Embed Size (px)
Citation preview
WWHHOO ccoonnssuullttaattiioonn oonn tteecchhnniiccaall aanndd ooppeerraattiioonnaall rreeccoommmmeennddaattiioonnss
ffoorr ssccaallee--uupp ooff llaabboorraattoorryy sseerrvviicceess aanndd mmoonniittoorriinngg HHIIVV aannttiirreettrroovviirraall
tthheerraappyy iinn rreessoouurrccee--lliimmiitteedd sseettttiinnggss
GENEVA13-15 December 2004
WWHHOO ccoonnssuullttaattiioonn oonn tteecchhnniiccaall aanndd ooppeerraattiioonnaall rreeccoommmmeennddaattiioonnss
ffoorr ssccaallee--uupp ooff llaabboorraattoorryy sseerrvviicceess aanndd mmoonniittoorriinngg HHIIVV aannttiirreettrroovviirraall
tthheerraappyy iinn rreessoouurrccee--lliimmiitteedd sseettttiinnggss

WHO Library Cataloguing-in-Publication DataWHO Consultation on Technical and OperationalRecommendations for Scale-Up of Laboratory Servicesand Monitoring HIV Antiretroviral Therapy in Resource-Limited Settings (2004: Geneva, Switzerland) WHOconsultation on technical and operational recommenda-tions for scale-up of laboratory services and monitoringHIV antiretroviral therapy in resource-limited settings.
1.Anti-retroviral agents - pharmacology 2.Anti-retroviralagents – supply and distribution 3.Clinical laboratorytechniques – standards 4.Viral load – methods 5.Casereports I.Title.
ISBN 92 4 159368 7 (NLM classification: WC 503.2)
© World Health Organization 2005All rights reserved. Publications of the World Health Organization canbe obtained from WHO Press, World Health Organization, 20 AvenueAppia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translate WHO publications – whether forsale or for noncommercial distribution – should be addressed to WHOPress, at the above address (fax: +41 22 791 4806; email: [email protected]).
The designations employed and the presentation of the material in thispublication do not imply the expression of any opinion whatsoever onthe part of the World Health Organization concerning the legal statusof any country, territory, city or area or of its authorities, or concerningthe delimitation of its frontiers or boundaries. Dotted lines on mapsrepresent approximate border lines for which there may not yet be fullagreement.
The mention of specific companies or of certain manufacturers’ prod-ucts does not imply that they are endorsed or recommended by theWorld Health Organization in preference to others of a similar naturethat are not mentioned. Errors and omissions excepted, the names ofproprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the infor-mation contained in this publication. However, the published materialis being distributed without warranty of any kind, either express orimplied. The responsibility for the interpretation and use of the mate-rial lies with the reader. In no event shall the World HealthOrganization be liable for damages arising from its use.
Printed in
Contacts: Dr C. Gilks, HIV Department, Treatment and Prevention Scale-up Team and Dr G. Vercauteren,Department of Essential Health Technologies, World Health Organization, Avenue Appia 20, 1211 Geneva 27, Switzerland.This document is available on the internet at: www. who.int/hiv/ and.www.who.int/eht/

1WHO DEPARTMENT OF HIV/AIDS
Abbreviations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
I. INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5The public health approach to antiretroviral therapy in resource-limited settings . . . . . . . . . . . . . . . . . . . . 5Review of HIV/AIDS diagnostics and laboratory support activities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
II. SCALE-UP EXPERIENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7a. Kenya . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7b. Senegal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7c. Thailand . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7d. Brazil . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7e. Médecins Sans Frontières . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
III.CLINICAL MONITORING ISSUES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9a. Clinical monitoring of adults . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9b. Clinical monitoring of children . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
IV. LABORATORY TECHNOLOGIES AND MONITORING . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11a. Resistance monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11b. Technologies for resistance monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11c. CD4 technologies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12d. Quality assurance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14e. HIV incidence testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14f. Relevant laboratory technologies in antiretroviral therapy roll-out programmes . . . . . . . . . . . . . . . . . . 14g. HIV/tuberculosis laboratory issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
V. PREQUALIFICATION AND PROCUREMENT ISSUES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17a. UN prequalification process for antiretroviral drugs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17b. UN assessment and selection of appropriate diagnostic technologies . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18c. WHO Contract Procurement Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19d. UNICEF procurement service . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19e. AIDS Medicines and Diagnostics Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19f. Global Fund for AIDS, Tuberculosis and Malaria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
VI.GROUP WORK AND RECOMMENDATIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Group work 1. Review of current laboratory requirements supporting antiretroviral therapy roll-out: clinical experts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Group work 2. Review of current laboratory requirements for antiretroviral therapy roll-out: laboratory experts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Group work 3. Scale-up: What is needed? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Group work 4. Innovative and operational research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Annex 1. Programme of work . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Annex 2. List of participants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35Annex 3. Summary of CD4+ T-cell enumeration technologies: flow cytometry . . . . . . . . 39Annex 4. Summary of CD4+ T-cell enumeration technologies:dedicated and manual assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Annex 5. Summary of main characteristics of viral load technologies based on nucleic acid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41Annex 6. Summary of main characteristics of viral load technologies not based on nucleic acid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
Co n t e n t s

WHO DEPARTMENT OF HIV/AIDS 3
AIDS acquired immunodeficiency syndromeALT alanine aminotransferaseAMDS AIDS Medicines and Diagnostics ServicesART antiretroviral therapyARV antiretroviralCD4 T-lymphocyte CD4+CPS Contract Procurement Services (of WHO)CRF circulating recombinant form (of HIV)CSF cerebrum spinal fluidDART Development of Antiretroviral Therapy in AfricaEDM Essential Drugs and Medicines Policy (WHO Department of)EHT Essential Health Technologies (WHO Department of)ELISA enzyme-linked immunosorbent assayEQA external quality assessmentFBC full blood countGFATM Global Fund for AIDS, Tuberculosis and MalariaGLP good laboratory practiceHb haemoglobinHIV immunodeficiency virusHIVDR HIV drug resistanceMAb monoclonal antibodyMSF Médecins Sans FrontièresMSH Management Sciences for HealthNGO nongovernmental organizationNRL National Serological Reference Laboratory (Australia)NVP nevirapineOEM original equipment manufacturerOI opportunistic infectionPCP Pneumocystis carinii pneumoniaPCR polymerase chain reactionQA quality assuranceQC quality controlQM quality managementRT reverse transcriptase`SOP standard operating procedureSTARHS serologic testing algorithm to detect recent seroconversionSTI sexually transmissible infectionTB tuberculosisUN United NationsUNAIDS Joint United Nations Programme on HIV/AIDSUNFPA United Nations Population Fund UNICEF United Nations Children's Fund VCT voluntary counselling and testing (= T&C: testing and counselling)VL viral loadWHO World Health OrganizationZDV zidovudine
A b b rev i at i o n s


5WHO DEPARTMENT OF HIV/AIDS
WHO consultation on technical and opera-tional recommendations for scaling uplaboratory services and monitoring HIV anti-retroviral therapy (ART) in resource-limited
settings was held on 13-15 December 2004 in Geneva.
Despite the progressive increase in access to HIV anti-retroviral (ARV) drugs in countries with limited resourcespromoted by the 3 by 5 initiative, WHO recognizes thatthe current limitations on laboratory capacity in resource-poor settings can be an important barrier in the way ofreaching the planned treatment target. WHO, as stated inits global HIV ART guidelines for resource-limitedsettings, will work together with the internationalcommunity and countries to improve the laboratory infra-structure at local and regional levels so as to permituniform availability of HIV and CD4 testing, wider avail-ability of automated haemoglobin and chemistry testing,and national availability of viral load (VL) testing, whilethe capacity for HIV drug resistance testing (HIVDR)should be available at regional level. Given current localrealities and future scenarios, this will require choosinguniform, simplified and cost-effective methodologies atthe country level and ensuring supplies of reagents andthe maintenance of equipment.
The aim of the consultation was to obtain clear and realistic guidelines as to which diagnostic and moni-toring schedules were optimal and how they could bedelivered in order to assist decision-making on treatmentand facilitate the implementation of strategies andnecessary actions for scaling up diagnosis and moni-toring at the local, regional and global levels, withparticular emphasis on resource-constrained settings. Itwas required that the resulting recommendations wouldprovide useful tools for the rational implementation ofscaling-up processes, taking into consideration varia-tions between developing countries in human resources,health structures and socioeconomic contexts.
The objectives of the consultation were to:
◗ revise and update recommendations for laboratorymonitoring of ART in line with a public healthapproach to treatment;
◗ review the current status of laboratory technolo-gies relevant to a public health approach to treatment and scale-up issues (availability, cost, performance issues, personnel requirements,reliability, etc.), and to consider them in respect of guidelines for selection and procurement;
◗ review the current status of the WHO system and other systems for assessing the performanceof technologies and reagents relevant to thelaboratory monitoring of ART;
◗ identify the operational and innovative researchagenda for laboratory tools to support wider accessto ART in resource-limited settings.
The consultation was opened by Dr Jim Kim, Director ofthe HIV Department. Dr James Hakim chaired themeeting and Dr John Parry and Dr William Rodriguezserved as rapporteurs.
Dr Kim emphasized the credibility gap that had becomeapparent between HIV prevention activities throughbehavioural change and the inadequate delivery of ARTin resource-poor settings. Since the inception of the 3 by5 initiative, many new alliances had provided a focus foractivity. As a result there was an urgent need to scale upthe public health response. A major deficit in thisresponse concerned access to appropriate laboratorysupport, particularly for the measurement of CD4 cells.It was urgently necessary to scale up the delivery of ARTin order to meet the 3 by 5 target, and doing so was highlydependent on simultaneous capacity-building of labora-tory services. Funds were available to facilitate therehabilitation of the laboratory infrastructure and theyhad to be used quickly. The consultation had been organ-ized in order to seek expert advice on the requirementsfor the laboratory support needed to ensure effectivehealth delivery systems.
The public health approachto antiretroviral therapyin resource-limited settingsWHO had adopted a public health approach to ART inresource-poor settings. The need was urgent becausemore than 8000 HIV-infected people died every dayfrom a preventable and treatable disease. The 3 by 5initiative aimed to deliver ART to 3 million eligiblepeople by the end of 2005, and the ultimate goal was toachieve universal access in accordance with need. InJune 2004 only 440 000 individuals were estimated tobe receiving ART. The major challenges were to scale upprevention so as to retard the epidemic and to convertHIV infection from being a fatal condition to being achronic manageable disease by strengthening healthsystems. A public health approach was seen as mostappropriate because there were too few trained physi-cians for an individualistic approach to be adopted and
I . I nt ro d u c t i o n
A

???????6
because laboratory support services were inadequate.Consequently, simplified standard care packages wereneeded for delivery by treatment teams with local adop-tion and adaptation. These packages would include:routine offers of testing and counselling; simplifiedtreatment; opportunistic infection (OI) prophylaxis andregular patient review; first-line and second-line regi-mens; simplified clinical decision-making; simplifiedlaboratory and clinical monitoring; standardized patientregisters, drug cards, etc.; community engagementinvolving adherence and chronic management; and freecare at the point of delivery.
The four key steps in the clinical management of ARTwere discussed, i.e. when to:
start therapy;
substitute for toxicity;
switch following failure;
stop and commence palliative care.
The most difficult decision, for which laboratory supportwas usually required, concerned the time of switching tosecond-line ART. Constraints of time and cost dictatedthat the support should be as simple as possible. WHOdid not recommend VL tests for routine basic patientfollow-up, nor resistance testing for individual patientcare. However, these technologies could be employed forpopulation monitoring.
Review of HIV/AIDS diagnostics and labo-ratory support activities The activities of the WHO Department of EssentialHealth Technologies (EHT) relevant to the ART scale-upinitiative were described. In response to the urgency ofthe 3 by 5 initiative, EHT had extended its HIV diagnos-tics work to activities needed for ART monitoring. Inaddition to the evaluations of HIV screening and diag-nostic tests previously undertaken, WHO had startedcomparative assessments of CD4 measurement tech-nologies and of possible alternative technologies to VLtesting. The development of innovative technologies wasalso being supported. WHO continued to provide tech-nical information and advice by publishing policies andguidelines for laboratory and diagnostic services andthrough advocacy and the sensitization of policy-makers.Essential requirements for HIV/AIDS diagnosticsupport in resource-limited countries were also beingupdated. Access to quality diagnostics, reagents andequipment was facilitated through the WHO Bulk
Procurement Scheme, which provided these commodi-ties at negotiated prices to its Member States. Severaladditional initiatives were supporting the provision ofgood laboratory services. Needs for capacity-buildingwere being met by the development of core curricula andtraining materials along with training-of-trainers work-shops addressing the diverse needs of laboratories at theregional, national and local levels. Laboratory perfor-mance was being monitored by an array of WHOexternal quality assessment (EQA) schemes, includingHIV serology, CD4 counts, haematology and clinicalchemistry. In addition, training in systems of goodquality and supporting quality assurance (QA) activitiesand management were being conducted at the national,regional and district levels.
DiscussionIn some settings, access to ART seemed to be limited bythe high costs of VL testing. It was stated that VL moni-toring was not a requirement for monitoring ART,although prices for VL assays were falling. It was arguedthat manufacturers and suppliers of diagnostics neededinformation about market requirements at the countrylevel and that this would permit price negotiations on thebasis of expected volumes. However, WHO had alwaysmanaged to secure low prices without being committedto volumes or any particular manufacturer. Prices alsooften depended on specific procurement routes: somecountries created additional costs by imposing signifi-cant import duties, and local distributors could alsointroduce substantial mark-ups. Attempts to minimizethese added costs were desirable.
When recommendations were being devised on theappropriateness of technology in different settings,consideration had to be given to the need for rapid accessto spares, maintenance and technical support. Theprocurement of appropriate technologies was oftenimpossible because of an inability to generate local dataensuring well-informed choices and because of a lack ofcommunication between purchasers and users of tech-nology. Moreover, local laboratory management oftenlacked the skills, knowledge and/or motivation to intro-duce technological innovations. It might be necessary tohave a stronger representation of laboratory experts innational AIDS programmes and ministries of health andto pool regional expertise, as with the HIV laboratorynetwork for African countries. Several comments weremade concerning the problems of early diagnosticapproaches for infants.

