Embed Size (px)
Citation preview

Dr Jonathan Koffman
Cicely Saunders Institute Department of Palliative Care, Policy & Rehabilitation King’s College London www.csi.kcl.ac.uk @jonathankoffman
WHO Collaborating Centre for
Palliative Care, Policy and
Rehabilitation
Is the experience and expression of living with severe MS ethnically and culturally patterned?
L.GB.03.2014.5852p November 2014
www.csi.kcl.ac.uk
Outline for this presentation
•Concepts, concepts, concepts
•MS and minority ethnic groups:
•What we know and importantly what we don’t:
• findings from mixed methods cross-sectional study
– MS progression and symptom burden
• Implications for clinical practice
www.csi.kcl.ac.uk 3
Understanding diversity and conceptual sloppiness
www.csi.kcl.ac.uk
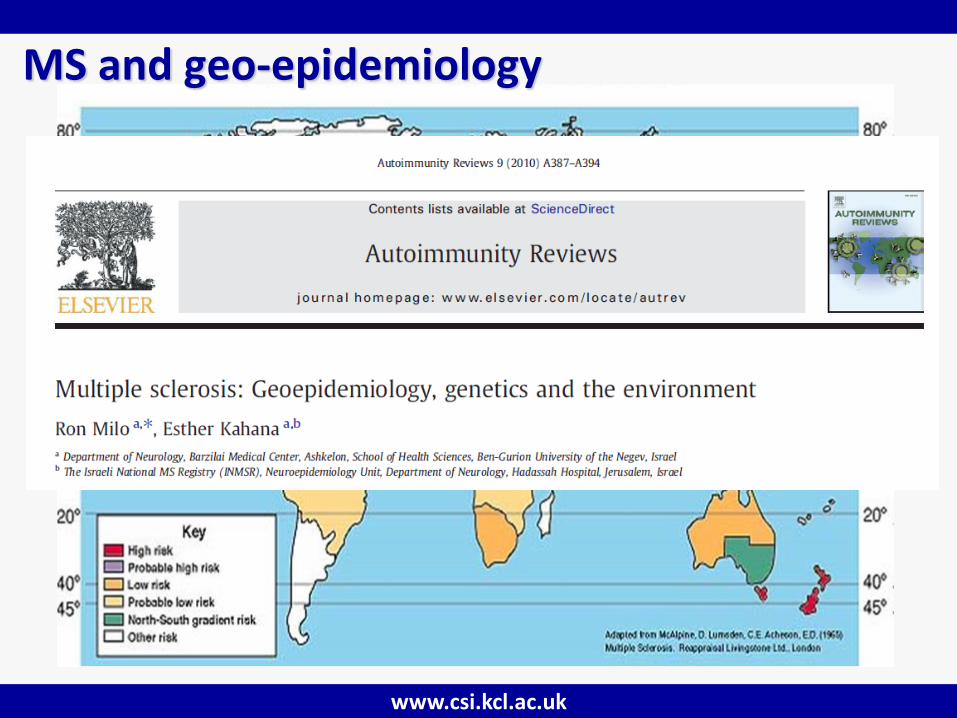
MS and geo-epidemiology
www.csi.kcl.ac.uk
MS and ethnicity: what do we know already and what questions remain?
