Embed Size (px)
Citation preview

What’s the Idea?
University of Toronto LifeScience Career Day
June 23, 2009
Debra Chanda

Key Questions to Challenge the Idea
Invention vs. innovation Solving the wrong problem What’s it worth? Understanding the product development cycle
6. Is it practicable? 7. Is it approvable? 8. Is it the “answer”? 9. Is there a market?

Inventor Views
Inventor views patent like offspring. Colors objectivity.
Patented IP is a necessary ingredient, but… Does not assure commercial success May not be relevant May have only minimal value to company in context of other IP Arguably is the “easiest” part of the innovation process Remember, innovation takes place only when new value is created.

What do you need for innovation?
Patent protection regimesSpeed of regulatory approvalsPharmaceuticals in Canada are granted eight years of data protectionHowever, Canada does not perform as well as other OECD countries with respect to regulatory approvals

New Product Innovation Process
TechnologyR&D
IDEAProof of Concept
ConceptDevelopment
PreliminaryClinical
EvaluationProduct
DevelopmentClinicalTrials
RegulatoryClearance
CommercialPhase
Feasibility
Next Generation Product
3 to 15 years
Breakthrough

Pharma or Devices?

Drugs and Devices Differ Significantly!
Devices DrugsDirect mechanism of action
● Readily apparent response
Indirect mechanism of action● Metabolites, liver inactivation
Site/organ-specific therapy Systemic treatment
Uniform patient response to therapy (generally)
Variable patient response● Dosing● Side-effects, toxicity
Relatively small clinicals – 100s pts.; most successful
Large clinicals – 1000s pts.; high risk even at Phase 3
High initial cost Costs accumulate over treatment
Automatic therapy Dependence on patient compliance
Progressive efficacy improvement Efficacy static
Next-generational cost-effectiveness improvement
Cost-effectiveness relatively constant

OR Both: Novel Drug Delivery Platforms
Unmet Needs/Indications
Hep C
MS
ALS
Chronic pain
Depression
Inflammatory disease
Advantages
Decreased dosage
Increased efficacy
Decreased side effects
Compliance
Site specific delivery

OR Where are We Going?
Tissue engineering and combinational devicesmerging devices with biological elements
Control Fixation Cage InFusetm BMP6 mo. primate

How do we finance the Idea?
Discovery Proof of Concept Product Design & Product Development Manufacturing and Delivery
Angels
Angel Groups
Idea Pre-seed Funding Seed Funding Start-up Funding Expansion and Mezzanine Operating Capital
Seed Funds
Venture Funds
Institutional Equity
Loans and Bonds
Founder/Friends & Family
Gov’t Grants and Loans

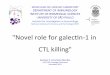
In 2004, the CDN federal government invested $1.1 billion in health research – its highest level ever. Of this amount 82% (or $906 million) was carried out by the higher education sector, industry and non-governmental organizations 18% (or $195 million) was performed in the federal government’s own laboratories
Where’s the Undiluted Money?

Expenditures on Health Research in Canada by Source of Funding, 1988 and 2004

Federal Funding for Health Research by Sector of Performance, 2004
18%
81%
0%1%
Federal Government
Higher Education
Industry
Non-governmentalOrganizations
Sector of Millions of
Performance Dollars
Federal Government 195
Higher Education 890
Industry 13
Non-governmental Organizations
3
Total 1,101
Source: Statistics Canada, “Estimates of Total Spending on Research and Development in the Health Field in Canada, 1988 to 2004,” Science Statistics, Catalogue 88-001-XIE, Vol. 29, No. 5, July 2005.

Level of Funding ($)
0100200300400500600700
Canad
a Res
earc
h Cha
irs In
frastr
uctur
e Fund
CFI Car
eer A
wards
Colleg
e Res
earch
Dev
elopm
ent F
und
Innov
ation
Fun
d
Lead
ing E
dge F
und
Resea
rch D
evelo
pment F
und
Resea
rch H
ospit
al Fun
d
TOTAL
Mill
ion
s
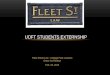
Level of Funding ($)
Source: Canada Foundation for Innovation, On-line Database, and Library of Parliament.
Canada Foundation for Innovation Funding inHealth Research Infrastructure by Program (As of 28 April 2006)

