Embed Size (px)
Citation preview
Articles
1066 www.thelancet.com Vol 367 April 1, 2006
IntroductionThe reduction of maternal deaths is a high priority for the international community, especially in view of the increased attention on the Millennium Development Goals.1 Maternal deaths arise from the risks attributable to pregnancy and childbirth as well as from the poor-quality care from health services.2 Eff ective services to improve overall maternal health need targeted health and social policies that are informed by reliable and valid epidemiological data. A comprehensive summary of the magnitude and distribution of the causes of maternal deaths is critical to inform reproductive health policies and programmes. The most widely referred source that is currently available3 dates back to the 1990s, although its methodology is not clear and it assumes a fi xed distribution across all regions. Regional variations are likely to exist, although their magnitude and direction are unknown. A more recent WHO Global Burden of Disease estimate gave a breakdown by cause and region but the methodology and the data sources for cause attribution and regional diff erences were not reported.4
Systematic reviews are increasingly used to summarise descriptive epidemiological evidence to provide summary estimates for the extent of important public-health problems.5,6 We undertook a systematic review that
aimed to estimate incidence and prevalence of a range of maternal conditions, including maternal mortality and its causes.7 The aim of this study was to ascertain and map the distribution of causes of maternal deaths, to identify data gaps in regional coverage, and to explore the extent to which countries’ development status, geographical location, and datasets’ methodological features explain variable distribution of causes of deaths.
MethodsOur systematic review followed an a-priori protocol developed with a widely recommended methodology7–9 to generate a comprehensive, standardised, and reliable evidence summary for conditions contributing to maternal deaths worldwide. This process included the breakdown of causes of maternal deaths and examination of heterogeneity of causes.
Dataset selection Participants included pregnant women or women within 1 year of the end of pregnancy who had maternal deaths. A maternal death is defi ned in the International Classifi cation of Diseases, 10th edition (ICD-10) as the death of a woman while pregnant or within 42 days (or
Lancet 2006; 367: 1066–74
Published Online March 28, 2006
DOI:10.1016/S0140-6736(06)
68397-9
UNDP/UNFPA/WHO/World Bank Special Programme of Research, Development and Research Training in Human
Reproduction, Department of Reproductive Health and
Research, WHO, Geneva 27, CH-1211, Switzerland
(L Say MD, A Metin Gülmezoglu MD,
P F A Van Look MD); Academic Department of Obstetrics and
Gynaecology, University of Birmingham, Birmingham, UK
(Prof K S Khan MRCOG); and Centro Rosarino de Estudios
Perinatales, Rosario, Argentina (D Wojdyla MSc)
Correspondence to: Dr A Metin Gülmezoglu
WHO analysis of causes of maternal death: a systematic review Khalid S Khan, Daniel Wojdyla, Lale Say, A Metin Gülmezoglu, Paul F A Van Look
SummaryBackground The reduction of maternal deaths is a key international development goal. Evidence-based health policies and programmes aiming to reduce maternal deaths need reliable and valid information. We undertook a systematic review to determine the distribution of causes of maternal deaths.
Methods We selected datasets using prespecifi ed criteria, and recorded dataset characteristics, methodological features, and causes of maternal deaths. All analyses were restricted to datasets representative of populations. We analysed joint causes of maternal deaths from datasets reporting at least four major causes (haemorrhage, hypertensive disorders, sepsis, abortion, obstructed labour, ectopic pregnancy, embolism). We examined datasets reporting individual causes of death to investigate the heterogeneity due to methodological features and geographical region and the contribution of haemorrhage, hypertensive disorders, abortion, and sepsis as causes of maternal death at the country level.
Findings 34 datasets (35 197 maternal deaths) were included in the primary analysis. We recorded wide regional variation in the causes of maternal deaths. Haemorrhage was the leading cause of death in Africa (point estimate 33·9%, range 13·3–43·6; eight datasets, 4508 deaths) and in Asia (30·8%, 5·9–48·5; 11, 16 089). In Latin America and the Caribbean, hypertensive disorders were responsible for the most deaths (25·7%, 7·9–52·4; ten, 11 777). Abortion deaths were the highest in Latin America and the Caribbean (12%), which can be as high as 30% of all deaths in some countries in this region. Deaths due to sepsis were higher in Africa (odds ratio 2·71), Asia (1·91), and Latin America and the Caribbean (2·06) than in developed countries.
Interpretation Haemorrhage and hypertensive disorders are major contributors to maternal deaths in developing countries. These data should inform evidence-based reproductive health-care policies and programmes at regional and national levels. Capacity-strengthening eff orts to improve the quality of burden-of-disease studies will further validate future estimates.
Articles
www.thelancet.com Vol 367 April 1, 2006 1067
1 year for late maternal deaths) of termination of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.10
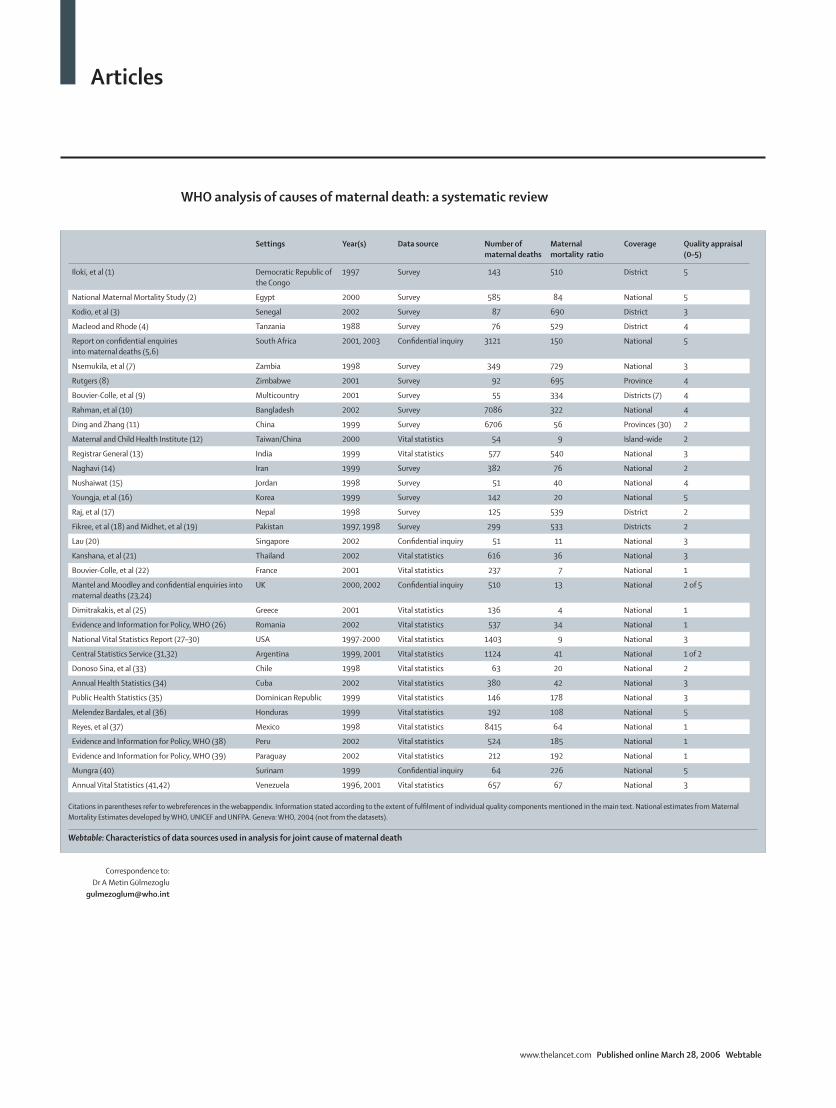
We used datasets providing counts or proportions attributed to specifi c conditions leading to maternal death, from direct counting or from special surveys. We use the term dataset because some sources are research studies but others are direct counts or other forms of routine data collection (such as vital registration; webtable). We included only datasets that represented the populations in the fi nal analysis. The population settings could be country, province, or city (or district).
Datasets were ineligible if data were taken before 1990, if part of the data was obtained before 1980 and disaggregation by year was not possible (in order to exclude data before 1980), or if data collection dates were not reported. In cases of partial data duplication with some data overlapping between diff erent datasets, we selected the most recent and largest dataset.
