Embed Size (px)
Citation preview
InspyredThe alternative EAO voice
Volume 2, Issue 2 / Winter 2014
Is the McGill consensus always
the best option?
Highlights from this summer’s
meeting in Rome
Wiki-implants:Shedding light on problematic cases
A new protocol for immediate implants
The rule of the 5 triangles: A case report

Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 02
‘Is the McGill consensus always the best option?’,
by Niklas Karl Oskar Angelus
O ne of the most interesting messages I took home from the EAO’s 2012 scientific meeting in Copenhagen was that there is no longer 100% agreement
on the McGill consensus¹. This view has been confirmed by one of the most striking cases from my own practice, described below.
If a patient has teeth in the lower jaw prior to treatment, and these all have to be removed during treatment, they are unlikely to be satisfied with a denture that attaches on two implants, as the McGill consensus suggests. Instead, an implant-supported bridge is likely to be the preferred option. However, the patient’s viewpoint will probably be different if they had an edentulous lower jaw and a poor prosthesis prior to treatment. In that case, a prosthesis supported by two implants is likely to be acceptable.
By deciding which of these two categories a patient falls into, we can speculate whether treatment according to the McGill consensus is likely to be appropriate or not.
The following case involved a 66-year-old female patient who was a smoker. She was healthy apart from atrial fibrillation, and took anticoagulation. She had a history of periodontitis and told the practice that some of her teeth had fallen out spontaneously.
The patient was informed about the treatment options that were available to her. These were:
a total prosthesis in the upper and lower jaw a total prosthesis in the upper jaw and an implant-retained overdenture in the lower jaw
a total prosthesis in the upper jaw and an implant-retained bridge in the lower jaw
Having discussed the options carefully, she selected the second one. All her teeth were extracted and she was provided with a total prosthesis in the upper jaw and a temporary total prosthesis in the lower jaw. After a healing time of eight weeks, two implants (Nobel Replace 4.3x13) were installed in regions 32 and 42. Following healing time of three months², the temporary prosthesis in the lower jaw was replaced by an overdenture secured by two ball attachments. We chose not to use locator abutments because the patient described herself as having limited manual dexterity, and a ball attachment-based overdenture is considered to be easier to manage than a locator-based one.
After initially being very satisfied with the overdenture, the patient started to complain about loss of retention. The problem was treated chairside by adjusting the ball attachment device. The patient was satisfied for some weeks, but then came back to the office complaining that in her opinion the ball
attachments and the prosthesis no longer fitted together properly. Having discussed the problem with the dental technician, we decided to reline the prosthesis. During this process, I started thinking about a lecture at the EAO’s 2011 conference in Athens, during which Professor S Eitner presented a thesis that in some cases his only explanation for an implant-related prosthodontic problem is that the implants have started wandering within the jaw. Although I feared this may have happened to this patient, I couldn’t find any signs that the implants had wandered.
The relined prosthesis solved the problem for some time, but the patient continued to be unsatisfied. Other factors contributed to the problems she was experiencing, including poor oral hygiene which resulted in calculus sticking to the ball attachments. Every time she came in for follow-up we pointed out this problem to her. However, over and above the poor maintenance, she still had an underlying dissatisfaction with her ball attachment-based overdenture. The literature says that overdentures secured by two implants may require some extra time chairside³, but my experience with this patient made me ask how much extra time should realistically be allowed for.
Discussion
Based on the patient’s history of smoking and severe periodontitis, I concluded that the treatment provided (a prosthesis supported by two implants) was a better option than an implant-supported bridge, as the former was easier to clean.
However, one argument against the chosen treatment was the age of the patient, which may have made it difficult for her to successfully adapt to removable prostheses. It has been documented that patients often find it difficult to use removable prostheses when they receive them late on in life.
A factor that may have led to the patient being dissatisfied was a failure to understand that an implant-retained overdenture isn’t a fixed prosthesis. Even though we always explain this to patients, they sometimes have difficulty understanding it because the implants themselves are fixed. This underlines the importance of providing clear information and discussing treatment options in detail.
In hindsight, a better option may have been to suggest an implant-retained bridge in the lower jaw. If one or two of the implants used to secure the bridge should subsequently fail, the remaining ones could be used for an implant-based overdenture at a later stage. This would provide the patient with the preferred option of a fixed prosthetic rehabilitation, the feeling of having her ‘own teeth’, and perhaps increased quality of life. Should the first option cease to be viable later on, the second option would be easy to implement.
Niklas Karl Oskar Angelus, Dr med dent (University of Ulm, Germany 1997), Spesialkompetanse implantatprotetikk (Haukeland Universitetssykehus Bergen, Norway 2010), private practice in Namsos, Norway.
The alternative voicePersonal opinions on implant related topics
03 | Volume 2, Issue 2: Winter 2014 | Inspyred: The alternative EAO voice
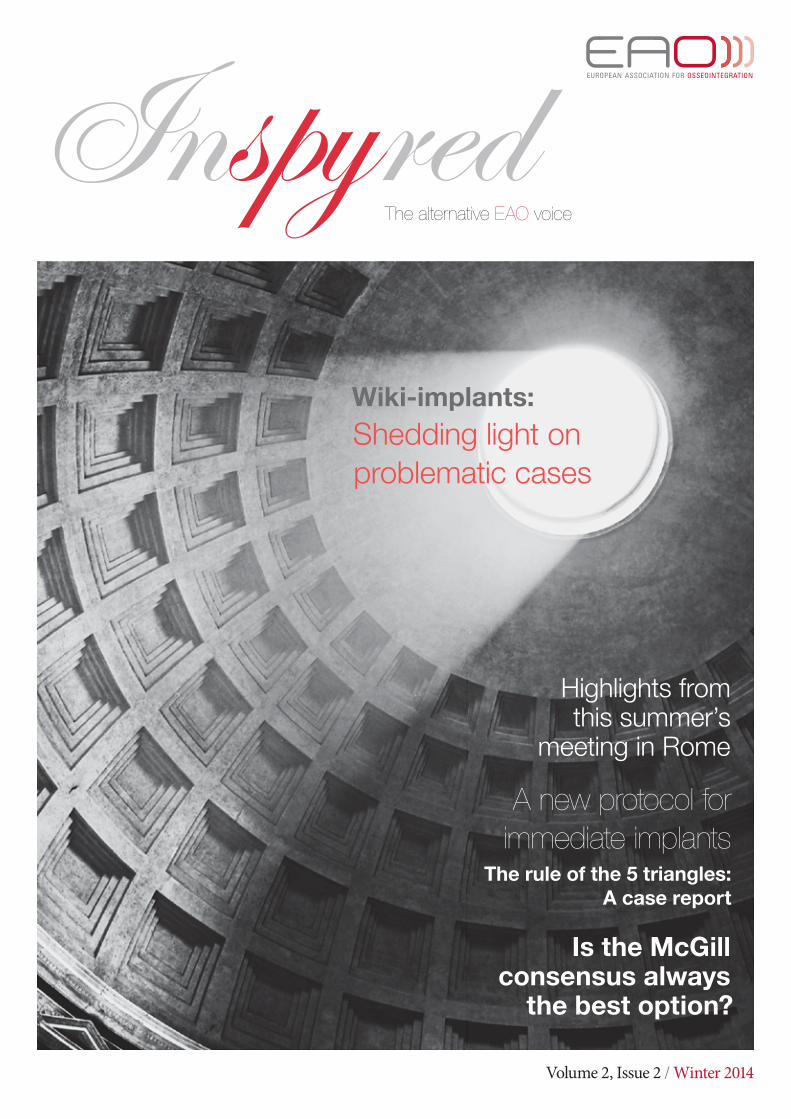
Figure 2. Implants installed.
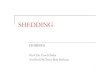
Figure 1. Status before treatment.
Figure 3. Coping abutments in situ.
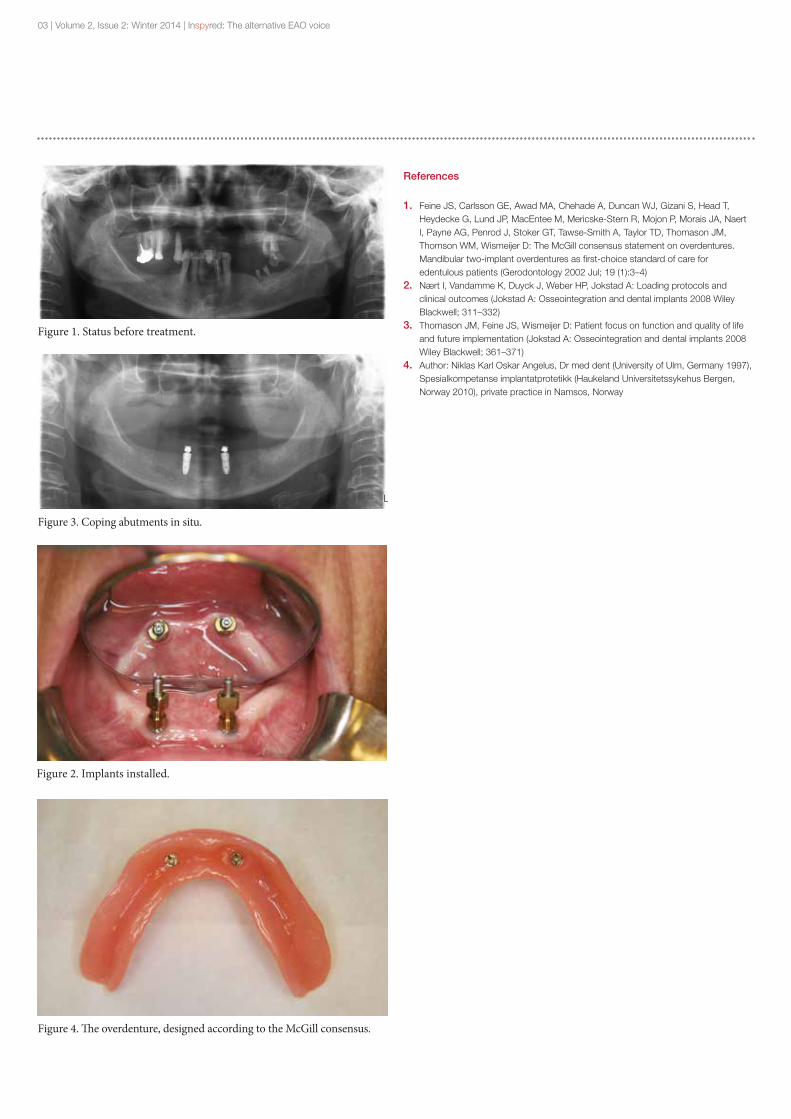
Figure 4. The overdenture, designed according to the McGill consensus.
References
1. Feine JS, Carlsson GE, Awad MA, Chehade A, Duncan WJ, Gizani S, Head T, Heydecke G, Lund JP, MacEntee M, Mericske-Stern R, Mojon P, Morais JA, Naert I, Payne AG, Penrod J, Stoker GT, Tawse-Smith A, Taylor TD, Thomason JM, Thomson WM, Wismeijer D: The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first-choice standard of care for edentulous patients (Gerodontology 2002 Jul; 19 (1):3–4)
2. Nært I, Vandamme K, Duyck J, Weber HP, Jokstad A: Loading protocols and clinical outcomes (Jokstad A: Osseointegration and dental implants 2008 Wiley Blackwell; 311–332)
3. Thomason JM, Feine JS, Wismeijer D: Patient focus on function and quality of life and future implementation (Jokstad A: Osseointegration and dental implants 2008 Wiley Blackwell; 361–371)
4. Author: Niklas Karl Oskar Angelus, Dr med dent (University of Ulm, Germany 1997), Spesialkompetanse implantatprotetikk (Haukeland Universitetssykehus Bergen, Norway 2010), private practice in Namsos, Norway
Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 04
W elcome to the fourth edition of Inspyred! We hope that you are starting to get a feel for the journal and are enjoying its mix of topical
interviews, opinion articles and clinical cases.We have deliberately selected ‘hot topics’ of the
moment to include in Inspyred. Th e aim is to challenge some of the preconceptions of our fi eld, and also to encourage your feedback. We would very much like to hear your views and comments on any articles you have particularly enjoyed. Equally, if you have a suggestion for an article for a future edition, please do let us know. You can get in touch at [email protected].
In September the EAO held its annual scientifi c meeting in Rome, which attracted over 4,000 attendees. Not surprisingly, the atmosphere in the historic city of Rome was unique. Th ere was a mixture of cutting-edge lectures and hands-on workshops, not to mention some wonderful social events. And above all it was a great chance to meet friends from around the world and network.
Th is issue includes a report on the Rome congress, an update on the 2014 EAO Junior Committee Summer Camp, plus clinical cases that include practical tips for your daily practice.
We have also introduced a new, regular feature for this edition: ‘wiki-implants’. It’s a place where you can share photographs and descriptions of a complication you have experienced in your practice. Each case is presented in a quick, concise way and you can be anonymous. Th e aim of wiki-implants is to gather and publish ‘real’ problematic cases, which will build up to create a valuable online resource of complications and how to avoid them. You’ll fi nd the fi rst two cases on the following pages, along with details of how to submit your own wiki case.
We hope you enjoy this issue of Inspyred. Please do keep in touch with us by emailing feedback and articles to [email protected].
Isabella Rocchietta and David Nisand
Editorial CommitteeDavid Nisand, France (Editor)Isabella Rocchietta, UK (Editor)Stefan Fickl, GermanyJaime Jiménez Garcia, SpainAilsa Nicol, UKIrena Sailer, SwitzerlandAlberto Sicilia, SpainTommie Van de Velde, Belgium
You can read about the EAO’s meeting in Rome on pages 22–23. A video was fi lmed at the meeting which you can view online by going to www.youtube.com and searching for ‘Who makes the EAO?’
Submit your own wiki-implant case to Inspyred! Visitwww.eao.org/inspyred for details of how to send us your case.
Editors welcomeHot topics in implant dentistry
05 | Volume 2, Issue 2: Winter 2014 | Inspyred: The alternative EAO voice
Authors: Jaime Jiménez García (pictured), DDS, PhD, Clinical Professor and Chairman of the Implant Department, School of Dentistry, Universidad Europea de Madrid. Madrid, Spain. Daniella Sanguino, DDS, Postgrad Implant Department, Universidad Europea de Madrid, School of Dentistry. Universidad Europea de Madrid. Madrid, Spain.
