Embed Size (px)
Citation preview

What the asthma end points we know and lovedo and do not tell us
Allan T. Luskin, MD Madison, Wis
Asthma is a disorder characterized by common features of
reversible airflow obstruction and bronchial hyperreactivity in
the setting of airway mucosal and submucosal inflammation.
However, the clinical manifestations are syndromic and not
unimodal. There is marked variability in severity of symptoms,
natural history, risks of adverse outcomes, pathologic
characteristics, and response to therapy. Understanding the
relationship between these factors has been complicated by the
variability of outcomes and the lack of correlation between
them. There is a striking absence of correlation among the
pathologic, physiologic, and clinical manifestations of the
asthmatic disorders. Lung function tends to correlate poorly
with clinical outcomes, and there is only modest correlation
between clinical outcomes. Response to therapy is variable both
externally (between patients) and internally, depending on
which outcome is evaluated. A more complete understanding of
the variability of disease and the genetic and environmental
causes of the variability likely will change how we approach
asthma and its therapy. (J Allergy Clin Immunol
2005;115:S539-45.)
Key words: Asthma, control, severity, outcomes, phenotypes, var-iability, asthma-related quality of life
Asthma is characterized by reversible airflow obstruc-tion and bronchial hyperreactivity (BHR), but the clinicalpresentations and responses to therapy are variable. Itis apparent that asthma is a syndrome with variablephysiologic, pathologic, and clinical manifestations. Thephenotypes represent the visible effects of the interactionsbetween the genetic makeup and environment. Asthmaphenotypes appear to be different in terms of control,severity, response to therapy, natural history, risk foradverse outcomes, the relationship among features of thedisease, and the relationship between various outcomes.
Initial guidelines made a superficial effort to recognizethis dramatic variability by grossly estimating severity.However, because the bulk of adverse outcomes appearto be related to underdiagnosis, inadequate therapy, andpoor adherence, and because most patients respondfavorably to inhaled corticosteroids and b-agonists, animproved understanding of the various asthma syndromes
From the Department of Medicine, University of Wisconsin.
Disclosure of potential conflict of interest: A. T. Luskin has consulting
arrangements with Genentech and Merck and has received grants–research
support from Merck and AstraZeneca.
Reprint requests: Lauri Sweetman, American Academy of Allergy, Asthma
and Immunology, 611 East Wells St, Milwaukee, WI 53202. E-mail:
0091-6749/$30.00
� 2005 American Academy of Allergy, Asthma and Immunology
doi:10.1016/j.jaci.2005.01.027
was not of major importance in the initial approach to im-proving asthma outcomes. Newer pharmacotherapy,better understanding of the pathophysiologies of asthma,and the beginnings of characterization of the genetics ofthe response to the environment and therapy make inves-tigations of the variability of disease a new frontier inasthma research and treatment. One of the first changes inthis new era is a refined focus on control instead of severityas the primary asthma measure and an integration ofpatient-derived outcomes into the dimensions of control.
GENERAL QUALITY OF LIFE OF PATIENTSWITH ASTHMA
Most of the variability that is observed in asthma canbe explained by genetic differences among asthmaticpatients. Asthma is monitored on the basis of severaloutcomes and therefore is recognized more as a syndromerather than a disease. Currently, outcomes monitored inasthma vary greatly and do not correlate with one another.Although several outcomes are assessed for each patient,the primary concern of most primary care physicians andpatients is the burden of the disease or the health-relatedquality of life (HRQOL). A recent study1 illustrated thatpatients with asthma experienced twice as many unhealthydays a year compared with individuals who have neverhad asthma. There were twice as many days with activitieslimited, twice as many mentally unhealthy days, and morethan twice as many physically unhealthy days.1 In total,patients in the United States with asthma experienceapproximately 150 million unhealthy functioning daysa year. The current review will examine frequently usedasthma end points and what we can learn from them.
CHARACTERISTICS OF THE IDEALASTHMA MEASURE
Choosing outcomes to measure in the assessment ofasthma control requires an understanding of what is anideal measure and the various dimensions of control.
