Embed Size (px)
Citation preview

This article was downloaded by: [University of Haifa Library]On: 02 November 2014, At: 00:38Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Administration in Social WorkPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/wasw20
Who's in Charge Here? Structures forCollaborative Governance in Children'sMental HealthSharon Hodges a , Kathleen Ferreira a , Debra Mowery a & EmilyNovicki aa Department of Child and Family Studies , Florida Mental HealthInstitute, College of Behavioral and Community Sciences, Universityof South Florida , Tampa , Florida , USAAccepted author version posted online: 10 Jun 2013.Publishedonline: 11 Sep 2013.
To cite this article: Sharon Hodges , Kathleen Ferreira , Debra Mowery & Emily Novicki (2013) Who'sin Charge Here? Structures for Collaborative Governance in Children's Mental Health, Administration inSocial Work, 37:4, 418-432, DOI: 10.1080/03643107.2012.758062
To link to this article: http://dx.doi.org/10.1080/03643107.2012.758062
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Administration in Social Work, 37:418–432, 2013Copyright © Taylor & Francis Group, LLCISSN: 0364-3107 print/1544-4376 onlineDOI: 10.1080/03643107.2012.758062
Who’s in Charge Here? Structures for CollaborativeGovernance in Children’s Mental Health
Sharon Hodges, Kathleen Ferreira, Debra Mowery, and Emily NovickiDepartment of Child and Family Studies, Florida Mental Health Institute, College of
Behavioral and Community Sciences, University of South Florida,Tampa, Florida, USA
Communities increasingly use community coalitions to promote collaborative action andcommunity-based problem solving. This article presents research findings on governance structures andinteragency collaboration in children’s mental health. Specific governance structures are discussed, aswell as lessons in collaborative governance applicable to coalitions serving a variety of communityneeds.
Keywords: children’s mental health, collaborative governance, community coalitions, governance struc-tures, interagency collaboration
INTRODUCTION
Communities across the United States use community coalitions (alliances among groups and indi-viduals with overlapping interests) to promote shared community commitment, collaborative action,and community-based problem solving (Assistant Secretary for Planning and Evaluation [ASPE],2010; Saxe & Hallfors, 1997). Community coalitions have become popular vehicles for address-ing community issues through shared decision making, the presumption being that this is a goodstrategy for sustaining impact in the community over time (ASPE 2010). Members of communitycoalitions work together to address a wide array of serious issues facing today’s youth, includingsubstance abuse (Hallfors, Cho, Livert, & Kadushin, 2002; Hingson et al., 2005), teen pregnancy(Paine-Andrews et al., 2002), and emotional and behavioral challenges (Hernandez & Hodges, 2006;Hodges, Friedman, & Hernandez, 2008).
Although efforts to establish collaborative community-based mental health care for individualswith serious mental illness began in the 1960s (e.g., Mental Retardation Facilities and CommunityMental Health Centers Construction Act, Public Law 88–164, 1963), the specific focus oncommunity-based systems of care for children and youth with serious emotional disturbance (SED)
This research was partially funded by the National Evaluation of the Children’s Mental Health Initiative (SubstanceAbuse and Mental Health Services Administration). The authors gratefully acknowledge the support of National Evaluationcolleagues Brigitte Manteuffel, PhD, and Freda Brashears, MSW.
Correspondence should be addressed to Sharon Hodges, Department of Child and Family Studies, Florida Mental HealthInstitute, College of Behavioral and Community Sciences, University of South Florida, 13301 Bruce B Downs Blvd, MHC2437, Tampa, FL 33612-3807, USA. E-mail: [email protected]
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

COLLABORATIVE GOVERNANCE IN CHILDREN’S MENTAL HEALTH 419
emerged 20 years later from the work of Knitzer (1982), who estimated that 3 million childrenwith SED were not getting needed services and many others were receiving inappropriate hospitalor institutional care. Knitzer described barriers to coordinated community-based care within andbetween child-serving agencies, and suggested specific strategies for organizing services acrosschild-serving agencies (e.g., mental health, child welfare, juvenile justice, and education) inorder to reduce restrictiveness of placement and support smooth transition from one service toanother (Hernandez & Hodges, 2003). Based on Knitzer and the work of Stroul and Friedman(1986), which also focused on interagency collaboration in service delivery, federal policy forchildren’s mental health has emphasized improved service planning and delivery through increasedcollaboration among community partners since the 1980s (e.g. National Institute of Mental Health,1983; President’s New Freedom Commission on Mental Health, 2003; Public Law 102–321, 1992;U.S. Public Health Service, 2000). Specifically, the Substance Abuse and Mental Health ServicesAdministration (SAMHSA) has provided more than $1.5 billion in funding through the CommunityMental Health Initiative (CMHI) to support the development of collaborative, community-basedservices for children and youth with serious emotional disturbance and their families known assystems of care (ICF Macro, 2011; U.S. Department of Health and Human Services [USDHHS],2009). This funding mechanism includes a requirement to establish collaborative governanceamong a coalition of groups and individuals to oversee children’s mental health services andsupports across multiple agencies.
Research on community coalitions has focused more often on coalition-building factors thattarget the development of collaborative capacities such as shared leadership, conflict resolution,planning processes, communication styles, and member recruitment and participation (Foster-Fishman, Berkowitz, Lounsbury, Jacobson, & Allen, 2001; Zakocs & Edwards, 2006), andnumerous foundation and federal funders provide resources for coalitions striving to develop effec-tive collaborative solutions (e.g., Butterfoss, 2007; Florin, Mitchell, & Stevenson, 1993). There isless information available specific to collaborative governance in community coalitions. This arti-cle will present findings of an analysis of governance structures and interagency collaboration incommunities funded during the 2002 cycle of the Children’s Mental Health Initiative (CMHI). Theresearch team examined requirements of the Guidance for Applicants (GFA), community fundingproposals, and System of Care Assessment (SOCA) data gathered as part of the national evaluationof this initiative for the purpose of determining the types of collaborative governance structuresused in public children’s mental health systems. The paper will provide a description of specificgovernance structures used in systems of care, examples of each type of governance structure, andlessons related to collaborative governance that may be applied more broadly to the implementationof community coalitions.
LITERATURE REVIEW
The concepts of interagency collaboration in the planning and delivery of services and a structurethat provides clarity around roles, responsibilities, and accountability of agency partners are notnew concepts to systems of care. In fact, interagency collaboration and collaborative governancehave been core components of systems of care since its inception. In the original monograph defin-ing systems of care, Stroul and Friedman (1986) discuss service system management at multiplelevels and describe “interagency entities for system-level coordination,” along with early efforts tojointly administer services (p. vi). Since that time, many definitions of interagency collaborationand collaborative governance have been put forth in the literature (Ansell & Gash, 2008; Emerson,Nabatchi, & Balogh, 2011), but for the purpose of this analysis, the research team used the defini-tions for interagency collaboration and governance provided in the CMHI 2002 GFA (USDHHS,2002). According to the GFA, interagency collaboration is defined as “formal arrangements that
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

