Embed Size (px)
Citation preview

When Athletes Can’t Breathe:Exercise-Induced Asthma/Bronchospasm
Mark A. Brown, M.D.
Professor of Pediatrics
Director, University of Arizona Pediatric Pulmonary Center
+
++++9+=9+/+
+
If from running, gymnastic exercises, or any other work, the breathing becomes difficult, it is called “Asthma”. The symptoms of its approach are heaviness of the chest…, difficulty of breathing in running or on a steep road.
Areteaus, The Cappadocian, First Century AD
Definitions
• EIB - Symptoms of chest tightness, shortness of breath, cough and/or wheezing following vigorous exercise
• EIA - chest tightness, shortness of breath, cough and/or wheezing - triggered by exercise in a patient with asthma (known or unknown)

Prevalence
• EIB– 14% of collegiate cross country runners (Thole,
et al. Med & Sci in Sports & Exer 2001; 33:1641-1646.)
– 50% of elite summer athletes had positive screening test (Holzer, et al. J Allergy Clin Immunol 2002; 101:374-380.)

Prevalence
EIB affects approximately:• 90% of asthmatics• 35-40% of those with allergic rhinitis• 12-15% of the general population• 3-25% of athletes (higher percentages in younger
age groups)
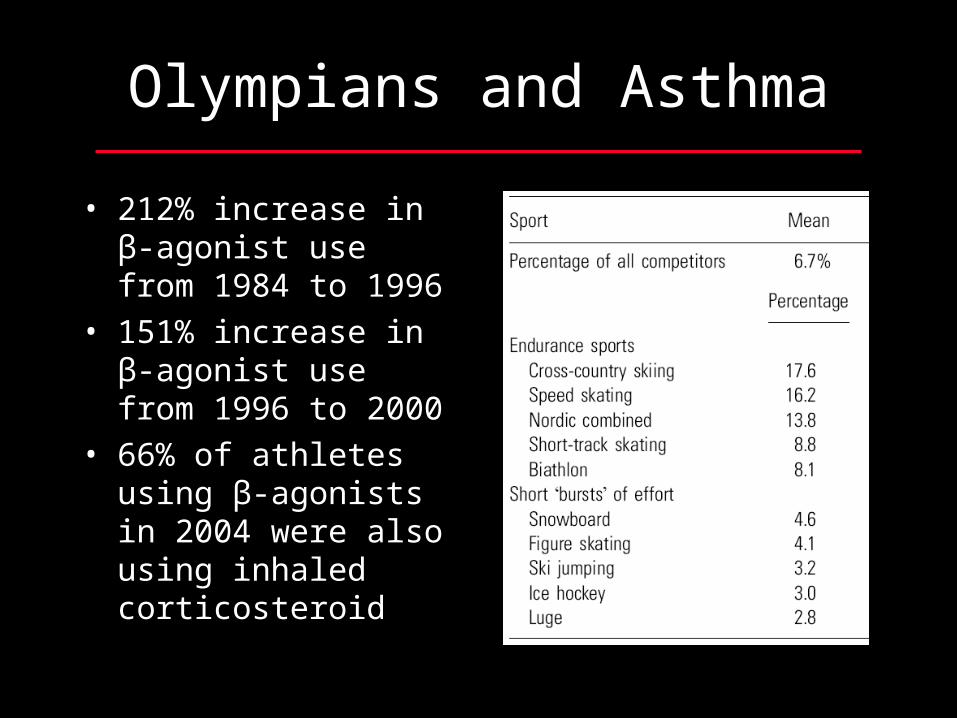
Olympians and Asthma
• 212% increase in β-agonist use from 1984 to 1996
• 151% increase in β-agonist use from 1996 to 2000
• 66% of athletes using β-agonists in 2004 were also using inhaled corticosteroid
Fitch, KD. Clin Rev Allergy Immunol 31:259, 2006Carlsen KH et al. Allergy 63:387, 2008