An ideal measure for asthma should be simple andpractical, meaningful, and applicable to doctors, patients,health system managers, and researchers. It needs to bereflective of short- and long-term control. It should be
Abbreviations usedBHR: Bronchial hyperreactivity
HRQOL: Health-related quality of life
S539
J ALLERGY CLIN IMMUNOL
APRIL 2005
S540 Luskin
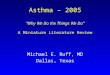
FIG 1. There is an approximate 40% divergence comparing positive or lack of response with lung function and
symptoms as outcomes. Reprinted with permission from Shingo et al. Copyright � 2001 European
Respiratory Society Journals Ltd. All rights reserved.2
selective of patients who are at risk of clinical worseningand those who have mild disease and will always remainminimally affected. It needs to be discriminatory andresponsive to change. Because asthma is a syndromerather than a disease, it has been and continues to be dif-ficult to identify such an indicator.
DIMENSIONS OF ASTHMA CONTROL
There are various dimensions of control that take formfrom the various burdensome aspects of asthma. There aremedical outcomes, including clinical, biologic, and phys-iologic markers; the humanistic outcomes, includingquality of life (QOL) and satisfaction; and the economicoutcomes, including costs to patients, society, health caresystems, and the workplace. It is reasonable to differen-tiate these markers into physiologic, symptoms, QOL,medications, health care use, exacerbations, activities ofdaily living, and comorbidites.
Current favored measurements include the following:(1) FEV1, (2) BHR, (3) symptom scores, (4) emergencydepartment visits and hospitalizations as major drivers ofhealth care use, (5) exhaled nitric oxide or other exhaledgases, (6) b-agonist use, (7) exacerbations, and (8) QOL.Because of the variability in these outcomes, it is likelythat there is no single measurement that is the bestindicator of asthma control, nor will one function as auniversally applicable surrogate for all patients.
As understanding improves about these issues, we alsomust consider that control is a continuum versus a pointin time, as analog versus digital, and variable betweenobservers and that there is a disconnect between variouscontrol outcomes.
SYNDROMIC NATURE OF ASTHMA
The phenotype of asthma is clinically and pathologi-cally variable between those with early-onset, late-onset,
neutrophilic, and eosinophilic asthma. In addition to clinicaland pathologic differences, there are also physiologicdifferences between patients. For example, there aresubjects with hyperacute or brittle asthma with markedBHR and others for whom BHR is not a major feature.Correlating the pathologic changes with clinical andphysiologic outcomes has been inconsistent. Furthermore,an overlooked variable is the individual response totherapy. AlthoughBHRand reversible air flowobstructionare important characteristics of asthma, they do not predictthe response to therapy. The outcomes monitored do notcorrelate well with each other or between observers.
RESPONDERS AND NONRESPONDERS
Simplistically, it would be helpful to characterizeasthmatic subjects as responding or not respondingadequately to a particular intervention. A widely heldbut incorrect belief is that patients either respond or not,and if they respond, they will improve in all importantfeatures of their disease (clinical, pathologic, and eco-nomic). However, evaluation leads to very differentconclusions. Asthmatic patients can be separated into 2groups on the basis of their FEV1 and symptom scoreresponses to therapy. If the FEV1 and the symptom scoresboth go up, that patient might be considered a responder.In contrast, a nonresponder is a patient whose FEV1 andsymptom scores do not change or worsen. However,although 60% of asthmatic patients can be classified aseither responders or nonresponders because their lungfunction and symptoms get better or not, 40% of asthmaticpatients have divergent responses (Fig 1).2 Thus in a largegroup of patients, symptoms improve in the absence oflung function improvement, or lung function improveswithout a parallel improvement in symptoms.
