Embed Size (px)
Citation preview
11/20/2015
1
Everything You Ever Wanted to Know About PNH(but didn’t know to ask!)
Lawrence Rice, MDChief, Division of HematologyHouston Methodist HospitalProfessor of MedicineWeill Cornell Medical CollegeHouston, Texas
25 yo woman referred for anemia
3 year hx episodic red urine, every 2 months, lasting hours to days, usually beginning on awakening in the morning
Associated Sx: substernal tightness and difficulty swallowing with episodes; chronic profound fatigue
Prior w/u (all negative): urine cultures, IVP, cystoscopies
Rxs: antibiotics; oral iron
Hgb 9.5, WBC 4.1, plate 225K, MCV110
Further w/u:Reticulocytes 7%; ferritin 38
Urine hgb and hemosiderin + (no RBC)
Ham’s Acidified Serum and Sucrose
Hemolysis tests strongly +
Dx: PNH
The year was 1976!
I can’t even pronounce what you’ve got!
Machiafava – Micheli Disease
PNH for 39 years Subsequent flow cytometries: clone size 80% Rx over the years: few days prednisone 3X/yr
often aborts hemolytic episodes
Hemoglobin levels 7.5 – 10.3 2004: Pulmonary Embolus
Coumadin ever since; also got first RBC Tx
2006: Most severe hemolytic episode; Tx 4 units; creatinine to 6.5, rapidly improved
2009: Last RBC Tx 2011: Rising creatinine (2.4)
11/20/2015
2
What is PNH? An acquired intracorpuscular RBC defect
arising from a stem cell PIG-A mutation(s)