• Number of people with the disease from BME groups has increased (Compston & Coles 2002)
• Ethnicity thought to influence clinical manifestations of MS e.g. more aggressive disease and greater disability (Alshami & Jeffrey 1998;Cree et al. 2004;Kaufman et al. 2003)
• BME groups also been shown to respond less well to treatment (Cree, Khan, Bourdette, & Goodin 2004)
www.csi.kcl.ac.uk

www.csi.kcl.ac.uk
www.csi.kcl.ac.uk
Study aim
•To describe and compare the experience of Black Caribbean and White British people severely affected by MS living in south London, and identify those with advanced disease that have needs that might benefit from palliative care

www.csi.kcl.ac.uk
Anatomy of our study
www.csi.kcl.ac.uk
Study design
• Concurrent mixed model:
• primary purpose to gain broader perspectives than using one method alone
• ‘embedded’ method addresses different questions than dominant method, or seeks different information
QUANT
qual

www.csi.kcl.ac.uk
Study setting
www.csi.kcl.ac.uk
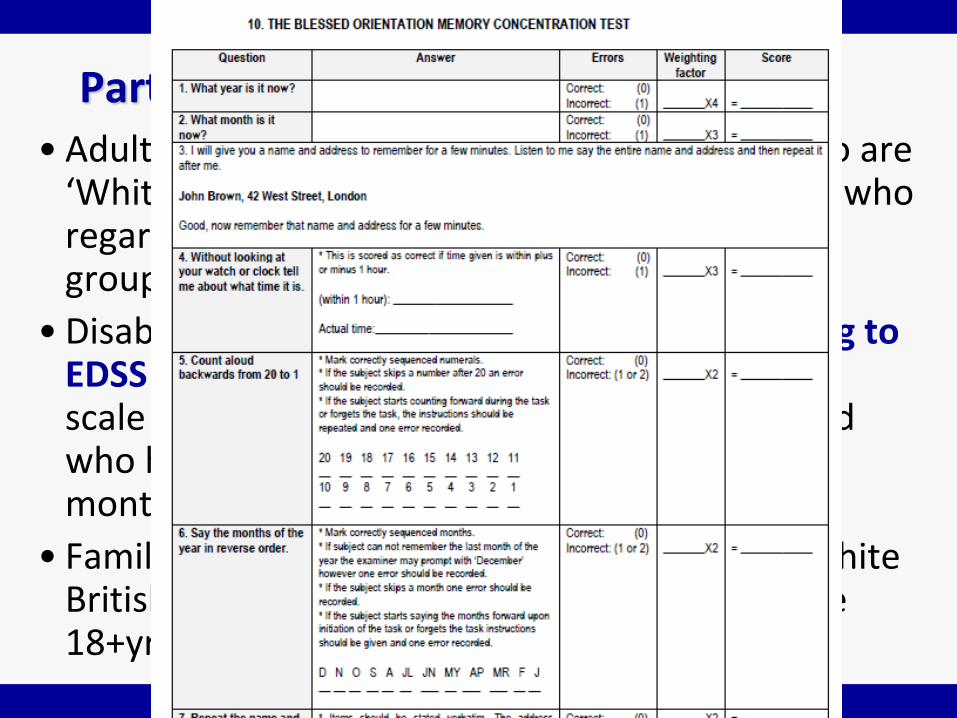
Participants: inclusion criteria • Adults (18+yr) with confirmed MS diagnosis who are
‘White British’, ‘Black Caribbean' and ‘Asian’, or who regard themselves as being from these ethnic groups;
• Disability score equal/greater than 6.0 according to EDSS (single item 10 point interviewer assessed scale used to assess disability (Kurtzke 1983) and who have been at level or lower for at least 2 months:
• Family members/main informal caregivers of White British and Black Caribbean PwMS only, who are 18+yrs, and able to consent
www.csi.kcl.ac.uk
Data collection: assessment of palliative care needs
• Multiple Sclerosis Impact Scale (MSIS) (Hobart et al 2001)
• Modified Fatigue Impact Scale (MFIS) (Fisk et al 1994)
• Hospital Anxiety and Depression Scale (HADS) Zigmond & Snaith 1983)
• Palliative Care Outcome Scale + POS-MS symptoms (Hearn & Higginson 1999, Higginson & Donaldson 2004))
www.csi.kcl.ac.uk
www.csi.kcl.ac.uk
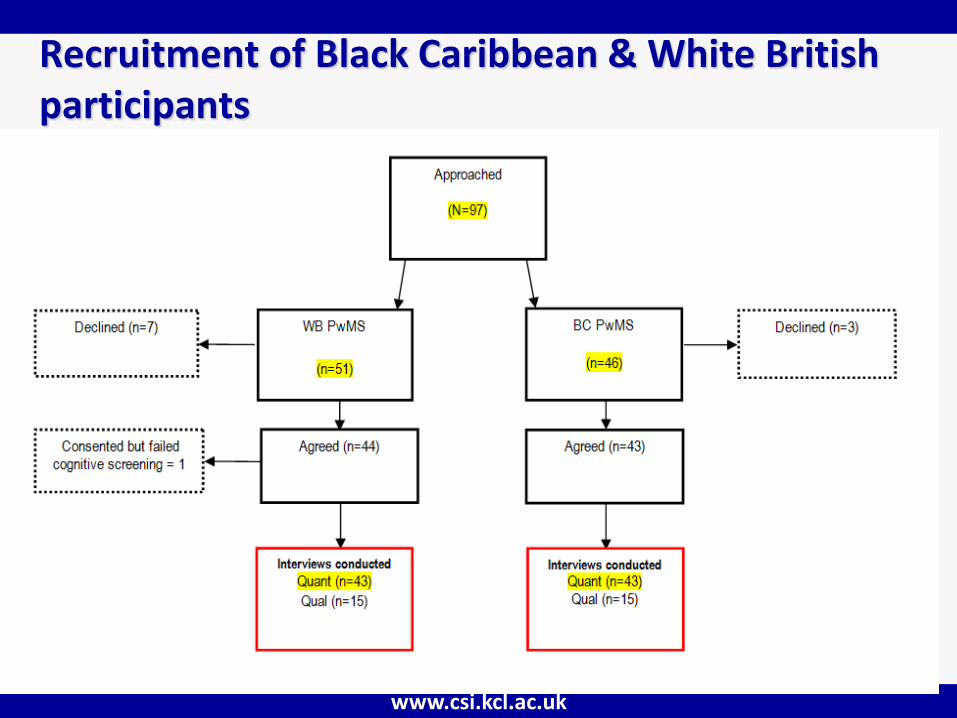
Recruitment of Black Caribbean & White British participants
www.csi.kcl.ac.uk
Doing the work: becoming a ‘reliable witness’
•Many potential transformations of identity wrought by study participants
•Not infrequently promoted to status of ‘reliable witness/confidante’ (Stanworth 2004)
www.csi.kcl.ac.uk
Doing the work: a divesting methodology • A very valuable lesson....
• Sensitive perceptions require suspension of conventional expectation
• Usually when you listen to some statement , you hear it as a kind of echo of yourself. You are actually listening to your own opinion (Longaker 1997:147)
• Counter intuitive that when listening to unwell people important to divest oneself from notion that MS was worst thing that could ever happen :
• overwhelming loneliness brought on by death of girlfriend
