Embed Size (px)
Citation preview

WILDERNESS & ENVIRONMENTAL MEDICINE, 25, 56–59 (2014)
CASE REPORT
Where Wilderness, Medicine, Technology, andReligion CollideLori Weichenthal, MD; Sameir Alhadi, MD
From the Medical Education and Research Center, University of California-San Francisco, Fresno, CA.
Correspondiand ResearchFresno Street,edu).
We report a case of a man injured in Yosemite National Park (YNP) whose use of technology andrefusal of medical care, based on his Christian Science religious beliefs, created multiple challenges tothe providers working to rescue and care for him. This case illustrates how our increasingly diverse andcomplex world requires flexibility and openness to provide the optimal care, both in the wilderness andin the front country.
Key words: search and rescue, technology, trauma, ethics, refusal of care, religion
Introduction
Yosemite Search and Rescue (YOSAR) was formallyestablished in 1974 to respond to emergencies withinYosemite National Park (YNP).1,2 In 2012, YOSARresponded to more than 245 incidents, including 15major search and rescue incidents.3 One of these majorincidents occurred in June 2012, when YOSAR came tothe aid of a man who sustained traumatic injuries whilehiking near Illilouette Falls in YNP. The subject’s refusalof medical care because of his Christian Sciencereligious beliefs created many challenges to thoseseeking to help him, both in the wilderness setting andonce he reached definitive medical care. We hope toshed light on the quarrels that can sometimes arise whenthe wilderness, medicine, technology, and religioncollide.
Case Report
On June 28, 2012, a 65-year-old man set out alone tohike in Yosemite. The subject was a regular visitor to thepark and was reportedly in excellent physical condition.Before setting off on his trek, he left a voice mail for hiswife indicating his planned route. As a backup method ofcommunication, he also sent a text to his wife with hisplans for the day. She was in the valley of YNP,
ng author: Lori Weichenthal, MD, Medical EducationCenter, University of California-San Francisco, 155 N.Suite 206, Fresno, CA 93701 (e-mail: [email protected].
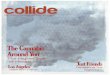
attending an art class. He then set off from the LowerPines Campground in Yosemite Valley (Figure 1).Starting his off-trail hike at the junction of the MercedRiver and Illilouette Creek he began his ascent towardIllilouette Falls. Four hours into his hike, he encounteredsteep Class 5 terrain (technical climbing requiring theuse of rope and belaying) near Glacier Point. Whenclimbing over a large boulder, he lost his footing and felldown a rock wall, tumbling approximately 30.5 m (100feet). He came to a halt on a granite ridge near the baseof the Illilouette Falls. The subject landed on his rightside and suffered intense pain in his neck, right hip, andlower back. He lay on his back, and could not move.The subject quickly surmised that his choice to
venture off standard trails lessened his chance of beingdiscovered by fellow hikers. At some point, he checkedhis cell phone, and upon discovering that he had service,he first attempted to call his wife. In a 30-minute period,he left 3 messages for her, all without an answer. He alsosent an “SOS” as a text message to 911 during this timeperiod. In reply, he received a standardized text messageasking him to make a voice call to 911 as text serviceswere not available. The subject never accessed 911 via avoice call.Our subject’s wife never received any of his calls as
she had turned her phone off during her art class. Whenshe finally turned her phone on, nearly an hour after hisfall, she discovered she had messages from her husbandbut could not access them because of her cell phonecoverage. She called her son, who was able to access hercell phone voice mail remotely and determine that our

Figure 1. Map of Yosemite Valley. Red squares illustrate the start of subject’s hike and where he became injured.
Figure 2. Example of a vacuum body splint.