7WHO DEPARTMENT OF HIV/AIDS
I I . S c a l e - u p ex p e r i e n c e s
a. Kenya The HIV epidemic had a negative impact on all sectors ofKenyan society. Previous health gains had been reversed.Life expectancy at birth had fallen from 62 to 46 years. Inthe medical wards of government hospitals, 50–70% ofbed occupancy was HIV-related. The prevalence of HIV in2003 was estimated to be 7%, equivalent to 1.25 millionKenyans estimated to be HIV-positive, of which 190 000were thought to need ART. The roll-out of ART was goingwell, fostered by clear political commitment at a high level.Strategic and operational plans were developed to supportthe 3 by 5 goal. A pragmatic public health approach to ARVprovision was adopted, based on the development andapplication of national guidelines, standardization andquality control. The national programme aimed to deliverART to 50% (95 000) of eligible people by 2005 and to75% by 2008. In order to achieve these goals it was recog-nized that multisectoral involvement was required andthat it would be necessary to work with various partners.Staff training was recognized as essential for successfulimplementation. The indicators of progress were verygood: substantially increased numbers of people wereseeking voluntary counselling and testing (VCT) and theART sites planned for 2005 were already active in 2004.Nevertheless, there was still a long way to go in order tomeet the need, strengthen the health delivery infrastruc-ture adequately and secure sufficient funding.
b. Senegal It was estimated that the prevalence of HIV in Senegalwas approximately 1.5% (80 000 cases). Pilot studies onthe introduction of ART began in 1998. In order toprepare for ART scale-up a programme of training forrelevant health care personnel had been developed. About450 people had already been trained. A national team hadprovided both theoretical and practical training, and ARTregimens had been harmonized. Further staff develop-ment was undertaken through a system of mentoring.The Government was providing funding for HIV testing,CD4 measurements, OI prophylaxis and ART. The moni-toring of ART encompassed clinical assessment and basiclaboratory tests, including CD4 determinations. Thestructured education of patients on ART concerning theneed for adherence to drug regimens was seen to be a keyelement of successful treatment. Access to VCT wasbeing enhanced: three centres were planned for eachregion and it was intended to introduce antenatal testingand testing at tuberculosis (TB) and sexually transmis-sible infection (STI) clinics. At the time of theconsultation, 2800 patients were receiving ART. It wasintended that 7000 would be doing so by 2006.
c. Thailand It was estimated that more than 1 million persons hadhad HIV infection, almost 600 000 of whom were stillliving with the virus and 61 394 of whom had AIDS.During 2004, approximately 20 000 new infections andnearly 50 000 new AIDS cases were expected. ART wasfirst used in 1992, employing zidovudine (ZDV)monotherapy. The national ART programme wasproviding free ART for HIV/AIDS patients who werecovered by the universal health insurance scheme of theMinistry of Public Health. Patients participating in clin-ical trials or university research projects, or qualifying forthe Social Security Fund Scheme, also obtained free treat-ment. Both treatment-naive and treatment-experiencedpatients were being enrolled on the basis of evidence ofclinical AIDS and/or CD4 measurement. Effective,affordable and manageable drug regimens had beendefined, the more costly regimens having been reservedfor second-line and third-line therapy. Specific trainingprogrammes for ART had been implemented. Protocolsfor the enrolment and management of children had beendeveloped. The planning of associated logistics,including the procurement and supply of drugs, labora-tory diagnostics and equipment, and informationtechnology and data collection, was well developed.During 2004, recruitment to the programme had beenincreased, over 3000 new persons having entered it eachmonth and over 900 hospitals providing ART services. Itwas expected that, by the end of 2004, approximately 50000 patients would be receiving ART. A target of 80 000on ART by the end of 2005 had been set.
d. BrazilThe situation in Brazil possibly differed somewhat fromthat in other countries affected by the HIV epidemic,since Brazil was a middle-income country with anannual per capita gross domestic product of US$ 2998and a life expectancy at birth of 68 years.
In mid 90's the Brazilian Government began to offerfree ARV drugs to all citizens infected with HIV, on thebasis of criteria set by an independent committee. Thetreatment guidelines were more conservative than thosein the USA, e.g. they were CD4-guided, therapy was initi-ated later and dual therapy regimens were accepted(triple therapy became available later). By the end of2002 there were 130 000 people on ARV drugs and, bythe end of 2004, 305 hospitals, 73 day clinics and 166special HIV units had been accredited for HIV care.

???????8
In order to support the national HIV programme, Brazilinvested heavily in laboratories that could perform allHIV-related testing, including both CD4 counts and VLtesting. At the time of the consultation there were 70 CD4 laboratories and 65 laboratories performing VLtesting throughout the country in the public health sector, and many more in the private sector.
The laboratory support programme and ART itself werenot instant successes. In 1997, only 28% of patients onART had VL < 400 copies/ml after six months on treat-ment. By 2004, however, 98% of patients had VL < 400copies/ml after six months. The laboratory programmehad also matured over that period. In 1996, five labora-tory specialists visited HIV laboratories in Canada andreturned to establish the first laboratories dedicated toHIV. This group evolved into a committee that was stillmeeting regularly. The major areas of focus were nolonger on scale-up but on limiting the attrition of trainedtechnologists, who often left for higher-paying positionselsewhere, and on formalizing the QA programme.Quality management (QM) had been an important partof Brazil’s laboratory support programme. Externalquality assurance for CD4 was conducted six times peryear, three in a national programme and three in aninternational programme, so that each laboratory wasassessed every two months. In the public health sector,few tests were done in real time and there were signifi-cant delays in the reporting back of results to the clinicalsites. For people who could afford it there was also a well-established private health sector. In answer to thequestion as to whether the building of capacity or therolling out of programmes should come first, Brazil hadshown that both could be done at the same time.
e. Médecins Sans Frontières Médecins Sans Frontières (MSF) was providing care andtreatment to 23 000 patients at 27 project sites in 23countries. In general, CD4 measurements were used asa tool for starting treatment (baseline) and then formonitoring the efficacy of the treatment regimen everysix months. Total lymphocyte counts were not used asthey were not felt to be sufficiently reliable. The equip-ment used in the MSF programmes includedBecton-Dickinson’s FACSCount (15 programmes),Dynal’s Dynabeads (five programmes) and Partec’sCyFlow (four programmes). In Malawi (Chiradzulu) andMozambique (Tete and Angonia), patients were enrolledon the basis of WHO clinical stages 3 and 4 without theuse of CD4 baseline data.
Four of the 27 MSF projects were measuring VL(Cameroon, Guatemala, South Africa and Thailand) bymeans of either Amplicor (Roche) or NASBA(bioMérieux). The major questions confronting MSF asit considered whether to pursue VL monitoring in itsprojects were as follows.
(1) Was individual monitoring of VL a viable option?
(2) What was the role of sentinel surveillance, and what VL systems would be most useful?
(3) Would new, practical technologies for VL measurement be available soon, e.g. dipstick, dried blood spots?
In MSF projects monitoring VL the treatment resultshad been consistent with other reported results in low-income countries. Thus a cross-sectional VL survey inMalawi showed that, after six months of treatment, 73%of 477 patients had VL < 40 copies/ml, 85 % had VL < 400 copies/ml and 88% had VL < 1000 copies/ml.Aftert two years, in a limited group, 14% of patients hadVL > 5000 copies/ml in two consecutive determinations.
MSF was still not sure how best to use VL. Initially, VLwas used as an advocacy tool for demonstrating that ARTwas feasible in resource-poor settings. Staff in SouthAfrica used VL to assess adherence but were often reluc-tant to change a treatment solely on basis of VL results.Operational research was necessary in order to deter-mine how VL could be used to decide when switching toan alternative regimen was required with a view toimproving patient outcomes.
Few tests were available for diagnosing OIs. MSF proj-ects could reliably detect and diagnose only TB andCryptococcus. There were no affordable tests for diag-nosing cytomegalovirus, Pneumocystis carinii (PCP) andother major OIs. These tests were at least as essential toHIV care as VL measurements. Strategic approachesinvolving decentralization and/or centralized testingwere presented. Where logistical constraints could beovercome and the quality of specimens could bepreserved, blood specimens could travel instead ofpatients.

9WHO DEPARTMENT OF HIV/AIDS
I I I . C l i n i c a l m o n i t o r i n g i s s u e s
a. Clinical monitoring of adults Monitoring the efficacy of ART included observations onclinical, immunological and virological parameters. Inthe first six months, clinical monitoring could be diffi-cult because of the continuation of OIs, immunereconstitution inflammatory syndrome and the appear-ance of side-effects of the drugs. It was necessary thatalgorithms for diagnosing treatment failure with limitedlaboratory support be based on treatment history, clinicalmanifestations, adherence information and simple labo-ratory tests It was felt that adherence history and theevaluation of adherence through self-reporting bypatients, the use of a visual analogue scale and treatmentcards were not being fully utilized.
It was necessary to address the question of VL moni-toring in the context of clinical decision-making. Ingeneral, VL should be regularly measured and if so,values need to be established as a trigger for determiningwhen to switch from first-line to second-line therapy. Itwas worth considering whether alternative data points existed, e.g. clinical parameters, laboratory test results orother patient information, which might be used toreduce dependence on expensive VL testing in guidingclinical decisions.
As a general rule it was desirable that physicians, beforeordering expensive tests, should consider the use to bemade of the results and the treatment options availablefor the patient.
b. Clinical monitoring of childrenThe Botswana programme was triggered by a survey in2001 which revealed that there were more than 300 000HIV-infected people in the country and that 100 000individuals were eligible for ART, of whom over 90 %did not know their HIV status. Among the many reasonsfor this hidden epidemic were substantial socioculturalbarriers and an almost total lack of laboratory capacity.
Several groups in Botswana began collaborating to estab-lish comprehensive HIV care. In December 2001 thefirst HIV laboratory opened, staffed by a team from theBotswana-Harvard Partnership. This sophisticatedfacility offered CD4 and VL testing, HIV serology andbasic haematology and chemistry. Resistance testing wasadded in 2004.
The initial laboratory monitoring protocol in Botswanamirrored that of high-income countries. Patients under-went baseline CD4 and VL testing, and were then testedfor CD4 and VL every three months. Full blood countswere obtained after one month on treatment and atthree-monthly intervals thereafter. Patients taking nevi-rapine (NVP) underwent regular liver enzyme testing.Lipid levels were measured every six months in patientstaking protease inhibitors.
The Botswanna-Baylor Children’s Clinical Centre ofExcellence in Gaborone had more than 1200 paediatricpatients. The clinical monitoring of children on ARTcovered:
(1) growth (weight and height measured every three months);
(2) development (occipitofrontal circumference measured every 3 months for children aged under 2 years, and neurodevelopmental assessment made every 3 months);
(3) social well-being (access to social benefits, schoolattendance and quality of care by carers);
(4) immunizations.
The Botswana roll-out encountered numerous problems,including a lack of trained pharmacists, poor stockmanagement, poor linkages between HIV programmesand the need to integrate HIV programming into thegeneral health system. With respect to laboratory services,the major problems were with centralized testing at asingle site, including difficulties in transporting samples.A significant investment in the laboratory infrastructurehad been critical in accelerating the pace of roll-out. It wasnecessary to make the system sustainable.

???????10
DiscussionThere was general agreement that it was necessary togive more attention to standardized clinical patient monitoring by means of a set questionnaire and to themonitoring of adherence. Although the potential role ofVL testing in the decision-making process for switchingto second-line treatment was debated, no data were available on which to base clear recommendations. Thelack of appropriate diagnostic tests for early detection ofHIV infection in infants born to HIV-positive mothers(qualitative HIV DNA/RNA tests and/or p24 Ag test)and for monitoring infants and CD4 %, and easy specimen collection and transport (filter paper) was identified as a gap that urgently need to the addressed.

11WHO DEPARTMENT OF HIV/AIDS
IV. Laboratory technologies and monitoring
a. Resistance monitoringThe accelerated roll-out of ART could lead to the emer-gence and transmission of ARV-resistant viruses.Although HIV drug resistance (HIVDR) could not beprevented, there might be a possibility of combating itsspread and impact. HIVDR developed as a result of thehigh replication rate of HIV and its error-prone tran-scription. ART, particularly if suboptimal, selectedmutations that could replicate in the presence of ARVdrugs, and virological failure could rapidly emerge.
WHO had prioritized the prevention, surveillance andmonitoring of HIVDR within its planning for the 3 x 5initiative and had developed an approach to preventingthe emergence and transmission of HIVDR. Thisapproach included the use of standard ART regimensthat were highly active and suited to the countries orregions concerned. Standard individual treatmentrecords and active monitoring of adherence were beingestablished. Measures to ensure the continued supply ofdrugs of satisfactory quality were essential to the successof the initiative, as were programmes for peoplereceiving ART in order to reduce HIV transmission. Theestablishment of HIVDR surveillance and monitoringwould provide a means of assessing whether implemen-tation had been successful. HIVDR surveys would targetuntreated individuals in specific geographical settingswho had recently become HIV-infected. WHO intendedto evaluate whether HIVDR was < 5%, 5–15% or > 15%in various regions by examining sufficient specimens toprovide adequate statistical power for a threshold survey.Public health action would be essential if such a surveyindicated HIVDR to be > 15%.
Monitoring would allow evaluation of the patterns ofdrug resistance emerging in sentinel centres with first-line regimens. It was planned to check for HIVDR beforethe initiation of ART, at 12 and 24 months, and beforechanging to second-line ART. This would provide dataon the appropriateness of first-line ART, patterns ofHIVDR associated with specific ART regimens atdifferent sites, the ability to monitor the appropriatenessof second-line ART, and validation of the HIVDR earlywarning measures. Standard laboratory protocols for thedetection of HIVDR would be applied and QA measureswould be strengthened. The findings would be assem-bled in national and regional databases and it wasintended that regional and global HIVDR reports wouldbe prepared twice a year.
b. Technologies for resistance monitoring There were two basic approaches to testing for the presence of HIVDR: phenotyping and genotyping.
Phenotyping measured the ability of the virus to infect orreplicate in vitro in the presence of drugs. Because ofproblems inherent in the isolation and culture of HIVfrom individuals under investigation, an approach usingrecombination to insert an amplified region from the polgene into a plasmid HIV was usually employed. Thisrecombinant was used in a cell culture system to assessthe phenotypic susceptibility of the originator virusagainst a range of drugs. Although expensive and time-consuming, this method provided a relatively directmeasure of susceptibility, assessed the effect of all muta-tions, even those not yet described, and could easily beadapted to test new classes of drugs.
Genotyping provided direct information on mutations atcodon positions of (RT) and protease genes associatedwith drug resistance. Because it relied on polymerasechain reaction (PCR) amplification of all the quasispecies present in an individual, population-basedsequencing generated a consensus sequence that wouldidentify only the major species present. However, thegenerated sequence would provide additional informa-tion, including the HIV subtype/ circulatingrecombinant form (CRF) and information on possiblecross-contamination. Point mutation assays woulddetect only the particular set of mutations designed intothe assays but might identify minority sequence popula-tions. Genotypic methods were more rapid, cheaper (butstill very expensive) and did not require the biosafetylevel 3 precautions needed for phenotyping. However,they required expert interpretation of drug resistancealgorithms, and these needed regular updating for newdrugs or combinations of drugs. Moreover, the presenceof naturally occurring polymorphisms in HIV-1 non-Bviruses at codons associated with resistance in HIV-1clade B viruses further complicated genotypic resistancetesting. Consequently, research was needed to developreliable genotypic interpretation algorithms for non-BHIV-1 strains and to study mutations selected in non-Bstrains. Performance assessment programmes for labo-ratories providing HIVDR testing were essential and hadto be further developed and expanded.