Typical EIB Time Course%
Bas
elin
e
Time (min)
Exercise
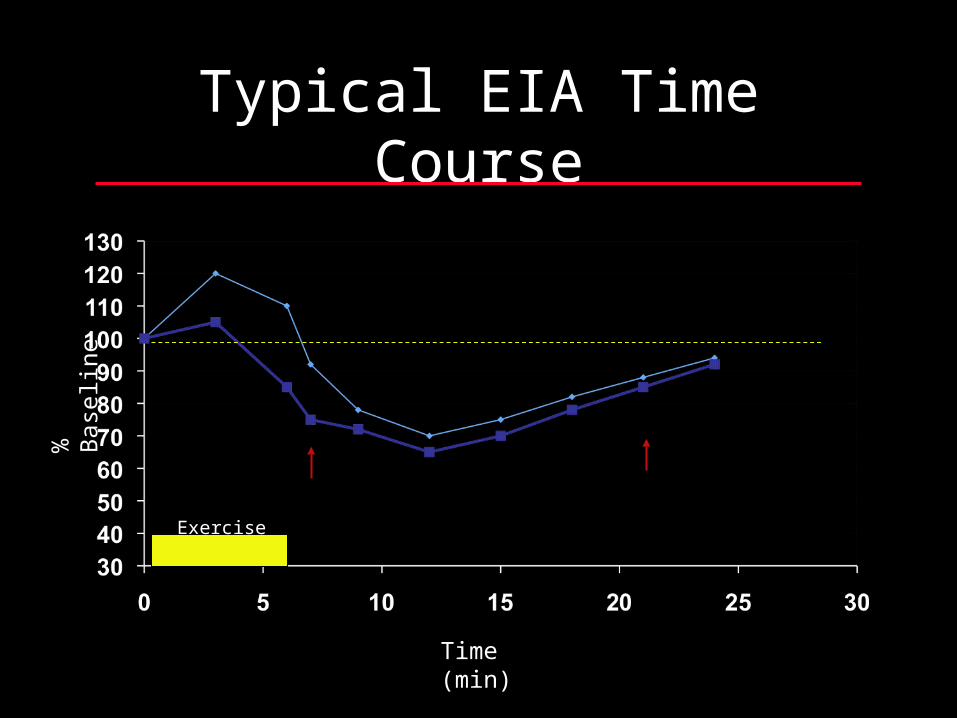
Typical EIA Time Course%
Bas
elin
e
Time (min)
Exercise

EIB Refractory period%
Bas
elin
e
Time (min)
Exercise
Physical Factors
• Exercise: type, intensity, duration
• Bronchial hyper-responsiveness (BHR)
• Environmental factors– Direct: temperature, humidity– Indirect (through increase in BHR): air
pollution, viral infections, allergen exposure

High Asthmagenic Activities
• High Minute Ventilation Activities– Long-distance running
– Cycling
– Basketball
– Soccer
– Rugby
• Activities associated with cool, dry conditions– Ice hockey
– Speed skating
– Cross country skiing
– Scuba diving

Low Asthmagenic Activities
• Low minute ventilation activities– Football– Baseball– Downhill skiing– Karate– Wrestling– Boxing– Sprinting– Gymnastics– Racquet sports– Golf
• Activities associated with warm, humid conditions– Swimming– Diving– Water polo– Water skiing

Proposed Stimuli
• Respiratory (airway) heat loss• Increased airway fluid osmolality• Rapid airway cooling and rewarming

Respiratory Heat Loss
• Degree of bronchoconstriction is proportional to respiratory heat exchange
• Sufficient respiratory heat exchange induces bronchoconstriction in the absence of exercise
» Deal, et al. J Appl Physiol 1979; 46:467-475
Respiratory Heat Loss
• Direct airway temperature measurements confirm fall with exercise/hyperventilation
» McFadden, et al. J Appl Physiol 1985; 58:564-570.
» McFadden, et al. J Appl Physiol 1985; 76:1007-1010.
• Bronchoconstriction induced following inhalation of hot dry air
» Anderson, et al. Eur J Respir Dis 1985; 67:20-30.

Increased Airway Fluid Osmolality
• Bronchoconstriction induced following inhalation of hot dry air
» Anderson, et al. Eur J Respir Dis 1985; 67:20-30.
• Level of minute ventilation necessary to induce bronchoconstriction same regardless of air temperature (humidity constant)
» Eschenbacher & Shepherd. Am Rev Respir Dis 1985; 131:894-901.