Where Wilderness, Medicine, Technology, and Religion Collide 57
subject was in need of assistance. His wife was then ableto contact volunteers at the Lower Pines Campgroundwho notified park rangers and YOSAR. Rescuers werethen able to talk with our subject on his cell phone, andnear sunset, a team of 3, including a park medic, headedup the Illilouette drainage in search of him. Park medicsare park rangers with specialty medical training that issimilar to an Advanced Emergency Medical Technician(AEMT) but with an expanded pharmacological andprocedural scope of practice.4
When the rescuers made contact with our subject, itwas after 8:00 PM and nearly dark. On initial survey theynoted he had severe back and leg pain and an open fingerfracture avulsion. Owing to the severity of his injuriesand the impending nightfall, rangers were unable totransport the patient and made the decision to campovernight. They placed him in a vacuum body splint tomaintain motion restriction and to help stabilize hisinjuries (Figure 2). Rangers stayed with him overnight.During this time, the subject refused all medical treatmentoutside of the stabilization provided by the vacuum bodysplint, citing his Christian Science religious beliefs. Carethat he refused included the placement of an IV andparenteral administration of isotonic fluids, antibiotics,and pain medications. He also refused all oralmedications but did accept food and water. At sunrise,a flight crew short hauled the subject out of thebackcountry via helicopter. A short haul is defined as atransport of one or more persons suspended beneatha helicopter (Figure 3). Crews then rendezvoused with aground ambulance unit, and he was transported to the
Yosemite Medical Clinic where a medical evaluation wasperformed.At the Yosemite Medical Clinic, the subject continued
to refuse medical interventions such as blood work,monitoring, antibiotics, wound care, and further splint-ing. Care providers at the clinic offered him the option ofsigning out against medical advice. However, when heattempted to stand up and walk, he was unable to do so,and the staff convinced him to accept transport to theclosest Level 1 trauma center, Community RegionalMedical Center (CRMC), in Fresno, California. Duringthe 2-hour transport to CRMC, the subject continued torefuse most medical interventions including an IV oranalgesics. Agreeing to only be immobilized and havebasic wound dressings, he repeatedly conveyed to his

Figure 3. Demonstration of a short haul rescue, Sequoia KingsCanyon National Park (used with permission by Dr Weichenthal).
Weichenthal and Alhadi58
medical providers that he was a devout ChristianScientist and that any other interventions went againsthis religious beliefs. The subject was a Glasgow ComaScale (GCS) of 15 throughout his prehospital course, andhis vital signs were stable.On arrival to CRMC, the emergency medicine and
trauma surgery teams evaluated him. His airway, breath-ing, and circulation were intact, and he had a GCS of 15.His vital signs included a heart rate of 62 beats/min, ablood pressure of 116/62 mm Hg, and a respiratory rateof 14 breaths/min. He was afebrile. He denied loss ofconsciousness. He also denied any allergies to medica-tions, and stated he had no prior medical or surgicalhistory. His examination revealed several deep scalplacerations, midline cervical tenderness, an open avul-sion fracture to his left fourth digit, and an abrasion withmoderate sized hematoma to his right flank and hip. Hewas unable to flex or extend his right lower extremitybecause of pain and could not ambulate.The subject continued to refuse placement of an IV and
also refused a tetanus injection or antibiotics for his visiblyopen finger fracture. He stated to one provider afterrefusing closure of his scalp wounds and finger avulsionthat through prayer his body would heal itself and that hisfractures will heal and his infections would clear.Despite his refusal of any therapeutic intervention, our
subject was agreeable to have any necessary imagingstudies performed and was open to consultation withspecialists, but wanted to have an active role in decidingwhat, if any, treatments or interventions were to be done.
His head computed tomography (CT) scan was negativefor acute hemorrhage. His CT cervical spine was notablefor a fifth cervical vertebral fracture at the right posteriorpedicle that extended into the inferior facet and lamina.Abdominal and pelvic scans were negative for solidorgan injury but did show a comminuted fracture of hisright sacral iliac wing. A magnetic resonance image ofhis lumbar spine was ordered to evaluate right lowerextremity weakness and was notable for a contusionalong his sacral bone. Plain radiographs of his left handshowed an open tuft fracture of his fourth digit.At this point neurosurgery, orthopedic surgery, hand
surgery, and social work were consulted, and the patientwas admitted to the trauma surgery service. The subjectrefused many commonly used evaluations for traumapatients including serial hemoglobin blood draws, enox-aparin for deep vein thrombosis prophylaxis, and generalnursing wound care. During his hospital stay, providersworked with him to provide the best possible care withinthe limits of his religious beliefs. He did participate withphysical therapy and was discharged on hospital day 4with a front wheel walker and follow-up with careproviders in his hometown.Our subject was lost to follow-up once he returned to
his home outside of the state of California. He was notbilled for the search and rescue effort, as YOSAR doesnot charge for their services, but he was billed for theemergency medical services (EMS) care, his visit to theYosemite Clinic, and his stay at CRMC. His healthcareinsurance covered the majority of the costs for hishospitalization at CRMC; we do not have access toinformation regarding whether the costs of his EMS andclinic care were covered.
