Embed Size (px)
Citation preview
CASE STUDY | SOUTH AFRICA
FROM BRAIN DRAIN TO BRAIN GAIN: NURSING AND MIDWIFERY MIGRATION TRENDS IN THE
SOUTH AFRICAN HEALTH SYSTEM

Funding for the development of this document was provided through the project “Brain Drain to Brain Gain - Supporting WHO
Code of practice on International Recruitment of Health personnel for Better Management of Health Worker Migration”, co-funded
by the European Union (DCI-MIGR/2013/282-931) and Norad, and coordinated by WHO. The contents of this document are the
sole responsibility of the African Institute for Health and Leadership Development, and can under no circumstances be regarded
as reflecting the position of the European Union or WHO.
© African Institute for Health and Leadership Development, all rights reserved.
October 2017
Acknowledgements
The authors of this report are Percy Mahlathi and Jabu Dlamini (African Institute of Health & Leadership Development).

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 1
Contents
Abbreviations ......................................................................................................................... 3
Abstract ................................................................................................................................ 4
1. Background ..................................................................................................................... 5
2. Policy context of nursing in South Africa ............................................................................. 6
3. Nursing workforce context ................................................................................................. 8
4. Education and training of nurses in South Africa .................................................................. 9
5. Registration requirements for foreign nurses ......................................................................10
6. Migration of the South African nursing workforce ................................................................12
7. Study objectives ..............................................................................................................13
8. Methods .........................................................................................................................13
9. Results ..........................................................................................................................13
9.1 Minimum data sets…. ..................................................................................................13
9.2 Stock of nurses, 2016 ...................................................................................................13
10. Distribution of nurse practitioners in South Africa ...............................................................18
11. Movements by South African nurses ...................................................................................19
12. Discussion .................................................................................................................... 22
13. Conclusion .................................................................................................................... 25
Acknowledgements .................................................................................................................26
References ............................................................................................................................27
FigureFigure 1. Organization of nursing leadership: public health service ................................................... 7
TablesTable 1. Mid-year population estimates by province, 2017 ................................................................ 5
Table 2. Demographic indicators, 2002–2017 ................................................................................ 6
Table 3. Selected list of human resources for health policies ............................................................. 8
Table 4. Categories of nursing p6ractitioners ................................................................................ 9
Table 5. Numbers in nurse training categories ..............................................................................14
Table 6. Outputs from all SANC ..................................................................................................14
Table 7. Outputs from public nursing education institutions ............................................................15
NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 1

2 FROM BRAIN DRAIN TO BRAIN GAIN:
Table 8. Outputs from universities, 2012–2016 (four-year programme) ..............................................15
Table 9. Increase in the registers of nurse practitioners, 2012–2016 .................................................16
Table 10. Age comparison of new entrants, 2011 and 2016 ..............................................................16
Table 11. Output of pupil nurses: private nursing institutions, by province, 2012–2016 ........................17
Table 12. Output of pupil nurses: public nursing institutions ...........................................................17
Table 13. SANC registrations by provincial distribution...................................................................18
Table 14. Requests for letters of verification ................................................................................20
Table 15. Foreign nurses registered by SANC ................................................................................20
Table 16. Strategies to mitigate health worker migration ................................................................21
Table 17. Nurse/midwife resignations across provinces, 2012–2016 ..................................................23
Contents (continued)

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 3
Abbreviations
CNO Chief Nursing Officer
DENOSA Democratic Nursing Organisation of South Africa
EM Enrolled Midwife
EN Enrolled Nurse
ENA Enrolled Nursing Auxiliary
ESMOE Essential Steps in the Management of Obstetric Emergencies
NQF National Qualifications Framework
OECD Organisation for Economic Co-operation and Development
PHC Primary Health Care
RN/RM Registered Nurse/Midwife
SANC South African Nursing Council
SAQA South African Qualifications Authority
SRN/M Specialist Registered Nurse/Midwife
WHO World Health Organization

AbstractBackground. The provision of health services is largely dependent on the sufficiency of the health workforce in terms of numbers, the quality of skills they possess, how and where they are deployed and how they are managed. With increasing urbanization, the issue of migration (including immigration, emigration and movement between the public and private sectors) of health personnel has become a critical factor in the debate about social justice in health, especially access and equity in the provision of health services. This case study seeks to better understand the patterns of movement of nurses and midwives and the development of associated policies in order to help health authorities to put in place the necessary systemic improvements for effective management of health workforce migration.
Objectives. The objectives of the study were (a) to assess the recorded movement of nurses and midwives employed in the public health facilities; and (b) to identify existing policy instruments and practices in place to maximize benefits and mitigate negative consequences of the migration of nurses.
Method. Data were collected from the provincial Departments of Health, the South African Nursing Council (SANC), the Democratic Nursing Organisation of South Africa and nursing education institutions through a survey. Follow-up telephonic or face-to-face interviews were conducted where a need was felt for verbal discussion. The data utilized were derived from responses to a survey questionnaire, published data from the SANC website and responses from oral interviews.
Results. Data analysis revealed that registered nurses and registered midwives form 34.45% (138 335) of 401 543 nurses appearing on the 2016 SANC register are employed by the provincial Departments of Health. Evidence of widespread migration by South African nurses is difficult to prove empirically despite several previous research studies. Over a five-year period, only 2158 registered nurses requested verification letters from SANC, either directly or through recruitment agencies. Nursing qualifications have undergone a major review and will be implemented in 2020. South African qualified nurses are trained to be generalists with grounded skills in midwifery. When nurses seek work in other countries, they do so utilizing their generalist nursing skills and experience rather than midwifery skills. There is variance between SANC registration data and provincial employment data for nurses.
Discussion. The country needs to develop a proactive mechanism to record and manage information regarding the mobility of its nursing workforce. SANC keeps records of nurses but cannot differentiate those in active practice from those in retirement or working overseas. SANC’s policy on foreign-trained nurses, based on the Department of Health’s Policy on the Recruitment and Employment of Foreign Health Professionals in the South African Health Sector, also requires review to align it with the new immigration laws of the country. Refugees and asylum seekers who are nurses form a component of migration but are not often considered in the literature on nurse migration. Given the long-standing interest in the international mobility of South African nurses, this paper advances an argument that migration by South African nurses is not as high as claimed in some studies. The most reliable indicator available currently is the record of requests for letters of verification, which are only issued by SANC. However, data from the Organisation for Economic Co-operation and Development appear to be at odds with SANC data.
Key words. emigration, immigration, nurses, midwives, experience, financial gain, foreign-trained nurses, South Africa, SANC
4 FROM BRAIN DRAIN TO BRAIN GAIN:

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM1. BackgroundThis study was undertaken as a follow-up to Minimum data sets for human resources for health and the surgical workforce in South Africa’s health system: a rapid analysis of stock and migration (1) and From Brain Drain to Brain Gain: understanding and managing the movement of medical doctors in the South African health system (2).
The South African health system is premised on primary health care (PHC) services that are delivered through a District Health System. The system is designed to ensure easy access to health services by every citizen in line with the Bill of Rights as enshrined in the Constitution of the Republic of South Africa. With effect from 1996, the gov-ernment endeavoured to extend access through a massive clinic building programme and revitalization of hospitals across the country. The public health service is divided into primary, secondary and tertiary care through health facilities that are located in, and managed by, the provin-cial Departments of Health. The provincial Departments of Health are thus the direct employers of the health workforce, including nurses, whilst the national Ministry of Health is responsible for policy development and coordination.
Between June 2016 and June 2017, the South African population is estimated to have grown by 2.85% from 54 956 900 to 56 521 900 (3). Most people access health services through the government’s public clinics and
hospitals, whilst approximately 16% access health services through private health facilities. The vast majority of health professionals that work in public health facilities are nurses. Stand-alone private nursing practices are not a common feature in the South African health system. The South African Nursing Council (SANC) register shows that as of 17 January 2017 there were 401 543 nurses and midwives eligible to practise nursing in South Africa (4), compared to 391 517 in 2015.
TABLE 1. MID-YEAR POPULATION ESTIMATES BY PROVINCE, 2017
Population estimate
% of total population
Urban/rural/nature of province
Eastern Cape 6 498 700 11.5 Rural
Free State 2 866 700 5.1 Rural
Gauteng 14 278 700 25.3 Urban
KwaZulu-Natal 11 074 800 19.6Rural but has large urban centres
Limpopo 5 778 400 10.2 Rural
Mpumalanga 4 444 200 7.9 Rural
Northern Cape 1 214 000 2.1 Rural
North West 3 856 200 6.8 Rural
Western Cape 6 510 300 11.5Urban but has farming and rural communities
Total 56 521 900 100.0
Source: Statistics South Africa, 2017.
NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 5

