Embed Size (px)
Citation preview

What determines trust in maternity care?: a cross-‐perspec5ve explora5on in peri-‐urban Kenya
Pooja Sripad
Mexico City, Mexico 20th October, 2015

“If you don’t trust an institution, you won’t go there for whatever service. Only if you don’t trust the hospital, then it’s really grave because in a hospital it sometimes
is between life and death.” (Medical of,icer)

Background: Trust
• The belief that one’s expecta9ons will be met by an individual or system
• Offers insight into – percep9ons of interac9ons – power differen9als – inequi9es in health experience
• Kenya: a “nested” understanding
Trust in maternity care
Confidence Communica9on Integrity Mutual Respect Competence Confiden9ality Fairness Systems Trust

Background: Kenya Context • Maternal health
– MMR: 488 deaths/100,000 live births – 61% women deliver in facili9es – 20% report disrespect and abuse during facility
delivery
• Heshima Project (‘promo9ng dignity’) – Organic emergence of “trust”
• Relevant poli9cal history – Culture of impunity – New Cons9tu9on (2010) – Devolu9on (roll out 2013) – Free-‐maternity policy (June 2013)
Sta9s9cs Sources: (KDHS 2008-‐09; KDHS 2015; Abyua, et al., 2015)
Source: hdp://www.mapsofworld.com/kenya/kenya-‐poli9cal-‐map.html

Research Ques9on
• What determines trust in a maternity segng?

Study segng: peri-‐urban county

Qualita9ve approach
• Theories: apprecia9ve inquiry and ins9tu9onal ethnography
“Women & community”
“Providers & Management”

Qualita9ve Process
Data collec5on & management • Introduc9ons & consent
• Guided FGD/IDI
• Brief ques9onnaire
• Audio-‐recording, transcrip9on, & transla9on
Data analysis • Constant comparison method
• Concurrent ini9al followed by final textual analysis – In-‐depth fieldnotes – Reading transcripts – Induc9ve coding – Memo-‐wri9ng

Key findings

Trust in Maternity Segng
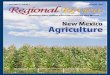
• Prior experience • Perceived risk or harm • Childbirth outcomes • Maternity care literacy
• Empathy & respect • Personalized aden9on & care • Perceived ability of provider • Discrimina9on • Corrup9on
• Responsiveness in emergencies & “good services” • Physical environment & cleanliness • Navigability of processes • Management and oversight • Discrimina9on • Corrup9on • Coordina9on amongst providers
• Reputa9on & social history • Corrup9on • Informa9on channels (social networks, CHW
promo9on, media) • Maternity care literacy
• Ac9ons align with expecta9ons • Adapt to policy changes • Community voice • Intra-‐facility feedback
Provider factors
Pa9ent/ individual factors
Health facility factors
Community factors
• Ins9tu9onal hierarchies • Policies and professional prac9ce
codes • Devolu9on
ACCOUNTABILITY
STRUCTURAL FACTORS
Figure: Mul+-‐faceted trust determinants in the maternity se7ng

Pa9ent/individual factors
Women & Community
Providers & Management
“(R1): There are also diseases like HIV. When one delivers in hospital, it is not easy for the baby to get infected. Also, they [TBAs] use things like razorblades, and in the process, one may cut themselves and infect the baby.” (Male partners, FGD)
“I have faith... even if you mistreat me…the baby will be well” (RDW in a facility)
“a woman came to deliver and had a very bad experience. She carries forward that bad experience to the next delivery .” (Medical officer)
“Some mothers come without knowing the role of a nurse or the role of a doctor…So some+mes they accuse the nurses for things which are beyond our capability.” (Nurse-‐midwife)

Community Factors
• Social history & reputa9on
• Informa9on channels – Social networks – CHWs – Media
“(R1): You get prepared psychologically [from conversa+ons]. If you get a certain feeling while at home, you may not be sure what it is. But not if one who has gone through such a thing has already told you of it. (R2): It helps you to be prepared.” (1st 9me pregnant women, FGD)
“An experience you or someone else had there that caused you to either trust it or not trust it. Its history.” (Male partner, FGD)