• There has been a major infusion of federal investment in health research since 1996.
• The proportion of federal funding to health research in Canada has remained largely unchanged over the years,
• Some organizations claim that the federal government must invest more in health research.
The growth in the federal government’s investment in health research has been achieved through increased Canadian Institute for Health Research, CIHR budgets, the establishment of new programs (NCE, CRC and ICR) and the creation of new funding bodies (namely CFI, Genome Canada and CHSRF).
Many feel that for a country the size of Canada, there are too many federal funding organizations in the field of health research.
In reviewing the information for these bodies, it is difficult to determine whether there is sufficient coordination to avoid duplication in the funding of projects.
Others feel that there is some element of competition between the various federal funding bodies.
Federal Money

Federal Money
Genome Canada was created in 2000-2001 as a not-for-profit organization that also reports to Parliament through the Minister of Industry.
• Its mandate is to develop and implement a national strategy in genomics and proteomics research for the benefit of all Canadians.
It is estimated that approximately 68.5% of the funding provided by Genome Canada is devoted to health research.
• In 2004-2005, Genome Canada contributed 4.7% of all federal health-research funding.
Canadian Health Services Research Foundation, CHSRF, which was established in 1997-1998, funds extramural research on the organization and delivery of health services under priority theme areas; it does not fund any clinical research.
• All CHSRF funding is devoted to health research. In 2004-2005, CHSRF provided less than 1% of federal health research funding.
• Unlike CIHR, the research themes are not based on particular health conditions such as cancer or mental illnesses, but are determined in consultation with various research partners.

Still Barriers
Canada compared to the US experiences 8 times lower Venture Capital investment in our sectorEven though Canada enjoys strong public investments in health-related R&DPost-secondary institutions, including teaching hospitals are less able to diffuse knowledge and turn research into marketable products/services (commercialization)Industry participation is lowNeed more collaboration among universities and business enterprises in Canada—Close the GapInvestment is critical to commercialization

Other Barriers to Entry
Regulation
Reimbursement
Product Liability

Regulatory Process• US process somewhat improved, but remains:
– Overly complex and getting more so• “Least burdensome” a term without meaning according to its
author – Inconsistent & unpredictable– Staffing & resource issues – Remains too slow and process driven
• Time is the enemy of desperately ill patients– Clinical trials requirements expanding
• “good science” paradox• Statistics is the gatekeeper rather than observed results
– Trials costs growing and channel innovations toward:• Incremental advancements vs. breakthroughs• Large markets at expense of small ones
• Over-zealous conflict-of-interest policies disqualify those with experience & direct knowledge.
Worldwide, process drifting toward US – regrettably.

Regulatory Process: The “Good Science” Paradox
For new medical devices, randomization (RCT’s) can chill the innovation process ● Technology still immature● Surgical technique evolving● Patient selection questions/recruitment issues● Slows technology evolution process● May be testing obsolete technology● Delays clinical availability● Adds to cost

~
~
~ ~
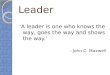
Biocor Stented Ht Valve
Activa Parkinsons
Acculink Carotid Stent
Contak Ht Failure Pacer
Regent Ht Valve
HeartMate II LVAD
5/97 CE
4/98 CE
2/99 CE
11/99 CE
10/01 CE
11/05 CE
8/05 FDA
1/02 FDA
5/02 FDA
3/02 FDA
8/04 FDA
4/08 FDA
99 Months
44 Months
37 Months
30 Months
30 Months
29 Months
Regulatory Approval Lag Time: CE Mark vs. FDA PMA
Implications for patients and innovation?
Biocor® St. Jude Medical; Activa® Medtronic; Regent® St. Jude Medical; Contak® Boston Scientific; Acculink™ Abbott Laboratories; Heartmate® Thoratec CorporationTrademarks:
© Paul Citron 2008

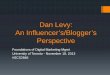
The Medical Device Industry: A Context
Implantable device industry founded in 1950sCardiac Pacemaker Large diameter vascular grafts
Key therapeutic market segments include:Cardiovascular Neurological SpinalOrthopedic Ophthalmic Reconstructive
– U.S. sales $86 billion in 2006– R&D intensive: 12.3% of sales1 (2006)
Dr.Lillihei with external pacemaker. Circa 1957
Dr. DeBakey sewing Dacron aortic grafts on his wife’s sewing machine. Circa 1953
1. 10 largest companies

Medical device innovation process is on-going, highly dynamic, highly technical, multidisciplinary, collaborative, and interdependent.
Scenario #1Physician identifies unmet need engineers implement solution
Scenario #2Engineer identifies opportunity physician applies to patient
In most instances, physicians and industry share a co-dependence:
-- Physicians can’t independently implement technology
-- Industry relies on physicians for patient access and care
-- Industry biomedical engineers hold peer status

Case Example: “Least Burdensome” FDA
Acorn Cardiovascular’s CorCap™ heart failure device.

