Embed Size (px)
Citation preview

M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 8 3 6 – 8 4 4
Ava i l ab l e on l i ne a t www.sc i enced i r ec t . com
Metabolismwww.metabo l i sm jou rna l . com
Whole-body glucose oxidation rate during prolonged exercisein type 1 diabetic patients under usual life conditions
Mario Geata, Giuliana Stel a, Stefano Posera, Caterina Driussi a, Elisabetta Stennerb,Maria Pia Francescatoa,⁎a Department of Medical and Biological Sciences, University of Udine, 33100-Udine, Italyb Department of Laboratory Medicine, A.O.U., Ospedali Riuniti di Trieste, 34100-Trieste, Italy
A R T I C L E I N F O
Abbreviations: CGM, Continuous Glucosehormone; HR, Heart Rate; HRmax, TheoreticalHRtarget, Target heart rate during the trials; IUV̇CO2, Carbon dioxide production; V̇O2, Oxyg⁎ Corresponding author. Tel.: +39 0432 494336
E-mail address: maria.francescato@uniud
0026-0495/$ – see front matter © 2013 Elsevihttp://dx.doi.org/10.1016/j.metabol.2013.01.00
A B S T R A C T
Article history:Received 20 July 2012Accepted 1 January 2013
Objective. Fuel oxidation during exercise was studied in type 1 insulin-dependent (T1DM)patients mainly under quite constant insulin and glycemia; these protocols, however, likelydo not reflect patients’ usual metabolic conditions. The glucose oxidation rate (GLUox) inT1DM patients under usual life conditions was thus investigated during prolonged exercise(3-h) and its behavior was described mathematically.
Materials/Methods. Whole-body GLUox was determined in eight T1DM patients (4/8 M;aged 35–59 years) and eightwell-matchedhealthy subjects. Venous bloodwas drawnprior toand every 30 min until the end of exercise; glycemia, insulin, cortisol, and growth hormoneconcentrations were determined. Oxygen consumption, carbon dioxide production, andventilation were measured at rest and thereafter every 30 min of the exercise. To preventhypoglycemia, patients were given fruit fudge (93% sucrose) prior to / during exercise.
Results. Insulin concentration and glycemia were significantly higher in patients acrossthe entire exercise period (group effect, p<0.001 for both). GLUox decreased significantlywith increasing exercise duration (time effect, p<0.001), but no significant difference wasdetected between the two groups (group effect, p=NS). GLUox, expressed as the percentageof the starting value, was described by an exponential function showing a time constant of90 min (n=96; mean corrected R2=0.666).
Conclusions. GLUox in T1DM patients was not significantly different from the rateobserved in the control subjects. The function describing the time course of GLUox may beuseful to correct an estimated GLUox for the duration of exercise and help T1DM patientsavoiding exercise-induced glycemic imbalances.
© 2013 Elsevier Inc. All rights reserved.
Keywords:MetabolismGlycemiaIndirect calorimetryCarbohydrates
1. Introduction
Regular moderate-intensity physical activity is stronglyrecommended in patients suffering from type 1 insulin-
Monitoring device; CHOmaximal heart rate calcu, Insulin Units; RER, Respen consumption.; fax: +39 0432 494301..it (M.P. Francescato).
er Inc. All rights reserved4
dependent diabetes (T1DM) because of its numerous benefi-cial effects [1,2]. In particular, exercise has protective effectsagainst several cardiovascular risk factors [3–5], improvesinsulin sensitivity [6,7], and, together with diet and insulin
, Carbohydrates; GLUox, Glucose oxidation rate; hGH, Growthlated as 220 − age (expressed in years); HRrest, Resting heart rate;iratory exchange ratio; T1DM, Type 1 insulin-dependent diabetes;
.

Table 1 – Characteristics of the study groups.
837M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 8 3 6 – 8 4 4
therapy, it may help patients achieve and maintain a bettermetabolic control [1,8]. Furthermore, exercise can enhancepsychological well-being by increasing self-esteem and qual-ity of life [9].
However, fear of exercise-induced hypoglycemia oftendiscourages T1DM patients from regular physical activities[10,11]. Several strategies have been proposed to counter anexcessive exercise-induced fall of glycemia, especially duringmoderate intensity exercise, with the more recent one beingthe performance of intermittent high-intensity exercise [12–15] or the association with a single bout of resistance exercise[16]. The most commonly suggested countermeasure tooppose the exercise-induced fall of glycemia, however, isadditional glucose ingestion [17–22], especially when exerciseis spontaneous and not planned in advance [23,24]. Never-theless, current guidelines to minimize the risk of early onsetof exercise-related glycemic imbalances in T1DM patientshave been mainly drawn on the basis of short durationexercises (up to 60 min) [20,25–34]. In contrast, several outdoorleisure time physical activities (e.g., hiking, hill walking,biking, cross-country skiing), although light to moderate inintensity, tend to be prolonged in time.
Our workgroup has recently proposed an algorithm [21,35],which estimates the amount of carbohydrates (CHO) requiredby a T1DM patient to minimize the risk of exercise-inducedglycemic imbalances. The keystone of the algorithm is theestimate of the amount of CHO oxidized during the effort onthe basis of heart rate (HR), taken as an index of exerciseintensity [36]. The fuel oxidation rates during exercise werestudied in T1DM patients mainly under constant insulininfusion rate and quite constant glycemia [14,37–40]. Un-doubtedly, these experimental protocols allow to carefullycontrol several parameters that are likely to affect metabo-lism. However, exercise metabolism under patients’ usual lifeconditions (i.e., insulin doses and orally administered CHO) isless studied [36,41], particularly during prolonged exercises. Inaddition, although a time-dependent decrease in the whole-body CHO oxidation rate has been observed in healthy people[42–50], no mathematical equations have ever been proposedto describe this behavior.
The present study thus aimed at investigating the timecourse of whole-body CHO oxidation rate during prolonged(3-h) exercise in a group of type 1 insulin-dependent patientsunder usual life conditions. In addition, a comparison withthe time course of CHO oxidation rate in well-matchedhealthy controls was also performed. The secondary aim ofthe study was to mathematically describe the behavior ofglucose oxidation rate (GLUox) as a function of exerciseduration. This function might be introduced in the algorithmproposed by our workgroup [21,35], thus enhancing itsperformance for prolonged exercises.