6 FROM BRAIN DRAIN TO BRAIN GAIN:
The health care system consumed about 8.8% of the country’s gross domestic product during 2012 (5). The private sector serves about 16% of the population, whilst the public sector serves 84% (6). The country’s population distribution indicates that about 64.7% inhabit the provinces, which are largely rural in nature. Table 2 and Table 3 present population and demographic statistics for South Africa.
There is a realization that the health workforce plays a critical role in advancing the health system goals (7), largely driven by a policy position of improving access to health care for all citizens. In the mid-2000s, the nursing profession, through their national association, the Democratic Nursing Organisation of South Africa (DENOSA), made several representations to the Ministry of Health for the creation of a post at national level that
would be dedicated to nursing issues. The driving force was a realization and acknowledgement that nursing, being the largest component of the health care professions, needed coordination at the highest policy level. Whilst the crude birth rate has remained fairly constant from 2002 (21.7) to 2017 (21.3), there has been a noticeable rate of natural increase requiring a steady provision of health workers.
2. Policy context of nursing in South Africa
The nursing profession is regulated through an act of Parliament – the Nursing Act No. 33 of 2005. This act replaced the previous Nursing Act No. 50 of 1978. The purpose of the act was to regulate the nursing profession, and to provide for matters connected therewith. It thus
TABLE 2. DEMOGRAPHIC INDICATORS, 2002–2017
Year
Crude birth rate (per 1000
pop.)
Life expectancy (years)
Infantmortality
rate (per 1000
pop.)
Under-5 mortality
rate (per 1000
pop.)
Crudedeath rate (per 1000
pop.)
Rate ofnatural
increase (%)Male Female Total
2002 21.7 52.9 56.6 54.9 48.1 71.3 13.4 0.83
2003 21.7 52.5 55.8 54.2 48.1 71.6 14.0 0.77
2004 22.7 52.2 55.3 53.8 48.7 71.8 14.4 0.83
2005 23.4 52.1 54.8 53.5 49.1 72.5 14.8 0.86
2006 24.1 52.3 54.7 53.5 48.7 71.7 14.8 0.93
2007 24.8 53.3 56.1 54.7 47.8 70.1 14.0 1.08
2008 24.8 54.3 57.9 56.1 46.6 67.6 13.0 1.18
2009 24.4 55.0 58.7 56.9 42.8 63.3 12.6 1.18
2010 23.9 56.4 60.6 58.5 41.1 58.4 11.6 1.23
2011 23.5 57.6 62.7 60.2 39.9 54.4 10.7 1.28
2012 23.3 58.5 63.6 61.1 38.8 51.5 10.2 1.31
2013 23.0 59.2 64.6 61.9 37.4 49.1 9.8 1.32
2014 22.7 59.7 65.1 62.5 36.0 47.1 9.6 1.31
2015 22.2 60.0 65.5 62.8 34.0 44.7 9.5 1.27
2016 21.7 60.6 66.1 63.4 33.5 43.6 9.2 1.25
2017 21.3 61.2 66.7 64.0 32.8 42.4 9.0 1.23
Source: Statistics South Africa, 2017.

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 7
enabled the establishment of the South African Nursing Council (SANC) to regulate such matters and spelled out clear functions that the council must regulate and adjudicate upon.
Some of SANC’s key objects are (a) to serve and protect the public in matters involving health services generally and nursing services in particular; (b) to perform its func-tions in the best interests of the public and in accordance with national health policy as determined by the Minister of Health; (c) to establish, improve, and control the con-ditions, standards, and quality of nursing education and training within the ambit of the act and any other appli-cable laws; and (d) to maintain professional conduct and practice standards for practitioners within the ambit of any applicable law.
SANC is therefore the custodian of nursing education, training and practice standards. It is required to work in concert with the Ministry of Health in matters related to nursing. In that context, the Ministry of Health established the office of the Chief Nursing Officer (CNO) in 2014 after considering representations from DENOSA. The major role of the CNO is to provide advice to the Minister of Health and the members of the Executive Council for Health in the nine provinces on technical and policy matters regarding nursing and health services generally. The establishment of this office has served to reinforce the central role that nursing plays in the provision of health services in South Africa. The location of the office within the Ministry of Health is strategic, as it places nursing at the centre of health policy development and coordination at national and global level. The CNO is part of the country delegation to the World Health Assemblies, which are held on an annual basis. The CNO therefore participates in the global CNO meetings that serve to advance the nursing agenda on the global health stage. Positive results have emanated from the establishment of CNOs in many WHO Member States, for example the inclusion of a chapter on nursing in the Global Strategy on Human Resources for Health: Workforce 2030.
At national level, the CNO policy focus areas include placing major emphasis on the centrality of nursing in PHC, for example in the areas of school health, ward-based PHC services, and maternal and child health services.
The CNO is supported at provincial level by a director for nursing practice, whose functions relate to operational policy implementation. The director is required to advise the members of the Executive Council for Health and the head of the Department of Health on all matters relating to the planning, organization and deployment of nursing services in public clinics and hospitals across the province. Their counterparts are the principals of the public nursing colleges, which are located within the provincial Departments of Health. The next layer of nursing leadership is at health service delivery level, namely hospitals and clinics, as depicted in Figure 1.
FIGURE 1. ORGANIZATION OF NURSING LEADERSHIP: PUBLIC HEALTH SERVICE
A number of policies have been adopted over the years aimed at improved management of the health workforce in South Africa (1, 2). Table 3 presents a set of policy and strategy documents relevant to the management of the health workforce, including nursing, that together contribute to improved distribution and retention of the workforce, and support implementation of the World Health Organization (WHO) Global Code of Practice on the International Recruitment of Health Personnel (8), with the Policy on the Recruitment and Employment of Foreign Health Professionals in the South African Health Sector being particularly notable.
Chief Nursing Officer(located at Ministry of Health)
Provincial nursing directors (x9)
Principals of nursing colleges (x9) and Nursing managers (hospitals and clinics)

8 FROM BRAIN DRAIN TO BRAIN GAIN:
TABLE 3. SELECTED LIST OF HUMAN RESOURCES FOR HEALTH POLICIES
Policy Year Focus/rationale
Human Resource Strategy 2001 Proposals on the definitions, entry requirements, and scope of practice of all categories of health care professionals
Scarce Skills Allowance 2003 Financial incentive to retain “scarce skills” in the public health service
Remunerative Work outside Public Service
2002 Incentive scheme allowing public servants to work in the private sector whilst fully employed by government
Human Resources for Health Planning Framework
2006 Highlighting the need for systematic national health workforce planning
Policy on Remuneration of Health Professionals Working in Public Health Service
2007 System of differentiated pay for health professionals employed in public health facilities with the objective of recruiting and retaining professionals in the public health service
Nursing Strategy 2008 Articulates how nursing education and training, practice, resources, social positioning, regulation and leadership are planned and linked together with prescripts of professionalism to support the nation’s health system
Policy on the Recruitment and Employment of Foreign Health Professionals in the South African Health Sector
2010 Principles and practices in the employment of health professionals who are non-citizens aligned to the immigration processes of the Department of Home Affairs
Human Resources for Health Strategy
2011 Focus on planning and staffing of health facilities in preparation for the introduction of the National Health Insurance. It built on the foundation laid by the 2001 Human Resource Strategy and the 2006 Human Resources for Health Planning Framework
National Strategic Plan for Nurse Education, Training and Practice
2012 Develop, reconstruct and revitalize the profession to ensure that nursing and midwifery practitioners are equipped to address the disease burden and population health needs within a revitalized health care system in South Africa
These policies are intended to work in harmony and extend to influence the operations of statutory health councils such as SANC and education institutions.
3. Nursing workforce contextIn recent years, nursing education and training has come under the spotlight due to the split mandate between the National Department of Health and the Department of Higher Education and Training. The National Department of Health is responsible for nursing service provision whilst the Department of Higher Education and Training is responsible for the education aspects through the Council on Higher Education. Nursing education and training takes place at three types of facilities – nursing colleges, which are located within provincial Departments of Health; private nursing schools, which either are attached to private hospitals or are independent; and university
nursing departments located within universities. Nursing constitutes the largest cadre of the South African health workforce.
When the health system was being transformed from 1996 onwards, the government took a decision to adopt PHC as the preferred system for making health services accessible to citizens. The White paper for the transformation of the health system (1997) articulated the values that would be pursued in line with the Bill of Rights enshrined in the country’s Constitution. Nursing is widely regarded as a critical component of the provision of health services. In 2009, a process for improving PHC, termed the Re-engineering of Primary Health Care, was introduced by the Ministry of

