Embed Size (px)
Citation preview


Why Pathways? Why Now?
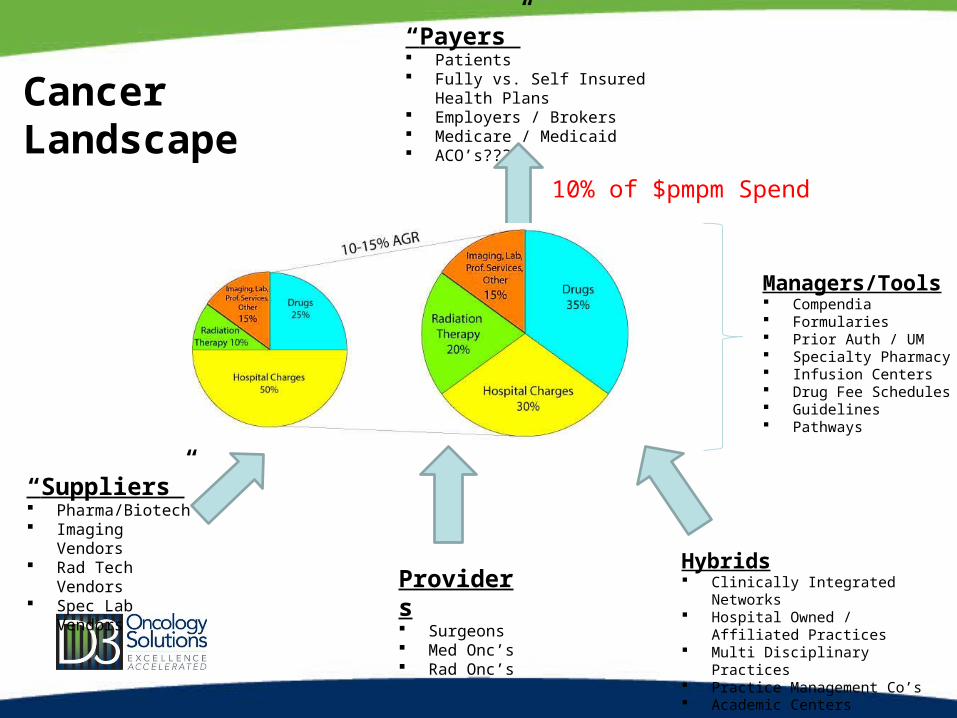
“Payers” Patients Fully vs. Self Insured Health Plans Employers / Brokers Medicare / Medicaid ACO’s???
Providers Surgeons Med Onc’s Rad Onc’s
“Suppliers” Pharma/Biotech Imaging Vendors Rad Tech Vendors Spec Lab Vendors
Managers/Tools Compendia Formularies Prior Auth / UM Specialty Pharmacy Infusion Centers Drug Fee Schedules Guidelines Pathways
Hybrids Clinically Integrated Networks Hospital Owned / Affiliated
Practices Multi Disciplinary Practices Practice Management Co’s Academic Centers
CancerLandscape
10% of $pmpm Spend

Why Pathways? Why Now?
Pathways are a proven model for tangibly demonstrating VALUE (Q/C)to your key stakeholders (patients, referring MD’s, hospitals, payers)
in the new healthcare milieu
And retaining control over decision making for your patients…

Agenda• Brief history of “Why Pathways at UPMC”• What do we mean by Via Oncology Pathways?
– How are Pathways developed & maintained?– What diseases / modalities / phases of care are addressed?– How are the Pathways “delivered” and measured?– What are the implementation options?– What is the road map for Pathways for 2012?– Who is using the Via Oncology Pathways today vs. tomorrow?
• Can we prove success?• How can the value of Pathways be monetized?• Demonstration of the Pathways Portal


2004 - 2009
2009 - 2011
January 2011
Providers

UPMC• UPMC is a large not-for-profit health system providing both leading health
services and insurance in Western Pennsylvania and the surrounding area.
• UPMC is the region’s largest employer, with 50,000 employees (including 2,800 physicians), 20 tertiary, specialty, and community hospitals, 400 outpatient sites and doctors’ offices, and retirement and long-term care facilities as well as international ventures
UPMC Stats
• Revenue: 7 Billion
• Assets: 6-7 Billion

UPMC Cancer Centers
• UPMC Cancer Centers is an distinct product line of the UPMC system
• Organized via a “regional hub and satellite” structure• Inpatient and specialized treatment provided at
central “hub” while outpatient care is offered at over 40 regional sites
• Academic and Community Based physicians treating 30,000 new patients per year

Needs at UPMC• 2000 - 2004
– Rapid expansion of the “UPMC Cancer Centers” brand to 25 sites of Medical Oncology service with a 250 mile geographic spread
– Concerns over Quality and Consistency of Care– Internal study revealed significant variability, though mostly within Guidelines– Some care outside of Guidelines
– Payers demanding solutions to the rising cancer costs• Take charge or lose control…