• long struggle with alcohol/drug dependency and refractory depression, suicide attempt
www.csi.kcl.ac.uk
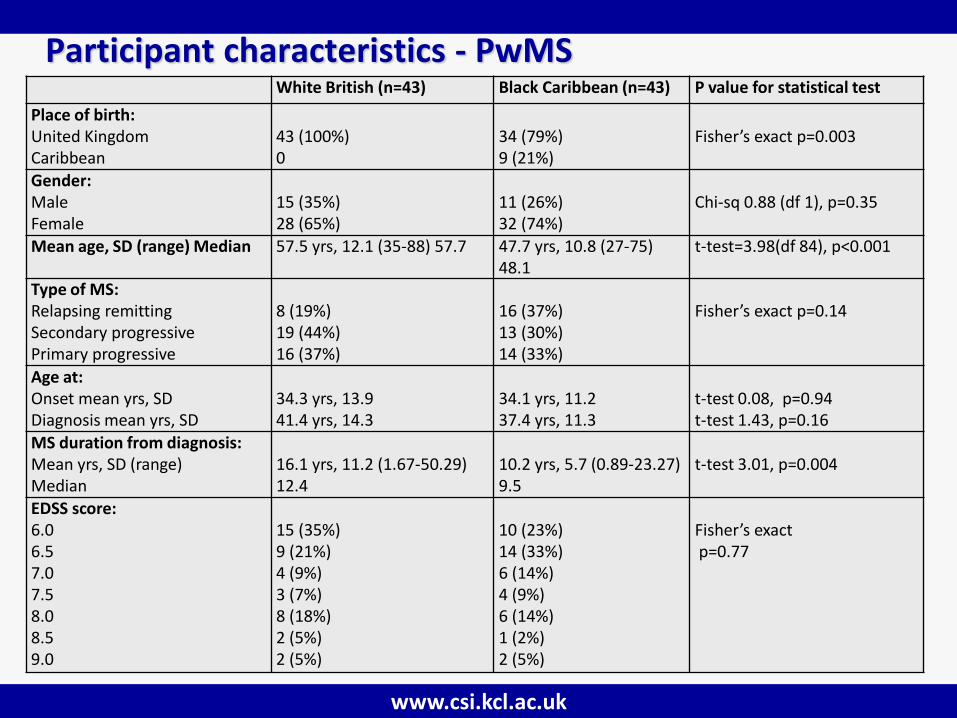
Participant characteristics - PwMS White British (n=43) Black Caribbean (n=43) P value for statistical test
Place of birth: United Kingdom Caribbean
43 (100%) 0
34 (79%) 9 (21%)
Fisher’s exact p=0.003
Gender: Male Female
15 (35%) 28 (65%)
11 (26%) 32 (74%)
Chi-sq 0.88 (df 1), p=0.35
Mean age, SD (range) Median 57.5 yrs, 12.1 (35-88) 57.7 47.7 yrs, 10.8 (27-75) 48.1
t-test=3.98(df 84), p<0.001
Type of MS: Relapsing remitting Secondary progressive Primary progressive
8 (19%) 19 (44%) 16 (37%)
16 (37%) 13 (30%) 14 (33%)
Fisher’s exact p=0.14
Age at: Onset mean yrs, SD Diagnosis mean yrs, SD
34.3 yrs, 13.9 41.4 yrs, 14.3
34.1 yrs, 11.2 37.4 yrs, 11.3
t-test 0.08, p=0.94 t-test 1.43, p=0.16
MS duration from diagnosis: Mean yrs, SD (range) Median
16.1 yrs, 11.2 (1.67-50.29) 12.4
10.2 yrs, 5.7 (0.89-23.27) 9.5
t-test 3.01, p=0.004
EDSS score: 6.0 6.5 7.0 7.5 8.0 8.5 9.0
15 (35%) 9 (21%) 4 (9%) 3 (7%) 8 (18%) 2 (5%) 2 (5%)
10 (23%) 14 (33%) 6 (14%) 4 (9%) 6 (14%) 1 (2%) 2 (5%)
Fisher’s exact p=0.77
www.csi.kcl.ac.uk
MS-related physical and psychological symptoms
•POS-S identified that BC and WB PwMS both reported mean of 9 symptoms (BC PwMS mean 8.6; SD: 3.4; range 2– 15 v/s WB PwMS mean 9.1; SD: 3.3; range: 2–16):.