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 9
Health. It has three strands, namely establishment of ward-based PHC outreach teams, expansion and strengthening of school health services, and establishment of district clinical specialist teams. Nurses play a key role in all these strands.
4. Education and training of nurses in South Africa
Education and training of nurses in South Africa is regu-lated by SANC through the Nursing Act No. 33 of 2005. For a person to be admitted to an academic programme leading to qualification as a nurse, they need to have suc-cessfully achieved a grade 12 school pass. This pass is at level 4 of the National Qualifications Framework (NQF) as defined by the South African Qualifications Authority (SAQA). The NQF is set up in terms of the National Qualifications Framework Act No. 67 of 2008, as amend-ed. In terms of the NQF Act, SANC is designated as a Quality Council, with responsibilities including (a) devel-oping and implementing policy and criteria, taking into account the policy and criteria contemplated in section 13(1)(h)(i) of the act, for the development, registration and publication of qualifications; (b) ensuring the devel-opment of such qualifications or part qualifications as are necessary for the sector, which may include appropriate measures for the assessment of learning achievement; and
TABLE 4. CATEGORIES OF NURSING PRACTITIONERS (BASED ON CURRENT QUALIFICATIONS) AND LENGTH OF TRAINING
Qualification category Length of education and training
Enrolled nursing auxiliary (ENA) 1 year
Enrolled nurse (EN) 2 years
Registered nurse/midwife (RN/M) 4 years
Specialist registered nurse/midwife (SRN/M) 1 or 2 years post RN/M training depending, on the post-basic programme
A nurse who holds any of these qualifications can provide health services in any environment as long as their scope of practice permits. Thus, nurses are found in every health facility – public and private – where health services are required.
According to the current education qualifications framework (9), four categories of nurses are recognized: enrolled nursing auxiliary (ENA), enrolled nurse (EN), registered nurse/midwife (RN/M), and specialist registered nurse/midwife (SRN/M). Table 4 indicates the length of training for each category.
(c) recommending qualifications or part qualifications to SAQA for registration.
The repeal of the Nursing Act No. 50 of 1978 necessi-tated a review of nursing qualifications. The unintend-ed consequence of the introduction of the four-year Comprehensive Diploma in Nursing through Government Notice No. R425 of 22 February 1985 (as amended) was the perception that the programme offered four qualifica-tions in one, namely general nursing, community health nursing, psychiatric nursing and midwifery. In addition, the registration of a qualified nurse in the current SANC register is registered nurse/midwife (RN/M). This also gives a perception that the RN/M is a double qualifica-tion. The policy intention of the Comprehensive Diploma in Nursing was the production of a generalist nurse with a wide range of relatively superficial competence in order to render a generalist level of care (10). Thus, the mid-wifery aspect of the four-year diploma is not a stand-alone qualification but rather a designation to indicate training in midwifery. A South African nurse with a four-year

10 FROM BRAIN DRAIN TO BRAIN GAIN:
Diploma in Nursing (under the current system) is there-fore expected to possess competencies that can be applied in the practice of midwifery under general conditions of nursing practice. These nurses operate at any level of the health service and are not confined to obstetric care.
With the enactment of the Nursing Act No. 33 of 2005, it became imperative that all nursing qualifications be reviewed so that each could be streamlined and operate in harmony with the relevant scopes of practice. These have now been configured such that the new Diploma in Nursing will be completed over a three-year period and confined to the PHC environment where the comprehen-sive generalist competencies will be required (11). A new register of specialist nurses will be established and is due to come into operation in 2020. The register with the cur-rent (legacy) qualifications will cease to exist at the end of 2019. There is therefore heightened activity in prepa-ration for the transformation of nursing education and training in South Africa.
The policy imperative is articulated by SANC as follows:
Nursing education and training across South Africa is responding to changing needs, develop-ments, priorities and expectations in health and healthcare. Nurses who acquire the knowledge, skills and behaviours that meet our standards will be equipped to meet these present and future chal-lenges, improve health and wellbeing and drive up standards and quality, working in a range of roles including practitioner, educator, leader and researcher.
The review of nursing qualifications was also necessitat-ed in part by an increasingly complex burden of disease requiring new competencies among nurses, and by the changing post-schooling education landscape as articu-lated by the NQF. The qualifications are now organized in the following manner (11):
Higher Certificate: Auxiliary Nursing. This qualifica-tion aims to (a) produce nurses that will provide basic nursing care in all spheres of health care service delivery; (b) provide the nurse with a wide range of cognitive, affec-tive and psychomotor skills; (c) hone skills in assessment,
planning and implementation of basic nursing care; and (d) develop writing and oral communication skills.
Diploma in Nursing: Staff Nurse. This diploma will ap-ply evidence-based nursing practice, based on research or established practices that have proven to be effective both nationally and internationally within the profession. It will also equip diplomates with a developed sense of eq-uity, justice and service ethics that will ensure that they work in an accountable manner, irrespective of their cho-sen workplace.
Bachelor’s Degree in Nursing and Midwifery. The graduate who completes this qualification will be able to, inter alia, (a) apply knowledge of theory of biological and natural sciences, psychosocial sciences and pharma-cology in the provision of comprehensive nursing and midwifery care; (b) develop, implement and evaluate population-based health care; and (c) utilize research in nursing and health-related problems to improve health care outcomes.
Advanced Diploma in Midwifery. The primary purpose of this qualification is to produce competent, independent and critically thinking midwives who will provide scien-tific, safe and comprehensive quality midwifery care to in-dividuals, families and communities within the legal and ethical framework.
These academic programmes can be offered at any post-school level – nursing college, technical and vocational education training institution, or university – as long as such an institution has satisfied the accreditation criteria set by SANC.
5. Registration requirements for foreign nurses
Since 2010 all health professionals from outside South Africa wishing to work in the country must comply with the Policy on the Recruitment and Employment of Foreign Health Professionals in the South African Health Sector. This policy was introduced to improve the flow of health professionals into South Africa and expresses the following objectives:

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 11
• promote high standards of practice in the recruitment and employment of health professionals who are not South African citizens or permanent residents;
• preclude the active recruitment of health professionals from developing countries unless there are specific government-to-government agreements to allow and support such recruitment.
The policy was crafted such that it is complementary to the Immigration Act and other laws, and is consistent with the country’s Constitution. SANC has in turn developed and adopted policy guidelines regarding registration of inter-nationally qualified nurses and midwives and/or foreign qualifications with SANC. The policy emphasizes the fact that SANC is responsible for the regulation of the nurs-ing profession in South Africa. In executing the function of registration of foreign nurses and qualifications from foreign countries, SANC takes cognizance of the Policy on the Recruitment and Employment of Foreign Health Professionals in the South African Health Sector (12). In pursuit of this function, SANC processes applications from foreign nurses and midwives who hold qualifications from a foreign country as well as South Africans who hold qual-ifications from a foreign country.
The fundamental principle is that “the evaluation of for-eign qualifications by SANC considers all South African National Qualifications Framework related legislation, regulations and policies”. The policy guidelines further em-phasize that “where substantial difference exists and can be demonstrated between foreign and local qualification, it re-mains SANC’s decision (prerogative) to recognize a foreign qualification at the designated NQF level”. Furthermore, SANC reserves the right to revoke a certificate of profes-sional registration should any evidence come to light that compromises its integrity and validity (12).
The guidelines advance the following requirements for a nurse affected by this policy:
• Applicants must provide SANC with a complete and credible set of documents to enable evaluation.
• Relevant information from foreign institutions and
professional bodies must be submitted in order for SANC to conduct a fair and authentic evaluation of a foreign qualification.
• Complete verification of a foreign qualification is required before it is recognized as authentic.
The categories that are envisaged in the policy are applicants who:
• hold a foreign qualification and wish to undergo basic/undergraduate nurse training and education in South Africa;
• hold a foreign qualification and wish to pursue postgraduate studies in South Africa;
• wish to do elective practicums in South Africa in order to gain experience in a specific area of practice;
• wish to do voluntary work or research in South Africa;
• wish to be registered for employment after successful completion of postgraduate studies in South Africa.
Foreign nationals who wish to be employed in South Africa as nurses must submit to SANC the following documents:
• letter of intent/application;
• letter of support from the National Department of Health’s Foreign Workforce Management Programme;
• certificate of English language proficiency from an accredited institution (applicable only to applicants whose nursing education was not done in English);
• evaluation certificate of foreign educational qualification by SAQA;
• certified copy of registration by the regulatory body from the country of origin;
• certified copy of qualification certificate;
12 FROM BRAIN DRAIN TO BRAIN GAIN:
• valid licence to practise as a nurse from the nurse’s reg-ulatory body where the applicant’s nursing qualification was registered;
• record of education and training (transcript) from the nursing education institution in the country of origin;
• verification certificate from the regulatory body of the country of origin confirming that the applicant is in good professional standing and has no professional misconduct cases pending against her/him (except for refugees);
• letter of competence from the last employer;
• police clearance letter from the country of origin (ex-cept for refugees).
The exclusion of refugees from some of these requirements is based on the provisions of South Africa’s Refugees Act No. 130 of 1998, as amended, which aims to protect those who come to South Africa because of persecution in their countries. However, a work permit or formal recognition of refugee status issued by the Department of Home Affairs must be produced. In the case of employment, once all con-ditions set by SANC have been satisfied, and once appoint-ed to a post, an expatriate nurse is entitled to the same sala-ry and benefits pertaining to the post as any South African counterpart who occupies a similar post. This is in line with section 18 of the Immigration Act, which states that:
(5) An application for a critical skills work visa shall be ac-companied by proof that the applicant falls within the critical skills category in the form of –
a) a confirmation, in writing, from the profession-al body, council or board recognized by South African Qualifications Authority (SAQA) in terms of section 13(1)(0) of the National Qualifications Framework Act, or any relevant government Department confirming the skills or qualifications of the applicant and appropriate post qualification experience;
b) if required by law, proof of application for a cer-tificate of registration with the professional body,
council or board recognized by SAQA in terms of section 13(1)(i) of the National Qualifications Framework Act; and
c) proof of evaluation of the expatriate qualification by SAQA and translated by a sworn translator into one of the official languages of the Republic (of South Africa).
(6) A critical skills work visa shall be issued for a period not exceeding five years.
(7) A spouse and dependent children of a holder of a crit-ical skills work visa shall be issued with an appropriate visa valid for a period not exceeding the period of valid-ity of the applicant’s critical skills work visa.
Section 18(3)(iii) of the Immigration Act also prescribes that the salary and benefits of the applicant are not inferi-or to the average salary and benefits of citizens or perma-nent residents occupying similar positions in South Africa. This is also in line with the provisions of the Occupation-Specific Dispensation policy, which regulates how health professionals in the public health service are remunerated.
There is acknowledgment that the National Department of Health’s Policy on the Recruitment and Employment of Foreign Health Professionals in the South African Health Sector requires urgent review so that it is completely in line with the amended Immigration Act of 2014. In addition, prevalent health workforce shortages have rendered some of the clauses of the policy irrelevant, for example princi-ple 5, which states that the employment of expatriate health professionals shall only be allowed after they have been successful in competing for an advertised post and there is record that no South African citizen or permanent resident was available or found suitable to fill the particular post. When faced with critical shortages, this clause is unlikely to be adhered to.
6. Migration of the South African nursing workforce
The migration of South African medical professionals has been a subject of discussion for a considerable period. Many studies have been conducted and have advanced

