Embed Size (px)
Citation preview
Why does winter in A&E get worse every year?
Why does winter in A&E get worse every year?
The Royal College of Emergency Medicine has been campaigning since June 2013 to improve emergency care in the A&E departments of the UK.Key to this has been our STEP campaign – highlighting the need for sustainable staffing, tariff reform and terms that support a work-life balance, the eradication of exit block and primary care co-location.
This infographic has become a familiar feature of the College’s submissions and presentations.
The rationale for the campaign is predicated on three key determinants of system performance – patient demand, hospital capacity and the rate at which patients progress through A&E. So we focus on demand, capacity and flow.
This paper gives an overview of some of the key data behind the College’s arguments as seen through the lens of winter.
£
RCEM’s steps to rebuilding emergency medicine

Demand
The Urgent and Emergency care review has been progressing since 2013. Much of its attention has been directed at reducing patient demand on A&E departments. This is commendable, though the College is of the opinion that the gains realisable from such a strategy are limited. In this context it is worth noting that the UK has a relatively low usage of A&E departments when measured as visits per annum per capita.
Patient attendances have certainly risen in the last 5 years - by 611,250 per annum, but importantly admissions have disproportionately risen by 443,059.
75
PERCENT
Sourec: 2013 Commonwealth Fund International Health Policy Survey in Eleven Countries.
22
AUS GER NETH UK NZ NOR SWIZ FR SWE US CAN USUNINSURED
PERCENTAGE OF POPULATION THAT USED EMERGENCY DEPARTMENTS IN THE PAST TWO YEARS
22 2427 28 28 28
31 32
39 41
4850
25
0
1,400,000
1,300,000
1,200,000
1,100,000
1,000,000