Correspondence to: Professor Dr Jaime Jiménez, [email protected]
Abstract:
To achieve excellence when placing immediate implants, the diagnosis and planning of the case must be precise. Th ere are 5 keys aspects to consider during the decision-making process, to help prevent blunders that can lead to diffi cult esthetic situations. Th e following are (I) the presence of a buccal plate, (II) primary stability, (III) implant design, (IV) fi lling of the gap between the buccal plate and the implant, and (V) tissue biotype.
Key words: immediate implants, buccal plate and immediate implants, aesthetic outcomes immediate implants
Introduction
Preserving soft and hard tissue once initiating an implant treatment is a crucial goal. Th e intention of placing immediate implants is to try to preserve tissue contour, dimension and also, decrease treatment time1. Nevertheless, immediate implants require a precise case selection to achieve successful results. If conditions are not favourable, an alternative approach,
like delayed placement, also has several advantages2.Moreover, appropriate surgical treatment,
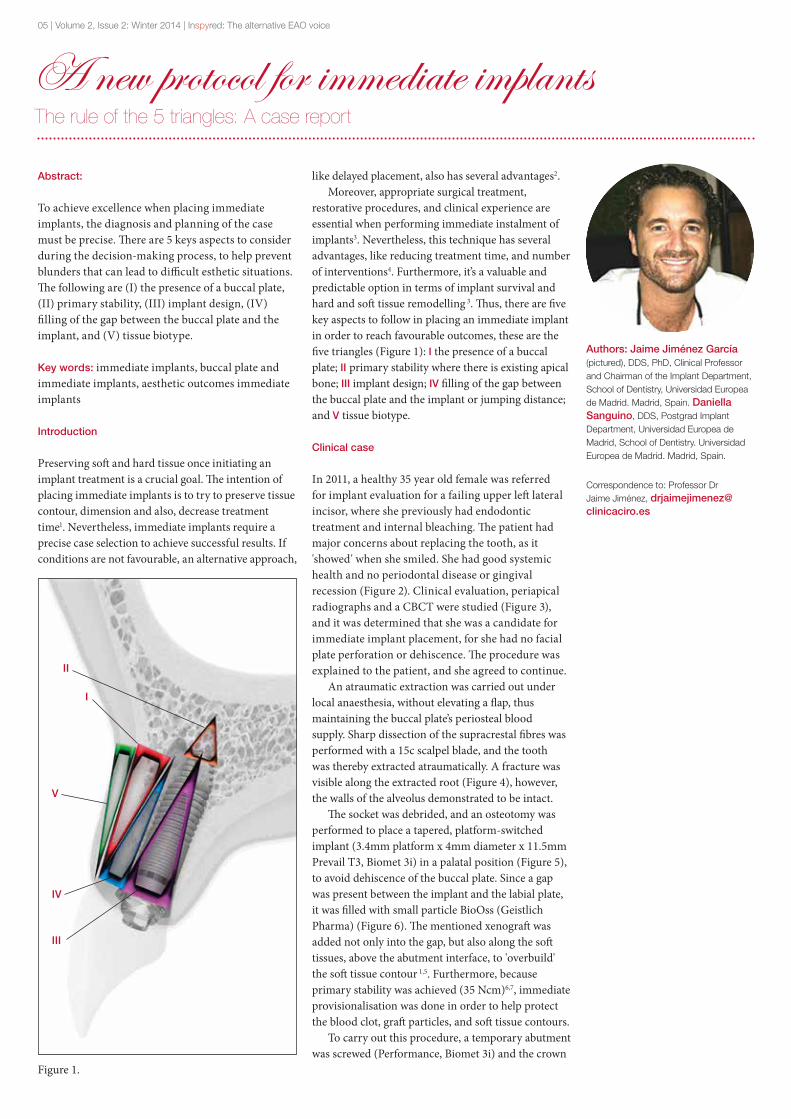
restorative procedures, and clinical experience are essential when performing immediate instalment of implants3. Nevertheless, this technique has several advantages, like reducing treatment time, and number of interventions4. Furthermore, it’s a valuable and predictable option in terms of implant survival and hard and soft tissue remodelling 3. Th us, there are fi ve key aspects to follow in placing an immediate implant in order to reach favourable outcomes, these are the fi ve triangles (Figure 1): I the presence of a buccal plate; II primary stability where there is existing apical bone; III implant design; IV fi lling of the gap between the buccal plate and the implant or jumping distance; and V tissue biotype.
Clinical case
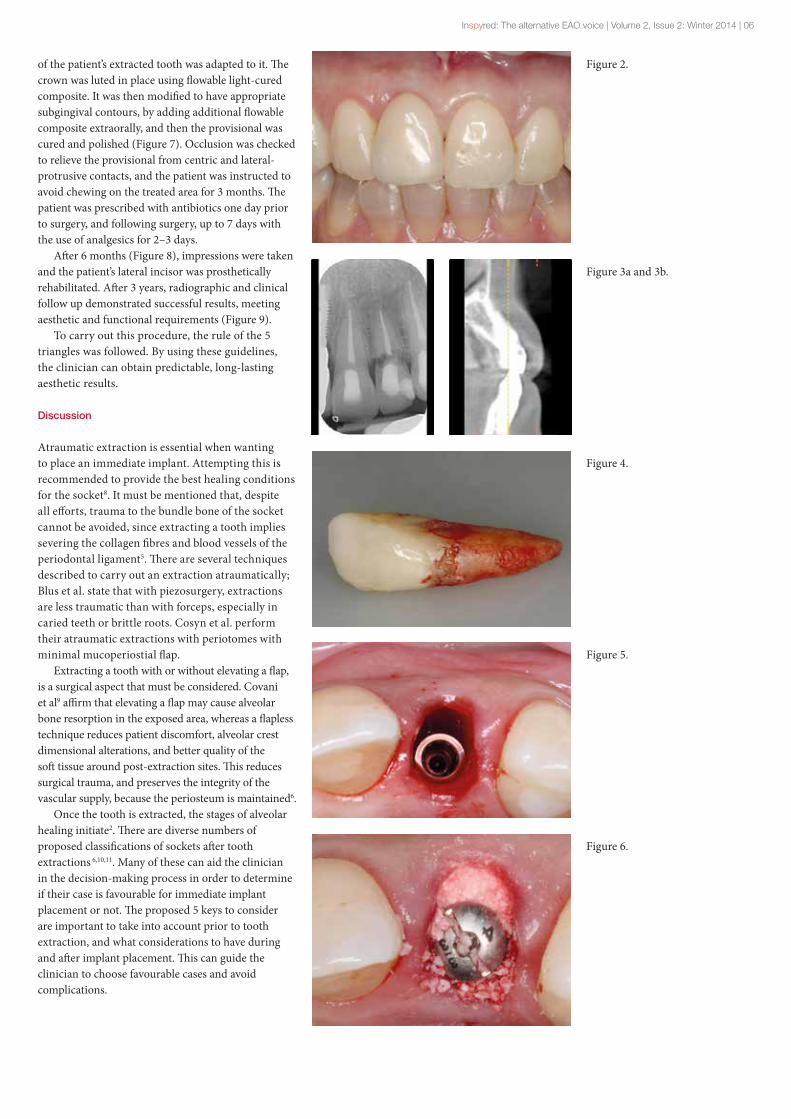
In 2011, a healthy 35 year old female was referred for implant evaluation for a failing upper left lateral incisor, where she previously had endodontic treatment and internal bleaching. Th e patient had major concerns about replacing the tooth, as it 'showed' when she smiled. She had good systemic health and no periodontal disease or gingival recession (Figure 2). Clinical evaluation, periapical radiographs and a CBCT were studied (Figure 3), and it was determined that she was a candidate for immediate implant placement, for she had no facial plate perforation or dehiscence. Th e procedure was explained to the patient, and she agreed to continue.
An atraumatic extraction was carried out under local anaesthesia, without elevating a fl ap, thus maintaining the buccal plate’s periosteal blood supply. Sharp dissection of the supracrestal fi bres was performed with a 15c scalpel blade, and the tooth was thereby extracted atraumatically. A fracture was visible along the extracted root (Figure 4), however, the walls of the alveolus demonstrated to be intact.
Th e socket was debrided, and an osteotomy was performed to place a tapered, platform-switched implant (3.4mm platform x 4mm diameter x 11.5mm Prevail T3, Biomet 3i) in a palatal position (Figure 5), to avoid dehiscence of the buccal plate. Since a gap was present between the implant and the labial plate, it was fi lled with small particle BioOss (Geistlich Pharma) (Figure 6). Th e mentioned xenograft was added not only into the gap, but also along the soft tissues, above the abutment interface, to 'overbuild' the soft tissue contour 1,5. Furthermore, because primary stability was achieved (35 Ncm)6,7, immediate provisionalisation was done in order to help protect the blood clot, graft particles, and soft tissue contours.
To carry out this procedure, a temporary abutment was screwed (Performance, Biomet 3i) and the crown
I
III
IV
V
II
Figure 1.
A new protocol for immediate implantsThe rule of the 5 triangles: A case report
Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 06
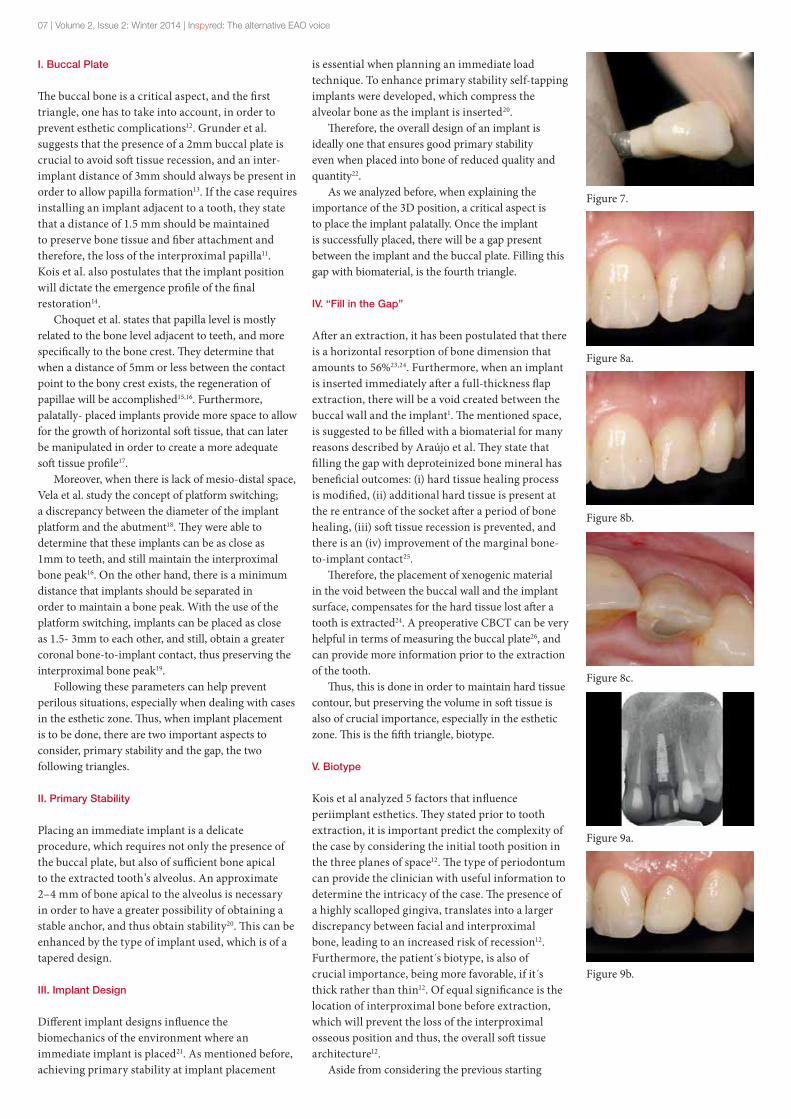
of the patient’s extracted tooth was adapted to it. The crown was luted in place using flowable light-cured composite. It was then modified to have appropriate subgingival contours, by adding additional flowable composite extraorally, and then the provisional was cured and polished (Figure 7). Occlusion was checked to relieve the provisional from centric and lateral-protrusive contacts, and the patient was instructed to avoid chewing on the treated area for 3 months. The patient was prescribed with antibiotics one day prior to surgery, and following surgery, up to 7 days with the use of analgesics for 2–3 days.
After 6 months (Figure 8), impressions were taken and the patient’s lateral incisor was prosthetically rehabilitated. After 3 years, radiographic and clinical follow up demonstrated successful results, meeting aesthetic and functional requirements (Figure 9).
To carry out this procedure, the rule of the 5 triangles was followed. By using these guidelines, the clinician can obtain predictable, long-lasting aesthetic results.
Discussion
Atraumatic extraction is essential when wanting to place an immediate implant. Attempting this is recommended to provide the best healing conditions for the socket8. It must be mentioned that, despite all efforts, trauma to the bundle bone of the socket cannot be avoided, since extracting a tooth implies severing the collagen fibres and blood vessels of the periodontal ligament5. There are several techniques described to carry out an extraction atraumatically; Blus et al. state that with piezosurgery, extractions are less traumatic than with forceps, especially in caried teeth or brittle roots. Cosyn et al. perform their atraumatic extractions with periotomes with minimal mucoperiostial flap.
Extracting a tooth with or without elevating a flap, is a surgical aspect that must be considered. Covani et al9 affirm that elevating a flap may cause alveolar bone resorption in the exposed area, whereas a flapless technique reduces patient discomfort, alveolar crest dimensional alterations, and better quality of the soft tissue around post-extraction sites. This reduces surgical trauma, and preserves the integrity of the vascular supply, because the periosteum is maintained6.
Once the tooth is extracted, the stages of alveolar healing initiate2. There are diverse numbers of proposed classifications of sockets after tooth extractions 6,10,11. Many of these can aid the clinician in the decision-making process in order to determine if their case is favourable for immediate implant placement or not. The proposed 5 keys to consider are important to take into account prior to tooth extraction, and what considerations to have during and after implant placement. This can guide the clinician to choose favourable cases and avoid complications.
Figure 2.
Figure 3a and 3b.
Figure 4.
Figure 5.
Figure 6.
07 | Volume 2, Issue 2: Winter 2014 | Inspyred: The alternative EAO voice
Figure 7.
