Embed Size (px)
Citation preview

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
WHCA Spring 2015WI Medicaid CMI Changes
5343 North 118th CourtMilwaukee WI 53225414 476 1112 fax 414 476 6118www.specializedmed.com
The materials contained herein include information and facts and the opinions and recommendations of
Specialized Medical Services, Inc. (SMS) regarding governmental regulations, statutes and practices, and potential changes to same. Notwithstanding anything to the contrary stated or implied in any of the
materials available herein, SMS and its employees cannot and do not make any representation, warranty, endorsement or guarantee, express or implied, regarding (I) the accuracy, completeness or
timeliness of any such information, facts or opinions or (ii) the merchantability or fitness for any particular purpose thereof, nor shall any of such materials be
deemed the giving of legal advice by SMS or its employees. All participants should consult their own legal advisors, applicable regulatory entities and other sources of legal information and advice for any
opinions or recommendations with respect to their own legal situation. Neither SMS nor its employees shall be liable to you or any other person or entity for any loss or injury or any direct, indirect, incidental, consequential, special, punitive or similar damages,
or any other damages of any nature whatsoever, arising out of any of the materials (or any portion thereof) contained or not contained herein.
BY ATTENDING THIS SEMINAR, YOU HEREBY WAIVE ANY AND ALL CLAIMS AGAINST SMS AND ITS EMPLOYEES ARISING OUT OF YOUR USE OF THE INFORMATION CONTAINED
HEREIN.We have provided URL addresses to Internet sites maintained by third parties. Neither SMS nor its
employees operates or controls in any respect any information, products or services on these sites, or endorses or makes any representation or warranty regarding these sites.
You assume total responsibility and risk for your use of these third party sites.
Specialized Medical Services, Inc.5343 North 118th Court
Milwaukee, WI 53225 414-476-1112 fax 414-476-6118
email: [email protected]
1

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Presenter: Theresa Lang, RN, BSN, WCCVice President Clinical ConsultingSMS for 19 yearsOver 30 years LTC experienceAHIMA ICD-10 Approved TrainerAreas of Expertise
Clinical Operations and Training Medicare MDS Wound Care
RUG 48 Calculation Changes:Impact on Facility ReimbursementEffective 7/1/2104
CMI Basics
MDS 3.0 uses 108 items to calculate a RUG 44 score
The ARD (Assessment Reference Date) determines how the assessment is used in the revised Medicaid formula
Picture Quarter vs Picture DatePicture Quarter Data Available as
of Date:Rate Effective
Date
Oct - Dec 2013 June 30, 2014 July 1, 2014
Jan - Mar 2014 Aug 31, 2014 Oct 1, 2014
Apr - Jun 2014 Nov 30, 2014 Jan 1, 2015
Jul - Sep 2014 Feb 28, 2015 Apr 1, 2015
Which MDSs are included The assessment for each resident that is
RUG-able, dated on or before the last day of the quarter, and correctly included in the WI MDS database by the “as of date” will determine the case mix grouping for that resident for that quarter.
New admissions will not be included in the CMI unless they have received a RUG-able MDS assessment on or before the last day of the quarter.
Which MDSs are included
Re-entries will be included in the CMI with their last valid RUG classification from their prior stay, if they were discharged “with return expected” and actually returned the facility, if there is no more recent valid RUG classification.
2