420 HODGES ET AL.
child-serving agencies make among themselves to enable provision of the broad array of services”(USDHHS, 2002, p. 25–26). The governance body is separately defined in the GFA as “a groupof individuals with the authority to make policy decision for the system of care” (USDHHS, 2002,p. 28).
Positive outcomes from collaboration within systems of care have been well documented andinclude improved relationships among child-serving agencies, enhanced understanding of system ofcare principles, increased relevance of mental health services, and improved relationships betweenfamilies and service providers (Hodges, Nesman, & Hernandez, 1999). In addition, collaborationallows agencies to better coordinate services, reduce deficiencies (i.e., children “falling through thecracks”), and address a lack of qualified or trained personnel (Huxham, Vangen, & Eden, 2000;Johnson, Tam, Zorn, LaMontagne, & Johnson, 2003; Pfeiffer & Cundari, 2000; Prince & Austin,2005; Walter & Petr, 2000). Furthermore, there are sound financial reasons for collaboration, mostnotably the efficiencies produced by avoiding duplication of services and the ability to spread thecost and risk of a large initiative across several agencies (Huxham et al., 2000; Johnson et al., 2003;Mattessich & Monsey, 1992; Walter & Petr, 2000).
The idea of collaborative governance is hardly unique to systems of care. Broadly, collaborativegovernance is seen as the only way to reach comprehensive solutions to complex, interconnectedissues that cannot be solved by one agency alone (Huxham et al., 2000; Imperial, 2005) and isincreasingly recognized as a necessary strategy for coordinating services across multiple sectors(Chambers, Tullys, Mayer, & Wigand, 2008; Huxham et al., 2000; Walter & Petr, 2000). Accordingto Emmerson, Nabatchi, and Balogh (2011) collaborative governance “ is seen by many as the newway of doing the business of government” (p. 23). Others have pointed out that collaboration isreplacing two alternate forms of governance: adversarialism, a “winner-takes-all” approach, andmanagerialism, wherein agency experts make decisions unilaterally or through closed decision-making processes. Collaborative governance, by contrast, is more inclusive and seeks to createcooperative relationships among relevant parties (Ansell & Gash, 2008). This growth in collab-orative governance is in part due to compulsory legislative mandates and funding requirements(Chambers et al., 2008; Huxham et al., 2000; Johnson et al., 2003; Pfeiffer & Cundari, 2000).
Despite the benefits of interagency collaboration and collaborative governance, systems of caresites frequently struggle to make these concepts a reality (Bazron, Curtis, King, & Kosier, 2006).The literature suggests that there are a number of challenges faced by communities embarking onmulti-agency change efforts. Pfeiffer and Cundari’s (2000) framework organized challenges intothree domains. The first domain is Informational or Skill Set Barriers, which relate to profession-als’ lack of knowledge of important information, skills, and terminology. Because agencies aresiloed by differences such as funding source and agency mandate, partners often do not under-stand what others do or speak a common language; jargon is often excessively employed (Evans,Armstrong, Beckstead, & Lee, 2007; Johnson et al., 2003; Pfeiffer & Cundari, 2000). The seconddomain is Attitudinal Barriers, which arises from the frame of reference each person brings to thetable based on past experiences, beliefs, expectations, hopes, and fears. This frame of reference can“filter, distort, or obscure information, or result in selective attention to information” (Pfeiffer &Cundari, 2000, p. 113). Attitudinal challenges include a history of conflict, different organizationalcultures, lack of commitment, lack of trust, and lack of a common vision or shared goals (Horwath& Morrison, 2007; Imperial, 2005; Johnson et al., 2003; Walter & Petr, 2000). The final domain isOrganizational or Regulatory Barriers, which are the product of differing missions, legislative man-dates, regulatory requirements, and funding mechanisms among agencies. Challenges in this domainconsist of asymmetries in power, knowledge, and resources; incompatible agency regulations andlegislation; categorical or inflexible funding streams; and constraints on information sharing, suchas privacy regulations (Ansell & Gash, 2008; Horwath & Morrison, 2007; Imperial, 2005; Johnsonet al., 2003; Pfeiffer & Cundari, 2000).
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