900,000
800,000
700,000
600,000
500,000
AU
G 1
0
DEC
10
APR
11
AU
G 1
1
DEC
11
APR
12
AU
G 1
2
DEC
12
APR
13
AU
G 1
3
DEC
13
APR
14
AU
G 1
4
DEC
14
APR
15
AU
G 1
5
DEC
15
TYPE1* A&E ATTENDANCES BY MONTH
*Type 1 departments are typical A&E departments, Type 2 are specialist departments such as Eye Casualty and Type 3 represent a range of urgent care centres, walk in centres, minor injury units and alike.
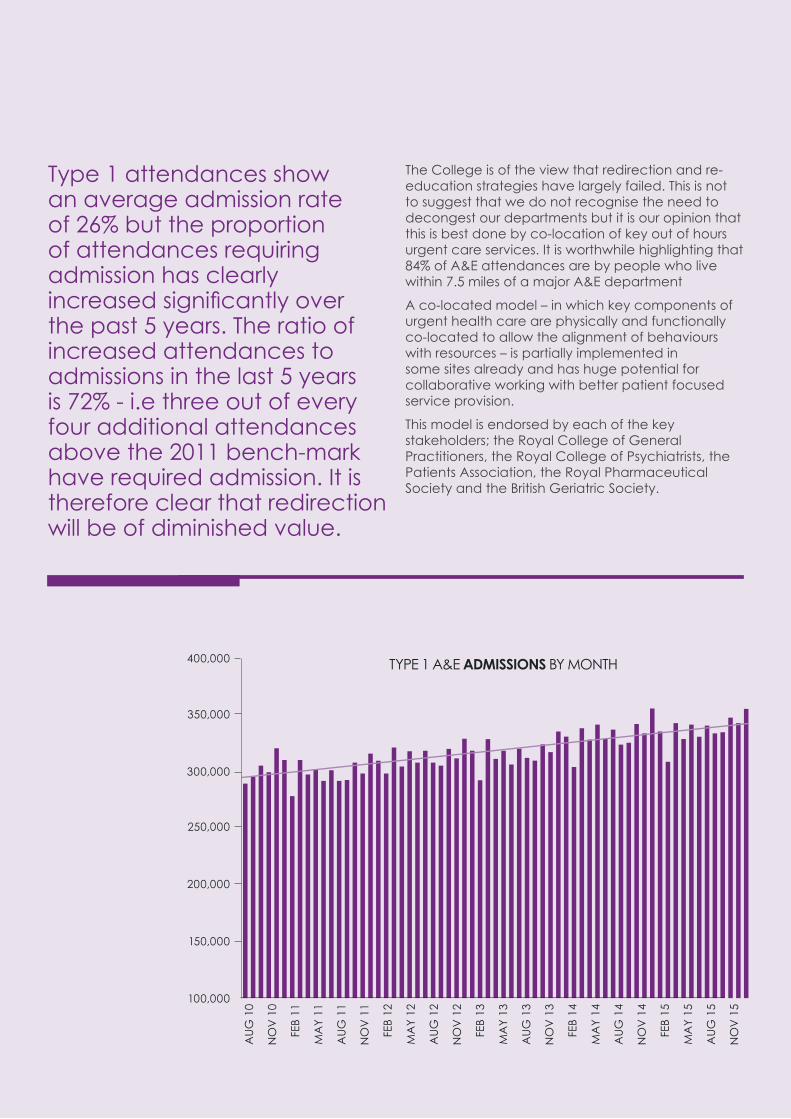
Type 1 attendances show an average admission rate of 26% but the proportion of attendances requiring admission has clearly increased significantly over the past 5 years. The ratio of increased attendances to admissions in the last 5 years is 72% - i.e three out of every four additional attendances above the 2011 bench-mark have required admission. It is therefore clear that redirection will be of diminished value.
The College is of the view that redirection and re-education strategies have largely failed. This is not to suggest that we do not recognise the need to decongest our departments but it is our opinion that this is best done by co-location of key out of hours urgent care services. It is worthwhile highlighting that 84% of A&E attendances are by people who live within 7.5 miles of a major A&E department
A co-located model – in which key components of urgent health care are physically and functionally co-located to allow the alignment of behaviours with resources – is partially implemented in some sites already and has huge potential for collaborative working with better patient focused service provision.
This model is endorsed by each of the key stakeholders; the Royal College of General Practitioners, the Royal College of Psychiatrists, the Patients Association, the Royal Pharmaceutical Society and the British Geriatric Society.
400,000
350,000
300,000
250,000
200,000
