Embed Size (px)
Citation preview

White Paper
Improving Outcomes for Patients with Type 2 Diabetes: A Bundle Measure ApproachTogether 2 Goal® Diabetes Bundle Best Practices Learning Collaborative

2
Diabetes: Together 2 Goal® is AMGA (American Medical Group Association) Foundation’s national campaign that challenges participating medical groups and health systems to improve care for one million people with type 2 diabetes. This initiative is part of a larger effort by AMGA to help improve quality of care and patient outcomes for chronic conditions that have the greatest impact on quality of life, productivity, and costs for Americans.
In May 2019, AMGA launched the Together 2 Goal® Diabetes Bundle Best Practices Learning Collaborative (T2G Bundle Collaborative), in partnership with Novo Nordisk, Inc., to augment the quality improvement work of 10 member healthcare organizations (HCOs) that were actively participating in Together 2 Goal®.
Improving Outcomes for Patients with Type 2 Diabetes: A Bundle Measure ApproachTogether 2 Goal® Diabetes Bundle Best Practices Learning Collaborative
Cori Grant, Ph.D., M.B.A., M.S.; Earlean Chambers, RN, M.S., CPHQ; Cori Rattelman, M.S.
White Paper, December 2020
Figure 1. T2G Bundle Collaborative Timeline
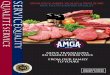
Bundle Measure Computation The T2G Bundle Collaborative focused on an all-or-none diabetes bundle measure. All-or-none measures more closely align with the patient’s perspective of care and promote both a holistic approach to chronic disease management and a system-wide approach to improvement of care. This bundle measure includes four indicators, hemoglobin A1c (A1c) control (<8%), blood pressure control (<140/90), lipid management, and medical attention for nephropathy. To achieve bundle control, a patient must be compliant (or in control) for all four individual metrics. In the example illustrated in Figure 2, this representative organization is performing relatively well on each of the four individual bundle component measures. Among patients with diabetes, 86% received medical attention for nephropathy, 66% have A1c <8%, 72% have blood pressure <140/90, and 66% are receiving lipid management. The best this organization could do at this current level of performance is a bundle control rate equal to their lowest scoring metric, or 66%. Despite performing well on each of the individual measures, the percent of patients meeting all four measures is less than half of their lowest scoring metric, or 31.4%. This example illustrates the importance of a bundle measure and the challenges involved in improvement of such a measure.
Revised due to COVID-19
Baseline Data Reported
Final Data Reported
Kick-off Meeting
Wrap-up Meeting
Intervention Period
• December 2018 • January 2020 • July 2020• March 2019 • March 2019 – January 2020

3
The T2G Bundle Collaborative The T2G Bundle Collaborative used the AMGA Best Practices Learning Collaborative framework (Figure 3). This framework creates a community of knowledge that helps participants accelerate systematic change and make lasting improvements to provide high-quality patient care. The following activities took place within the collaborative framework.
Project Teams. Participating organizations in the T2G Bundle Collaborative created a project team with designated clinical and administrative champions, a project manager, an IT/data specialist, and team members including a physician and frontline staff.
QI Reporting. Action plans were drafted by each HCO at the start of the T2G Bundle Collaborative and updated bimonthly. Action plans defined specific objectives and monitored interventions, progress toward goals, and lessons learned. Each month the participants reported aggregate data in the form of numerators and denominators for the previous 12 months of data. This included the bundle measure
Figure 3. AMGA Best Practices Learning Collaborative Framework
Figure 2. Example of the Bundle Measure Computation
Attention for Nephropathy – 86.0%
BP <140/90 – 72.0%
A1c <8 – 66.1%
Lipid Management – 65.9%

4
and each of the individual measures. AMGA Analytics used this information to provide transparent monthly progress and benchmarking reports to collaborative participants.
Tools and Resources. The Collaborative used the resources of the T2G campaign, including the original Together 2 Goal® Campaign Toolkit and Campaign Toolkit Supplement, newsletters, and recorded webinars.
Engagement. Participating organizations met in person at the start of the T2G Bundle Collaborative to discuss plans, challenges, lessons learned, achievements, and new tools and resources, and to receive inspiration and encouragement. Webinars were held every other month to share benchmarking reports and best practices, as well as provide additional education from the advisors. Site visits and regular calls with interactive team discussion and coaching from AMGA quality improvement staff were held to maintain engagement between webinars. An AMGA listserv and portal were used to enable asynchronous communication and access to webinar recordings, extra tools, comparative data, and more.
Interventions Each participating HCO selected interventions for implementation at their health system that fit within their local contexts. Those interventions, implemented by all participating HCOs, included scorecards, provider and staff education, and daily huddles (Figure 4).
Figure 4. Number of Healthcare Organizations Implementing Each Intervention
0 2 4 6 8 10
HCOs
Daily Huddles
Provider/Staff Education
Physician Performance Reports
CDEs in Clinics or Referrals
Labs in Clinics/POC A1c
Provider Incentives
Bundle Included in Quality Metrics
Patient Outreach - 1 Uncontrolled Measure
Patient Education
Standard Orders
PharmD in Clinics
EHR Enhancements
Weekly/Enhanced Huddles
Virtual Patient Education
Patient Outreach - >1 Uncontrolled Measures