???????12
c. CD4 technologiesThe latest information on CD4+ T-cell enumerationtechnology was reviewed, with particular reference toresource-limited settings. The following trends in flowcytometry were leading towards low-cost monitoringtools:
(1) smaller instruments;
(2) fewer reagents;
(3) digital image analysis;
(4) improved sample stability;
(5) wireless data transmission for quality control.
One of the first tasks in the development of CD4 tech-nology for resource-limited settings was to define thespecifications of the instrument and the estimated work-load, in order to ensure an appropriate choice oftechnology. The following important questions had to beconsidered.
◗ Would the technology be used to measure CD4+ T-cell counts in adults, children or both?
◗ Would it be used in a rural setting or an urban setting?
◗ Would it be used in a central referral centre, a district hospital or a peripheral health care site?
◗ Would testing be done at the point of clinical service or would blood be shipped from theclinical site to a nearby or distant laboratory?(Advances in CD4 technology make it possible to consider whether to bring the laboratory to the patient or vice versa.)
High-end flow cytometers (e.g. the Becton-DickinsonFACSCalibur and the Beckman Coulter EPICS XL) werestill being used in low-income countries, primarily inmajor cities with well-developed central laboratories. Inorder to meet the needs of ART scale-up, however, thesehigh-end, expensive and technically more complex high-throughput machines would not be useful in moreremote settings, including most district hospitals withlimited financial and human resources. In these settings, less expensive and simpler equipment andtechniques were needed.
At least two companies, Partec and Guava Technologies,were producing middle-end flow cytometers designedfor use in resource-limited settings. Their technologieswere being evaluated.
The Partec CyFlow Counter was a self-contained flowcytometer with one parameter, while the same firm’sCyflow Green had two parameters. Both of these instru-ments could run on a car battery. More powerful,build-on-order flow cytometers were obtainable fromPartec. Field experience had shown that the CyFlowsystems might not have overcome technical challengesrelated to the robustness of the equipment or the repro-ducibility of the results. The Cyflow Counter waspossibly inappropriate for TB-coinfected patients.
The EasyCD4 system of Guava Technologies used a lessexpensive light source and coupled the cytometer to alaptop computer for analysis. Prices per test could bereduced to $1.00–2.00 because the method involvedusing low volumes of reagents and did not need sheathfluid. The instrument was undergoing independentinvestigation by the Centers for Disease Control andPrevention (USA) and WHO in order to determine itsrobustness and accuracy in the field. Laboratory techni-cians required a sufficient understanding of flowcytometry in order to be able to operate these middle-endinstruments reliably and make adjustments if necessary.
The following three distinct approaches were currentlyavailable for measuring CD4 T-cells in resource-limitedsettings where the throughput was low, i.e. fewer than 30specimens/day.
(1) Automated equipment could be used whichproduced a CD4 T-cell result without significanttechnical expertise or interpretation on the part of theuser. Two systems meeting the criteria were avail-able, only one of which, the Becton-DickinsonFACSCount, had been widely adopted. This systemused proprietary reagents to produce an absoluteCD4 T-cell count from a single 1-ml sample of wholeblood. It measured CD3, CD4 and CD8 cells, but hadnot been configured to measure CD4 T-cells aslymphocyte percentages. Consequently, theFACSCount system was only useful for CD4 T-cellcounting in adults. The company had been asked toalter the parameters so as to allow CD4 percentagedeterminations for paediatric use.
In 2004, PointCare Technologies introduced theFlowCare system of CD4 measurement. The productwas being marketed by Beckman Coulter under thename of PointCare. The approach differed slightlyfrom that of traditional flow cytometry. It used exclu-sively light-scattering parameters to distinguish

13WHO DEPARTMENT OF HIV/AIDS
lymphocytes from other white blood cells. CD4 cellslabelled with a colloidal gold-coupled antibody werethen identified on the basis of wide-angle light scatter. The net result was that the entire system wasautomated as from the point of blood collection. Awhole blood sample of 3–5 ml was placed in themachine, and after single-button operation a CD4result was reported in approximately 17 minutes.PointCare provided CD4 percentages and absolutecounts, total white blood cell counts, total lymphocytecounts and lymphocyte percentages.
The company was currently finalizing some modifi-cations of methods which would soon allow the system to deal with samples from both adults andchildren. However, as PointCare used a differentanti-CD4 antibody-labelling method there were nogeneric reagents available, and the system was notcompatible with existing EQA programmes.
(2) The following manual methods could be used. Theyhad a lower throughput, i.e. fewer than six speci-mens/day, but were less expensive overall. Bothemployed microbeads for the identification of CD4 T-cells. Both systems provided only absolute CD4counts.
(a) Dynals’ Dynabead system used two immuno-magnetic separation steps to (i) remove CD4monocytes and (ii) isolate CD4 lymphocytes,which could then be counted under a light orfluorescence microscope.
(b) Coulter’s Cytosphere method blocked the CD4 receptors on monocytes with one set of microbeads and labelled the remaining CD4-positive cells with a larger set of colour-labelledbeads. These rosetting cells could be distin-guished under a light microscope.
The principal problems concerned the time involvedin processing and analysing the specimens and thethroughput, as the two-step cell isolation and micro-scopic counting process took a single technician upto one hour per patient result. No EQA programmewas available for these manual techniques.
(3) Whole blood specimens from patients could be stabilized and transported to a central laboratory withhigh-end equipment. Four blood stabilizers were onthe market: Cyto-Chex BCT (Streck Laboratories),Cellsave (Immunocon) (R&D Systems), ThromboFix(Beckman Coulter) and TransFix (UKNEQAS). Theseblood fixatives all appeared to stabilize blood reliablyfor up to seven days at 22°C but only with Transfixwere specimens stable for three days at 37°C.Unfortunately, temperatures above 37°C werecommon in many parts of the world where HIV wasprevalent.
LabNow was developing a point-of-care CD4 T-cellcounting instrument based on microfluidic sampleprocessing and digital image analysis. It would possiblybe battery-operated and portable, thus providing a usefulapproach to CD4 counting in resource-limited settings.It was anticipated that the product would be available forvalidation in the second half of 2005 and that, if all wentwell, it would be ready for wide-scale use in 2006.
Other assays under development for use near the pointof care included various dipstick approaches and a cellcapture assay involving microscopy (Sembio).
Attention was repeatedly drawn to the lack of affordableinstruments that could produce a CD4 percentage oftotal lymphocytes, which was desirable for monitoringinfants and children aged up to 6 years. To date, onlyhigh-end flow cytometry equipment could produce reli-able CD4 percentages. The FACSCount system had notbeen configured for paediatric use, although appropriatereconfiguration would be feasible. PointCare providedCD4 T-cell percentages but had not yet been validated inrespect of CD4 percentage assays in children. Theabsence of affordable paediatric CD4 counting technolo-gies was a huge barrier to ART roll-out in children. Thedevelopment of such technologies was of the utmostimportance.
L a b o ra t o r y t e c h n o l o g i e s a n d m o n i t o r i n g

???????14
DiscussionSeveral middle-end and low-end CD4 technologies hadrecently been commercialized or would soon becomeavailable. Although several of the instruments seemedvery promising, it was necessary to assess their performance with specimens from both adults and chil-dren in independent studies. Negotiations with andcompetition between manufacturers of CD4 technolo-gies were resulting in price reductions. It was desirableto organize a survey that would give a better view of theoperational aspects and down time of CD4 equipment atthe country level. It was emphasized that local mainte-nance expertise was crucial for reducing the down timeof the instruments.
d. Quality assuranceThe activities managed from the Australian NationalSerological Reference Laboratory (NRL) were used as amodel in describing the elements of QA. In addition toorganizing EQA and producing quality control (QC)samples for Australia, NRL had provided, in collabora-tion with WHO/EHT, similar services to many countriesof the South-East Asia Region and the Western PacificRegion. The WHO EQA and QC activities had beensupported by an active programme of training and othersupport through workshops, published guidelines andadvice. It was essential to have mechanisms in place forensuring the availability and use of kits of high integrity,monitoring continued quality from batch to batch, andensuring their correct use. Error rates in the WHO HIV/ hepatitis B / hepatitis C serology EQA schemes run byNRL in the South-East Asia Region and the WesternPacific Region had fallen, presumably as a result of theconsistent application of quality activities. EQA for HIV-1 VL measurements had shown that performance in Thailaboratories was similar to that in Australia. A web-basedEQA system called Electronic Data Collection was a valu-able tool permitting real-time monitoring both oflaboratory performance and the various diagnostic kits inuse. A similar approach had been followed byWHO/EHT for providing a QA programme supportingCD4 T-cell counting in the African and Asian regions.WHO was working closely with the Canadian EQAscheme for CD4 and had established a network ofcentres of excellence in the regions to provide EQA forCD4 T-cell counting, training and technical support.
e. HIV incidence testingThe ability to discriminate between long-standing andrecently acquired or incident HIV infection was impor-tant, providing insight into current transmission trendswithin epidemiological surveys, aiding the tracking ofoutbreaks and possibly assisting in the monitoring oftreatment programmes. Several techniques had beendescribed, including STARHS (serologic testing algo-rithm to detect recent seroconversion or detuned) IgGcapture assay (BED assay) and antibody avidity assays.NRL had also researched methods of detecting incidentHIV infection and had identified a new method thattested for the IgG3 isotype of HIV antibody, whichseemed to appear for a period of several months afterseroconversion. Additional work was needed on tests forincident infection so as to improve the identification ofthresholds and window periods and their specificity andsensitivity. How they performed when applied to indi-viduals with non-B subtype infections also requiredfurther elucidation.
f. Relevant laboratory technologiesin antiretroviral therapy roll-outprogrammesSeveral countries had progressed significantly withnational ART roll-outs, and important lessons could belearnt on the implementation of appropriate diagnosticand laboratory monitoring systems. In a very short timeSouth Africa had rolled out its ART programme andscaled up its laboratory capacity. Many problems hadbeen solved but some remained.
For haematology it was important for the national labo-ratory system to recognize that the method and approachto full blood counting was driven by the choice of CD4technologies. Many systems were still of the dual plat-form kind and required a lymphocyte differential from afull blood count in order to back-calculate an absoluteCD4 count. The choice of a single-platform as opposedto a dual-platform CD4 counting system therefore hadsignificant implications for the haematology analysersthat could be used.

15WHO DEPARTMENT OF HIV/AIDS
Moreover, the values being used as reference rangeswere based on published data, most of which wereobtained from studies in high-income Western coun-tries. Little was known about the normal reference rangefor white blood cell counts and subsets in much of sub-Saharan Africa and South-East Asia. This informationcould be critically important as widespread CD4counting became available and CD4 counts began to beused for decisions about expensive treatments. However,even if normal ranges varied there were no data tosuggest different trigger points (e.g. CD4 < 200, orCD4% < 15%) for the initiation of treatment.
The challenges associated with chemistry results wereeven more significant. The most pressing problem wasthat nearly all currently manufactured automated chem-istry systems were high-end expensive machinesbundling chemistry assays in one device. It could thus bedifficult to obtain a single result for a liver enzyme, e.g.alanine aminotransferase (ALT), at low cost with lesscomplex equipment. There were ways of obtaining thesesingle chemistry results at lower cost but they were notgenerally automated and involved low throughput.
Perhaps the biggest challenge facing national laboratoryprogrammes was the need to handle extremely highvolumes of CD4 testing. In South Africa the nationalprogramme had had to expand from 3 to 22 laboratoriescapable of performing CD4 counts in less than a year. Itcould be difficult, but not impossible with good plan-ning, to maintain an effective programme that met QAstandards. Analysis of the South African data had shownthat CD4 counts below 200 cells/mm3 had beenobserved in more than 50% of patient tests.
In South Africa, regular VL measurements were part ofthe national protocol. This had led to extremely highvolumes of VL testing, which had also been scaled upfrom a few to many laboratories. It was necessary toconsider carefully the volume of testing when decidingwhat equipment to use. Systems relying heavily onmanual nucleic acid extraction at the front end,including the bioMérieux system used in South Africa,began to struggle if volumes were high. Automatedsample extraction was likely to be more appropriate forhigh-volume settings.
In addition to these specific concerns there were generalchallenges to laboratory scale-up. Although there was atendency to focus on CD4 and VL, many laboratories in
resource-limited settings still struggled with basic testsinvolving HIV serology, basic haematology and basicchemistry.
QM and QA systems were essential for the achievementof accurate laboratory results. These systems could berapidly introduced in resource-limited settings by usingexisting EQA programmes for assistance. A trainingplan was essential for implementing laboratory scale-up.Technicians and staff had to be trained in good labora-tory practice (GLP) and the use of specific equipment.Laboratory site initiation modules could support GLP,standard operating procedures (SOPs), QM systems andspecific training.
It was necessary for laboratory operational plans to beprepared for the enormous volumes that were likely toaccompany national roll-out, particularly for CD4testing, which were used for both patient staging andpatient monitoring.
Infant diagnostics were still being neglected. There wasno validated low-cost method for diagnosing infection inchildren aged under 15–18 months, yet this was a vitalrequirement, especially for programmes concerningtransmission between mothers and their children.
Laboratory information systems were still unlinked toclinical information systems, making communicationbetween laboratories and clinics both more critical andmore difficult.
L a b o ra t o r y t e c h n o l o g i e s a n d m o n i t o r i n g

???????16
g. HIV/tuberculosis laboratory issuesIt was estimated that 10–30 % of HIV-infected peoplehad TB. In certain regions more than 50% of TB patientswere HIV-positive. Because of the scope of HIV/TB coin-fection it was necessary for HIV ART roll-outprogrammes to take this into consideration. It was essen-tial for HIV and TB programmes to collaborate closely,particularly with regard to laboratory matters. Both at thecase-finding level and the ARV entry-point level, it wasdesirable for HIV diagnosis to trigger an algorithm forTB case-finding, and vice versa. The tests were carriedout in the same laboratory, sometimes even by the sametechnician. Consequently, it was desirable for there to bemore integration and the building of linkages andreferral mechanisms between the HIV and TB laboratoryprogrammes, including cross-checks of HIV and TBlaboratory registers, the strengthening of QA, joint labo-ratory supervision and overall monitoring.
There were significant limitations on the availability ofappropriate and easy-to-use diagnostics for TB. The accu-racy of the smear test was declining because of HIVcoinfection. Furthermore, the percentage of extrapul-monary TB was increasing and X-ray facilities weretherefore required. However, they were not always available. TB diagnosis by culture was relatively costly,complex and time-consuming and required an appro-priate laboratory infrastructure.
New TB diagnostics were being assessed but noneseemed to be working satisfactorily. New approaches andtechnologies were urgently needed for identifying latentTB infection in a rapid and inexpensive manner.
DiscussionIt became apparent that there were several overarchingissues related to laboratory monitoring. In resource-limited settings with low throughput there was arequirement for appropriate, reliable, easy-to-use andinexpensive laboratory technology for haematology,chemistry, CD4 counting, VL testing and TB diagnostics.Another recurrent issue was the need for QA andtraining, particularly when new technologies were beingintroduced and in low-throughput settings, i.e. incircumstances associated with roll-out programmes.Integration of the different laboratory componentswould be vital to the success of 3 x 5 programmes.National laboratory committees would have to demandand actively support the roll-out of ART programmes.