150,000
100,000
AU
G 1
0
AU
G 1
4
AU
G 1
2
NO
V 1
0
NO
V 1
4
NO
V 1
2
FEB
11
FEB
15
FEB
13
MA
Y 11
MA
Y 15
MA
Y 13
AU
G 1
1
AU
G 1
5
AU
G 1
3
NO
V 1
1
NO
V 1
5
NO
V 1
3
FEB
12
FEB
14
MA
Y 12
MA
Y 14
TYPE 1 A&E ADMISSIONS BY MONTH
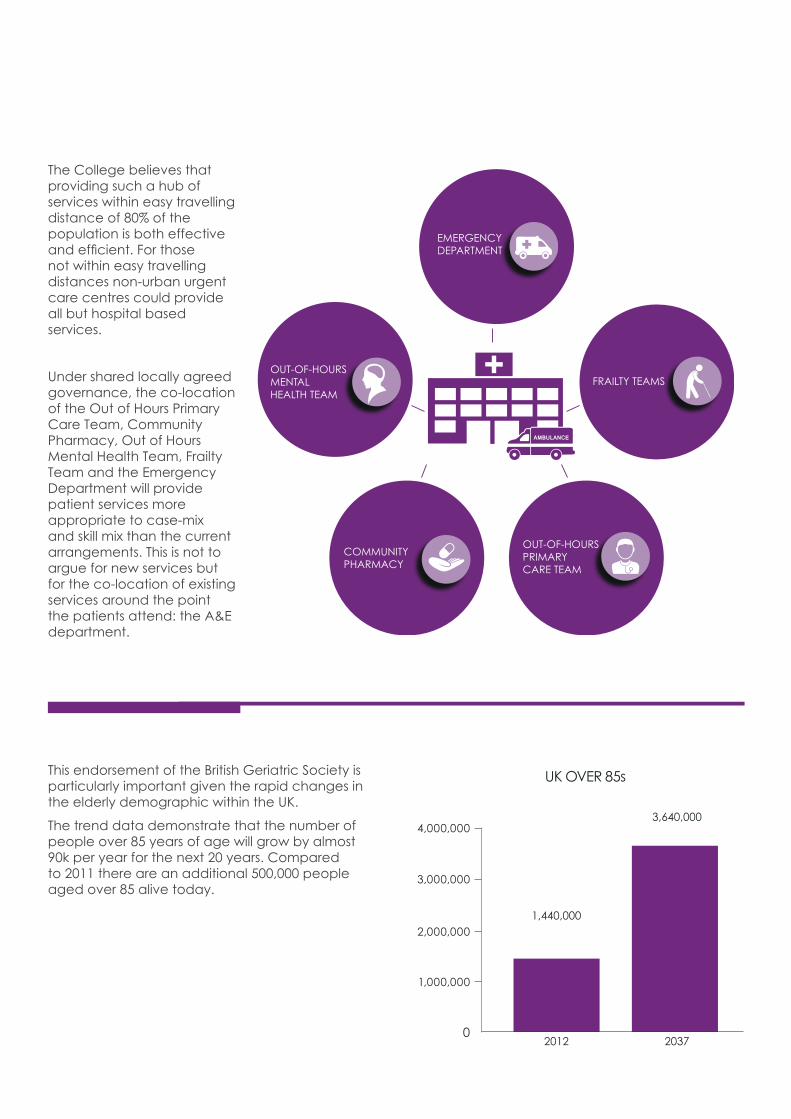
The College believes that providing such a hub of services within easy travelling distance of 80% of the population is both effective and efficient. For those not within easy travelling distances non-urban urgent care centres could provide all but hospital based services.
Under shared locally agreed governance, the co-location of the Out of Hours Primary Care Team, Community Pharmacy, Out of Hours Mental Health Team, Frailty Team and the Emergency Department will provide patient services more appropriate to case-mix and skill mix than the current arrangements. This is not to argue for new services but for the co-location of existing services around the point the patients attend: the A&E department.
OUT-OF-HOURSPRIMARY CARE TEAM
COMMUNITY PHARMACY
EMERGENCY DEPARTMENT
OUT-OF-HOURS MENTAL HEALTH TEAM
FRAILTY TEAMS
The A&E Hub Concept
Supported by:
£
For more information see: http://bit.ly/1nT1pbE
This endorsement of the British Geriatric Society is particularly important given the rapid changes in the elderly demographic within the UK.
The trend data demonstrate that the number of people over 85 years of age will grow by almost 90k per year for the next 20 years. Compared to 2011 there are an additional 500,000 people aged over 85 alive today.
2012
1,440,000
2037
3,640,000
1,000,000
2,000,000
3,000,000
4,000,000
0
UK OVER 85s
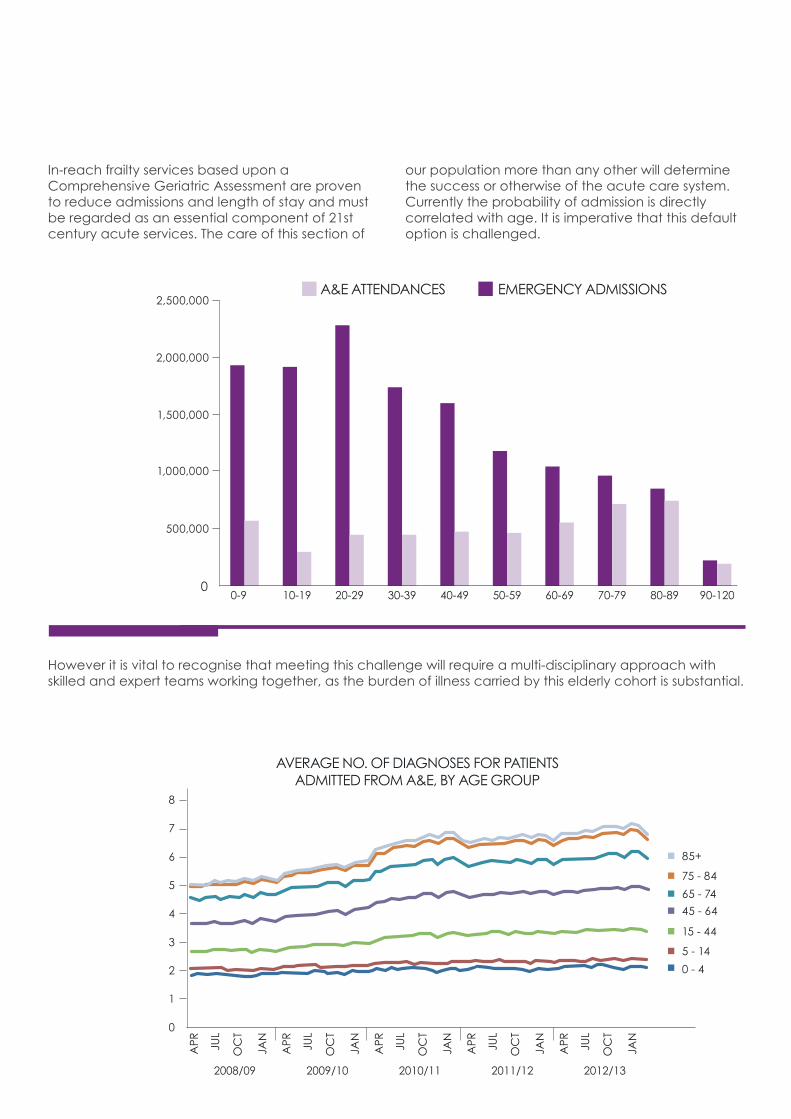
In-reach frailty services based upon a Comprehensive Geriatric Assessment are proven to reduce admissions and length of stay and must be regarded as an essential component of 21st century acute services. The care of this section of