To allow more stable and reliable estimation of proportions attributed to the various causes of maternal deaths, we excluded datasets with less than 25 maternal deaths in the series. The decision for this cutoff was arbitrary. Specifi cally for the joint distribution of cause analysis, we further excluded datasets that did not have a cause attributed to more than 25% of deaths, or did not include at least four of the following direct causes of death: haemorrhage, hypertensive disorder, sepsis, abortion, obstructed labour, ectopic pregnancy, and embolism.
Identifi cation of data sourcesWe searched general and specialised bibliographic databases: MEDLINE, Popline, CAB, Sociofi le, CINAHL, Econlit, EMBASE, BIOSIS, PAIS International, the Latin American and Caribbean Health Science Information (LILACS), African Index Medicus (AIM), Index Medicus for the Eastern Mediterranean Region (IMEMR), Index Medicus for the South-East Asian Region (IMSEAR), websites of ministries of health in all 192 WHO member states, and WHO Reproductive Health databases from 1997 to 2002, a time limit chosen to allow a review of recent data on causes of maternal deaths. Reference lists of the identifi ed reports were screened and personal contacts were made with country representatives of WHO, non-governmental organisations (NGOs), and other organisations known to be active in the maternal-health fi eld to fi nd datasets not captured by bibliographic searches. Our search term combinations are described in detail elsewhere.7 We did not apply language restrictions in the search or in the selection process. Potentially eligible datasets included journal articles, registries, and published or unpublished information from government or other agencies, whether available in print or online.
Methodological quality assessmentThe methodological quality of all eligible datasets was assessed to investigate internal validity (the extent to which the information is probably free of bias) with the following attributes:8 (1) reporting of maternal deaths defi nition to reduce bias in ascertainment of denominator data in the series (any published defi nition reported vs no defi nition); (2) adequacy of data source to ascertain a capture of denominator data that is as complete as possible (use of multiple data sources, special surveys, or clinical studies vs routine registration systems, in which adequate attribution of cause of death has been shown to be questionable for maternal deaths, leading to substantial underreporting);11 (3) use of a robust approach to ascertain that the cause of death is a representation of the underlying condition that is as true as possible (confi dential enquiries, verbal autopsies, use of multiple
See Online for webtable
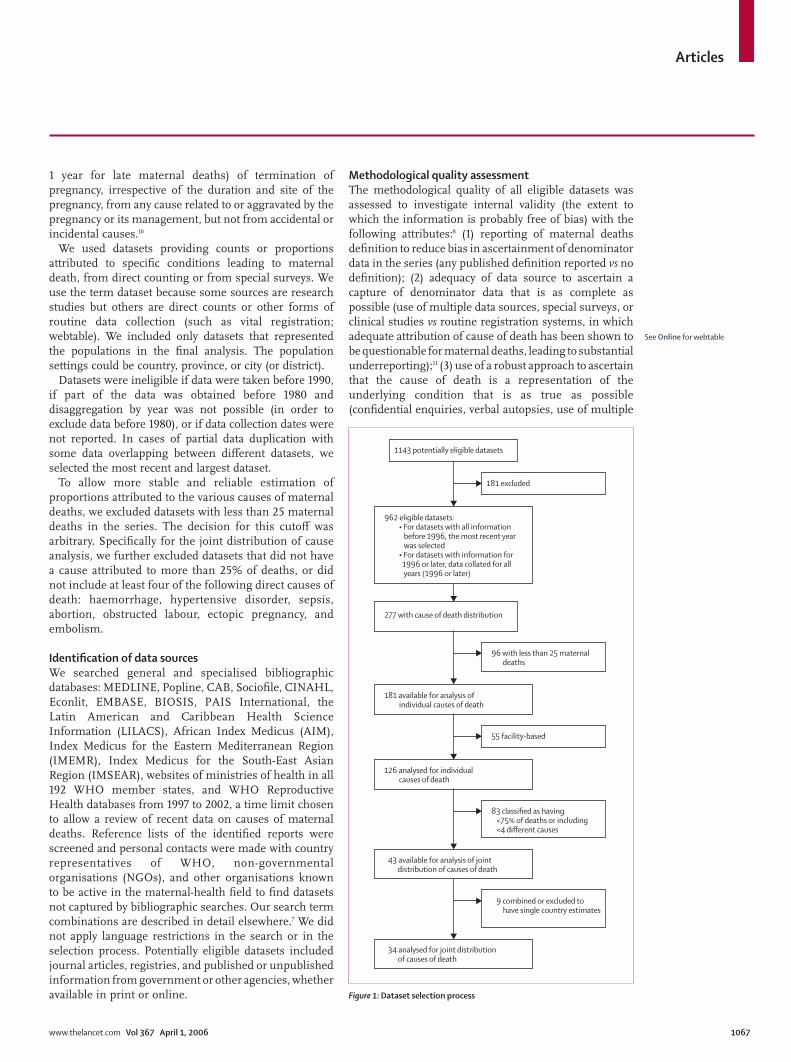
1143 potentially eligible datasets
181 excluded
277 with cause of death distribution
96 with less than 25 maternal deaths
181 available for analysis of individual causes of death
55 facility-based
126 analysed for individual causes of death
83 classified as having <75% of deaths or including <4 different causes
9 combined or excluded to have single country estimates
43 available for analysis of joint distribution of causes of death
34 analysed for joint distribution of causes of death
962 eligible datasets: • For datasets with all information before 1996, the most recent year was selected • For datasets with information for 1996 or later, data collated for all years (1996 or later)
Figure 1: Dataset selection process
Articles
1068 www.thelancet.com Vol 367 April 1, 2006
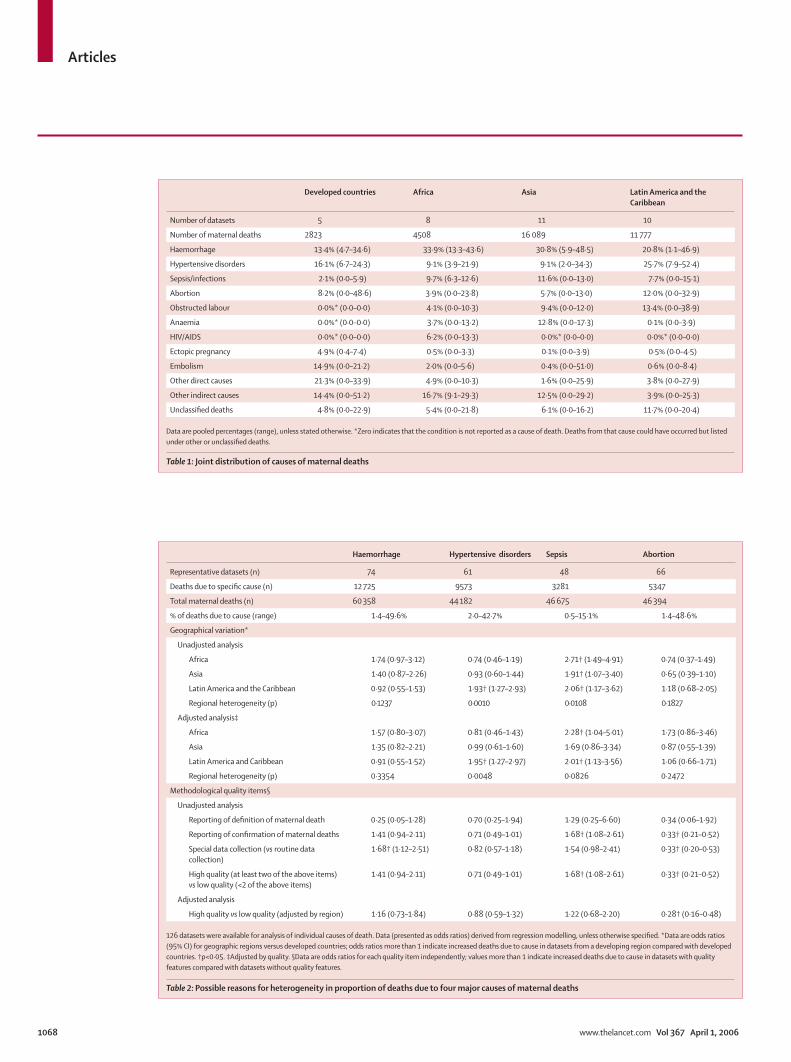
Developed countries Africa Asia Latin America and the Caribbean
Number of datasets 5 8 11 10
Number of maternal deaths 2823 4508 16 089 11 777
Haemorrhage 13·4% (4·7–34·6) 33·9% (13·3–43·6) 30·8% (5·9–48·5) 20·8% (1·1–46·9)
Hypertensive disorders 16·1% (6·7–24·3) 9·1% (3·9–21·9) 9·1% (2·0–34·3) 25·7% (7·9–52·4)
Sepsis/infections 2·1% (0·0–5·9) 9·7% (6·3–12·6) 11·6% (0·0–13·0) 7·7% (0·0–15·1)
Abortion 8·2% (0·0–48·6) 3·9% (0·0–23·8) 5·7% (0·0–13·0) 12·0% (0·0–32·9)
Obstructed labour 0·0%* (0·0–0·0) 4·1% (0·0–10·3) 9·4% (0·0–12·0) 13·4% (0·0–38·9)
Anaemia 0·0%* (0·0–0·0) 3·7% (0·0–13·2) 12·8% (0·0–17·3) 0·1% (0·0–3·9)
HIV/AIDS 0·0%* (0·0–0·0) 6·2% (0·0–13·3) 0·0%* (0·0–0·0) 0·0%* (0·0–0·0)
Ectopic pregnancy 4·9% (0·4–7·4) 0·5% (0·0–3·3) 0·1% (0·0–3·9) 0·5% (0·0–4·5)
Embolism 14·9% (0·0–21·2) 2·0% (0·0–5·6) 0·4% (0·0–51·0) 0·6% (0·0–8·4)
Other direct causes 21·3% (0·0–33·9) 4·9% (0·0–10·3) 1·6% (0·0–25·9) 3·8% (0·0–27·9)
Other indirect causes 14·4% (0·0–51·2) 16·7% (9·1–29·3) 12·5% (0·0–29·2) 3·9% (0·0–25·3)
Unclassifi ed deaths 4·8% (0·0–22·9) 5·4% (0·0–21·8) 6·1% (0·0–16·2) 11·7% (0·0–20·4)
Data are pooled percentages (range), unless stated otherwise. *Zero indicates that the condition is not reported as a cause of death. Deaths from that cause could have occurred but listed under other or unclassifi ed deaths.