17WHO DEPARTMENT OF HIV/AIDS
a. UN prequalification process for antiretroviral drugsIt was pointed out that millions of people living withHIV/AIDS did not have access to treatment.Substandard medicines and counterfeit products wereprocured and supplied in various countries. QA systemsin medicine supply chains were often weak or did notexist. The sourcing of products of poor quality presentedrisks to patients by increasing treatment failure andresistance.
The objective of the project was to propose a list ofprequalified manufacturers and products whose quality,efficacy and safety had been assessed, inspected andcontrolled so that they met the international norms andstandards.
WHO managed the prequalification project on behalf ofthe UN. Its main partners were UNAIDS, UNFPA,UNICEF and the World Bank.
Prequalification involved a standard procedure devel-oped by the WHO Expert Committee on Specificationsfor Pharmaceutical Preparations. The assessment ofproduct dossiers submitted by companies and inspec-tions on good manufacturing practice were followedpromptly by feedback to the companies concerned.Medicines were added to the list of prequalified productsonly when the products and manufacturing sites met therequired standards. The list of HIV-related products andmanufacturers which were found to be acceptable inprinciple was available on the web sites of collaboratingUN agencies.
WHO provided the technical and scientific expertise andguarantees that international norms and standards wereapplied throughout the process, including the assess-ment of the dossiers, inspection and quality control.
The submitted dossiers were reviewed by a team of eightto twelve experts in order to check their acceptability withrespect to quality and efficacy. Additional data could berequested. For reasons of objectivity, each dossier wasassessed by two experts and an assessment report waswritten and made available. The second step was theinspection of the manufacturing site or sites and theinspection of the research laboratory where the bioe-quivalence study was performed. The QC programmewas also assessed and products were requalified afterthree years.
The experts involved in this process were mainly asses-sors and inspectors from national drug regulatoryauthorities or national QC laboratories of Member coun-tries of the International Conference on Harmonizationof Technical Requirements for Registration ofPharmaceuticals for Human Use.
In December 2004, only 85 HIV-related medicines, 8antituberculosis drugs and 2 antimalarial drugs had beenprequalified out of a total of 500 products for whichdossiers had been submitted. It was necessary to developthe prequalification project further so as to cope with theincreasing number of dossiers, the follow-up of varia-tions, and periodic requalification, and to extend itsassistance to both manufacturers and the national drugregulatory authorities in resource- constrained countries.
V. P r e q u a l i f i c a t i o n a n dp r o c u r e m e n t i s s u e s
???????18
b. UN assessment and selection of appropriate diagnostic technologies WHO, on behalf of the UN family, provided technicaladvice to Member States on the quality and operationalcharacteristics of diagnostics for HIV care and treat-ment. As part of this effort, several diagnosticinstruments and assays had already been assessed orwere scheduled for evaluation.
In general the evaluation should proceed along thefollowing steps:
(1) WHO should receive a request from a manufactureror the request should be initiated by WHO.
(2) WHO should review independent data on perform-ance generated in trials and review existingcertifications, e.g. FDA approval or the CE mark.
(3) If not the manufacturer but a third party requests theevaluation, an OEM investigation should be pursued.An original equipment manufacturer investigationshould be conducted into the repackaging of an assaysourced from a single manufacturer under a differentlabel which did not involve alterations in the produc-tion of the assay components.
(4) A letter of agreement should be signed betweenWHO and the manufacturer or third party.
(5) The operational characteristicts and the assay and/orequipment performance should be evaluated.Assayand/or equipment performance should be evaluatedat WHO collaborating centres in various part of theworld.
(6) The data from each stage of the evaluation should beanalysed and the information should be disseminated.
The evaluation of HIV serological assays relied on a well-characterized WHO reference panel of specimens and astandardized algorithm. Minimal performance criteriahad been established with regard to sensitivity (> 99%for rapid, 100 % for enzyme-linked immunosorbentassay (ELISA), specificity (> 98%) inter-reader variability(< 4%) and seroconversion sensitivity. The clarity of thetest kit insert, the labelling of the component of the kitand the easiness of the test procedure were also assessed.
The validation of CD4 technologies was conducted atseveral sites in accordance with one protocol. Specimenswere collected in a prospective manner and a certainnumber of control specimens were included in each
assessment. The results were compared to thoseobtained by gold standard methods. The performancecriteria included accuracy, linearity,reproducibility/precision, inter/intra-run variability andtechnician variability. The Dynabeads, Cytospheres,FACSCount and a few assays no longer available hadpreviously been assessed by WHO. Several performanceassessments were in progress, covering CyFlowCounter, Cyflow Green, EasyCD4 and PointCare.Contacts had been made with the manufacturers ofFlowCare and Sembio with a view to assessing their tech-nologies as soon as they became commercially available.
The assessment of VL assays covered sensitivity to thevarious HIV subtypes, reproducibility/precision andaccuracy. The data were compared to those obtained bygold standard methods for these assays. The ExaVir v2.0(Cavidi®) and the Retina Rainbow assay (Primagen®)were currently under evaluation.
WHO was concerned mainly with diagnostics and equip-ment appropriate for use in resource-limited settings. Inmany of the countries heavily affected by the HIVepidemic, the regulatory capacity for diagnostics wasweak or non-existent. WHO could ease the work of thenational regulatory authorities by providing technicalperformance data as well as criteria that were not relatedto performance, e.g. ease of use and the appropriate levelof health service for use, e.g. VCT centre versus districtversus regional. Manufacturers of assays that had beensuccessfully evaluated were eligible to tender for bulkprocurement through the UN. The one-year procure-ment agreements between companies and WHOcovered the UN family (UNAIDS, UNDP, UNFPA,UNICEF, World Bank, etc.). Access to diagnostics ofsatisfactory quality at reasonable cost was thus madeavailable to Member States.
19WHO DEPARTMENT OF HIV/AIDS
P r e q u a l i f i c a t i o n a n d p r o c u r e m e n t i s s u e s
c. WHO Contract Procurement ServicesWHO was directly involved in the procurement of labo-ratory equipment and test kits. Orders could be placedthrough WHO by Member States, nongovernmentalorganizations (NGOs) in official relation with WHO, andmembers of the UN family. A new electronic catalogueand ordering system, WebBuy, was now on line andaccessible in the offices of WHO countryRepresentatives. The on-line catalogue made simplifiedbulk procurement possible for Member countries.Currently, ten catalogues were available, including onedevoted to HIV laboratory materials which providedinformation to potential buyers. A purchase ordersystem, facilitating the whole process, was linked to thecatalogue. The WHO bulk procurement scheme for HIVdiagnostics, established in 1989, was continuing toevolve and to adapt to current needs.
d. UNICEF Procurement ServicesUNICEF had established a supplies procurement systemthat worked directly with country offices, other UN agen-cies and NGOs. There was a UNICEF warehouse inCopenhagen where commodities could be stored ifnecessary. It could serve as a link to bulk procurementfor the end user. ARV drugs, HIV test kits and CD4 andVL equipment valued at $18 million were procuredduring 2004 through the UNICEF Supply Division;26 % of the procurement had been in Ghana, 21 % inMalawi, 14 % in Myanmar, 7 % in the DemocraticRepublic of the Congo, 7 % in Zambia and 5 % inCambodia. It was difficult to forecast demand as goodsystems for data collection were not yet in place.Quantities of HIV test kits were small and mainly fornew customers, resulting in classic start-up problems.Among other problems linked to scale-up were thefrequent disregard of the costs of in-country distributionin plans and a lack of knowledge of appropriate labora-tory infrastructures and general laboratory commodities.The Supply Division developed survey questionnairesand equipment planning bulletins for HIV/AIDS serviceproviders, with a view to facilitating planning at theprimary and first-referral levels.
e. AIDS Medicines and DiagnosticsServices AIDS Medicines and Diagnostics Services (AMDS) wasa network supporting procurement and supply manage-ment for HIV drugs and diagnostics. Members of thenetwork included WHO (EDM, EHT, CPS, regionaloffices), UNICEF, the World Bank, UNAIDS, UNDP,UNFPA, the Centre for Collaborative AIDS Research,the Clinton HIV/AIDS initiative, the CommonwealthPharmaceutical Association, the Crown Agents, theEcumenical Pharmaceutical Network, Esther, the GlobalFund for AIDS, Tuberculosis and Malaria (GFATM),IDA, the International Pharmaceutical Federation, JohnSnow Incorporated and Management Sciences forHealth. AMDS served as a clearing house for informa-tion and as a broker for assistance to country partners forbulk procurement. It could provide forecasting tools andsupply management tools to enable centralized planningof bulk procurement.

???????20
f. Global Fund for AIDS, Tuberculosis andMalaria The contributions paid to GFATM in 2004 amounted to$1446 million. A large number of proposals had beenreceived and funded. The Board anticipated that arequest for Round 5 proposals would be launched bymid-2005.
The procurement of ARV drugs and HIV/AIDS-relateddiagnostics constituted a substantial component of mostof the proposals. GFATM was not being prescriptive onthe types of products or their suppliers. Countries werefree to order any products from any supplier at any givencost. However, GFATM acknowledged the UN prequali-fication project for priority medicines, and countrieswere encouraged to buy prequalified products. In manycountries, relatively weak procurement and supplymanagement systems had hampered the implementa-tion of accepted proposals. Consequently, the beneficialaspects of working with well-experienced supply agen-cies had been recognized.
DiscussionSome concerns were raised about the duplication ofefforts in procurement and supply management withinWHO and between UN agencies. It was explained thatthere was good collaboration between WHO andUNICEF as well as with the other UN agencies. WHOwas the lead agency on technical issues such as theprequalification of ARV drugs (EDM) and on the valida-tion and selection of HIV/AIDS-related diagnostics(EHT). The AMDS web pages provided a one-stop shopfor the technical information relevant to countries andpartners.
The advantages of the existing UN procurement systemswere that countries did not need to go through a lengthytendering process and had access to products of satisfac-tory quality at reasonable cost not linked to volume.However, both shortages and wastage of diagnosticsoccurred because forecasting was difficult in a scale-upsituation. Stock management systems were required withregular feedback to the central purchase point so as toensure continuous access to ARV drugs and diagnostics.

21WHO DEPARTMENT OF HIV/AIDS
VI. Group work and recommendations
Group work 1. Review of currentlaboratory requirements supportingantiretroviral therapy roll-out: clinicalexpertsThe clinical expert team comprised two groups (A and B)and the major issue was to review and strengthen thebasic laboratory monitoring recommendations previ-ously established on pages 24-26 of the current WHOART guidelines (Scaling up ART in resource-limitedsettings – 2003 revision). With regard principally to TableE (Recommended tiered laboratory capabilities for ARVmonitoring in limited-resource settings) and Table F (Basiclaboratory monitoring for WHO-recommended first-lineregimens at community health and district hospital centres)of these guidelines, the basic questions for debate wereas follows.
1) What tests were needed?
2) When (what frequency)?
3) Where (i.e. at which level of care, e.g. tertiary hospital,district hospital, health centre)?
Recommendations of Group AGroup A was in general agreement with the content ofTable E but emphasized that clinical and laboratory inves-tigation was essential for the diagnosis of TB at all levelsand that the link between TB and HIV programmes hadto be strengthened. It was suggested that any HIV anti-body testing (not restricted to rapid test methodologies)should be considered for HIV diagnosis at all levels.
Regarding Table F, it was recommended that a moredetailed frequency schedule for monitoring thesuggested tests should be established, particularly forregimens based on ZDV and NVP. For patients to beconsidered for the use of ZDV, it was recommended thatthere should be an Hb monitoring schedule at baseline,followed by monitoring at 4, 8 and 12 weeks during thefirst 3 months, and, thereafter, in accordance with symp-toms. For NVP users the recommendation was forbaseline CD4 and ALT measurements before the initia-tion of treatment, ALT measurements at 4, 8 and 12weeks, and symptom- directed monitoring thereafter, ifthese tests were available.
It was suggested that a specific table for second-line drugswas needed and that, for TDF users, creatinine and urineprotein should be checked. For patients considering theuse of lopinavir/r it was desirable to monitor bloodglucose and lipids if possible. A symptom-directed inves-tigation for pancreatic toxicity was recommended forusers of ddI. No specific laboratory test was recom-mended for abacavir.
Regarding laboratory efficacy monitoring, Group Asuggested that the CD4+ cell count should be evaluatedevery 3–6 months if possible. There was a long debateabout VL but no agreement was reached on a definitionof virological failure. Sequential measurements, ratherthan a single result, were more useful in monitoring thevirological response. Some comments and questions forfuture evaluation were highlighted: the potential existedfor using the 6-month VL measurement to detect earlyadherence problems, and it was important not to createobstacles to scale-up for countries with no capacity toperform VL testing. For countries with this capacity,however, specific guidelines were needed.
Recommendations of Group BAlthough Group B highlighted the importance of thephysical environment (laboratory safety, biohazards), itwas emphasized that this consideration should nothamper efforts to scale up laboratory capacity. It was feltthat the investment in laboratory services should be basedon volume and prevalence and that clinical capabilitiesshould be enhanced accordingly, taking into account thelearning curve.
Group B considered that the HIV antibody test was theonly test that was invariably essential at the primary carelevel, but that Hb and pregnancy tests were desirable andthat the sputum smear test for TB evaluation should bereferred if microscopy was not locally available.
It was considered that, at the district hospital level, thefollowing tests should be available for monitoring ART:HIV test, full blood count (FBC), differential blood count,pregnancy test, sputum smear test for TB, second HIVserological method (to confirm HIV antibody test results),CD4+ cell count, ALT and possibilities for the diagnosisof treatable OIs (e.g. cryptococcosis, toxoplasmosis, PCP)in accordance with clinical capabilities.