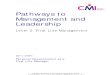
RUG IV 48 Classification System WI MedicaidCMI Index Maximized
ExtensiveServices
ES33.00
ES22.23
ES12.22
Special CareHigh
ADL
SpecialCare Low
LE2 1.61LD2 1.54
LC2 1.30
LB2 1.21
LE1 1.26LD1 1.21
ClinicallyComplex
ADL
Depresed
BehaviorSX
Cognition
ADL
ADL
BB2 .81
BA2 .58BB1 .75
BA1 .53
2-5
2-5
0-1
0-1
ADL
Nursing Rehab
Nursing Rehab
Nursing Rehab
Nursing Rehab
Nursing Rehab
PE2 1.25
PE1 .17PD2 1.15
PD1 1.06
PC2 .91PC1 .85
PB2 .70
PB1 .65PA2 .49
PA1 .45
2+ 0-1
2+
2+ 0-1
2+ 0-1
2+ 0-1
15-1
6
11-146-102-5
0-1
0-1
Specialized Medical Services, Inc.5343 North 118th CourtMilwaukee WI 53225
414 476 1112 fax 414 476 6118Copyright 10/2010
Ventilator, Trach,Medical Isolation
Rehabiliation ADL
RAD 1.58
RAC 1.36
RAB 1.10
RAA.82
ReducedPhysical
Functioning
RAE 1.65
ADL
Depressed
NotDepressed
HE2 1.88HD2 1.69
HC2 1.57
HB2 1.55HE1 1.47
HD1 1.33
HC1 1.23
HB1 1.22
Rest. Nsg 2+
Rest. Nsg 0-1
ADL
NotDepressed
Depressed
LC1 1.02
LB1 .95
15-1
6
11-146-10
ADL
2-5
0-1
15-1611-14
6-102-5
15-16
6-1011-14
15-16
2-56-10
11-14
2-5
15-1611-14
6-102-5
ADL
NotDepressed
CD2 1.29CE2 1.39
CC2 1.08
CB2 .95
CA2 .73
15-16 11-146-10
2-50-1CE1 1.25
CD1 1.15CC1 .96
CB1 .85CA1 .65
15-1611-14
6-102-5
0-1
3

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Which MDSs are included
A RUG-able MDS assessment includes:Admission Assessments,
Annual Assessments,
Quarterly Review Assessments,
Medicare Assessments,
Significant Change in Status MDS, and Significant Correction to Prior Comprehensive MDS Assessments.
Which MDSs are included
The average quarterly CMI for the facility shall include all valid RUGS scores, which may include multiple distinct RUGS scores for an individual resident, subject to the limitations described above.
Medicaid CMI for entire quarter vs. "picture date"
Picture Date
6/30/2014MDS closest to the
picture date is used
Example 4/15/14 RAB 1.10
6/1/14 PA1 .45
The PA 1 would be used
Picture Quarter
Effective 7/1/2014 All MDSs during the 3
month window will be averaged by days
Example: RAB 1.10 x 47 days
PA1 .45 x 30 days
51.7 + 13.5 = 65.2
65.2/77 = .8767
CMI to Dollars
Every .01 in the CMI is equal to $.85 to $1.05
60 Medicaid residents at .85 per day $51 a day
$4590 per 90 day quarter
60 Medicaid residents at .85 per day with a .04 increase$204 a day
$ 18,360 per 90 day quarter
Impact of the ARD Medicaid CMI calculations are based on
the MDS ARD
The ARD determines the # of days of a given CMIExample:
April 1 ARD- with not additional MDS
RUG CMI of the 4/1 MDS will be used for 91 days
Impact of the ARD Days in SNF prior to the ARD will not be
used in calculating the CMI
ExampleResident is admitted on 4/1/2015
First MDS ARD is 4/10/15
81 days will be used to calculate the CMI
Example:Resident is sent to hospital on 3/28/15
Readmitted to SNF on 4/4/15
4/1 to next MDS CMI will be based on
last MDS in prior quarter
4

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Should we not do all MDS on day 1? NO- you will have insufficient data to
complete the MDS and a low RUG score
Example:ARD 4/1/15 RUG Score CC1 CMI: .96
90 days at .96
ARD 4/10/15 RUG Score RAB CMI 1.10 80 days at 1.10
Identify Strategies for calculating Medicaid CMI for entire quarter vs. "picture date"
Watch MDSs due in the first 1-2 weeks of January, April, July, October
Would it benefit for the quarterly MDS to be done “early”? In the prior quarter
Watch Individual MDS CMI
If RUG is going to go down:Set ARD as close to day 92 or 366 as
possible
If RUG is going to go upSet ARD as soon as it the change is identified
MDS Schedule Requirements
OBRA Requirements
First MDS ARD must be on/before the 14th
day of admission
Then quarterly MDS at least every 92 days
Annual assessment at least every 366 days
MDS scheduling is based on ARD
Early Quarterly: Example 1
10/15/14 RAB 1.10
12/1/14 CC1 .96
Quarterly MDS needs an ARD no later than 1/5/2015 done 12/20
RUG will drop to PC1 .85
October 16 days at 1.10
November 30 days at 1.10
December 19 days at .96
December 12 days at .85
CMI: 1.0278
Example 2 10/15/14 RAB 1.10
12/1/14 CC1 .96
12/31/14 Picture quarter this resident will be a 1.03
At $.85 x 90 day
$76.50 for the quarter
Quarterly
Quarter July- September
5/20/14 PB1 .65
8/1/14 CC2 1.08
The 5/20 MDS is used to calculate the first 31 days of July
July: 31 days at .65 = 20.15
August/September: 62 days at 1.08 = 66.96
Quarter CMI 87.11 or .9468
5