Table 1: Joint distribution of causes of maternal deaths
Haemorrhage Hypertensive disorders Sepsis Abortion
Representative datasets (n) 74 61 48 66
Deaths due to specifi c cause (n) 12 725 9573 3281 5347
Total maternal deaths (n) 60 358 44 182 46 675 46 394
% of deaths due to cause (range) 1·4–49·6% 2·0–42·7% 0·5–15·1% 1·4–48·6%
Geographical variation*
Unadjusted analysis
Africa 1·74 (0·97–3·12) 0·74 (0·46–1·19) 2·71† (1·49–4·91) 0·74 (0·37–1·49)
Asia 1·40 (0·87–2·26) 0·93 (0·60–1·44) 1·91† (1·07–3·40) 0·65 (0·39–1·10)
Latin America and the Caribbean 0·92 (0·55–1·53) 1·93† (1·27–2·93) 2·06† (1·17–3·62) 1·18 (0·68–2·05)
Regional heterogeneity (p) 0·1237 0·0010 0·0108 0·1827
Adjusted analysis‡
Africa 1·57 (0·80–3·07) 0·81 (0·46–1·43) 2·28† (1·04–5·01) 1·73 (0·86–3·46)
Asia 1·35 (0·82–2·21) 0·99 (0·61–1·60) 1·69 (0·86–3·34) 0·87 (0·55–1·39)
Latin America and Caribbean 0·91 (0·55–1·52) 1·95† (1·27–2·97) 2·01† (1·13–3·56) 1·06 (0·66–1·71)
Regional heterogeneity (p) 0·3354 0·0048 0·0826 0·2472
Methodological quality items§
Unadjusted analysis
Reporting of defi nition of maternal death 0·25 (0·05–1·28) 0·70 (0·25–1·94) 1·29 (0·25–6·60) 0·34 (0·06–1·92)
Reporting of confi rmation of maternal deaths 1·41 (0·94–2·11) 0·71 (0·49–1·01) 1·68† (1·08–2·61) 0·33† (0·21–0·52)
Special data collection (vs routine data collection)
1·68† (1·12–2·51) 0·82 (0·57–1·18) 1·54 (0·98–2·41) 0·33† (0·20–0·53)
High quality (at least two of the above items) vs low quality (<2 of the above items)
1·41 (0·94–2·11) 0·71 (0·49–1·01) 1·68† (1·08–2·61) 0·33† (0·21–0·52)
Adjusted analysis
High quality vs low quality (adjusted by region) 1·16 (0·73–1·84) 0·88 (0·59–1·32) 1·22 (0·68–2·20) 0·28† (0·16–0·48)
126 datasets were available for analysis of individual causes of death. Data (presented as odds ratios) derived from regression modelling, unless otherwise specifi ed. *Data are odds ratios (95% CI) for geographic regions versus developed countries; odds ratios more than 1 indicate increased deaths due to cause in datasets from a developing region compared with developed countries. †p<0·05. ‡Adjusted by quality. §Data are odds ratios for each quality item independently; values more than 1 indicate increased deaths due to cause in datasets with quality features compared with datasets without quality features.
Table 2: Possible reasons for heterogeneity in proportion of deaths due to four major causes of maternal deaths
Articles
www.thelancet.com Vol 367 April 1, 2006 1069
sources of death certifi cation vs no special eff orts to confi rm cause); (4) suffi ciently high proportion of cases with attributable cause of death established (<5% unclassifi ed); and (5) identifi cation of suffi ciently large number of causes within a series to ensure that a fuller range of conditions have been included to reduce the risk of misclassifi cation of cause of death (>5 causes was taken as a cutoff ).
(4) and (5) are good-quality items relevant mainly to the joint cause of death analysis. For example, in a report that analysed deaths due to abortion only, a large proportion of deaths could be unclassifi ed, but the report could still present a detailed and good-quality dataset for a specifi c cause if it complied with the quality items (1), (2), and (3). For this reason, in the appraisal of individual causes of death datasets, we only took three quality items into account. The datasets were classifi ed into high-quality and low-quality groups, on the basis of compliance with at least two quality criteria.
Data extractionTwo reviewers independently assessed titles or abstracts from a randomly selected sample of citations identifi ed by the electronic search that achieved 88·9% (95% CI 86·0–91·4) agreement (κ 0·60, 95% CI 0·52–0·69), a value corresponding to moderate to substantial concordance.12 If one reviewer was unsure, the full text of the report was retrieved. In case of disagreement about the application of the selection criteria, the case was discussed with reference to the protocol criteria and, if needed, the full paper was retrieved. We extracted dataset characteristics, methodological quality information, and proportions of various causes among all maternal deaths.
Statistical analysisWe analysed two groups of population-based representative datasets: the joint cause of death distribution and the individual cause dataset. For the joint cause of death analysis, countries with several datasets for diff erent times were combined to produce a nationally representative estimate per country. If estimates were from the same period because of overlapping settings, national data took precedence over data from provinces, states, or cities.