???????22
It was suggested that, at the regional level, full serumchemistries be added if available, including but notrestricted to electrolytes, renal function, liver enzymesand lipids. VL testing was desirable but not essential atthis level.
The following recommendations were made on thefrequency of testing.
◗ HIV antibody testing (confirmed result): baseline(once).
◗ Hg measurement: baseline, 1 and 3 months, thensymptom-directed or if clinically indicated
◗ Pregnancy test: if indicated.
◗ Sputum smear test for TB: if indicated.
◗ ALT: if indicated.
◗ FBC and differential: baseline, 1 and 3 months, andthen symptom-directed or if clinically indicated
◗ CD4+ cell count: baseline and every 6 months (ifavailable at district level and recommended atregional level).
◗ Diagnosis of treatable OIs: if indicated.
◗ Full serum chemistries: baseline and every 6months.
◗ VL: if indicated.
Tables 1–3 harmonize and clarify the recommendationsmade by Group A and Group B.
23WHO DEPARTMENT OF HIV/AIDS
Group work and recommendations
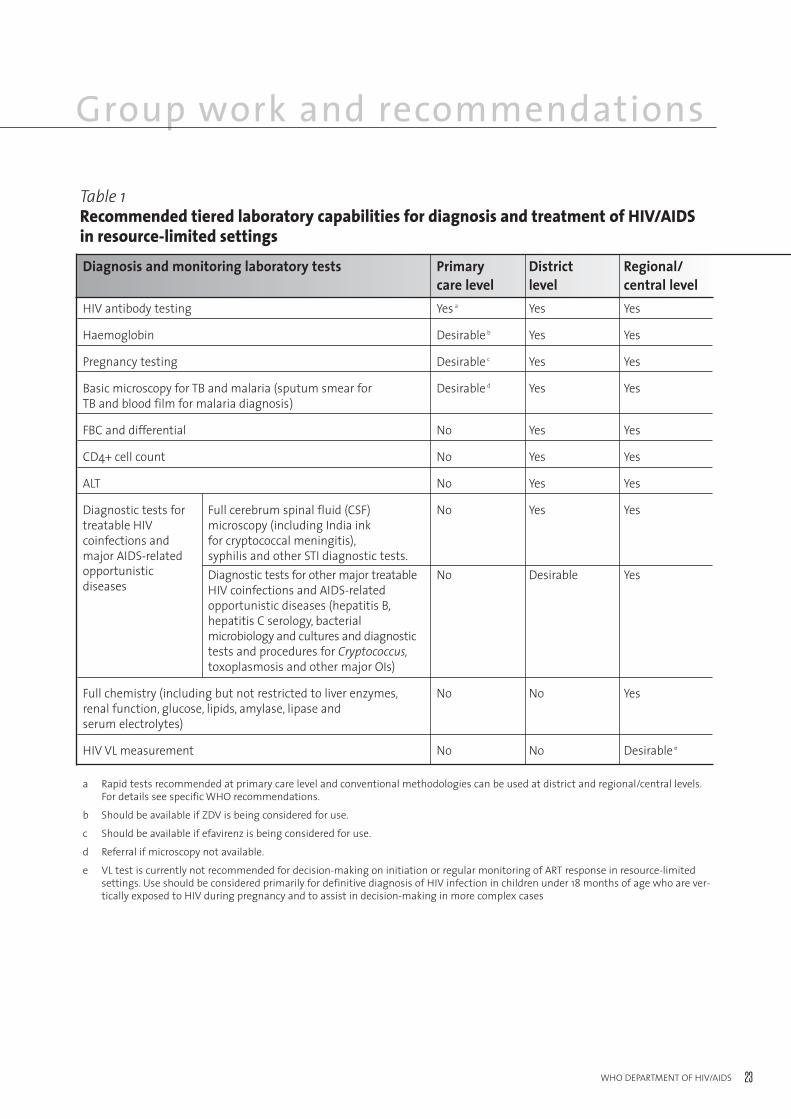
a Rapid tests recommended at primary care level and conventional methodologies can be used at district and regional/central levels.For details see specific WHO recommendations.
b Should be available if ZDV is being considered for use.
c Should be available if efavirenz is being considered for use.
d Referral if microscopy not available.
e VL test is currently not recommended for decision-making on initiation or regular monitoring of ART response in resource-limitedsettings. Use should be considered primarily for definitive diagnosis of HIV infection in children under 18 months of age who are ver-tically exposed to HIV during pregnancy and to assist in decision-making in more complex cases
Table 1Recommended tiered laboratory capabilities for diagnosis and treatment of HIV/AIDS in resource-limited settings
Diagnosis and monitoring laboratory tests Primary District Regional/care level level central level
HIV antibody testing Yes a Yes Yes
Haemoglobin Desirable b Yes Yes
Pregnancy testing Desirable c Yes Yes
Basic microscopy for TB and malaria (sputum smear for Desirable d Yes YesTB and blood film for malaria diagnosis)
FBC and differential No Yes Yes
CD4+ cell count No Yes Yes
ALT No Yes Yes
Diagnostic tests for Full cerebrum spinal fluid (CSF) No Yes Yestreatable HIV microscopy (including India ink coinfections and for cryptococcal meningitis),major AIDS-related syphilis and other STI diagnostic tests.opportunistic Diagnostic tests for other major treatable No Desirable Yesdiseases HIV coinfections and AIDS-related
opportunistic diseases (hepatitis B,hepatitis C serology, bacterial microbiology and cultures and diagnostic tests and procedures for Cryptococcus,toxoplasmosis and other major OIs)
Full chemistry (including but not restricted to liver enzymes, No No Yesrenal function, glucose, lipids, amylase, lipase andserum electrolytes)
HIV VL measurement No No Desirable e
???????24
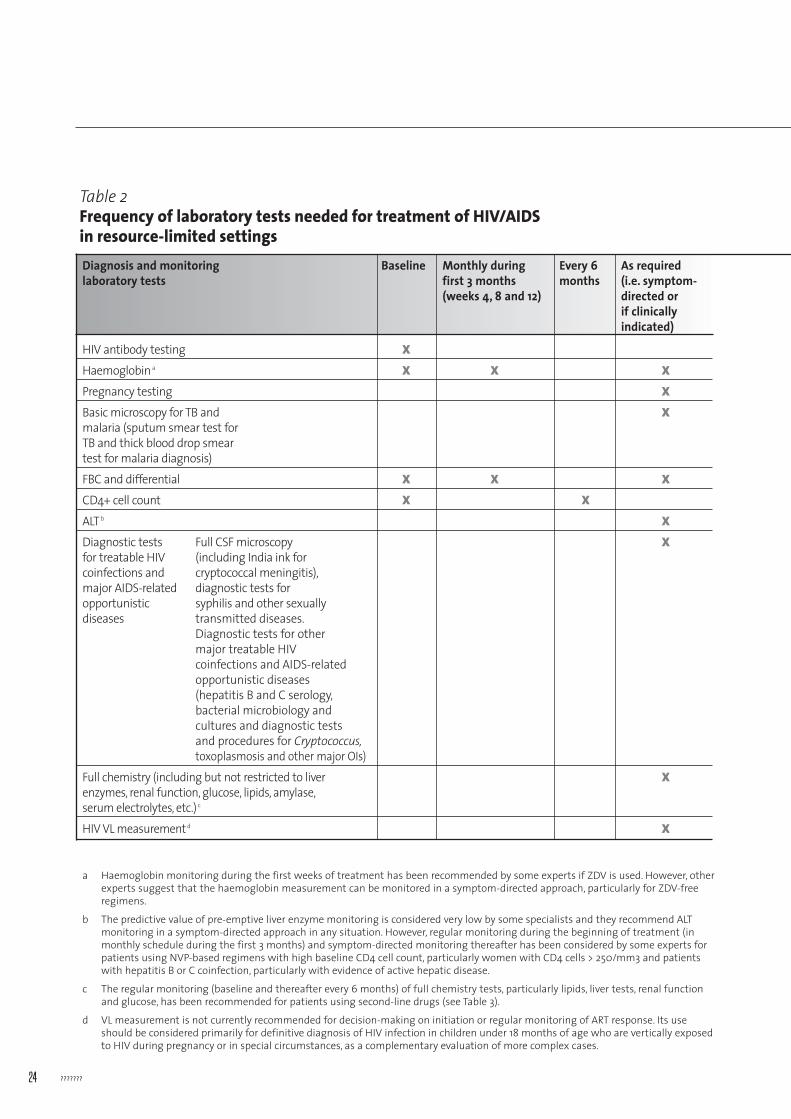
a Haemoglobin monitoring during the first weeks of treatment has been recommended by some experts if ZDV is used. However, otherexperts suggest that the haemoglobin measurement can be monitored in a symptom-directed approach, particularly for ZDV-freeregimens.
b The predictive value of pre-emptive liver enzyme monitoring is considered very low by some specialists and they recommend ALTmonitoring in a symptom-directed approach in any situation. However, regular monitoring during the beginning of treatment (inmonthly schedule during the first 3 months) and symptom-directed monitoring thereafter has been considered by some experts forpatients using NVP-based regimens with high baseline CD4 cell count, particularly women with CD4 cells > 250/mm3 and patientswith hepatitis B or C coinfection, particularly with evidence of active hepatic disease.
c The regular monitoring (baseline and thereafter every 6 months) of full chemistry tests, particularly lipids, liver tests, renal functionand glucose, has been recommended for patients using second-line drugs (see Table 3).
d VL measurement is not currently recommended for decision-making on initiation or regular monitoring of ART response. Its useshould be considered primarily for definitive diagnosis of HIV infection in children under 18 months of age who are vertically exposedto HIV during pregnancy or in special circumstances, as a complementary evaluation of more complex cases.
Table 2Frequency of laboratory tests needed for treatment of HIV/AIDS in resource-limited settingsDiagnosis and monitoring Baseline Monthly during Every 6 As required laboratory tests first 3 months months (i.e. symptom-
(weeks 4, 8 and 12) directed or if clinicallyindicated)
HIV antibody testing X
Haemoglobin a X X X
Pregnancy testing X
Basic microscopy for TB and Xmalaria (sputum smear test for TB and thick blood drop smear test for malaria diagnosis)
FBC and differential X X X
CD4+ cell count X X
ALT b X
Diagnostic tests Full CSF microscopy Xfor treatable HIV (including India ink for coinfections and cryptococcal meningitis),major AIDS-related diagnostic tests for opportunistic syphilis and other sexuallydiseases transmitted diseases.
Diagnostic tests for other major treatable HIV coinfections and AIDS-relatedopportunistic diseases (hepatitis B and C serology,bacterial microbiology and cultures and diagnostic tests and procedures for Cryptococcus,toxoplasmosis and other major OIs)
Full chemistry (including but not restricted to liver Xenzymes, renal function, glucose, lipids, amylase,serum electrolytes, etc.) c
HIV VL measurement d X
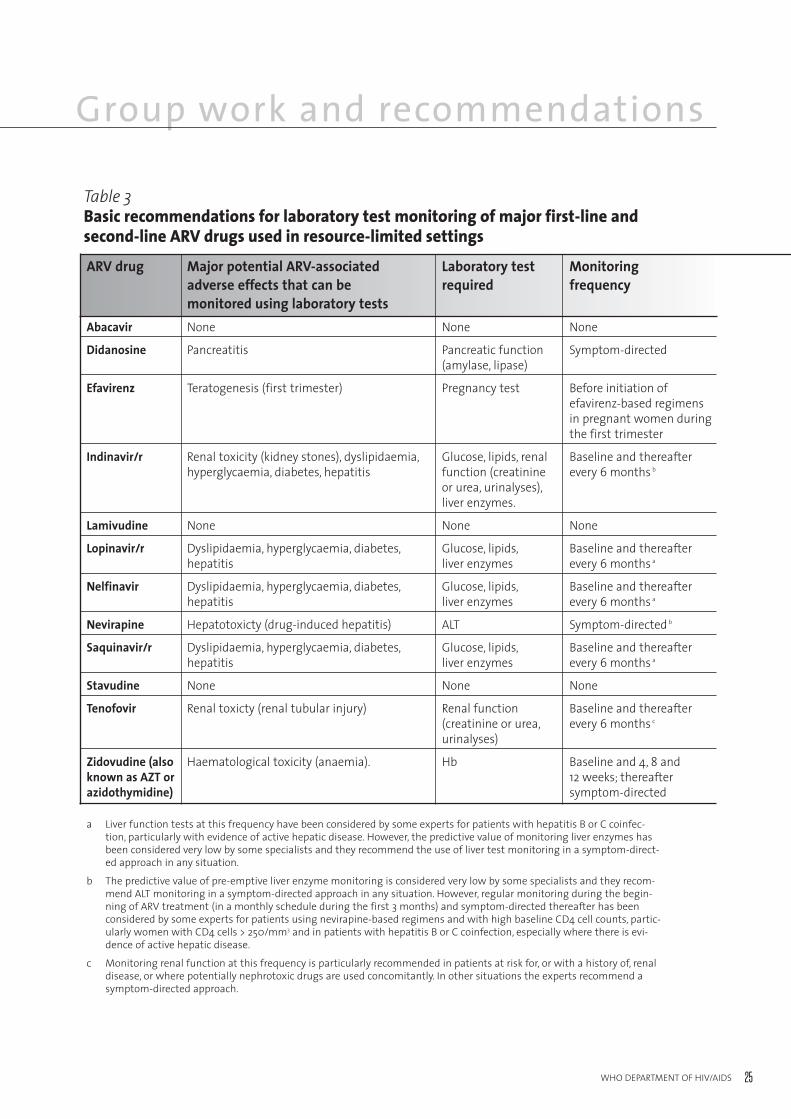
25WHO DEPARTMENT OF HIV/AIDS
Group work and recommendations
a Liver function tests at this frequency have been considered by some experts for patients with hepatitis B or C coinfec-tion, particularly with evidence of active hepatic disease. However, the predictive value of monitoring liver enzymes hasbeen considered very low by some specialists and they recommend the use of liver test monitoring in a symptom-direct-ed approach in any situation.
b The predictive value of pre-emptive liver enzyme monitoring is considered very low by some specialists and they recom-mend ALT monitoring in a symptom-directed approach in any situation. However, regular monitoring during the begin-ning of ARV treatment (in a monthly schedule during the first 3 months) and symptom-directed thereafter has beenconsidered by some experts for patients using nevirapine-based regimens and with high baseline CD4 cell counts, partic-ularly women with CD4 cells > 250/mm3 and in patients with hepatitis B or C coinfection, especially where there is evi-dence of active hepatic disease.
c Monitoring renal function at this frequency is particularly recommended in patients at risk for, or with a history of, renaldisease, or where potentially nephrotoxic drugs are used concomitantly. In other situations the experts recommend asymptom-directed approach.
Table 3Basic recommendations for laboratory test monitoring of major first-line and second-line ARV drugs used in resource-limited settings
ARV drug Major potential ARV-associated Laboratory test Monitoringadverse effects that can be required frequencymonitored using laboratory tests
Abacavir None None None
Didanosine Pancreatitis Pancreatic function Symptom-directed(amylase, lipase)
Efavirenz Teratogenesis (first trimester) Pregnancy test Before initiation of efavirenz-based regimens in pregnant women during the first trimester
Indinavir/r Renal toxicity (kidney stones), dyslipidaemia, Glucose, lipids, renal Baseline and thereafter hyperglycaemia, diabetes, hepatitis function (creatinine every 6 months b
or urea, urinalyses),liver enzymes.
Lamivudine None None None
Lopinavir/r Dyslipidaemia, hyperglycaemia, diabetes, Glucose, lipids, Baseline and thereafter hepatitis liver enzymes every 6 months a
Nelfinavir Dyslipidaemia, hyperglycaemia, diabetes, Glucose, lipids, Baseline and thereafter hepatitis liver enzymes every 6 months a
Nevirapine Hepatotoxicty (drug-induced hepatitis) ALT Symptom-directed b
Saquinavir/r Dyslipidaemia, hyperglycaemia, diabetes, Glucose, lipids, Baseline and thereafter hepatitis liver enzymes every 6 months a
Stavudine None None None
Tenofovir Renal toxicty (renal tubular injury) Renal function Baseline and thereafter(creatinine or urea, every 6 months c
urinalyses)
Zidovudine (also Haematological toxicity (anaemia). Hb Baseline and 4, 8 and known as AZT or 12 weeks; thereafter azidothymidine) symptom-directed
???????26
Group work 2. Review of current labora-tory requirements for antiretroviral therapy roll-out: laboratory expertsThe points for discussion were as follows.
What technologies are available? What needs to be evaluated? What is in the pipeline?
◗ Selection of appropriate technologies for differenthealth care levels.
– CD4; VL; basic laboratory tests, others
> What is available?
> What are the parameters? (See draft tablefor CD4.)
> What are acceptable quality standards?
◗ Review minimum laboratory requirements andamend where necessary.
◗ Need for CD4 counts at primary health care level –is this realistic? Will depend on tests currently indevelopment
◗ More guidance needed on sample collection/storage/transport, stability of samples for samplereferrals to higher-level laboratories
◗ QA/QC issues
◗ Service and maintenance
The following recommendations were made.
◗ There should be a clear understanding of thetargeted population for CD4+ T-cell monitoring,e.g. adults versus children.
◗ The performance and quality of technologiesshould be assessed and validated by means ofmultisite evaluation studies, with independent dataanalysis, e.g. through WHO.
◗ The selection of appropriate technologies shouldbe based on scientific evidence, the estimatedcurrent and future workload (number of speci-mens to be processed daily), the volumethroughput, the physical laboratory infrastructure,the capacity of laboratory staff and the availabilityof technical maintenance support.
◗ Demographic forecasts should be obtained withreference to rural versus urban numbers, theprevalence and incidence of HIV, volume catchareas and national coverage.
◗ The option of centralized testing should be consid-ered with reference to sample collection andstorage/transport, as should QA/QC issues, e.g.the use of samples from the previous day.
◗ CD4 determinations were not required at theprimary health care level. Either patients or speci-mens could be referred to district or provinciallaboratories.
◗ Service and maintenance contracts should beobtained when sophisticated equipment was beingpurchased. WHO should advocate to manufac-turers that capacity be developed for better servicefrom local distributors at the country or regionallevel.
◗ WHO should provide training and develop trainingmaterials, including generic SOPs, for laboratorytests supporting the roll-out of ART.
◗ WHO and its partners should continue to nego-tiate reduced prices for HIV/AIDS-relatedtechnologies.
27WHO DEPARTMENT OF HIV/AIDS
Group work and recommendations
Group work 3. Scale-up: What is needed?The points for discussion were as follows.
◗ National short-term and long- term plan
> National coverage (How many units of each type of equipment and where are they needed?)
> Current and future estimation of needs for each of the laboratory technologies
> Degree of standardization at national level
> Organization and management of laboratories / testing sites (including supervision)
> Allowance for flexibility, introduction of future technologies
> Sustainability
◗ Centralization versus decentralization (logistics)
◗ Infrastructure requirements and technologyrequirements
> Scale-up of ART with scale-up of laboratory support
> Catering for all types of patients (adults and children)
◗ Procurement and supply management issues
◗ Local capacity for maintenance of technologies,good service delivery ( knowledgeable local distrib-utors)
◗ Training on technologies , appropriate use of tech-nologies, SOPs
◗ QA
The following recommendations were made.
◗ Each ministry of health should establish a nationalplan of laboratory support for ART roll-out with a specific budget component. Input from both clinical and laboratory experts, people living withHIV/AIDS, and relevant programmes, e.g. TB,NGOs, should be incorporated. Communicationand collaboration between all parties should be fostered.
◗ In order to ensure the sustainability ofprogrammes, budget allocations should be real-istic, covering not only the purchase of equipmentand reagent costs but also transport, data entry,training, maintenance and QA. Long-term political
commitment is vital for the continuity of supplies,staff retention and annual strategic planningreviews.
◗ Health ministries should estimate how manypatients require treatment within the budget allo-cation at each level of the health care setting andshould forecast the volume of testing accordingly.
◗ Each health ministry should establish both a clin-ical and a laboratory referral network. Minimumrequirements for human resources and infrastruc-ture for both networks should be defined. Theimpact on the other services should not be compro-mised. An integrated data management systemcovering clinical and laboratory data, and linkagesbetween centralized and decentralized laboratories,should be set up.
◗ Each health ministry should develop a short-term(1–2-year) and longer-term (5-year) forecast plan inrespect of equipment needs, covering the range oftests, the anticipated volumes and the availablesuppliers. When contracts are being negotiated it isnecessary to consider training requirements, main-tenance, QA and technological developments. Ifnew, more appropriate technology is likely tobecome available shortly it may be wise to leaserather than buy current technology.
◗ Each health ministry should, as far as possible,standardize the technologies used ( CD4, VL,haematology, clinical chemistry, HIV serology, OI,STI, TB, etc) at each health care level. Thisapproach should cover training, SOPs , QAprogrammes and supervision.
◗ WHO should develop generic plans for each of theelements/components of a national laboratory andARV support plan.
◗ WHO should develop generic SOPs for the maintechnologies and maintain and expand QA activi-ties, including guidelines and training on GLP.
◗ WHO should rapidly disseminate new informationon relevant technologies.
◗ WHO should build capacity for the local evaluationof technologies.
◗ Procurement and supply management at thecountry level should be strengthened with the helpof WHO and its partners.
???????28
Group work 4. Innovative and operational research The discussion covered the following points.
What specifications, operational characteristics and costsfor technologies appropriate in resource-poor settings arerequired?
> Simplified techniques for ease of use (less specialized training/support; suitable for children)
> Electricity
> Temperature and humidity
> Cost of equipment and reagents
> Dried fluid spots
> QC
◗ What technologies are currently under develop-ment and when are they expected to becomeavailable on the commercial market?
◗ Current technologies; develop and assess testprocedures for paediatric use
◗ Are all current technologies suitable for monitoring?
> CD4 manual methods?
◗ What are the optimal time intervalsfor determining:
> CD4 levels?
> Do TLCs equal CD4 counts?
> Toxicity tests?
> Early diagnosis infants with RNA tests?
The following recommendations were made.
◗ In five years it should be possible to diagnose HIVinfection and monitor ARV in infants, childrenand adults at the primary health care level.
◗ In five years it should be possible, at the districtlevel, to diagnose HIV infection, to monitortherapy with CD4 counts, to diagnose and treatcommon OIs (TB, toxoplasmosis, cryptococcaldiseases), identify toxicity and flag patients(infants, children and adults) in whom therapy isfailing, ideally with a multiplex instrument. WHO should advocate the development of suchinstruments
Currently, there were alternative options forfulfilling these tasks. Once validated, the PointCareinstrument would come close to meeting the CD4monitoring needs. However, QA/QC would have tobe developed.
◗ WHO should facilitate the development of innova-tive diagnostics that are simple, rapid, robust andinexpensive point-of-care assays for absolute andpercentage CD4 counts and for the diagnosis ofinfants aged up to 2–3 months.
◗ The dried blood or fluid spot referral systemapproach for DNA PCR and VL for early diagnosisof infants should be validated under field condi-tions.
◗ Independent comparative multisite evaluations ofnew CD4 technologies, including Cyflow Counter,Cyflow Green, EasyCD4, PointCare, LabNow andSemibio versus the gold standard methods (flowcytometry and FACSCount) should be conductedonce the technologies are commercially available.The tolerance for accuracy divergence should beestablished on clinical needs, with reference towhat is acceptable (1%, 5%, 10% or 20% awayfrom the gold standard if other specifications aremet).
◗ Independent multisite comparative evaluation ofVL assays, e.g. ExaVir and Retina Rainbow, shouldbe conducted once commercially available. (WHOhad a pilot comparative evaluation at one site.)
◗ The performance of all assays should be subject toappropriate quality measures, including built-inQC as well as external quality assessment.
◗ Strong linkages should be established betweenclinical sites and laboratory sites, and databasescorrelating clinical and laboratory outcomes shouldbe set up. Harmonization was vital.
◗ WHO should conduct a clinical study to definetreatment failure and should assess the impact of early versus late switching to second-line regimens.
◗ WHO should develop a standardized adherencequestionnaire and investigate its value for makingtreatment decisions.
◗ More precise guidance was needed to determinethe best switch options on the basis of clinical findings.