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Early Quarterly
Quarter July - September
5/20/14 PB1 .65
7/15/14 CC2 1.08
July 1 to July 14: 14 days at .65 = 9.1
July 15 to September 30:78 days at 1.08 = 84.24
Quarterly CMI: 93.34/92= 1.0145
Calculating CMI Daily
Yes it can be done but it may not be a reflection on your quarterly CMI scoreWhy: Residents in house today may not have
a claim submitted in September 2015
If daily CMI is calculated remember If the resident will be used in the quarterly
sample
All days in the quarter will be averaged
Watch for Significant Change in Status Assessment MDS Criteria Improvement or decline in 2 or more areas
Will not improve with normal interventions
UTI, Pneumonia, etc. are not reason to do SCSA- as they are expected to improve-IF THEY DO NOT then a SCSA would be appropriate
Watch for Significant Change in Status Assessment MDS Criteria Improvement or decline in 2 or more areas
Will not improve with normal interventions
Resident has declined in ADL- therapy is started
If a SCSA is done due to the decline- then another would be indicated when therapy ends
Watch for Significant Change in Status Assessment MDS Criteria:When a resident is in therapy and improving
SCSA are not required as long a process is being made
SCSA is required when the resident reaches his/her maximum potential
Key Factors
MDS staff must know and understandCMI and how CMI’s are calculated
Ability to estimate a CMI without doing an MDS
Impact of ARD selection on quarterly CMI calculation
“Early” quarterlies if RUG/CMI is going up
IF RUG/CMI is decreasing – set ARD as close to 92 or 366 days as possible
6

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Key Factors
Facilities that do quarterly MDS every 70-77 or 84 days may have more MDS to averageWIN SOME- LOSE SOME
Behavior Incentive
Only MDS 10/1/2010 or after are included
Behavioral Incentive: MDS 3.0 and ICD -9 Codes Incentive is based on:MDS scoring
Diagnosis database (CHRSA) SNF claims
Physicians claims
Does your Medicaid claim reflect a mental health/cognitive diagnosis?290.00 to 331.00
Portal only requires 2 diagnosis
18 are allowed
3.657 Behavioral/Cognitive Impairment (BEHCI) Access and Improvement Incentives
The funding available for the SFY2015 BEHCI Incentive will be distributed as two incentives. Each is 50%Access Incentive
Improvement Incentive
5.460 Behavior/Cognitive Impairment Incentives The Behavior/Cognitive Impairment
Access Incentive Base Rate is $0.380
The Behavior/Cognitive Impairment Improvement Incentive Base Rate is $0.369
3.657 Behavioral/Cognitive Impairment (BEHCI) Access and Improvement Incentives The Department will apply two scores, an Access Score
and an Improvement Score, to each resident based on values defined by:
The MDS elements listed in section 5.971; and
Acuity categories ranging from 0 to 5 based upon psychiatric and related diagnosis codes under the International Classification of Diseases, version 9 (ICD-9), as organized via decision rules promulgated under the nationally-recognized Chronic Illness and Disability Payment System (CDPS).
7