COLLABORATIVE GOVERNANCE IN CHILDREN’S MENTAL HEALTH 421
Although the literature offers a number of models for interagency collaboration and shared gov-ernance useful to community coalitions, the models created by Ansell and Gash (2008), Emersonet al. (2011), and Horwath and Morrison (2007) are particularly comprehensive and applicableto multi-agency community coalitions. These models share several key elements characteristic ofwell-functioning collaborative governing bodies. First is the importance of establishing a diverse,inclusive membership; diversity must be sought out, rather than tolerated, in order to incorporate abroad range of views (Ansell & Gash, 2008; Emerson et al., 2011). Ansell and Gash (2008) pointout that inclusiveness is closely linked to the exclusiveness of the collaborative group, explaining,“When the collaborative forum is ‘the only game in town,’ it is easier to motivate stakeholders toparticipate; conversely when they are excluded, they may be impelled to seek out alternative venues”(p. 556). An invitation to collaborate is necessary but insufficient; stakeholders must feel they havea legitimate opportunity to participate before they will buy in to the collaborative process (Ansell &Gash, 2008).
Incentives to participate are also considered an important facilitator of engaged membership(Emerson et al., 2011). According to Ansell and Gash (2008), incentives to participate increasewhen stakeholders can see a direct relationship between their participation and tangible outcomes,while, conversely, incentives decrease when stakeholders feel their role is advisory or ceremonial.Emerson et al. (2011) see incentives as just one of four possible system drivers leading to collabora-tion: leadership (a strong champion leading the way), consequential incentives (internal problems,resource needs, interests, opportunities or external crises, threats, or opportunities), interdependence(individuals or organizations are unable to accomplish a goal on their own), and uncertainty (ifgroups are unable to deal with uncertainty internally, they may be driven to collaborate in order toreduce, diffuse, or share risk). In any case, stakeholders must see some gain for their participation,either for themselves, their organization, or the larger cause.
The literature also indicates that clear rules and a transparent decision-making processes shouldbe established by community coalitions. Clear and consistently applied ground rules reassurestakeholders (who often have misgivings) that the process is fair, equitable, and open (Ansell &Gash, 2008). To this end, resources, which are often unequally distributed among stakeholders,must be carefully managed to preserve feelings of fairness and legitimacy (Emerson et al., 2011).The nature of the ground rules depends on the group, but more complex and long-lived collab-orations may need more structure and formal rules such as bylaws and charters (Emerson et al.,2011). The literature is mixed on whether consensus is the best decision-making process, andwhether deadlines are helpful (Ansell & Gash, 2008). Whatever the decision-making processmay be, it should be based on a shared and articulated mission, vision, and theory of change(Emerson et al., 2011; Horwath & Morrison, 2007). Articulation is particularly important whenthe collaboration is externally mandated, since partners may assume the mandate provides suffi-cient motivation and clarity regarding goals when this may not be the case (Horwath & Morrison,2007).
In systems of care, analyses of collaborative governance have been conducted with communitiesfunded in 1993–1994 (Vinson, Brannan, Baughman, Wilce, & Gawron, 2001) and 1998 (Paulson,Fixen, & Friedman, 2004; Vinson, Brannan, Baughman, Wilce, & Gawron, 2001). Buildingupon this work, the findings reported here address the 2002 GFA requirement that CMHI-fundedcommunities establish a collaborative governing body as a decision-making group rather thanthe advisory or information-sharing/educational group required of earlier funded communities, anoteworthy shift in funder guidelines. The reader will note that for the purpose of this analysis,the research team intentionally used the term “collaborative governance” instead of “interagencygovernance” to reflect more comprehensive governance structures that include not only traditionalpublic agency partners but also family members, youth, private nonprofit providers, and informalsupports within the site.
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

422 HODGES ET AL.
METHODS
Research Questions
The overall goal of this research project was to identify key governance structures used withinsystems of care funded through the CMHI. This qualitative secondary data analysis consid-ers the intersection of system of care governance with the core system of care component ofinteragency collaboration. In addition to identifying key governance structures, this study examinedthe following research questions:
1. Why and under what circumstances are particular governance structures successful?2. How do the various components of governance structures (e.g. roles, responsibilities) impact
their success?3. What factors influence the successful functioning of the governance structures initially
proposed by communities?
For the purpose of this paper, success is defined according to the requirements for governance andinteragency collaboration described in the GFA and summarized in Table 1. Because the focus ofthis paper is on cross-agency governance structures, service access and child and family outcomedata were not included in this analysis.
Sample
This study sample included 24 of 29 sites funded during Phase IV of the CMHI program in the early2000s. Five sites were not included in the analyses because they either did not complete the fundingperiod or cultural differences created unique contexts that made comparison difficult. Of the 24 sitesincluded in the study, the service delivery catchment areas varied such that six sites were fundedto develop systems of care for cities or municipalities, seven for counties, three for multi-countyareas, six for states, and two for U.S. territories. Geographically, seven sites were located in thewest, three in the southwest, four in the Midwest, four in the northeast, four in the southeast, andthe two territories were non-contiguous. It should be noted that eligibility requirements for fundinglimit applicants to public entities such as states, political subdivisions of states (e.g., counties orcities), tribal organizations, the District of Columbia, or U.S. territories (USDHHS, 2002).
Data Sources
Three sources of data were used in this analysis: 1) the 2002 GFA document for the CMHI program,2) site proposals in response to the GFA, and 3) the biannual system of care assessment conductedas part of the national evaluation of the CMHI program. The GFA was used to gain clarity aroundthe expectations for governance and interagency collaboration for funded systems of care. Table 1summarizes how the concepts of interagency collaboration and governance were operationalized inthe 2002 GFA.
Funding proposals submitted in response to the GFA were analyzed for the purpose of under-standing community context and proposed plans for system of care governance. Anticipated gover-nance structures were specifically addressed in each of the proposals, often including organizationalcharts and proposed lines of authority. Finally, the biannual System of Care Assessment (SOCA)reports were used for the purpose of assessing the development of governance structures during sys-tem of care implementation according to the requirements outlined in the GFA and in considerationof any changes to the governance plan initially proposed. Nineteen sites received three site visits,which resulted in three SOCA reports during program years 2, 4, and 6; however, due to a change inthe National Evaluation protocol, five sites received only two assessments (in program years 2 and
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