• 14/18 symptoms reported in both groups as ‘severe’ / ‘overwhelming’ [Especially fatigue, pain and problems with ambulation]
www.csi.kcl.ac.uk
MS-related physical and psychological symptoms
•No differences between two groups using Multiple Sclerosis Impact Scale-29 (MSIS-29)
•BC PwMS reported mean of 22 areas associated with MS impact (range 7–29) compared to 23 areas among WB PwMS (range 10–29)
www.csi.kcl.ac.uk
MS-related physical and psychological symptoms
•Fatigue, measured by MFIS, and depression and anxiety measured by HADS similar between groups
•But…cognitive impairment measured by Blessed Orientation Memory Concentration Test (BOMCT) differed between groups – scores for BC PwMS more than 1.5X greater than WB counterparts (F=9.65, p=0.003)
www.csi.kcl.ac.uk
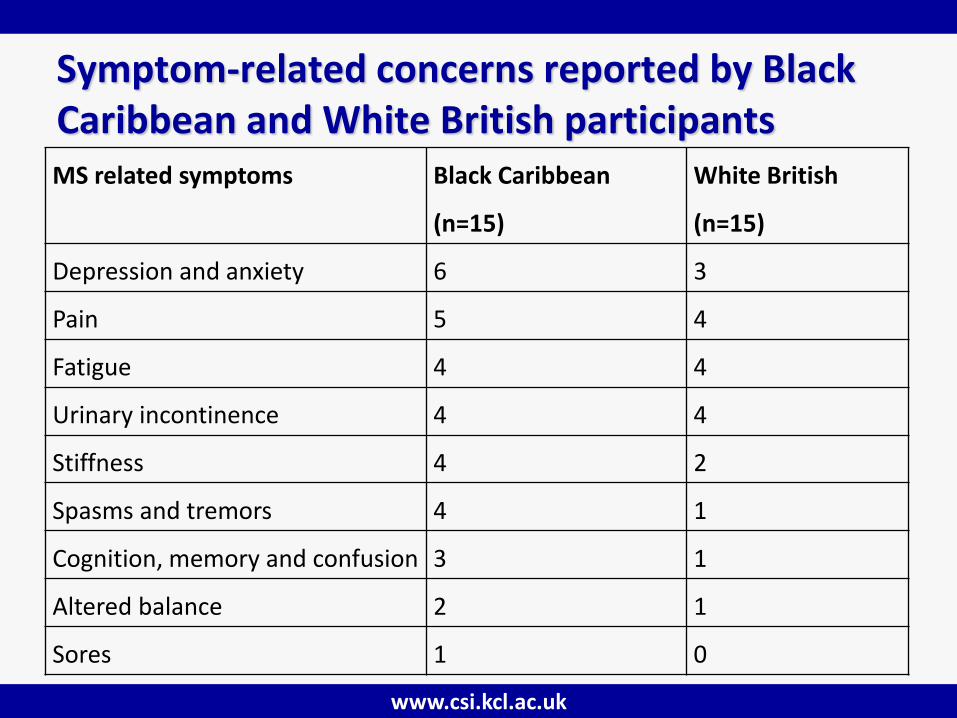
Symptom-related concerns reported by Black Caribbean and White British participants MS related symptoms Black Caribbean
(n=15)
White British
(n=15)
Depression and anxiety 6 3
Pain 5 4
Fatigue 4 4
Urinary incontinence 4 4
Stiffness 4 2
Spasms and tremors 4 1
Cognition, memory and confusion 3 1
Altered balance 2 1
Sores 1 0

www.csi.kcl.ac.uk
Unplugged, hollow and empty

www.csi.kcl.ac.uk
Unplugged, hollow and empty
www.csi.kcl.ac.uk
Scared of living

www.csi.kcl.ac.uk
Everything’s like a sieve

www.csi.kcl.ac.uk
MS disease progression
www.csi.kcl.ac.uk
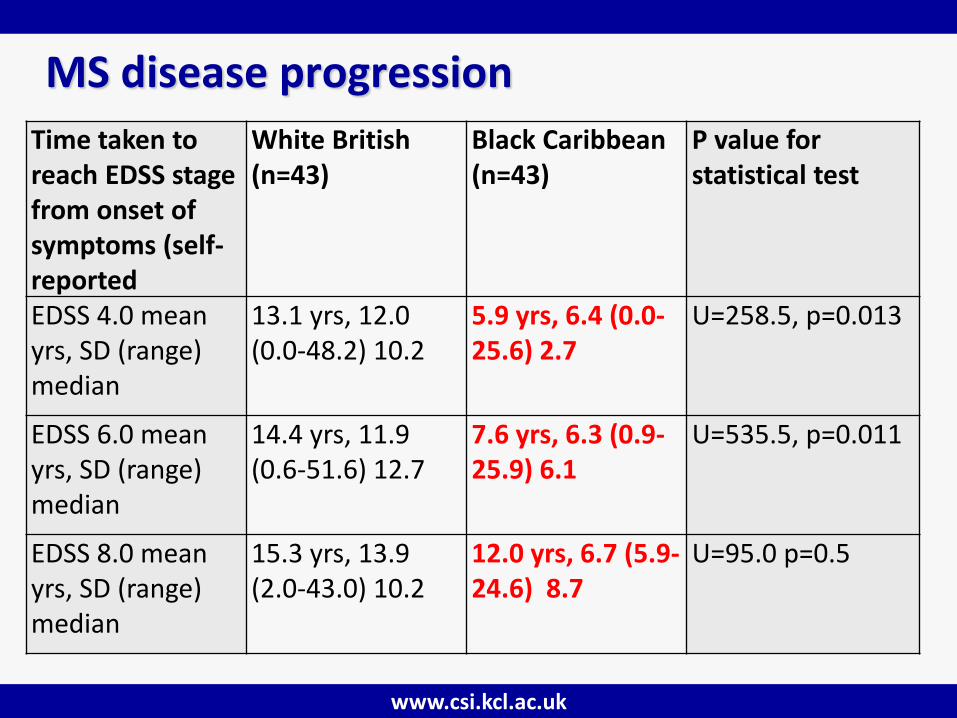
MS disease progression
Time taken to reach EDSS stage from onset of symptoms (self- reported
White British (n=43)
Black Caribbean (n=43)
P value for statistical test
EDSS 4.0 mean yrs, SD (range) median
13.1 yrs, 12.0 (0.0-48.2) 10.2
5.9 yrs, 6.4 (0.0-25.6) 2.7
U=258.5, p=0.013
EDSS 6.0 mean yrs, SD (range) median
14.4 yrs, 11.9 (0.6-51.6) 12.7