TN #14-019 -65- Supersedes Attachment 4.19-D TN #13-015 Approval Date Effective Date 7-1-14
5.971 BEHCI – MDS Behavioral Score VARIABLE MDS 3 CODE BEHAVIORAL SCORE WEIGHT WANDERING: E0900 Wandering Presence & Frequency 1 .4 2 .8 3 1.2 E01000A Wandering Impact 1 1.5 E01000B Wandering Impact 1 1.5 BEHAVIOR SYMPTOMS: E0200A Physical directed toward others 1 .6 2 1.2 3 1.8 E0200B Verbal directed toward others 1 .6 2 1.2 3 1.8 E0200C Other symptoms 1 .6 2 1.2 3 1.8 E0500A Risk of physical injury 1 1.5 E0500B Interferes with care 1 .75 E0500C Interferes with activities 1 1.5 E0600A Others at risk 1 1.5 E0600B Intrudes on others 1 .75 E0600C Disrupts care 1 .75 E0800 Rejects care 1 .6 2 1.2 3 1.8 SEVERITY SCORE: D0300 Resident Mood Interview 15 or greater 1.5 D0600 Staff Assessment of Mood 15 or greater 1.5 LOCOMOTION: G0110E Resident movement 0 1.0 1 .75 2 .75
8

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
WI Behavior Index The BEHCI Access and Improvement Scores
are based on index values aggregated at the facility level, calculated using data available for Title 19 FFS Non-DD residents present in the facility on the last day of the second quarter of the fiscal year (December 31, 2013) that also had a RUGable MDS assessment on or prior to that date.
The BEHCI Access and Improvement Scores are only calculated for individuals when they have both a RUGable MDS assessment and a CDPS score greater than zero.
BEHCI Access Incentive
The Access Score for each resident is calculated by subtracting 1.00 from the higher of the resident’s first two available MDS Behavioral Scores and setting any negative results to zero.
The first and second MDS behavioral scores are defined as the resident’s first and second scores after whichever of the following Starter Events occurred most recently:.
BEHCI Access Incentive
Starter EventsAdmission to the facility;
A change in the PopID;
A break in stay of more than 30 days;
October 1, 2010.
The BEHCI Access Incentive is determined by multiplying the BEHCI Access Score by the BEHCI Access Base Rate in Section 5.460.
BEHCI Improvement Incentive
The Improvement Score for each resident is calculated using the six most recent RUGable MDS Behavioral Scores since the Starter Event determined for the BEHCI Access Incentive.
If fewer than six RUGable MDS Behavior Scores exist, all available scores are used.
BEHCI Improvement Incentive First, an Improvement Baseline is set.
If the Starter Event occurred far enough in the past that the resident has more than six available MDS Behavioral Scores, the Improvement Baseline is set to the fifth most recent MDS Behavioral Score.
If six or fewer MDS Behavioral Scores are available, the Improvement Baseline is set to the greater of the two earliest available MDS Behavioral Scores.
BEHCI Improvement Incentive Next, the Improvement Score is
determined by a) calculating the change from the
Improvement Baseline to the average of the MDS Behavioral Scores that remain after excluding the two earliest MDS Behavioral Scores;
b) setting negative results to zero; and
c) multiplying the calculated change by a CDPS factor ranging from zero to five.
9

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
BEHCI Improvement Incentive The CDPS factor is the CDPS score that
the individual had on the date of the MDS Behavioral Score used for the BEHCI Access Incentive.
The BEHCI Improvement Incentive is calculated by multiplying the Improvement Score by the BEHCI Improvement Base Rate in Section 5.460.
Behavior Incentive Must have at least 3 MDS in the database
First 2 MDS are used as the base
Remaining MDS up to 4 (average) are used to determine improvement
CDPS Score has to be greater than 1 but can be no greater than 5
Behavior IncentiveMany facilities will loss behavior incentive
How to get it backDiagnosis on the Medicaid Claims
Accurate MDS CodingTracking target behaviors
Changing target behaviors
Role of the MDS in CMI calculation
MDS Scoring Hot Spots for Medicaid Reimbursement
Restorative Nursing .04 to .08 CMI increase
Respiratory TherapyTrained nurses
Capture minutes
Documentation
Isolation (overcoming)
Part B therapy – Section O
Evaluating your CMI
Quarterly Review the CMI listing found in the rate notice
Look at the following areas
10