our population more than any other will determine the success or otherwise of the acute care system. Currently the probability of admission is directly correlated with age. It is imperative that this default option is challenged.
However it is vital to recognise that meeting this challenge will require a multi-disciplinary approach with skilled and expert teams working together, as the burden of illness carried by this elderly cohort is substantial.
0-9 10-19 20-29 30-39 40-49 50-59 60-69 70-79 80-89 90-1200
2,500,000
2,000,000
1,500,000
1,000,000
500,000
A&E ATTENDANCES EMERGENCY ADMISSIONS
AVERAGE NO. OF DIAGNOSES FOR PATIENTS ADMITTED FROM A&E, BY AGE GROUP
8
7
6
5
4
3
2
1
0
85+
75 - 84
65 - 74
45 - 64
15 - 44
5 - 14
0 - 4
2008/09
APR JU
L
OC
T
JAN
2009/10
APR JU
L
OC
T
JAN
2010/11
APR JU
L
OC
T
JAN
2011/12
APR JU
L
OC
T
JAN
2012/13
APR JU
L
OC
T
JAN

Non EM attenders
The College recognises that a significant proportion of patients attending an A&E department can be managed at least as well if not better by other services/ staff. Data from the Royal College of Emergency Medicine Sentinel Sites study published in 2014 shows that more than a third of attendances could be managed without input from an EM doctor.
Moreover A&E has become ‘Anything and Everything’ in the out of hours period, a function it is not resourced to deliver. The lack of other services for urgent care needs leads to clinically improbable spikes in attendances at weekends and bank holidays. The following graphic highlights this phenomenon and the consequent increase in A&E dispositions by NHS 111 to A&E at weekends.
Establishing an A&E hub model of service provision would ensure that many of the additional weekend attenders were seen by more appropriate services further decongesting the emergency department.