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 13
varying estimates of emigration by health professionals in the African continent (13–15). Several causes of migration by health professionals have also been recorded. Measuring the extent of emigration – particularly by South African nurses – remains a challenge, as several research studies have been based on incomplete data. Previously, challenges have been reported relating to collection of systematic data on international flows of health workers from South Africa, including to the rest of the continent, resulting in a tendency to rely on destination country data systems to estimate the extent of emigration of medical doctors from South Africa (2). Clemens and Pettersson have previously utilized destination country census data to make such an estimation (15).
As reported in the authors’ previous study on the surgical workforce and management of migration by medical doctors (1, 2), South Africa still does not have a systematized mechanism for measuring and monitoring emigration of its health professionals. SANC has a system of issuing verification letters for nurses who request these for purposes of seeking employment overseas. However, even this method does not accurately estimate the number of nurses who end up taking employment in other countries.
Due to the difficulty of producing empirical evidence, some studies have resorted to making deductions based on “intention to leave” of respondents (16, 17).
7. Study objectivesThe objectives of the study were to:
(a) assess the recorded movement of nurses employed in the public health facilities;
(b) identify existing policy instruments and practices in place to maximize benefits and mitigate negative con-sequences of the migration of nurses.
The study also sought to identify whether any synergies or gaps existed between the workforce data systems of provincial Departments of Health (the major employer within the health sector), SANC and the national nursing association – DENOSA.
8. MethodsA survey questionnaire was sent through SANC, the nursing directors of the nine provincial Departments of Health, the principals of the nursing colleges locat-ed within the provincial Departments of Health, and DENOSA. The nine provincial Departments of Health were included in the study on the basis that they are the biggest direct employing entity of nurses. SANC was in-cluded on the basis that it carries the legislative mandate to maintain the registers of all nurses in the country, including those in active practice and those no longer practising. DENOSA was included on the basis that it is an umbrella organization of nurses, and the nursing col-leges and universities on the basis that they are respon-sible for the training of nurses. The Society of Midwives of South Africa was also included in the study. A face-to-face interview was held with the CNO to discuss and explore various policy issues relating to nursing and the role of her office.
Each respondent was sent a questionnaire to complete and, based on the responses, telephonic follow-up in-terviews were conducted for further explanations or closure of gaps in the information supplied. Guiding the research data-gathering process was a protocol de-veloped by the Global Health Workforce Alliance that provided a list of minimum data sets against which to match responses.
9. Results9.1 Minimum data setsIn relation to the minimum data sets, no data elements were probed, as the previous study responses (1) were deemed to be still relevant.
9.2 Stock of nurses, 2016The major data source was SANC, which maintains a register of all student nurses and qualified nurses that are licensed to practise in South Africa. The second source was the provincial Departments of Health.
As of 31 January 2017, the register of individuals undergoing training to be nurses as student nurses, pupil nurses, or pupil nursing auxiliaries was as indicated in
14 FROM BRAIN DRAIN TO BRAIN GAIN:
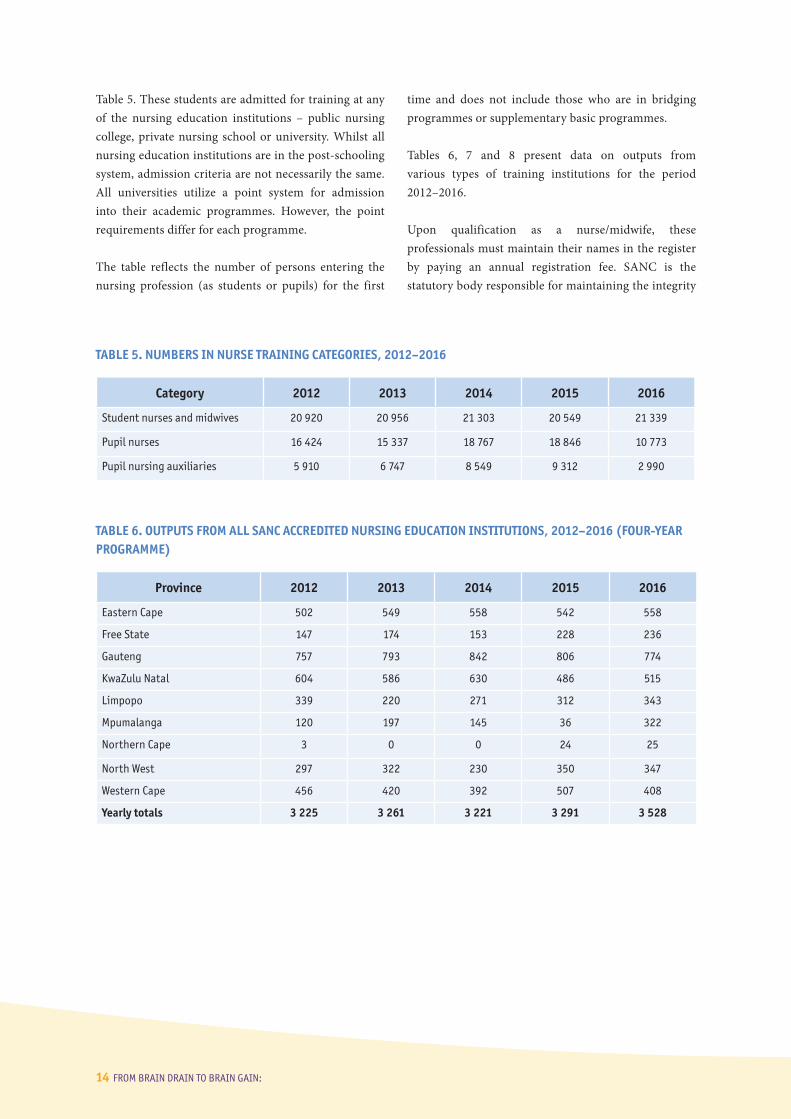
Table 5. These students are admitted for training at any of the nursing education institutions – public nursing college, private nursing school or university. Whilst all nursing education institutions are in the post-schooling system, admission criteria are not necessarily the same. All universities utilize a point system for admission into their academic programmes. However, the point requirements differ for each programme.
The table reflects the number of persons entering the nursing profession (as students or pupils) for the first
time and does not include those who are in bridging programmes or supplementary basic programmes.
Tables 6, 7 and 8 present data on outputs from various types of training institutions for the period 2012–2016.
Upon qualification as a nurse/midwife, these professionals must maintain their names in the register by paying an annual registration fee. SANC is the statutory body responsible for maintaining the integrity
TABLE 5. NUMBERS IN NURSE TRAINING CATEGORIES, 2012–2016
Category 2012 2013 2014 2015 2016
Student nurses and midwives 20 920 20 956 21 303 20 549 21 339
Pupil nurses 16 424 15 337 18 767 18 846 10 773
Pupil nursing auxiliaries 5 910 6 747 8 549 9 312 2 990
TABLE 6. OUTPUTS FROM ALL SANC ACCREDITED NURSING EDUCATION INSTITUTIONS, 2012–2016 (FOUR-YEAR PROGRAMME)
Province 2012 2013 2014 2015 2016
Eastern Cape 502 549 558 542 558
Free State 147 174 153 228 236
Gauteng 757 793 842 806 774
KwaZulu Natal 604 586 630 486 515
Limpopo 339 220 271 312 343
Mpumalanga 120 197 145 36 322
Northern Cape 3 0 0 24 25
North West 297 322 230 350 347
Western Cape 456 420 392 507 408
Yearly totals 3 225 3 261 3 221 3 291 3 528

