Embed Size (px)
Citation preview

WHO Osteoporosis Definition (1996)
“A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration, with a consequent increase in bone fragility with susceptibility to fracture.”*
Bone density T-score 2.5 SD below young normal mean†
*Consensus Development Conference: Diagnosis, prophylaxis, and treatment of osteoporosis, Am J Med 1993;94:646.† Kanis JA et al, J Bone Miner Res 1994;9:1137.

Who Is At Risk?Who Is At Risk?
• Early menopause, surgical menopause• Low body weight compared to height• Diet - low intake of milk products and lack of
vitamin D• Life-style factors: cigarette smoking, caffeine,
alcohol abuse, lack of exercise• Drugs and diseases, corticoseroid treatment,
hyperthyroidism, anorexia nervosa, amenorrhoea, arthritis
• Genetic factors (family history, race)
• Early menopause, surgical menopause• Low body weight compared to height• Diet - low intake of milk products and lack of
vitamin D• Life-style factors: cigarette smoking, caffeine,
alcohol abuse, lack of exercise• Drugs and diseases, corticoseroid treatment,
hyperthyroidism, anorexia nervosa, amenorrhoea, arthritis
• Genetic factors (family history, race)

Bone turnover Bone turnover
Trabecular bone20% of the skeletal mass80% of bone turnover
Cortical bone80% of the skeletal mass20% of bone turnover

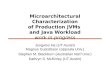
Bone Loss or Low Peak Bone MassBone Loss or Low Peak Bone Mass
Age (years)
Re
lati
ve
Bo
ne
Ma
ss(%
ide
al p
eak
bo
ne
mas
s)
80
60
40
20
20 30
40
50
60
70
80
100
Low Peak
Fast Loss
Normal

OsteoporosisOsteoporosis
0.600
0.700
0.800
0.900
1.000
1.100
1.200
20 40 60 80 100
Female
Male
Age (years)

INDICATIONS FOR BONE MINERALDENSITY (BMD) TESTING
INDICATIONS FOR BONE MINERALDENSITY (BMD) TESTING
• Women aged 65 and older
• Postmenopausal women under age 65 with risk factors
• Men aged 70 and older
• Adults with a fragility fracture
• Adults with a disease or condition associated with low bone mass or bone loss
• Adults taking medications associated with low bone mass or bone loss
• Anyone being considered for pharmacologic therapy
• Anyone being treated, to monitor treatment effect
• Anyone not receiving therapy in whom evidence of bone loss would lead to treatment
• Women discontinuing estrogen
• Women aged 65 and older
• Postmenopausal women under age 65 with risk factors
• Men aged 70 and older
• Adults with a fragility fracture
• Adults with a disease or condition associated with low bone mass or bone loss
• Adults taking medications associated with low bone mass or bone loss
• Anyone being considered for pharmacologic therapy
• Anyone being treated, to monitor treatment effect
• Anyone not receiving therapy in whom evidence of bone loss would lead to treatment
• Women discontinuing estrogen
INTERNATIONAL SOCIETY FOR CLINICAL DENSITOMETRY, Official position 2005

Bone DensitometryBone Densitometry

Bone DensitometryBone Densitometry
• Non-invasive test for measurement of BMD
• Major technologies– Dual-energy X-ray Absorptiometry (DXA)– Quantitative Ultrasound (QUS)– Quantitative Computerized Tomography
(QCT)
• Many manufacturers• Numerous devices• Different skeletal sites
• Non-invasive test for measurement of BMD
• Major technologies– Dual-energy X-ray Absorptiometry (DXA)– Quantitative Ultrasound (QUS)– Quantitative Computerized Tomography
(QCT)
• Many manufacturers• Numerous devices• Different skeletal sites

Dual energy X Ray absorptiometry

DXA TechnologyDXA Technology
X-ray Source (produces 2 photon energies with different attenuation profiles)
Photons Collimator (pinhole for pencil beam, slit for fan beam)
Patient
Detector (detects 2 tissue types - bone and soft tissue)
Very low radiation to patient.
Very little scatter radiation to technologist

DXADXA
• “Gold-standard” for BMD measurement• Measures “central” or “axial” skeletal sites: spine
and hip• May measure other sites: total body and forearm• Extensive epidemiologic data• Correlation with bone strength in-vitro• Validated in many clinical trials • Available
• “Gold-standard” for BMD measurement• Measures “central” or “axial” skeletal sites: spine
and hip• May measure other sites: total body and forearm• Extensive epidemiologic data• Correlation with bone strength in-vitro• Validated in many clinical trials • Available

• What is measured?– BMC: Bone Mineral Content (g)– BMD: Bone Mineral Density (g/cm²)
– T-score: BMD compared to young normal– Z-score: BMD compared to same age
• What is measured?– BMC: Bone Mineral Content (g)– BMD: Bone Mineral Density (g/cm²)
– T-score: BMD compared to young normal– Z-score: BMD compared to same age
Dual-energy X-ray absorptiometry (DXA)
Dual-energy X-ray absorptiometry (DXA)