Diabetic Patients Control Subjects
Age (years) 45±9 42±12Body mass (kg) 71.6±14.5 73.0±12.7Stature (m) 1.69±0.09 1.73±0.05Body Mass Index (kg/m2) 25.0±3.2 24.3±3.4Illness duration (years) 27.9±15.3 –HbA1c (%) 7.2±1.2 5.9±0.4 ⁎
⁎ Significantly lower than the values of T1DM patients (p<0.05).
2. Methods
2.1. Subjects
Eight type 1 diabetic patients (4 men and 4 women; aged 35 to59 years, and diagnosed with diabetes since 5 to 49 years)volunteered to be subjects. A control group of 8 well-matched
healthy subjects (4 males and 4 females) was also studied. Allthe subjects practiced aerobic physical exercise regularly, butnone was highly trained. We were aware of the fact thatwomen rely more on fat oxidation than men [51–54] and thatthe hormonal status in females might influence substrateutilization [55–57]. It was thus expected that the heterogeneityin the two groups of volunteers may introduce some noise inthe results. The patients were accepted if they were notaffected by other chronic diseases and had no evidence ofdiabetes complications contraindicating physical activity. Thephysical and clinical characteristics of the two study groupsare summarized in Table 1.
All the participants were informed of the nature, purpose,and possible risks involved in the study before giving theirvoluntary written consent to participate in this study. Thestudy was approved by the Ethical Committee of theUniversity of Udine and was conducted according to theprinciples expressed in the Declaration of Helsinki.
2.2. Experimental protocol
All the volunteers were asked to refrain from strenuousphysical activity, alcohol, and caffeine during the 24-h periodpreceding the experimental session. In addition, the patientswere advised to maintain their usual diet and insulin regimenand carefully control their blood glucose levels according tothe self-management procedures to avoid the occurrence ofhypoglycemic events.
All volunteers arrived at the laboratory early in themorning. At 7:30 AM, the T1DM patients injected themselveswith their usual insulin dose (0.08±0.04 IU·kg−1) subcutane-ously in the abdomen wall and consumed their usualbreakfast, which included 0.6±0.2 g·kg−1 of CHO in the formof starch. Immediately thereafter, a care-provider inserted thesensor of a continuous glucose monitoring device (CGM;Paradigm Revel 523, MedTronic Mini-Med, Northridge, CA,USA) in the patients' abdomen wall paying attention to avoidlocations that are constrained by clothing or accessories, orare subjected to vigorous movement during exercise. Inaccordance with the manufacturer's instructions for use, 2 hafter the sensorwas installed (and before the start of exercise),a capillary glucose valuewas uploaded for calibration. Healthycontrol subjects had only breakfast at 7:30 AM, whichincluded their usual average CHO intake (~0.7 g·kg−1). There-after, all participants rested in an armchair.
About 45 min prior to the start of the exercise, thevolunteers were equipped with the belt of a heart rate

838 M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 8 3 6 – 8 4 4
monitoring system (Polar Electro, Kempele, Finland) toacquire HR values every 15 s throughout the whole exercise.Immediately thereafter, an indwelling catheter was insertedinto a forearm vein of the subjects; patency of the catheterwas maintained by intermittent flushing with saline.
To counter an excessive fall of glycemia, the algorithmrecently proposed by our workgroup was applied every half anhour of exercise [21,35], and the estimated amounts of CHOwere administered to the patients in the form of fruit fudge(Perugina, Italy; 93% sucrose). In brief, the algorithm firstestimates the overall amount of glucose burned on the basisof the expected HR and exercise duration (in our case 30 minfor all periods). This quantity was then arbitrarily reduced by8%, 16%, 23%, 30% and 34% [46] to calculate the CHOrequirement for the second to the sixth half-of-an-hourexercise period, respectively. According to the algorithm, theamount of CHO required to minimize the risk of hypoglyce-mia is a percentage of the overall amount of glucose burned,which depends on insulin concentration, which, in turn, isestimated on the basis of the type and dose of administeredinsulin and the time elapsed from the injection. Finally, thealgorithm takes into account the possible excess/lack ofglucose solved in the body by considering actual glycemia atthe start of the exercise. Accordingly, glycemia as measuredby means of the reactive strips before the start of the trial andat the end of every 30 min duration of exercise was used. Thepatients were thus given 0.14±0.11 g · kg−1 (range 0.0–0.4 g·kg−1) of sucrose in the form of fruit fudge before thestart of the exercise. Thereafter, additional amounts of thesame fruit fudge were administered to patients for each of thefollowing half an hour of exercise periods. In addition,whenever glycemia was below 5.0 mmol ·L−1, to rapidlyrestore a safe blood glucose level, 10 mL of 33% w/v glucosesolution was infused. Overall, the patients received anamount of sucrose and/or infused glucose in the range of0.0–0.4 g·kg−1 every half an hour of exercise. No CHO weregiven to the control subjects. All volunteers were allowed todrink water ad libitum.
All the volunteers performed a 3-h (from 10:00 AM to1:00 PM) constant HR exercise on a treadmill (Saturn, H-PCosmos, Traunstein, Germany). The target HR was keptconstant by automatically adjusting the speed and/or slope.To minimize dizziness due to prolonged treadmill exercise, a5-min rest was allowed at the end of each hour of exercise.Work intensity was set to 30% of individual HR reserve(HRtarget=HRrest+(HRmax − HRrest) ·0.3), corresponding to anaverage target HR of 102±4 bpm, which reasonably guaran-teed that all the subjects could complete the task. In addition,the risk of exercise-related hypoglycemia in patients wouldprobably be increased by higher work intensities.
Oxygen consumption, carbon dioxide production, andventilation were measured breath-by-breath by means of ametabolic unit (Quak b2, Cosmed, Rome, Italy) at rest, beforethe start of the trial, and during the 10 central min of each halfof an hour period of the exercise.
Venous blood (~5 mL) was drawn 30 min prior to and atsubsequent 30 min intervals until the end of the exercise. Indiabetic subjects, a drop of blood collected was used toimmediately test glycemia using reactive strips (ContourLink,Bayer Healthcare Diabetes Division); in addition, whenever
the glucose level displayed on the receiver of the CGM wasfalling quickly, the same strips were used to further testglycemia from finger-stick capillary blood.