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 15
of the register. Table 9 shows the increase in numbers of various registered categories.
The age analysis of students entering nurse training for the first time indicates the continued popularity of the profession to South Africans. A contributing factor may be that it remains one of the few professions that the government still takes responsibility for in terms of providing funding for studies. Table 10 shows the comparative ages of new entrants to various courses.
Over the same comparable period, the population of South Africa increased from approximately 47.850 million in 2007 to 55.909 million in 2016, an increase of 16% (Statistics South Africa, midyear estimate). SANC compiles and publishes its statistics annually on 31 December. Upon completion of training nurses have to perform community service, which amounts to one year working in the public health service. This system commenced with medical interns and was extended to nurses as from 2006. This is performed in terms of section
TABLE 8. OUTPUTS FROM UNIVERSITIES, 2012–2016 (FOUR-YEAR PROGRAMME)
Province 2012 2013 2014 2015 2016
Eastern Cape 127 142 147 175 200
Free State 49 35 32 59 71
Gauteng 110 113 100 136 93
KwaZulu Natal 70 62 124 116 199
Limpopo 109 72 94 116 125
Mpumalanga No university-based programme
Northern Cape No university-based programme
North West 297 322 230 350 347
Western Cape 456 420 392 507 408
TABLE 7. OUTPUTS FROM PUBLIC NURSING EDUCATION INSTITUTIONS, 2012–2016 (FOUR-YEAR PROGRAMME)
Category 2012 2013 2014 2015 2016
Eastern Cape 375 407 411 367 358
Free State 98 139 121 169 165
Gauteng 647 680 742 670 681
KwaZulu Natal 534 524 506 370 316
Limpopo 230 148 177 196 218
Mpumalanga 120 197 145 36 322
Northern Cape 62 56 3 24 25
North West 237 265 166 259 275
Western Cape 229 250 213 301 243

16 FROM BRAIN DRAIN TO BRAIN GAIN:
40(1) of the Nursing Act, 2005, which states: “A person who is a citizen of South Africa intending to register for the first time to practise a profession in a prescribed category must perform remunerated community service for a period of one year at a public health facility.” The associated Regulation 2.1 of the Regulations Relating to Performance of Community Service states: “Any person who is a citizen of South Africa intending to register for the first time as a professional nurse in terms of the Act, as having met the prescribed requirements to qualify as such, must perform remunerated community service for a period of one year.” These regulations pertain to South African citizens and permanent residents. Exemption will be granted to persons who may have performed a similar service elsewhere (12).
Health workforce planning is a critical element of any health system planning, and the age analysis of the workforce plays a major role in managing the workforce stock inflows and outflows. Nurses form the front line of health services in the public health sector. Evidence shows that the private nursing schools contribute significant numbers of nurses to the health system through the training of current staff nurses. Table 11 shows the output of pupil nurses from private nursing institutions by province, 2012–2016, while Table 12 shows the output of pupil nurses from public nursing institutions for the same period.
TABLE 10. AGE COMPARISON OF NEW ENTRANTS, 2011 AND 2016
Average age Minimum age Maximum age No.
Course 2011 2016 2011 2016 2011 2016 2011 2016
4-Yr Diploma 25 23 15 15 57 56 4 649 4 922
Bridging 36 36 20 21 61 62 3 051 5 131
Psychiatry 46 45 27 30 60 60 111 114
Midwifery 44 43 25 24 66 62 1 108 1 506
EN-Gen 30 34 17 18 60 60 7 622 845
EN-Comm 37 37 26 24 61 58 142 55
EN-Aged Care – 34 – 20 – 45 – 4
EN-Psy 39 38 27 38 53 38 41 2
AN 29 32 20 18 61 55 4 374 518
CHATC (PHC) 41 41 24 24 64 63 314 789
EN-Gen = enrolled nurse general; EN-Comm = enrolled nurse community health; EN-Psy = enrolled nurse psychiatry; AN = assistant nurse; CHATC = clinical nursing science, health assessment, treatment and care.
TABLE 9. INCREASE IN THE REGISTERS OF NURSE PRACTITIONERS, 2012–2016
Category 2012 2013 2014 2015 2016
RN/RM 124 045 129 015 133 127 136 854 140 598
EN/EM 58 722 63 788 66 891 70 300 73 558
ENA 65 969 67 895 70 419 71 463 73 302
RN/RM = registered nurses and registered midwives; EN/EM = enrolled nurses and enrolled midwives; ENA = enrolled nursing auxiliaries.

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 17
TABLE 11. OUTPUT OF PUPIL NURSES: PRIVATE NURSING INSTITUTIONS, BY PROVINCE, 2012–2016
Province 2012 2013 2014 2015 2016
Eastern Cape 195 211 246 406 271
Free State 41 62 57 66 65
Gauteng 1 978 2 345 1 998 2 848 2 414
KwaZulu-Natal 2 448 2 951 2 301 2 633 2 332
Limpopo 99 120 132 108 99
Mpumalanga 34 46 25 32 24
Northern Cape 0 0 0 0 0
North West 103 183 153 126 141
Western Cape 345 387 260 478 426
Yearly totals 5 243 6 305 5 172 6 697 5 772
TABLE 12. OUTPUT OF PUPIL NURSES: PUBLIC NURSING INSTITUTIONS, BY PROVINCE, 2012–2016
Province 2012 2013 2014 2015 2016
Eastern Cape 501 416 377 582 593
Free State 173 129 154 191 192
Gauteng 540 802 394 333 435
KwaZulu-Natal 536 634 297 199 8
Limpopo 409 162 134 237 246
Mpumalanga 211 271 216 262 399
Northern Cape 0 0 0 0 0
North West 1 23 41 71 82
Western Cape 119 212 164 184 152
Yearly totals 2 490 2 649 1 777 2 059 2 107
Note: Pupil nurses are those nurses who study towards the registration qualifications of enrolled nurse and enrolled nurse assistant.

18 FROM BRAIN DRAIN TO BRAIN GAIN:
TABLE 13. SANC REGISTRATIONS BY PROVINCIAL DISTRIBUTION, AS AT 31 DECEMBER 2016
Province SexRegistered
nursesEnrolled nurses
Auxiliary nurses Total Students Pupils Pupil NAs
Eastern Cape
Female 13 975 5 244 6 563 25 782 2 596 911 351
Male 1 588 873 1 216 3 677 1 160 289 136
Total 15 563 (11.07%)
6 117 (8.32%)
7 779 (10.61%)
29 459 (10.25%)
3 756 (17.6%)
1 200 (11.14%)
487 (16.29%)
Free State
Female 7 103 2 066 2 828 11 997 971 151 63
Male 1 102 416 359 1 877 242 25 16
Total 8 205 (5.84%)
2 482 (3.37%)
3 187 (4.35%)
13 874 (4.83%)
1 213 (5.68%)
176 (1.63%)
79 (2.64%)
Gauteng
Female 34 024 17 263 18 553 69 840 3 829 3 583 1 055
Male 2 579 1 471 1 214 5 264 908 350 95
Total 36 603 (26.03%)
18 734 (25.47%)
19 767 (26.97%)
75 104 (26.12%)
4 737 (22.2%)
3 933 (36.51%)
1 146 (38.33%)
KwaZulu Natal
Female 28 609 22 755 12 759 64 123 2 650 3 459 522
Male 2 999 2 537 1 302 6 838 981 546 84
Total 31 608 (22.48%)
25 292 (34.38%)
14 061 (19.18%)
70 961 (24.68%)
3 631 (17.02%)
4 005 (37.17%)
606 (20.27%)
Limpopo
Female 10 355 5 965 9 224 25 544 1 376 119 85
Male 1 498 652 838 2 988 519 27 11
Total 11 853 (8.43%)
6 617(9%)
10 062(13.73%)
28 532(9.93%)
1 895(8.88%)
146(1.36%)
96(3.21%)
10. Distribution of nurse practitioners in South Africa
One of the challenges that South Africa faces is urbaniza-tion, which has consequences for the availability of ser-vices across the country. Registration statistics at SANC show that the highest number of registrations is in three out of nine provinces. This does not necessarily mean that all those nurses are working in those provinces, as the SANC database is not linked to the employee databases of the Departments of Health in the provinces. Table 13 shows the provincial spread of nurses in terms of SANC registration, but not necessarily employment.
The figures in Table 13 indicate that the provinces of Gauteng, KwaZulu-Natal and Western Cape share be-tween them more than 60% of the country’s RN/RM reg-istrations. Similarly, these provinces share about 52% of the student nurse population amongst them. These pro-vincial distribution figures are based on registration data at SANC and do not reflect accurately the place of em-ployment of each nurse. SANC also does not keep a regis-ter based on the employment status of anyone appearing in its register.
(continued)