Increased Airway Fluid Osmolality
• Osmolality of nasal secretions increases in response to cold dry air
» Togias, et al. Am Rev Respir Dis 1988; 137:625-629.
• Osmolality of tracheal lining fluid is increased in tracheostomy patients
» Potter, et al. Am Rev Respir Dis 1967; 96:83-87.
• Osmolality of tracheal lining fluid is increased in dog trachea exposed to air
» Boucher, et al. J Appl Physiol 1981; 50:613-620.

Proposed Mechanisms
• Neuropeptide release• Mediator release• Vascular engorgement

Neuropeptide Release
• Hypertonic saline induces changes of neurogenic inflammation
» Umeno, et al. J Clin Invest 1990; 85:1905-1908.
• Little evidence to support sympathetic/vagal mechanisms

Mediator Release
• Supported by studies of– Direct measurement of mediators released into
lung fluid following hypertonic, hyperventilation and exercise stimuli;
– Effects of specific mediator antagonists or synthesis inhibitors on induced bronchoconstriction

Mediator Release
• Histamine• Prostaglandins• ECP• PAF• Bradykinin
• Leukotrienes• Neutrophil
chemotactic activity (IL-8, LTB4)
• Substance P/NEP

Diagnosis
• History alone is an unreliable indicator of EIB.– 45.8% of adolescents who screened negative by history
had EIB (Bukolic RE. J Peds 2002; 141:306-308.)
– Poor correlation between reported symptoms and exercise challenge in collegiate cross-country runners/elite athletes (Thole, et al. Med & Sci in Sports & Exer 2001; 33:1641-1646. Rundell, et al. Med & Sci in Sports & Exer 2001; 33:208-213. Rundell, et al. Med & Sci in Sports & Exer 2000; 32:309-316.)
Diagnosis
• Diagnosis confirmed by >15-20% fall in PEFR or FEV1 after– formal exercise challenge test taking into
account the type of exercise, temperature and relative humidity (confirmed by a positive test, but not excluded by a negative test);
– formal eucapnic hyperventilation challenge as an alternative (more sensitive; negative test usually excludes EIA).

Exercise Challenge
• Baseline spirometry or PEFR
• Exercise Challenge– Exercise to 80% calculated
maximal heart rate or O2 consumption of 30-35 ml/min/kg for 6-10 min
– FEV1 or PEFR every 3-5 min after exercise for 20-30 min
Eucapnic Hyperventilation
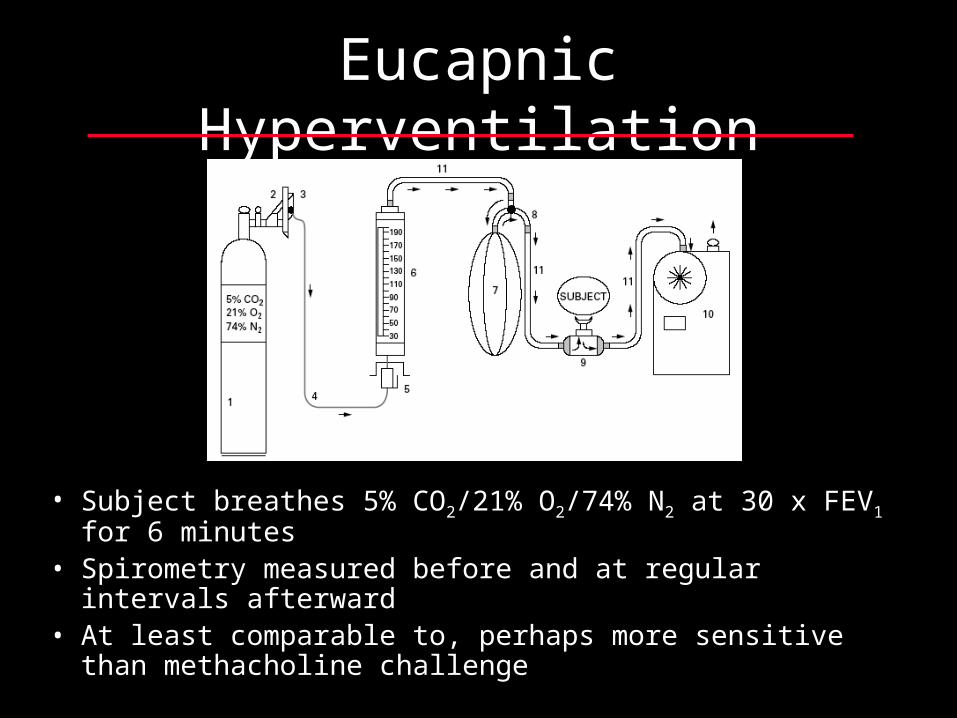
• Subject breathes 5% CO2/21% O2/74% N2 at 30 x FEV1 for 6 minutes
• Spirometry measured before and at regular intervals afterward• At least comparable to, perhaps more sensitive than
methacholine challenge