At the end of the exercises, the healthy control subjectswere free to leave the laboratory. In contrast, to minimize therisk of late-onset hypoglycemic events, the patients were keptunder supervision of a physician trained in diabetes and anexpert nurse until the following morning. This time intervalwas considered sufficient to minimize the risk of severe late-onset hypoglycemic events. Indeed, it is known that even ifthere is evidence that physical activity can affect insulinsensitivity up to 48 h [58], inwell-insulinized patients, the pre-exercise muscle glycogen level is restored to about 91% after12 h recovery [59]. During their recovery period, our patientsreceived their usual insulin doses and meals for lunch anddinner (at 1:30 PM and 7:30 PM, respectively). They wereallowed to sit quietly in an armchair (or lie in bed) whiletheir glucose level was tested using reactive strips every houruntil bedtime and, thereafter, at least at 2:00 AM and 5:00 AM.In addition, whenever the CGM readings showed glucoselevels below 5.0 mmol·L−1 with a decreasing pattern, thevalue was checked by a fingerstick capillary measurement,and the infusion of a 5% glucose solutionwas started if the lowglycemic value was confirmed. At 7:00 AM, the sensor of CGMwas removed. All the glycemic levels were recorded onappropriate forms, and its analysis confirmed that theoccurrence of late-onset hypoglycemia after the trials wasactually avoided in all cases.
2.3. Analyses
A drop of the blood drawn was used to determine lactateconcentration by means of reactive strips (Lactate Pro LT-1710, Arkray, Kyoto, Japan) and to test glycemia in thepatients (ContourLink, Bayer Healthcare Diabetes Division).The remaining blood was divided into a 2-mL Vacutainertube (#368920) containing a glycolysis inhibitor (4 mg ofkalium oxalate+5 mg of sodium fluoride) and a 3.5-mLVacutainer SST™ II advance tube (#368965) with gel andclot activator. Immediately thereafter, both the tubes weregently inverted and stored at +4 °C until the hospitallaboratory centrifuged the samples to separate serum andperform the measurements.
Plasma glucose concentration was determined by applyinga hexokinase-based methodology (Olympus Diagnostic Sys-tems AU2700), and our determined coefficient of analyticalvariation was <2% in the range of 3.27–11.67 mmol ·L−1.Cortisol and growth hormone (hGH) were measured usingthe Siemens Healthcare Diagnostics (Deerfield, IL, USA)automated immunoassay systems (ADVIA Centaur, andImmulite 2000, respectively) by employing original reagentsfor both determinations; the coefficient of analytical variationwas <5% in the range of 155–1025 nmol·L−1 for cortisol and<2% in the range of 2.6–17 ng·mL−1 for hGH. Insulin concen-trations were determined by means of the Beckman Access 2Automated Immunoassay system (Beckman Coulter, Fuller-ton, CA); coefficient of analytical variation was <6% in therange of 73.9–327.5 pmol·L−1. This insulin assay was chosenbecause itmeasures all the relevant insulin analogs showing across-reactivity of about 80% [60].

839M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 8 3 6 – 8 4 4
2.4. Calculations
HR data were downloaded to a personal computer andaveraged offline over 15-min periods.
Oxygen consumption (V̇O2) and carbon dioxide production(V̇CO2) data were averaged over the corresponding 10-minrecording periods. These averaged data allowed us to calculatethe respiratory quotient, assumed to be equal to the respira-tory exchange ratio (RER). Hence, by assuming that proteins donot contribute to any significant extent to the energyproduction during exercise [61,62] the whole-body glucose(GLUox) and fat oxidation rates as well as the total energyexpenditure were estimated by applying commonly usedequations [63]. The amount of energy yield by the oxidationof CHO was subsequently computed by assuming an energypotential of 3.95 kcal ·g−1 [61].
Finally, the CHO oxidation rates observed in the diabeticsubjects, expressed as the percentage of the first value (i.e.,the value during the 10–20 min exercise period), weremodeled as follows:
Perc tð Þ ¼ CHO 0ð Þ−ΔCHO⋅ 1−e−tτ
� �
where CHO(0) is the estimated percentage GLUox at the actualstart of exercise, ΔCHO is the percentage decrease in theoxidation rate at the asymptote, and τ is the time constant ofthe time course (expressed in min).
2.5. Statistical analysis
The data were analyzed using standard statistical methods(Systat vs. 11). Two-way analysis of variance with repeatedmeasures design (MANOVA, with study group and gender asbetween-subjects factor and time as within-subjects factor)was applied, followed by specific contrasts when appropriate.To appropriately use the repeated measure analysis ofvariance, Mauchly's test was used to check if the sphericityassumption appeared to be violated, i.e. if the variances of thedifferences between all possible pairs of groups were notequal. In instances where Mauchly's test was significant,modification had to be made to the degrees of freedom. TheGreenhouse–Geisser ε provides a measure of departure fromsphericity, and can be used to adjust the degrees of freedom.
Table 2 – Physiological characteristics of the two study groups
Rest 15 min 45 mi
Diabetic PatientsHeart rate (bpm) 72.5±6.8 101.8±7.0 101.5±4Progression speed (m·s−1) – 1.4±0.2 1.4±0V̇O2 (mL·min−1·kg−1) 4.0±0.6 13.9±3.3 13.5±3V̇CO2 (mL·min−1·kg−1) 3.5±0.5 12.3±3.0 11.7±2RER 0.84±0.03 0.89±0.03 0.87±0
Control SubjectsHeart rate (bpm) 73.0±3.6 102.3±3.7 101.9±4Progression speed (m·s−1) – 1.5±0.2 1.5±0V̇O2 (mL·min−1·kg−1) 4.2±0.5 14.6±3.0 14.1±2V̇CO2 (mL·min−1·kg−1) 3.8±0.5 13.0±2.9 12.1±2RER 0.86±0.04 0.89±0.03 0.86±0
In fact, when sphericity is exactly met, then epsilon will beexactly 1, and if sphericity is violated, then epsilon will be<1;the further the epsilon is from 1, the worse is the violation. A pvalue of<0.05 was assumed as statistically significant. Dataare expressed as means±SD.