A study by Malmstrom et al3 evaluated subjects withmoderate asthma treated with the leukotriene modifiermontelukast and evaluated FEV1 as an outcome. One third
J ALLERGY CLIN IMMUNOL
VOLUME 115, NUMBER 4
Luskin S541
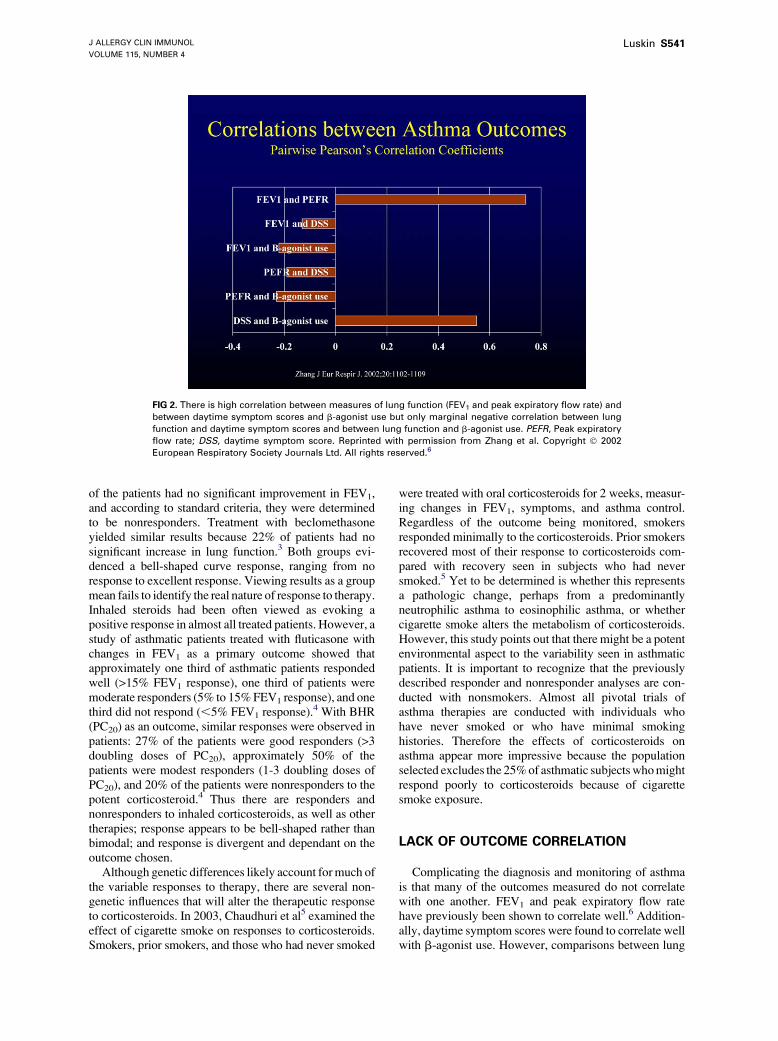
FIG 2. There is high correlation between measures of lung function (FEV1 and peak expiratory flow rate) and
between daytime symptom scores and b-agonist use but only marginal negative correlation between lung
function and daytime symptom scores and between lung function and b-agonist use. PEFR, Peak expiratory
flow rate; DSS, daytime symptom score. Reprinted with permission from Zhang et al. Copyright � 2002
European Respiratory Society Journals Ltd. All rights reserved.6
of the patients had no significant improvement in FEV1,and according to standard criteria, they were determinedto be nonresponders. Treatment with beclomethasoneyielded similar results because 22% of patients had nosignificant increase in lung function.3 Both groups evi-denced a bell-shaped curve response, ranging from noresponse to excellent response. Viewing results as a groupmean fails to identify the real nature of response to therapy.Inhaled steroids had been often viewed as evoking apositive response in almost all treated patients. However, astudy of asthmatic patients treated with fluticasone withchanges in FEV1 as a primary outcome showed thatapproximately one third of asthmatic patients respondedwell (>15% FEV1 response), one third of patients weremoderate responders (5% to 15%FEV1 response), and onethird did not respond (,5% FEV1 response).
4 With BHR(PC20) as an outcome, similar responses were observed inpatients: 27% of the patients were good responders (>3doubling doses of PC20), approximately 50% of thepatients were modest responders (1-3 doubling doses ofPC20), and 20% of the patients were nonresponders to thepotent corticosteroid.4 Thus there are responders andnonresponders to inhaled corticosteroids, as well as othertherapies; response appears to be bell-shaped rather thanbimodal; and response is divergent and dependant on theoutcome chosen.
Although genetic differences likely account for much ofthe variable responses to therapy, there are several non-genetic influences that will alter the therapeutic responseto corticosteroids. In 2003, Chaudhuri et al5 examined theeffect of cigarette smoke on responses to corticosteroids.Smokers, prior smokers, and those who had never smoked
were treated with oral corticosteroids for 2 weeks, measur-ing changes in FEV1, symptoms, and asthma control.Regardless of the outcome being monitored, smokersresponded minimally to the corticosteroids. Prior smokersrecovered most of their response to corticosteroids com-pared with recovery seen in subjects who had neversmoked.5 Yet to be determined is whether this representsa pathologic change, perhaps from a predominantlyneutrophilic asthma to eosinophilic asthma, or whethercigarette smoke alters the metabolism of corticosteroids.However, this study points out that there might be a potentenvironmental aspect to the variability seen in asthmaticpatients. It is important to recognize that the previouslydescribed responder and nonresponder analyses are con-ducted with nonsmokers. Almost all pivotal trials ofasthma therapies are conducted with individuals whohave never smoked or who have minimal smokinghistories. Therefore the effects of corticosteroids onasthma appear more impressive because the populationselected excludes the 25%of asthmatic subjectswhomightrespond poorly to corticosteroids because of cigarettesmoke exposure.