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Report Changes
Picture Quarter is a date rangeAdj T19 Inhouse Res Count: is patient days
Report Changes
Review Line 51:This is the # of days that there is not an RUG score available for such as new admissions up to the ARD for the first MDS
Most facilities will have a number in this field- previously the goal was 0
Extensive Services
Do you have residents that really meet this criteria? Isolation, Trach, Vent
Isolation is a 14 day look-back may conflict with MDS Section G coding
What do the nurses say about the isolation?Does it specify day started and ended
Do weekly or daily notes contradict
Rehabilitation
This should be an indicator of the # of residents who are receiving Part B therapy
If you have no residents in this category ask? Is therapy getting the quarterly MDS
Schedule?
Are SCSA MDSs being done?
Does therapy begin after the MDS is completed not before?
11

Picture Qtr = Census Apr - Jun 2014
134 1334
69 327 48 56
PC1 Pt2 PD1 PD PEi PE2
0.85 0.91 1.06 1.15 1.17 1.25
29 13 8 0
31.90 17.68 12.64 0.00
' v v' RAB RAC RAD RAE
1.10 1.36 1.58 1.65
1.1'1
CONFIDENTIAL! Per HIPAA regulations this information is deemed confidential and not f
. . . POP-ID:
1 BA1 2 BA2 3 BB1 4 BB2 5 CA1 0.65 6 w CA2 0.73 7 CB1 0.85 8 CB2 0.95 9 CC1 0.96 10 CC2 1.08 11 CD1 1.15 12 CD2 1.29 13 CE1 1.25 14 CE2 1.39 15 ES1 2.22 16 ES2 2.23 17 ES3 3.00 el. 18 HB1 1.22 19 HB2 1.55 20 HCi 1.23 21 FIC2 1.57 22 HD1 1.33 23 HD2 1.69 24 HE1 1.47 25 HE2 1.88 26
a■Trrjr.
27 28 29 LO2 1.30 30 'Di 1.21 31 LD2 1.54 32 Lei 1.26 33 00,„ LE2 1.61 34 PA1 0.45 35 PA2 0.49 36 PB1 0.65 37 PB2 0.70 38 39 40 41 42 43 44 45 46 47 48
0.53 0.58 0.75 0.81
LB2 LC1
1.21 1.02
AlsololaWalfilirt
O 8.00
161 1305
0 0.00
300 288.00
0 0.00
48 55.20
0 0.00
99 123.75 O 0.00
U.00
0 0.00 O 0.00
'616 U. O 0.00
197 242.31 O 0.00
0 0.00 O 0.00
83 122.01
0 0.00
0 0.00
239 243.78
0 0.00
7 8.47
0 0.00
8 10.08
0 0.00 iU.DU
0 0.00
91 59.15 93 ' t 65.10
113.90 1,213.94
73.14 76.05 56.16 70.60(;
j: 19 .01100030C owht0.0.
85 45.05 0 0.00
226 169.50 193 156.33 Til U5.15
49 Non-DD In House
4,128 3883.69
50 Non-DD Bedhold
na
51 w/o RUGable MDS
6
52 Total Non-DD
4,134
53 NonDD_T19_RUGCMI
Line 53 (Weighted /Pds) 3883.69 / 41.408IR
To page 4, line 9
BNHS - Rate1_012015FinalvlAsm
CONFIDENTIAL! Per HIPAA regulations this information is deemed confidential and not
Cognition and Behavior
Clinically Complex
Extensive Services
Special Care High
Special Care Low
Reduced Physical Functioning
Rehab
12

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Special Care High
Is respiratory therapy being coded on the MDS?
Why are residents sleeping with HOB elevated? Does it relate to diagnosis (Asthma/COPD) and
SOB?
Enteral Calorie requirements>26% of calories
>501 cc of fluid
Respiratory Therapy
Trained nurses or RT’s
Actual minutes spent with resident
Nebulizer count- inhalers do not
Pre-Post treatment assessment counts
Definition is in Appendix A of the RAI Manual
Services that are provided by a qualified professional (respiratory therapists, respiratory nurse).
Respiratory therapy services are for the assessment, treatment, and monitoring of patients with deficiencies or abnormalities of pulmonary function.
Respiratory therapy services include coughing, deep breathing, heated nebulizers, aerosol treatments, assessing breath sounds and mechanical ventilation, etc., which must be provided by a respiratory therapist or trained respiratory nurse.
A respiratory nurse must be proficient in the modalities listed above either through formal nursing or specific training and may deliver these modalities as allowed under the state Nurse Practice Act and under applicable state laws.
Cannot count- nebulizer treatments done by med techs. Nurse must do pre-post assessments
Special Care Low
13

