Embed Size (px)
Citation preview

S369
Author Disclosure: A. Mahadevan, None; C.A. Reddy, None; P.A. Kupelian, None; E.A. Klein, None.
Proceedings of the 49th Annual ASTRO Meeting
2298 Whole Prostate to 75.6 With Concurrent IMRT Boost to 95 Gray for Biopsy Proven, MRI Defined
Dominant Intraprostatic Lesions: Early Results of a Phase I NCI StudyA. K. Singh, P. Guion, N. Sears-Crouse, K. Ullman, S. Smith, P. S. Albert, P. Choyke, B. Wood, H. Ning
National Cancer Institute, Bethesda, MD
Purpose/Objective(s): To assess the feasibility and toxicity, using IMRT, of selective intra-prostatic dose escalation to biopsyproven dominant lesions visible on MRI.
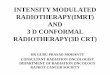
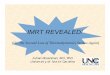
Materials/Methods: Patients with localized prostate cancer, low risk of lymph node metastases, and an MRI abnormality wereeligible. All patients underwent a MRI guided biopsy procedure to document the presence of prostate cancer at the location ofthe MRI abnormality. Gold fiducial markers were also placed. Approximately one week later, with fiducials in place, patients un-derwent another MRI scan which was fused with the treatment planning CT scan. This fused MRI scan was used to delineate theregion of the biopsy proven intraprostatic lesion. A 3 mm expansion was performed on this intraprostatic lesion, defined as a sep-arate volume within the prostate. The lesion +3 mm received 95 Gray (Gy) while the remainder of the prostate +7 mm received 75.6Gy in 1.8 Gy daily fractions. Daily port films verified that seed position was within 3 mm of the planned location. The maximumpoint dose to rectum and bladder was limited to 80 Gy.
Results: Two patients were treated. Follow-up was 12 and 6 months. The first patient had a single intraprostatic lesion. The secondpatient had 2 intraprostatic lesions. All three intraprostatic lesions, with margin, were successfully targeted and treated to 95 Gy.Both patients experienced acute RTOG Grade 2 GI toxicity and Grade 2 urinary toxicity. These symptoms completely resolved by3 months. No late toxicity was observed (Figures).

S370 I. J. Radiation Oncology d Biology d Physics Volume 69, Number 3, Supplement, 2007
Conclusions: These early results demonstrate the feasibility using IMRT for selective intra-prostatic dose escalation to biopsyproven dominant lesions visible on MRI. The treatment was well tolerated.
Author Disclosure: A.K. Singh, None; P. Guion, None; N. Sears-Crouse, None; K. Ullman, None; S. Smith, None; P.S. Albert,None; P. Choyke, None; B. Wood, None; H. Ning, None.
2299 The Effect of Family History on Outcome in Patients Treated With Low-Dose Rate Brachytherapy for
Clinically Localized Prostate CancerC. A. Peters, N. N. Stone, J. A. Cesaretti, R. G. Stock
Mount Sinai School of Medicine, New York, NY
Purpose/Objective(s): There is conflicting data regarding the outcome of patients harboring a family history of prostate cancertreated with external beam radiotherapy but no data on patients treated with brachytherapy. The purpose of this study was to de-termine the impact of a known family history of prostate cancer on the biochemical control rate of localized prostate cancer treatedwith low-dose rate brachytherapy.