LACK OF OUTCOME CORRELATION
Complicating the diagnosis and monitoring of asthmais that many of the outcomes measured do not correlatewith one another. FEV1 and peak expiratory flow ratehave previously been shown to correlate well.6 Addition-ally, daytime symptom scores were found to correlate wellwith b-agonist use. However, comparisons between lung
J ALLERGY CLIN IMMUNOL
APRIL 2005
S542 Luskin
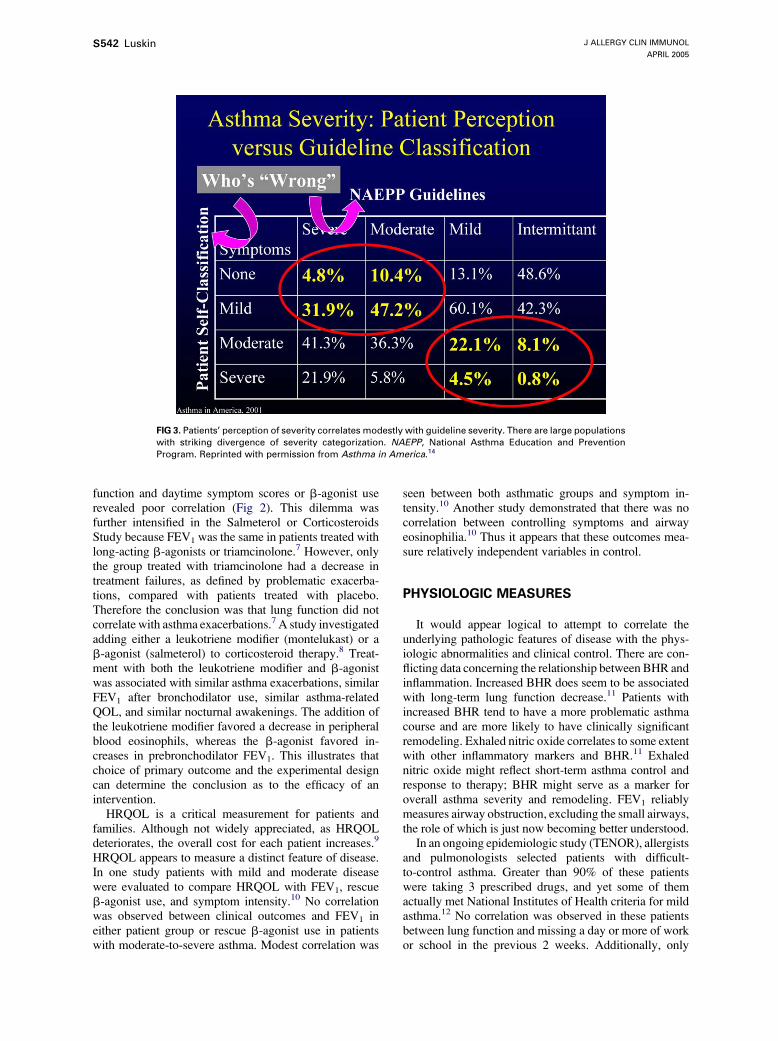
FIG 3. Patients’ perception of severity correlates modestly with guideline severity. There are large populations
with striking divergence of severity categorization. NAEPP, National Asthma Education and Prevention
Program. Reprinted with permission from Asthma in America.14
function and daytime symptom scores or b-agonist userevealed poor correlation (Fig 2). This dilemma wasfurther intensified in the Salmeterol or CorticosteroidsStudy because FEV1 was the same in patients treated withlong-acting b-agonists or triamcinolone.7 However, onlythe group treated with triamcinolone had a decrease intreatment failures, as defined by problematic exacerba-tions, compared with patients treated with placebo.Therefore the conclusion was that lung function did notcorrelate with asthma exacerbations.7 A study investigatedadding either a leukotriene modifier (montelukast) or ab-agonist (salmeterol) to corticosteroid therapy.8 Treat-ment with both the leukotriene modifier and b-agonistwas associated with similar asthma exacerbations, similarFEV1 after bronchodilator use, similar asthma-relatedQOL, and similar nocturnal awakenings. The addition ofthe leukotriene modifier favored a decrease in peripheralblood eosinophils, whereas the b-agonist favored in-creases in prebronchodilator FEV1. This illustrates thatchoice of primary outcome and the experimental designcan determine the conclusion as to the efficacy of anintervention.