Exercise/Eucapnic Hyperventilation Response
% B
asel
ine
Time (min)
Exercise/EH

Inhaled Mannitol
• Inhalation of powdered mannitol increases lung lining fluid osmolality, perhaps mimicking changes associated with exercise.
• Compared to eucapnic hyperventilation, mannitol challenge was 96% sensitive and 92% specific for EIB. (Holzer, et al. Am J Respir Crit Care Med 2003; 167:534-537.)

Differential Diagnosis
• Poorly controlled asthma
• Poor conditioning
• Vocal cord dysfunction
• Cardiac disease

Vocal Cord Dysfunction

Exercise-associated respiratory symptoms
Symptoms FOLLOWING exerciseSymptoms DURING exercise
Undiagnosed or poorly controlled asthma
Further history, exam, spirometry
Classification of severity, selection of appropriate therapy, patient
education
Follow-up 6-8 weeks
Presumptive diagnosis of EIB
Further history, exam, spirometry
Prophylaxis with -agonist
Optimal Response Suboptimal Response
Exercise/EH Challenge
Normal
Reconsider Dx, Reassess
Abnormal
Escalate therapy

Prevention
• Careful sport selection– Low minute ventilation/warm humid conditions
• Simple Measures• Prophylactic pharmacologic therapy
-agonists– Inhaled anti-inflammatories: Cromolyn, Nedocromil,
steroids– LABA– LTRA
• Induction of refractory period

Simple Preventive Measures
• Improve physical conditioning
• Exercise in warm humidified environment
• In cold weather cover mouth/nose with scarf or mask
• Gradually decrease intensity of exercise at end of work-out
• Avoid aeroallergens, pollutants