7.6 yrs, 6.3 (0.9-25.9) 6.1
U=535.5, p=0.011
EDSS 8.0 mean yrs, SD (range) median
15.3 yrs, 13.9 (2.0-43.0) 10.2
12.0 yrs, 6.7 (5.9-24.6) 8.7
U=95.0 p=0.5
www.csi.kcl.ac.uk
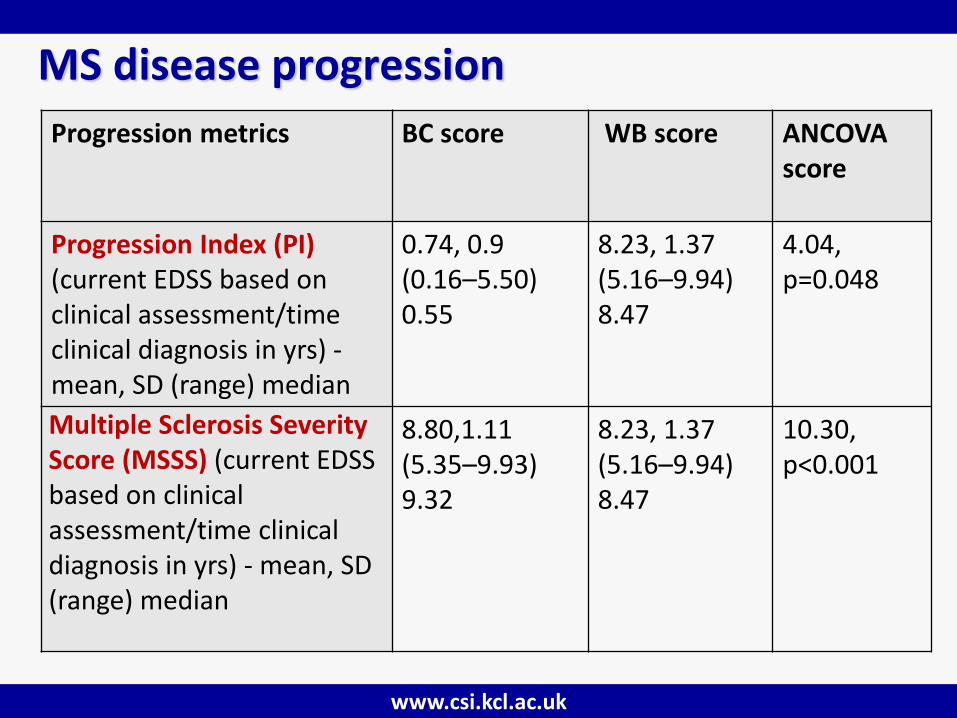
MS disease progression
Progression metrics BC score WB score ANCOVA score
Progression Index (PI) (current EDSS based on clinical assessment/time clinical diagnosis in yrs) - mean, SD (range) median
0.74, 0.9 (0.16–5.50) 0.55
8.23, 1.37 (5.16–9.94) 8.47
4.04, p=0.048
Multiple Sclerosis Severity Score (MSSS) (current EDSS based on clinical assessment/time clinical diagnosis in yrs) - mean, SD (range) median
8.80,1.11 (5.35–9.93) 9.32
8.23, 1.37 (5.16–9.94) 8.47
10.30, p<0.001
www.csi.kcl.ac.uk
MS disease progression
• It was, it was that quick. ...It was very scary…It’s just a lot of frustration you know, and it plays with your mind as well. It had a lot of psychological effect. Because I wasn’t always in a wheelchair and you know, people have commented on, you’re, you’re getting worse. You were on sticks to crutches, now to the wheelchair. And its playing on your mind and you’re thinking ‘‘Oh OK, maybe I am getting worse’’. I just thought, I’d have gone right down hill. (BC PwMS 79)
www.csi.kcl.ac.uk
MS disease progression
• I got sick so quickly. I lost the feeling down all the left side of my body ...and then I was OK. And then after about a year… my daughter being born I got sick again. But I got worse. I had to go back on, on the treatment. I couldn’t stay off the treatment. I wanted to breast feed her for as long as I could, but I couldn’t, I couldn’t do it. You’re upset and you’re, you’re hurting but you don’t want to explain it to other people or see other people, see that you’re hurting, you’re crying. I didn’t want that.