COLLABORATIVE GOVERNANCE IN CHILDREN’S MENTAL HEALTH 423
TABLE 1Requirements for Governance and Interagency Collaboration in the 2002 CMHI GFA
GFA Requirements for Governance
• Group with authority to make decisions• Membership should include: representatives from entity that received funding, collaborating state/community child
serving agencies, family members, and community representatives including racial/ethnic populations• Group should develop and uphold formal agreements• Group should be accountable for standards of care such as cultural competence, family involvement, and standards of
practice shown effective through research and evaluation studies• Group should ensure that cooperative agreement funds are expended appropriately within the community by keeping up
to date with reforms• Group should monitor clinical and functional outcomes• Group can be a board of directors, committee, task force, or workgroup
GFA Requirements for Interagency Collaboration
• Includes formal arrangements (memoranda of understanding, policy manuals, board minutes)• Provides a broad array of services• Should include child-serving agencies such as mental health, education, child welfare, child protective services, juvenile
court, juvenile corrections, primary healthcare, substance abuse treatment & prevention, vocational counseling, andrehabilitation
• Is located in the community• Specifies roles of agencies in a system of care: financial contributions, representatives in governance structure,
participation in strategic planning and service delivery• Specifies if agencies are local or state entities
4). In total, 24 site proposals and 67 SOCA reports were analyzed, allowing for longitudinal studyof governance over three or four points in time, depending upon the initial funding date.
Data Analysis
This study used a team-based approach to qualitative analysis that incorporated multiple researchers;the analysis team included the principal investigator and three trained team members. The standardfor team-based qualitative analysis requires that data be coded individually by multiple team mem-bers and then compared and discussed regularly as themes are identified (Guest & MacQueen, 2008;LeCompte & Schensul, 1999a; Miles & Huberman, 1994; Silverman, Ricci, & Gunter, 1990). Theseconventions were used in this analysis, with team members coding each site’s funding proposals andSOCA reports using a priori codes developed from the definitions of governance and interagencycollaboration in the GFA and the work of Vinson et al. (2001). The final coding framework includedvariables such as whether a new or existing structure was used for governance, membership, roles,and responsibilities of the governance group(s), the fiscal agent, and feedback from the SOCAreports regarding strengths and challenges of governance and interagency collaboration. Data foreach site were entered into a matrix in which there was a column for each data source and a rowfor each variable. During the analysis, the coding system was refined and intercoder agreementwas established (Guest & MacQueen, 2008; LeCompte & Schensul, 1999a, 1999b). This study wascertified exempt by the University of South Florida’s Institutional Review Board.
Data entered into the matrices were then analyzed using an inductive, constant comparativeapproach (LeCompte & Schensul, 1999a, 1999b) to develop typologies of the governance structuresfound in CMHI community coalitions. The entire team examined the data matrix for each site, anda simple graphic depicting its governance structure was developed and compared to previous sites.
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

424 HODGES ET AL.
Team members debated whether each site fit into an existing typology or represented an entirelynew structure. Disagreements were resolved through group discussion of indicators and contra-indicators in the data. Once basic typologies were developed, the team identified an example foreach governance structure in order to provide more detailed description of collaborative governance.Examples were chosen based on the clear articulation of the roles, responsibilities, and membershipof the governing bodies in the grant application and subsequent SOCA reports; progress made inthe development of interagency and stakeholder communication; and demonstration of overcom-ing challenges in a proactive, constructive way. Strengths and challenges across funded sites wereanalyzed inductively, and themes emerged that were organized into lessons learned. Examples werechosen that were particularly representative or illuminating for each lesson learned.
RESULTS
CMHI-funded communities were asked to respond to service gaps, inadequacies, and barriers forchildren and youth with or at risk of serious emotional disturbance by providing access to servicesand supports across agency administrative jurisdictions. Data indicate that CMHI systems of carewere required, as a condition of funding, to establish a governance body with authority to make col-laborative decisions regarding the development and implementation of community-based servicesand supports for children and youth with or at risk of serious emotional disturbance and their fam-ilies. These governance groups were expected to develop and uphold formal agreements to ensurestandards of care, monitor clinical and functional outcomes, provide a broad array of services, andensure that CMHI funds were expended appropriately. The funding requirements gave the govern-ing bodies a primary cross-agency responsibility to facilitate a coordinated and systemic responseto meeting service needs; however, the funder provided much latitude as to the actual structure ofthese bodies, the specifics of their membership, and their linkages to other organizations within thecommunities they served. It should be noted that the participation of child-serving agencies suchas education, child welfare, and juvenile justice in the children’s mental health governing bodies iscompletely voluntary, and data indicate that interagency participation varied over time according tothe willingness and ability of partners to participate in system activities.
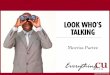
The data indicate that the funded communities put two types of governance structures into place(Figure 1). The single-level governance structure was used in systems of care that are boundedas a single entity or considered “stand alone.” In this type of structure, decision making andfunding authority remain at a single level, and the system operates independently of state oversight.A single interagency council acts as the governing structure, often accomplishing tasks throughworkgroups, subcommittees, or smaller executive committees. Fourteen of the 24 sites used asingle-level governance structure: seven county-based systems of care, four city-based systems,two state/territory systems, and one multi-county system of care.
FIGURE 1 Collaborative governance structures used.
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

COLLABORATIVE GOVERNANCE IN CHILDREN’S MENTAL HEALTH 425
The second type of governance structure is the tiered governance structure, which is character-ized by multiple levels of linked governance. This is most often carried out in state to regional tolocal linkages, but may also be implemented in state to local, regional to local, and city to local link-ages. In this type of structure, decision making and funding authority originates at the top tier butmay be distributed to lower levels. Governance is accomplished through interagency councils oper-ating at multiple levels, but the top tier usually has the ultimate authority to make fiscal and policydecisions. Ten sites used a tiered governance structure: six states, two cities, and two multi-countysystems of care.
Single-Level Governance Example
The single-level governance example, Site 1, was a county-based system of care that operatedthrough county government. The governance council was an interagency group formed several yearsprior to CMHI funding, when Site 1 initially received funding to create a system of care in theircounty. The governance council applied for the CMHI grant in order to expand the populationsserved by the Site 1 system of care.
Like many systems sampled in this analysis, SOCA data indicate that membership of this gover-nance council changed significantly over time. In the site’s funding proposal, the Site 1 governancecouncil was relatively small, consisting of high-ranking representatives from the public child-serving agencies. as well as the judiciary, a family member, and several community organizations.A smaller executive cabinet was also described, which included the directors of the two consoli-dated human services agencies, the probation chief, the superintendent of the county Departmentof Education, and a juvenile court judge. While the executive cabinet membership remained largelyunchanged throughout the funding cycle, the larger governance body saw greater change. Over thesix-year span of the CHMI grant, the governance council lost education and public health membersdue to non-attendance, then gained additional school and community members.
SOCA data indicate that Site 1 worked throughout the grant period to ensure that the key play-ers were engaged in governance. Family involvement grew over time, as system partners activelyworked to recruit more families as members changed meeting times to accommodate families.Family participation was further facilitated by transportation assistance, childcare reimbursement,and stipends. Site 1 did not have complete success at achieving stakeholder diversity, however,as they struggled with youth involvement and obtaining racial/ethnic diversity among governancecouncil membership reflective of the population of children and families they served.
As part of the Site 1 grant application, child-serving agencies signed a memorandum of under-standing (MOU) outlining their commitment to shared governance and the activities that would berequired for its implementation. Bylaws further cemented their commitment. SOCA data show thatthe roles of both the governance council and executive cabinet remained fairly stable over the courseof the grant. The governance council’s responsibilities included strategic planning, budget reviewand recommendations, development of a service array, establishment of formal arrangements amongagencies, and addressing interagency issues. The executive cabinet was initially tasked with systemof care oversight, developing the vision, and contracting with other agencies and organizations. Overtime, it took on tasks related to sustainability, systems integration, and upper-level managementissues that concerned all agency partners. The governance council also had responsibilities beyondthe system of care, as it served as the child abuse committee and interagency service coordina-tion group. Work within the governing body was accomplished through several subcommittees thatfocused on particular concerns, such as cultural competence and communication and collaboration.
Although the executive cabinet was identified in the funding application as the final decision-making authority, SOCA data indicate that its decisions were not binding in the first two years butgrant staff implemented decisions and recommendations 95% of the time. However, by the secondSOCA site visit in Year 4, the authority of Site 1 governance appeared more clearly exercised. The
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