Figure 8a.
Figure 8b.
Figure 8c.
Figure 9a.
Figure 9b.
I. Buccal Plate
The buccal bone is a critical aspect, and the first triangle, one has to take into account, in order to prevent esthetic complications12. Grunder et al. suggests that the presence of a 2mm buccal plate is crucial to avoid soft tissue recession, and an inter-implant distance of 3mm should always be present in order to allow papilla formation13. If the case requires installing an implant adjacent to a tooth, they state that a distance of 1.5 mm should be maintained to preserve bone tissue and fiber attachment and therefore, the loss of the interproximal papilla11. Kois et al. also postulates that the implant position will dictate the emergence profile of the final restoration14.
Choquet et al. states that papilla level is mostly related to the bone level adjacent to teeth, and more specifically to the bone crest. They determine that when a distance of 5mm or less between the contact point to the bony crest exists, the regeneration of papillae will be accomplished15,16. Furthermore, palatally- placed implants provide more space to allow for the growth of horizontal soft tissue, that can later be manipulated in order to create a more adequate soft tissue profile17.
Moreover, when there is lack of mesio-distal space, Vela et al. study the concept of platform switching; a discrepancy between the diameter of the implant platform and the abutment18. They were able to determine that these implants can be as close as 1mm to teeth, and still maintain the interproximal bone peak16. On the other hand, there is a minimum distance that implants should be separated in order to maintain a bone peak. With the use of the platform switching, implants can be placed as close as 1.5- 3mm to each other, and still, obtain a greater coronal bone-to-implant contact, thus preserving the interproximal bone peak19.
Following these parameters can help prevent perilous situations, especially when dealing with cases in the esthetic zone. Thus, when implant placement is to be done, there are two important aspects to consider, primary stability and the gap, the two following triangles.
II. Primary Stability
Placing an immediate implant is a delicate procedure, which requires not only the presence of the buccal plate, but also of sufficient bone apical to the extracted tooth’s alveolus. An approximate 2–4 mm of bone apical to the alveolus is necessary in order to have a greater possibility of obtaining a stable anchor, and thus obtain stability20. This can be enhanced by the type of implant used, which is of a tapered design.
III. Implant Design
Different implant designs influence the biomechanics of the environment where an immediate implant is placed21. As mentioned before, achieving primary stability at implant placement
is essential when planning an immediate load technique. To enhance primary stability self-tapping implants were developed, which compress the alveolar bone as the implant is inserted20.
Therefore, the overall design of an implant is ideally one that ensures good primary stability even when placed into bone of reduced quality and quantity22.
As we analyzed before, when explaining the importance of the 3D position, a critical aspect is to place the implant palatally. Once the implant is successfully placed, there will be a gap present between the implant and the buccal plate. Filling this gap with biomaterial, is the fourth triangle.
IV. “Fill in the Gap”
After an extraction, it has been postulated that there is a horizontal resorption of bone dimension that amounts to 56%23,24. Furthermore, when an implant is inserted immediately after a full-thickness flap extraction, there will be a void created between the buccal wall and the implant1. The mentioned space, is suggested to be filled with a biomaterial for many reasons described by Araújo et al. They state that filling the gap with deproteinized bone mineral has beneficial outcomes: (i) hard tissue healing process is modified, (ii) additional hard tissue is present at the re entrance of the socket after a period of bone healing, (iii) soft tissue recession is prevented, and there is an (iv) improvement of the marginal bone-to-implant contact25.
Therefore, the placement of xenogenic material in the void between the buccal wall and the implant surface, compensates for the hard tissue lost after a tooth is extracted24. A preoperative CBCT can be very helpful in terms of measuring the buccal plate26, and can provide more information prior to the extraction of the tooth.
Thus, this is done in order to maintain hard tissue contour, but preserving the volume in soft tissue is also of crucial importance, especially in the esthetic zone. This is the fifth triangle, biotype.
V. Biotype
Kois et al analyzed 5 factors that influence periimplant esthetics. They stated prior to tooth extraction, it is important predict the complexity of the case by considering the initial tooth position in the three planes of space12. The type of periodontum can provide the clinician with useful information to determine the intricacy of the case. The presence of a highly scalloped gingiva, translates into a larger discrepancy between facial and interproximal bone, leading to an increased risk of recession12. Furthermore, the patient s biotype, is also of crucial importance, being more favorable, if it s thick rather than thin12. Of equal significance is the location of interproximal bone before extraction, which will prevent the loss of the interproximal osseous position and thus, the overall soft tissue architecture12.
Aside from considering the previous starting
Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 08
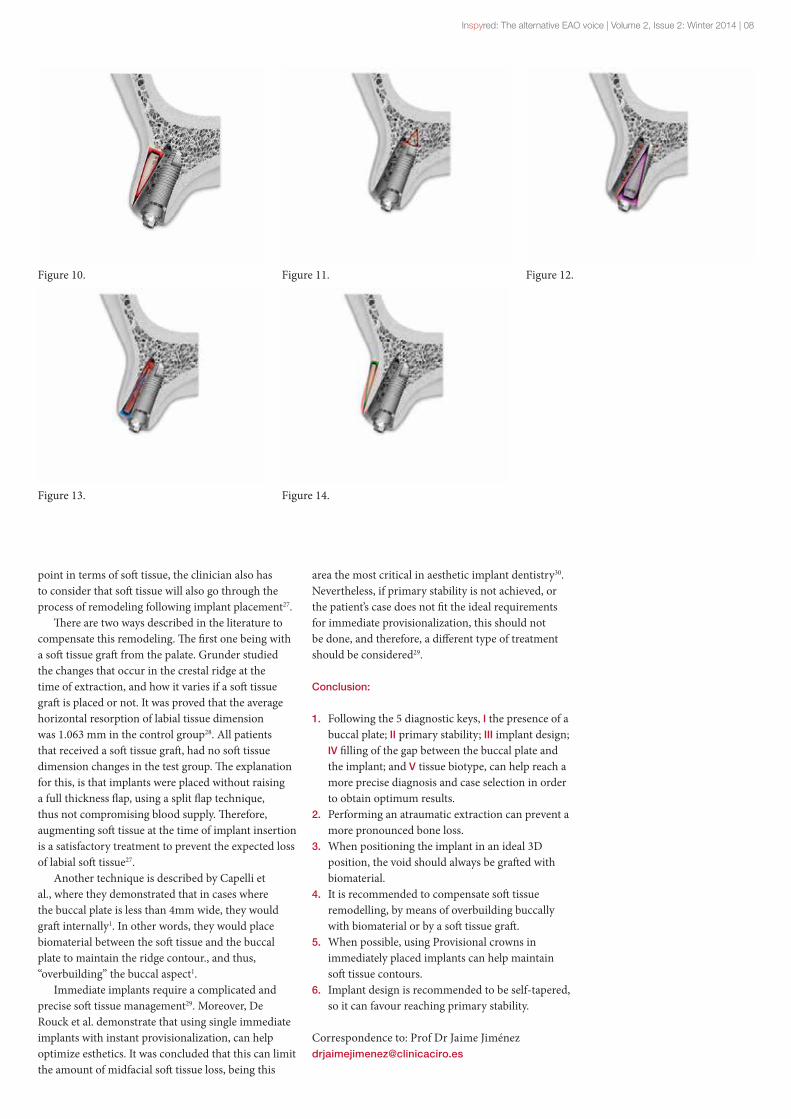
point in terms of soft tissue, the clinician also has to consider that soft tissue will also go through the process of remodeling following implant placement27.
There are two ways described in the literature to compensate this remodeling. The first one being with a soft tissue graft from the palate. Grunder studied the changes that occur in the crestal ridge at the time of extraction, and how it varies if a soft tissue graft is placed or not. It was proved that the average horizontal resorption of labial tissue dimension was 1.063 mm in the control group28. All patients that received a soft tissue graft, had no soft tissue dimension changes in the test group. The explanation for this, is that implants were placed without raising a full thickness flap, using a split flap technique, thus not compromising blood supply. Therefore, augmenting soft tissue at the time of implant insertion is a satisfactory treatment to prevent the expected loss of labial soft tissue27.
Another technique is described by Capelli et al., where they demonstrated that in cases where the buccal plate is less than 4mm wide, they would graft internally1. In other words, they would place biomaterial between the soft tissue and the buccal plate to maintain the ridge contour., and thus, “overbuilding” the buccal aspect1.
Immediate implants require a complicated and precise soft tissue management29. Moreover, De Rouck et al. demonstrate that using single immediate implants with instant provisionalization, can help optimize esthetics. It was concluded that this can limit the amount of midfacial soft tissue loss, being this
area the most critical in aesthetic implant dentistry30. Nevertheless, if primary stability is not achieved, or the patient’s case does not fit the ideal requirements for immediate provisionalization, this should not be done, and therefore, a different type of treatment should be considered29.
Conclusion:
1. Following the 5 diagnostic keys, I the presence of a buccal plate; II primary stability; III implant design; IV filling of the gap between the buccal plate and the implant; and V tissue biotype, can help reach a more precise diagnosis and case selection in order to obtain optimum results.
2. Performing an atraumatic extraction can prevent a more pronounced bone loss.
3. When positioning the implant in an ideal 3D position, the void should always be grafted with biomaterial.
4. It is recommended to compensate soft tissue remodelling, by means of overbuilding buccally with biomaterial or by a soft tissue graft.
5. When possible, using Provisional crowns in immediately placed implants can help maintain soft tissue contours.
6. Implant design is recommended to be self-tapered, so it can favour reaching primary stability.
Correspondence to: Prof Dr Jaime Jiménez [email protected]
Figure 10.
Figure 13. Figure 14.
Figure 11. Figure 12.
09 | Volume 2, Issue 2: Winter 2014 | Inspyred: The alternative EAO voice
References
1. Capelli M, Testori T, Galli F, Zuffetti F, Motroni A, Weinstein R, Del Fabbro M. Implant–Buccal Plate Distance as Diagnostic Parameter: A Prospective Cohort Study on Implant Placement in Fresh Extraction Sockets. Journal of Periodontology 2013 84:12, 1768–1774
2. Chen ST, Wilson TG Jr, Hämmerle CH.Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes. Int J Oral Maxillofac Implants. 2004;19 Suppl:12–25.
3. Cosyn J, Sabzevar MM, De Bruyn H. Predictors of inter-proximal and midfacial recession following single implant treatment in the anterior maxilla: a multivariate analysis. J Clin Periodontol 2012; 39: 895–903
4. Marconcini S, Barone A, Gelpi F, Briguglio F, Covani U. Immediate Implant Placement in Infected Sites: A Case Series Journal of Periodontology 2013 84:2, 196–202
5. Tarnow D, Chu Stephen J,. Salama, Maurice A, Stappert Christian F.J., Salama Henry,. Garber, David A, Sarnachiaro Guido O, Sarnachiaro Evangelina, Gotta Sergio Luis, Saito Hanae. Flapless postextraction socket implant plaement in the esthetic zone: part 1. The effectof bone frafting and/or provisional restoration on the facial-palatal ridge dimensional change--A Retrospective cohort study.
6. Norton. The influence of insertion torque on the survival of immediately placed and restored single-tooth implants. Int J Oral Maxillofac Implants. 2011 Nov-Dec;26(6):1333–43.
7. Juodzbalys G(1), Wang HL. Socket morphology-based treatment for implant esthetics: a pilot study. Int J Oral Maxillofac Implants. 2010 Sep-Oct;25(5):970–8
8. Blus C, Szmukler-Moncler S.Atraumatic Tooth Extraction and Immediate Implant Placement with Piezosurgery: Evaluation of 40 sites after at least 1 year of loading. Int J Periodontics Restorative Dent 2010;30:355–363
9. Covani U, Cornelini R, Barone A. Buccal bone augmentation around implants with and without flap elevation: a modified approach. Int J Oral Maxillofac Implants 2008;23: 841–846
10. Hämmerle CH, Chen ST, Wilson TG Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int J Oral Maxillofac Implants. 2004;19 Suppl:26–8
11. Juodzbalys G(1), Sakavicius D, Wang HL Classification of extraction sockets based upon soft and hard tissue components. J Periodontol. 2008 Mar;79(3):413–24
12. Park JB. Immediate placement of dental implants into fresh extraction socket in the maxillary anterior region: a case report. J Oral Implantol. 2010;36(2):153–7
13. Grunder U, Gracis S, Capelli M. Influence of the 3D bone-to-implant relationship on esthetics. Int J Periodontics Restorative Dent. 2005 Apr; 25(2):113–9
14. Kois JC. Predictable single-tooth peri-implant esthetics. five diagnostic keys. Compend Contin Educ Dent. 2004 Nov;25(11):895–6, 898, 900
15. Choquet V, Hermans M, Adriaenssens P, Daelemans P, Tarnow DP, Malevez C. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region.J Periodontol. 2001 Oct;72(10):1364–71.
16. Caneva M1, Salata LA, de Souza SS, Baffone G, Lang NP, Botticelli D. Influence of implant positioning in extraction sockets on osseointegration: histomorphometric analyses in dogs.Clin Oral Implants Res. 2010 Jan;21(1):43–9
17. Chuan-Yi Su, Fu J, and Wang HL. The Role Of Implant Position On Its Long Term Success Clinical Advances in Periodontics 2013,0:0 1–4
18. Vela X, Méndez V, Rodríguez X, Segalà, M, Tarnow, D. Crestal bone changes on platform-switched implants and adjacent teeth when the tooth-implant distance is less than 1.5 mm. Int J Periodontics Restorative Dent 2012;32:149–155
19. Rodriguez X, Vela X, Segalà, M, Clavo J, Cambra J, Méndez V, Tarnow, D. The effect of interimplant distance on the height of the interimplant bone crest when using platform-switched implants. Int J Periodontics Restorative Dent 2009;29:141–151
20. Schwartz D, Chaushu. The ways and wherefores of immediate placement of implants into fresh extraction sites: a literature review. J Periodontol 1997;68:915–923
21. Pessoa RS, Coelho PG, Muraru L, Marcantonio E Jr, Vaz LG, Vander Sloten J, Jaecques SV. Influence of implant design on the biomechanical environment of immediately placed implants: computed tomography-based nonlinear three-dimensional finite element analysis. Int J Oral Maxillofac Implants. 2011 Nov-Dec;26(6):1279–87
22. O'Sullivan D, Sennerby L, Meredith N. Influence of implant taper on the primary and secondary stability of osseointegrated titanium implants.Clin Oral Implants Res. 2004 Aug;15(4):474–80.