We obtained causes of death distribution within each geographical region by combining the estimates for all the countries within each region. For this purpose, the number of maternal deaths in countries with causes of death distribution was estimated and used to derive weights to be applied to the distribution of causes within each region. The number of maternal deaths were estimated with the maternal mortality ratio and the number of livebirths per country.13 The weights were based on the number of maternal deaths because this apportions importance according to the disease burden contributed by each country. The traditional approach to
Unclassified deaths <5%†
Causes reported >5†
48
26
25
47
48 133Confirmation of cause of death 31 42
42 139Adequate data source 29 44
Datasets for analysis ofdistribution of individualcauses of deaths (n=181)
133
126
48
55
0% 50% 100%
Definition of maternal mortality
Representative(population-based)
Datasets for analysis ofjoint distribution ofcauses of deaths (n=73)*
55
43
18
30
0% 50%
100%
40
25
29
18
24
31
3
18
14
25
19
12
Unclassified deaths <5%†
Causes reported >5†
Confirmation of cause of death
Adequate data source
Definition of maternal mortality
High quality* (>3 of 5 items)
All datasets
Representative datasets
0% 50%
112
37
36
14
89
90
Adequate/yesInadequate/no/unreported
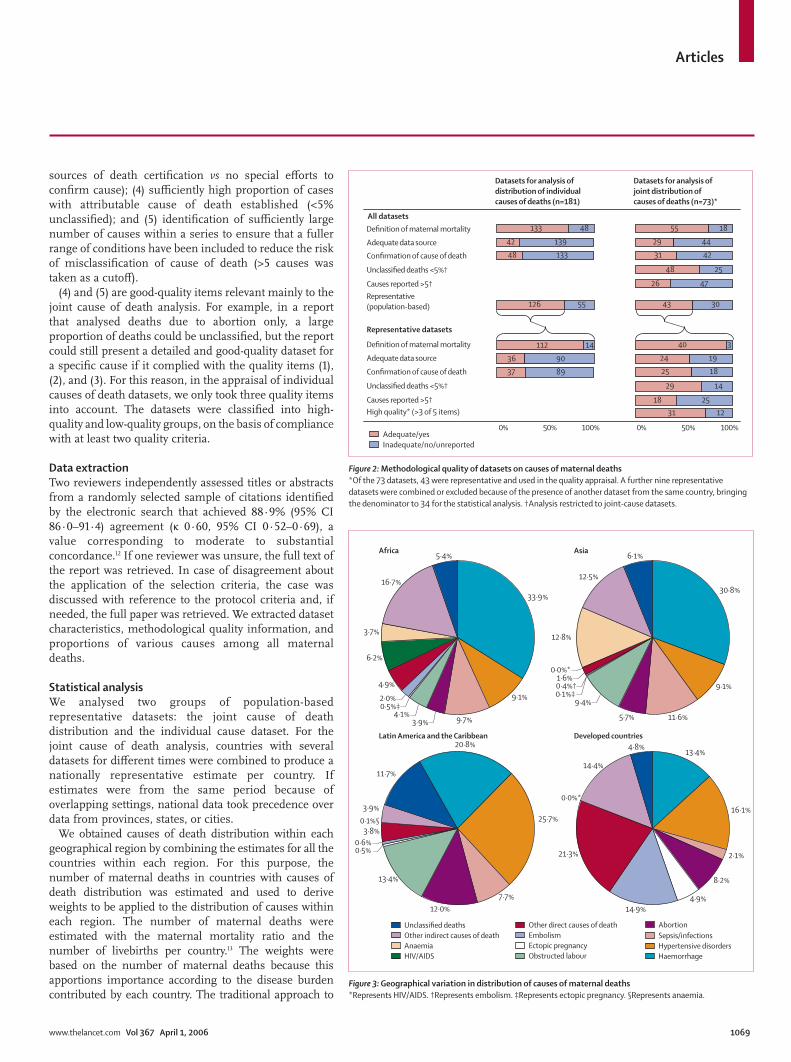
Figure 2: Methodological quality of datasets on causes of maternal deaths*Of the 73 datasets, 43 were representative and used in the quality appraisal. A further nine representative datasets were combined or excluded because of the presence of another dataset from the same country, bringing the denominator to 34 for the statistical analysis. †Analysis restricted to joint-cause datasets.
Unclassified deathsOther indirect causes of deathAnaemiaHIV/AIDS
Other direct causes of deathEmbolismEctopic pregnancyObstructed labour
AbortionSepsis/infectionsHypertensive disordersHaemorrhage
Africa Asia
Latin America and the Caribbean Developed countries
33·9%
9·1%
9·7%3·9%4·1%
0·5%‡2·0%
4·9%
6·2%
3·7%
16·7%
5·4%
30·8%
9·1%
11·6%5·7%
9·4%0·1%‡0·4%†1·6%
0·0%*
12·8%
12·5%
6·1%
20·8%
25·7%
7·7%12·0%
13·4%
0·5%0·6%
3·8%0·1%§3·9%
11·7%
13·4%
16·1%
2·1%
8·2%
4·9%14·9%
21·3%
0·0%*
14·4%
4·8%
Figure 3: Geographical variation in distribution of causes of maternal deaths*Represents HIV/AIDS. †Represents embolism. ‡Represents ectopic pregnancy. §Represents anaemia.
Articles
1070 www.thelancet.com Vol 367 April 1, 2006
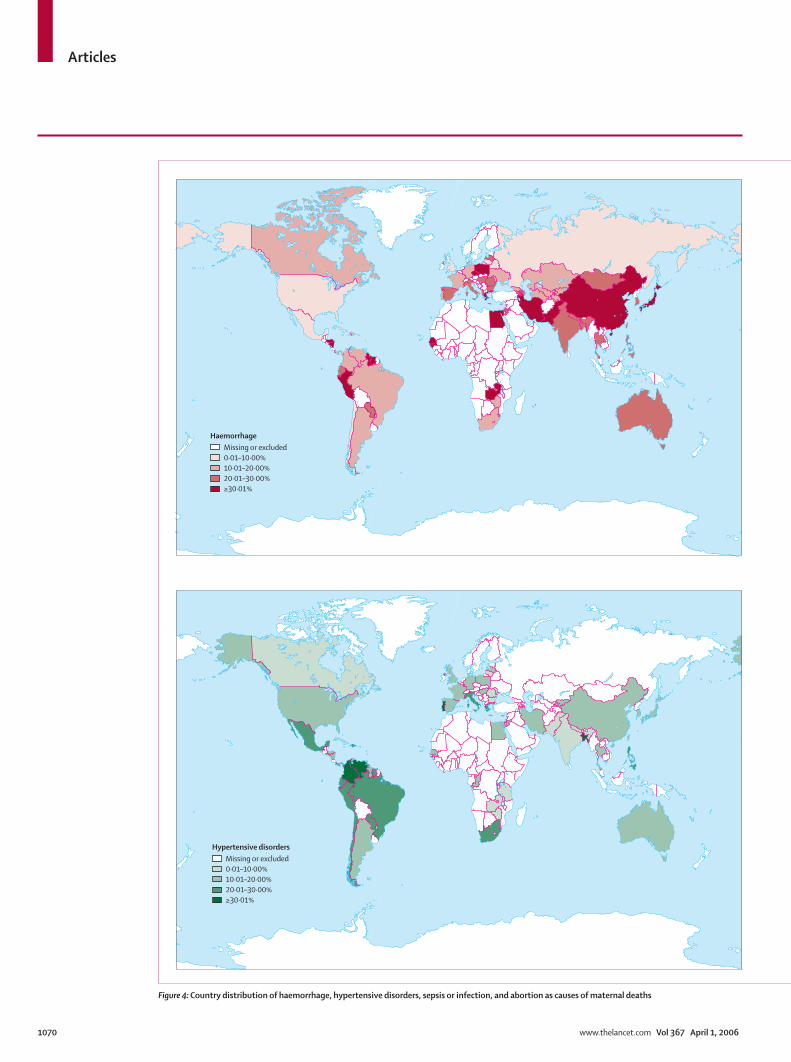
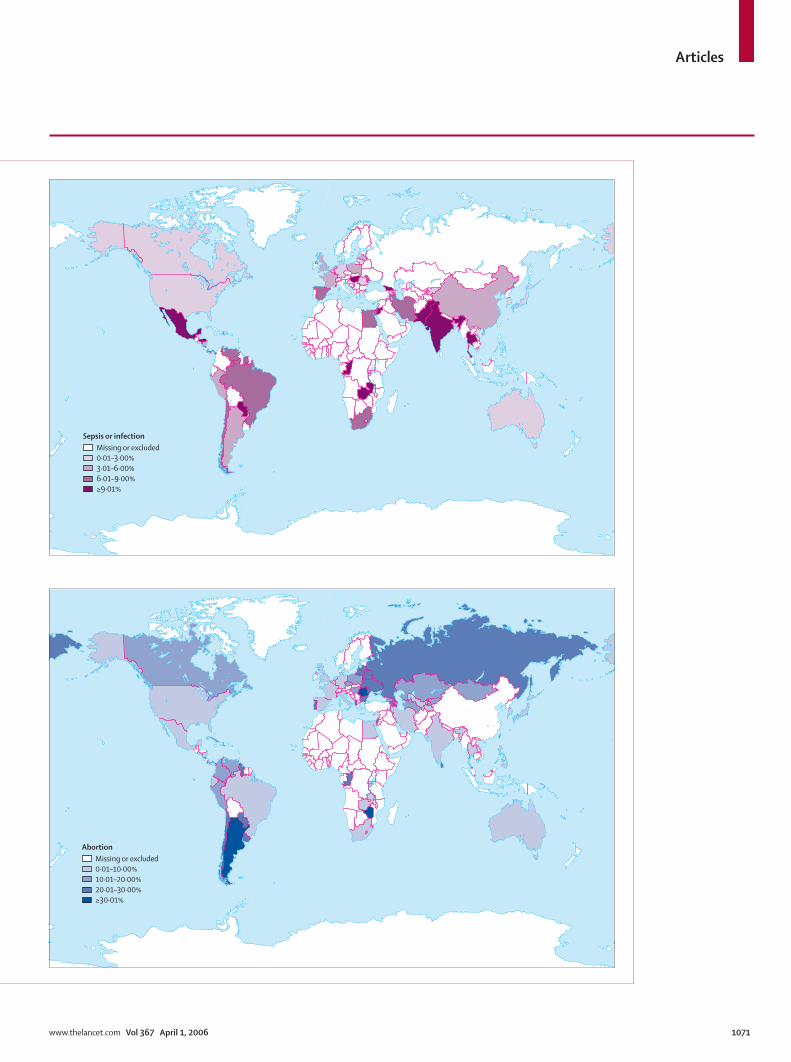
Figure 4: Country distribution of haemorrhage, hypertensive disorders, sepsis or infection, and abortion as causes of maternal deaths
Missing or excluded0·01–10·00%10·01–20·00%20·01–30·00%≥30·01%
Haemorrhage
Missing or excluded0·01–10·00%10·01–20·00%20·01–30·00%≥30·01%
Hypertensive disorders
Articles
www.thelancet.com Vol 367 April 1, 2006 1071
Missing or excluded0·01–3·00%3·01–6·00%6·01–9·00%≥9·01%
Sepsis or infection
Missing or excluded0·01–10·00%10·01–20·00%20·01–30·00%≥30·01%
Abortion

Articles
1072 www.thelancet.com Vol 367 April 1, 2006
weighting based on sample size or inverse variance has the disadvantage that it could apportion more importance to larger studies of causes of death distributions from smaller countries that make a small contribution to the overall disease burden.