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Do not focus on depression- near impossible to achieve
Skin alterations with 2 treatments
Parkinson's Disease 332.0 Paralysis Agitans
Clinically Complex
Chemotherapy
Oxygen
IV meds
Cognition and Behavior
ADL score is 5 or less
Are ADLs coded correctly- could they be 6 or higher
BIMS is 9 or less
CPS is 3 or more
Reduced Physical Functioning
14

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
How many PA, PB, PC, PD, PE end in a 2? Indicator of strength of restorative nursing
PA and PB residentsDo they have cognitive issues not reflected on
the MDS that would move to a BA or BB?
Is ADL Score is 5, 10, 14 is it correct?
ADL Scoring
Late Loss ADLsTransfers
Toileting
Eating
Bed Mobility
Are MDSs being coded accurately Is the Rule of 3 being applied correctly If not may result in underscoring
Is scoring being done on # of opportunities for an event versus # of shiftsTransfer- there may be 5 or more transfers in
a day
Are the Nursing Assistants charting frequency on every shift not just most dependent on a shift
Are MDSs being coded accurately 8 means it never occurred
7 means in happened 1-2 times in the past 7 days
Staff support is based on most dependence – even if only happened onceSoftware issue
Restorative Nursing
Key in Behavior/Cognition as well as Physically Reduced Functioning RUG categories
2 Restorative Programs
6 days a week
At least 5 minutes a day
Toileting programs are considered a restorative program
Implementation Steps
Establish a philosophyPrint on small cards- laminate- distribute-
CARRY THEM
Include concepts in orientation
Have philosophy imprinted on plaques- post in locations visible to visitors and staff
15

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Implementation Steps
Community education regarding long term care
Policies/ProceduresOrders
Physician Communication Educate Boards/Owners Train staff Add philosophy to admission packet
Implementation Steps
Reinforce restorative during administrative rounds
Develop themes that can be used on posters, stickers, buttons
Develop specific activities every month-HAVE FUN
Incorporate into QI processes
Implementing a Restorative Program TEACH-TEACH-TEACHNurses
Therapists
Aides
Physicians
Administration
All departments
Implementing a Restorative Program TEACH-TEACH-TEACH CONTENTAccurate assessments
Hands on- patient content Not a nurse in an office ADL Scoring- actual ability
MDS Coordinator is a clinical leaderBe enthused about the MDS
Appreciate the tools it provides Instill ownership and confidence in the process
Implementing a Restorative Program TEACHMDS is not paper compliance
Standardize assessment procedures- reduce paperwork Standards of care versus Care Plans
Maximize skilled therapy Coverage days/times
Flexible ARD’s
Implementing a Restorative Program TEACH
Teach physicians Role of rehab versus maintenance programs
How to write orders
How to write progress notes which support skilled services
If physicians are a problem What is the role of the medical director?
Consider establishment of a credentialing process which affects admitting privileges
16

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Implementing a Restorative Program Policies and ProceduresRAI/MDS
Scheduling- notification
Diagram the process Section responsibility
How is data obtained over 24 hours
Implementing a Restorative Program Nursing Assistants
How are NA’s assigned Consistent assignments with flexibility
Frequent change Unreliable data from the NA’s
More difficult to instill accountability
Documentation THINK MINUTES
Nursing
Rehab
Implementing
It takes time and perseverance If staff are not excited and enthused the program is
mediocre and is a paper compliance tool only
Don’t expect 100% immediately Cooperation and understanding will not happen at the
same time for all employees
Walk the talk DON/Administrator do rounds together
Why Programs Fail
Failure to realize that successful implementation of the program entails extensive interdisciplinary planning and work with the mistaken belief that the restorative nurse coordinator can implement the program independently
Lip service from the administrator/DON, showing no real support or belief
Why Programs Fail
Failure to make training mandatory Lack of a concrete plan to present initial
training Lack of team approach- “It is a nursing
program” Assignment of duties(responsibility) but
lack of time and authority to make it happen
Why Programs Fail
If rehab aides are usedReassignment to NA duties
Not 7 days per week
Not at least 12 hours per day
17