ALL HOSPITALS
3,053TOTAL
% OF ATTENDEES
UNDER 16
691
16 TO 65
1,744
65 AND OVER
618
COULD BE SEEN BY GP IN 24 HOURS
GP IN ED
EM DOCTOR IN ED
EM DOCTOR AND ADMITTED
A&E ATTENDEES WHO COULD BE TREATED BY A GP OR EM DOCTOR
1,000 30
-NO
V
07-DEC
14-D
EC
21-DEC
28-D
EC
04-JA
N
11-JAN
18-JA
N
25-JA
N
01-FEB
08
-FEB
15-FEB
1,500
2,000
2,500
3,000
3,500
4,000
4,500
NHS 111 ALL ENGLAND A&E REFERRALS 30TH NOV TO 21ST FEB 2016

Capacity
The increase in attendances in the last 5 years is equivalent to the workload of 10 medium sized departments in England alone. Unfortunately the mismatch between patient volumes/casemix and senior medical staff has been exacerbated by the problem of retaining emergency medicine registrars and, to a lesser extent, consultants.
450 registrars were lost to the system as they chose other specialties or emigrated. Although recruitment and retention in 2015 reached a five year high the permanent loss of these senior trainees will be felt for many years.
Workload has therefore increased by a volume equivalent to 10 A&E departments yet the senior workforce has seen an attrition rate equivalent to 15 A&E departments. The cumulative shortfall is the resource equivalent of 25 A&E departments.
These staff shortages are accentuated by the variability in patient attendances per hour. Surges in demand can occur rapidly throughout the day or week and effectively exacerbate acute staff shortages. Such surges lead to queue formation and diminished efficiencies. As such even if departments are staffed for average attendance numbers it is frequently the case that they are substantially understaffed for much of the time.
450 REGISTRARS
WORKING LIFE OF 35 YEARS
2000 PATIENTS EACH PER YEAR
15 District General
Hospitals EDS
900,000 PATIENTS PER
YEAR
31 MILLION PATIENTS
SUNDAY
150
100
50
0
MONDAY
VARIABILITY IN NUMBER OF ATTENDEES AT A SINGLE A&E UNIT BY TIME OF THE WEEK OVER THE COURSE OF ONE YEAR
TUESDAY WEDNESDAY
TIME AND DAY OF THE WEEK
THURSDAY FRIDAY SATURDAY
06:0
0
12:0
0
18:0
0
06:0
0
12:0
0
18:0
0
06:0
0
12:0
