Embed Size (px)
Citation preview
6/20/2011
1
What’s New in Heart Failure
Dana McGlothlin, MDAssociate Professor of Medicine
Advanced Heart Failure and Transplant ProgramMedical Director, CCU
Disclosures
I have no relevant disclosures to reportI will discuss investigational and off-label therapies
A complex clinical syndrome that can result from an y structural or functional cardiac disorder that impa irs the ability of the ventricle to fill with or eject blood
Two main clinical types– Systolic HF (HFREF)– Diastolic HF (HFPEF)
Severity of clinical symptoms may vary substantiall y during course of the disease process and may not correlate with changes in underlying cardiac functi on
Definition of Heart Failure “Heart Failure” vs. “Congestive Heart Failure”
Because not all patients have volume overload atthe time of initial or subsequent evaluation, theterm “heart failure” is preferred over the older term “congestive heart failure”
6/20/2011
2
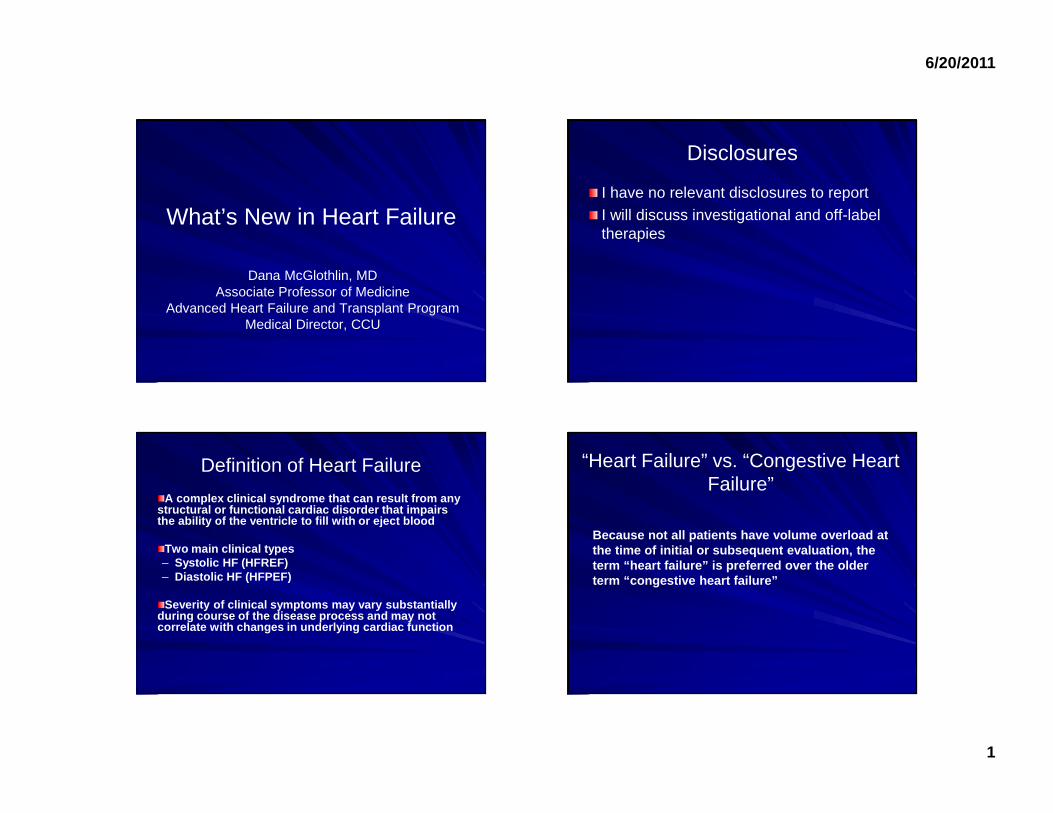
Heart Failure: Scope of the Problem
US prevalence*: 5.8 millionUS annual incidence: 670,000
Annual mortality: 282,754– 5-10% depending on severity
Cost: $39.2 billion– 53% of cost due to
hospitalization
Circulation 2010;121:e46-e215
1991 2001 2037
3.54.8
10.0
0
2
4
6
8
10
Pat
ient
s in
US
(mill
ions
)
0
15
%
50’s 60’s 70’s >80
HF increases with age
Rich M. J Am Geriatric Soc. 1997;45:968–974.Croft JB et al. J Am Geriatr Soc. 1997;45:270–275.AHA. Heart Disease and Stroke Statistics—2004 Update
Classification of Heart Failure
IV. Cardiac disease resulting in inability to carry out any physical activity without discomfort. Sx @ rest
III. Cardiac disease resulting in marked limitation of physical activity. Modest activity causes HF symptoms
II. Cardiac disease resulting in slight limitation of physical activity
I. Presence of cardiac disease without limitations on physical activity
NYHA Functional Classification of
HF2
D.Refractory heart failure requiring specialized interventions
C.Symptomatic heart failure; structural heart disease
B.Structural heart disease; high risk for developing heart failure
A.High risk for developing heart failure
ACC/AHA HF Stages 1
NYHA=New York Heart Association.
1. Hunt SA et al. Circulation. 2005;112:e154-e235.2. American Heart Association. Available at: http://www.americanheart.org. Accessed January 16, 2006.