29WHO DEPARTMENT OF HIV/AIDS
Group work and recommendations
◗ The utility of CD4 and VL testing in the clinicalmanagement of patients on ART living inresource-limited settings should be investigatedin other trials like DART.
◗ WHO should validate the utility of manual CD4methods as tools for initiating and monitoringART and making appropriate clinical decisionsconcerning patients on ART in resource-limitedsettings.
◗ WHO should validate the utility of total lympho-cyte counts as tools for initiating and monitoringART and making appropriate clinical decisions for patients on ART.
◗ The utility of toxicity tests (ALT ) for clinicalmanagement should be investigated.
◗ The influence of viral clades and coinfections (TB, malaria, etc.) on the effectiveness of currentassays and monitoring protocols should be studied.
◗ Reference values for CD4 for adults and infants ≤in countries most affected by the epidemic shouldbe collated.
◗ WHO should promote even more strongly the combination of two or three rapid HIV tests to confirm HIV seropositivity.
◗ WHO should conduct a survey of CD4 technolo-gies in order to compare them in respect of costper patient-result, daily throughput, days lost toequipment failure, staffing levels and trainingrequirements.
◗ WHO should promote the development and validate the reliability of simple bedside VL tests.
◗ WHO should conduct studies to determine the VL level appropriate to triggering a clinical decision to switch therapy. (Were there othersimple inexpensive laboratory tests? What was the role of hepatitis B virus and hepatitis C virusscreening in relation to treatment regimens withnevirapine and lamivudine)
◗ WHO should conduct studies on the value of VL as an adherence tool.
◗ WHO should develop and validate a standardizedpatient questionnaire for the assessment of adher-ence and should compare both adherence tools.
◗ WHO should support the development and vali-date the reliability of new technologies that detectlatent TB infection and can diagnose smear-nega-tive active TB infections in under 24 hours.
◗ WHO should assess the performance of currentlyavailable technologies for the early detection ofHIV infection in children and should provide guidance on HIV diagnosis in children. (Whatwere the technologies and what were the timeintervals for specific available technologies?)
◗ WHO should support the development of newsimple technologies for detecting ARV resistance.
There was no agreement concerning further studies onmanual CD4 methods. WHO was potentially interestedin validating a reverse external quality assessmentapproach for manual methods. However, if manualmethods were becoming obsolete this might no longer bea priority.
Closing RemarksDr Gilks thanked the participants for their commitmentand three days of hard work. Bringing the clinicians andlaboratory experts together at the global level had beenvery fruitful and it was desirable for similar meetings tobe held at the regional and national levels.