23. Botticelli D, Berglundh T, Lindhe J: Hard-tissue alterations following immediate implant placement in extraction sites. J Clin Periodontol 2004; 31: 820–828
24. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003 Aug;23(4):313–23
25. Araújo MG, Linder E, Lindhe J. Bio-Oss collagen in the buccal gap at immediate implants: a 6-month study in the dog. Clin Oral Implants Res. 2011 Jan;22(1):1–8.
26. Benic GI, Mokti M, Chen CJ, Weber HP, Hämmerle CH, Gallucci GO. Dimensions of buccal bone and mucosa at immediately placed implants after 7 years: a clinical and cone beam computed tomography study. Clin Oral Implants Res. 2012 May;23(5):560–6
27. Rungcharassaeng K1, Kan JY, Yoshino S, Morimoto T, Zimmerman G. Immediate implant placement and provisionalization with and without a connective tissue graft: an analysis of facial gingival tissue thickness
28. Grunder U. Crestal ridge width changes when placing implants at the time of tooth extraction with and without soft tissue augmentation after a healing period of 6 months: report of 24 consecutive cases.Int J Periodontics Restorative Dent. 2011 Feb;31(1):9–17.
29. Rosenquist B, Grenthe B. Immediate placement of implants into extraction sockets: implant survival. Int J Oral Maxillofacial Implants 1996: 11:205–209
30. De Rouck T, Collys K, Wyn I, Cosyn J. Instant provisionalization of immediate single-tooth implants is essential to optimize esthetic treatment outcome. Clin Oral Implants Res. 2009 Jun;20(6):566-70FIG 1
Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 10
Immediate implant placement in the aesthetic zoneStrategies for counteracting tissue deficiencies following implant placement
Introduction
Implants have evolved to become an important treatment strategy for replacing missing or failing teeth. According to the Third International Team for Implantology (ITI) Consensus Conference, dental implants can be placed into the extraction socket immediately; in a delayed fashion following soft tissue healing (4–8 weeks); in an early-delayed fashion following substantial hard tissue healing (12–16 weeks); or late on after complete socket healing1. Among these different options, immediate implant placement is often described as being particularly suitable for the aesthetic zone, due to the opportunities it provides for tissue preservation. On the other hand, it is also documented that immediate implant placement might be associated with certain risks, in particular buccal soft tissue dehiscences. A review by Hämmerle et al. stated that ‘immediate implant placement is primarily indicated in premolar sites with low aesthetic risk’2. The aim of this case report is to demonstrate measures that can be taken to potentially counteract tissue deficiencies following immediate implant placement.
Basic considerations
Multiple experimental and clinical studies have shown that tooth extraction is followed by substantial alterations of the ridge dimension. A meta-analysis by Tan et al. reports that bucco-lingual shrinkage after tooth extraction is 3.79 ± 0.23 mm3. It has also been demonstrated that immediate implant placement cannot counteract the resorptive processes that follow tooth extraction. However, recent scientific evidence clearly shows that these alterations are dependent on many variables, in particular the periodontal biotype of the patient and the thickness of the bone plate. Hence proper case selection may be associated with less atrophy following tooth extraction. Lee et al. report that following tooth extraction and immediate implant placement (presumably in cases where a proper case selection was performed) a bucco-lingual shrinkage of 1.07mm on the buccal and 0.78mm on the lingual can be expected4. This is clearly significantly less than reported previously.
As well as appropriate case selection (intact buccal bone plate; thick periodontal biotype), several surgical and technical factors may contribute to successful results when placing implants immediately. Among these, a one-stage procedure could potentially limit the resorptive process. De Rouck et al. demonstrated that immediately provisionalised implants reveal 2–3.5 fold less tissue shrinkage when compared with a provisional phase after tissue healing5. Additionally, immediate sealing of the implant-abutment junction using a platform-switched design could also be an important factor in reducing buccal dehiscences following implant placement. Canullo et al. revealed that immediate implants with a platform-switched design are associated with only minute buccal shrinkage, thus leading to soft tissue stability on the buccal and interproximal aspect6.
When proper case selection is performed and certain surgical and technical measures are taken, immediate implant placement can lead to aesthetically pleasing and successful restorations. However, the long-term prognosis of this procedure is still currently rather unclear.
Case report
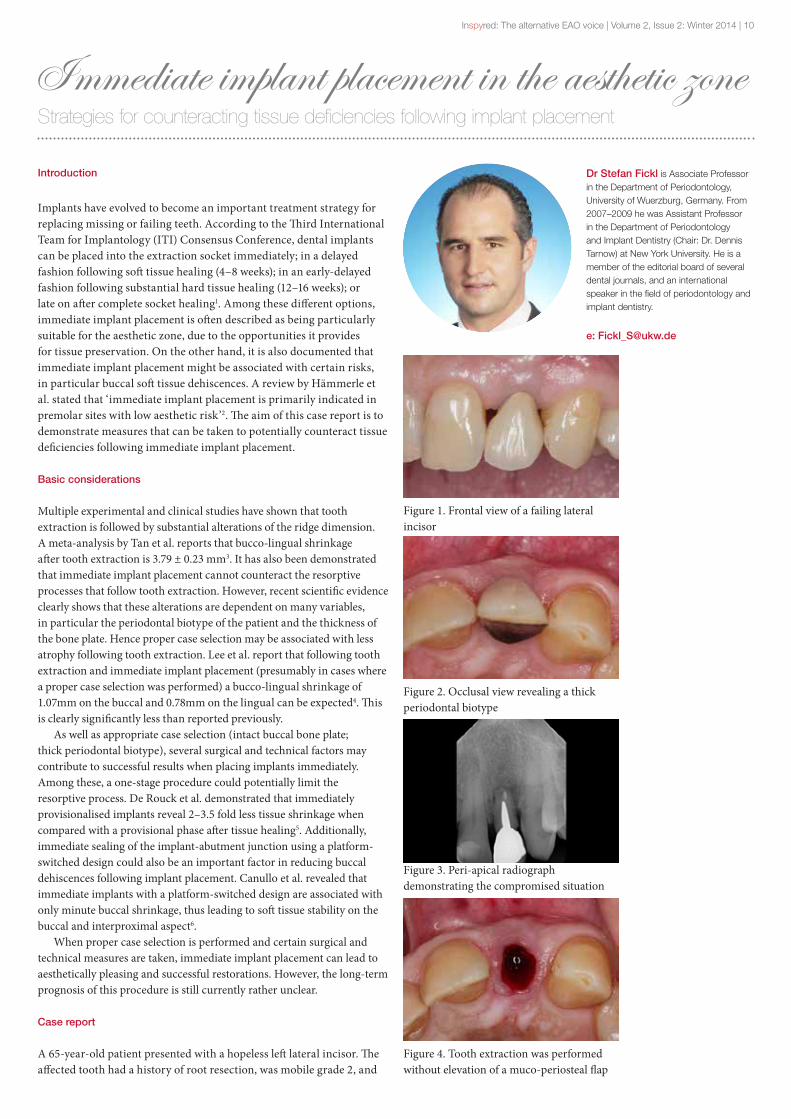
A 65-year-old patient presented with a hopeless left lateral incisor. The affected tooth had a history of root resection, was mobile grade 2, and
Dr Stefan Fickl is Associate Professor in the Department of Periodontology, University of Wuerzburg, Germany. From 2007–2009 he was Assistant Professor in the Department of Periodontology and Implant Dentistry (Chair: Dr. Dennis Tarnow) at New York University. He is a member of the editorial board of several dental journals, and an international speaker in the field of periodontology and implant dentistry.
Figure 1. Frontal view of a failing lateral incisor
Figure 2. Occlusal view revealing a thick periodontal biotype
Figure 3. Peri-apical radiograph demonstrating the compromised situation
Figure 4. Tooth extraction was performed without elevation of a muco-periosteal flap
11 | Volume 2, Issue 2: Winter 2014 | Inspyred: The alternative EAO voice
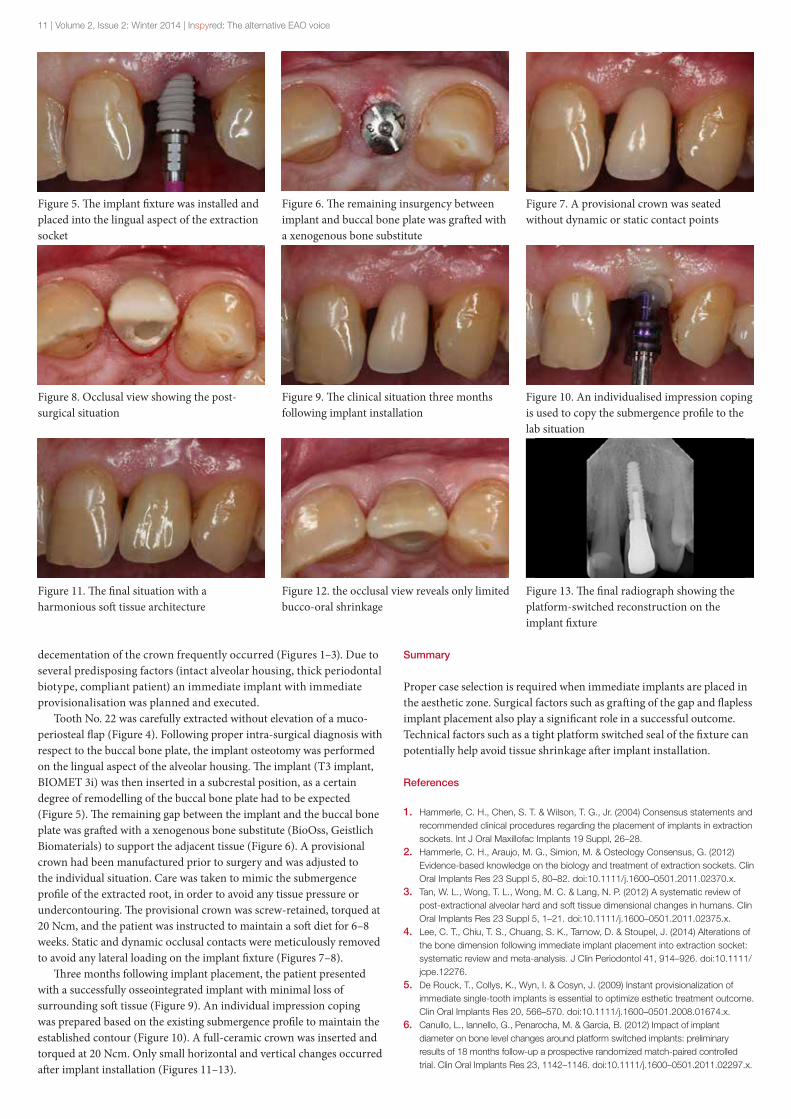
Figure 7. A provisional crown was seated without dynamic or static contact points
Figure 8. Occlusal view showing the post-surgical situation
Figure 11. The final situation with a harmonious soft tissue architecture
Figure 12. the occlusal view reveals only limited bucco-oral shrinkage
Figure 13. The final radiograph showing the platform-switched reconstruction on the implant fixture
Figure 9. The clinical situation three months following implant installation
Figure 10. An individualised impression coping is used to copy the submergence profile to the lab situation
Figure 5. The implant fixture was installed and placed into the lingual aspect of the extraction socket
Figure 6. The remaining insurgency between implant and buccal bone plate was grafted with a xenogenous bone substitute
decementation of the crown frequently occurred (Figures 1–3). Due to several predisposing factors (intact alveolar housing, thick periodontal biotype, compliant patient) an immediate implant with immediate provisionalisation was planned and executed.
Tooth No. 22 was carefully extracted without elevation of a muco-periosteal flap (Figure 4). Following proper intra-surgical diagnosis with respect to the buccal bone plate, the implant osteotomy was performed on the lingual aspect of the alveolar housing. The implant (T3 implant, BIOMET 3i) was then inserted in a subcrestal position, as a certain degree of remodelling of the buccal bone plate had to be expected (Figure 5). The remaining gap between the implant and the buccal bone plate was grafted with a xenogenous bone substitute (BioOss, Geistlich Biomaterials) to support the adjacent tissue (Figure 6). A provisional crown had been manufactured prior to surgery and was adjusted to the individual situation. Care was taken to mimic the submergence profile of the extracted root, in order to avoid any tissue pressure or undercontouring. The provisional crown was screw-retained, torqued at 20 Ncm, and the patient was instructed to maintain a soft diet for 6–8 weeks. Static and dynamic occlusal contacts were meticulously removed to avoid any lateral loading on the implant fixture (Figures 7–8).
Three months following implant placement, the patient presented with a successfully osseointegrated implant with minimal loss of surrounding soft tissue (Figure 9). An individual impression coping was prepared based on the existing submergence profile to maintain the established contour (Figure 10). A full-ceramic crown was inserted and torqued at 20 Ncm. Only small horizontal and vertical changes occurred after implant installation (Figures 11–13).
Summary
Proper case selection is required when immediate implants are placed in the aesthetic zone. Surgical factors such as grafting of the gap and flapless implant placement also play a significant role in a successful outcome. Technical factors such as a tight platform switched seal of the fixture can potentially help avoid tissue shrinkage after implant installation.
References
1. Hammerle, C. H., Chen, S. T. & Wilson, T. G., Jr. (2004) Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int J Oral Maxillofac Implants 19 Suppl, 26–28.
2. Hammerle, C. H., Araujo, M. G., Simion, M. & Osteology Consensus, G. (2012) Evidence-based knowledge on the biology and treatment of extraction sockets. Clin Oral Implants Res 23 Suppl 5, 80–82. doi:10.1111/j.1600–0501.2011.02370.x.
3. Tan, W. L., Wong, T. L., Wong, M. C. & Lang, N. P. (2012) A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res 23 Suppl 5, 1–21. doi:10.1111/j.1600–0501.2011.02375.x.
4. Lee, C. T., Chiu, T. S., Chuang, S. K., Tarnow, D. & Stoupel, J. (2014) Alterations of the bone dimension following immediate implant placement into extraction socket: systematic review and meta-analysis. J Clin Periodontol 41, 914–926. doi:10.1111/jcpe.12276.