Less severe Asymptomatic
Symptomatic at rest
More severe
Biomarkers in Heart Failure
Natriuretic PeptidesBrain natriuretic peptide (BNP) and NT pro-BNP are polypeptides secreted by the ventricles in response to excessive stretching of cardiomyocytes – BNP biological effects are vasodilation and natriuresis– NT pro-BNP is biologically inactive
BNP and NT pro-BNP equally effective in aiding the diagnosis of HF in patients with dyspnea presenting to the EDNT pro-BNP slightly better in detecting less severe cardiomyopathyBNP may be better at predicting 90 day adverse events than ED physician (REDHOT study)BNP and NT pro-BNP are strong predictors of mortality– Change in levels most predictive
Levels must be interpreted in the context of other clinical conditions and confoundersBNP analysis should be adjunctive and should not replace good clinical judgement
6/20/2011
3
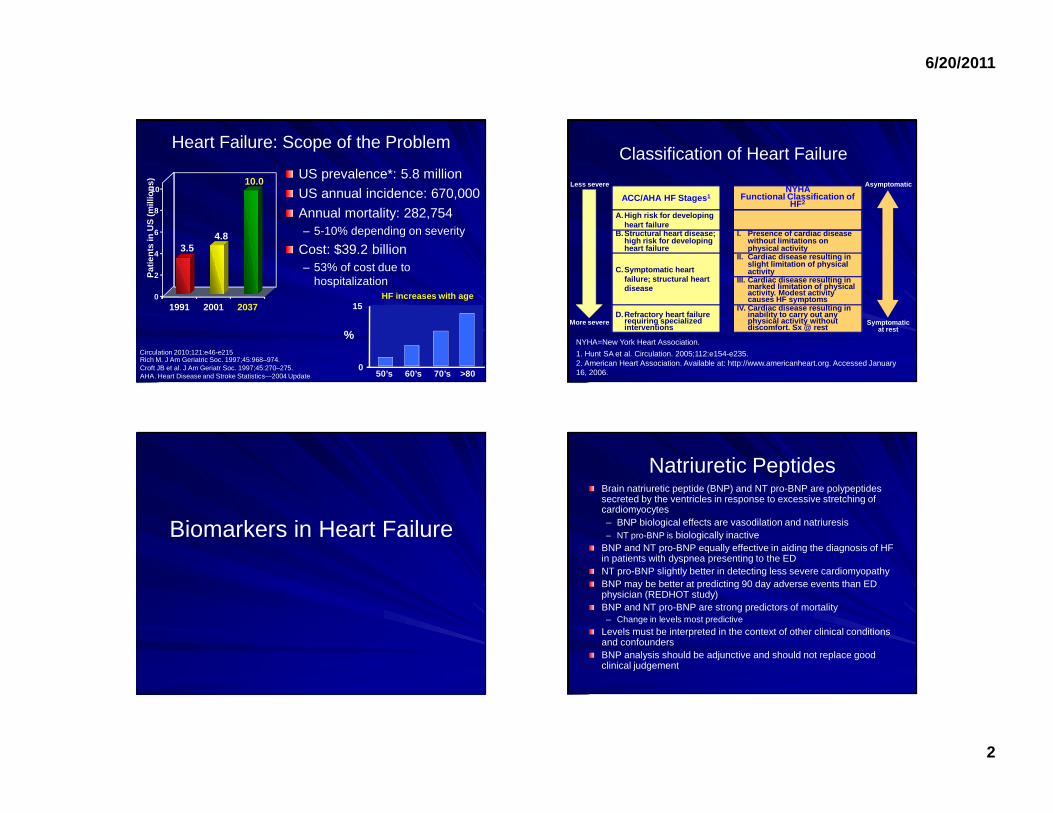
Galectin-3:New Biomarker for
Heart Failure
HF ACTION Sub-study
COACH Sub-study
Galectin-3 levels:Gal-3 is a lectin is a key mediator involved in myocardial fibrosis and remodelingGal-3 levels (ELISA) reflect underlying disease, NOT affected by acute decompensationGalectin-3 levels over 17.8 ng/mL are associated with an increased risk of adverse outcomesNOT to be used to monitor pharmacologic therapies for HFProvides independent and complementary information to BNP on the prognosis in patients with HFFDA approved, but not in guidelines yet
36.5%
6.9%
15.6%19.3%
Therapies for Chronic Heart Failure
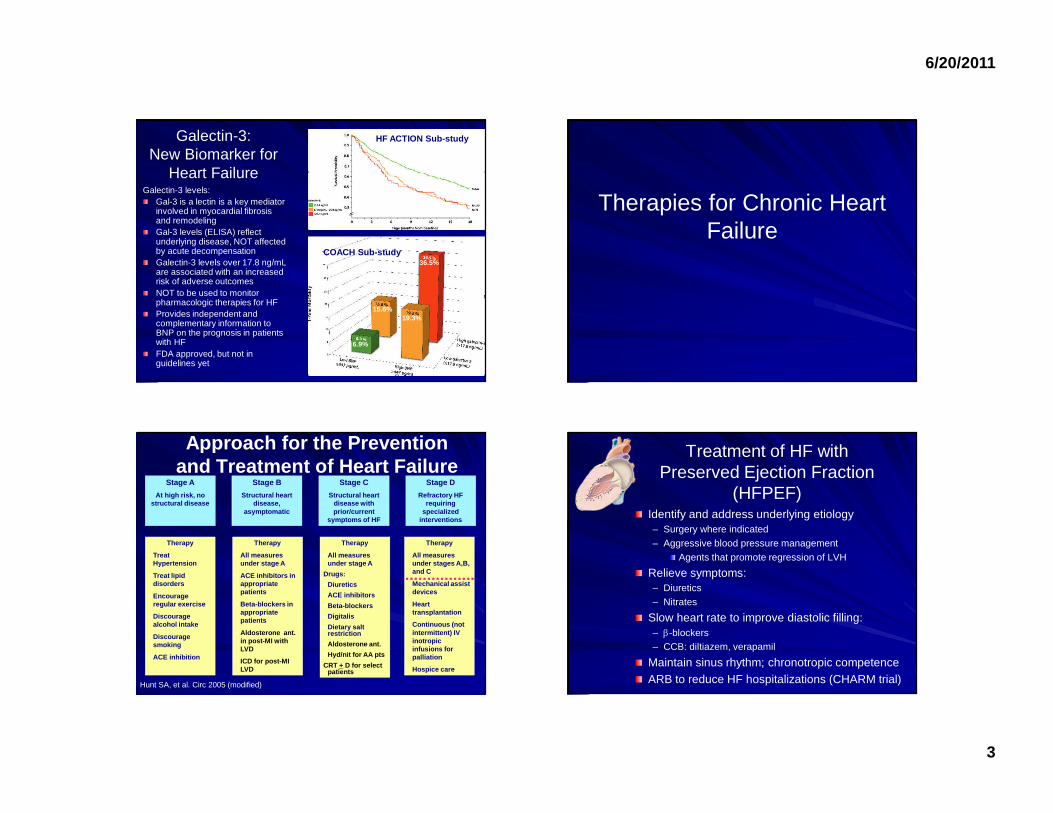
Approach for the Prevention and Treatment of Heart Failure
Stage A
At high risk, no structural disease
Stage B
Structural heart disease,
asymptomatic
Stage D
Refractory HF requiring
specialized interventions
Therapy
• Treat Hypertension
• Treat lipid disorders
• Encourage regular exercise
• Discourage alcohol intake
• Discourage smoking
• ACE inhibition
Therapy
• All measures under stage A
• ACE inhibitors in appropriate patients
• Beta-blockers in appropriate patients
• Aldosterone ant. in post-MI with LVD
• ICD for post-MI LVD
Therapy
• All measures under stage A
Drugs:
• Diuretics
• ACE inhibitors
• Beta-blockers
• Digitalis
• Dietary salt restriction
• Aldosterone ant.