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 19
11. Movements by South African nurses
The majority of South African nurses are employed in the public health service, with the provinces of Gauteng, KwaZulu-Natal and Western Cape taking the bulk of these. Up to 1994 it was not easy for nurses to seek work overseas. However, this changed when the country elected a democratic government. This enabled all citizens to have freedom of movement and work, as enshrined in the Constitution of the Republic of South Africa, section 22 of the Bill of Rights, which states: “Every citizen has the right to choose their trade, occupation or profession freely. The practice of a trade, occupation or profession may be regulated by law.”
The movement of South African nurses has remained a sensitive topic since 1995. It is a matter that evokes public
interest irrespective of the accuracy or inaccuracy of reports about it. The issue that evokes most public emotions is per-ceived emigration by highly skilled nurses. On 2 February 2016, a local newspaper published the following story with the headline “Nurses leaving SA in droves”:
More and more South African nurses are taking their skills and knowledge abroad for the promise of more pay and better working conditions. This has plunged the country’s healthcare sector and nursing profession deep into crisis, the Pretoria News learnt on Monday. The hardest-hit victims of the exodus are children, the sick, poor and elderly and those who live in areas where healthcare was already scarce, stakeholders said. Hundreds of thousands of well-trained and highly skilled professional nurses were working in countries such as the UK, Canada and Arab countries. (18)
Province SexRegistered
nursesEnrolled nurses
Auxiliary nurses Total Students Pupils Pupil NAs
Mpumalanga
Female 6 621 3 179 3 579 13 379 650 119 74
Male 881 310 245 1 436 341 20 26
Total 7 502 (5.34%)
3 489 (4.74%)
3 824 (5.22%)
14 815 (5.15%)
991 (4.64%)
139 (1.29%)
100 (3.34%)
Northern Cape
Female 2 085 407 978 3 470 196 - 74
Male 199 45 97 341 68 - 43
Total 2 284 (1.62%)
452 (0.61%)
1 075 (1.47%)
3 811 (1.33%)
264 (1.24%)
- (0%)
117 (3.91%)
North West
Female 8 555 3 095 4 430 16 080 1 585 329 67
Male 1 290 329 579 2 198 486 37 17
Total 9 845 (7.00%)
3 424 (4.66%)
5 009 (6.83%)
18 278 (6.36%)
2 071 (9.71%)
366 (3.4%)
84 (2.81%)
Western Cape
Female 15 841 6 516 7 967 30 324 2 229 704 246
Male 1 294 435 571 2 300 552 104 29
Total 17 135 (12.19%)
6 951 (9.45%)
8 538 (11.64%)
32 624 (11.35%)
2 781 (13.03%)
808 (7.5%)
275 (9.2%)
100% of workforce 140 598 73 558 73 302 287 458 21 339 (7.5%) 2 990
(%) of national nursing workforce in each column.
TABLE 13. (continued)

20 FROM BRAIN DRAIN TO BRAIN GAIN:
However, close scrutiny of SANC records (letters of veri-fication) revealed the opposite. Over the past five years, only 2158 requests for letters of verification were processed by SANC. Table 14 provides a breakdown of numbers by country.
The numbers of foreign nurses in South Africa (as regis-tered by SANC) and percentages of total South African
nursing stock were 488 (0.378%) for 2013, 501 (0.376%) for 2014, 388 (0.284%) for 2015, and 501 (0.356%) for 2016. These have been calculated for categories 1 to 5 and 8 to 9 of table 16 and fall within the RN/RM regis-tration category of SANC. Some of these foreign nurses are recruited under special permit conditions to work in private hospitals, such as those operated by Netcare. Zimbabwe also contributes to the pool of foreign nurses.
TABLE 14. REQUESTS FOR LETTERS OF VERIFICATION WITH COUNTRY DESTINATIONS, 2012–2016
Country 2012 2013 2014 2015 2016 5-year totals
Abu Dhabi 25 13 31 7 12 88
Australia 106 43 66 54 75 344
Bahrain – 9 2 3 3 17
Botswana 7 – – – – 7
Canada 33 21 33 1 1 89
Ireland 3 4 11 10 15 43
Namibia 17 7 15 5 10 54
New Zealand 41 10 20 26 37 134
Qatar 12 – – – – 12
United Kingdom 45 21 59 81 132 338
United States of America 59 23 18 62 78 240
Zimbabwe – – – – 7 7
Other countries 30 14 101 127 98 370
Agencies – – 230 83 102 415
Totals 378 165 586 459 570 2 158
Source: SANC, 2017.
TABLE 15. FOREIGN NURSES REGISTERED BY SANC, BY CATEGORY, 2012–2016
Programme 2012 2013 2014 2015 2016 5-year Totals
1. General nurse – 373 426 313 419 1 531
2. General nurse and psychiatry – 4 4 6 4 18
3. General nurse and midwifery/accoucheur – 102 62 50 71 285
4. Psychiatric nursing science – 3 – 2 1 6
5. Midwifery – 4 8 17 6 35
6. Enrolled nurse – 3 5 4 2 14
7. Enrolment as a nursing auxiliary – 2 1 4 – 7
8. General nurse, psychiatric nurse and midwife – 1 1 – – 2
9. General nurse, midwife community health – 1 – – – 1

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 21
The fact that a nurse has requested that a verification be sent to a potential employer or a recruitment agency does not necessarily mean that she or he has taken up the offer of a position in another country. The news report cited above (18) is also contradicted by other empirical studies that have been conducted on health worker mi-gration in South Africa. Based on their study, Labonté et al. concluded that even though in the recent past South Africa’s health worker shortages as a result of emigration were viewed as significant and harmful, currently domes-tic policies to improve health care and the health work-force, including such innovations as new skilled health worker cadres and Occupation-Specific Dispensation policies, appear to have served to decrease skilled health worker shortages to some extent (17). They further observed that there are indications that South African
skilled health workers primarily use migratory routes for professional development, suggesting that health worker shortages as a result of permanent migration no longer pertain to South Africa. Temporary migration of South African health professionals motivated by professional development and short-term financial reasons is an es-tablished phenomenon (2).
Recent research suggests that “moonlighting” (having a second job in addition to a primary job) is a predictor of nurses’ intention to leave South Africa (19). This re-search is also inconclusive about the real migration of nurses out of South Africa, either on a temporary or on a long-term basis. However, the most promising initi-atives to mitigate health worker migration and associ-ated shortages of health workers are those undertaken
TABLE 16. STRATEGIES TO MITIGATE HEALTH WORKER MIGRATION AND ADDRESS HEALTH WORKER SHORTAGES IN SOUTH AFRICA
Scope Strategy
Global agreements Commonwealth Code (2003)
Health Worker Migration Initiative (2007)
WHO Global Code of Practice on the International Recruitment of Health Personnel (2010)
Domestic policy statements on migration South Africa’s policy statements on health worker immigration (2001, 2006)
Bilateral agreements United Kingdom/South Africa memorandum of understanding (2003)
Cuba (1996)
Germany
Tunisia (1999 and 2007 technical agreements)
Islamic Republic of Iran (2004)
United States PEPFAR/Medical and Nursing Education Partnership Initiative (2013)
Destination country agreements with potential to impact South African migrants
United Kingdom Code of Practice for the Ethical Recruitment of International Healthcare Professionals (2004)
South African initiatives to prevent migration by improving health system human resources for health and living and working conditions for health workers
Examples include:• increasing skilled health worker production• student sponsorship programmes• community service programme• new skilled health worker cadres• task shifting• African health placements• Occupation-Specific Dispensation
Source: Labonté et al. (17).

22 FROM BRAIN DRAIN TO BRAIN GAIN:
within South Africa itself through the improvement of health system human resources for health and living and working conditions for health workers (17). Several ac-tions have been undertaken internally and are reported to have led to a decline in the numbers of nurses wishing to work overseas. Table 16 summarizes strategies to mit-igate health worker migration and address health worker shortages in South Africa.
One of the key retention strategies was the introduction of the Occupation-Specific Dispensation, which was de-vised as an incentive strategy to attract and retain health professionals within the public health service. Whilst many researchers and professionals alike regarded it as purely a financial incentive, it was meant to address other aspects beyond salary, for example by encouraging new career paths, helping to manage career progression and contributing to performance management. The first professional group to benefit from this strategy was the nurses. It is reported to have stemmed, but not halted, the tide of unmanaged movement of nurses into and out of South Africa. From a purely financial perspective, the movement of nurses has not been dented and the system has its critics (20). Criticism of the system can be part-ly attributed to an interpretation of policy interventions only in terms of the financial gain for individual prac-titioners. It has been reported in literature that salary alone is a poor retention incentive for health profession-als. Good working conditions, including availability of medicines and other tools of trade, are key measures to retaining health professionals.
The practice whereby individual nurses seek extra in-come by holding a second, temporary job, termed moonlighting, has been reported as prevalent in South Africa (19, 20). This is despite the OSD appearing to have lowered the risk of health workers migrating due to low salaries (21). Moonlighting is defined as occurring when no permission has been granted by the employing department for a professional to engage in private remu-nerative work. In the survey, all the employer partici-pants reported that they allowed nurses to engage in pri-vate work on condition that the criteria were fulfilled as legislated by section 30 of the Public Service Act No. 103 of 1994, as amended. This section allows government employees to engage in remunerative work outside pub-lic service provided that there is no conflict of interest.
12. DiscussionSouth African nurse training is esteemed for the high standard of training it offers its practitioners, a quality that renders them prime candidates for recruitment (22). The nursing profession, in common with the teaching profession and police training, has for a long time been easier to access by ordinary South Africans than other fields of study, such as law, engineering, medicine, pharmacy, and dentistry. Nursing has over the years been the first point of contact that patients have with a health system. Nurses are found in every health facility across the country and play a vital role in the delivery of health services, from PHC to highly specialized medical interventions. Their training is extensive, in line with the demanding accreditation criteria set by SANC for nursing education institutions. SANC has recently revised the competencies of nurse educators to include the following key elements: (a) scholarship of teaching and learning; (b) academic and student management; (c) curriculum development; (d) management and leadership; (e) personal development of the nurse educator; and (f) research and knowledge creation (23).
These are some of the criteria being utilized when nursing education institutions are accredited for nurse training. Nursing education takes place in a complex institutional environment, which includes 20 out of 23 public universities, 12 public sector nursing colleges (with numerous satellite training campuses) that are the responsibility of the nine provincial health departments, a nursing college run by the defence force, private nursing colleges run by the three major private hospital groups in South Africa, and private nursing schools that are run for profit (24). These education institutions provide the nursing workforce, the majority of whom are employed in public health facilities. Their employment is linked to the bursary agreements wherein nurses who received government funding assistance are required to serve the public through employment by provincial Departments of Health. Such bondage assists in reducing the unemployment of nurses.
Despite the high level of training of midwives, the letters of verification are requested for confirmation of the nurse’s competence as a general nurse, not as a midwife.