3. Results
The respiratory data at rest and during the 3-h exercise forboth T1DM patients and healthy volunteers are summarizedin Table 2. The actual HR during the exercises was notsignificantly different between T1DM patients and healthycontrols (group effect, F=0.028, p=NS), or between genders(gender effect, F=2.803, p=NS), amounting to an average of101±5 bpm. It reached the target value in a few minutes, andthereafter remained stable over time in both the groups (timeeffect, F=1.460, p=NS; group × time effect, F=0.566, p=NS).Progression speed was not significantly different betweenT1DM patients and controls (group effect, F=1.740, p=NS), butwas significantly lower in women, when compared with men(gender effect, F=4.763, p<0.05); it decreased slightly duringthe exercises from 1.5 ± 0.2 to 1.4 ± 0.2 m·s−1, even if thedecline was not statistically significant (time effect, F=1.513,p=NS). Oxygen consumption (V̇O2), expressed per unit bodymass, was not significantly different between diabetic pa-tients and healthy controls (group effect, F=0.146, p=NS;group × time effect, F=1.814, p=NS), but was significantlylower in women, when compared with men (gender effect, F=8.423, p<0.05).V̇O2 decreased slightly during the 3-h exercisefrom 14.3±3.1 mL·min−1 ·kg−1 to 12.8±3.6 mL·min−1 ·kg−1
(time effect, F=4.320, p<0.01). The overall energy expenditurefor 3-h exercise was not significantly different between theT1DM patients and controls (un-paired t-test, P=NS), amount-ing to 3238±970 kJ and 3628±974 kJ in patients and healthycontrols, respectively. The overall amounts of sucrose andinfused glucose administered to patients remained constantover time (time effect, F=0.669, p=NS), amounting to anaverage of 0.13±0.11 g·kg−1.
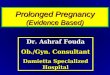
GLUox, expressed per unit bodymass, is illustrated in Fig. 1as a function of exercise duration. GLUox decreased signifi-cantly with increasing exercise duration (time effect, F=52.224, p<0.001), but no significant difference could be
at rest and during the 3 h walks.
n 75 min 105 min 135 min 165 min
.9 100.6±8.3 101.9±6.9 100.7±6.4 101.3±4.3
.1 1.4±0.2 1.4±0.2 1.4±0.1 1.4±0.2
.3 12.9±3.3 12.9±3.4 12.8±3.5 13.2±4.1
.8 11.0±2.8 10.9±3.0 10.7±2.9 10.8±3.3
.03 0.85±0.03 0.84±0.03 0.83±0.03 0.82±0.03
.5 100.3±1.4 102.3±3.6 102.5±3.4 102.1±2.6
.1 1.5±0.1 1.5±0.2 1.5±0.1 1.4±0.2
.9 14.1±3.6 13.5±2.7 13.7±2.9 12.3±3.2
.8 11.9±3.2 11.1±2.4 11.1±2.6 10.1±2.8
.03 0.84±0.02 0.82±0.03 0.81±0.03 0.82±0.03
Fig. 1 – Time course of the glucose oxidation rate in the T1DMpatients (full dots) and in the healthy control subjects (opendots). Glucose oxidation rate decreased significantly withincreasing exercise duration (p<0.001), but the two groups ofvolunteers were not significantly different.
840 M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 8 3 6 – 8 4 4
detected between T1DM patients and controls (group effect,F=0.007, p=NS; group × time effect, F=1.571, p=NS). Further-more, a tendency towards a lower GLUox in women was
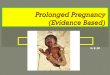
Fig. 2 – Time course of the insulin concentration (panel A) inthe two groups of volunteers. Insulin concentration decreasedsignificantly during the trial in both groups (p<0.005) but wassignificantly higher in patients across thewhole experimentalperiod (p<0.001). Time course of the blood glucose level (panelB) in the two groups of volunteers. Glycemia was significantlyhigher in the diabetic patients (p<0.005); it decreased signif-icantly during the exercises (p<0.05), following a differentbehavior in the two groups (p<0.01). In both panels: full dots=T1DM patients; open dots=healthy control subjects.
observed (gender effect, F=3.589, p=0.083). The percentageenergy yielded by glucose oxidation during the 3-h exercisewas not significantly different between T1DM patients andhealthy volunteers (group effect, F=0.721, p=NS) or betweenthe genders (gender effect, F=0.002, p=NS). Overall, thepercentage energy from glucose oxidation decreased from67.0%±8.8% during the first half an hour to 42.7%±10.9%during the last half an hour of exercise (time effect, F=55.182,p<0.001), showing a similar behavior in patients and controls(group × time effect, F=1.535, p=NS).
Fig. 2A illustrates the average insulin concentrations(pmol·L−1) of diabetic patients and controls during the trials.Insulin concentrationwas significantly higher in patients acrossthe whole experimental period (group effect, F=216.1, p<0.001).In both the groups, the insulin concentration decreasedsignificantly during the trial (time effect, F=8.209, p<0.005).
Glycemia (Fig. 2B) was significantly higher in the patients(group effect, F=16.10, p<0.005), but decreased significantlyduring the exercises (time effect, F=4.700, p<0.05), following adifferent behavior in the two groups (group × time effect, F=6.443, p<0.01). The patients’ glycemia decreased on average
Fig. 3 – Time course of the concentration of growth hormone(hGH; panel A) in the two groups of volunteers. Growthhormone concentration showed a similar behavior in the twogroups (group effect, F=1.038, p=NS; group × time effect, F=1.873, p=NS), peak values being observed after the first hour ofexercise (difference contrast, F=6.688, p<0.05). Time course ofthe concentrationof cortisol in blood (panel B) in the twogroupsof volunteers. Cortisol concentration changed throughout the3-h exercise (p<0.001), but did not show any significantdifference between the two study groups. In both panels: fulldots=T1DM patients; open dots=healthy control subjects.

Fig. 4 – Individual carbohydrate oxidation rates observed inthe diabetic subjects, expressed as percentage of the firstvalue (corresponding to the oxidation rate during the 10–20 min exercise period) are illustrated as a function ofexercise duration. The exponential equation describing thedata is as follows:
Perc tð Þ ¼ 109:2−62:2� ð1−e−t90Þ
(n=96; mean corrected R2=0.666).
841M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 8 3 6 – 8 4 4
from 10.5±4.5 mmol·L−1 30 min prior to the start of exerciseto 6.3±1.5 mmol · L−1 at the very end of the exercises;conversely, healthy volunteers showed a rather stable valueof about 4.7±0.5 mmol·L−1.
Lactate concentration slightly decreased during the exer-cises (time effect, F=7.867, p<0.001) from 1.15±0.24 mmol·L−1
at the start of the exercises to 0.91±0.17 mmol·L−1 at the endof the exercises, without any significant difference betweenthe two groups of volunteers (group effect, F=3.401, p=NS;group × time effect, F=0.494, p=NS).