426 HODGES ET AL.
executive cabinet began to make final policy decisions for cross-system issues based on recommen-dations by the larger governance council. However, the project administrators still maintained finaldecision-making authority for project policies, although SOCA data indicate that grant staff con-tinued to nearly always implement recommendations and decisions from the governance council.At the time of the third SOCA site visit in Year 6, the division of authority was largely the same,although the executive cabinet had undertaken the additional responsibility of cross-system fiscaldecisions.
Tiered Governance Example
The tiered governance example, Site 18, was a statewide initiative in which five regions receivedfunding to pilot systems of care in their designated areas. The plan was to rollout systems of carestatewide once the five regional pilots reached maturation, incorporating lessons learned through-out the implementation process. In order to facilitate this, a three-tiered governance structure wasestablished. Tier 1 was the Site 18 state-level governance body; Tier 2 included five regional-levelgovernance bodies (one for each pilot site); and Tier 3 consisted of governance bodies intended torepresent local communities. The State Team, comprised of executive leadership of the state-levelchild-serving agencies, families, youth, members of the faith community, and providers, providedoversight and system-level coordination for the five pilot regions. SOCA data indicate that, althoughthe Site 18 State Team provided guidance, the governing bodies in the pilot sites were responsiblefor their own strategic planning, budgeting, grant implementation, and local evaluation. SOCA datafurther indicate that within Site 18, the regional governance of Pilot Site A found it challenging tobalance governance of the multi-county region with the need to establish community-level bodiesthat would provide local-level input. The regional governance structure of Pilot Site A consistedof a single governing body for the region and three smaller local community teams to providelocal governance. Membership on all three bodies was open, meaning that members were notnecessarily selected or voted upon for a specified period of membership, resulting in fluctuatingattendance.
Data indicate that adequate representation across stakeholders and linkage across tiers requirescareful attention to successfully implement a tiered governance structure. The regional and localtiers of Pilot Site A did not function as well as anticipated: although described as collaborative,there were no clear lines of authority between these tiers, and it was unclear if the bodies wereadvisory or decision making in nature. As a result, a regional executive committee was formed thatrepresented all five child-serving agencies as well as all five counties in the service area of Pilot SiteA. Eventually, the executive committee expanded its membership to include a representative fromthe family organization and leadership at the state level. At the same time, the local communityteams transformed into community coalitions with representatives from county-level child-servingagencies, families, community-based organizations, and private providers. During these transitions,Pilot Site A governance worked to ensure diverse membership by offering stipends, childcare reim-bursement, and transportation reimbursement to facilitate family participation at the governancemeetings for the majority of their funding cycle. They also successfully worked to engage publichealth, which had not originally participated in governance.
Over time, governance membership in Pilot Site A became more specified, and the roles andresponsibilities of the regional and local-level groups became better defined. Data indicate that,over time, the relationship between the regional and local groups became more hierarchical, with theexecutive committee holding the policy and decision-making authority (with guidance from a stateliaison), while the local community coalitions served in an advisory capacity. At the time of the finalSOCA assessment, the Pilot Site A executive committee was responsible for overall implementationof the system of care across the service region, as well as strategic planning, monthly budget review,fundraising, and review of evaluation data. The local-level bodies were responsible for providing
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

COLLABORATIVE GOVERNANCE IN CHILDREN’S MENTAL HEALTH 427
recommendations to the executive committee, providing local governance, identifying service gapsand resources, developing and implementing local projects, and strategic planning.
Although participation in governance at the state level was mandated in part by legislation and inpart by an MOU signed by state child-serving agencies, the regional and local tiers of governancewere implemented without formalizing their relationships through memoranda of understanding.SOCA data indicate that evaluators recommended that Pilot Site A create MOUs or some other typeof formal agreement to improve their interagency collaboration.
DISCUSSION
Data suggest that both single-level and tiered governance structures are effective options for collab-orative governance. The tiered structure appears to work effectively in larger geographic areas aswell as states in which authority is highly centralized. Single-level structures are often appropriatefor smaller city or county initiatives, especially in states in which authority is largely delegated tocounties and/or cities. Despite these differences, several lessons related to collaborative governanceemerged from this analysis that cross cut governance structure typologies in their application toboth tiered and single-level governance structures. These lessons, discussed in more detail below,indicate that attention to size, membership, diversity, budget authority, and formalization of rolesand relationships support sustainable collaborative governance structures.
A Well-Functioning Governance Body Requires Attention To Practical Size
SOCA data indicate that the struggle to find a balance between inclusiveness and functionality ingovernance membership often resulted in governing bodies expanding and contracting in mem-bership, sometimes rather dramatically. At one site, system partners realized that their governingbody, with its voluntary and unspecified membership, had become too large, leading to diffu-sion of responsibility and difficulty making decisions. This site re-organized its governing bodytwice as stakeholders worked to find a size that would be diverse without being too large. It isimportant to note that SOCA data do not suggest a “perfect size” for a functional governing body—appropriate size is unique to each community and the service needs of its youth and families.However, extremes (i.e., systems with governing bodies that were too exclusive or too expansivein membership) appeared to make decision making difficult. Across the 24 systems included inthis study, the most functional governing bodies were those able to make mid-course correctionsand adapt their governing body to respond to changing needs. An example of this is the pairing ofan executive committee with a larger advisory council. This strategy was used in both tiered andsingle-level governance structures in order to include a wide array of stakeholders in governancewhile ensuring that important decisions could be made in a timely manner.
Cultivating Membership Diversity Requires A Committed Effort
Many communities in this sample had to make special efforts to engage particular agency partnerswho were either uninvolved or minimally involved in governance. For example, one site realized thatconflicting organizational cultures were challenging their partnership with juvenile justice. Buildingthis partnership required consciously orienting juvenile justice professionals in their site to the prin-ciples of systems of care, as well as clearly articulating how participation in systems of care wouldsupport juvenile justice partners in achieving their goals. Similarly, nearly every governance body inthis sample made special efforts to engage families and youth in governance processes. These effortsoften included tangible assistance such as stipends, transportation, childcare, and meals that helpedfacilitate family and youth participation. Some sites also worked to educate families and youth on
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