• Hyd/nit for AA pts
CRT + D for select patients
Stage C
Structural heart disease with prior/current
symptoms of HF
Hunt SA, et al. Circ 2005 (modified)
Therapy
• All measures under stages A,B, and C
• Mechanical assist devices
• Heart transplantation
• Continuous (not intermittent) IV inotropic infusions for palliation
• Hospice care
Treatment of HF with Preserved Ejection Fraction
(HFPEF)Identify and address underlying etiology– Surgery where indicated– Aggressive blood pressure management
Agents that promote regression of LVH
Relieve symptoms:– Diuretics– Nitrates
Slow heart rate to improve diastolic filling:– β-blockers– CCB: diltiazem, verapamil
Maintain sinus rhythm; chronotropic competenceARB to reduce HF hospitalizations (CHARM trial)
6/20/2011
4
Audience Response Question32 y/o AA male with NIDCM, LV EF 30%, NYHA
FC II symptoms. Which HF therapy is not recommended in the current ACC/AHA guidelines?
Core
g S
pironola
ctone
Lis
inopr
il H
ydra
lazi
ne A
ll ar
e indi
ca...
8%9%
38%
42%
3%
A. CoregB. Spironolactone
C. Lisinopril
D. HydralazineE. All are indicated for this patient
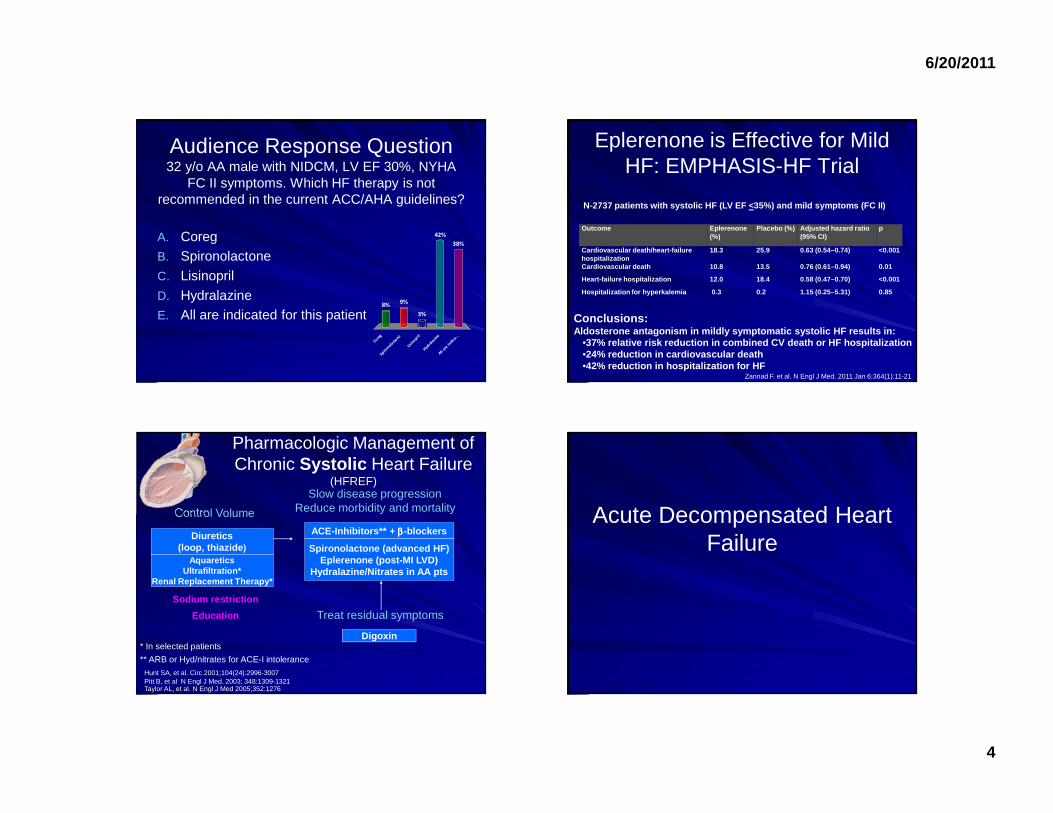
Eplerenone is Effective for Mild HF: EMPHASIS-HF Trial
Outcome Eplerenone (%)
Placebo (%) Adjusted hazard ratio (95% CI)
p
Cardiovascular death/heart-failure hospitalization
18.3 25.9 0.63 (0.54–0.74) <0.001
Cardiovascular death 10.8 13.5 0.76 (0.61–0.94) 0.01
Heart-failure hospitalization 12.0 18.4 0.58 (0.47–0.7 0) <0.001
Hospitalization for hyperkalemia 0.3 0.2 1.15 (0.25–5. 31) 0.85
•37% relative risk reduction in combined CV death or HF hospitalization•24% reduction in cardiovascular death•42% reduction in hospitalization for HF
Conclusions:Aldosterone antagonism in mildly symptomatic systol ic HF results in:
N-2737 patients with systolic HF (LV EF <35%) and m ild symptoms (FC II)
Zannad F. et al. N Engl J Med. 2011 Jan 6;364(1):11-21
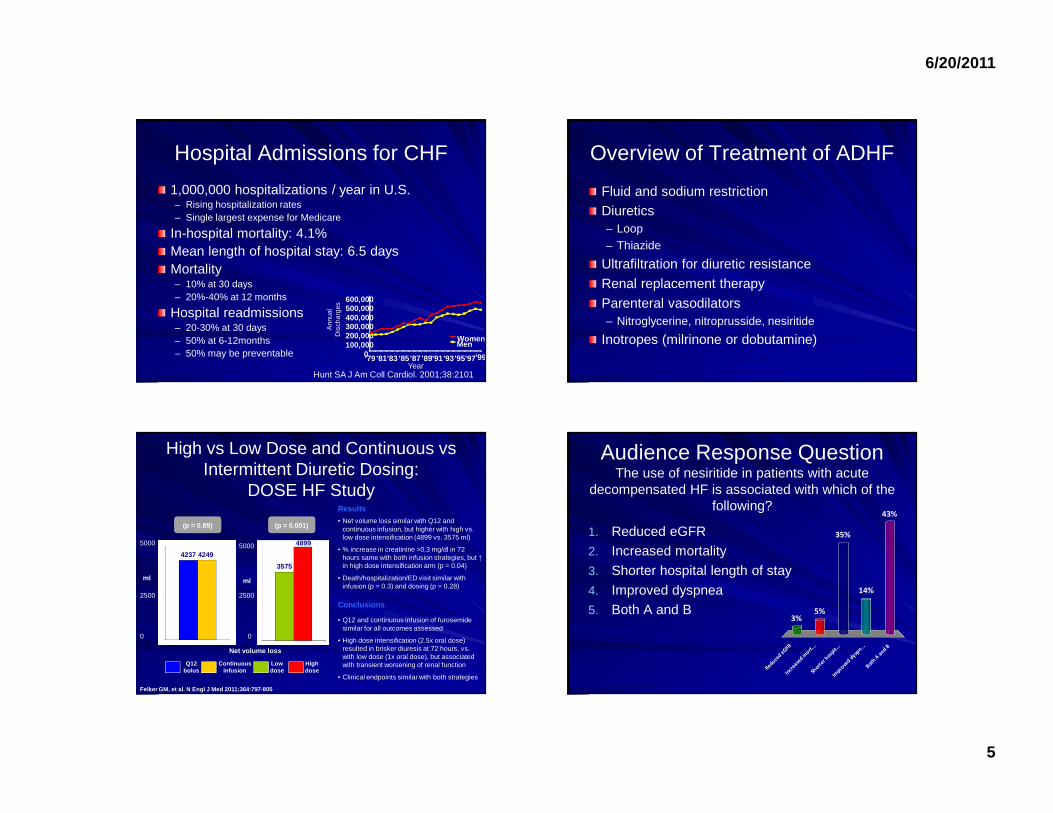
Pharmacologic Management of Chronic Systolic Heart Failure
(HFREF)
* In selected patients
** ARB or Hyd/nitrates for ACE-I intolerance
ACE-Inhibitors** + ββββ-blockers
Digoxin
Spironolactone (advanced HF)Eplerenone (post-MI LVD)
Hydralazine/Nitrates in AA pts
Control Volume
Slow disease progressionReduce morbidity and mortality
Treat residual symptoms
Diuretics(loop, thiazide )