5. De Rouck, T., Collys, K., Wyn, I. & Cosyn, J. (2009) Instant provisionalization of immediate single-tooth implants is essential to optimize esthetic treatment outcome. Clin Oral Implants Res 20, 566–570. doi:10.1111/j.1600–0501.2008.01674.x.
6. Canullo, L., Iannello, G., Penarocha, M. & Garcia, B. (2012) Impact of implant diameter on bone level changes around platform switched implants: preliminary results of 18 months follow-up a prospective randomized match-paired controlled trial. Clin Oral Implants Res 23, 1142–1146. doi:10.1111/j.1600–0501.2011.02297.x.
Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 12
Wiki-implantsDiscover other people's failed cases and learn how to avoid the same problems yourself!
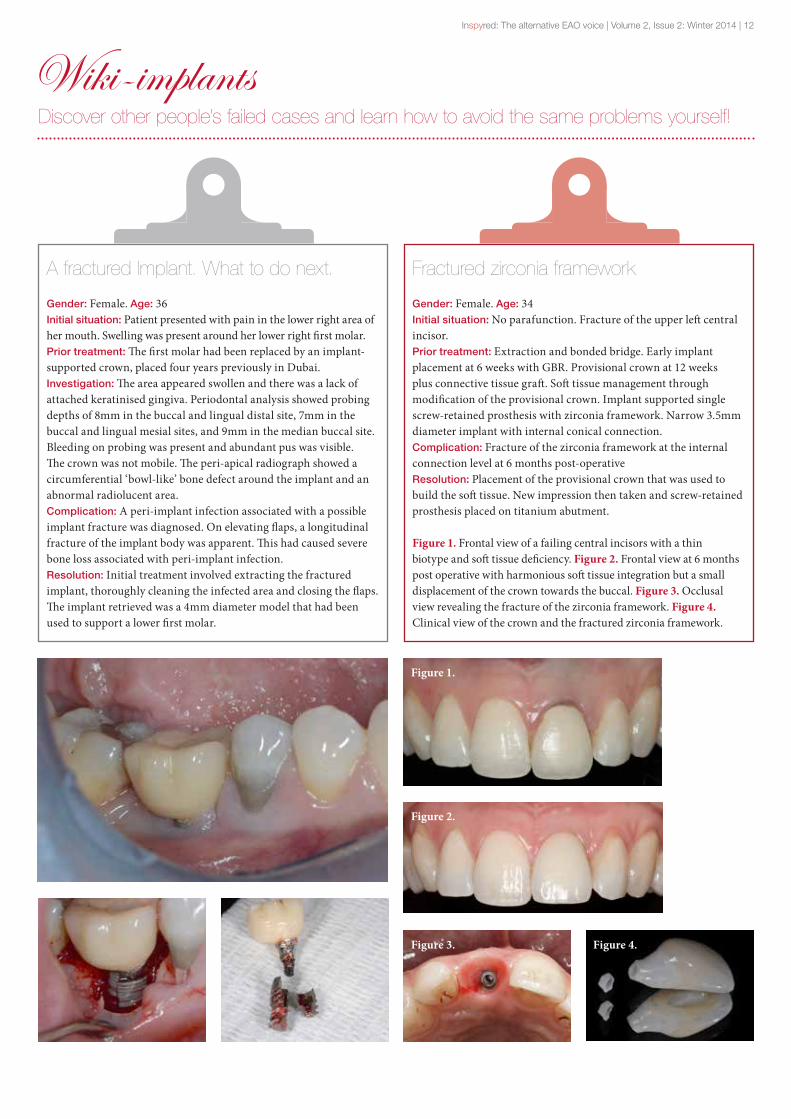
A fractured Implant. What to do next.
Gender: Female. Age: 36Initial situation: Patient presented with pain in the lower right area of her mouth. Swelling was present around her lower right first molar.Prior treatment: The first molar had been replaced by an implant-supported crown, placed four years previously in Dubai.Investigation: The area appeared swollen and there was a lack of attached keratinised gingiva. Periodontal analysis showed probing depths of 8mm in the buccal and lingual distal site, 7mm in the buccal and lingual mesial sites, and 9mm in the median buccal site. Bleeding on probing was present and abundant pus was visible. The crown was not mobile. The peri-apical radiograph showed a circumferential ‘bowl-like’ bone defect around the implant and an abnormal radiolucent area.Complication: A peri-implant infection associated with a possible implant fracture was diagnosed. On elevating flaps, a longitudinal fracture of the implant body was apparent. This had caused severe bone loss associated with peri-implant infection.Resolution: Initial treatment involved extracting the fractured implant, thoroughly cleaning the infected area and closing the flaps. The implant retrieved was a 4mm diameter model that had been used to support a lower first molar.
Fractured zirconia framework
Gender: Female. Age: 34Initial situation: No parafunction. Fracture of the upper left central incisor.Prior treatment: Extraction and bonded bridge. Early implant placement at 6 weeks with GBR. Provisional crown at 12 weeks plus connective tissue graft. Soft tissue management through modification of the provisional crown. Implant supported single screw-retained prosthesis with zirconia framework. Narrow 3.5mm diameter implant with internal conical connection.Complication: Fracture of the zirconia framework at the internal connection level at 6 months post-operativeResolution: Placement of the provisional crown that was used to build the soft tissue. New impression then taken and screw-retained prosthesis placed on titanium abutment.
Figure 1. Frontal view of a failing central incisors with a thin biotype and soft tissue deficiency. Figure 2. Frontal view at 6 months post operative with harmonious soft tissue integration but a small displacement of the crown towards the buccal. Figure 3. Occlusal view revealing the fracture of the zirconia framework. Figure 4. Clinical view of the crown and the fractured zirconia framework.
Figure 1.
Figure 2.
Figure 3. Figure 4.

13 | Volume 2, Issue 2: Winter 2014 | Inspyred: The alternative EAO voice
I n the last issue of Inspyred, we discussed a method to rationalise the clinical decision-making process. The article described a tool called FORDEC (Facts, Options, Risks, Decision, Execution, Check), which
was assessed during a serious game session at the 2012 French Dental Association (ADF) congress. A clinical situation was presented to a group of 719 clinicians. This involved a 28-year-old patient with a lower right first molar (n°46) and second premolar (n°45) with resorbed roots as a result of a supernumerary retained tooth (n°45’) (Figures 1 & 2). The first aim of this follow-up article is to go through the decision-making process and the treatment options proposed for this patient. The second aim is to assess the clinical consequences of using a decision-making tool.
Background and diagnosis
Tooth 45 exhibits a pressure root resorption. Tooth 46 exhibits an invasive cervical pressure resorption. The stimulation factor for both teeth appears to be the evolution of the retained supernumerary tooth1. According to Martinez-Gonzalez et al, a supernumerary premolar is recorded in 0.32% of the population. In 89% of these patients, this premolar is located in the mandible. A mechanical or obstructive pathology is associated with 2.7% of these supernumerary premolars2.
Prognosis
Analysis of the clinical situation dictates that at least one tooth has to be extracted. Root resorption resulting from a retained tooth is a well-recognised and well-documented phenomenon. In most cases, the resorption can be halted by the removal or displacement of the causal retained tooth3. However, the prognosis of tooth 45 is questionable due to its loss of distal attachment. The prognosis of tooth 46 remains questionable with regard to the degree of invasiveness of its cervical resorption, and a decision about which tooth should be extracted cannot be made at this point.
Options and external risks
A. Extraction of tooth 45. Following extraction of tooth 45, the only way to restore tooth 46 would be by using orthodontic treatment to move tooth 45’ into the 45 position. This treatment is complex, but theoretically possible. It requires a huge apical movement of 14mm. Its prognosis is not good, especially regarding the apical integrity of tooth 45’.
B. Extraction of tooth 46. Following extraction of tooth 46, tooth 45’ can be moved in the 46 position. The prognosis of this orthodontic option is good. Afterwards, two therapeutic options would remain.
B1. First, the orthodontic treatment could be continued to re-establish a continuous arch by mesialisation of teeth 45’ and 47. The short-term biologic cost of this option is low, but the occlusion would be altered and a long-term splinting would be required from tooth 45 to tooth 47.
B2. The second option would be to keep tooth 45’ in the 46 position and to change its anatomy with a prosthetic approach (ceramic crown on a vital tooth). The occlusion would be preserved and would act as a splint, but the biologic cost is of course higher and the functional forces on 45’ would be increased, altering its own prognosis.
C. Extraction of teeth 45 and 46. Extracting two teeth would lead to greater biological cost. Afterwards, tooth 45’ could be moved using orthodontic treatment. Depending on the target position chosen, this option could be seen as a second step following options A and B if the preserved tooth (45 or 46) proved to be hopeless and had to be extracted and replaced by an implant-supported crown.
D1. Extraction of teeth 45’ and 46. If these two teeth were extracted, the most rational option for replacing 46 would be an osseointegrated implant. This is because tooth 45, given its questionable prognosis, would not be a good candidate to support a fixed dental prosthesis. Regardless of the option chosen to replace 46 (see D2 below), this approach would not require an orthodontic stage, so the
Martin Brient had a variety of different jobs, including construction worker and bicycle mechanic, before receiving his dental degree from the University Paris-Descartes in 2003. He is currently a general dental practitioner in Paris.
Figure 1. Initial situation.
Figure 2. Initial situation.
Improving our clinical decisionsPart 2: decision-making and treatment implementation.
Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 14
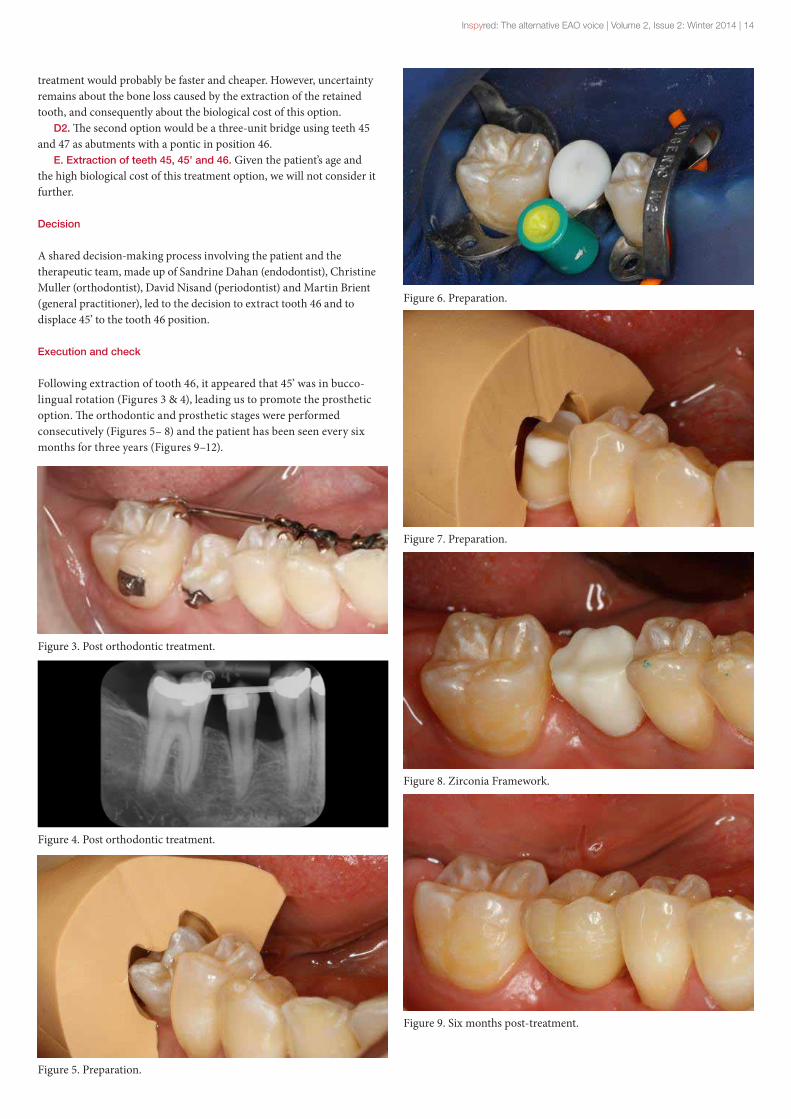
Figure 3. Post orthodontic treatment.
Figure 4. Post orthodontic treatment.
Figure 5. Preparation.
Figure 6. Preparation.
treatment would probably be faster and cheaper. However, uncertainty remains about the bone loss caused by the extraction of the retained tooth, and consequently about the biological cost of this option.
D2. The second option would be a three-unit bridge using teeth 45 and 47 as abutments with a pontic in position 46.
E. Extraction of teeth 45, 45’ and 46. Given the patient’s age and the high biological cost of this treatment option, we will not consider it further.
Decision
A shared decision-making process involving the patient and the therapeutic team, made up of Sandrine Dahan (endodontist), Christine Muller (orthodontist), David Nisand (periodontist) and Martin Brient (general practitioner), led to the decision to extract tooth 46 and to displace 45’ to the tooth 46 position.
Execution and check
Following extraction of tooth 46, it appeared that 45’ was in bucco-lingual rotation (Figures 3 & 4), leading us to promote the prosthetic option. The orthodontic and prosthetic stages were performed consecutively (Figures 5– 8) and the patient has been seen every six months for three years (Figures 9–12).
Figure 7. Preparation.
Figure 8. Zirconia Framework.
Figure 9. Six months post-treatment.