0
18:0
0
06:0
0
12:0
0
18:0
0
06:0
0
12:0
0
18:0
0
06:0
0
12:0
0
18:0
0
06:0
0
12:0
0
18:0
0
NU
MBE
R O
F PA
TIEN
TS IN
A&
E D
EPA
RTM
ENT MIN/MAX +_ 1 STANDARD DEVIATION AVERAGE
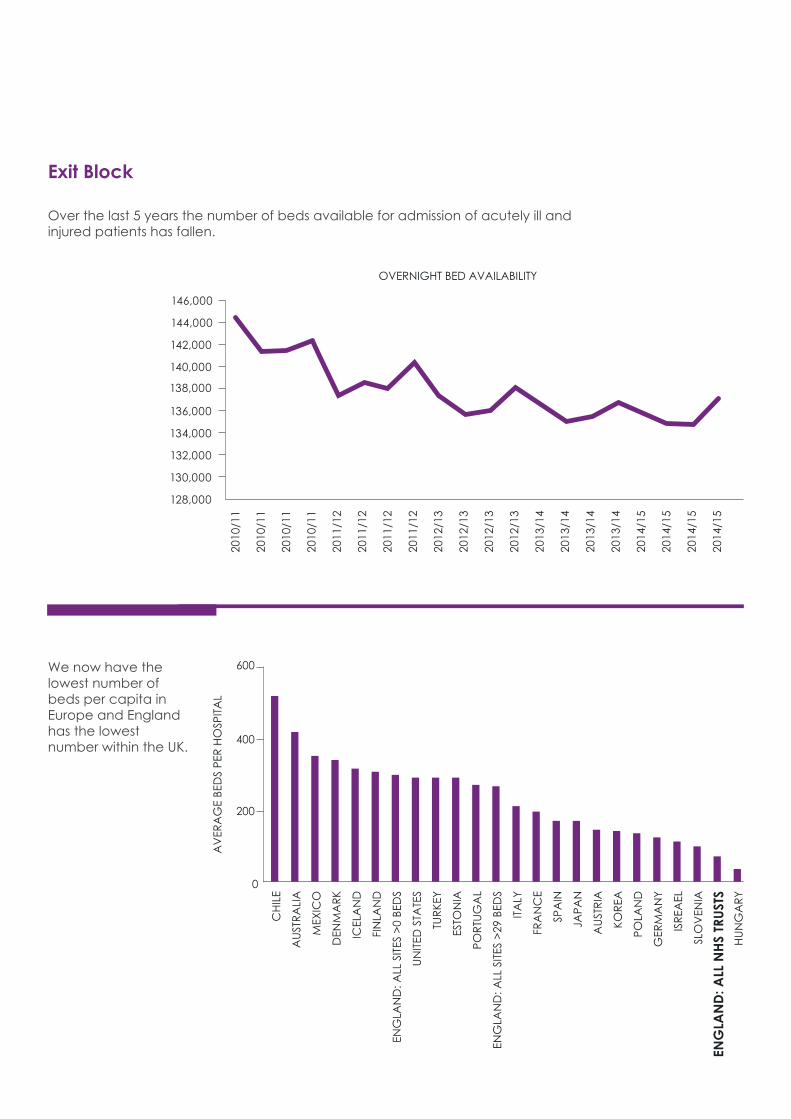
Exit Block
Over the last 5 years the number of beds available for admission of acutely ill and injured patients has fallen.
We now have the lowest number of beds per capita in Europe and England has the lowest number within the UK.
OVERNIGHT BED AVAILABILITY
2010
/11
2010
/11
2010
/11
2010
/11
2011
/12
2011
/12
2011
/12
2011
/12
2012
/13
2012
/13
2012
/13
2012
/13
2013
/14
2013
/14
2013
/14
2013
/14
2014
/15
2014
/15
2014
/15
2014
/15
128,000
130,000
132,000
134,000
136,000
138,000
140,000
142,000
144,000
146,000
CH
ILE
0
200
400
600
AU
STR
ALI
A
AU
STR
IA
KOR
EA
POLA
ND
GER
MA
NY
ISR
EAEL
SLO
VEN
IA
MEX
ICO
DEN
MA
RK
ICEL
AN
D
FIN
LAN
D
ENG
LAN
D: A
LL S
ITES
>0
BED
S
ENG
LAN
D: A
LL S
ITES
>29
BED
S
ENG
LAN
D: A
LL N
HS
TRU
STS
HU
NG
AR
Y
ITA
LY
FRA
NC
E
SPA
IN
JAPA
N
UN
ITED
STA
TES
TUR
KEY
ESTO
NIA
POR
TUG
AL
AV
ERA
GE
BED
S PE
R H
OSP
ITA
L
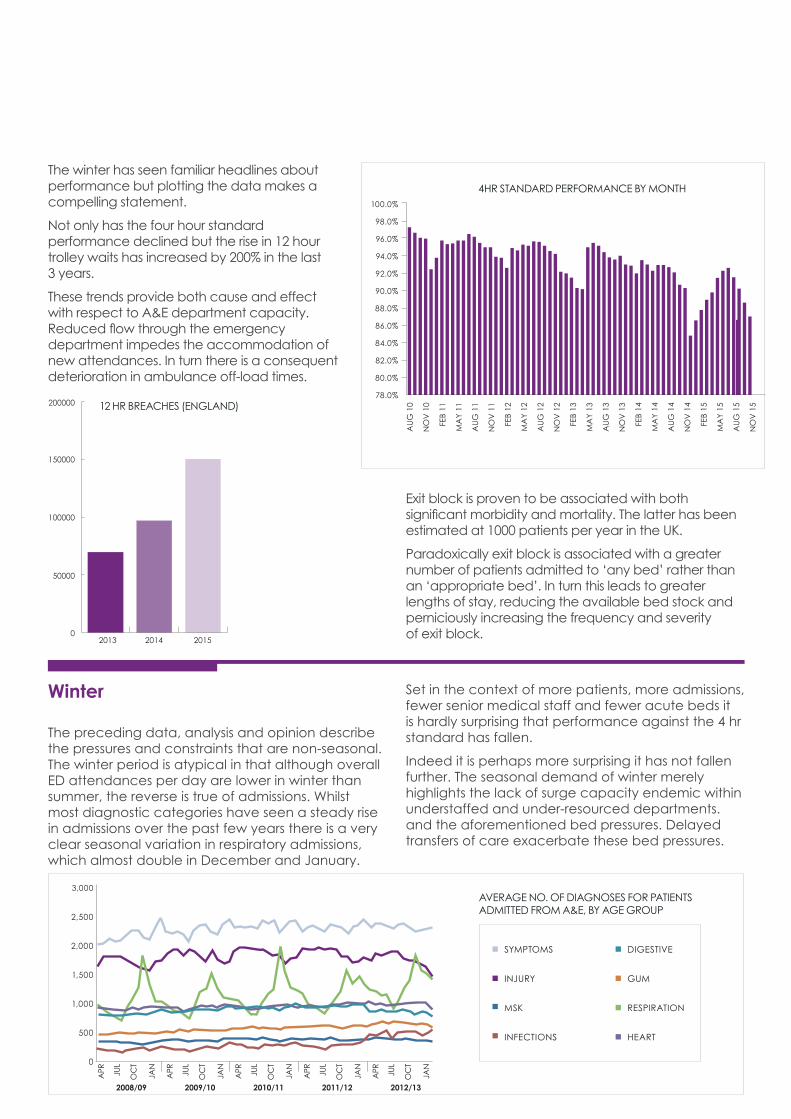
The winter has seen familiar headlines about performance but plotting the data makes a compelling statement.
Not only has the four hour standard performance declined but the rise in 12 hour trolley waits has increased by 200% in the last 3 years.
These trends provide both cause and effect with respect to A&E department capacity. Reduced flow through the emergency department impedes the accommodation of new attendances. In turn there is a consequent deterioration in ambulance off-load times.
Winter
The preceding data, analysis and opinion describe the pressures and constraints that are non-seasonal. The winter period is atypical in that although overall ED attendances per day are lower in winter than summer, the reverse is true of admissions. Whilst most diagnostic categories have seen a steady rise in admissions over the past few years there is a very clear seasonal variation in respiratory admissions, which almost double in December and January.