Sodium restriction
Education
AquareticsUltrafiltration*
Renal Replacement Therapy*
Hunt SA, et al. Circ 2001;104(24):2996-3007Pitt B, et al N Engl J Med. 2003; 348:1309-1321Taylor AL, et al. N Engl J Med 2005;352:1276
Acute Decompensated Heart Failure
6/20/2011
5
Hospital Admissions for CHF
1,000,000 hospitalizations / year in U.S.– Rising hospitalization rates– Single largest expense for Medicare
In-hospital mortality: 4.1%Mean length of hospital stay: 6.5 daysMortality– 10% at 30 days– 20%-40% at 12 months
Hospital readmissions– 20-30% at 30 days– 50% at 6-12months– 50% may be preventable
Hunt SA J Am Coll Cardiol. 2001;38:2101
Ann
ual
Dis
char
ges
Year'990
100,000200,000300,000400,000500,000600,000
'79 '81'83 '85'87 '89'91'93'95'97
WomenMen
Overview of Treatment of ADHF
Fluid and sodium restrictionDiuretics– Loop– Thiazide
Ultrafiltration for diuretic resistance
Renal replacement therapy
Parenteral vasodilators– Nitroglycerine, nitroprusside, nesiritide
Inotropes (milrinone or dobutamine)
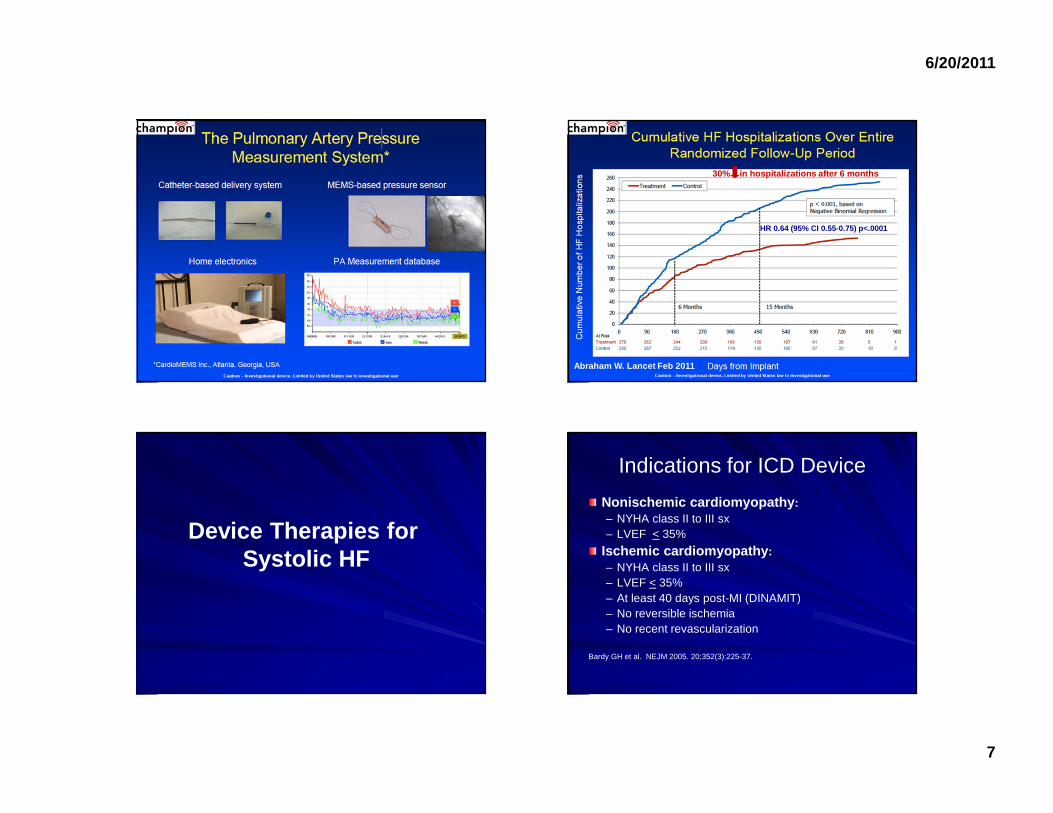
High vs Low Dose and Continuous vs Intermittent Diuretic Dosing:
DOSE HF Study
(p = 0.89)
Net volume loss
0
2500
5000
ml
4237 4249
ml
(p = 0.001)
3575
48995000
2500
0
Q12 bolus
High dose
Continuous infusion
Low dose
• Q12 and continuous infusion of furosemide similar for all outcomes assessed
• High dose intensification (2.5x oral dose) resulted in brisker diuresis at 72 hours, vs. with low dose (1x oral dose), but associated with transient worsening of renal function
• Clinical endpoints similar with both strategies
• Net volume loss similar with Q12 and continuous infusion, but higher with high vs. low dose intensification (4899 vs. 3575 ml)
• % increase in creatinine >0.3 mg/dl in 72 hours same with both infusion strategies, but ↑in high dose intensification arm (p = 0.04)
• Death/hospitalization/ED visit similar with infusion (p = 0.3) and dosing (p = 0.28)
Conclusions
Results
Felker GM, et al. N Engl J Med 2011;364:797-805
Audience Response QuestionThe use of nesiritide in patients with acute
decompensated HF is associated with which of the following?
Reduce
d eG
FR In
crea
sed m
ort...
Short
er hosp
it...
Impro
ved d
yspn...
Both
A a
nd B
3%5%
43%
14%
35%1. Reduced eGFR2. Increased mortality
3. Shorter hospital length of stay
4. Improved dyspnea5. Both A and B