15 | Volume 2, Issue 2: Winter 2014 | Inspyred: The alternative EAO voice
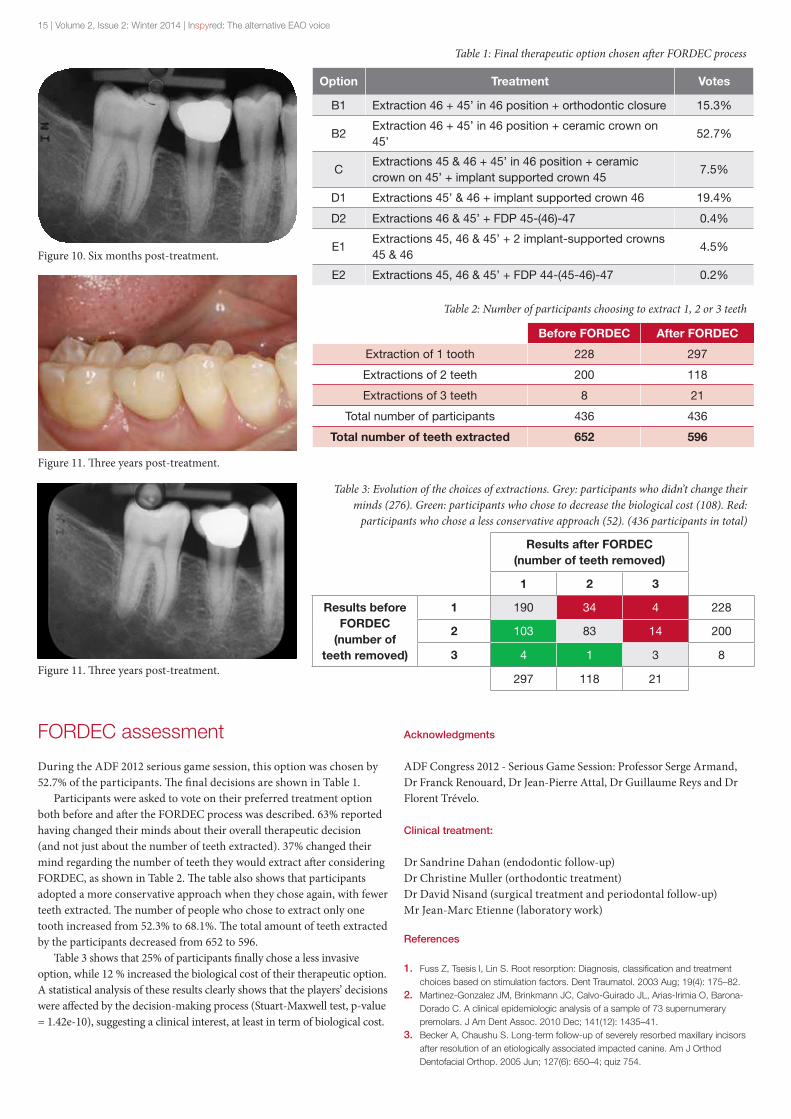
Table 1: Final therapeutic option chosen after FORDEC process
Option Treatment Votes
B1 Extraction 46 + 45’ in 46 position + orthodontic closure 15.3%
B2Extraction 46 + 45’ in 46 position + ceramic crown on 45’
52.7%
CExtractions 45 & 46 + 45’ in 46 position + ceramic crown on 45’ + implant supported crown 45
7.5%
D1 Extractions 45’ & 46 + implant supported crown 46 19.4%
D2 Extractions 46 & 45’ + FDP 45-(46)-47 0.4%
E1Extractions 45, 46 & 45’ + 2 implant-supported crowns 45 & 46
4.5%
E2 Extractions 45, 46 & 45’ + FDP 44-(45-46)-47 0.2%
Table 2: Number of participants choosing to extract 1, 2 or 3 teeth
Before FORDEC After FORDEC
Extraction of 1 tooth 228 297
Extractions of 2 teeth 200 118
Extractions of 3 teeth 8 21
Total number of participants 436 436
Total number of teeth extracted 652 596
Table 3: Evolution of the choices of extractions. Grey: participants who didn’t change their minds (276). Green: participants who chose to decrease the biological cost (108). Red:
participants who chose a less conservative approach (52). (436 participants in total)
Results after FORDEC (number of teeth removed)
1 2 3
Results before FORDEC
(number of teeth removed)
1 190 34 4 228
2 103 83 14 200
3 4 1 3 8
297 118 21
FORDEC assessment
During the ADF 2012 serious game session, this option was chosen by 52.7% of the participants. The final decisions are shown in Table 1.
Participants were asked to vote on their preferred treatment option both before and after the FORDEC process was described. 63% reported having changed their minds about their overall therapeutic decision (and not just about the number of teeth extracted). 37% changed their mind regarding the number of teeth they would extract after considering FORDEC, as shown in Table 2. The table also shows that participants adopted a more conservative approach when they chose again, with fewer teeth extracted. The number of people who chose to extract only one tooth increased from 52.3% to 68.1%. The total amount of teeth extracted by the participants decreased from 652 to 596.
Table 3 shows that 25% of participants finally chose a less invasive option, while 12 % increased the biological cost of their therapeutic option. A statistical analysis of these results clearly shows that the players’ decisions were affected by the decision-making process (Stuart-Maxwell test, p-value = 1.42e-10), suggesting a clinical interest, at least in term of biological cost.
Acknowledgments
ADF Congress 2012 - Serious Game Session: Professor Serge Armand, Dr Franck Renouard, Dr Jean-Pierre Attal, Dr Guillaume Reys and Dr Florent Trévelo.
Clinical treatment:
Dr Sandrine Dahan (endodontic follow-up)Dr Christine Muller (orthodontic treatment)Dr David Nisand (surgical treatment and periodontal follow-up)Mr Jean-Marc Etienne (laboratory work)
References
1. Fuss Z, Tsesis I, Lin S. Root resorption: Diagnosis, classification and treatment choices based on stimulation factors. Dent Traumatol. 2003 Aug; 19(4): 175–82.
2. Martinez-Gonzalez JM, Brinkmann JC, Calvo-Guirado JL, Arias-Irimia O, Barona-Dorado C. A clinical epidemiologic analysis of a sample of 73 supernumerary premolars. J Am Dent Assoc. 2010 Dec; 141(12): 1435–41.
3. Becker A, Chaushu S. Long-term follow-up of severely resorbed maxillary incisors after resolution of an etiologically associated impacted canine. Am J Orthod Dentofacial Orthop. 2005 Jun; 127(6): 650–4; quiz 754.
Figure 10. Six months post-treatment.
Figure 11. Three years post-treatment.
Figure 11. Three years post-treatment.
Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 16
Book now.
Limite
d pla
ces available
.
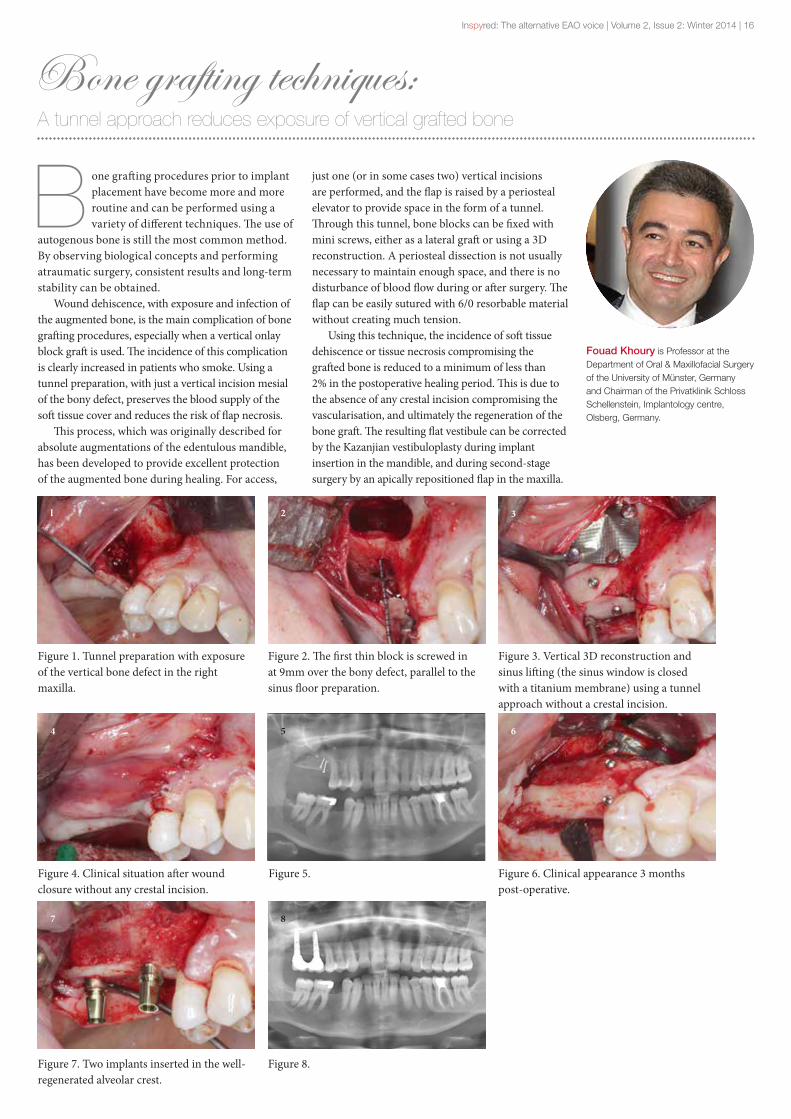
Bone grafting techniques:A tunnel approach reduces exposure of vertical grafted bone
B one grafting procedures prior to implant placement have become more and more routine and can be performed using a variety of different techniques. The use of
autogenous bone is still the most common method. By observing biological concepts and performing atraumatic surgery, consistent results and long-term stability can be obtained.
Wound dehiscence, with exposure and infection of the augmented bone, is the main complication of bone grafting procedures, especially when a vertical onlay block graft is used. The incidence of this complication is clearly increased in patients who smoke. Using a tunnel preparation, with just a vertical incision mesial of the bony defect, preserves the blood supply of the soft tissue cover and reduces the risk of flap necrosis.
This process, which was originally described for absolute augmentations of the edentulous mandible, has been developed to provide excellent protection of the augmented bone during healing. For access,
just one (or in some cases two) vertical incisions are performed, and the flap is raised by a periosteal elevator to provide space in the form of a tunnel. Through this tunnel, bone blocks can be fixed with mini screws, either as a lateral graft or using a 3D reconstruction. A periosteal dissection is not usually necessary to maintain enough space, and there is no disturbance of blood flow during or after surgery. The flap can be easily sutured with 6/0 resorbable material without creating much tension.
Using this technique, the incidence of soft tissue dehiscence or tissue necrosis compromising the grafted bone is reduced to a minimum of less than 2% in the postoperative healing period. This is due to the absence of any crestal incision compromising the vascularisation, and ultimately the regeneration of the bone graft. The resulting flat vestibule can be corrected by the Kazanjian vestibuloplasty during implant insertion in the mandible, and during second-stage surgery by an apically repositioned flap in the maxilla.
Fouad Khoury is Professor at the Department of Oral & Maxillofacial Surgery of the University of Münster, Germany and Chairman of the Privatklinik Schloss Schellenstein, Implantology centre, Olsberg, Germany.
l
Figure 1. Tunnel preparation with exposure of the vertical bone defect in the right maxilla.
4
Figure 4. Clinical situation after wound closure without any crestal incision.
7
Figure 7. Two implants inserted in the well-regenerated alveolar crest.
8
Figure 8.
5
Figure 5.
6
Figure 6. Clinical appearance 3 months post-operative.
2
Figure 2. The first thin block is screwed in at 9mm over the bony defect, parallel to the sinus floor preparation.
3
Figure 3. Vertical 3D reconstruction and sinus lifting (the sinus window is closed with a titanium membrane) using a tunnel approach without a crestal incision.
Book now.
Limite
d pla
ces available
.
To reserve your place, please contact Soazig Daniel, EAO Secretariat at [email protected] or on +33 (0) 1 44 64 15 15
Course fees
EAO members:1,190€
Non members:1,490€
MasterClinicians’
Course
Current concepts in bone grafting and soft tissue managementAdvanced surgical procedures with autogenous bone
Prof. Dr. Fouad Khoury, DMD, PhD
20–21 March 2015, Paris
The EAO is pleased to announce a Master Clinicians’ Course, hosted by Professor Fouad Khoury, on current concepts in bone grafting and soft tissue management. Don’t miss this opportunity to take part in a practical course with this world-renowned practitioner.
The course will cover topics including safe bone harvesting from all intraoral sites, and advanced grafting procedures, and will feature several practical elements.
EAO members receive a substantially discounted registration fee.
Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 18
Extrusion before extraction: an extra optionUsing orthodontic treatment to improve the outcome of implant placement
F rom an aesthetic perspective, the extraction of a central upper incisor and its replacement with an implant-supported crown is a particularly challenging treatment. It
becomes even more tricky and ‘dangerous’ when dealing with a young patient who has a high smile line, a thin-scalloped gingival biotype and particularly high aesthetic demands. For all these reasons every effort should be made to preserve a questionable anterior tooth in order to ensure preservation of the soft tissue architecture1,2.
Unfortunately, this is not always an option, as we sometimes have to deal with a hopeless tooth. One such example would be a huge and untreatable external root resorption class IV3, possibly caused by repeated trauma3, and combined with internal bleaching4,5. Such a case calls for extraction3.
In implant treatment, the crown can be designed to ideally mimic the symmetric situation on the contralateral site, provided that the implant is appropriately positioned. The aesthetic outcome is, however, often compromised due to soft tissue recession from unpredictable healing following tooth extraction and implant surgery. Incisors have a marked undulation of the cemento-enamel junction, as well as of the gingival margin, with long interproximal papillae. These are specific to anterior teeth and are bound to a sound periodontium. The collagen fibres in the gingiva surrounding teeth are attached to the root cementum and are arranged in groups or bundles. They have distinct orientations, including dentogingival, dentoperiosteal, circular and transseptal fibres6. Around implants, however, there is no periodontal ligament and the implant lacks a lining cementum with attached collagen fibres7. Implant treatment in external resorption cases is complicated by the fact that huge resorptions compromise not only the teeth but also the surrounding bone8.
When considering implant treatment, the presence of bone is the first determining factor for the soft tissue contour. The presence of a papilla depends on the level of the bone, the volume of the connective tissue, and the proximal support of the crowns9. When an implant is next to a tooth, the presence of the papilla is mostly determined by the bone peak level on the tooth side10,11. In order to preserve the bone level next to the adjacent teeth, the extraction has to be performed atraumatically. Additionally, the osseous lacuna should be filled with a biomaterial and the volume of the soft tissue may need to be improved. In the case presented here, a forced orthodontic extrusion of the tooth was performed before extraction in order to achieve the latter goal12.