Therapeutic Sequence
• Simple Measures-agonists
• Inhaled corticosteroids
• Inhaled long-acting -agonists
• Ipratropium or leukotriene receptor antagonists
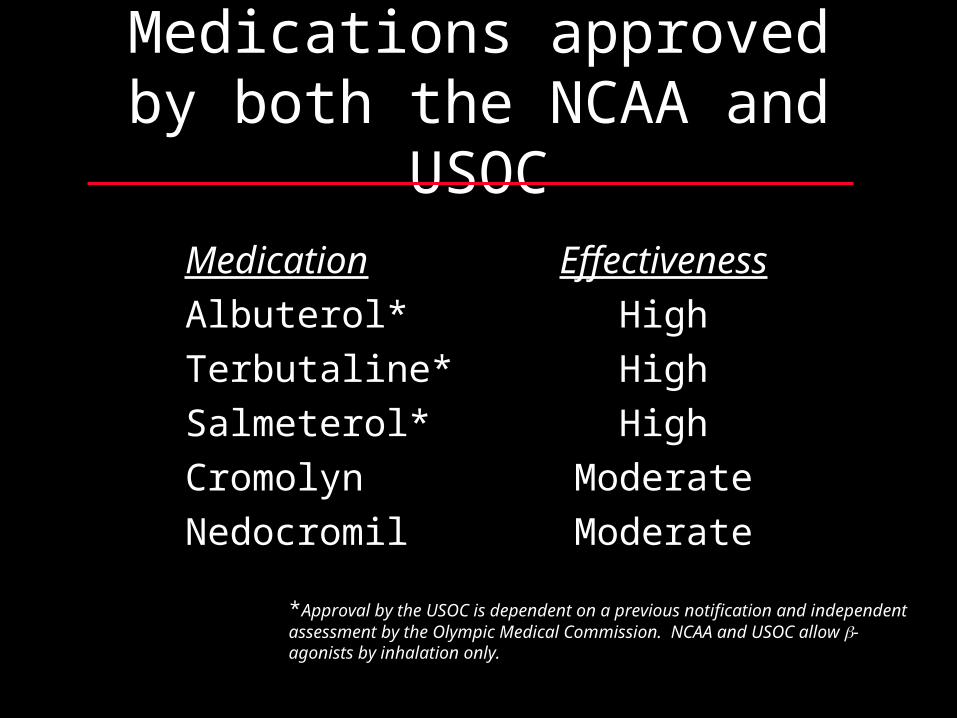
Medications approved by both the NCAA and USOC
Medication Effectiveness
Albuterol* High
Terbutaline* High
Salmeterol* High
Cromolyn Moderate
Nedocromil Moderate
*Approval by the USOC is dependent on a previous notification and independent assessment by the Olympic Medical Commission. NCAA and USOC allow -agonists by inhalation only.
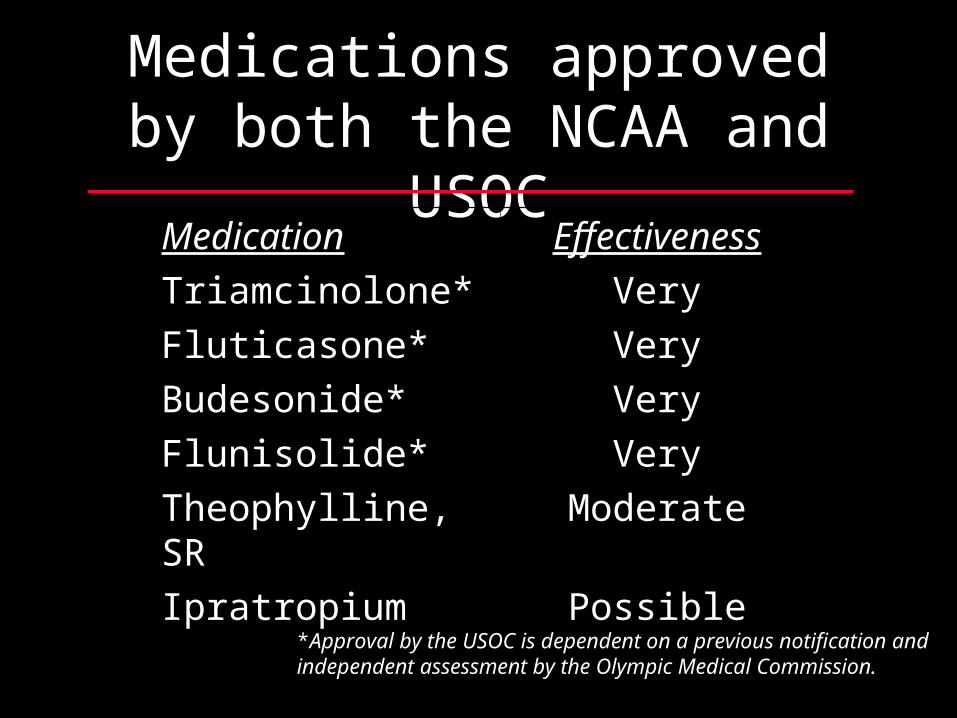
Medications approved by both the NCAA and USOC
Medication Effectiveness
Triamcinolone* Very
Fluticasone* Very
Budesonide* Very
Flunisolide* Very
Theophylline, SR Moderate
Ipratropium Possible
*Approval by the USOC is dependent on a previous notification and independent assessment by the Olympic Medical Commission.

Alternative Medicine Approaches
• Omega-3 fatty acid supplementation» Mickleborough, et al. Am J Respir Crit Care Med
2003; 168:1181-1189.
• Buteyko Breathing Technique - relaxation?» Bowler, et al. Med J Australia. 1998; 169:575-578.» Cooper, et al. Thorax 2003; 58:674-679
May there never develop in me the notion that my education is complete, but give me the strength and leisure and zeal continually to enlarge my knowledge.
Maimonides





