HRQOL is a critical measurement for patients andfamilies. Although not widely appreciated, as HRQOLdeteriorates, the overall cost for each patient increases.9
HRQOL appears to measure a distinct feature of disease.In one study patients with mild and moderate diseasewere evaluated to compare HRQOL with FEV1, rescueb-agonist use, and symptom intensity.10 No correlationwas observed between clinical outcomes and FEV1 ineither patient group or rescue b-agonist use in patientswith moderate-to-severe asthma. Modest correlation was
seen between both asthmatic groups and symptom in-tensity.10 Another study demonstrated that there was nocorrelation between controlling symptoms and airwayeosinophilia.10 Thus it appears that these outcomes mea-sure relatively independent variables in control.
PHYSIOLOGIC MEASURES
It would appear logical to attempt to correlate theunderlying pathologic features of disease with the phys-iologic abnormalities and clinical control. There are con-flicting data concerning the relationship between BHR andinflammation. Increased BHR does seem to be associatedwith long-term lung function decrease.11 Patients withincreased BHR tend to have a more problematic asthmacourse and are more likely to have clinically significantremodeling. Exhaled nitric oxide correlates to some extentwith other inflammatory markers and BHR.11 Exhalednitric oxide might reflect short-term asthma control andresponse to therapy; BHR might serve as a marker foroverall asthma severity and remodeling. FEV1 reliablymeasures airway obstruction, excluding the small airways,the role of which is just now becoming better understood.
In an ongoing epidemiologic study (TENOR), allergistsand pulmonologists selected patients with difficult-to-control asthma. Greater than 90% of these patientswere taking 3 prescribed drugs, and yet some of themactually met National Institutes of Health criteria for mildasthma.12 No correlation was observed in these patientsbetween lung function and missing a day or more of workor school in the previous 2 weeks. Additionally, only
J ALLERGY CLIN IMMUNOL
VOLUME 115, NUMBER 4
Luskin S543
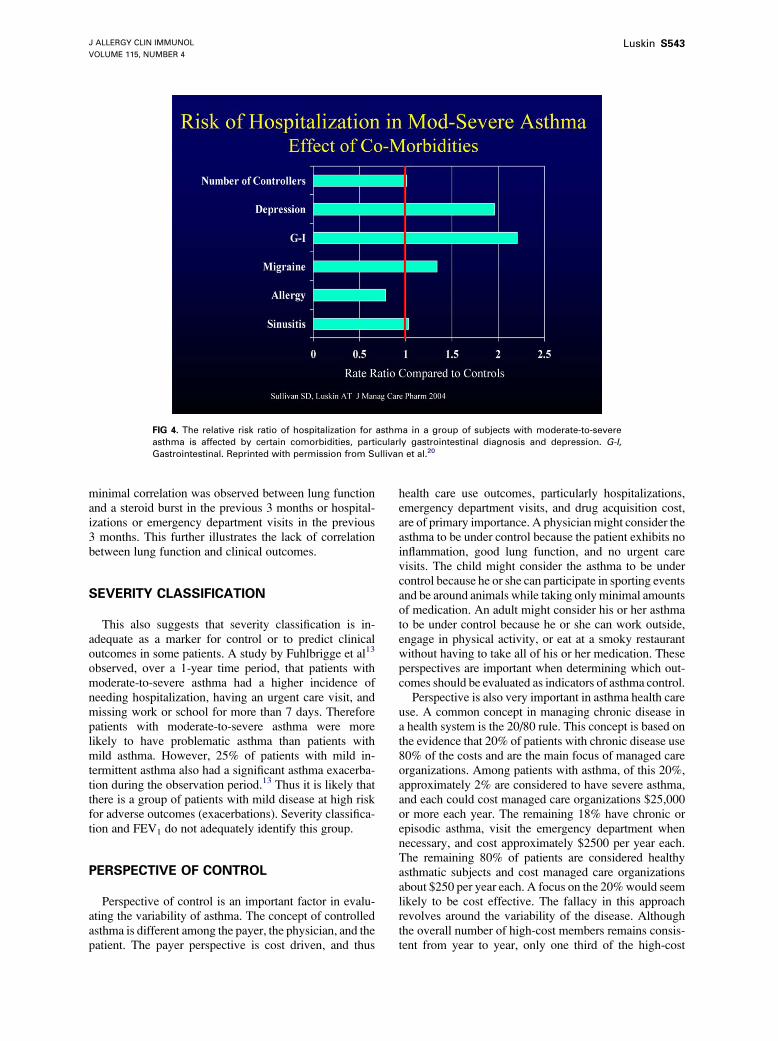
FIG 4. The relative risk ratio of hospitalization for asthma in a group of subjects with moderate-to-severe
asthma is affected by certain comorbidities, particularly gastrointestinal diagnosis and depression. G-I,
Gastrointestinal. Reprinted with permission from Sullivan et al.20
minimal correlation was observed between lung functionand a steroid burst in the previous 3 months or hospital-izations or emergency department visits in the previous3 months. This further illustrates the lack of correlationbetween lung function and clinical outcomes.
SEVERITY CLASSIFICATION
This also suggests that severity classification is in-adequate as a marker for control or to predict clinicaloutcomes in some patients. A study by Fuhlbrigge et al13