Discussion
This case represents a unique intersection of the wilder-ness, medicine, technology, and religion. Our subject,who was reportedly an experienced hiker, made thedecision to hike off-trail with minimal supplies and,when he became injured, reached for his cell phone. Hewas extremely lucky to have cell phone service at thelocation where he was injured, but even so, the way hesought to access help (calling family and texting 911)delayed officials’ awareness of his accident. He and hisrescuers had to spend the night in the wilderness beforetransport to definitive care.Many recent papers have sought to define the relation-
ship between technology and the wilderness.5–7 Thesedocuments have suggested that we need to be aware ofthe dangers of technology damaging the very qualitiesthat we seek from our experience in the wildernessincluding the opportunity to revel in natural awe, beauty,

Where Wilderness, Medicine, Technology, and Religion Collide 59
and solitude. At the same time, it has shown that peoplewho believe that technology increases safety in thewilderness may be more willing to take risks.8
Layered on top of this debate regarding the appro-priate interaction between the wilderness and technologywas our subject’s religious beliefs. He described himselfas a devout Christian Scientist. Based on his personalbeliefs, he refused multiple treatments that he wasoffered in the wilderness, prehospital, and hospitalsettings. Christian Science is a system of religiousthought first described in 1875 by Mary Baker Eddy inher book Science and Health, which continues to be oneof the religion’s central texts. Adherents espouse aradical form of philosophical idealism in which spiritualreality is the only reality and the material world,including sickness and death, is an illusion.9 Given thisbelief that sickness is an error of the mind, ChristianScientists have traditionally turned to prayer and spiritualhealers for the treatment of illness or injury.10 This beliefhas come in conflict with mainstream society, asevidenced by several high-profile cases in which parentsrefused medical care for their children.11
Autonomy is one of the fundamental guidelines ofmedical ethics and includes a patient’s right to refusemedical treatment that the care provider may believe isessential. Whereas in the hospital setting such refusal ofcare does not usually endanger the care providers orother patients, in austere settings with limited resourcesit has the potential to do so. On the same day that oursubject was being rescued, there were 16 other 911 callsfor medical service in YNP. During that same 24-hourperiod, there were only 7 park medics on duty. Threerescuers, including 1 park medic, spent 14 hours withour subject and placed themselves at risk to locate,stabilize, spend the night with, and ultimately extricatehim. The advanced medical skills of the park medicwere all refused by the patient. This care provider’sabilities might have been better used by other peoplewho found themselves injured or ill in YNP during thatperiod.
This case displays the complexity of all humaninteractions. We may view the wilderness as a place ofsimplicity and clarity, but as human beliefs and technol-ogy become more entwined in these regions that we havereserved as austere sanctuaries, we will need to be moreaware of how humans, the wilderness, medicine, tech-nology, and our personal religious beliefs interact.
References
1. Boore SM, Bock D. Ten years of search and rescue inYosemite National Park: examining the past for futureprevention. Wilderness Environ Med. 2013;24:2–7.
2. Fimrite P. United States honors Yosemite search andrescue ranger. San Francisco Chronicle. October 30, 2008.
3. Search and Rescue: Lessons from the Field. Available at:http://www.nps.gov/yose/blogs/psarblog.htm. AccessedJanuary 28, 2013.
4. Kaufman TI, Knopp R, Webster T. The ParkmedicProgram: prehospital care in the national parks. Ann EmergMed. 1981;10:156–160.
5. Shultis J. The impact of technology on the wildernessexperience: a review of common themes and approaches inthree bodies of literature. USDA Forest Service Proceed-ings. 2012:110–118.
6. Borrie WT. The impacts of technology on the meaning ofwilderness. Proceeding of Sixth World Congress Sympo-sium on Research, Management, and Allocation. 1998:87–88.
7. Pohl S. Technology and wilderness experience. EnvironEthics. 2006;28:147–163.
8. Pope K, Martin SR. Visitor perceptions of technology, risk andrescue in wilderness. Int J Wilderness. 2011;17:19–26, 48.
9. Schoepflin RB. Christian Science on Trial: ReligiousHealing in America. 1st ed. Baltimore, MD: JohnsHopkins University Press; 2002.
10. Benson H, Dusek JA. Self-reported health and illness andthe use of conventional and unconventional medicine andmind/body healing by Christian Scientists and others. JNerv Ment Dis. 1999;187:539–548.
11. May L. Challenging medical authority: the refusal oftreatment by Christian Scientists. Hastings Cent Rep.1995;25:15–21.