Embed Size (px)
Citation preview

78 • Australasian Psychiatry • Vol 7, No 2 • April 1999
Dr Harvey WhitefordThe World BankHealth, Nutrition and Population
Human Development NetworkRoom G-30171818 H Street, N.W.Washington DC 20433 USA
This is the most common question Ihave been asked since the
announcement of my appointment tothe World Bank. This paper provides abrief history of the development of theBank, its role in social development,population health and health servicedelivery, and the reasons behind itsrecent interest in mental health.
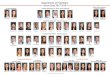
The World Bank actually consists of twoorganisations, the International Bank forReconstruction and Development (IBRD) and theInternational Development Association (IDA).Three additional agencies work very closely withthe IBRD and IDA. These are the InternationalFinance Corporation (IFC), the MultilateralInvestment Guarantee Agency (MIGA) and theInternational Centre for the Settlement ofInvestment Disputes (ICSID). These five agenciestogether form the World Bank Group (Fig. 1).
The IBRD was established in 1945. Therationale for its creation grew out of post WorldWar Two economic thinking and the attitude of theallies towards Germany. It was believed thateconomic problems following World War Onewere, in part, a contributing factor towardscreating the social, economic and politicalenvironments which led to World War Two [1]. The
WHY WOULD A PSYCHIATRIST WORKIN A BANK?
HARVEY WHITEFORD
allies, meeting after World War Two in BrettonWoods in New Hampshire USA, designed anumber of institutions with the aim of preventing arecurrence of these problems. They establishedthe IBRD to fund long term social developmentand the International Monetary Fund (IMF) topromote economic reform and provide funds torectify short term balance of payments deficits [2].These were followed a few years later by the ill-fated International Trade Organisation (ITO)which was replaced by the General Agreement onTariffs and Trade (GATT) and subsequently theWorld Trade Organisation (WTO). The aims of theWTO and its predecessors have been to promotefree trade and investment. Others, including theOrganisation for Economic Cooperation andDevelopment (OEDC) and the United NationsConference on Trade and Development(UNCTAD), later joined these institutions. Theseorganisations have become known as the BrettonWoods system which as a whole aims to fostertrade and economic benefits internationally and topromote the economic development of countrieswhich were not industrialised at the end of WorldWar Two.
The mandate of the World Bank is therefore topromote economic and social progress indeveloping countries with the aim of reducingpoverty, improving the quality of life for theworld’s poorest and increasing prosperity. TheIBRD and IDA make loans to governments forprojects and programs that promote economic andsocial development and help raise economicproductivity to enhance people’s quality of life.Since 1944 the Bank has lent $US426 billion for7500 projects in 163 countries. Along with theseloans the Bank provides policy and service adviceand technical assistance.
The governments of 180 member countriesnow own the IBRD. To join the IBRD, countriesmust first be a member of the IMF. Upon joiningthe IBRD, members subscribe to its capital stock.The number of shares each member is allocatedreflects its quota in the IMF which in turn reflectsthe country’s relative economic strength in theworld economy. Members pay in a small portion ofthe value of their shares, the reminder is ‘callablecapital’ and would only be paid should the IBRDbe unable to meet its financial obligations — asituation that has never arisen [3].
The IBRD lends funds to developing countriesfor social development and only for projects thatpromise high rates of economic return to the
Figure 1: Structure – World BankGroup
IBRD: International Bank for Reconstruction andDevelopment
• lends on commercial terms to governments• money raised on global markets
IDA: International Development Association• makes low cost finance available to the
poorest countries• contributions from member countries and
from IBRD
IFC: International Finance Corporation• supports private enterprise
MIGA: Multilateral Investment Guarantee Agency• promotes foreign investment through
guarantee
ICSID: International Centre for the Settlement ofInvestment Disputes
• arbitration for investment disputes

Australasian Psychiatry • Vol 7, No 2 • April 1999 • 79
country. The IBRD borrows most of the money it lends throughmedium and long term borrowing in the global capital markets.It also borrows funds at market-based rates from central banksand other government institutions [3].