www.csi.kcl.ac.uk
Methodological reflections
•‘Racialised’ differences’ between research participant and interviewer
•PI can be skewed toward higher scores by short disease duration and toward lower scores by long disease durations
•Recall bias
•Cultural equivalence of measurement tools
•Study cross sectional
www.csi.kcl.ac.uk
Discussion of findings 1
• MS progression noted as being more aggressive among some ethnic groups (Ferreira Vasconcelos et al 2010, Kaufman 2003)
• MS appears to progress more quickly among BC than WB PwMS
• NO consensus method for measuring progression using single, cross-sectional assessments of disability Used PI, MSSS and patients’ recall of events
• Correspondence with qualitative findings
www.csi.kcl.ac.uk
Discussion of findings 2
•Higher levels of cognitive impairment among BC than WB PwMS
•Cognitive issues among African Americans severely affected by MS previously reported (Buchanan et al 2004)
•triangulation with qualitative findings
www.csi.kcl.ac.uk
Discussion of findings 3
•Observed high symptom prevalence and burden across both ethnic groups with participants experiencing average of 9 symptoms according to POS-S
•Most symptoms rated as severe or overwhelming
•Again considerable correspondence with qualitative findings
www.csi.kcl.ac.uk
Clinical implications
• Delays in diagnosis must be avoided
• More frequent reviews justified by healthcare services
• Interventions to support people who perceive MS as assault on identity should be developed to achieve ‘normalisation’ and enhance self-identity
•cognitive behavioural therapy may offer solutions
•role for palliative care

www.csi.kcl.ac.uk
Find out more about our research and education activities @ www.csi.kcl.ac.uk





