428 HODGES ET AL.
jargon, acronyms, and relevant legal issues so that they could fully participate in the governance pro-cess. Finally, GFA requirements include racial and ethnic diversity of governance members. SOCAdata indicate that achieving racial and ethnic diversity within a governing body was particularlychallenging for the communities within this sample. This challenge was common across sites in thissample, suggesting that identification of successful strategies for increasing diversity of governancemembers within a community coalition is a topic worthy of further investigation.
Clarity Around the Overall Role And Responsibilities of the Governing Body SupportsSuccessful Interagency Collaboration
Roles and responsibilities must be considered at three levels: those of the overall system of caregoverning body compared to other governing bodies, committees, and workgroups within the com-munity; those of individual agencies or organizations within the system of care effort; and those ofindividual members within the governing body. The data suggest that having clarity around the rolesand responsibilities of the overall governing body allows the roles and responsibilities of partnerorganizations and of individual participants to be more clearly articulated.
Governing bodies are most effective when their roles and responsibilities (e.g., oversight ofblended or braided funding, strategic planning, development and implementation MOUs) are clearlyarticulated and agreed upon by members. The communities in this sample took great effort to clar-ify the roles and responsibilities of the governing body in their funding proposals, but governanceimplementation was frequently more challenging than anticipated. As the system developed, it wasoften necessary to make adjustments to the roles of the governing bodies, including the addition ofadvisory and executive committees with specific purposes. Several sites in this sample intended touse an existing community governing body for governance of the newly funded children’s mentalhealth initiative. This approach has much efficiency, as there is often overlap with the mission andmembership of existing community councils or committees. However, SOCA data indicate that, ifthe purposes of the new initiative and the existing group do not closely align, adding significantresponsibilities and different priorities to an existing group is often unsuccessful. For example, onesite proposed using an existing interagency group as its governing body, but during the first year ofimplementation quickly realized that system of care governance would require more authority andautonomy. A new governing body was ultimately created.
Subcommittees and workgroups configured to report to the larger governing body were oftenused as an efficient way to complete specific governance activities within the systems of care. Thisapproach can be challenging if certain stakeholder groups are not able to contribute to importantgovernance decisions because they are not included in a particular subcommittee. At one site,families voiced frustration when they were excluded from a powerful subcommittee that handledbudgetary matters. One strategy for ensuring inclusion of multiple stakeholders while benefittingfrom the increased efficiencies of subcommittees is to establish processes by which the larger gov-erning body reviews or votes on decisions and recommendations made by subcommittees. Anotherissue was finding a balance between the strategic use of subcommittees and a tendency to estab-lish so many subcommittees that there was a point of diminishing return. One site had so manysubcommittees and interagency groups that the sheer number of meetings became overwhelmingand their governing body eventually disbanded.
The clear articulation of roles and responsibilities is also important for agencies and othercommunity organizations participating in collaborative governance structures. Data suggest thatparticipants must understand the reason for their membership, how their organization’s participationsupports the work of the system, and in turn how their participation supports the mission of theirindividual organization. For example, one site focused specifically on serving their early childhoodpopulation. Because these young children were not directly involved in the juvenile justice system,the juvenile justice partner did not recognize the significance of their involvement and ceased
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

COLLABORATIVE GOVERNANCE IN CHILDREN’S MENTAL HEALTH 429
participation. Rather than risk the loss of an important collaborator, communities should articulatethe value of each partner’s contribution to the community coalition. For example, the role ofjuvenile justice in a system of care serving young children seems critical if one considers theinvolvement of older siblings in juvenile justice or parents in adult justice systems. Similarly, itcould be argued that the success of system of care efforts for this young population pays significantlong-term dividends for juvenile justice partners, as these children are diverted from juvenile justiceto a path of positive functioning in the community.
Individual members must also have clarity regarding their roles and responsibilities on the gov-erning body. Data suggest that the active engagement of individual members depends on whetherthey feel that their participation is meaningful rather than symbolic. This includes ensuring thatmembers of the governing body have sufficient authority to make decisions on behalf of their orga-nizations. Many sites within the sample recognized the importance of decision-making authorityand specified in their proposal that agency representatives would be high ranking in order to ensurethat they would have sufficient decision-making authority. It should be noted that the data werenot clear on how leadership of governing bodies (e.g., elected chairs, workgroup leaders, boardofficers) were selected; this may be an interesting topic for future research using primary datacollection.
Budgetary Authority Often Shapes Decision-Making Power
SOCA data offered several examples of communities in which a governance subcommittee, ratherthan the overall governing body, was given complete fiscal authority. In several cases, the influenceof these subcommittees expanded over time until the subcommittee became the main governingbody. Data indicate that the original governing body was sometimes reduced to an advisory bodyas the group with budgetary authority assumed more control. This transformation is not necessar-ily negative, but communities should carefully consider the placement of fiscal authority and anypossible ramifications.
To Ensure Coalition Sustainability, the Participation of Organizations in Governance MustBe Formalized Without Being Too Prescriptive
In communities where system partners already have a strong commitment to their shared vision,MOUs, bylaws, or other formal organizational commitments can seem redundant and even counter-productive to the trust and functionality that has been established. However, SOCA data indicate thatconcrete MOUs or similar mechanisms that articulate interagency agreements for shared adminis-trative processes, blending or braiding of funds, and integrating or co-locating staff provide stabilityin times of member transition. The data offer several instances in which a member of the gov-erning body retired or changed jobs, leaving that individual’s seat on the governing body vacantfor an extended period of time. In the absence of formal agreements articulating organizationalinvolvement in the coalition and responsibilities toward the coalition and the governance body,sustainability may be challenged by the transition of an individual member. Formalizing the com-mitment of organizational partners through MOUs and similar vehicles helps to institutionalizecollaboration to the point that it is sustained regardless of significant leadership changes.
The data suggest a related concern with regard to organizational participation when the compo-sition of a collaborative governance body is formally mandated by state or local legislation. Dataindicate that, although this strategy provides clearly articulated membership, the engaged partici-pation of governance members is motivated by shared values and trusting relationships rather thanmandate. For governing bodies in which membership is legislated or in some other way mandated,careful attention to orienting membership to the values, mission, and vision of the group is stronglyadvised. In fact, data indicate that membership appointments made by the governor or someone else
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