6/20/2011
6
Nesiritide in ADHF: speculations put to rest in ASCEND-HF Trial
N=7141 patients with ADHF randomized to nesiritide vs placebo
End points Placebo (%), n=3511 Nesiritide (%), n=3496
p
30-d death/HF hospitalization* 10.1 9.4 0.31
Dyspnea at 6 h* 42.1 44.5 0.030
Dyspnea at 24 h* 66.1 68.2 0.007
>25% decrease eGFR 29.5 31.4 0.11
Conclusions:*Nesirtide was safe but is NOT effective in patients
with ADHF
Acute HF—Discharge Criteria HFSA 2010 Practice Guideline
Recommended for all HF patients
Exacerbating factors addressedNear optimal volume status observedTransition from intravenous to oral diuretic succes sfully completedPatient and family education completed, including c lear discharge instructionsNear optimal pharmacologic therapy achieved, includ ing ACEI and BB (for patients with reduced LVEF) or intolera nce documentedFollow-up clinic visit scheduled, usually for 7-10 days
Should be considered for patients with advanced HF or recurrent admissions for HF
Oral medication regimen stable for 24 hoursNo intravenous vasodilator or inotropic agent for 2 4 hoursAmbulation prior to discharge to assess functional capacity after therapyPlans for post-discharge management (scale present in home, visiting nurse or telephone follow up general ly no longer than 3 days after discharge)
Referral for disease management, if available
Strategies to Prevent Readmissions for HF
Telemonitoring is not effective– Tele-HF (n=1653), TIM-HF (n=710), TEHAF (n=382)
Transition of care and early follow-up visit are key!– Ideally within 7 days
Disease management programs are recommended– MDs, NPs, pharmacists, nutritionists
Current Initiatives to reduce hospital readmissions– BOOST, H2H, BEAT-HF, etc.
CMS is considering reducing payments to hospitals with high readmission rates starting 2012
Ingris, Cochrane 2010Chaudhry SI, et al. NEJM 2010;363(24):2301-9.
6/20/2011
7
Abraham W. Lancet Feb 2011
HR 0.64 (95% CI 0.55-0.75) p<.0001
30% in hospitalizations after 6 months
Device Therapies for Systolic HF
Indications for ICD Device
Nonischemic cardiomyopathy :– NYHA class II to III sx– LVEF < 35%
Ischemic cardiomyopathy :– NYHA class II to III sx– LVEF < 35%– At least 40 days post-MI (DINAMIT)– No reversible ischemia– No recent revascularization
Bardy GH et al. NEJM 2005. 20;352(3):225-37.