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
The Restorative Aide
SkillsPatienceSlow movementsGood communication skillsPersuasive skillsAbility to documentAbility to identify changeWillingness to interact with families
The Restorative Aide
SelectionLong versus new NA’s
Willingness to change
Enthusiasm
The Restorative Aide
TrainingADL techniques
Promoting self-involvement
Continuous/On-going Patient specific
The Restorative Aide
MentoringCharacteristics of Mentoring
Role modeling Role clarification Role rehearsal
Advantages of Mentoring Gradual integration of a new philosophy Improved career ladder Increases interdisciplinary collaboration
Why Programs Flounder
Personnel problems do not disappear-they get worse and compound
Rounds and monitoring is need to assure strong reliable personnel remain that way
10% of your employees take 80% of your time
Why Programs Flounder
Staff watch the actions of administration-they see how you really feel even if you do not say it
Speak the language of the staff Laissez-faire is not a form of management Shift reports are a way to monitoring
progress
18

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Why Programs Flounder
Inconsistent rounds by management Not telling staff what is expected of them Inability to diagnosis the cause of a
situation as Process/SystemPerformanceEducational
Why Programs Flounder
Nurses who refuse to accept supervision duties and responsibilities
Inconsistent meetings and progress reports
Lack of accountability and authority
Inconsistent and unequal treatment of staff
Why Programs Flounder
Outdated job descriptions
Policies and procedures which are not current
Restorative is a day shift only program
Restorative is a second priority
Lack of respect for management/ leadership
Nurses do not know how to make rounds to supervise the work of the NA’s
Program Success
Orientation to new and existing staff
Involvement of all departments
Participation in communication
Utilization of the care plan
Utilizing novel approachesHumor
Themes
Program Success
Maintaining interest and enthusiasm
Track progress monthlyBe proud of the progress
Report the progress
Program Evaluation
MDS Validity
Restorative Nursing CQI Tool
QMPhysical Functioning Domain
Late Loss ADL Decline
Incidence of Decline in ROM
19

WI Medicaid CMI Changes 4-2015All materials are copyrighted. Copying and redistribution of these materials in
any means including print or electronic is a violation of copyright laws.
5343 North 118th Court Milwaukee WI 53225414 476 1112 fax 414 476 6118
www.specializedmed.com
Program Evaluation
Charge Nurses/Care Plan CoordinatorsUse QI/QM’s when care planning
Administration/DONUse QI’s as basis for quality rounds
All department managersUse QI/QM’s as basis for weekly rounds
20