Our Solution: Via Oncology Pathways• Continually updated, evidence-based treatment algorithms
for most cancer presentations and unique patient co-morbidities,
• Developed and maintained by the oncologists themselves,
• Delivered in a point of care, patient specific, interactive decision support tool,
• Resulting in measurable proof of performance and likely savings in healthcare resources

Via Oncology Pathways vs. Guidelines
Via Oncology PathwaysG
uide
lines
Via OncologyPathways
Gui
delin
es
Cancer Incidences Covered
Variability Allowed

How are Via Oncology Pathways developed and maintained?
• Physician Disease Specific Committees (18 unique committees)– Two co-chairs for each committee (academic & community based)– Committee participation open to all Via Oncology Pathways physicians
• Committee Process:– Conflict of Interest Disclosure– Review prior period metrics by patient presentation– Where physicians are going Off Pathway >30%, review reasons cited and what regimen
was used instead• Consider adding additional “sub-presentations” to achieve goal of 80% coverage
– Review new evidence and debate until consensus is established for a single-best

What is “single best”? • Disease Committees define a single best treatment for each state and
stage of disease based upon:
First Decision Tier:
Efficacy
- If there is a clear choice, this is the pathway
Second Decision Tier:
Toxicity
- If efficacy is comparable…pick the treatment with less toxicities to improve QOL
and reduce hospitalizations/ED visits
Third Decision Tier:
Cost
- Only if efficacy and toxicities are comparable…
pick the lowest cost treatment

“On Pathway” Rate Goal:
70-90%

How often is Pathway maintenance performed?
• Quarterly meetings to review new data and change Pathway if needed
• Software is updated (after MD review) for ALL customers within 2-4 weeks of approved Pathway change by committee
• For “game changing” new data, call Ad Hoc committee meeting

Lymphomas
MDS
Prostate
Lung
Breast
Colon/Rectal
Melanoma
Renal
Head & Neck
Esophageal
Myeloma
Ovarian
Pancreatic GastricBladder
95% of all new cancer cases
Uterine CML
Medical Oncology Disease Coverage

Modality CoverageMedical Oncology Treatment
Infused Chemo & Biologics (Avastin, Erbitux, etc)
Orals (Xeloda, Tykerb, etc.)
Supportive Care
Antiemetics (5HT3’s, Aloxi, Emend)
WBC Growth Factors
Prognostic Testing(Personalized Medicine)
Her2KRAS
OncotypeDXEGFR
Advance Care PlanningPrompts physician to consider
hospice/palliative care for METS
Document Treatment Intent and how it was discussed with patient
Prompt Physician to consider hospice upon each disease progression
Radiation Oncology TreatmentConventional 3D
IMRTSRS
Brachytherapy
11/10/2010 – Peter G. Ellis, M.D.
How do we make it easy for the physician to use the
pathways?
And prove their results???

The Pathways PortalNovel Software Application
– Point of Care Decision Support Tool• Physicians utilize when selecting
treatment– Patient Specific / Personalized
• Interfaced with practice’s demographics and scheduling applications
– Easily Implemented• Web-Based Application (centrally or
locally hosted)– Stand Alone or Integrated with EMR
• Avoids duplicate entry of treatment orders by physicians

The Pathways PortalFocused on Physician Efficiency
– Highly intuitive and user friendly • Minimal training required• Presents the “right patient at the right
time”
– Provides additional tools to Physician• Chemo Order Sets (for non EMR sites)• Clinical references and full text articles• Patient Education Materials• Dose Modification Guidelines• Staging references
– Email alerts to physicians each day regarding prior Missed Patients

Supporting Clinical Research– Practice specific trials imbedded in
Pathways Portal
– Trials are always 1st option in Pathways
– Trials are always counted as “On Pathway”
– If patient NOT accrued, require “Reasons for Not Accruing” are captured and reported back to PI’s

Implementation Options
Pathways Treatment
Regimens: Via Oncology
Standard or Practice Customized
Physician Decision Support
Tool OR
Staff Data Entry Tool
Diseases: Some or All
Patients: All or Payer
Specific
Clinical Trials: All, Some, or
none
Peer Review: On or Off
Standalone Application
OR Interfaced to
EMR

Why can’t you get Pathways in an EHR*?
Medications / Allergies Lists
Scheduling
Lab Results
Progress Notes
Ord
ers
Chemo
Mgmt
Mis
sing
Link?
Decis
ion
Support!
EHR Functions
* - with the possible exception of iKnowMed

2012: Laying down additional lanes!!!
• Deeper integration with Aria EMR– Inbound clinical data such as Stage, Her2, etc.– Outbound orders
• Expand pathways for:– G-CSF’s– Prognostic Testing – what should/should NOT be ordered– Surveillance / Survivorship Pathways
• Phase II of Advance Care Planning• “Virtual Tumor Board” within Portal

Market Expansion

RESULTS:Adherence
&Cost Savings
Pathways Metrics
9 months ended Sept 30, 2011:• 94% Patient Capture Rate (denominator is all patient visits – 280,000
visits per year)
• 77% “On Pathway” Rate (denominator is all new treatment decisions – 17,000 annual new treatment decisions)– Goal is never 100%...intended to meet the majority of clinical situations
but never all… 80-90% is general goal.
• 100% capture of Reasons for Going “Off Pathway”• Most common (30%) is Exceeded Line of Therapy