430 HODGES ET AL.
of high-ranking elected authority can have a destabilizing effect on coalition sustainability becausemembership may change abruptly with turns in political will.
IMPLICATIONS FOR COLLABORATIVE GOVERNANCE
This paper presented a description of specific governance structures used in systems of care,examples of each type of governance structure, and lessons related to collaborative governance.An important limitation of this analysis is that it is focused on a narrow segment of collabora-tive governance models, one focused on public agencies serving children and youth with seriousemotional disturbance and their families. The issues and concerns identified through the reviewof literature suggests that the contextual understanding developed through this analysis regardinggovernance structures and lessons related to collaborative governance might aptly be applied morebroadly to community coalitions focused on a variety of community needs. This might include appli-cation for coalitions that organize services and supports for specific populations such as coalitionsfor transition-age youth, homelessness coalitions, and community development and empowermentcoalitions. Regardless of the issue being addressed, the success and sustainability of communitycoalitions depends on their ability to build understanding and commitment to shared goals andactions among a broad group of stakeholders. Successful collaborative governance requires recog-nition that stakeholders, however committed to the cause at hand, come to the coalition with differentagency and organizational mandates, different roles and responsibilities in the community, differ-ent funding sources and requirements, and different resources and fiscal authorities. Understandingthe potential advantages and disadvantages of different governance structures as well as lessonslearned about collaborative governance can support a coalition’s ability to strengthen the planningand implementation of services, support service access, availability, and coordination, and engagein advocacy and social awareness efforts. We believe this supports greater coalition functionalityand sustainability.
While this study provided guidance on two different kinds of governance structures and fiveimportant lessons learned about collaborative governance, it should be noted that no primary datawere collected and analyzed for this study. A limitation of this type of qualitative secondary anal-ysis is that the documents reviewed were created for another purpose. The research team believesthat future research might involve primary data collection and could focus on the processes of gov-ernance, rather than its form or structure. The effectiveness of various decision-making processes(consensus, voting, use of deadlines, etc.), mechanisms for conflict resolution among members, andnegotiation of written agreements (such as MOUs and bylaws) would all be worthy topics for pri-mary data collection and analysis. Additionally, further research to explore less tangible aspects ofinteragency collaboration such as development of shared values, fostering effective working rela-tionships, and the influence of culture on governance structure and process, would provide valuablecontributions to our understanding of collaborative governance in community coalitions.
REFERENCES
Ansell, C., & Gash, A. (2008). Collaborative governance in theory and practice. Journal of Public Administration Researchand Theory, 18(4), 543–571. doi: 10.1093/jopart/mum032
Assistant Secretary for Planning and Evaluation (ASPE). (2010). Developing a conceptual framework to assess thesustainability of community coalitions post-federal funding. Washington, DC: U.S. Department of Health and HumanServices.
Bazron, B. J., Curtis, T. J., King, T., & Kosier, E. R. (2006). Governance: Process, function and structure TechnicalAssistance Partnership Start-Up Webinar Series. Washington, DC: Technical Assistance Partnership for Child and FamilyMental Health.
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