We estimated the coverage of data for regions by calculating the proportion of estimated number of maternal deaths in areas for which cause distribution was analysed to total number of maternal deaths per year for each region. For geographical classifi cation and development status, we used the UN classifi cation system. Developing countries were grouped according to their geographical regions as Africa, Asia, and Latin America and the Caribbean. Developed countries from all regions were combined into a separate group, which included European countries, North America, Australia, New Zealand, and Japan.
For the individual cause of death analysis, the point estimates of proportions and their 95% CIs were represented in forest plots to explore heterogeneity and the possibility of the diff erences being due to chance were assessed statistically by Cochran Q test. To explore the presence of heterogeneity and its causes, regression models were adjusted to the proportions attributed to every individual cause of death.14 The proportions were previously transformed with the logit transformation.15 Explanatory variables considered in these models were: geographical region (which correlated with country development status) and dataset methodological quality items. The eff ect of methodological quality was assessed separately for individual items and for a summary score comparing high-quality with low-quality datasets. After univariate analysis, we did multivariable analysis to assess the unique eff ects of regional variation and methodological quality, adjusting for any interdependence between the two factors.
Role of the funding sourceThe sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had fi nal responsibility for the decision to submit for publication.
ResultsThe search strategy yielded 64 585 citations for all defi ned maternal morbidity conditions and maternal mortality, of which 4606 were assessed in full-text form. Of these, 2581 reporting on a range of morbidities or mortality were included in the systematic review. 305 datasets provided information on causes of maternal deaths for 1 or more years or geographical locations (or both), with 1143 datasets (for a particular time or location) potentially eligible for this analysis. Figure 1 shows the detailed processing of these 1143 datasets for fi nal inclusion in the analysis. The joint cause of death analysis was based on 34 population-based datasets representative for the
populations concerned (table 1). The countries from which data were analysed contributed 21·9% of estimated deaths per year in Africa, 78·1% in Asia, 31·5% in Latin America and the Caribbean, and 41·1% in developed countries. The webtable and webappendix provide further details of the 34 datasets.
The individual cause of death analysis was based on 126 population-based representative datasets, which were used for analysis of haemorrhage, hypertensive disorders, sepsis, and abortion complications (table 2). Quality assessment revealed defi ciencies in many areas of methodology (fi gure 2). Joint cause of death datasets tended to have higher rates of causes confi rmed and more use of adequate data sources than datasets included in the analysis for individual causes. Of the 43 representative datasets for the joint cause of death analysis that were critically appraised, 31 (72%) met 3 of 5 criteria for quality assessment.
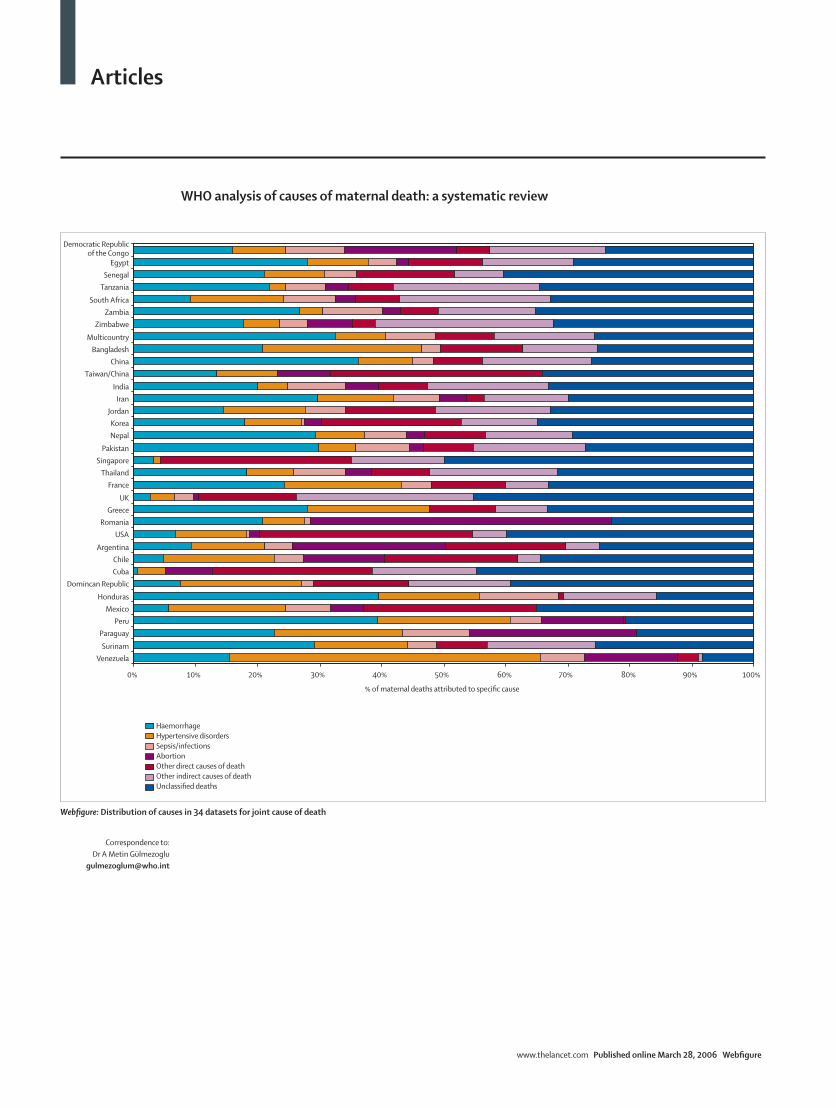
In our analysis of joint causes of death, haemorrhage was the leading cause of maternal death in Africa and Asia (>30% of deaths; table 1, fi gure 3). Hypertensive disorders represent the highest cause of death in Latin America and the Caribbean. There was also wide variation within regions (webfi gure). Other important regional diff erences included HIV/AIDS causing about 6% of deaths in Africa, and anaemia and obstructed labour each causing about a tenth of deaths in Asia. Abortion-related mortality was highest in Latin America and the Caribbean. Ectopic pregnancy was recorded as the cause in less than 1% of deaths in developing countries and almost 5% in developed countries.