Types of Cost Savings Studies
Practice Based Services
The 80% of Patients “On” Pathway
Practice Based Services
The 20% of Patients“Off” Pathways
vs.
US OncologyStudy with Aetna
35% difference in outpatient costs
Journal of Oncology PracticeJanuary 2010
NSCLC Only
Total Cost of Care
Patients seen atPathways Practice
Total Cost of Care
Patients seen atNON-Pathways
Practice
vs.Breast
&NSCLC
Via Oncology Studieswith Highmark BCBS

Highmark Study DesignTwo Separate Studies:
• Breast and NSCLC • Population Studied
• Patients in active therapy (excluded patients in remission)• Both commercial and Medicare Advantage with full coverage (e.g., Rx Benefit
with Highmark)
• Analysis completed by Highmark using Highmark claims data• Measured Total Cost of Care, not just drugs
• Two arms• Control = non-UPMC patients (40%)• Experimental = UPMC patients (60%)
• Two periods measured• 12 months before Pathway implementation• 12 months after Pathway implementation (measured months 6-18 to give a 6 mo
gap for ramp up)

Highmark Cost Savings – Total Cost of Care
• Highmark/UPMC - Breast Study Results (see details in Appendix)– 9% absolute Growth Rate differential
• 16% growth in Non–Pathways Practices
• 7% growth in the Experimental Arm – Pathways Practices
• Highmark/UPMC - NSCLC Study Results (see details in Appendix)– 5% absolute Growth Rate differential
• 6% growth in Non–Pathways Practices
• 1% growth in the Experimental Arm – Pathways Practices

IntrinsiQ Study of NSCLC Drug Costs
• Large oncology EMR and data analytics company• Database of EMR prescribing data for 700 nationally distributed oncologists at very granular
level– Regimen– Disease and Stage– Line of Therapy– Performance Status– Clinical Markers (Her2, etc.)
• Compared for Non Small Cell Lung Cancer:• Real world treatment patterns versus• UPMC / Via Oncology Pathways
• Results:
– 10% savings on Drug Costs if adhered to national Guidelines
– 40% savings on Drug Costs if adhered to Via Pathways• Assuming an On Pathway Rate of 80%, the savings would likely be 32%
Cost Savings Study – Drugs Only

Up Next – Look for results from Horizon Study• Two community based practices in New Jersey
• Similar study design to Highmark except no radiation costs
• Results compiled this month by 3rd party hired by Horizon
• Shows costs grew in Non-Pathways practices compared to substantial reductions in Pathways practices
• Working towards publication in early 2012

How do you monetize the VALUE of Pathways?

Internal Practice Value of Pathways• Lower bad debt risk
• Staying “on” Pathway reduces risk of Payer denials
• Practice efficiencies through uniformity of care and less variability• Staffing productivity• Lower inventory holding costs
• Potential for reducing medical errors
• Engage patients in shared decision making
• Stressing accrual to Clinical Trials

Contracting Opportunities with Payers
• Gain Share on Savings• $1,000 savings to payer is $15 from
practice, $485 from Pharma and $500 from hospital
• Increase existing fee schedule• RVU based services• Drugs (advise against…)
• Extend current reimbursement rates• Decrease Administrative Burden
• Eliminate pre-certs / prior auth / Box 19 data
• Prevent Payer from pulling drugs out of practice• Specialty Pharmacy• Infusion Centers
• Reverse rate decreases
• Payer Steerage to Practice• Network Status
• Benefit design to allow for lower copay/coinsurance
• Accept case/bundled rates

Why Gain Share is difficult…• Difficult to measure – requires Payer to roll up costs from
variety of systems • Results without statistical validity can give false negatives • Long timeline for pilot followed by claims runout…then
measurement• Tends to be a “one year” phenomenon…hard to repeat
savings!• Payer Unique Issues
– Cancer is not their top priority…not even top 3• Most don’t have the information to measure their total $pmpm for cancer
– Pathways are the proverbial “elephant in the room” – who at the Health Plan has jurisdiction???
– Some believe that oncologists are already paid too much…– They are not used to outsourcing “UM” to the providers
themselves

Opportunities with Other Healthcare Entities• Patient Centered Medical Homes (PCMH)
– Participate directly or become a preferred practice for referrals
• Design Hospital <=> Private Practice affiliation (co-management) incentive structures through enhanced data capture and monitoring; benchmark performance
• Form a clinically integrated network (CI) with other oncologists and negotiate single payer contracts
• Accountable Care Organization (ACO) – Participate directly or become a preferred practice for referrals

Why Pathways? Why Now?
Pathways are a proven model for tangibly demonstrating VALUE (Q/C)to your key stakeholders (patients, referring MD’s, hospitals, payers)
in the new healthcare milieu
And retaining control over decision making for your patients…

Questions?
Discussion…





