6/20/2011
8
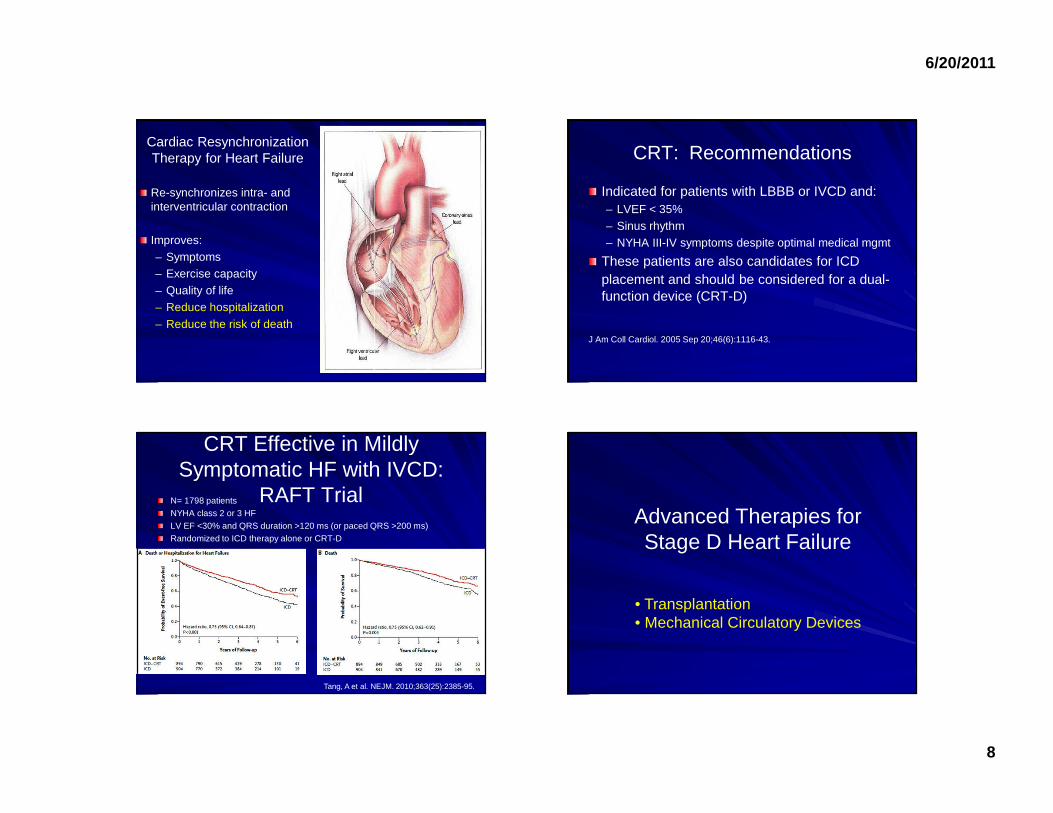
Re-synchronizes intra- and interventricular contraction
Improves:– Symptoms– Exercise capacity– Quality of life– Reduce hospitalization
– Reduce the risk of death
Cardiac ResynchronizationTherapy for Heart Failure CRT: Recommendations
Indicated for patients with LBBB or IVCD and:– LVEF < 35%– Sinus rhythm– NYHA III-IV symptoms despite optimal medical mgmt
These patients are also candidates for ICD placement and should be considered for a dual-function device (CRT-D)
J Am Coll Cardiol. 2005 Sep 20;46(6):1116-43.
CRT Effective in Mildly Symptomatic HF with IVCD:
RAFT TrialN= 1798 patientsNYHA class 2 or 3 HFLV EF <30% and QRS duration >120 ms (or paced QRS >200 ms)Randomized to ICD therapy alone or CRT-D
Tang, A et al. NEJM. 2010;363(25):2385-95.
Advanced Therapies for Stage D Heart Failure
• Transplantation• Mechanical Circulatory Devices
6/20/2011
9
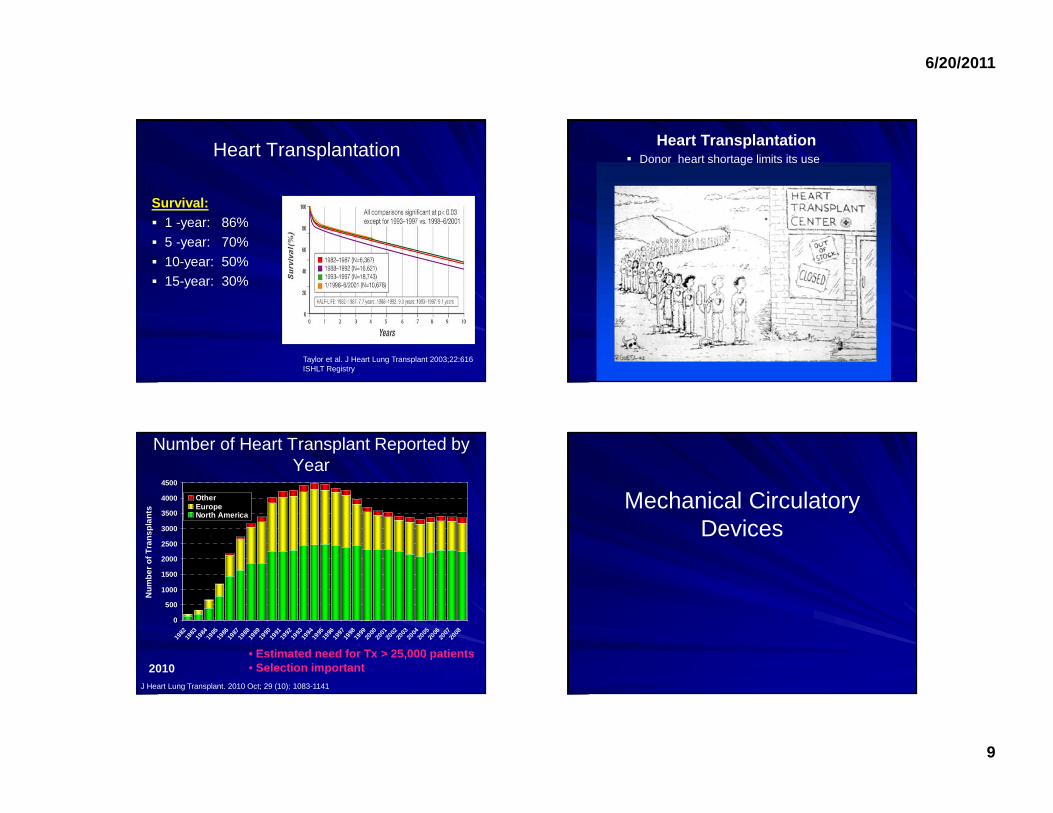
Heart Transplantation
Survival:� 1 -year: 86%
� 5 -year: 70%
� 10-year: 50%� 15-year: 30%
Taylor et al. J Heart Lung Transplant 2003;22:616ISHLT Registry
Heart Transplantation� Donor heart shortage limits its use
Number of Heart Transplant Reported by Year
• Estimated need for Tx > 25,000 patients• Selection important
J Heart Lung Transplant. 2010 Oct; 29 (10): 1083-1141
2010
0
500
1000
1500
2000
2500
3000
3500
4000