Case presentation
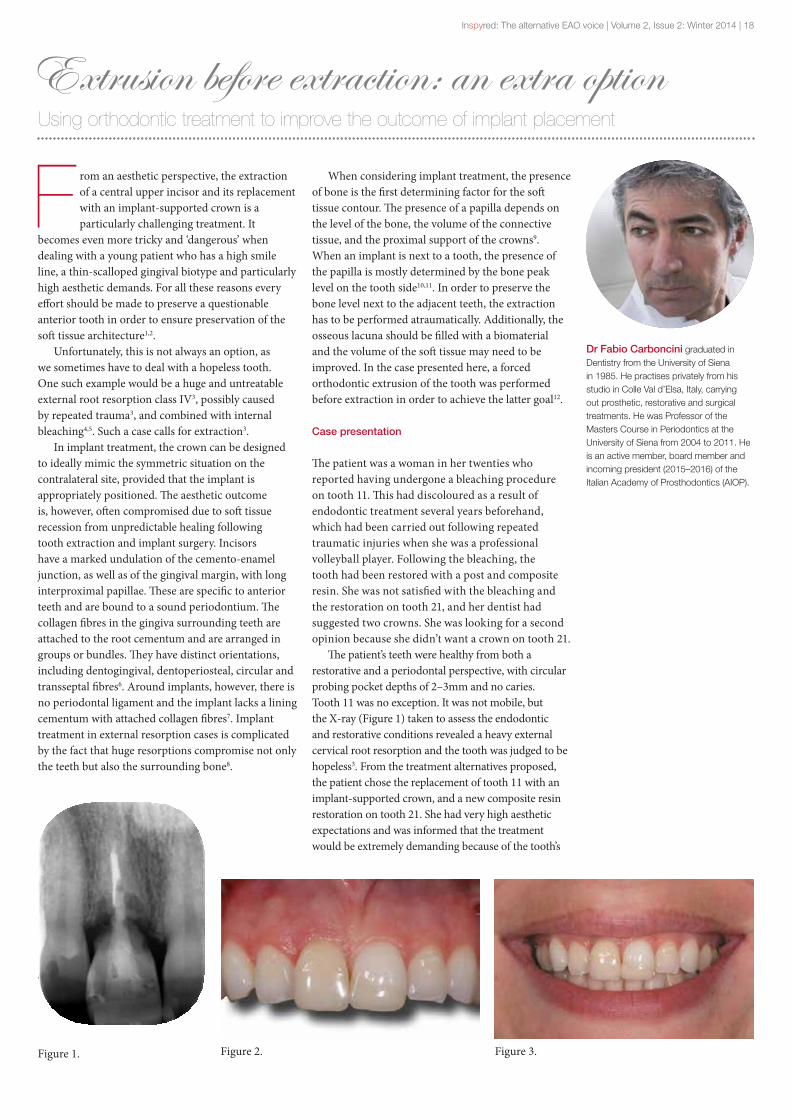
The patient was a woman in her twenties who reported having undergone a bleaching procedure on tooth 11. This had discoloured as a result of endodontic treatment several years beforehand, which had been carried out following repeated traumatic injuries when she was a professional volleyball player. Following the bleaching, the tooth had been restored with a post and composite resin. She was not satisfied with the bleaching and the restoration on tooth 21, and her dentist had suggested two crowns. She was looking for a second opinion because she didn’t want a crown on tooth 21.
The patient’s teeth were healthy from both a restorative and a periodontal perspective, with circular probing pocket depths of 2–3mm and no caries. Tooth 11 was no exception. It was not mobile, but the X-ray (Figure 1) taken to assess the endodontic and restorative conditions revealed a heavy external cervical root resorption and the tooth was judged to be hopeless3. From the treatment alternatives proposed, the patient chose the replacement of tooth 11 with an implant-supported crown, and a new composite resin restoration on tooth 21. She had very high aesthetic expectations and was informed that the treatment would be extremely demanding because of the tooth’s
Dr Fabio Carboncini graduated in Dentistry from the University of Siena in 1985. He practises privately from his studio in Colle Val d’Elsa, Italy, carrying out prosthetic, restorative and surgical treatments. He was Professor of the Masters Course in Periodontics at the University of Siena from 2004 to 2011. He is an active member, board member and incoming president (2015–2016) of the Italian Academy of Prosthodontics (AIOP).
Figure 3.Figure 1. Figure 2.
19 | Volume 2, Issue 2: Winter 2014 | Inspyred: The alternative EAO voice
position, her thin gingival biotype (Figure 2) and her high upper lip line (Figure 3).
The following treatment plan was proposed:
1. Orthodontic extrusion2. Extraction and socket preservation3. Implant placement and immediate temporary
crown4. Soft tissue modelling through temporary crown
management5. Final prosthetic restoration
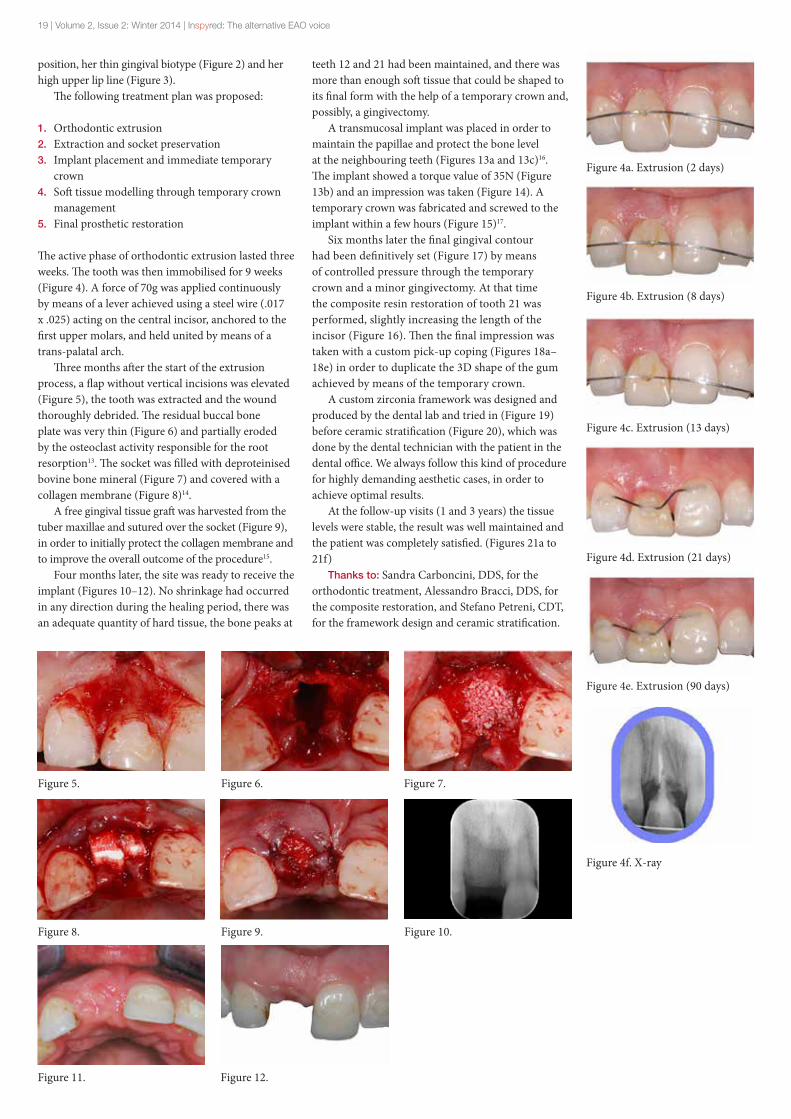
The active phase of orthodontic extrusion lasted three weeks. The tooth was then immobilised for 9 weeks (Figure 4). A force of 70g was applied continuously by means of a lever achieved using a steel wire (.017 x .025) acting on the central incisor, anchored to the first upper molars, and held united by means of a trans-palatal arch.
Three months after the start of the extrusion process, a flap without vertical incisions was elevated (Figure 5), the tooth was extracted and the wound thoroughly debrided. The residual buccal bone plate was very thin (Figure 6) and partially eroded by the osteoclast activity responsible for the root resorption13. The socket was filled with deproteinised bovine bone mineral (Figure 7) and covered with a collagen membrane (Figure 8)14.
A free gingival tissue graft was harvested from the tuber maxillae and sutured over the socket (Figure 9), in order to initially protect the collagen membrane and to improve the overall outcome of the procedure15.
Four months later, the site was ready to receive the implant (Figures 10–12). No shrinkage had occurred in any direction during the healing period, there was an adequate quantity of hard tissue, the bone peaks at
teeth 12 and 21 had been maintained, and there was more than enough soft tissue that could be shaped to its final form with the help of a temporary crown and, possibly, a gingivectomy.
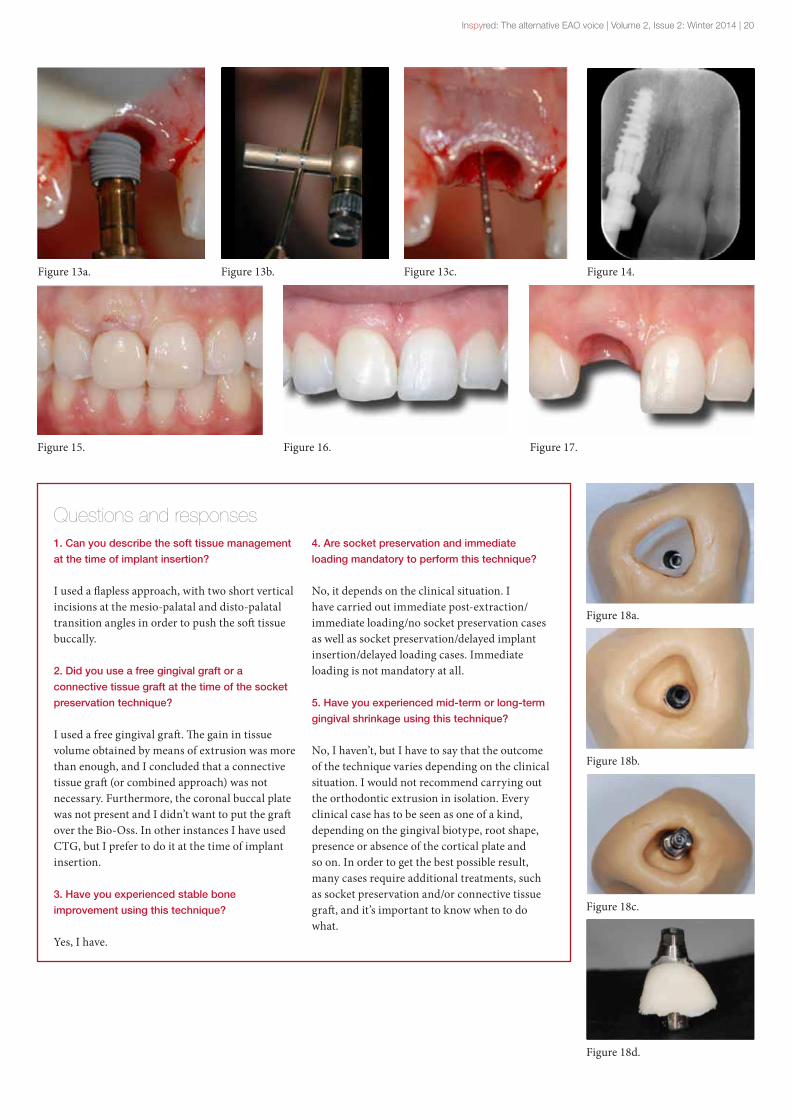
A transmucosal implant was placed in order to maintain the papillae and protect the bone level at the neighbouring teeth (Figures 13a and 13c)16. The implant showed a torque value of 35N (Figure 13b) and an impression was taken (Figure 14). A temporary crown was fabricated and screwed to the implant within a few hours (Figure 15)17.
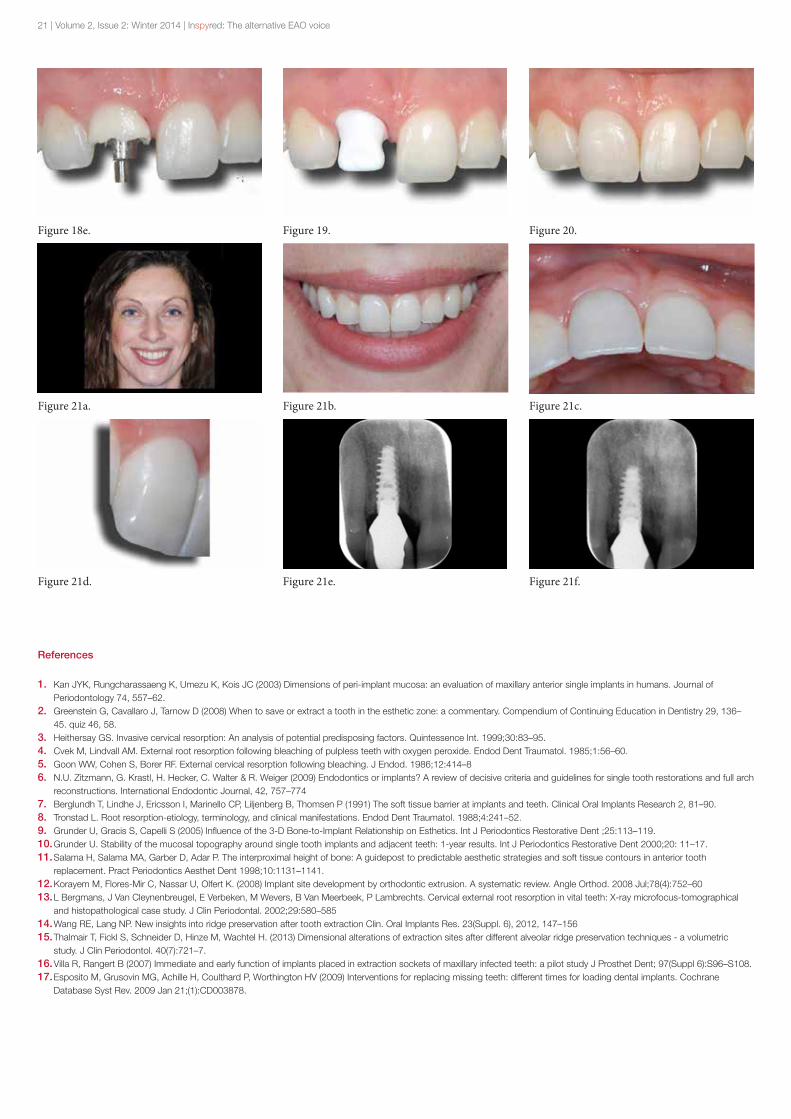
Six months later the final gingival contour had been definitively set (Figure 17) by means of controlled pressure through the temporary crown and a minor gingivectomy. At that time the composite resin restoration of tooth 21 was performed, slightly increasing the length of the incisor (Figure 16). Then the final impression was taken with a custom pick-up coping (Figures 18a–18e) in order to duplicate the 3D shape of the gum achieved by means of the temporary crown.