???????30
31WHO DEPARTMENT OF HIV/AIDS
Annex 1. Programme of work
Monday 13 December 2005
08:30 – 09:00 Registration
09:00 – 09:30 Opening address Dr Jim Yong Kim, Director, HIV/AIDS
09:30 – 10:00 Objectives of the meeting and Dr Charles Gilks, Coordinator, TPSreview of current WHOrecommendations
10:00 – 10:15 Review of HIV/AIDS diagnostic Dr Gaby Vercauterensupport activities
10:15 – 10:30 Discussion
10:30 – 10:45 Tea/coffee
10:45 – 11:00 Scale-up experience in country Dr Sylvia Ojoo(Kenya)
11:00 – 11:15 Scale-up experience in country Dr Salif Sow(Senegal)
11:15 – 11:30 Scale-up experience in country Dr Anupong Chitwarakorn(Thailand)
11:30 – 11:45 Scale-up experience in country (MSF) Dr Alexandra Calmy
11:45 – 12:00 Scale-up experience in country (Brazil) Dr Mauro Schechter
12:00 – 13:00 Discussion
13:00 – 14:00 Lunch
14:00 – 14:20 Clinical issues: monitoring adults Dr Robert Colebunders
14:20 – 14:40 Clinical issues: monitoring children Dr Gabriel Anabwani
14:40 – 15:00 Resistance Dr Don Sutherland
15:00 – 15:20 Technology for resistance monitoring Dr Martine Peeters
15:20 – 15:40 CD4 technologies Dr Frank Mandy
15:40 – 16: 00 Tea/coffee
16:00 – 16:10 CD4 technologies (Partec) Dr Luc Kestens
16.10 – 16:20 CD4 determinations for paediatrics Dr Frank Denny
16:20 – 16:40 VL technologies and incidence assay Dr Elizabeth Dax Taylor
16:40 – 17:00 ARV toxicity monitoring (haematology / Dr Wendy Stevensclinical chemistry)
17:00 – 17:20 TB/HIV laboratory issues Dr Pierre-Yves Norval
17:20 – 18:00 Discussion
???????32
Tuesday 14 December 2005
09:00 – 09:15 Review of day 1 Rapporteurs
Procurement issues
09:15 – 09:30 WHO prequalification process Dr Olivier Gross
09:30 – 09:40 WHO selection of appropriate Ms Anita Sands diagnostic technology
09:40 – 10:00 WHO procurement – CPS Ms Françoise Mas
10:00 – 10:15 UNICEF Dr Ludo Scheerlinck
10:15 – 10:30 AMDS Dr Jos Perriëns
10:30 – 10:45 Discussion
10:45 – 11:00 Tea/coffee11:00 – 13:00 Working groups
Review of clinical recommendations:Groups A and BReview of laboratory recommendations:Groups C and D
13:00 – 14:00 Lunch
14:00 – 15:00 Continuation of working groups
15:00 – 15:10 Presentations: Clinical Group A
15:10 – 15:20 Presentations: Clinical Group B
15:20 – 15:45 Discussion
15:45 – 16:00 Tea/coffee
16:00 – 16:10 Presentation: Laboratory Group C
16:10 – 16:20 Presentation: Laboratory Group D
16:20 – 17:00 Discussion
33WHO DEPARTMENT OF HIV/AIDS
Wednesday 15 December 2005
09:00 – 09:30 Review of day 2 Rapporteurs
09:30 – 10:45 Group work. Scale-up: what is needed?Clinical Group A and Laboratory Group CGroup work: Innovative and operational research: Clinical Group B and Laboratory Group D
10:45 – 11:00 Tea/coffee
11:00 – 11:50 Group work continued
11:50 – 12:00 Presentation of group work:Scale-up, clinical
12:00 – 12:30 Discussion
12:30 – 12:40 Presentation of group work:Scale-up, laboratory
12:40 – 13:00 Discussion
13:00 – 14:00 Lunch
14:00 – 14:10 Presentation of group work:Research agenda, clinical
14:10 – 14:30 Discussion
14:30 – 14:40 Presentation of group work:Research agenda, laboratory
14:40 – 15:00 Discussion
15:00 – 15:15 Updated recommendations: Plenary
15:15 – 15:45 Discussion
15:45 – 16:00 Tea/coffee
16:00 – 16:30 Recommendations and closure
Annex 1. Programme of work