©Specialized Medical Services, Inc. 5343 North 118th Court Milwaukee, WI 53225 414-476-1112 fax 414-476-6118 www.specializedmed.com 3/10/2015 1
RUG 44 Estimator This assessment can be used to estimate the RUG 44 used for Medicaid Reimbursement .
REHABILITATION RAE: ADL score 15-6 5 days or more (15 min per day minimum) in any combination of SLP,OT or PT in last 7
days AND 150 minutes or greater in any combination of SLP, OT, or PT in last 7 days OR
3 days or more (15 min per day minimum) in any combination of SLP, OT, or PT in last 7 days AND 45 minutes or greater in any combination of SLP, OT, or in last 7 days AND
at least 2 nursing rehabilitation services (see details on Page 2)
RAD: ADL Score 11-4 RAC: ADL Score 6-10 RAB: ADL Score 2-5 RAA: ADL Score 0-1
Extensive Care (ADL Score 2-16) Will the resident be receiving these services in the SNF? Tracheostomy care AND ventilator/respiratory ES3 Tracheostomy care OR ventilator/respiratory ES2 Infection isolation ES1
Special Care HIGH (End Split with/without depression) HBx-HEx Depression Criteria Total Severity Score >= 10
Coma and ADL dependent COPD and SOB while lying flat Septicemia Fever with one of the following:
- pneumonia - weight loss - vomiting - feeding tube* Diabetes with daily injections (7) and insulin order changes (2) Parenteral/IV feedings (within 7 days- can be prior to
admission) Quadriplegia and ADL score >= 5 Respiratory Therapy (7 days) * 51% or more of total calories OR 26% to 50% of total calories and 501cc fluid intake per day
Special Care LOW (with/without depression) LBx-LEx Depression Criteria Total Severity Score >= 10
Cerebral Palsy and ADL >= 5 Stage 3 or 4 pressure ulcers with 2+ ulcer treatments Multiple Sclerosis and ADL >=5 Stage 2 pressure ulcer (1) and venous/arterial ulcer (1) with 2 +
ulcer treatments Parkinson’s Disease and ADL >=5 Foot infection, diabetic foot, or other open lesion of foot with
dressing Respiratory Failure and Oxygen Radiation while a resident Feeding Tube(see criteria special care high) Dialysis while a resident 2+ Stage 2 pressure ulcers with 2+ ulcer treatments 2+ venous ulcers with 2+ ulcer treatments
If the patients TOTAL ADL Score is 0-2 the patient will not qualify for Special Care although the patient will meet the criteria for Clinically complex.
Clinically Complex (with/without depression) CAx-CEx Resident with Extensive Services, Special Care High, or Special Care Low with ADL Score 0-1
Depression Criteria Total Severity Score >= 10 Pneumonia Chemotherapy while a resident Hemiplegia/hemiparesis and ADL >= 5 Oxygen Therapy while a resident Surgical wounds or open lesions with treatment IV medications while a resident Burns Transfusions while a resident
Behavioral Symptoms and Cognitive Performance BAx-BBx BIMS score of 9 or less AND an ADL score of 5 or less OR Defined as Impaired Cognition by the Cognitive Performance Scale AND an ADL score of 5 or less (See description of BIMS and Cognitive performance scale) ♦ Hallucinations [E0100A] ♦ Delusions [E0100B] ♦ Physical behavioral symptoms directed towards others (E0200A = 2 or 3) ♦ Verbal behavioral symptoms directed towards others (E0200B = 2 or 3) ♦ Other behavioral symptoms not directed towards others (E0200C = 2 or 3) ♦ Rejection of care (E0800 = 2 or 3) ♦ Wandering (E0900 = 2 or 3)
Reduced Physical Function PAx to PEx No Clinical Conditions Exist
21

©Specialized Medical Services, Inc. 5343 North 118th Court Milwaukee, WI 53225 414-476-1112 fax 414-476-6118 www.specializedmed.com 3/10/2015 2
DETERMINING ADL SCORE FOR RUG IV CLASSIFICATIONS ADL: Bed Mobility, Transfer and Toilet Use From the MDS Section G
ADL SCORING for Bed Mobility, Transfer and Toilet Use
MDS Item Self- Performance
Support RUG IV SCORE
If self performance equals ___
If support equals ___
RUG IV ADL SCORE IS
G1a: Bed Mobility -, 0 or 1, 7. or 8 Any # 0
G1b: Transfer 2 Any # 1
G1I: Toilet Use 3 -, 0, 1, or 2 2
4 -, 0, 1, or 2 3
3 or 4 3 4 TOTAL ADL SCORE FOR
Bed Mobility, Transfers and Toilet UseCannot exceed 12
EATING ADL SCORE MDS Item Self-
Performance Support Eating
Score RUGS SCORING FOR EATING
Eating If self perform-ance equals ___
If support equals ___
RUG III ADL SCORE IS
-, 0, 1, 2, 7, 8 -, 0, 1, or 8 0
TOTAL ADL EATING SCORECannot exceed 4
-, 0, 1, 2, 7, 8 2 or 3 2
3 or 4 -, o, or 1 2
3 2 or 3 3
4 2 or 3 4
TOTAL ADL AND EATING SCORE (0-16)
Restorative Nursing Programs 2 or more required to be provided 6 or more days a week for at least 15 minutes
Passive range of motion (O0500A) and/or Active range of motion (O0500B)* Bed mobility training (O0500D) and/or walking training (O0500F)* Splint or brace assistance ( O0500C) Transfer training (O0500E) Dressing and/or grooming training (O0500G) Eating and/or swallowing training (O0500H) Amputation/prosthesis (O0500I) Communication training (O0500J)
No count of days required for: Current toileting program or trial (H0200C) and/or Bowel toileting program (H0500)* * Count as one service even if both are provided
22