The IDA was established in 1960 to provide assistance topoorer developing countries that cannot meet the IBRDrepayment terms. To qualify for IDA loans (referred to ascredits), the country would usually have an annual per capitaGross National Product of $785 or less (in 1996 US dollars). Bythis criterion, about 70 countries in the world are eligible. IDAcredits are made only to governments. The repayment period isusually thirty-five to forty years with a ten year grace period.The credits carry no interest. All members of the IBRD areeligible to join IDA and 159 countries had done so by 1997 [3].
The IDA and IBRD share the same staff and IDA projectshave to meet the same criteria as IBRD projects. Because theBank (essentially the member countries) guarantee IBRD andIDA loans, the interest rates able to be secured are favourablecompared with the interest developing countries would expect topay on loans raised independently.
The three other agencies of the World Bank Groupcomplement this work. The International Finance Corporation(IFC) works closely with private investors and invests incommercial enterprises in developing countries. TheMultilateral Investment Guarantee Agency (MIGA) encouragesdirect foreign investment in developing countries by offeringinsurance against non-commercial risk. The InternationalCentre for the Settlement of Investment Disputes (ICSID)provides facilities for settling disputes between foreign investorsand their host countries.
The World Bank, with headquarters in Washington DC andapproximately 90 offices around the world, employs about fiveand a half thousand staff. The Bank was restructured in 1997and now has four networks:1. Human Development2. Environmentally and Socially Sustainable Development3. Finance, Private Sector and Infrastructure4. Poverty Reduction and Economic Management
The Human Development Network was the first network inthe Bank’s revised structure. It brought together staff working onhealth, nutrition, population, education, training and socialprotection. The Network promotes policies and funds programswhich support economic growth and poverty alleviation throughimproving the health and educational status of individuals andthe provision of social safety nets. The Network is organised intothree sectors:1. Health, nutrition and population (HNP).2. Education3. Social protection
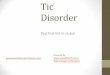
The World Bank is the single largest source of externalfinance for HNP in developing countries. The mountingevidence that investments in health, nutrition and educationcontribute to individual productivity, and therefore to nationaleconomic growth, has influenced the Bank (Fig. 2), and HNP isnow one of the fastest growing areas of Bank lending. The HNPsector has about 250 staff. The investments aim for allocativeefficiency in lending (buying cheap health gains first), betterhealth policy and research. Funding for health sector reformaddresses health financing and management, healthinformation, and enhancing quality, efficiency and equity inservice delivery. These initiatives must be developed andimplemented in a way that is sensitive to the macro and microeconomic policies of the country [4].
Currently the Bank lends over $US25 billion per year, ofwhich some 10% is invested in health, population and nutrition,up from 6% in 1992–94. In 1995–96, $US1 billion was lent forHNP initiatives. In 1996–97, this had increased to $US2 billionand in 1997–98, $2.5 billion was lent for 260 projects in 93countries. The largest recipient countries of HNP funds between
1988 and 1998 have been India, Mexico, Brazil, Argentina,China, Bangladesh, Indonesia, Russia, Venezuela, and Nigeria.
Traditionally HNP lending has been for areas such asinfectious disease control and reproductive health. Seventy-seven per cent of the Bank’s HNP loans are in the area ofprimary health care. The publication of the World Bank’s WorldDevelopment Report in 1993: Investing in Health [5], focussedattention on the burden of disease able to be identified using astandardised comparison of both mortality and morbidity, thedisability adjusted life year (DALY). Subsequent reports,especially the 1996 Global Burden of Disease report [6], haveemphasised the significant burden associated with what thereport refers to as neuropsychiatric disorders (epilepsy,substance abuse and mental disorders). Five of the ten leadingcauses of disability worldwide are mental illnesses, accountingfor a quarter of total disability and 10% of total burden. Theburden is estimated to rise to 15% by the year 2020 and the risewill be particularly sharp in developing countries.