4500
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Num
ber o
f Tra
nspl
ants
OtherEuropeNorth America
Mechanical Circulatory Devices
6/20/2011
10
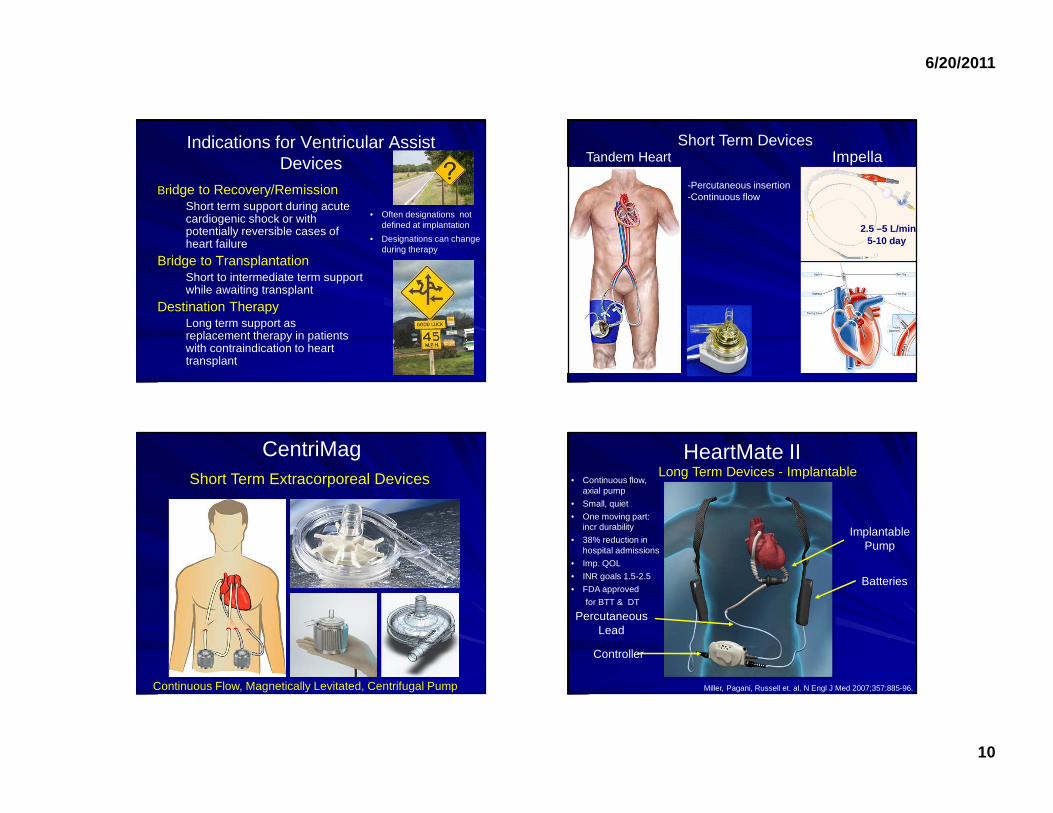
Indications for Ventricular Assist Devices
• Often designations not defined at implantation
• Designations can change during therapy
Bridge to Recovery/Remission Short term support during acute cardiogenic shock or with potentially reversible cases of heart failure
Bridge to Transplantation Short to intermediate term support while awaiting transplant
Destination Therapy Long term support as replacement therapy in patients with contraindication to heart transplant
2.5 –5 L/min5-10 day
Impella
-Percutaneous insertion-Continuous flow
Tandem HeartShort Term Devices
CentriMag
Continuous Flow, Magnetically Levitated, Centrifugal Pump
Short Term Extracorporeal Devices
HeartMate II
Controller
Batteries
PercutaneousLead
ImplantablePump
Long Term Devices - Implantable• Continuous flow,
axial pump
• Small, quiet
• One moving part: incr durability
• 38% reduction in hospital admissions
• Imp. QOL
• INR goals 1.5-2.5
• FDA approved
for BTT & DT
Miller, Pagani, Russell et. al. N Engl J Med 2007;357:885-96.
6/20/2011
11
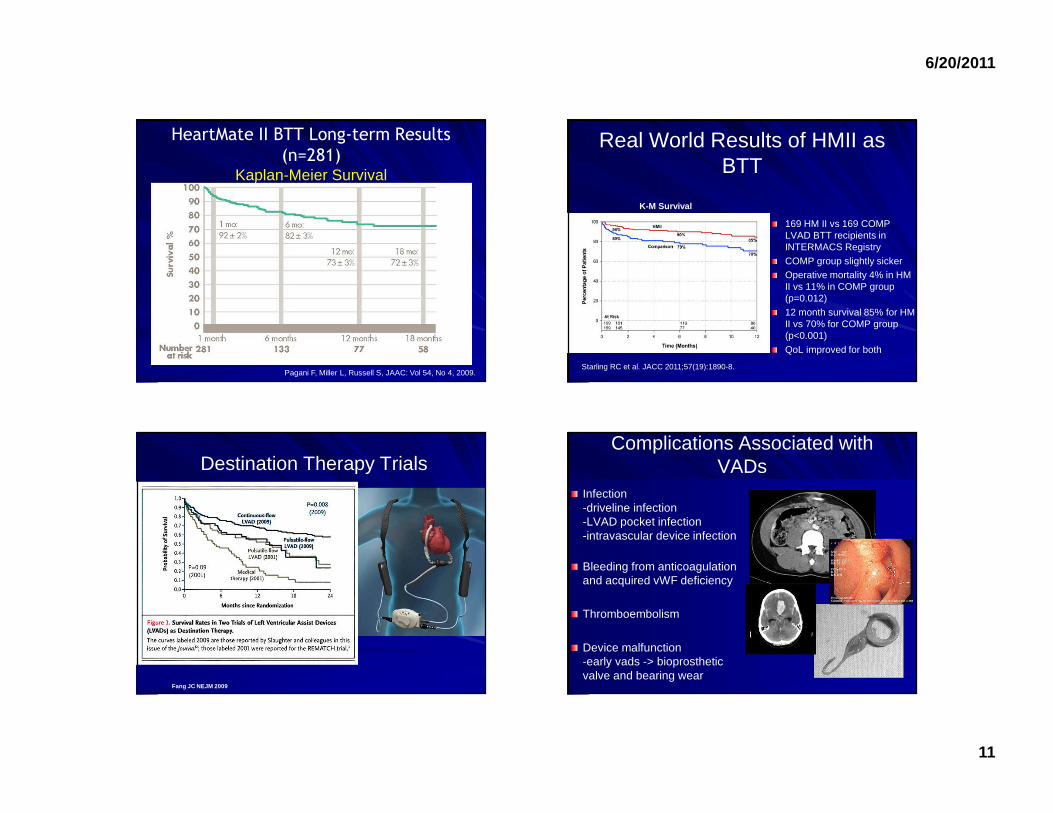
HeartMate II BTT Long-term Results
(n=281)Kaplan-Meier Survival
Pagani F, Miller L, Russell S, JAAC: Vol 54, No 4, 2009.