The CorCap is a:
mesh wrap that is implanted around the heart, to provide gentle support.
CSD is intended to prevent and reverse the progression of heart failure by improving the heart’s structure and function, leading to improvements in the quality of a patient’s life.
Many heart failure patients develop oversized, dilated hearts as increasing pressure within the heart pushes out against the muscle wall.
CSD is the first medical device specifically designed to alleviate this pressure, thereby addressing a major contributing factor in heart failure progression.
Provide end-diastolic ventricular support to reduce wall stress and myocardial stretchNegate the stimuli for ventricular remodeling and promote myocardial reverse remodelingReverse progressive dilation and improve cardiac function and patient functional status
CorCap™
Cardiac Support Device
Source: Acorn Cardiovascular, Inc.

Key event chronology: CorCap™
Incorporated 1996. Has spent $83 million.Received CE Mark (permission to sell in Europe) – 2000Developed 180 pt. clinical study protocol with FDA input– New reviewer caused a study redesign; increased to 300 pts.– Agency turnover led to 5 different reviewers requiring learning
curve and causing delays and added expense with each new reviewer.
Study met all success goals (fewer cardiac procedures, ↑QOL)– June 2005 FDA Panel voted against approval: needs more
statistical evidence– With FDA suggestions, revised PMA application
Oct. 2005 FDA determined a new clinical study needed to confirm earlier results. Company appealed ruling.Dec 2006 FDA rejected appeal. Needed additional $30 million for another large clinical trial. Company survival at riskMay 2007 – FDA Dispute Resolution Panel grants permission for smaller (50 pt.) trial. Trial plus operations will cost $15 million.

US Reimbursement Design
Reimbursement is the lifeblood for new technologies– Critical for start-ups and small companies
CMS is most influential body for medical technology payment– FDA determines “safe & effective”– CMS determines “reasonable & necessary”– CMS has taken an overly cautious position regarding
new technologyCMS process for determining coverage:– Is additive to FDA time-line and remains slow and
inconsistent– Can redefine scope of FDA’s “safe and effective”
findings by limiting covered indications– Can add new clinical trial requirements for coverage
of safe and effective products

Approval/reimbursement reforms needed.
Existing process acceptable for:– Diseases where effective treatments exist– Where disease is not progressive or life-threatening
Process flawed for progressive, chronic, life-threatening diseases where effective treatments do not exist or are deficient
Overly focused on preventing harms vs. offering benefitsOverly focused on statisticsClinical studies not “least burdensome” as required by law

Remedies
Post-market studies should include peer-reviewed single center reportsFor well studied diseases of last/late resort:
Expedited clinicals that adhere to “ least burdensome”Shift focus to providing benefit vs. elimination of harmsGreater use of historical controls vs. active controlsCMS should not limit FDA’s safe and effective findings
Can require post market study if it desires to limit/sharpen criteria
Provisional coverage for new technologies upon FDA finding of “safe & effective”. “Reasonable & necessary” determination must acknowledge reality of next-generational improvements in cost effectiveness and functionality.

Expansion of Neurological Indications
Vision
Locomotion
Blood pressure
Inflammatory diseases
Spinal cord repair
Etc, etc
+

Where is the industry headed?
Implanted diagnostics & monitorsEnabled by sensors
ContinuousRemoves compliance issuesCaptures rare eventsCaptures events of daily living activities
• Disease management vs. device centered
Wellness At Risk Initial Event
PatientMonitoring
Medical Procedure
Therapeutic Device

Yes, the past is prologue to the future!!
Innovation is alive and well in academia and industryClinical community is receptiveVC and Grant financing is availableNew technologies tell an impressive storyImprovements in regulatory and reimbursement can accelerate the pace of innovation