observed, over a 1-year time period, that patients withmoderate-to-severe asthma had a higher incidence ofneeding hospitalization, having an urgent care visit, andmissing work or school for more than 7 days. Thereforepatients with moderate-to-severe asthma were morelikely to have problematic asthma than patients withmild asthma. However, 25% of patients with mild in-termittent asthma also had a significant asthma exacerba-tion during the observation period.13 Thus it is likely thatthere is a group of patients with mild disease at high riskfor adverse outcomes (exacerbations). Severity classifica-tion and FEV1 do not adequately identify this group.
PERSPECTIVE OF CONTROL
Perspective of control is an important factor in evalu-ating the variability of asthma. The concept of controlledasthma is different among the payer, the physician, and thepatient. The payer perspective is cost driven, and thus
health care use outcomes, particularly hospitalizations,emergency department visits, and drug acquisition cost,are of primary importance. A physician might consider theasthma to be under control because the patient exhibits noinflammation, good lung function, and no urgent carevisits. The child might consider the asthma to be undercontrol because he or she can participate in sporting eventsand be around animals while taking only minimal amountsof medication. An adult might consider his or her asthmato be under control because he or she can work outside,engage in physical activity, or eat at a smoky restaurantwithout having to take all of his or her medication. Theseperspectives are important when determining which out-comes should be evaluated as indicators of asthma control.
Perspective is also very important in asthma health careuse. A common concept in managing chronic disease ina health system is the 20/80 rule. This concept is based onthe evidence that 20% of patients with chronic disease use80% of the costs and are the main focus of managed careorganizations. Among patients with asthma, of this 20%,approximately 2% are considered to have severe asthma,and each could cost managed care organizations $25,000or more each year. The remaining 18% have chronic orepisodic asthma, visit the emergency department whennecessary, and cost approximately $2500 per year each.The remaining 80% of patients are considered healthyasthmatic subjects and cost managed care organizationsabout $250 per year each. A focus on the 20%would seemlikely to be cost effective. The fallacy in this approachrevolves around the variability of the disease. Althoughthe overall number of high-cost members remains consis-tent from year to year, only one third of the high-cost

J ALLERGY CLIN IMMUNOL
APRIL 2005
S544 Luskin
members remain high cost from one year to the next. Twothirds of the patients who are high-cost members in thesecond year were previously low-cost members in the firstyear. This further supports the variability of asthma andthe difficulty in identifying specific outcomes that willserve as markers of asthma control and identify those atrisk for adverse outcomes.