COLLABORATIVE GOVERNANCE IN CHILDREN’S MENTAL HEALTH 431
Butterfoss, F. D. (2007). Coalitions and partnerships in community health. San Francisco, CA: Jossey-Bass.Chambers, R., Tullys, T., Mayer, K., & Wigand, D. (2008). Regional collaborative practice in psychiatric rehabilita-
tion and recovery: A best practice model. Journal of Social Work in Disability & Rehabilitation, 7(3), 187–231. doi:10.1080/15367100802487457
Emerson, K., Nabatchi, T., & Balogh, S. (2011). An integrative framework for collaborative governance. Journal of PublicAdministration Research and Theory. doi: 10.1093/jopart/mur011
Evans, M. E., Armstrong, M. I., Beckstead, J. W., & Lee, J. (2007). Examining the impact of policy on collaboration insystems of care. Journal of Child and Family Studies, 16(4), 567–576. doi: 10.1007/s10826-006-9107-0
Florin, P., Mitchell, R., & Stevenson, J. (1993). Identifying training and technical assistance needs in community coalitions:a developmental approach. Health Education Research, 8, 417–432. doi: 10.1093/her/8.3.417
Foster-Fishman, P. G., Berkowitz, S. L., Lounsbury, D. W., Jacobson, S., & Allen, N. A. (2001). Building collaborativecapacity in community coalitions: A review and integrative framework. American Journal of Community Psychology,29(2), 241–261. doi: 10.1023/A:1010378613583
Guest, G., & MacQueen, K. M. (2008). Handbook for team-based qualitative research. Walnut Creek, CA: AltaMira Press.Hallfors, D., Cho, H., Livert, D., & Kadushin, C. (2002). Fighting back against substance abuse: Are community coalitions
winning? American Journal of Preventive Medicine, 23(4), 237–245. doi: 10.1016/S0749-3797(02)00511-1Hernandez, M., & Hodges, S. (2003). Building upon a theory of change for systems of care. Journal of Emotional and
Behavioral Disorders, 11, 19–26.Hernandez, M., & Hodges, S. (2006). Applying a theory of change approach to interagency planning in child mental health.
American Journal of Community Psychology, 38(3–4), 165–173. doi: 10.1007/s10464-006-9079-7Hingson, R. W., Zakocs, R. C., Heeren, T., Winter, M. R., Rosenbloom, D., & DeJong, W. (2005). Effects on alcohol related
fatal crashes of a community based initiative to increase substance abuse treatment and reduce alcohol availability. InjuryPrevention, 11(2), 84–90. doi: 10.1136/ip.2004.006353
Hodges, S., Friedman, R. M., & Hernandez, M. (2008). Integrating the components into an effective comprehensive systemof care. In B. Stroul & G. Blau (Eds.), The System of Care Handbook: Transforming Mental Health Services for Children,Youth, and Families. Baltimore, MD: Brookes Publishing
Hodges, S., Nesman, T., & Hernandez, M. (1999). Promising practices: Building collaboration in systems of care Systemsof Care: Promising Practice in Children’s Mental Health, 1998 Series, Volume VI. Washington, DC: Center for EffectiveCollaboration and Practice, American Institutes for Research.
Horwath, J., & Morrison, T. (2007). Collaboration, integration and change in children’s services: Critical issues and keyingredients. Child Abuse & Neglect, 31(1), 55–69. doi: 10.1016/j.chiabu.2006.01.007
Huxham, C., Vangen, S., & Eden, C. (2000). The challenge of collaborative governance. Public Management Review, 2(3),337–358. doi: 10.1080/14719030000000021
ICF Macro. (2011). Children’s Mental Health Initiative (CMHI), from http://www.macrointernational.com/projects/cmhi/default.aspx
Imperial, M. T. (2005). Using collaboration as a governance strategy. Administration & Society, 37(3), 281–320. doi:10.1177/0095399705276111
Johnson, L. J., Tam, B., Zorn, D., LaMontagne, M., & Johnson, S. A. (2003). Stakeholders’ views of factors that impactsuccessful interagency collaboration. Exceptional Children, 69(2), 195–210.
Knitzer, J. (1982). Unclaimed children: The failure of public responsibility to children and adolescents in need of mentalhealth services. Washington, DC: Children’s Defense Fund.
LeCompte, M., & Schensul, J. (1999a). The ethnographers toolkit (Vol. 5). Analyzing and interpreting ethnographic data.Walnut Creek, CA: AltaMira Press.
LeCompte, M., & Schensul, J. (1999b). The ethnographers toolkit (Vol. 1). Deigning and conducting ethnographic research.Walnut Creek, CA: AltaMira Press.
Mattessich, P. W., & Monsey, B. R. (1992). Collaboration: What makes it work. A review of research literature on factorsinfluencing successful collaboration. St. Paul, MN: Amherst H. Wilder Foundation.
Miles, M.B., & Huberman, A.M. (1994). Qualitative data analysis (2nd ed.). Thousand Oaks, CA: Sage Publications.National Institute of Mental Health. (1983). Program announcement: Child and Adolescent Service System Program.
Rockville, MD: Author.Paine-Andrews, A., Fisher, J. L., Patton, J. B., Fawcett, S. B., Williams, E. L., Lewis, R. K., & Harris, K. J. (2002). Analyzing
the contribution of community change to population health outcomes in an adolescent pregnancy prevention initiative.Health Education & Behavior, 29(2), 183–193. doi: 10.1177/109019810202900204
Paulson, R., Fixen, D., & Friedman, R. M. (2004). An analysis of implementation of systems of care at fourteen CMHS grantcommunities. Tampa, FL: Louis de la Parte Florida Mental Health Institute, University of South Florida.
Pfeiffer, S. I., & Cundari, L. (2000). Interagency collaboration: Recurring obstacles and some possible solutions. SpecialServices in the Schools, 15(1), 109–123. doi: 10.1300/J008v15n01_06
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014

432 HODGES ET AL.
President’s New Freedom Commission on Mental Health. (2003). Achieving the promise: Transforming mental health carein america, final report (Pub. No. SMA-03-3832). Rockville, MD: U.S. Department of Health and Human Services.
Prince, J., & Austin, M. J. (2005). Inter-agency collaboration in child welfare and child mental health systems. Social Workin Mental Health, 4(1), 1–16. doi: 10.1300/J200v04n01_01
Public Law 88–164 (1963).Public Law 102–321 STAT 347 (July 10, 1992).Saxe, E. L., & Hallfors, C. D. (1997). Think globally, act locally: Assessing the impact of community-based substance abuse
prevention. Evaluation and Program Planning, 20(3), 357–366. doi: 10.1016/S0149-7189(97)00015-3Silverman, M., Ricci, E. M., & Gunter, M. J. (1990). Strategies for increasing the rigor of qualitative methods in evaluation
of health care programs. Evaluation Review, 14, 57–74. doi: 10.1177/0193841X9001400104Stroul, B. A., & Friedman, R. M. (1986). A system of care for severely emotionally disturbed children & youth. Washington,
DC: CASSP Technical Assistance Center, Georgetown University Child Development Center.U.S. Department of Health and Human Services (USDHHS). (2002). Cooperative Agreements for the Comprehensive
Community Mental Health Services for Children and Their Families Program Guidance for Applicants (GFA) No.SM-02-002. Washington, DC: Substance Abuse and Mental Health Services Administration Center for Mental HealthServices.
U.S. Department of Health and Human Services (USDHHS). (2009). Cooperative agreements for the ComprehensiveCommunity Mental Health Services for Children and their Families Request for Applications (RFA). (SM-09-002).Washington, DC: Substance Abuse and Mental Health Services Administration, Center for Mental Health Services.
U.S. Public Health Service. (2000). Report of the Surgeon General’s Conference on Children’s Mental Health: A NationalAction Agenda. Washington, DC: U.S. Department of Health and Human Services.
Vinson, N. B., Brannan, A. M., Baughman, L. N., Wilce, M., & Gawron, T. (2001). The System-of-Care Model:Implementation in twenty-seven communities. Journal of Emotional and Behavioral Disorders, 9(1), 30–42.
Walter, U. M., & Petr, C. G. (2000). A template for family-centered interagency collaboration. Families in Society, 81(5),494–503. doi: 10.1606/1044-3894.1051
Zakocs, R. C., & Edwards, E. M. (2006). What explains community coalition effectiveness?: A review of the literature.American Journal of Preventive Medicine, 30(4), 351–361. doi: 10.1016/j.amepre.2005.12.004.
Dow
nloa
ded
by [
Uni
vers
ity o
f H
aifa
Lib
rary
] at
00:
38 0
2 N
ovem
ber
2014