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 23
Consequently, it can be assumed that nurses’ movements are based on their basic nursing competencies, except those of highly specialized categories such as critical care, intensive care unit and theatre nursing. The prevalence of the moonlighting phenomenon can be attributed to a desire by health professionals generally to augment their salaries. This practice also exists in other professions, such as medicine, where it is termed “remunerative work outside public service”. All provincial nursing directors reported that this practice is officially allowed on condition that the services provided in the private health facilities do not conflict with the nurse’s normal duties. They however concede that it is a practice that is very difficult to control or monitor.
Whilst the movement of nurses to other countries appears insignificant in terms of recorded verifications,
it is the moonlighting phenomenon that must be addressed. The number of persons registered by SANC forms the largest proportion of all those registered by all three statutory health councils – SANC, 401 543 (57.93%); Health Professions Council of South Africa, 249 827 (36.05%); and the South African Pharmacy Council, 41 745 (6.02%). This indicates the need for the implementation of the National Health Insurance system to be heavily reliant on (a) the continued production of highly qualified nurses; (b) equitable distribution of qualified nurses between urban and rural public health facilities; and (c) ensuring that effective retention strategies for nurse practitioners are in place, especially for rural hospitals and clinics.
Another notable finding is the variance between registration of nurses by SANC per province versus the
TABLE 18. NURSE/MIDWIFE RESIGNATIONS ACROSS PROVINCES, 2012–2016
Province 2012 2013 2014 2015 2016
Eastern Cape 1 121 (19 051)[5.88%]
1 069 (19 067)[5.61%]
1 562 (18 330)[8.52%]
1 226 (19 226)[6.38%]
(19 432)[%]
Free State 309 (6 900)[4.48%]
410 (7 138)[5.74%]
469 (5 166)[9.08%]
446 (6 737)[6.62%]
(6 820)[%]
Gauteng 1 106 (24 784)[4.46%]
1 302 (24 909)[5.23%]
1 925 (25 017)[7.69%]
1 649 (26 173)[6.30%]
(27 245)[%]
KwaZulu Natal 1 738 (30 846)[5.63%]
1 418 (32 782)[4.33%]
2 649 (33 186)[7.98%]
1 902 (33 585)[5.66%]
(34 419)[%]
Limpopo 407 (18 321)[2.22%]
329 (18 245)[1.80%]
422 (18 164)[2.32%]
825 (18 192)[4.53%]
(18 675)[%]
Mpumalanga 302 (7 862)[3.84%]
409 (7 850)[5.21%]
660 (8 272)[7.99%]
432 (8 327)[5.19%]
(8 523)[%]
Northern Cape 124 (2 496)[4.97%]
187 (2 474)[7.56%]
362 (2 478)[14.61%]
228 (2 439)[9.34%]
(2 558)[%]
Western Cape 882 (12 044)[7.32%]
871 (12 321)[7.07%]
1 513(11 531)[13.12%]
1 272(12 583)[10.11%]
(12 867)[%]
Numbers in parentheses ( ) represent total numbers employed; numbers in brackets [ ] represent percentage resignations. No data on resignations retrieved for 2016.
Source: Vulindlela 10/2017.

24 FROM BRAIN DRAIN TO BRAIN GAIN:
total employment numbers as supplied by the Vulindlela human resource system in public service. Vulindlela, a derivative of the payroll system in public service, provides employment figures relating to financial years. Table 18 shows a number of data gaps that were experienced when extracting figures for the present study; for example, the North West province did not show any resignation record for the years 2012 to 2016. This is most likely due to a system glitch. The 2016/2017 figures could also not be reliably extracted. The option would therefore be to do a headcount at provincial level to obtain accurate figures. However, provincial Departments of Health also rely on the Vulindlela system, which does not make a separation between a registered nurse and a midwife. This is one aspect that the nursing profession has to work on and clarify because not every nurse is a midwife, even though many have midwifery skills. The employment system records a nurse generically as “registered nurse” and does not separate that from a midwife. This will hopefully be addressed through the new nursing qualifications and creation of a nurse specialist register. There is also a need to devise a mechanism for matching data between SANC, provincial Departments of Health and private sector employers.
Direct measurement of the movement between the public and private sectors, and in and out of the country, will require good cooperation between the government and SANC. This should yield better data and information, but discussions regarding such attempts should include the leadership of health professional associations. This is to allay fears of perceived victimization by the professionals (2). From a nursing perspective, there is an urgent need to address leadership in all respects, building on the successful establishment of the post of Chief Nursing Officer. A lack of emphasis on leadership development in nursing education and its professional associations, meaning that not enough nurses have the background to assume prominent roles in addressing South Africa’s health care policy issues, is a serious concern (25). In the long run, addressing nursing leadership development will address the problem reported in a previous study by Ditlopo et al. that nurses’ participation in policy-making is both contested and complex, and that there is a disjuncture between nursing leadership and front-line nurses in their levels of awareness of nursing policies (26).
Migration patterns between the public and private health nursing sectors are difficult to quantify. The moonlighting practice, even though not officially sanctioned, enables nurses to work in both sectors without losing their formal employment. However, for those who officially leave the public health service, several reasons have been advanced. The most prevalent reasons provided for resignation from the public health service by nurses relate to (a) increasing workloads, with midwives reporting inability to cope with the increasing pressure of work, especially where there is a shortage of medical doctors, thus placing more pressure on their practice; (b) financial constraints attributed to inability to manage finances, including payments for housing loans, school fees and other necessities; (c) accessing pension funds, whereby some nurses resign with the intention of accessing their pension and applying for re-employment; (d) negative practice environments compounded by lawsuits, especially in the obstetric units, which is again linked to the shortage of medical doctors who would normally shoulder responsibility; and (e) moving to the private health sector with a belief that private hospitals have lighter workloads, fewer patients and more doctors to support in the clinical management of patients.
There are variations in the requirements for nurses that wish to return to the public health service. One province reported requiring the returning nurse to provide a certificate of service, whilst two other reported no requirement to prove competencies. Instead, midwives are oriented on assuming duties in the relevant department. The midwife has to attend in-service training, including in such activities as fire drills and essential steps in the management of obstetric emergencies (ESMOE), in order to raise their professional competencies. There is no prescribed format through which nurses returning to the public health service are assessed to establish whether they still have the requisite competencies.
South Africa needs to improve the involvement of nursing education institutions and nursing directorates in nursing workforce planning. Production of nurses without involvement of these critical organs hampers the equitable distribution of nursing services across the country. Only the Western Cape nursing directorate reported a purposeful participation in nursing workforce

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 25
planning, whilst others, such as KwaZulu-Natal and North West, reported no participation. This lack of uniformity has implications for the prioritization of financial resources to fund nursing in the country. The private nursing schools continue to produce significantly higher numbers of nurses in the EN and ENA categories, which are largely utilized in the private hospitals. There is a view in health policy circles that the high production of nurses in those categories is driven by commercial interests rather than a linkage to health service delivery needs.
On the issue of migration trends, all provinces reported that when a nurse decides to resign, there is no mechanism by which the employer is informed where the nurse has sought employment. The only entity that has the ability to establish that is SANC, though the method applied also has its limitations. The actual numbers of nurses requesting letters of good standing, which enable nurses to obtain employment overseas, do not portray a serious exodus of South African nurses. However, the Organisation for Economic Co-operation and Development (OECD) has recently reported an increase in the expatriation rate for nurses in South Africa from 12.6% in 2000/2001 to 16.5% in 2010/2011 (27). Whilst the OECD figures were for a decade prior to the decade measured for this study, it points to disjuncture between OECD and SANC data. The expatriation rate of South African nurses as observed in OECD countries could be a result of several factors, among them circulation within these countries following initial exit from South Africa. Previous studies have alluded to a decrease in the movement of South African nurses out of the country due in part to certain policy successes (17). An argument against the expatriation rate increase is another observation that the economic crisis that started in 2007/2008 had varying effects on international flows of migrant health workers, in that some countries recruited fewer international health care professionals as they set limits on their health systems’ financial resources (27). This necessitates efforts at direct measurement of migration trends from source countries rather than at the host country.
This will have its own limitations, especially in the South African environment, where those who wish to
move and explore other working environments may interpret the effort as aimed at curbing their freedom of movement – a constitutional guarantee in South Africa. Attempts at getting South African expatriate nurses in both the United Arab Emirates and the United Kingdom to participate in the survey for this study failed. The reasons advanced included scepticism about a possible unintended consequence of the survey results, namely a reduction in the freedom of movement of professionals. This was despite the aims of the Global Code being made clear to potential participants. This fear has roots in the political history of South Africa where, before 1994, freedom of movement, especially of black professionals, was severely curtailed. Indirect measures of movements by South African nurses and other health professionals, including doctors, pharmacists and physiotherapists, have not provided the health policy-makers with better information and understanding of the magnitude of migration trends. New mechanisms have to be devised to achieve the objective.
13. ConclusionMeasuring the migration trends of nurses is critical for the provision of health services in South Africa from a workforce planning and human resource deployment perspective. Over the years indirect measures have been attempted, particularly for medical doctors and nurses. However, these remain inaccurate, as some professionals choose to keep their registrations active in some overseas countries to facilitate temporary work stints, as revealed by the Royal College of Surgeons in Ireland study on medical doctors (28). Migration, whether temporary or permanent, has an impact on resource planning of the national health system, impacting the production of nurses (education and training numbers) and service provision (number and skills base of nurses deployed at health facilities). The funding of nursing education and training within the public nursing colleges is in line with the country’s policy thrust on access to education and attempts at alleviating poverty. The provision of bursaries to nursing students assists them and their families by reducing the burden of training fees.
Whilst the government is providing funding for nurse training at college level, the area of nursing workforce