PATIENT CLASSIFICATION OF SEVERITYAND CONTROL
There is a discrepancy among patient, guideline, andclinician ratings of control. One third of patients classifiedas having severe disease as defined by the NationalAsthma Education and Prevention Program guidelinesreported only mild or no symptoms (Fig 3).14 On the otherhand, 10% of the patients with intermittent asthma saythat they have moderate or severe symptoms.14 In a studyasthma severity classification was evaluated by using 3different criteria: (1) patient-perceived severity, (2) symp-tom-derived severity, or (3) medication-derived severity.Patient-perceived severity asked the following question:How severe do you think your asthma is? Symptomseverity was a measure of overall or nocturnal symptomsover the previous 4 weeks. Medication-derived severitymeasuring rescue medication has been used.15 Markedvariability among these 3 methods of evaluating asthmaseverity was noted.15
Nathan et al16 used a modified asthma control test toacquire data on control. Five questions were asked asfollows: (1) Does your asthma keep you from getting asmuch work done at work and school? (2) How would yourate your asthma control? (3) How often have you hadshortness of breath? (4) Does your asthma wake you up atnight or earlier than usual? (5) Have you needed yourrescue inhaler or nebulized medicine? These 5 questionswere found to correlate well with the specialists’ assess-ment of asthma control. This might provide a convenientmeasure of patient perception of control and an easy-to-use data collection tool for important markers of control.
ASTHMA CONTROL
Studies to date strongly indicate that clinical, physio-logic, and inflammatory markers are disparate and corre-late poorly. They appear to reflect different expressionsof disease. Ultimately, a unified view of control will benecessary to balance the weight given to each outcomeby payers, clinicians, and patients. Regardless of whichmeasurements are used, interventions have various effectson outcomes. Some interventions might improve FEV1
and not change exacerbation rates. Others might decreaseexacerbations and have little effect on lung function.
ALTERNATIVE APPROACHES
A study compared standard guideline-based therapyfor asthma and sputum eosinophil counts to determine
therapy for patients with moderate-to-severe asthma. Theinvestigators concluded that sputum eosinophil countsmight have value as a marker of asthma control anda guide for therapy. Fewer patients managed by means ofthis outcome reported hospital visits and severe exacer-bations of their asthma.17 Another study compared 2different asthma management strategies. In one groupBHR (methacholine challenge) every 3 months was usedto guide therapy. These patients used higher doses ofinhaled corticosteroids and had a longer time to the firstmild exacerbations than patients managed in the usualway.18 Therefore changes in the way that patients aremonitored might also affect the degree of asthma control.
Another study investigated the relationship betweenfrequent mental distress and parameters of health-relatedquality of life. Patients with asthma had twice theprevalence of frequent mental distress than non-asth-matics, and asthmatics with frequent mental distress hadlower HRQOL than asthmatics without.19 There was nodifference in FEV1 between the depressed and the non-depressed groups. A separate study demonstrated thatcomorbidities (ie, depression, gastrointestinal symptoms,and migraine headaches) increase the risk of hospitaliza-tion for patients with moderate-to-severe asthma (Fig 4).20
CONCLUSIONS
Asthma is a complex syndromewith variable outcomes.This variability has made it difficult to appropriatelymonitor and control asthma. There is no single parameterthat serves as an accurate marker of asthma control oreffectiveness of therapy. Multifaceted markers are neces-sary to adequately characterize this complex disorder.Outcomes do not always correlate with each other, andtherefore patient-derived information will be essential inevaluating asthma status.
Asthma phenotypes differ from one another and re-spond differently to treatment, and there is variabilitybetween patients, regardless of which outcome is moni-tored. A better understanding of the variability in diseaseand response to treatment and interactions between thepathology of disease and its clinical expression is essentialto the appropriate selection of therapy and maximizationof outcomes.
REFERENCES
1. Ford ES, Mannino DM, Homa DM, Gwynn C, Redd SC, Moriarty DG,
et al. Self-reported asthma and health-related quality of life: findings from
the behavioral risk factor surveillance system. Chest 2003;123:119-27.
2. Shingo S, Zhang J, Reiss TF. Correlation of airway obstruction and
patient-reported endpoints in clinical studies. Eur Respir J 2001;17:220-4.
3. Malmstrom K, Rodriguez-Gomez G, Guerra J, Villaran C, Pineiro A,
Wei LX, et al. Oral montelukast, inhaled beclomethasone, and placebo
for chronic asthma. A randomized, controlled trial. Montelukast/
Beclomethasone Study Group. Ann Intern Med 1999;130:487-95.
