual loses control– Irreversible (though can heal)
• Adaptation– A gradual process– Can be traced over time– Individual remains in control– Reversible

Three Mechanisms of Stress Injury
TRAUMATRAUMATRAUMATRAUMA
• An impact injury
• Due to events involving terror, horror, or helplessness
GRIEFGRIEFGRIEFGRIEF
• A loss injury• Due to the loss
of people who are cared about
FATIGUEFATIGUEFATIGUEFATIGUE
• A wear-and-tear injury
• Due to the accumulation of stress over time
COMBAT / OPERATIONAL COMBAT / OPERATIONAL STRESSSTRESS
COMBAT / OPERATIONAL COMBAT / OPERATIONAL STRESSSTRESS

Operational Stress Injuries Correlate with DSM-IV Diagnoses
V62.82V62.82 MDDMDDASDASD
PTSDPTSD
TRAUMATRAUMATRAUMATRAUMA GRIEFGRIEFGRIEFGRIEFFATIGUEFATIGUEFATIGUEFATIGUE
COMBAT / OPERATIONAL STRESSCOMBAT / OPERATIONAL STRESSCOMBAT / OPERATIONAL STRESSCOMBAT / OPERATIONAL STRESS
GADGAD
PanicPanic
Adj D/OAdj D/O
MDDMDD

Traumatic Stress Injuries
• Abrupt injuries to the brain and mind• Due to specific event(s) that provoke:
– Terror, horror, or helplessness– Physiological hyper-arousal – Dissociation (abrupt and transient loss of mental integrity)– Damage to necessary or deeply-held beliefs– Shame or guilt

Traumatic Events in OIF
• Multi-casualty incidents (SVBIEDs, ambushes)• Friendly fire• Death or maiming of children and women• Seeing gruesome scenes of carnage• Handling dead bodies and body parts• “Avoidable” casualties and losses• Witnessed or committed atrocities• Witnessed death/injury of a close friend or leader• Killing unarmed or defenseless enemy• Being helpless to defend or counterattack• Injuries or near misses• Killing someone up close

The Greater the Exposure to Combat, the Higher the Risk for PTSD
Hoge et al. (2004)
4.5%
9.3%
12.7%
19.3%
0%
5%
10%
15%
20%
0 1-2 3-5 >5Number of firefights in Iraq in OEF & OIF-I
Sig
nifi
cant
PTSD
Sym
pto
ms
(3-
4 m
os.
afte
r O
EF
and
OIF
-I)

• Definition: A stress-induced, abrupt and transient loss of ability to integrate:– Perceptions (external and internal)– Thoughts, emotions, and behavior– Conceptions of the self and the world
• Three types or aspects– Going blank, like in a trance– Loss of control of one’s body (paralysis, deafness, stuttering, shaking,
blindness)– Change in personality (e.g., becoming cruel, fearless, or childlike)
• Always involves a loss of control — mentally, emotionally, and physically
Peri-Traumatic Dissociation

• Belief in one’s basic safety• Belief in being the master of oneself and one’s
environment• Belief in “what’s right” — moral order• Belief that “they” deserved to die, and we deserve
to live• Belief that our cause is honorable• Belief that every Marine and Soldier is valued• Belief in the basic goodness of people (especially
oneself)
Beliefs That Can Be Damaged By Traumatic Stress

• Failing to act• Surviving when others did not• Failing to save or protect others• Killing or injuring others• Helplessness• Loss of control• Even just having stress symptoms of any kind
Causes of Shame or Guilt In Traumatic Stress Injuries

• Allostatic shifts in set points in brain neurotransmitter systems due to stress NE activity, and down-regulation of alpha-2 autoreceptors CRF (corticotropin releasing factor) activity serotonin activity, and up-regulation of serotonin receptors NPY (neuropeptide-Y) activity
• Hippocampal dysfunction and possible neuronal damage– Cortisol toxicity to glutamate neurons BDNF (brain-derived neurotrophic factor)– Excitotoxicity mediated by glutamate NMDA receptors
What is Damaged in the Brain in Combat Stress Injuries?

• Most warfighters are resilient, and recover quickly from combat/operational and homecoming stress
• Aiding those with persistent stress problems requires sensitivity to military cultures & identity
• Common “normal” post-deployment stress problems include (1) aggression, (2) substance abuse, and (3) emotional numbness
• “Stress injuries” occur when stress is too intense or lasts too long
• The three mechanisms of stress injury are (1) trauma, (2) fatigue, and (3) grief
• Traumatic stress injuries are comprised of both biological damage to brain systems and psychosocial damage to beliefs and self-esteem
Summary