The significance of this burden and how to address it hasbeen debated by the international mental health community andis now being discussed in the international economiccommunity [7]. Individuals from the World Health Organisation(WHO) and the World Federation for Mental Health (WFMH)[8] held discussions with officials from the World Bank during1997 and 1998 to consider how the Bank might respond to thisincreasing problem. A decision was made to establish a newposition at World Bank headquarters in Washington DC. Keyplayers from the international mental health communityinvolved in this development were Dr Rachel Jenkins, Directorof the WHO Collaborating Centre at the Institute of Psychiatry,London; Professor Marten deVries, Professor of Psychiatry,Maastricht University, The Netherlands and President of theWorld Federation for Mental Health; Dr John Gates, MentalHealth Director at the Carter Center, Atlanta, USA; ProfessorArthur Kleinman, School of Public Health, Harvard University,USA; and Professor Eugene Brody, Sheppard and Enoch PrattHospital, Baltimore, USA. Strong support was received fromWorld Bank officials.
The duties and responsibilities of the position have beenidentified by the Bank as:1. the provision of policy and technical advice on population
mental health, mental health services and clinicalinterventions within the World Bank and to the Bank’s clientcountries;
2. to prepare lending components of IBRD, IDA projectsrelated to mental health;
3. to create a capacity within the Bank to help ensure projectsfunded in the mental health area are cost effective in thecountry in which they will be implemented and will also beresponsive to the demography and culture of the country;
Figure 2: Investing in health, nutrition andpopulation (HNP)
Why the Bank works with governments to invest in HNP
1. In all countries a large share of GDP is devoted to health2. Key role for the state in the health sector3. The human capital equation
HealthyPeople
EducatedPeople
A necessary basis for enhanced welfare, reducedpoverty, and sustainable growth.
+
=

80 • Australasian Psychiatry • Vol 7, No 2 • April 1999
4. to develop and implement a training program on mentalhealth for staff in the HNP Sector of the Bank and
5. to identify an international network of experts to assist theBank in the area of mental health.To meet these responsibilities access to a wide range of
mental health policy, program, service delivery and clinicalexpertise will be needed. Support has been secured from keyagencies such as the WHO, WFMH and the US Government’sCentre for Mental Health Services. The World PsychiatricAssociation, US National Institute of Mental Health and theAmerican Psychiatric Association have also offered assistance.Access to additional expertise is being sought from identifiedacademic departments of psychiatry and public health andindividuals around the world. It is critically important that thework undertaken is sensitive to the demographic, cultural,economic and political environments of the Bank’s clientcountries [9]. Foreign aid can bring problems as well assolutions [10,11]. Governments and individuals in the Bank’sclient countries must be committed and be able to implementthe projects and programs that are funded. Support for theBank’s work is essential from key individuals, professional andnon-government organisations and government officials indeveloping countries. A number have already offered support.
My appointment is, I believe, an acknowledgment by theinternational mental health community and the World Bank ofthe work undertaken by psychiatrists, other mental healthprofessionals, policy makers, administrators, consumers, carersand governments to improve mental health services in Australia.
We still have a long way to go but, by international standards,our achievements over the last decade have been impressive.The political, economic and social situations as well as thehealth status and health services in many of the Bank’s clientcountries are very different to Australia. Nevertheless, thelessons we have learned in developing and implementing mentalhealth reform can, I believe, be adapted and applied to thebenefit of those countries.
References1. Jackson JH. The world training system, 2nd edn. Cambridge, MA: TheMIT Press, 1997.2. Walt G. Health policy. London: Zed Books, 1994.3. The World Bank Annual Report. Washington DC: World Bank,1997.4. Maddock R. Economic policy in the 1990s. In Hede A, Prasser S (eds).Policy making in volatile times. Hale and Iremonger, 1993.5. World Bank. World Development Report: Investing in health.Washington DC: World Bank, 1993.6. Murray CJL, Lopez AD. The global burden of disease. World HealthOrganisation, Harvard University Press, 1996.7. The Economist. Vol 349, 19 December, 1998, 113–121.8. Brody EB. The search for mental health: A history and memoir of theWorld Federation for Mental Health (WFMH) 1948–1997. WorldFederation for Mental Health, 1998.9. Harpham T, Blue I (eds). Urbanisation and mental health in developingcountries. Vermont: Ashgate Publishing, 1995.10. Lawyers Committee for Human Rights. The World Bank: Governanceand human rights. Washington DC: Lawyers Committee for Human Rights,1995.11. Landers DS. The wealth and poverty of nations. Little Brown andCompany, 1998.