What DXA Really MeasuresWhat DXA Really Measures
• “Areal” BMD is calculated in g/cm2
• “T-score” compares the patient’s BMD with the young-normal mean BMD and expresses the difference as a standard deviation (SD) score
• “Areal” BMD is calculated in g/cm2
• “T-score” compares the patient’s BMD with the young-normal mean BMD and expresses the difference as a standard deviation (SD) score

DXADXA
0.600
0.650
0.700
0.750
0.800
0.850
0.900
0.950
1.000
1.050
1.100
20 30 40 50 60 70 80 90
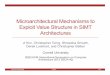
T=-3,1
Peak Bone Mass = 1.047
Z=-0,4BMD = 0.700
AGE = 80
T-score and Z-score

T-scoreT-score
Example:
T-score = 0.7 g/cm2 - 1.0 g/cm2
0.1 g/cm2= - 3.0
Patient’s BMD – Young-Adult Mean BMD
1 SD of Young-Adult Mean BMD
Patient’s BMD – Young-Adult Mean BMD
1 SD of Young-Adult Mean BMD

Z-scoreZ-score
Low Z-score (less than -2.0) may suggest increased likelihood of secondary osteoporosis, however . . .– This is not validated in clinical trials– High index of suspicion for secondary causes of
osteoporosis is suggested in all patients
Low Z-score (less than -2.0) may suggest increased likelihood of secondary osteoporosis, however . . .– This is not validated in clinical trials– High index of suspicion for secondary causes of
osteoporosis is suggested in all patients
Patient’s BMD – Age-Matched Mean BMD
1 SD of Age-Matched Mean BMD in g/cm2

DXADXA
WHO definition of diagnostic categories
– Normal: T > -1– Osteopenia: -1 > T > -2,5– Osteoporosis: - 2,5 > T– Severe osteoporosis: plus fracture
WHO definition of diagnostic categories
– Normal: T > -1– Osteopenia: -1 > T > -2,5– Osteoporosis: - 2,5 > T– Severe osteoporosis: plus fracture
Which Skeletal Sites Should Be Measured?
Spine L1-L4
Hip (Total Proximal Femur, Femoral Neck)
Use lowest T-score of these sites

AP SpineAP Spine

AP FemurAP Femur



Diagnosis CaveatsDiagnosis Caveats
• T-score -2.5 or less does not always mean osteoporosis (osteomalacia)
• Clinical diagnosis of osteoporosis may be made with T-score greater than -2.5• Example: atraumatic vertebral fracture with T-score
equals -1.9
• Low T-score does not identify the cause• Medical evaluation should be considered• Example: celiac disease with malabsorption
• T-score -2.5 or less does not always mean osteoporosis (osteomalacia)
• Clinical diagnosis of osteoporosis may be made with T-score greater than -2.5• Example: atraumatic vertebral fracture with T-score
equals -1.9
• Low T-score does not identify the cause• Medical evaluation should be considered• Example: celiac disease with malabsorption

Diagnosis CaveatsDiagnosis Caveats
• BMD measurements are not accurate in patients with
• degenerative disease• compression fractures• Soft tissue calcifications• Metallic hardware
• BMD measurements are not accurate in patients with
• degenerative disease• compression fractures• Soft tissue calcifications• Metallic hardware

Why T-score And Not Z-score?Why T-score And Not Z-score?
• T-score is related to bone strength
• T-score is related to fracture risk
• Using Z-scores would result in many “normal”
patients having fragility fractures, and suggest
that osteoporosis does not increase with age
• T-score is related to bone strength
• T-score is related to fracture risk
• Using Z-scores would result in many “normal”
patients having fragility fractures, and suggest
that osteoporosis does not increase with age

T-score DiscordanceT-score Discordance
• Different skeletal sites have different peak bone mass at different times and lose bone at different rates
• Different machines• Different ROIs• Different reference databases have different means and
SD (the hip is the only skeletal site with a standardized reference database used by all manufacturers – National Health and Nutrition Examination Survey III)
• Different skeletal sites have different peak bone mass at different times and lose bone at different rates
• Different machines• Different ROIs• Different reference databases have different means and
SD (the hip is the only skeletal site with a standardized reference database used by all manufacturers – National Health and Nutrition Examination Survey III)

Why -2.5?Why -2.5?
“Such a cutoff value identifies approximately 30% of postmenopausal women as having osteoporosis using measurements made at the spine, hip or forearm. This is approximately equivalent to the lifetime risk of fracture at these sites.”
“Such a cutoff value identifies approximately 30% of postmenopausal women as having osteoporosis using measurements made at the spine, hip or forearm. This is approximately equivalent to the lifetime risk of fracture at these sites.”
Kanis JA et al. J Bone Miner Res. 1994;9:1137.