The concentration of growth hormone (Fig. 3A) showeda similar behavior in the two groups (group effect, F=1.038,p=NS; group × time effect, F=1.873, p=NS), increasingsignificantly during the first hour of exercise (differencecontrast, F=6.688, p<0.05). On the other hand, cortisolconcentration (Fig. 3B) was not significantly different betweenthe two study groups (group effect, F=0.063, p=NS); it changedduring the 3-h exercise (time effect, F=6.634, p<0.001),without any difference between patients and healthy controls(time × group effect, F=0.582, p=NS).
Individual GLUox values for both the groups, expressed aspercentage of the appropriate first value (i.e., the value of the10–20 min exercise period was taken as 100%), are illustratedin Fig. 4 as a function of exercise duration. The fittingprocedure yielded the following exponential equation:
Perc tð Þ ¼ 109:2−62:2⋅ 1−e−t90
� �
(n=96; mean corrected R2=0.666).
4. Discussion
The present study showed that during prolonged exercise, thetime course of GLUox in T1DMpatients exercising under usual
therapy and diet was not significantly different from theoxidation rates observed in the control subjects. Despite theadministration of fruit fudge required by T1DM patients toavoid an excessive fall of glycemia, a very similar time-dependent decrease in GLUoxwas observed in the two groups,which is in agreement with previous studies [64,65]. SimilarGLUox values (and the contribution to total energy yield) werealso observed between the controls and diabetic patientsduring shorter aerobic exercises (≤ 1-h duration) [31,41].Indeed, increased extracellular glucose availability, does nottranslate into increased intracellular GLUox [37,40]. At vari-ance, T1DM patients exercising under high insulin infusionrates showed a slightly increased whole-body CHO oxidationrate [39]. Nevertheless, patients exercising under four signif-icantly different insulin concentrations behaved metabolical-ly similar to healthy people, suggesting that GLUox is notdirectly related to blood insulin concentration [66].
In response to the prolonged exercise, T1DM patientsshowed a higher hGH stimulation (though not significant),when compared with healthy control subjects, with peakvalues observed after about 1 h of exercise. Despite the lessstable glycemia, the average increase in hGH concentration isfound to be in agreement with previous observations [67]. Theadministration of an oral glucose bolus before exerciseresulted in a blunted hGH response in both healthy volunteersand T1DM patients [68]. In the present investigation, fruitfudge was administered to patients prior to / during theexercises to counter an excessive fall of glycemia, whichmight have reduced the counter-regulatory response of hGH.Some “noise” might have been introduced in our results,which, however, reflect the usual life conditions of patients.
No significant difference between T1DM patients andhealthy controls was found for cortisol concentration. Theobserved pattern of cortisol concentration is in agreementwith the known circadian rhythm with peak levels notedearly in the morning [69,70]. In addition, it also suggests thatthe exercise intensity chosen for the present study did notinduce an important stress in the body. In fact, in view of theprolonged duration of the exercise (3-h), the selectedprogression speed was slightly lower than the mean briskwalking speed observed in a group of recreational walkers[71]. Under hyperglycemic conditions, Jenni et al. [37]observed similar cortisol levels at the start and end ofexercises performed by a group of T1DM patients. Theauthors claimed a blunted cortisol secretion to explain thehigher GLUox observed under hyperglycemia. Indeed, corti-sol, together with hGH, has been found to induce peripherallipolysis [72], which in turn may play a role in the shifttowards lipid oxidation. In agreement with previous results[65], T1DM patients of the present investigation showedsimilar GLUox, when compared with healthy volunteers,despite their higher blood glucose and insulin levels. It can behypothesized that the higher GLUox observed under hyper-glycemia by Jenni et al. [37] might be the consequence, atleast in part, of the higher insulin concentration maintainedduring their clamp procedures. The evidence of a higherGLUox in T1DM patients exercising under high insulin levels[39] supports this hypothesis.
The main strength of the current study is that the T1DMpatients were studied under their usual metabolic conditions,

842 M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 8 3 6 – 8 4 4
i.e. without changing either their insulin levels or clampingtheir glucose levels. In addition, in the present investigationHR was held constant throughout the exercises instead ofintensity, to mimic outdoor physical activities, during whichHR is the most commonly used index of exercise intensity.The automatic adjustments of progression speed during theexercises allowed us to achieve a constant HR throughout thetrials. As expected, GLUox decreased during exercise, due tothe combined effect of exercise duration and of the reducedprogression speed. However, even if progression speeddecreased slightly from the start to the end of the exercises,this change was not statistically significant, suggesting thatthe decrease in GLUox was mainly due to the exerciseduration effect. Considering all the above-mentioned condi-tions, we are confident that our experimental protocol yieldedresults that can be directly employed to draw concretesuggestions for T1DM patients to avoid excessive falls ofglycemia during exercise.
The present investigation is not without some limitations.Indeed, despite the fact that we were aware that women relymore on fat oxidation than men [51–54] and that substrateutilization in females is also influenced by the hormonalstatus [55–57], our study groups were composed of quitediverse subjects and no particular attention was paid to themenstrual cycle phase of women. The heterogeneity in therecruited volunteers might probably have introduced somenoise in the obtained results. Nevertheless, the percentageenergy yielded by glucose oxidation was not significantlydifferent between the genders, giving us confidence that theproposed mathematical description of the behavior of GLUoxis actually applicable in almost all conditions (e.g., indepen-dent of gender and the menstrual cycle phase). Finally, notracers were used to specifically depict the contribution of theendogenous glucose production [e.g., [14,37]] or of theexogenous GLUox [e.g., [41]] on the whole-body GLUox.However, the main purpose of the present investigation wasto study whole-body GLUox.