As with the joint cause of death datasets, the individual cause of death datasets often had wide variability. However, these datasets allowed us to examine the distribution of four major causes in more detail (table 2). We investigated the variations in the percentages of the four major causes of deaths according to development status and methodological quality in individual cause of death datasets. Deaths due to hypertensive disorders and sepsis varied by development status. Compared with developed countries (reference group), sepsis was signifi cantly more frequent in Africa, Asia, and Latin America and the Caribbean (table 2).
Methodological quality tended to produce variation in diff erent directions for diff erent individual causes of deaths. Compared with datasets with poor-quality features, high-quality datasets had a reduced percentage of deaths due to abortion, whereas they had an increased percentage of deaths due to haemorrhage and sepsis. Figure 4 shows the regional variation of haemorrhage, hypertensive disorders, sepsis or infections, and abortion, according to countries. Abortion-related deaths can exceed 30% in parts of Latin America and eastern Europe. We compared the contributions of the most common causes of maternal deaths reported in individual-cause datasets and joint-cause datasets and found these two data sources to be compatible (data not shown).
See Online for webappendixand webfi gure

Articles
www.thelancet.com Vol 367 April 1, 2006 1073
DiscussionAs expected, our systematic analysis of the causes of maternal deaths, showed variation both across and within geographical regions. Our fi ndings confi rm the prominent role of haemorrhage as a cause of maternal death in developing countries. Hypertensive disorders are among the leading causes of deaths in Latin America and the Caribbean. In developed countries, most deaths are due to other direct causes, mainly complications of anaesthesia and caesarean sections. The contributions of sepsis and HIV in Africa, anaemia in Asia, abortion in Latin America and the Caribbean, and other direct causes (related to caesarean section and anaesthesia) and embolism in developed countries seem to be more region-specifi c.
Deaths due to abortion are high in Latin America and the Caribbean and some eastern European countries (fi gure 4). We can only speculate on possible reasons for the variation in abortion rates. The reasons for the relatively high contribution of abortion in Latin America could be because of fewer deaths due to other causes or restrictive abortion laws, compared with the other world regions. Abortion deaths are likely to be biased downwards by under-reporting and misclassifi cation (as haemorrhage or sepsis). It is probably safe to assume that abortion deaths are most likely due to unsafe abortion. Abortion rates also seemed to be aff ected by methodological quality, because good-quality studies showed reduced rates, suggesting possible reporting bias in studies of low quality.
We believe this review has several strengths. Our search strategy was extensive, comprehensive, and reproducible, as required by systematic reviews of published work. We identifi ed a large number of national reports and special surveys that might not have been accessible otherwise. We did a rigorous and transparent methodological quality assessment, and attempted to keep the risk of bias due to methodological weakness to a minimum by applying strict inclusion and exclusion criteria. We excluded datasets that were not representative of an administrative region (city or province or nation) from both analyses for individual and joint cause of death. This distinction is important because it is very diffi cult (if not impossible) to use facility-based data and adjust the results accordingly. The inclusion of facility-based datasets would have introduced potentially biased information and would have limited the generalisability of the whole analysis. Moreover, our approach of restriction to representative datasets limited the analysis for cause of death distribution to a subset of higher quality (fi gure 2), which adds to the internal validity of our inferences. Finally, we present the joint cause of death datasets (webfi gure) with their descriptive details, quality assessments,9 and corresponding maternal mortality ratios (webtable), which made our approach as explicit as possible.
The results and conclusions of a systematic review can only be as robust as the data provided by the primary datasets. Confi rmation of the cause of death is important for maternal mortality reports. However, only 37 of 126 datasets in the analysis for individual causes of death reported this confi rmation. The joint cause of death datasets did better in this respect (25 of 43). Although the restrictions we imposed for the number of causes reported (>5) and unclassifi ed (<5%) are arbitrary, we believe that they provide a fairly strict assessment.
The second limitation is the modest coverage of deaths within the regions, especially in Africa. Nevertheless, the eight datasets represent countries in north Africa (Egypt), west Africa (Senegal, another dataset covering seven countries), and east and south sub-Saharan Africa (Democratic Republic of Congo, South Africa, Tanzania, Zambia, Zimbabwe). This restricted coverage is partly because countries without a joint cause of death distribution were not included in the computation of the summary distribution for every region. This approach limits the power of our analysis, but also reduces the possibility of bias being introduced in the distributions of causes. Heterogeneity existed within and across regions. Logistic regression (table 2) showed that inadequacy of methods accounted for variation in rates of deaths due to haemorrhage, sepsis, and abortion.
We used UN defi nitions for the regions, which are commonly used in the classifi cation of regions. Further subregional breakdown was not possible because of the restricted number of datasets. The regional estimates are useful as broad indicators of causes of deaths, but national and subnational data are also important to identify diff erentials due to emerging causes and other local characteristics, such as access to services. A specifi c example is the proportion of HIV/AIDS-related maternal deaths in Africa (fi gure 3). The 1998 South African Confi dential Enquiries into Maternal Deaths identifi ed HIV/AIDS as the cause in 14·5% of deaths. However, in three-quarters of all maternal deaths, the HIV/AIDS status was unknown, suggesting that had this information been available the contribution of HIV/AIDS might have been higher than had been reported.16
We followed most of the quality criteria for reviews of observational datasets.9 Despite the fact that the procedural guidelines we used were not necessarily developed for prevalence or incidence reviews, they do provide a framework for high-quality systematic reviews.
Our systematic review provides an up-to-date, critically appraised, and reproducible analysis of causes of maternal deaths. The commonly cited report3 undertaken previously on cause distribution attributed 25% of maternal deaths to haemorrhage, 20% to indirect causes, 15% to infection, 13% to abortions, 12% to eclampsia, 8% to obstructed labour, and 8% to other direct causes globally.3 Our estimates agree that haemorrhage continues to be a major killer in Asia and Africa, and

Articles
1074 www.thelancet.com Vol 367 April 1, 2006
they also highlight causes that have not been examined systematically before.
This systematic review highlights the need for increased emphasis on programmes relevant to specifi c settings such as the prevention and treatment of haemorrhage both prepartum and postpartum. At the very least, most postpartum haemorrhage deaths should be avoidable by appropriate diagnosis and management. Hypertensive disorders and sepsis continue to be a concern. Increased availability and use of magnesium sulphate should be a goal in all regions, especially in Latin America and the Caribbean. The regional variation in abortion-related deaths is a call for increased attention to access in those areas to services that can help women avoid unwanted births.
The absence of epidemiological information in many low-income countries should lead to eff orts to increase capacity for data collection and reporting for vital statistics in those countries.17 Methodological studies are needed to improve our understanding of data synthesis in incidence and prevalence studies. Capacity-strengthening eff orts to improve the quality of recording, reporting, and geographical coverage of burden-of-disease studies will increase the robustness of future estimates. This systematic review should be updated at regular intervals to record changes in the profi le of causes of maternal deaths.ContributorsA M Gülmezoglu and L Say planned the study design and did the systematic review. K S Khan, D Wojdyla, L Say, and A M Gülmezoglu planned the analysis. D Wojdyla maintained the database and did the analysis. A M Gülmezoglu and K S Khan coordinated the analysis and writing of the manuscript. P F A Van Look reviewed and provided input into the manuscript. All authors contributed intellectually to the work.
Confl ict of interest statementWe declare that we have no confl ict of interest.
AcknowledgmentsThe opinions expressed in this paper are those of the authors only. UNDP/UNFPA/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction, Department of Reproductive Health and Research, WHO, funded the study. We thank Ana Pilar Betran, Felipe Santana and Genc Kabili, for their participation in this study. The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city, or area, or of its boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
References1 United Nations General Assembly. United Nations Millennium
Declaration. A/RES/55/2. 1-9-2000. UN General Assembly, 55th session, agenda item 60(b).
2 Freedman LP, Waldman RJ, de Pinho H, Wirth ME, Chowdhury AMR, Rosenfi eld A. Transforming health systems to improve the lives of women and children. Lancet 2005; 365: 997–1000.