Real World Results of HMII as BTT
169 HM II vs 169 COMP LVAD BTT recipients in INTERMACS RegistryCOMP group slightly sickerOperative mortality 4% in HM II vs 11% in COMP group (p=0.012)12 month survival 85% for HM II vs 70% for COMP group (p<0.001)QoL improved for both
Starling RC et al. JACC 2011;57(19):1890-8.
K-M Survival
Destination Therapy Trials
Fang JC NEJM 2009
Infection-driveline infection-LVAD pocket infection-intravascular device infection
Bleeding from anticoagulation and acquired vWF deficiency
Thromboembolism
Device malfunction-early vads -> bioprosthetic valve and bearing wear
Complications Associated with VADs
6/20/2011
12
Future of VAD Therapies: What’s
Coming?Third Generation VAD technology and beyond
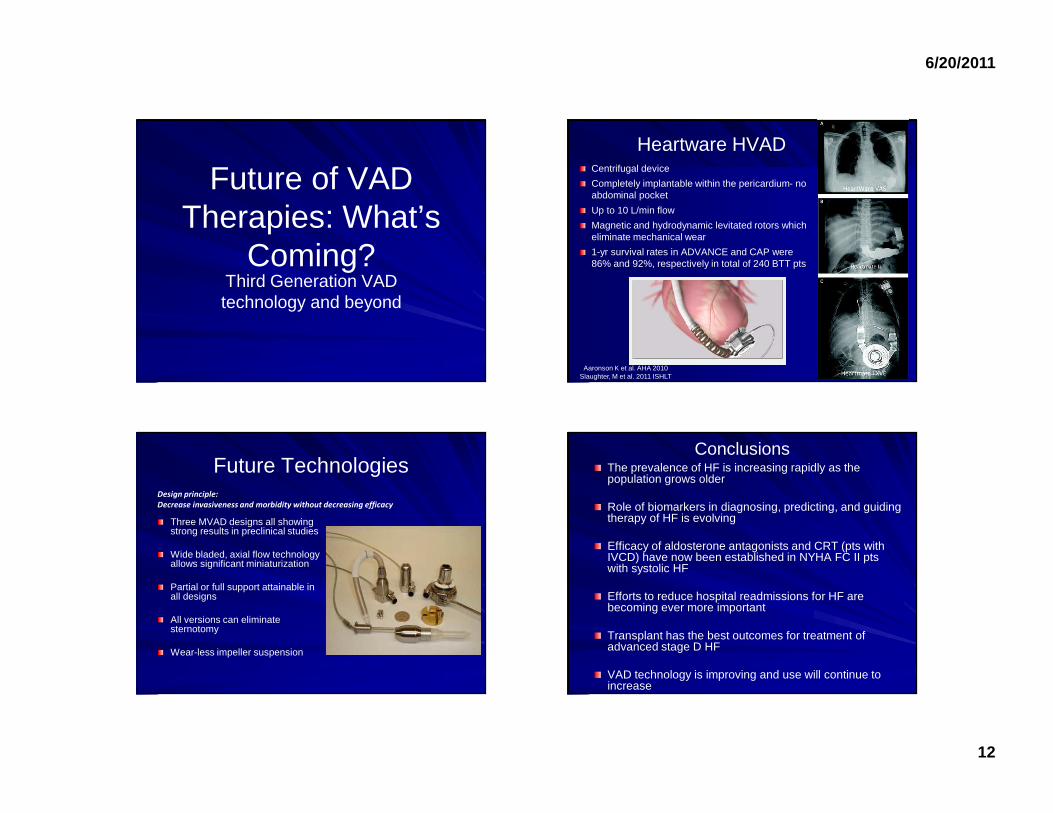
Centrifugal device
Completely implantable within the pericardium- no abdominal pocket
Up to 10 L/min flow
Magnetic and hydrodynamic levitated rotors which eliminate mechanical wear
1-yr survival rates in ADVANCE and CAP were 86% and 92%, respectively in total of 240 BTT pts
Heartware HVAD
Aaronson K et al. AHA 2010Slaughter, M et al. 2011 ISHLT
Future Technologies
Three MVAD designs all showing strong results in preclinical studies
Wide bladed, axial flow technology allows significant miniaturization
Partial or full support attainable in all designs
All versions can eliminate sternotomy
Wear-less impeller suspension
Design principle:
Decrease invasiveness and morbidity without decreasing efficacy
ConclusionsThe prevalence of HF is increasing rapidly as the population grows older
Role of biomarkers in diagnosing, predicting, and guiding therapy of HF is evolving
Efficacy of aldosterone antagonists and CRT (pts with IVCD) have now been established in NYHA FC II pts with systolic HF
Efforts to reduce hospital readmissions for HF are becoming ever more important
Transplant has the best outcomes for treatment of advanced stage D HF
VAD technology is improving and use will continue to increase
6/20/2011
13
Thank You!