Provider factors Women & Community Providers & Management
“That is a good doctor, a doctor who does not discriminate against anybody. You look at her when she is talking to you – or to another person – she does not have a bad heart.” (RDW, IDI)
“They take you in immediately... They examine you to know how close you are to delivery…. they don’t leave you. They stay around and come quickly when it’s +me for you to deliver. They later then make you tea, and show you to a bed with your baby where they cover you. They keep checking on you frequently +ll you leave the hospital.” (RDW in facility, FGD)
You [the midwife] are alone and you have to handle all those cases and out of that tension, you want the mother to behave right the way so you kind of end up shou>ng at the mother. (Facility matron)

Health facility factors • “good services” and responsiveness in emergencies
• Physical and material resource environment – Infrastructure, space, cleanliness, beds, ancillary care, supplies chains, drugs
• Human resources: morale, management, oversight, supervision
• Navigability of facility processes (e.g. unclear payment mechanisms)
• Corrup9on
• Coordina9on amongst providers
“pa+ents are very innocent. Some+mes they come and whoever is aWending might ask for some money -‐ nobody will know because they are alone in the room.... So pa+ents should also know their rights and they should know that if they pay for anything they should be given a receipt.” (Nurse-‐midwife)

Accountability
• Women’s expecta9ons align with facility ac9ons
• Facility ability to respond to free maternity
• Engage voices to ensure facility responsiveness – Women & community – Frontline providers
“if we are expected to serve these pa+ents well… somebody somewhere should listen to me.” (Nurse-‐midwife)
“I think that will help in a big way for women who are underprivileged…But also, I feel like the services could deteriorate…I feel like if someone could insult you now during delivery yet you pay for the service. So when they know you didn’t pay, won’t they insult you more? ….” (RDW, IDI)

Structural factors • Ins9tu9onal hierarchies
• Devolu9on
“it’s just that doctor-‐nurse rela+onship… ‘I am more superior cause am a doctor’ …I think every individual deserves respect.” (Medical officer)
“You cannot stand back and wait for a pa+ent to be mismanaged just because somebody is a doctor…you have to correct them...It’s difficult, it’s a man [says empha+cally] bringing you down…” (Nurse-‐midwife, in-‐charge)
“They are s+ll at that stage of trying to nego+ate to see who will be where, how will it be done… it is important to have some structure between the county and the health facility levels.” (DPHO)

Summary and Implica9ons • Theory and perspec9ve enable understanding of what affects trust in the
maternity segng
• Factor clusters relate to each other and affect trust in more than one way
• Mul9-‐faceted determinants demand a complex set of trust building mechanisms
• Future research needed – Compara9ve inquiry of framework – Interac9ons between factor clusters and determinant saliency – Social networks and trust

Conclusion
• Trust is an important lens for maternity care and health systems
• Trust has many determinants that may interact in complex ways
• Poli9cs of health care segngs have implica9ons for trust

Acknowledgements • Study par9cipants
• Thesis commidee and readers (JHSPH) – Maria MerriI (advisor)* – Robert Lawrence – Deanna Kerrigan* – Sachiko Ozawa* – Larissa Jennings*
• Popula9on Council – CharloIe Warren* – Timothy Abuya* – Charity Ndwiga* – Janet Munyasa – Jackie Kivunaga
• Research Assistants – Brigide Nelima – Florence Thungu – Helen Chepkorir Tanui – Grace Rogena – Dennis Bravo Adipo – Rose Shivambo
• USAID TRAc9on • Global Maternal Newborn Health Conference
2015 Conference Organizers
* Co-‐authors on abstract

Asante!/Thank you!/Gracias!
Ques5ons? /Preguntas?