3 WHO. AbouZahr C, Royston E. Maternal mortality: a global factbook. WHO/MCH/MSM/91.3. Geneva: World Health Organization, 1991.
4 WHO. Revised Global Burden of Disease 2002 Estimates. http://www.who.int/healthinfo/bodgbd2002revised/en/index.html (accessed Jan 13, 2006).
5 Dickersin K. Systematic reviews in epidemiology: why are we so far behind? Int J Epidemiol 2002; 31: 6–12.
6 Rudan I, Lawn J, Cousens S, et al. Gaps in policy-relevant information on burden of disease in children: a systematic review. Lancet 2005; 365: 2031–40.
7 Gülmezoglu AM, Say L, Betran AP, Villar J, Piaggio G. WHO systematic review of maternal mortality and morbidity: methodological issues and challenges. BMC Med Res Methodol 2004; 4: 16.
8 Glasziou P, Irwig L, Bain C, Colditz G. Frequency and rate. In: Systematic reviews in health care: a practical guide, 2nd edn. Cambridge, UK: Cambridge University Press, 2001: 67–73.
9 Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D. Meta-analysis of observational studies in epidemiology. A proposal for reporting. JAMA 2000; 283: 2008–12.
10 WHO. International Classifi cation of Diseases and Related Health Problems, 10th revision. Geneva: World Health Organization, 1992.
11 Smith JC, Hughes JM, Pekow PS, Rochat RW. An assessment of the incidence of maternal mortality in the United States. Am J Public Health 1984; 74: 780–83.
12 Landis JR, Koch GC. The measurement of observer agreement for categorical data. Biometrics 1977; 33: 159–74.
13 Betran AP, Wojdyla D, Posner S, Gülmezoglu AM. Maternal mortality at country level: an analysis based on the WHO systematic review. BMC Public Health 2005; 5: 131.
14 Sterne JA, Egger M, Smith GD. Systematic reviews in health care: investigating and dealing with publication and other biases in meta-analysis. BMJ 2001; 323: 101–05.
15 Allison PD. Logistic regression using the SAS system: theory and application. Cary, NC: SAS Institute, 1999.
16 Pattinson RC, ed. Saving mothers: report on confi dential enquiries into maternal deaths in South Africa 1998. October, 1999. http://www.doh.gov.za/docs/index.html (accessed March 2, 2006).
17 WHO. Beyond the numbers: reviewing maternal deaths and complications to make pregnancy safer. Geneva: World Health Organization, 2004.
Articles
www.thelancet.com Published online March 28, 2006 Webfigure
WHO analysis of causes of maternal death: a systematic review
Ref numberEditor
AuthorCreated by
Special instructions (PLEASE MARK WITH RED SPOT IF URGENT)05TL_838_web.epsVCKHANSW
Specialty coloursLancet journal colours100% 10%
use for background tint
35% 100% 10%use for
background tint
35%Shapes
XXXXXXXXXXXXXXXXXXXXXXXXXX
HaemorrhageHypertensive disordersSepsis/infectionsAbortionOther direct causes of deathOther indirect causes of deathUnclassified deaths
0% 10% 20% 30% 40% 50%
% of maternal deaths attributed to specific cause
60% 70% 80% 90% 100%
Democratic Republicof the Congo
EgyptSenegal
Tanzania
South AfricaZambia
Zimbabwe
MulticountryBangladesh
ChinaTaiwan/China
IndiaIran
JordanKoreaNepal
PakistanSingapore
ThailandFrance
UKGreece
RomaniaUSA
ArgentinaChileCuba
Domincan Republic
HondurasMexico
PeruParaguay
SurinamVenezuela
Correspondence to: Dr A Metin Gülmezoglu
Webfigure: Distribution of causes in 34 datasets for joint cause of death
Articles
www.thelancet.com Published online March 28, 2006 Webtable
WHO analysis of causes of maternal death: a systematic review
Correspondence to: Dr A Metin Gülmezoglu
Settings Year(s) Data source Number of maternal deaths
Maternal mortality ratio
Coverage Quality appraisal (0–5)
Iloki, et al (1) Democratic Republic of the Congo
1997 Survey 143 510 District 5
National Maternal Mortality Study (2) Egypt 2000 Survey 585 84 National 5
Kodio, et al (3) Senegal 2002 Survey 87 690 District 3
Macleod and Rhode (4) Tanzania 1988 Survey 76 529 District 4
Report on confidential enquiries into maternal deaths (5,6)
South Africa 2001, 2003 Confidential inquiry 3121 150 National 5
Nsemukila, et al (7) Zambia 1998 Survey 349 729 National 3
Rutgers (8) Zimbabwe 2001 Survey 92 695 Province 4
Bouvier-Colle, et al (9) Multicountry 2001 Survey 55 334 Districts (7) 4
Rahman, et al (10) Bangladesh 2002 Survey 7086 322 National 4
Ding and Zhang (11) China 1999 Survey 6706 56 Provinces (30) 2
Maternal and Child Health Institute (12) Taiwan/China 2000 Vital statistics 54 9 Island-wide 2
Registrar General (13) India 1999 Vital statistics 577 540 National 3
Naghavi (14) Iran 1999 Survey 382 76 National 2
Nushaiwat (15) Jordan 1998 Survey 51 40 National 4
Youngja, et al (16) Korea 1999 Survey 142 20 National 5
Raj, et al (17) Nepal 1998 Survey 125 539 District 2
Fikree, et al (18) and Midhet, et al (19) Pakistan 1997, 1998 Survey 299 533 Districts 2
Lau (20) Singapore 2002 Confidential inquiry 51 11 National 3
Kanshana, et al (21) Thailand 2002 Vital statistics 616 36 National 3
Bouvier-Colle, et al (22) France 2001 Vital statistics 237 7 National 1
Mantel and Moodley and confidential enquiries into maternal deaths (23,24)
UK 2000, 2002 Confidential inquiry 510 13 National 2 of 5
Dimitrakakis, et al (25) Greece 2001 Vital statistics 136 4 National 1
Evidence and Information for Policy, WHO (26) Romania 2002 Vital statistics 537 34 National 1
National Vital Statistics Report (27–30) USA 1997-2000 Vital statistics 1403 9 National 3
Central Statistics Service (31,32) Argentina 1999, 2001 Vital statistics 1124 41 National 1 of 2
Donoso Sina, et al (33) Chile 1998 Vital statistics 63 20 National 2
Annual Health Statistics (34) Cuba 2002 Vital statistics 380 42 National 3
Public Health Statistics (35) Dominican Republic 1999 Vital statistics 146 178 National 3
Melendez Bardales, et al (36) Honduras 1999 Vital statistics 192 108 National 5
Reyes, et al (37) Mexico 1998 Vital statistics 8415 64 National 1
Evidence and Information for Policy, WHO (38) Peru 2002 Vital statistics 524 185 National 1
Evidence and Information for Policy, WHO (39) Paraguay 2002 Vital statistics 212 192 National 1
Mungra (40) Surinam 1999 Confidential inquiry 64 226 National 5
Annual Vital Statistics (41,42) Venezuela 1996, 2001 Vital statistics 657 67 National 3
Citations in parentheses refer to webreferences in the webappendix. Information stated according to the extent of fulfilment of individual quality components mentioned in the main text. National estimates from Maternal Mortality Estimates developed by WHO, UNICEF and UNFPA. Geneva: WHO, 2004 (not from the datasets).
Webtable: Characteristics of data sources used in analysis for joint cause of maternal death

Articles
www.thelancet.com Published online March 28, 2006 Webappendix
WHO analysis of causes of maternal death: a systematic review
Correspondence to: Dr A Metin Gülmezoglu
1 Iloki LH, G’Bala Sapoulou MV, Kpekpede F, Ekoundzola JR. [Maternal mortality in Brazzaville (1993–1994)]. J Gynecol Obstet Biol Reprod (Paris) 1997; 26: 163–68.
2 Ministry of Health and Population. Egypt National Maternal Mortality Study 2000. Cairo, Egypt: Ministry of Health and Population, 2001.
3 Kodio B, de Bernis L, Ba M, Ronsmans C, Pison G, Etard JF. Levels and causes of maternal mortality in Senegal. Trop Med Int Health 2002; 7: 499–505.