???????34
35WHO DEPARTMENT OF HIV/AIDS
Annex 2. List of participants
LABORATORY EXPERTSEl-Hadj BELABBESInstitut Pasteur d’Algerie Annexe de Sidi fredj AlgerALGERIA
Deborah BURGESSProgram Officer, Global Health Technologies Global Health Program Bill and Melinda Gates Foundation USA
Ben CHENGProject ManagerForum for Collaborative HIV ResearchThe George Washington University Medical CenterUSA
Suzanne CROWEMacfarlane Burnet Institute AUSTRALIA
Elizabeth DAX National Serology Reference LaboratoryAUSTRALIA
Thomas N. DENNYAssociate Professor, PathologyLaboratory Medicine and PediatricsAssistant Dean for Research in Health Policy New JerseyDepartment of PediatricsUSA
Alsane DIAWUniversité Cheikh Anta DIOPLaboratoire de Bactériologie VirologieSENEGAL
Robert DOWING (unable to attend)Laboratory DirectorCenters for Disease Control and Prevention UgandaUGANDA
Katrien FRANSENDirector ARLDepartment of MicrobiologyInstitute of Tropical MedicineBELGIUM
Martine GUILERMELaboratory ExpertMédecins Sans Frontières SWITZERLAND
Ilesh JANI Department of ImmunologyInstituto Nacional de SaùdeMOZAMBIQUE
Luc KESTENSDr Luc KESTENS Department of Infectious Diseases(Immunology)Institute of Tropical MedicineBELGIUM
Frank MANDYBureau of HIV/AIDS, STD and TB CANADA
Catherine MUNDYPrincipal Programme Associate for Laboratory ServicesCenter for Health Systems and ServicesManagement Sciences for Health Inc USA
John PARRYDeputy DirectorSexually Transmitted and Bloodborne Virus LaboratoryHealth Protection Agency UNITED KINGDOM
Kovit PATTANAPANYASATOffice for Research and DevelopmentFaculty of MedicineSiriraj HospitalMahidol University THAILAND
???????36
Martine PEETERSProgramme SIDA/ORMSTROMLaboratoire RétrovirusFRANCE
N. PYNDIAHHIV/AIDS/STI Reference LaboratoryCentral Health Laboratory MAURITIUS
William R. RODRIGUEZDirectorOffice of Internatinal ProgramsThe Landmark CenterUSA
Boran SARLaboratory of Medical MicrobiologyPasteur Institute of CambodiaCAMBODIA
Bobilwinde Robert SOUDREUniversité de OuagadougouFaculté des Sciences de la SantéBURKINA FASO
Wendy STEVENSDepartment of Haematology and Molecular MedicineUniversity of WitwatersrandFaculty of Health SciencesSOUTH AFRICA
Peter TREVOR (unable to attend)Botswanna Harvard HIV Reference LaboratoryPrincess Marina HospitalBOTSWANNA
Dawit WOLDAYLaboratory Manager Ethio-Netherlands AIDS Research Project (ENARP) Ethiopian Health and Nutrition Research Institute ETHIOPIA
CLINICAL EXPERTSGabriel ANABWANIBotswana Baylor Children's ClinicalCentre of ExcellencePrincess Marina Hospital CampusGABORONE
Alexandra CALMYClinical ExpertMédecins Sans FrontièresSWITZERLAND
Anupong CHITWARAKORNSenior Expert, HIV/STIDepartment of Disease ControlMinistry of Public HealthTHAILAND
Karen COHENUniversity of Cape TownSOUTH AFRICA
Robert COLEBUNDERSInfectious Diseases Institute Mulago Hospital UGANDA
Gregg GONSALVESDirector of Treatment and Prevention AdvocacyGay Men's Health CrisisUSA
Kate GRIMWADEDepartment of Clinical Infection City General HospitalStoke-on-TrentUNITED KINDGOM
James HAKIMAssociate Professor and ChairmanDepartment of MedicineUniversity of ZimbabweZIMBABWE
37WHO DEPARTMENT OF HIV/AIDS
Annex 2. List of participants
OTHERSPaul LALVANIProcurement ManagerThe Global Fund for AIDS, Tuberculosis and MalariaSWITZERLAND
Ludo SCHEERLINCKTechnical Officer, MedicalUNICEF Supply DivisionDENMARK
WHO SECRETARIATGuy-Michel GERSHY-DAMETRPA/DDCAFRO ZIMBABWE
Anthony GOMESDHS/TLROffice of the WHO Representative PAPUA NEW GUINEA
Israel KALYESUBULAConsultant PaediatricianMulago HospitalMakerere University Department of Paediatrics UGANDA
N. KUMARASAMYChief Medical Officer and Clinical ResearchYRG Centre for AIDS for Research and EducationVoluntary Health Services INDIA
Jean-Élie MALKINDirecteur MédicalPartners for Nairobi FRANCE
Paula MUNDERIDisease Manager, HIV/AIDSEuropean and Developing Countries Clinical Trials PartnershipNETHERLANDS
Sylvia OJOONASCOPKenyatta National Hospital GroundsKENYA
Mauro SCHECHTERHead, AIDS Research LaboratoryHospital Universitario Clementino Fraga FilhoUniversidade Federal de Rio de JaneiroBRAZIL
Papa Salif SOW Dakar University Teaching HospitalDepartment of Infectious DiseasesSENEGAL
WHO HEADQUARTERSCharles GILKS CoordinatorTreatment and Prevention Scale-upDepartment of HIV/AIDS
Oliver GROSSEssential Drugs and MedicinesHealth Technology and Pharmaceuticals
Jim Yong KIMDirectorDepartment of HIV/AIDS
Françoise MASInfrastructure and Logistics Services
Pierre-Yves NORVALTB/HIV and Drug ResistanceStop TB Department
Jos PERRIENSCoordinatorAIDS Medicines and Diagnostics ServiceDepartment of HIV/AIDS
Anita SANDSEssential Health TechnologiesHealth Technology and Pharmaceuticals
Don SUTHERLANDStrategic Information and ResearchDepartment of HIV/AIDS
Kenji TAMURAAIDS Medicines and Diagnostics ServiceDepartment of HIV/AIDS
Gaby VERCAUTERENEssential Health TechnologiesHealth Technology and Pharmaceuticals
Marco VITORIATreatment and Prevention Scale-upDepartment of HIV/AIDS
???????38
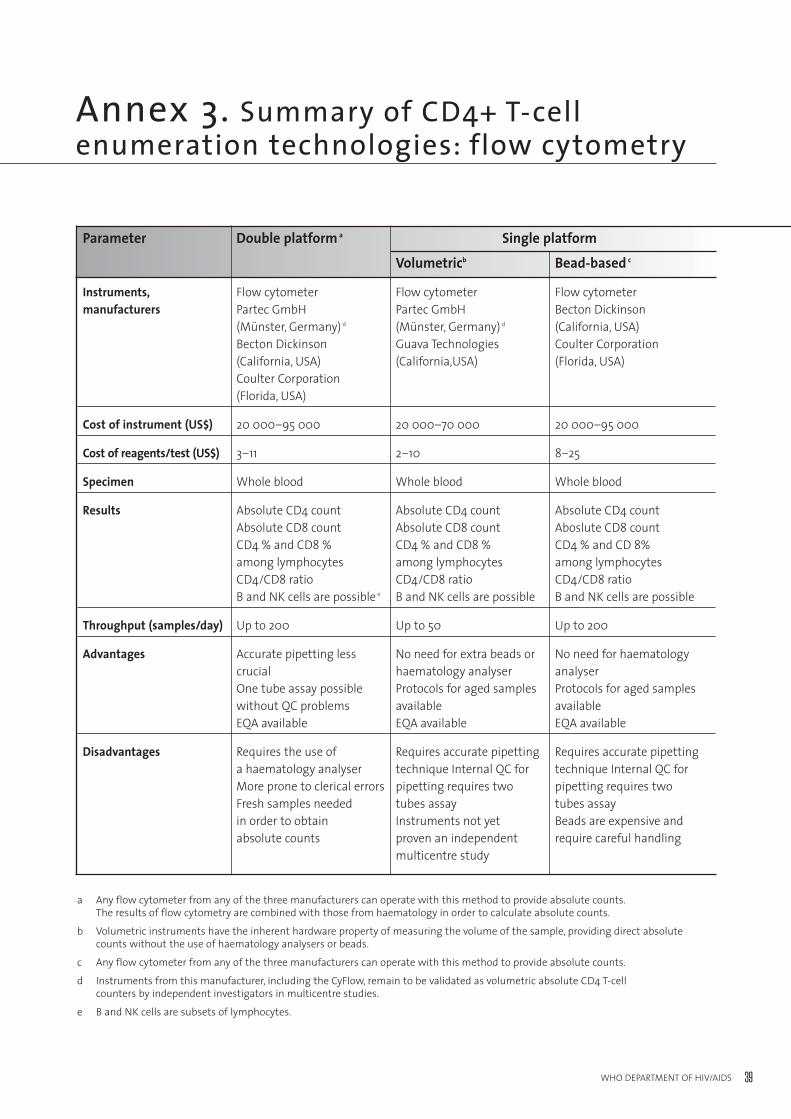
39WHO DEPARTMENT OF HIV/AIDS
Annex 3. Summary of CD4+ T-cell enumeration technologies: flow cytometry
a Any flow cytometer from any of the three manufacturers can operate with this method to provide absolute counts.The results of flow cytometry are combined with those from haematology in order to calculate absolute counts.
b Volumetric instruments have the inherent hardware property of measuring the volume of the sample, providing direct absolutecounts without the use of haematology analysers or beads.
c Any flow cytometer from any of the three manufacturers can operate with this method to provide absolute counts.
d Instruments from this manufacturer, including the CyFlow, remain to be validated as volumetric absolute CD4 T-cell counters by independent investigators in multicentre studies.
e B and NK cells are subsets of lymphocytes.
Parameter Double platform a Single platform
Volumetricb Bead-based c
Instruments, Flow cytometer Flow cytometer Flow cytometermanufacturers Partec GmbH Partec GmbH Becton Dickinson
(Münster, Germany) d (Münster, Germany) d (California, USA)Becton Dickinson Guava Technologies Coulter Corporation(California, USA) (California,USA) (Florida, USA)Coulter Corporation (Florida, USA)
Cost of instrument (US$) 20 000–95 000 20 000–70 000 20 000–95 000
Cost of reagents/test (US$) 3–11 2–10 8–25
Specimen Whole blood Whole blood Whole blood
Results Absolute CD4 count Absolute CD4 count Absolute CD4 countAbsolute CD8 count Absolute CD8 count Aboslute CD8 countCD4 % and CD8 % CD4 % and CD8 % CD4 % and CD 8%among lymphocytes among lymphocytes among lymphocytesCD4/CD8 ratio CD4/CD8 ratio CD4/CD8 ratioB and NK cells are possible e B and NK cells are possible B and NK cells are possible
Throughput (samples/day) Up to 200 Up to 50 Up to 200
Advantages Accurate pipetting less No need for extra beads or No need for haematology crucial haematology analyser analyser One tube assay possible Protocols for aged samples Protocols for aged samples without QC problems available availableEQA available EQA available EQA available
Disadvantages Requires the use of Requires accurate pipetting Requires accurate pipetting a haematology analyser technique Internal QC for technique Internal QC forMore prone to clerical errors pipetting requires two pipetting requires two Fresh samples needed tubes assay tubes assayin order to obtain Instruments not yet Beads are expensive and absolute counts proven an independent require careful handling
multicentre study
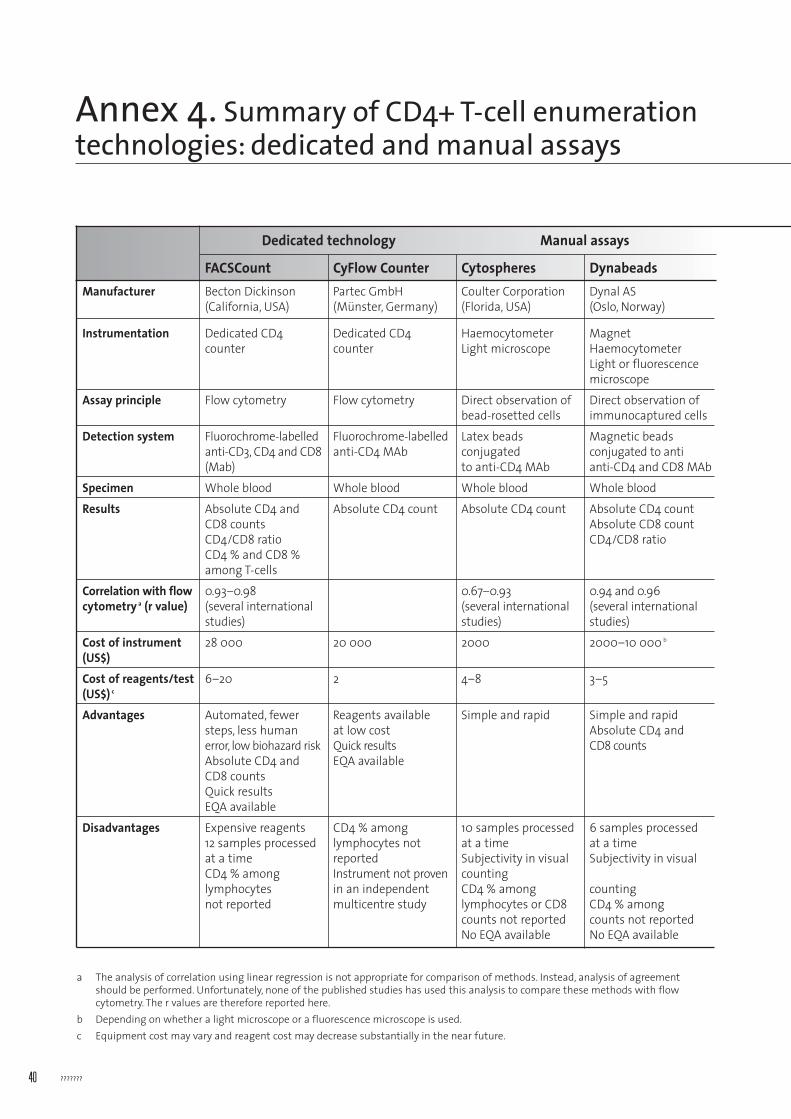
???????40
Annex 4. Summary of CD4+ T-cell enumerationtechnologies: dedicated and manual assays
a The analysis of correlation using linear regression is not appropriate for comparison of methods. Instead, analysis of agreementshould be performed. Unfortunately, none of the published studies has used this analysis to compare these methods with flowcytometry. The r values are therefore reported here.
b Depending on whether a light microscope or a fluorescence microscope is used.c Equipment cost may vary and reagent cost may decrease substantially in the near future.
Dedicated technology Manual assays
FACSCount CyFlow Counter Cytospheres DynabeadsManufacturer Becton Dickinson Partec GmbH Coulter Corporation Dynal AS
(California, USA) (Münster, Germany) (Florida, USA) (Oslo, Norway)
Instrumentation Dedicated CD4 Dedicated CD4 Haemocytometer Magnetcounter counter Light microscope Haemocytometer
Light or fluorescence microscope
Assay principle Flow cytometry Flow cytometry Direct observation of Direct observation of bead-rosetted cells immunocaptured cells
Detection system Fluorochrome-labelled Fluorochrome-labelled Latex beads Magnetic beads anti-CD3, CD4 and CD8 anti-CD4 MAb conjugated conjugated to anti(Mab) to anti-CD4 MAb anti-CD4 and CD8 MAb
Specimen Whole blood Whole blood Whole blood Whole blood
Results Absolute CD4 and Absolute CD4 count Absolute CD4 count Absolute CD4 countCD8 counts Absolute CD8 countCD4/CD8 ratio CD4/CD8 ratioCD4 % and CD8 % among T-cells
Correlation with flow 0.93–0.98 0.67–0.93 0.94 and 0.96 cytometry a (r value) (several international (several international (several international
studies) studies) studies)
Cost of instrument 28 000 20 000 2000 2000–10 000 b
(US$)
Cost of reagents/test 6–20 2 4–8 3–5(US$) c
Advantages Automated, fewer Reagents available Simple and rapid Simple and rapidsteps, less human at low cost Absolute CD4 and error, low biohazard risk Quick results CD8 countsAbsolute CD4 and EQA availableCD8 countsQuick results EQA available
Disadvantages Expensive reagents CD4 % among 10 samples processed 6 samples processed 12 samples processed lymphocytes not at a time at a timeat a time reported Subjectivity in visual Subjectivity in visual CD4 % among Instrument not proven countinglymphocytes in an independent CD4 % among counting not reported multicentre study lymphocytes or CD8 CD4 % among
counts not reported counts not reportedNo EQA available No EQA available
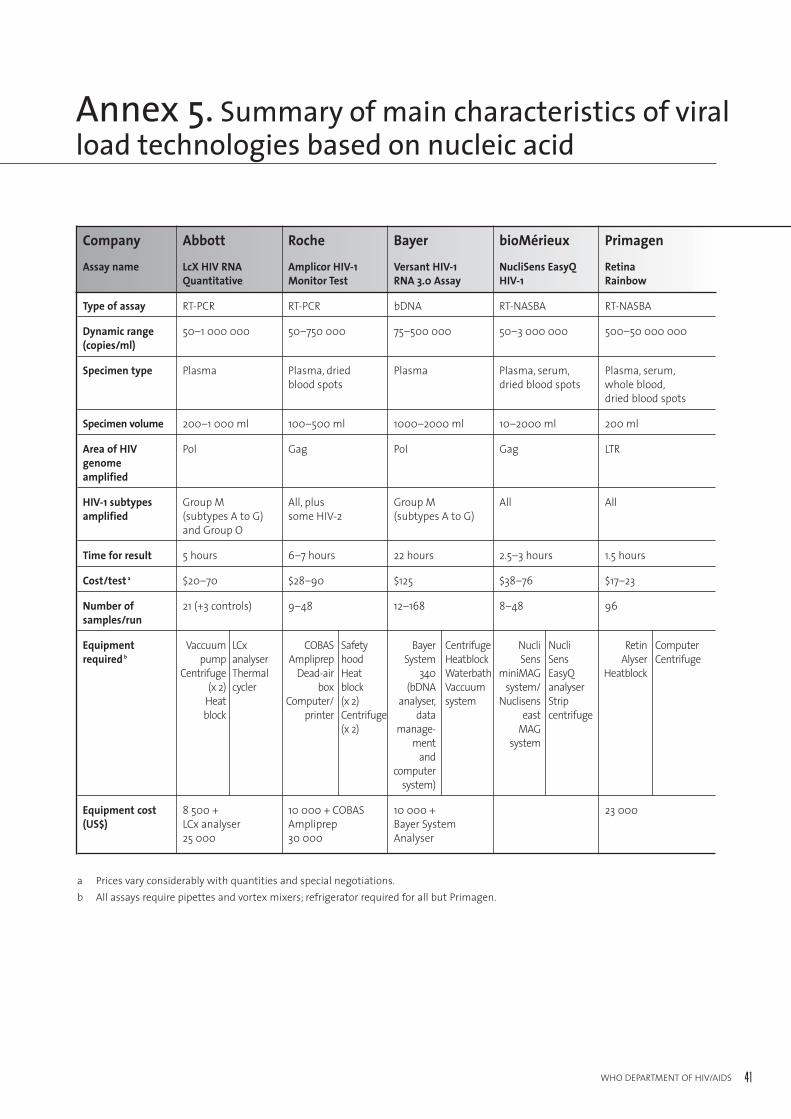
41WHO DEPARTMENT OF HIV/AIDS
Annex 5. Summary of main characteristics of viralload technologies based on nucleic acid
a Prices vary considerably with quantities and special negotiations.b All assays require pipettes and vortex mixers; refrigerator required for all but Primagen.
Company Abbott Roche Bayer bioMérieux Primagen
Assay name LcX HIV RNA Amplicor HIV-1 Versant HIV-1 NucliSens EasyQ RetinaQuantitative Monitor Test RNA 3.0 Assay HIV-1 Rainbow
Type of assay RT-PCR RT-PCR bDNA RT-NASBA RT-NASBA
Dynamic range 50–1 000 000 50–750 000 75–500 000 50–3 000 000 500–50 000 000(copies/ml)
Specimen type Plasma Plasma, dried Plasma Plasma, serum, Plasma, serum,blood spots dried blood spots whole blood,
dried blood spots
Specimen volume 200–1 000 ml 100–500 ml 1000–2000 ml 10–2000 ml 200 ml
Area of HIV Pol Gag Pol Gag LTRgenome amplified
HIV-1 subtypes Group M All, plus Group M All Allamplified (subtypes A to G) some HIV-2 (subtypes A to G)
and Group O
Time for result 5 hours 6–7 hours 22 hours 2.5–3 hours 1.5 hours
Cost/test a $20–70 $28–90 $125 $38–76 $17–23
Number of 21 (+3 controls) 9–48 12–168 8–48 96samples/run
Equipment Vaccuum LCx COBAS Safety Bayer Centrifuge Nucli Nucli Retin Computerrequired b pump analyser Ampliprep hood System Heatblock Sens Sens Alyser Centrifuge
Centrifuge Thermal Dead-air Heat 340 Waterbath miniMAG EasyQ Heatblock(x 2) cycler box block (bDNA Vaccuum system/ analyser
Heat Computer/ (x 2) analyser, system Nuclisens Strip block printer Centrifuge data east centrifuge
(x 2) manage- MAGment system
andcomputer
system)
Equipment cost 8 500 + 10 000 + COBAS 10 000 + 23 000(US$) LCx analyser Ampliprep Bayer System
25 000 30 000 Analyser
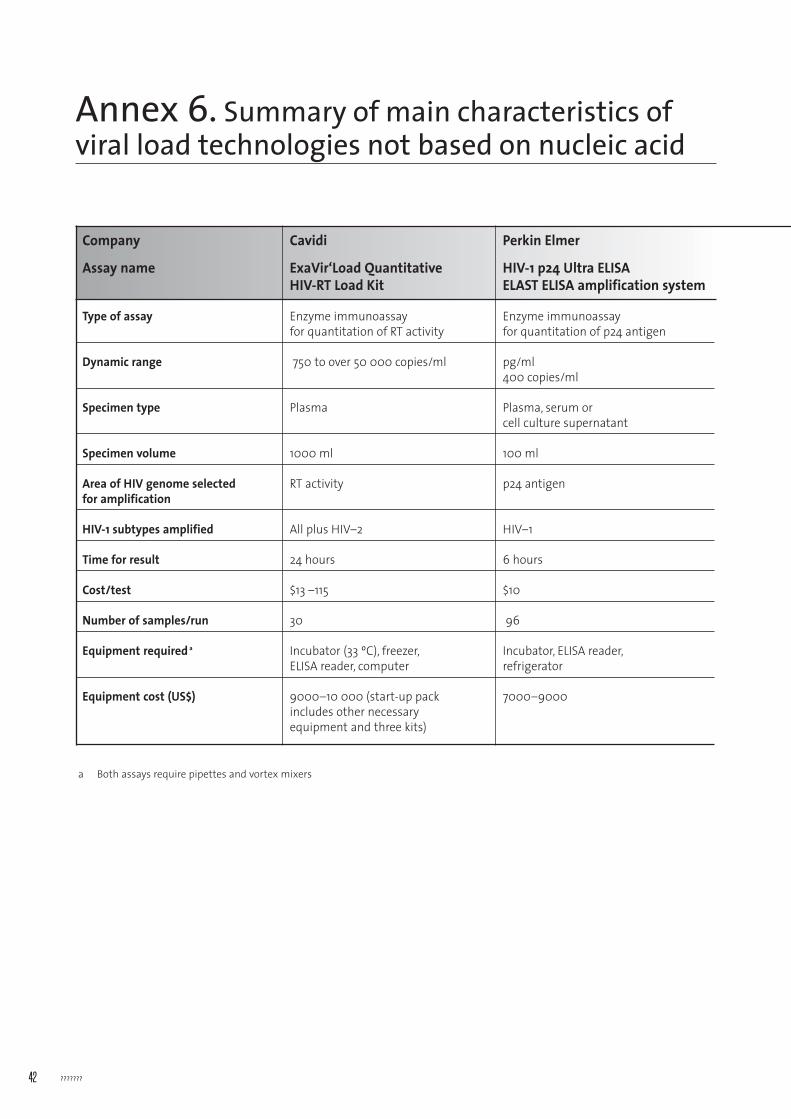
???????42
Annex 6. Summary of main characteristics of viral load technologies not based on nucleic acid
Company Cavidi Perkin Elmer
Assay name ExaVir‘Load Quantitative HIV-1 p24 Ultra ELISA HIV-RT Load Kit ELAST ELISA amplification system
Type of assay Enzyme immunoassay Enzyme immunoassay for quantitation of RT activity for quantitation of p24 antigen
Dynamic range 750 to over 50 000 copies/ml pg/ml400 copies/ml
Specimen type Plasma Plasma, serum or cell culture supernatant
Specimen volume 1000 ml 100 ml
Area of HIV genome selected RT activity p24 antigenfor amplification
HIV-1 subtypes amplified All plus HIV–2 HIV–1
Time for result 24 hours 6 hours
Cost/test $13 –115 $10
Number of samples/run 30 96
Equipment required a Incubator (33 ºC), freezer, Incubator, ELISA reader,ELISA reader, computer refrigerator
Equipment cost (US$) 9000–10 000 (start-up pack 7000–9000includes other necessary equipment and three kits)
a Both assays require pipettes and vortex mixers


For further information, contact:WORLD HEALTH ORGANIZATIONDepartment of HIV/AIDS20, avenue Appia – CH-1211 Geneva 27 – SWITZERLANDE-mail: [email protected] – http://www.who.int/hiv/en
ISBN 92 4 159368 7