Exit block is proven to be associated with both significant morbidity and mortality. The latter has been estimated at 1000 patients per year in the UK.
Paradoxically exit block is associated with a greater number of patients admitted to ‘any bed’ rather than an ‘appropriate bed’. In turn this leads to greater lengths of stay, reducing the available bed stock and perniciously increasing the frequency and severity of exit block.
Set in the context of more patients, more admissions, fewer senior medical staff and fewer acute beds it is hardly surprising that performance against the 4 hr standard has fallen.
Indeed it is perhaps more surprising it has not fallen further. The seasonal demand of winter merely highlights the lack of surge capacity endemic within understaffed and under-resourced departments. and the aforementioned bed pressures. Delayed transfers of care exacerbate these bed pressures.
78.0%
80.0%
82.0%
84.0%
86.0%
88.0%
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
AU
G 1
0
NO
V 1
0
FEB
11
MA
Y 11
MA
Y 13
MA
Y 14
MA
Y 15
AU
G 1
1
AU
G 1
3
AU
G 1
4
AU
G 1
5
NO
V 1
1
NO
V 1
3
NO
V 1
4
NO
V 1
5
FEB
12
MA
Y 12
AU
G 1
2
NO
V 1
2
FEB
13
FEB
14
FEB
15
4HR STANDARD PERFORMANCE BY MONTH
RESPIRATION
HEART
DIGESTIVE
GUM
SYMPTOMS
INJURY
MSK
INFECTIONS
AVERAGE NO. OF DIAGNOSES FOR PATIENTS ADMITTED FROM A&E, BY AGE GROUP
500
1,000
1,500
2,000
2,500
3,000
0
2008/09
APR JU
L
OC
T
JAN
2009/10
APR JU
L
OC
T
JAN
2010/11
APR JU
L
OC
T
JAN
2011/12
APR JU
L
OC
T
JAN
2012/13
APR JU
L
OC
T
JAN
12 HR BREACHES (ENGLAND)
2013 20152014
200000
150000
100000
50000
0
Tariffs
Tariffs have led to chronic underfunding of acute care in general and emergency care in particular. In addition they have created perverse activity incentives. The 30% marginal tariff for acute admissions guaranteed acute services in hospitals were dependent upon cross subsidies from elective care. This meant that any arguments for increasing acute care capacity were subordinated to the delivery of more elective services.