Our workgroup has recently developed an algorithm(ECRES; Exercise Carbohydrate Requirement Estimating Soft-ware) [21,35], which helps the T1DM patients to determine,on a patient- and situation-specific basis, the amount ofCHO that they need before and/or during moderate aerobicexercise to maintain blood glucose levels within therecommended range, i.e. 3.9–10.0 mmol·L−1 [73], thus min-imizing the risk of immediate exercise-induced glycemicimbalances. Of note, as a reduction in the premeal insulindose has been proposed to counter the risk of an excessiveexercise-induced fall of blood glucose [74,75], the algorithmhas been designed to also take into account occasionalchanges in the usual therapy, e.g., the reduced insulin dosesin anticipation of exercise. This strategy, however, oftendoes not exempt patients from a CHO supplement [18]. Thealgorithm is based on the observation that the amount ofCHO needed to prevent hypoglycemia is strictly related toinsulin concentration and represents a fraction of theoverall amount of glucose burned during the exercise [66].In turn, the overall amount of glucose oxidized during theeffort may be estimated on the basis of the expectedexercise intensity (defined by HR) [36]. This algorithmunfolds the prospect of a method to estimate the amount
of CHO required by a T1DM patient to minimize exercise-induced glycemic imbalances, given the overall amount ofglucose oxidized is correctly predicted. Nevertheless, to date,it has not been possible to estimate GLUox taking intoaccount the exercise duration as well, because no mathe-matical equations were available describing the time courseof the CHO oxidation rate during prolonged exercise. Thepresent investigation yields an exponential function de-scribing the behavior of GLUox, expressed as the percentageof the first value (i.e., the value of the 10–20 min exerciseperiod taken as 100%), as a function of exercise duration.Indeed, the relationship between GLUox and duration ofexercise could also be well described by other mathematicalfunctions, yielding very similar correlation coefficients.Nevertheless, an exponential description was chosen, hy-pothesizing that GLUox reaches a stable asymptotic valuefor very prolonged exercises. The proposed equation will beintroduced in the aforementioned algorithm [21], thusallowing to correct the estimated amount of glucose burnedduring exercise according to its duration, and consequentlyenhancing the performance of the algorithm for prolongedexercise conditions. In its current version, our algorithmseemed adequate for estimating the supplemental CHOrequired by a T1DM patient to avoid immediate exercise-induced glycemic imbalances in about 70% of the exercises,independent of the time of day when the activity wasperformed [21,35]. Several different implementations of thealgorithm can be foreseen, ranging from software imple-mentations for single patient's use to web-based solutions.The algorithm can also be easily integrated into manydifferent devices, such as training equipment or glucosemonitoring systems. Finally, a real-time version of thealgorithm, implemented on a portable device and designedto estimate in real time the residual supplemental CHO stillavailable during exercise on the basis of actual HR (acquiringdata similarly to the commercial HR monitors), will be avery intriguing device able to warn patients of the actualrisk of hypoglycemia during their physical activities. Thissolution may be of very simple use, liberating the patientsfrom the need of understanding in some detail themetabolic responses to exercise and allowing them to safelyenjoy the benefits of physical activity.
In conclusion, the present investigation provides evidencethat under usual life conditions, GLUox in T1DM patientsshows the same time-dependent decreases as those noted inhealthy people, and can be well described by an exponentialfunction. The proposed equation, introduced in the recentlydeveloped algorithm [21], will allow to correct the estimatedamount of glucose burned during exercise according to itsduration, thus enhancing the estimate of the amount of CHOrequired to avoid hypoglycemia.
Author contributions
GM andMPF designed the experiments, PS, CD and GM carriedout the experiments, SG and SE provided lab equipment andtest materials, all authors contributed to the data interpreta-tion, the writing of this manuscript was led by MPF, and allauthors approved the final manuscript.

843M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 8 3 6 – 8 4 4
Funding
Unconditioned financial support by Bayer Italia and by theFondazione Cassa di Risparmio di Gorizia allowed the study tobe carried out.
Acknowledgments
We gratefully thank all the volunteers who accepted toparticipate to the study.
Conflict of interest
None of the authors has conflicts of interest to declare.
R E F E R E N C E S
[1] American Diabetes Association. Physical activity/exerciseand diabetes. Diabetes Care 2004;27(S1):S58–62.
[2] Waden J, Forsblom C, Thorn LM, et al. Physical activity anddiabetes complications in patients with type 1 diabetes: theFinnish Diabetic Nephropathy (FinnDiane) Study. DiabetesCare 2008;31(2):230–2.
[3] Haider DG, Pleiner J, Francesconi M, et al. Exercise traininglowers plasma visfatin concentrations in patients with type 1diabetes. J Clin Endocrinol Metab 2006;91(11):4702–4.
[4] Laaksonen DE, Atalay M, Niskanen LK, et al. Aerobic exerciseand the lipid profile in type 1 diabetic men: a randomizedcontrolled trial. Med Sci Sports Exerc 2000;32(9):1541–8.
[5] Lehmann R, Kaplan V, Bingisser R, et al. Impact of physicalactivity on cardiovascular risk factors in IDDM. Diabetes Care1997;20(10):1603–11.
[6] Hawley JA. Exercise as a therapeutic intervention for theprevention and treatment of insulin resistance. DiabetesMetab Res Rev 2004;20(5):383–93.
[7] Stallknecht B, Larsen JJ, Mikines KJ, et al. Effect of training oninsulin sensitivity of glucose uptake and lipolysis in humanadipose tissue. Am J Physiol 2000;279(2):E376–85.
[8] Rowland T, Swadba LA, Biggs DE, et al. Glycemic control withphysical training in insulin-dependent diabetes mellitus. AmJ Dis Child 1985;139(3):307–10.
[9] Steppel JH, Horton ES. Exercise in the management of type 1diabetes mellitus. Rev Endocr Metab Disord 2003;4(4):355–60.
[10] Brazeau AS, Rabasa-Lhoret R, Strychar I, et al. Barriers tophysical activity among patients with type 1 diabetes.Diabetes Care 2008;31(11):2108–9.
[11] Zoppini G, Carlini M, Muggeo M. Self-reported exercise andquality of life in young type 1 diabetic subjects. Diabetes NutrMetab 2003;16:77–80.
[12] Bussau VA, Ferreira LD, Jones TW, et al. The 10-s maximalsprint. A novel approach to counter an exercise-mediated fallin glycemia in individuals with type 1 diabetes. Diabetes Care2006;29(3):601–6.
[13] Guelfi KJ, Jones TW, Fournier PA. New insights into managingthe risk of hypoglycaemia associated with intermittent high-intensity exercise in individuals with type 1 diabetesmellitus. Sports Med 2007;37(11):937–46.
[14] Guelfi KJ, Ratnam N, Smythe GA, et al. Effect of intermittenthigh-intensity compared with continuous moderate exerciseon glucose production and utilization in individuals with type
1 diabetes. Am J Physiol Endocrinol Metab 2007;292(3):E865–70.
[15] Dubé M-C, Lavoie C, Weisnagel SJ. Glucose or intermittenthigh-intensity exercise in glargine/glulisine users with T1DM.Med Sci Sports Exerc 2013;45(1):3–7.
[16] Yardley JE, Kenny GP, Perkins BA, et al. Effects of performingresistance exercise before versus after aerobic exercise onglycemia in type 1 diabetes. Diabetes Care 2012;35(4):669–75.