5
Scorecards. Timely and transparent performance feedback was provided by the HCO through physician performance reports which allowed them to see how they performed against their peers. Additionally, most had quality goals with compensation tied to the bundle measure.
Clinical Education. Information was shared across specialties and disciplines. Topics such as clinical standards for diabetes care, frequency of laboratory testing and targets, key medications, and recommendations for statin use were included.
Team-Based Approach. All participants performed pre-visit planning sessions, or daily huddles, conducted by clinical staff to review patient records and close gaps in care during patient visits. Several implemented point of care (POC) A1c testing in the office during primary care appointments, which allowed the primary care physician (PCP) to have up-to-date A1c results to discuss with the patient during the visit. Some participants created multidisciplinary teams—including a clinical pharmacist, nurse navigator, social worker, dietitian, and patient panel manager—to conduct weekly huddles prior to the daily huddles. Additionally, standing orders for insulin titration, registered dietitian (RD)/Certified Diabetes Care and Education Specialist (CDCES) referrals, and A1c testing were implemented. The combination of daily huddles, on-site screening, and standing orders enabled staff to work at the top of their license.
Patient Engagement. Outreach campaigns and patient education were utilized by nearly all of the participating groups. Most targeted outreach to patients who were missing one clinical measure in order to rapidly bring those patients into full bundle compliance, while others focused outreach on the highest risk patients who were out of compliance on multiple measures. One HCO mailed letters containing patient education to 5,000 patients. Several contacted patients after a hospitalization to schedule an office visit for them.
EHR Enhancements. One participant added a Diabetes Super Best Practice Advisory to their EHR which enabled providers to reinforce standards of care and alerted them to patients with overdue health maintenance. Another conducted patient outreach using Epic’s MyChart to send a message to patients who were due for a test or had a high A1c result. An academic medical center expanded their ability to complete A1c testing on their patients in need of testing by programming a best practice alert (BPA) that notified the team when patients who were seen for a cardiology appointment were overdue for testing. The cardiology team referred the patient to the lab to have blood drawn, and results were mailed to the patient with a note asking them to follow up with their PCP. Results were also sent to the referring physician.
Innovation. Pharmacy students were utilized to review charts and identify patients who were appropriate candidates for statins. When patients were identified, after consulting with the PCP and if there were no contraindications, the student reached out to the patients and coordinated the prescribing of a statin between the patient and the PCP.

6
ResultsDuring the T2G Bundle Collaborative, the bundle measure, as well as each of the individual measures, improved over the 13 months from baseline reporting (Table 1). The relative improvement rate (RIR) for the bundle measure, which included all HCOs in the T2G Bundle Collaborative, was 6.7% (ranging from 3% to 11% across the 10 organizations). The RIR for each of the individual measures ranged from a low of 0.7% for attention to nephropathy to 2.7% for blood pressure control (RIR for each measure can be seen in Table 1, Column 4).
When compared to HCOs participating in the T2G Campaign over a similar time period (in this case December 2018 through December 2019), participants in the T2G Bundle Collaborative showed greater improvement over time for each of the individual measures and for the bundle relative to the campaign participants (Table 1, Column 5).
Challenges and Lessons LearnedImproving the bundle measure took time, focus, and teamwork across multidisciplinary teams. Teamwork was successfully endorsed through goals that were aligned across specialties and focused on a smaller number of quality measures closely aligned with the bundle.
Creating tools for providers did not always translate into use. It required establishing formal processes that integrated the tools to facilitate adoption. Some stressed the importance of integrating the tools into the EHR when possible with a focus on user experience. For example, enabling users to enter information in fewer steps was complicated and took more time on the front end, but it was important to the users. Strong partnerships with good communication are important for POC A1c testing. For example, one organization had difficulty garnering support to do POC testing due to concerns about the accuracy of the results if they were processed outside of the laboratory. A pilot study was conducted to validate the results from POC tests. Results were consistent with the laboratory testing, and the program was expanded into more areas. Initially, results were entered manually into the EHR, but were ultimately successfully uploaded automatically into the EHR, which made them more accessible during the PCP visit.
Buy-in from patients and providers was key. For example, some patients were reluctant to take statins, and physicians were sometimes reluctant to prescribe them for this reason. Participants found that including education for patients and providers, employing motivational interviewing techniques, and consistent messaging during
Table 1. Improvement in Collaborative Measures over Time and vs Campaign Participants
Collaborative1 Average Group Outcomes
Baseline Report
(Dec 2018)(1)
Final Report
(Jan 2020)(2)
AbsoluteChange
(3)
RelativeChange
(4)
Relative Improvement Compared to Campaign2
(as of 2019Q4)(5)Measures
1 Collaborative includes 10 healthcare systems2 Campaign includes 51 healthcare systems that reported in both the bundle baseline reporting period and 2019Q4
A1c < 8.0 67.% 68.5% 1.2% 1.8% 2.2x
BP < 140/90 76.5% 78.6% 2.1% 2.7% 1.6x
Attention for Nephropathy 90.7% 91.3% 0.6% 0.7% 1.8x
Lipid Management 77.3% 79.2% 1.9% 2.5% 1.2x
T2G Bundle 40.2% 42.9% 2.7% 6.7% 1.8x