4. Szefler SJ, Martin RJ, King TS, Boushey HA, Cherniack RM, Chinchilli
VM, et al. Significant variability in response to inhaled corticosteroids
for persistent asthma. J Allergy Clin Immunol 2002;109:410-8.
5. Chaudhuri R, Livingston E, McMahon AD, Thomson L, Borland W,
Thomson NC. Cigarette smoking impairs the therapeutic response to oral

J ALLERGY CLIN IMMUNOL
VOLUME 115, NUMBER 4
Luskin S545
corticosteroids in chronic asthma. Am J Respir Crit Care Med 2003;168:
1308-15.
6. Zhang J, Yu C, Holgate ST, Reiss TF. Variability and lack of predictive
ability of asthma end-points in clinical trials. Eur Respir J 2002;20:
1102-9.
7. Lazarus SC, Boushey HA, Fahy JV, Chinchilli VM, Lemanske RF,
Sorkness CA, et al. Long-acting beta2-agonist monotherapy vs continued
therapy with inhaled corticosteroids in patients with persistent asthma:
a randomized controlled trial. JAMA 2001;285:2583-93.
8. Bjermer L, Bisgaard H, Bousquet J, Fabbri LM, Greening AP, Haahtela T,
et al. Montelukast and fluticasone compared with salmeterol and
fluticasone in protecting against asthma exacerbation in adults: one year,
double blind, randomised, comparative trial. BMJ 2003;327:891-6.
9. Eisner MD, Ackerson LM, Chi F, Kalkbrenner A, Buchner D, Mendoza
G, et al. Health-related quality of life and future health care utilization for
asthma. Ann Allergy Asthma Immunol 2002;89:46-55.
10. Moy ML, Israel E, Weiss ST, Juniper EF, Dube L, Drazen JM, et al.
Clinical predictors of health-related quality of life depend on asthma
severity. Am J Respir Crit Care Med 2001;163:924-9.
11. Langley SJ, Goldthorpe S, Custovic A, Woodcock A. Relationship
among pulmonary function, bronchial reactivity, and exhaled nitric oxide
in a large group of asthmatic patients. Ann Allergy Asthma Immunol
2003;91:398-404.
12. Chipps B, Sutton L, Emmett A, Dorinsky P. Variability in asthma
severity/control in pediatric asthma patients previously receiving
short-acting beta2-agonists. J Allergy Clin Immunol 2004;113(suppl):
S277.
13. Fuhlbrigge AL, Adams RJ, Guilbert TW, Grant E, Lozano P, Janson SL,
et al. The burden of asthma in the United States: level and distribution are
dependent on interpretation of the national asthma education and
prevention program guidelines. Am J Respir Crit Care Med 2002;166:
1044-9.
14. Asthma in America. 2001. Available at: http://www.asthmainamerica.
com. Accessed March 1, 2004.
15. Lee S, Kirking DM, Erickson SR. Methods of measuring asthma severity
and influence on patient assignment. Ann Allergy Asthma Immunol
2003;91:449-54.
16. Nathan RA, Sorkness CA, Kosinski M, Schatz M, Li JT, Marcus P, et al.
Development of the asthma control test: a survey for assessing asthma
control. J Allergy Clin Immunol 2004;113:59-65.
17. Green RH, Brightling CE, McKenna S, Hargadon B, Parker D, Bradding
P, et al. Asthma exacerbations and sputum eosinophil counts: a rando-
mised controlled trial. Lancet 2002;360:1715-21.
18. Sont JK, Willems LN, Bel EH, van Krieken JH, Vandenbroucke JP, Sterk
PJ. Clinical control and histopathologic outcome of asthma when using
airway hyperresponsiveness as an additional guide to long-term treatment.
TheAMPULStudyGroup. Am JRespir Crit CareMed 1999;159:1043-51.
19. Strine TW, Ford ES, Balluz L, Chapman DP, Mokdad AH. Risk
behaviors and health-related quality of life among adults with asthma:
the role of mental health status. Chest 2004;126:1849-54.
20. Sullivan SD, Crown WH, Bresnahan BW, Orsini LS, Kennedy S, Luskin
AT. Healthcare utilization and expenditures: a study of asthma patients
with exacerbations in the United States. J Managed Care Pharm. In press
2005.