26 FROM BRAIN DRAIN TO BRAIN GAIN:
planning requires attention. Only one nursing college, located within a Department of Health, reported being actively engaged in workforce planning. Other public nursing colleges seem not to be involved, calling into question the role of directors of nursing in the respective provincial departments. Data accuracy remains a problem for the regulatory bodies, despite the critical role that the deployment of health professionals will play in the health sector reform initiatives of the Ministry of Health. The National Health Insurance scheme is predicated on appropriate staffing of public health facilities with highly qualified health professionals, with nurses playing a leading role. The current Re-engineering of Primary Health Care is heavily reliant on the nursing profession to make its three pillars functional. Observing, measuring and managing the migration trends of nurses is of major relevance to how the South African health system undertakes nursing workforce planning.
The following recommendations are made:
1. SANC to establish a register of nurses who work overseas. This could be achieved through collaboration with sister nursing regulatory bodies in countries such as Australia, New Zealand and the United Kingdom by matching data on an annual basis.
2. A mechanism for monitoring migration trends of nurses to be established through the involvement of SANC, the Ministry of Health and the Department of Home Affairs. The Department of Home Affairs already has a mechanism for determining priority skills among immigrants that seek employment in South Africa.
3. A separate register for nurses who are not in active practice to be established at SANC. Calculating the attrition rate due to retirement and death is important for workforce planning.
4. The registration categories to be aligned to the new nursing qualifications such that it is easy to distinguish midwives from those who may possess midwifery skills but are not applying those skills in their daily work environment, for example in a mental health facility.
5. A collaboration to be set up with other statutory health councils for mapping out accurately where registered practitioners are employed.
6. A mechanism to be devised for matching nursing workforce data between SANC, provincial Departments of Health and private sector employers.
7. Active engagement to be practised between SANC, nursing education institutions and provincial Departments of Health for nursing workforce planning.
8. SANC to become the custodian migration monitoring body for nurses, whose role should include the contextual relationship with the Department of Health to meet the reporting requirements of the Global Code.
9. SANC to regularly interact with nursing regulators in countries where most South African nurses regularly seek employment for the purpose of comparing statistics on requests for verification letters and actual employment. This will provide a better measure of actual migration than indirect estimates.
10. SANC and the Ministry of Health to engage nursing professional associations to impress on them the need for monitoring migration trends as one of the mechanisms to positively influence nursing planning and eventually education, training and deployment.
11. SANC to engage the recruitment agencies to improve the request form for letters of good standing (verification letters) so that the intended destination country or countries are declared in the form.
AcknowledgementsThe African Institute of Health and Leadership Development wishes to express its appreciation for the support given to this project by the Global Health Workforce Alliance through the funding provided by the European Commission in support of the implementation of the WHO Global Code of Practice on the International Recruitment of Health Personnel.

NURSING AND MIDWIFERY MIGRATION TRENDS IN THE SOUTH AFRICAN HEALTH SYSTEM 27
References 1. Mahlathi P, Dlamini J. Minimum data sets for hu-
man resources for health and the surgical workforce in South Africa’s health system: a rapid analysis of stock and migration. African Institute of Health and Leadership Development; 2015.
2. Mahlathi P, Dlamini J. From Brain Drain to Brain Gain: understanding and managing the movement of medical doctors in the South African health system. African Institute of Health and Leadership Development; 2016.
3. Mid-year population estimates. Pretoria: Statistics South Africa; 2017.
4. Growth in registers of the SANC 2016. South African Nursing Council (www.sanc.co.za, accessed 24 October 2017).
5. OECD health statistics 2014: how does South Africa compare? Paris: Organisation for Economic Co-operation and Development; 2014.
6. Naidoo S. The South African National Health Insurance: a revolution in health care delivery! Journal of Public Health. 2012;34(1):149–50.
7. Human Resources for Health Strategy. Pretoria: Ministry of Health; 2011.
8. WHO Global Code of Practice on the International Recruitment of Health Personnel. WHA63.16. Geneva: World Health Organization; 2010 (http://apps.who.int/gb/ebwha/pdf_files/WHA63/A63_R16-en.pdf, accessed 24 October 2017).
9. National Qualifications Framework Act No. 67 of 2008, as amended. Government of South Africa.
10. Uys LR, Klopper HC. What is the ideal ratio of categories of nurses for the South African public health system? South African Journal of Science. 2013;109(5/6): Art. a0015. http://dx.doi.org/10.1590/sajs.2013/a0015, accessed 24 October 2017).
11. Nursing education and training standards. South African Nursing Council; 2016 (www.sanc.co.za, accessed 24 October 2017).
12. Policy guidelines regarding registration of inter-nationally qualified nurses and midwives and/or foreign qualifications with South African Nursing Council. South African Nursing Council; 2016.
13. Blaauw D, Ditlopo P, Maseko F, Chirwa M, Mwisongo A, Bidwell P et al. Comparing the job satisfaction and intention to leave of different categories of health workers in Tanzania, Malawi, and South Africa. Global Health Action. 2013;6:19287. doi:10.3402/gha.v6i0.19287.
14. van Rensburg JC. South Africa’s protracted strug-gle for equal distribution and equitable access: still not there. Human Resources for Health. 2014;12:26 (http://www.human-resources-health.com/content/12/1/26, accessed 24 October 2017). doi:10.1186/1478-4491-12-26.
15. Clemens MA, Pettersson G. New data on African health professionals abroad. Human Resources for Health. 2008;6:1. doi:10.1186/1478-4491-6-1.
16. Awases M, Gbary A, Nyoni J, Chatora R. Migration of health professionals in six countries: a synthesis report. Brazzaville: World Health Organization; 2004.
17. Labonté R, Sanders D, Mathole T, Crush J, Chikanda A, Dambisya Y et al. Health worker migration from South Africa: causes, consequences and policy responses. Human Resources for Health. 2015;13:92. doi:10.1186/s12960-015-0093-4.
18. Makhubu N. Nurses leaving SA in droves. IOL news, 2 February 2016 (https://www.iol.co.za/news/south-africa/gauteng/nurses-leaving-sa-in-droves-1978572, accessed 25 October 2017).
19. Rispel LC, Blaauw D. The health system consequenc-es of agency nursing and moonlighting in South Africa. Global Health Action. 2015;8:26683.
20. Ditlopo P, Blaauw D, Rispel L, Thomas S, Bidwell P. Policy implementation and financial incentives for nurses in South Africa: a case study on the Occupation Specific Dispensation. Global Health Action. 2013;6:138–46.
21. George G, Atujuna M, Gow J. Migration of South African health workers: the extent to which financial considerations influence internal flows and exter-nal movements. BMC Health Services Research. 2013;13:297.

28 FROM BRAIN DRAIN TO BRAIN GAIN:
22. Xaba J, Phillips G. Understanding nurse recruit-ment: fi nal report. Pretoria: Democratic Nursing Organization of South Africa (DENOSA); 2001.
23. Competencies for a nurse educator. South African Nursing Council (www.sanc.co.za, accessed 25 October 2017).
24. Rispel LC. Transforming nursing policy, practice and management in South Africa. Global Health Action. 2015;8:28005 (http://dx.doi.org/10.3402/gha.v8.28005, accessed 25 October 2017).
25. Transforming health care in South Africa: a summary evaluation of the Atlantic Philanthropies’ Nursing Programme. Atlantic Philanthropies; 2014.
26. Ditlopo P, Blaauw D, Penn-Kekana L, Rispel LC. Contestations and complexities of nurses’ participa-tion in policy-making in South Africa. Global Health Action. 2014;7:25327 (http://dx.doi.org/10.3402/gha.v7.25327, accessed 25 October 2017).
27. International migration outlook 2015. Paris: Organisation for Economic Co-operation and Development; 2015 (http://dx.doi.org/10.1787/migr_outlook-2015-en, accessed 25 October 2017).
28. Brugha R, Walsh A. Brain Drain to Brain Gain: Ireland’s two-way flow of doctors. Ireland country case study, Year 2. Royal College of Surgeons in Ireland; 2017.


For further information, please contact:African Institute of Health and Leadership Development
181 Lancia Street, Lynnwood Ridge,
0081 Pretoria, South Africa
www.selizwe.co.za





