[17] Younk LM, Mikeladze M, Tate D, et al. Exercise-relatedhypoglycemia in diabetes mellitus. Expert Rev EndocrinolMetab 2011;6(1):93–108.
[18] Grimm JJ, Ybarra J, Berné C, et al. A new table for prevention ofhypoglycaemia during physical activity in type 1 diabeticpatients. Diabetes Metab 2004;30(5):465–70.
[19] Kemmer FW. Prevention of hypoglycemia during exercise intype I diabetes. Diabetes Care 1992;15(11):1732–5.
[20] Riddell MC, Bar-Or O, Ayub BV, et al. Glucose ingestionmatched with total carbohydrate utilization attenuateshypoglycemia during exercise in adolescents with IDDM. Int JSport Nutr Exerc Metab 1999;9(1):24–34.
[21] Francescato MP, Geat M, Accardo A, et al. Exercise andglycemic imbalances: a situation-specific estimate of glucosesupplement. Med Sci Sports Exerc 2011;43(1):2–11.
[22] Riddell MC, Milliken J. Preventing exercise-induced hypogly-cemia in type 1 diabetes using real-time continuous glucosemonitoring and a new carbohydrate intake algorithm: anobservational field study. Diabetes Technol Ther 2011;13(8):819–25.
[23] Dubé MC, Lavoie C, Galibois I, et al. Nutritional strategies toprevent hypoglycemia at exercise in diabetic adolescents.Med Sci Sports Exerc 2012;44(8):1427–32.
[24] Gallen I, Hume C, Lumb A. Fuelling the athlete with type 1diabetes. Diabetes Obes Metab 2011;13:130–6.
[25] Guelfi KJ, Jones BH, Fournier PA. Intermittent high-intensityexercise does not increase the risk of early postexercisehypoglycemia in individuals with type 1 diabetes. DiabetesCare 2005;28(2):416–8.
[26] Harmer AR, Chisholm DJ, McKenna MJ, et al. High-intensitytraining improves plasma glucose and acid–base regulationduring intermittent maximal exercise in type 1 diabetes.Diabetes Care 2007;30(5):1269–71.
[27] Tsalikian E, Kollman C, Tamborlane WB, et al. Prevention ofhypoglycemia during exercise in children with type 1diabetes by suspending basal insulin. Diabetes Care2006;29(10):2200–4.
[28] Soo K, Furler SM, Samaras K, et al. Glycemic responses toexercise in IDDM after simple and complex carbohydratesupplementation. Diabetes Care 1996;19(6):575–9.
[29] Perrone C, Laitano O, Meyer F. Effect of carbohydrateingestion on the glycemic response of type 1 diabeticadolescents during exercise. Diabetes Care 2005;28(10):2537–8.
[30] Iscoe KE, Riddell MC. Continuousmoderate-intensity exercisewith or without intermittent high-intensity work: effects onacute and late glycaemia in athletes with type 1 diabetesmellitus. Diabet Med 2011;28(7):824–32.
[31] Riddell MC, Bar-Or O, Mollidge-Horvat M, et al. Glucoseingestion and substrate utilization during exercise in boyswith IDDM. J Appl Physiol 2000;88:1239–46.
[32] Mauvais-Jarvis F, Sobngwi E, Porcher R, et al. Glucoseresponses to intense aerobic exercise in type 1 diabetes.Diabetes Care 2003;26(4):1316–7.
[33] Ruegemer JJ, Squires RW, Marsh HM, et al. Differencesbetween prebreakfast and late afternoon glycemic responsesto exercise in IDDM patients. Diabetes Care 1990;13:104–10.
[34] Rabasa-Lhoret R, Bourque J, Ducros F, et al. Guidelines forpremeal insulin dose reduction for postprandial exercise ofdifferent intensities and durations in type 1 diabetic subjects

844 M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 8 3 6 – 8 4 4
treated intensively with a basal-bolus insulin regimen(ultralente-Lispro). Diabetes Care 2001;24(4):625–30.
[35] Francescato MP, Carrato S. Management of exercise-inducedglycemic imbalances in type 1 diabetes. Curr Diabetes Rev2011;7(4):253–63.
[36] Francescato MP, Cattin L, Geat M, et al. Glucose pulse: asimple method to estimate the amount of glucose oxidizedduring exercise in type 1 diabetic patients. Diabetes Care2005;28(8):2028–30.
[37] Jenni S, Oetliker C, Allemann S, et al. Fuel metabolism duringexercise in euglycaemia and hyperglycaemia in patients withtype 1 diabetes mellitus—a prospective single-blinded ran-domised crossover trial. Diabetologia 2008;51:1457–65.
[38] Raguso CA, Coggan AR, Gastaldelli A, et al. Lipid andcarbohydrate metabolism in IDDM during moderate andintense exercise. Diabetes 1995;44:1066–74.
[39] Chokkalingam K, TzinTzas K, Norton L, et al. Exercise underhyperinsulinaemic conditions increases whole-body glucosedisposal without affecting glycogen utilisation in type 1diabetes. Diabetologia 2007;50(2):414–21.
[40] Stettler C, Jenni S, Allemann S, et al. Exercise capacity insubjects with type 1 diabetes mellitus in eu- and hypergly-caemia. Diabetes Metab Res Rev 2006;22(4):300–6.
[41] Robitaille M, Dube M-C, Weisnagel SJ, et al. Substrate sourceutilization during moderate intensity exercise with glucoseingestion in type 1 diabetic patients. J Appl Physiol2007;103(1):119–24.
[42] Lecoultre V, Benoit R, Carrel G, et al. Fructose and glucose co-ingestion during prolonged exercise increases lactate andglucose fluxes and oxidation compared with an equimolarintake of glucose. Am J Clin Nutr 2010;92(5):1071–9.
[43] Jeukendrup AE, Raben A, Gijsen AP, et al. Glucose kineticsduring prolonged exercise in highly trained human subjects:effect of glucose ingestion. J Physiol (Lond) 1999;515(2):579–89.
[44] Arkinstall MJ, Bruce CR, Clark SA, et al. Regulation of fuelmetabolism by preexercise muscle glycogen content andexercise intensity. J Appl Physiol 2004;97(6):2275–83.
[45] Caron A, Lavoie C, Péronnet F, et al. Oxidation of [13C]glucoseingested before and/or during prolonged exercise. Eur J ApplPhysiol 2004;91:217–23.