7
patient outreach, using dedicated and trained staff and scripting, contributed to acceptance of statin use. Furthermore, converting patients who typically fill 30-day prescriptions to 90-day prescriptions resulted in more consistent use of all medications.
SustainabilityThe participants described several strategies they are employing for sustaining progress in the bundle measure.
Transparency. One participating HCO is in the process of developing a portal so providers can log in to see their quality scores on demand.
Consistency. Several developed standard processes, templates, and other tools that are integrated into the EHR. Another rolled the bundle subcommittee under the larger quality committee to expand support for the initiative. Another is maintaining POC A1c testing and developing standards for frequency of testing patients, for example, POC testing three times per year with full labs annually.
Education. Most participants are continuing frequent clinical education and communication across the organization. One participant is using monthly “Q-TIPS” (Figure 5) to provide small bites of information.
Innovation. Many are continuing to find ways to leverage opportunities for remote patient monitoring.
COVID-19The intervention period was originally planned to be a full 12 months ending in March 2020; however, the T2G Bundle Collaborative reporting period ended in January 2020 due to COVID-19. An unintended positive consequence of this work may have been an enhanced capability to adjust to and overcome the disruptions to diabetes care management as a result of the pandemic. During the wrap-up session in July 2020, we asked participants to tell us how they had adapted in response to COVID-19. Most reported that they employed new technologies, remote monitoring, or other innovative approaches to engage patients with diabetes when more visits were converted to telehealth. Some of the activities they reported included:
• Monitoring patients virtually, for example, allowing them to report readings from blood pressure cuffs during telehealth visits
• Collaborating with payers to do in-home testing and screening (colorectal and microalbumin)
• Offering drive-up services for A1c testing, blood pressure monitoring, and immunizations
• Repurposing a bus used for events to perform laboratory services, including phlebotomy, a retinal camera, and nephropathy screening to their patients
• Conducting virtual education visits
• Patient outreach to ensure patients had things like food and to schedule past-due appointments
Figure 5.

8
ConclusionThe HCOs that participated in the intensive T2G Bundle Collaborative achieved greater improvement in the bundle measure when compared to those in the T2G campaign that did not participate. In addition, the T2G Bundle Collaborative touched the lives of more than 296,000 patients with diabetes. Beyond the achievements in the T2G campaign, the improvements achieved in the T2G Bundle Collaborative resulted in an additional 3,100 patients with A1c control, 5,900 patients with blood pressure control, 1,500 patients with attention for nephropathy, 6,000 patients receiving lipid management, and 8,000 additional patients achieving the bundle measure.
Table 2. Additional Patients who Improved for Each Measure
* These numbers are beyond the achievements of the T2G campaign
Measure Number*
Achieved A1c control 3,100
Achieved blood pressure control 5,900
Received attention for nephropathy 1,500
Received lipid management 8,000
Diabetes Bundle Collaborative Participants, National Advisors, AMGA Staff, and Novo Nordisk Representatives at the Kick-off In-Person Meeting, May 2019.
Participation Healthcare Organizations:
Excela HealthGeisinger Health SystemMercy Clinic East CommunitiesMichigan Medicine University of MichiganNorton Medical Group
Ochsner Health SystemPalo Alto Medical FoundationPrivia HealthSummit Medical Group, P.A.Valley Medical Group

AMGA is a trade association leading the transformation of health care in America. Representing multispecialty medical groups and integrated systems of care, we advocate, educate, and empower our members to deliver the next level of high performance health. AMGA is the national voice promoting awareness of our members’ recognized excellence in the delivery of coordinated, high-quality, high-value care. More than 170,000 physicians practice in our member organizations, delivering care to one in three Americans. For more information, visit amga.org.
One Prince StreetAlexandria, VA 22314-3318
amga.org






![3 AMGA Manager AMGA Hands-on 20110916 v2.ppt [호환 모드] · 09/06/2011 The Plan of AMGA Manager for Belle II 1.User Friendly Interface 2.Fast AMGA Connections 3.Powerful Schema](https://img.pdfslide.us/doc/110x75/5ed328981270b562de153f3c/3-amga-manager-amga-hands-on-20110916-v2ppt-eeoe-09062011-the-plan.jpg)