A custom zirconia framework was designed and produced by the dental lab and tried in (Figure 19) before ceramic stratification (Figure 20), which was done by the dental technician with the patient in the dental office. We always follow this kind of procedure for highly demanding aesthetic cases, in order to achieve optimal results.
At the follow-up visits (1 and 3 years) the tissue levels were stable, the result was well maintained and the patient was completely satisfied. (Figures 21a to 21f)
Thanks to: Sandra Carboncini, DDS, for the orthodontic treatment, Alessandro Bracci, DDS, for the composite restoration, and Stefano Petreni, CDT, for the framework design and ceramic stratification.
Figure 4a. Extrusion (2 days)
Figure 4b. Extrusion (8 days)
Figure 4c. Extrusion (13 days)
Figure 4d. Extrusion (21 days)
Figure 4e. Extrusion (90 days)
Figure 4f. X-ray
Figure 5.
Figure 8.
Figure 11. Figure 12.
Figure 9. Figure 10.
Figure 6. Figure 7.
Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 20
Figure 13a.
Figure 16.Figure 15. Figure 17.
Figure 18a.
Figure 18b.
Figure 18c.
Figure 18d.
Figure 13b. Figure 13c. Figure 14.
Questions and responses1. Can you describe the soft tissue management
at the time of implant insertion?
I used a flapless approach, with two short vertical incisions at the mesio-palatal and disto-palatal transition angles in order to push the soft tissue buccally.
2. Did you use a free gingival graft or a
connective tissue graft at the time of the socket
preservation technique?
I used a free gingival graft. The gain in tissue volume obtained by means of extrusion was more than enough, and I concluded that a connective tissue graft (or combined approach) was not necessary. Furthermore, the coronal buccal plate was not present and I didn’t want to put the graft over the Bio-Oss. In other instances I have used CTG, but I prefer to do it at the time of implant insertion.
3. Have you experienced stable bone
improvement using this technique?
Yes, I have.
4. Are socket preservation and immediate
loading mandatory to perform this technique?
No, it depends on the clinical situation. I have carried out immediate post-extraction/immediate loading/no socket preservation cases as well as socket preservation/delayed implant insertion/delayed loading cases. Immediate loading is not mandatory at all.
5. Have you experienced mid-term or long-term
gingival shrinkage using this technique?
No, I haven’t, but I have to say that the outcome of the technique varies depending on the clinical situation. I would not recommend carrying out the orthodontic extrusion in isolation. Every clinical case has to be seen as one of a kind, depending on the gingival biotype, root shape, presence or absence of the cortical plate and so on. In order to get the best possible result, many cases require additional treatments, such as socket preservation and/or connective tissue graft, and it’s important to know when to do what.
21 | Volume 2, Issue 2: Winter 2014 | Inspyred: The alternative EAO voice
References
1. Kan JYK, Rungcharassaeng K, Umezu K, Kois JC (2003) Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humans. Journal of Periodontology 74, 557–62.
2. Greenstein G, Cavallaro J, Tarnow D (2008) When to save or extract a tooth in the esthetic zone: a commentary. Compendium of Continuing Education in Dentistry 29, 136– 45. quiz 46, 58.
3. Heithersay GS. Invasive cervical resorption: An analysis of potential predisposing factors. Quintessence Int. 1999;30:83–95.4. Cvek M, Lindvall AM. External root resorption following bleaching of pulpless teeth with oxygen peroxide. Endod Dent Traumatol. 1985;1:56–60.5. Goon WW, Cohen S, Borer RF. External cervical resorption following bleaching. J Endod. 1986;12:414–86. N.U. Zitzmann, G. Krastl, H. Hecker, C. Walter & R. Weiger (2009) Endodontics or implants? A review of decisive criteria and guidelines for single tooth restorations and full arch
reconstructions. International Endodontic Journal, 42, 757–7747. Berglundh T, Lindhe J, Ericsson I, Marinello CP, Liljenberg B, Thomsen P (1991) The soft tissue barrier at implants and teeth. Clinical Oral Implants Research 2, 81–90.8. Tronstad L. Root resorption-etiology, terminology, and clinical manifestations. Endod Dent Traumatol. 1988;4:241–52.9. Grunder U, Gracis S, Capelli S (2005) Influence of the 3-D Bone-to-Implant Relationship on Esthetics. Int J Periodontics Restorative Dent ;25:113–119.10. Grunder U. Stability of the mucosal topography around single tooth implants and adjacent teeth: 1-year results. Int J Periodontics Restorative Dent 2000;20: 11–17.11. Salama H, Salama MA, Garber D, Adar P. The interproximal height of bone: A guidepost to predictable aesthetic strategies and soft tissue contours in anterior tooth
replacement. Pract Periodontics Aesthet Dent 1998;10:1131–1141.12. Korayem M, Flores-Mir C, Nassar U, Olfert K. (2008) Implant site development by orthodontic extrusion. A systematic review. Angle Orthod. 2008 Jul;78(4):752–6013. L Bergmans, J Van Cleynenbreugel, E Verbeken, M Wevers, B Van Meerbeek, P Lambrechts. Cervical external root resorption in vital teeth: X-ray microfocus-tomographical
and histopathological case study. J Clin Periodontal. 2002;29:580–58514. Wang RE, Lang NP. New insights into ridge preservation after tooth extraction Clin. Oral Implants Res. 23(Suppl. 6), 2012, 147–15615. Thalmair T, Fickl S, Schneider D, Hinze M, Wachtel H. (2013) Dimensional alterations of extraction sites after different alveolar ridge preservation techniques - a volumetric
study. J Clin Periodontol. 40(7):721–7.16. Villa R, Rangert B (2007) Immediate and early function of implants placed in extraction sockets of maxillary infected teeth: a pilot study J Prosthet Dent; 97(Suppl 6):S96–S108.17. Esposito M, Grusovin MG, Achille H, Coulthard P, Worthington HV (2009) Interventions for replacing missing teeth: different times for loading dental implants. Cochrane
Database Syst Rev. 2009 Jan 21;(1):CD003878.
Figure 18e. Figure 19. Figure 20.
Figure 21a. Figure 21b. Figure 21c.
Figure 21d. Figure 21e. Figure 21f.

Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 22
Highlights from the 2014 meeting in RomeOver 4,000 people attended the EAO’s 23rd annual scientifi c meeting in September
Over 4,000 delegates and industry representatives gathered at the Auditorium Parco Della Musica in Rome between 25 and 27 September for the EAO’s 23rd annual scientifi c meeting. As well as participating in cutting-edge scientifi c sessions, delegates enjoyed the warm weather and wonderful ambience at the magnifi cent auditorium, designed by architect Renzo Piano. Social events included a never-to-be-forgotten private tour of the Vatican Museums, including a fi ve course banquet in the Sala dei Busti.
Th e theme of the meeting, inspired by the Roman motto ‘Senatus Populusque Romanus’, was SPQR: ‘Simplifi cation, Predictability and Quality to achieve Results’. Th ree main sessions, held over the event’s three days, discussed this concept and how quality of life for patients can be improved using these principles. During these main sessions, eleven presenters spoke about how to improve the quality of dental implant treatment, discussing surgical alternatives, prosthetic alternatives and the health and social implications of implants for patients.
For the fi rst time, a guest country from outside Europe was invited to present its own session at the scientifi c meeting. A group of experts from South Korea fl ew to Rome to attend the event and discuss the advances being made in implant dentistry in Asia. Th ey presented their own set of well-attended speaker sessions.
As a leading scientifi c meeting, the presentation of new research is always central to the congress. Th is year, a record number of 752 research abstracts were submitted, of which 617 were selected and 54 were shortlisted for a series of prestigious competitions. Four delegates were awarded EAO European Prizes for Research in Implant Dentistry (opposite).
Th e EAO would like to thank everyone who attended and to warmly invite you to the 2015 meeting in Stockholm, which will be held between 23 and 26 September 2014.

23 | Volume 2, Issue 2: Winter 2014 | Inspyred: The alternative EAO voice
At the EAO’s General Assembly, held in Rome on 26 September, several new office-bearers were appointed to the Board of Directors. Professor Björn Klinge became the association’s new president, succeeding Professor Pascal Valentini, who was president from 2012–2014. Professor Alberto Sicilia was appointed as the new president elect, and Professor Henning Schliephake became the treasurer. Professor Luca Cordaro was elected to serve a second two-year term as secretary general.
New office-bearers appointed to EAO board
On 27 September, EAO President Professor Pascal Valentini announced the winners of the EAO's four prestigious European prizes for research in implant-based therapy. These were selected from among the 752 scientific abstracts submitted for meeting – a record-breaking number. These abstracts were reviewed by members of the 20-strong Abstract Subcommittee, who each have expertise in one of six key areas of implant therapy. Of the abstracts submitted for the research competition, the 14 with the highest mean scores for basic research, the 15 with the highest mean score for clinical research (prosthetic) and the 14 with the highest mean score for clinical research (surgical aspects) were selected
to participate in the research competition. 11 abstracts were shortlisted for inclusion in the poster presentation category. The four winners, pictured below, received a trophy and a €2,000 award.
A separate award, the EAO’s Certificate in Implant-based Therapy, was also given to three candidates at the meeting. These certificates represent the only Europe-wide standardised assessment of skills and expertise within the field of implant-based therapy. Each candidate had to submit six clinical cases, sit a multiple choice examination and be interviewed about their cases. Certificates were awarded to Kamil Khabiev, Algirdas Puisys and Gang Chen.
Winners of scientific prizes announced
European Prize for Clinical Research in Implant Dentistry: Prosthetic Aspects. Awarded to: Nicole Winitsky (Sweden). ‘Implant infra-position after 15-year follow-up of Brånemark implants in the anterior maxilla in young patients. A prospective cohort study.’
European Prize for Clinical Research in Implant Dentistry: Surgical Aspects. Awarded to: Yvonne De Waal (Netherlands) (accepted on her behalf by colleague Gerry Raghoebar.): ‘Factors associated with success or failure of surgical peri-implantitis treatment.’
European Prize for Basic Research in Implant Dentistry. Awarded to: Yuelian Liu (Netherlands) ‘Osteoinductive biomimetic calcium phosphate bone substitute for bone regeneration.’
European Prize for Research in Implant Dentistry: Poster Presentation. Awarded to: Georg D. Strbac (Austria). ‘Thermal effects of a combined irrigation method during implant site drilling. A standardized in vitro study using a bovine rib model.’
Professor Søren Schou (above) retired from the EAO board during the Rome meeting and was awarded with a medal for outstanding service (close-up below).

Inspyred: The alternative EAO voice | Volume 2, Issue 2: Winter 2014 | 24In
spyr
ed is
des
igne
d a
nd p
rod
uced
by
ww
w.p
ublis
hing
bur
eau.
co.u
k
Published by:European Association for Osseointegrationc/o Colloquium Group, Avenue E. Van Nieuwenhuyse, 6 B1160 Brussels
Tel: +33 (0)1 44 64 15 15Email: [email protected]
The views expressed in the articles published in this magazine are those of the author(s) and do not necessarily represent EAO’s position on these issues. EAO cannot be held liable for any statements expressed therein.
EA O Junior CommitteeReport on the Summer Camp and new committee appointments
The EAO summer camp is organised every two years by the Junior Committee with the support of the EAO board. Its aim is to develop innovative ideas about the future
development of implantology, and to establish an international network for exchanging ideas between participants and the societies they represent.
The third EAO summer camp was held in Barcelona, Spain, from 4 to 6 July 2014. A group of young dental professionals from different countries and with different backgrounds came together with the purpose of exploring the future of dentistry in Europe.
The associations represented were: Academy of Osseointegration (AO); European Federation of Periodontology (EFP); Deutsche Gesellschaft für Parodontologie (DGParo); Deutsche Gesellschaft für Implantologie (DGI); Societa Italiana di Parodontologia (SIdP); Sociedad Española de Prótesis Estomatológica (SEPES); Sociedad Española de Periodoncia y Osteointegración; European Academy of DentoMaxilloFacial Radiology (EADMFR); Sociedade Portuguesa de Periodontologia e Implantes (SPPI); Belgian Society of Periodontology (BSP); Ukrainian Society of Periodontists; Osteology Foundation; British Association of Oral Surgeons; Swiss Society of Periodontology; and the European Association for Osseointegration.
The topics discussed at the summer camp were:
what will be the role of societies and associations in 10 years?
what will certification processes and specialties look like in 10 years?
how will continuing education look in 10 years? what will be the innovations in the field of dentistry in 10 years?
To help answer these questions, three moderators used a variety of motivation and moderation techniques to facilitate the discussions. A World Café exercise was used to begin the brainstorming process among
participants. Different topics were discussed and a task-group was created to discuss each of the four questions.
Each group was given the task of developing ideas and expanding on their topic. There was a high level of motivation among participants, who used innovative techniques to generate and record ideas. The format of the camp, combined with the venue (which was far away from normal day-to-day distractions), contributed to very effective outcomes from the workshops and sessions, and encouraged friendships, communication and fun. Participants shared novel ideas and laughed and fought for their thoughts and beliefs. The scientific and competitive character stimulated each group to work as hard as they could over the three days of the camp. By the end, each one had prepared a draft of a future paper.
This was the third EAO summer camp organised by the Junior Committee and it was a success. The concept of bringing together young and motivated researchers created a unique and dynamic atmosphere within the very short period of intensive scientific exchange.
New committee members appointed
During the EAO meeting in Rome in September, two new members were elected to the Junior Committee: Stefan Fickl, from Germany, and Iva Milinkovic, from Serbia.
Above: participants at the 2014 summer camp.
Below: The EAO Junior Committee (left to right): Stefan Fickl; Helena Francisco; Jose Manuel Navarro (Chair); Nele Van Assche; Daniel Thoma; Katarzyna Gurzawska; Iva Milinkovic; and Ferruccio Torsello.
europeanassociationforosseointegration
eao_association
European Association for Osseointegration
Keep in touch with the EAO via social media!