This failure to align incomes with activity only changed with the uplift of the tariff to 70% when it became clear that bed occupancy rates in England were so high that elective activity and hence income had become compromised. Regrettably this revision was too little too late.
Within the A&E department itself tariffs are also ill conceived. Those patients requiring least intervention, investigation or treatment are remunerated at a rate that enables services to be maintained. However the maximum tariff for the most seriously ill or injured is less than £250. This ensures that treating the very patients emergency departments are established to treat is a loss making endeavour for a hospital.
There are ample examples of finances driving behaviour in the NHS. Poor systems of reimbursement for acute care have led to almost two decades of underfunding. We are currently reaping the consequences with A&E departments woefully understaffed much of the time.
Were this situation associated with significant cost savings an independent scrutineer might adjudge the constraints and consequences as worthwhile. However the costs of supporting this overstretched system are considerable. Examining just the locum costs for A&E doctors (i.e. excluding all other medical locums and nursing agency costs) demonstrates the weekly spend is £3 million. The average annual running cost of a medium sized emergency department is £8.5 million. It is therefore a matter of simple arithmetic that if invested rather than spent we could actually run an additional 17 medium sized A&E departments per year and still save money.
Building consensus
The foregoing data is provided by the Department of Health, NHS England, statutory bodies and health foundations. The College has worked tirelessly to participate in the current debates on urgent and
emergency care, offering a unique insight and expertise from the perspective of frontline clinicians working in the A&E departments of the UK.
In September of 2015 we welcomed the publication of the document ‘Safer, Faster, Better’, published by NHS England. In particular the following conclusions
• Emergency departments (EDs) should be fully resourced to practice an advanced model of care where the focus is on safe & effective assessment, treatment and onward care.
• Whilst it is essential to manage demand on EDs, this should not detract from building capacity to deal with the demand faced, rather than the demand that is hoped-for.
• ED crowding adversely affects every measure of quality and safety for patients & staff.
• The main causes of ED crowding include surges in demand and lack of access to beds in the hospital system due to poor patient flow and high hospital occupancy rates.
• EDs should be staffed so that capacity meets variation in demand NOT average demand.
• Performance against the 4-hour standard is a useful proxy measure of crowding.
Conclusion
Data shows that admissons are likely to continue to rise by more than 50,000 patients per year. It is beyond dispute that our hospitals will need greater acute bed capacity and more senior decision makers within the emergency department and A&E hub. Planning must address the need to cope with rising numbers of attendances by the frail elderly – with complex interactions between health and social care and long term co-morbidities rather than focussing on reducing attendances by other groups – which are already amongst the lowest per capita in Western Europe. Correct funding of emergency care, fairness of contracts to promote a sustainable career in emergency medicine and the creation of A&E hubs to decongest emergency departments will underpin a successful strategy that is patient centred, affordable, efficient and effective.
Dr Clifford Mann
President of the Royal College of Emergency Medicine
© The Royal College of Emergency Medicine 2016
Data Sources
The Nuffield Trust
The Royal College of Emergency Medicine
Health Education England
Department of Health
NHS England
NHS Confederation
The Commonwealth Fund
£
RCEM’s steps to rebuilding emergency medicine
![[Winter Admission] Guidelines for Applicants to the Apr. 2020, Oct. … › admission › forms › master › m... · 2019-11-01 · admissions score as shown below. Less than 350](https://img.pdfslide.us/doc/110x75/5f0bbad87e708231d431eebe/winter-admission-guidelines-for-applicants-to-the-apr-2020-oct-a-admission.jpg)




