4 Macleod J, Rhode R. Retrospective follow-up of maternal deaths and their associated risk factors in a rural district of Tanzania. Trop Med Int Health 1998; 3: 130–37.
5 Moodley, J. Saving mothers. Report on confidential enquiries into maternal deaths in South Africa. Pattinson B, ed. Pretoria, South Africa: Ministry of Health, Republic of South Africa, 1999.
6 Ministry of Health, Republic of South Africa. Saving mothers: second report on confidential enquiries into maternal deaths in South Africa 1999–2001. Johannesburg, South Africa: Ministry of Health, Republic of South Africa, 2001.
7 Nsemukila BG, Phiri DS, Diallo HM, Banda SS, Benaya WK, Kitahara N. A study of factors associated with maternal mortality in Zambia, 1998. Lusaka, Zambia: Ministry of Health, 1999.
8 Rutgers S. Two years maternal mortality in Matebeleland north Province, Zimbabwe. Cent Afr J Med 2001; 47: 39–43.
9 Bouvier-Colle M-H, Ouedraogo C, Dumont A, Vangeenderhuysen C, Salanave B, Decam C. Maternal mortality in West Africa: Rates, causes and substandard care from a prospective survey. Acta Obstet Gynecol Scand 2001; 80: 113–19.
10 Rahman MH, Akhter HH, Khan CMEE, Yusuf HR, Rochat RW. Obstetric deaths in Bangladesh, 1996–1997. Int J Gynecol Obstet 2002; 77: 161–69.
11 Ding H, Zhang L. Analysis of national maternal mortality rate surveillance. Maternal Death Investigation Cooperative Group of China. [Chinese]. Chung Hua Fu Chan Ko Tsa Chih 1999; 34: 645–48.
12 Statistics relating to maternal and child health in Taiwan. Taiwan: Maternal and Child Health Institute, Department of Health, 2000.
13 Registrar General India. SRS bulletin. SRS Bull 1999; 33: 1–8.14 Naghavi, M. Maternal mortality rate (MMR) measured by the
reproductive age mortality survey (RAMOS) method. Islamic Republic of Iran—1996. Teheran, Iran: Ministry of Health, 1998.
15 Nushaiwat MI. Maternal mortality: extent and causes; strategies for reduction. In: Jordan's Health Status. Amman, Jordan: Ministry of Health and Health Care and USAID, 1998.
16 Youngja H, Serok D, Junghan P, Seungwook, L. Maternal mortality ratio and causes of death in 1995–1996 in Korea. Korea: Korea Institute for Health and Social Affairs, Ministry of Health and Welfare, 1999.
17 Raj LP, Malla DS, Pradhan A, Rajlawat R, Campbell BB, Kwast B. Maternal Mortality and Morbidity Study. Nepal: Family Health Division, Department of Health Services, Ministry of Health, 1998: 1–123.
18 Fikree FF, Midhet F, Sadruddin S, Berendes HW. Maternal mortality in different Pakistani sites: ratios, clinical causes and determinants. Acta Obstet Gynecol Scand 1997; 76: 637–45.
19 Midhet F, Becker S, Berendes HW. Contextual determinants of maternal mortality in rural Pakistan. Soc Sci Med 1998; 46: 1587–98.
20 Lau G. Are maternal deaths on the ascent in Singapore? A review of maternal mortality as reflected by coronial casework from 1990 to 1999. Ann Acad Med Singapore 2002; 31: 261–75.
21 Kanshana S, Amornwichet P, Nuntamanop S, Kullerk N. Maternal mortality in Thailand during 1997–1998. Thai J Obstet Gynaecol 2002; 14: 111–20.
22 Bouvier-Colle M-H, Pequignot F, Jougla E. Maternal mortality in France: frequency, trends and causes. J Gynecol Obstet Biol Reprod (Paris) 2001; 30: 768–75.
23 Mantel GD, Moodley J. Can a developed country's maternal mortality review be used as the 'gold standard' for a developing country? Eur J Obstet Gynecol Reprod Biol 2002; 100: 189–95.
24 National Statistics Office. Why mothers die 1997–1999. Report from the confidential enquiries into maternal deaths in the United Kingdom. London: National Statistics Office, 2000.
25 Dimitrakakis C, Papadogiannakis J, Sakelaropoulos G, Papazefkos V, Voulgaris Z, Michalas S. Maternal mortality in Greece (1980–1996). Eur J Obstet Gynecol Reprod Biol 2001; 99: 6–13.
26 Evidence and Information for Policy, WHO. WHO Maternal Mortality data base. Romania 2004. Geneva, Switzerland: Evidence and Information for Policy, World Health Organization, 2004.
27 Minino AM, Arias E, Kochanek KD, Murphy SL, Smith BL. Deaths: final data for 2000. Natl Vital Stat Rep 2002; 50: 1–119.
28 Hoyert DL, Arias E, Smith BL, Murphy SL, Kochanek KD. Deaths: final data for 1999. Natl Vital Stat Rep 2001; 49: 1–113.
29 Hoyert DL, Kochanek KD, Murphy SL. Deaths: final data for 1997. Natl Vital Stat Rep 1999; 47: 1–104.
30 Peters KD, Kochanek KDMA, Murphy SL. Deaths: final data for 1996. Natl Vital Stat Rep 1998; 47: 1–98.
31 Instituto Nacional de Estadisticas y Censos (INEC) and Ministerio de Salud (MINSA). Anuario Estadístico de la República Argentina 2001. Buenos Aires, Argentina: Instituto Nacional de Estadisticas y Censos (INEC) and Ministerio de Salud (MINSA), 2002.
32 Montero HE, Dorfman, MS. Anuario Estadistico de la Republica Argentina. Instituto Nacional de Estadistica y Censos se encuetran a la vene en INDEC, Centro Estadisico de Servicios. Roca, Buenos Aires, Argentina: Instituto Nacional de Estadistica y Censos se encuetran a la vene en INDEC,Centro Estadisico de Servicios, 1999.
33 Donoso Sina E, Poblete L, Villarroel del Pino L. Mortalidad materna: Chile 1990–1996. Rev Chil Obstet Ginecol 1998; 63: 290–97.
34 Ministry of Health. Anuario Estadístico de Salud de Cuba 2002. http://bvs.sld.cu/cgi-bin/wxis/anuario/?IsisScript=anuario/iah.xis &base=anuario&lang=e, Biblioteca Virtual de la Salud, Cuba. (accessed March 16, 2006).
35 Secretaría de Estado de Salud Pública. Situación mortalidad materna 1998: informe elaborado al 21/4/99 1999. Santo Domingo, República Dominicana. Secretaría de Estado de Salud Pública y Asistencia, 1999.
36 Melendez Bardales JH, Ochoa Vasquez JC, Yanira VM. [Research on maternal mortality and mortality of women of reproductive age in Honduras. Final report for 1997]. [Unpublished] Honduras, 1999.
37 Reyes FS, Lezana Fernandez MA, Garcia P, Bobadilla Fernandez JL. Maternal mortality regionalization and trend in Mexico (1937–1995). Arch Med Res 1998; 29: 165–72.
38 Evidence and Information for Policy, WHO. WHO Maternal Mortality data base. Peru. Geneva: Evidence and Information for Policy, World Health Organization, 2004.
39 Evidence and Information for Policy, WHO. WHO Maternal Mortality data base. Paraguay. 2004. Geneva: Evidence and Information for Policy, World Health Organization, 2004.
40 Mungra A. Confidential enquiries into maternal deaths in Surinam. Leiden: TNO (Netherlands Organisation for Applied Scientific Research)—Prevention and health in Leiden, The Fetal Maternal Research Foundation in Leiden (Oranjekliniek), 1999.
41 Ministerio de Salud y Desarrollo Social, Republica Boliviana de Venezuela. Anuario de Mortalidad 2001. Caracas, Venzuela: Dirección de Información Social y Estadística, Ministerio de Salud y Desarrollo Social, 2002.
42 Ministerio de Sanidad y Asistencia Social. Anuario de Epidemiología y Estadística Vital. Año 1996. Caracas, Venezuela: Ministerio de Sanidad y Asistencia Social, 1998.





