[46] Watt M, Heigenhauser J, Dyck DJ, et al. Intramusculartriacylglycerol, glycogen and acetyl group metabolism during4 h of moderate exercise in man. J Physiol 2002;541(3):969–78.
[47] Brooks GA, Mercier J. Balance of carbohydrate and lipidutilization during exercise: the "crossover" concept. J ApplPhysiol 1994;76(6):2253–61.
[48] Stellingwerff T, Boon H, Gijsen AP, et al. Carbohydratesupplementation during prolonged cycling exercise sparesmuscle glycogen but does not affect intramyocellular lipiduse. Pflugers Arch 2007;454:635–47.
[49] Ahlborg G, Felig P, Hangenfeldt L, et al. Substrate turnoverduring prolonged exercise in man: splanchnic and legmetabolism of glucose, free fatty acids and amino acids. J ClinInvest 1974;53:1080–90.
[50] Romijn JA, Coyle EF, Sidossis LS, et al. Regulation ofendogenous fat and carbohydrate metabolism in relation toexercise intensity and duration. Am J Physiol 1993;265:E380–91.
[51] Wallis GA, Dawson R, Achten J, et al. Metabolic responses tocarbohydrate ingestion during exercise inmales and females.Am J Physiol Endocrinol Metab 2006;290:E708–15.
[52] Horton TJ, Grunwald GK, Lavely J, et al. Glucose kinetics differbetween women and men, during and after exercise. J ApplPhysiol 2006;100(6):1883–94.
[53] Tarnopolsky MA. Sex differences in exercise metabolism andthe role of 17-beta estradiol. Med Sci Sports Exerc 2008;40(4):648–54.
[54] Tremblay J, Peronnet F, Massicotte D, et al. Carbohydratesupplementation and sex differences in fuel selection duringexercise. Med Sci Sports Exerc 2010;42(7):1314–23.
[55] Kraemer RR, Francois M, Castracane VD. Estrogen mediationof hormone responses to exercise. Metabolism 2012;61(10):1337–46.
[56] Isacco L, Duché P, Boisseau N. Influence of hormonal statuson substrate utilization at rest and during exercise in thefemale population. Sports Med 2012;42(4):327–42.
[57] Horton T, Miller E, Glueck D, et al. No effect of mentrual cyclephase on glucose kinetics and fuel oxidation during moder-ate-intensity exercise. Am J Physiol 2002;282:E752–62.
[58] Mikines KJ, Sonne B, Farrell PA, et al. Effect of physicalexercise on sensitivity and responsiveness to insulin inhumans. Am J Physiol Endocrinol Metab 1988;254(3):E248–59.
[59] Maehlum S, Hostmark AT, Hermansen L. Synthesis of muscleglycogen during recovery after prolonged severe exercise indiabetic and non diabetic subjects. Scand J Clin Lab Invest1977;37:309–16.
[60] Owen W, Roberts W. Cross-reactivity of three recombinantinsulin analogs with five commercial insulin immunoassays.Clin Chem 2004;50(1):257–9.
[61] Jeukendrup AE, Wallis GA. Measurement of substrate oxida-tion during exercise by means of gas exchange measure-ments. Int J Sports Med 2005;26(Suppl 1):S28–37.
[62] Wagenmakers AJM. Protein and amino acid metabolism inhuman muscle. Adv Exp Med Biol 1998;441:307–19.
[63] Frayn KN. Calculation of substrate oxidation rates in vivofrom gaseous exchange. J Appl Physiol 1983;55(2):628–34.
[64] Krzentowski G, Pirnay F, Pallikarakis N, et al. Glucoseutilization during exercise in normal and diabetic subjects.The role of Insulin. Diabetes 1981;30(12):983–9.
[65] Chokkalingam K, Tsintzas K, Snaar JEM, et al. Hyperinsuli-naemia during exercise does not suppress hepatic glycogenconcentrations in patients with type 1 diabetes: a magneticresonance spectroscopy study. Diabetologia 2007;50(9):1921–9.
[66] Francescato MP, Geat M, Fusi S, et al. Carbohydrate require-ment and insulin concentration during moderate exercise intype 1 diabetic patients. Metabolism 2004;53(9):1126–30.
[67] Jenni S, Christ E, Stettler C. Exercise-induced growth hormoneresponse in euglycaemia and hyperglycaemia in patientswith type 1 diabetes mellitus. Diabet Med 2010;27:230–3.
[68] Ramires PR, Forjaz CLM, Strunz CMC, et al. Oral glucoseingestion increases endurance capacity in normal anddiabetic (type I) humans. J Appl Physiol 1997;83(2):608–14.
[69] Debono M, Ghobadi C, Rostami-Hodjegan A, et al. Modified-release hydrocortisone to provide circadian cortisol profiles. JClin Endocrinol Metab 2009;94(5):1548–54.
[70] Weitzman ED, Fukushima D, Nogeire C, et al. Twenty-fourhour pattern of the episodic secretion of cortisol in normalsubjects. J Clin Endocrinol Metab 1971;33(1):14–22.
[71] Murtagh E, Boreham C, Murphy M. Speed and exerciseintensity of recreational walkers. Prev Med 2002;34(4):397–400.
[72] Møller N, Jørgensen JOL, Alberti KGMM, et al. Short-termeffects of growth hormone on fuel oxidation and regionalsubstratemetabolism in normalman. J Clin Endocrinol Metab1990;70(4):1179–86.
[73] American Diabetes Association. Standards of medical care indiabetes — 2011. Diabetes Care 2011;34(Suppl 1):S11–61.
[74] American Diabetes Association. Diabetes mellitus and exer-cise. Diabetes Care 2002;25(Suppl 1):s64.
[75] Kilbride L, Charlton J, Aitken G, et al. Managing blood glucoseduring and after exercise in type 1 diabetes: reproducibility ofglucose response and a trial of a structured algorithmadjusting insulin and carbohydrate intake. J Clin Nurs2011;20(23–24):3423–9.









![The Guide - Diabetic Retinopathy - Vision Lossvisionloss.org.au/wp-content/uploads/2016/05/The... · the guide [diabetic retinopathy] What is Diabetic Retinopathy? Diabetic Retinopathy](https://img.pdfslide.us/doc/110x75/5e3ed00bf9c32e41ea6578a8/the-guide-diabetic-retinopathy-vision-the-guide-diabetic-retinopathy-what.jpg)