1,500 – 5,000 affected in US (≥ 5 per
million); more people study it than have it
Illustrates important scientific insights can emerge from dissecting rare disorders
Median age of diagnosis is early 30’s
Diminished quality of life and shortened survival Chronic Intravascular Hemolysis Thrombosis occurs in about 40% of patients
Pathophysiology of PNH
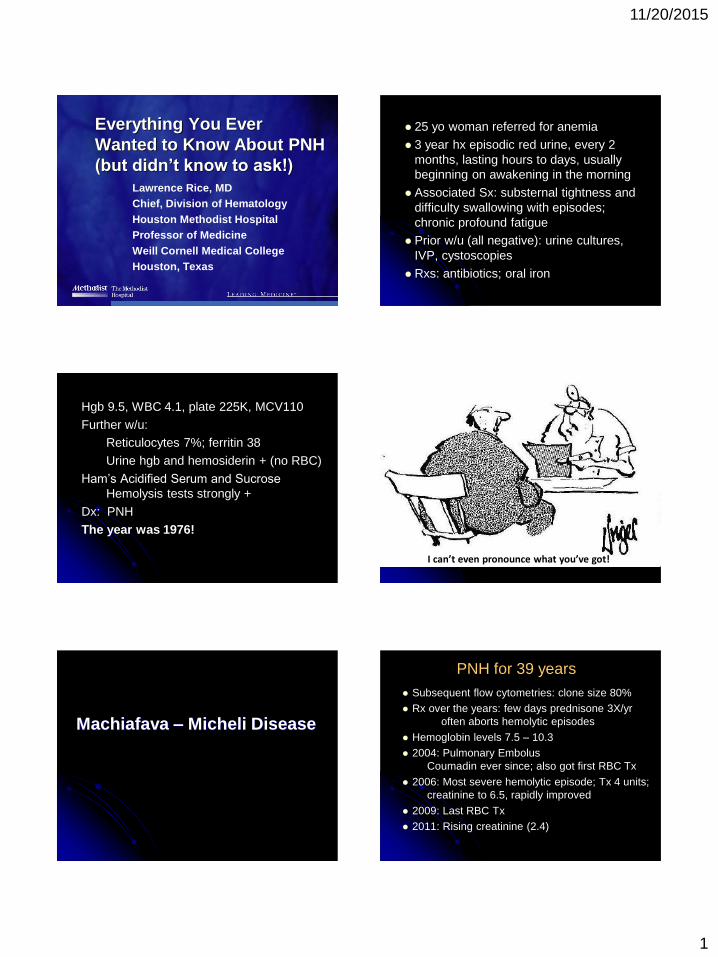
GPI Anchor Defect in PNH
2 2CH CH CH
C=O
O
O
O-P-O
O
O
(18:0,1)
(22:4,5)
C=O
Asp
C=O2 2
O
O=P=O
O
O
CH CH CH
C=O
O
CH2
CH2
NH
CH2
CH2
NH
O2
O
O-P=O
O-P-O
O
O
(18:0,1)
(22:4,5)
(16:0)
N
( 1-2)
( 1-6)
( 1-4)
PROTEIN
NORMAL PNH
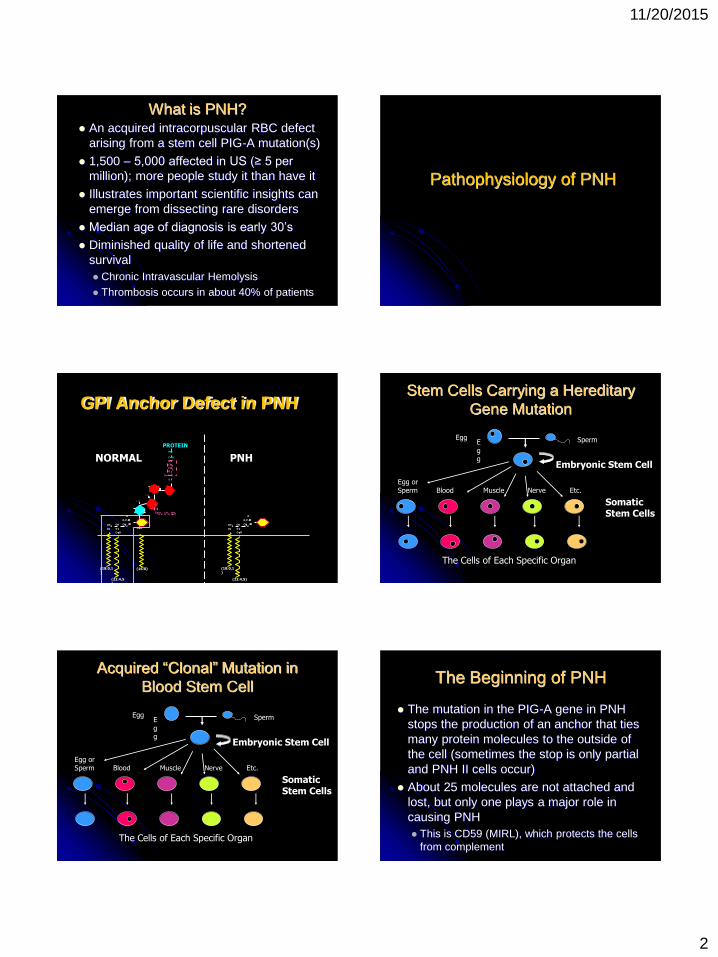
Stem Cells Carrying a Hereditary Gene Mutation
Embryonic Stem Cell
Somatic Stem Cells
Blood Muscle Nerve Etc.Egg or Sperm
Egg
Egg Sperm
The Cells of Each Specific Organ
Acquired “Clonal” Mutation in
Blood Stem Cell
Embryonic Stem Cell
Somatic Stem Cells
Blood Muscle Nerve Etc.Egg or Sperm
Egg
Egg Sperm
The Cells of Each Specific Organ
The Beginning of PNH
The mutation in the PIG-A gene in PNH stops the production of an anchor that ties many protein molecules to the outside of the cell (sometimes the stop is only partial and PNH II cells occur)
About 25 molecules are not attached and lost, but only one plays a major role in causing PNH This is CD59 (MIRL), which protects the cells
from complement
11/20/2015
3
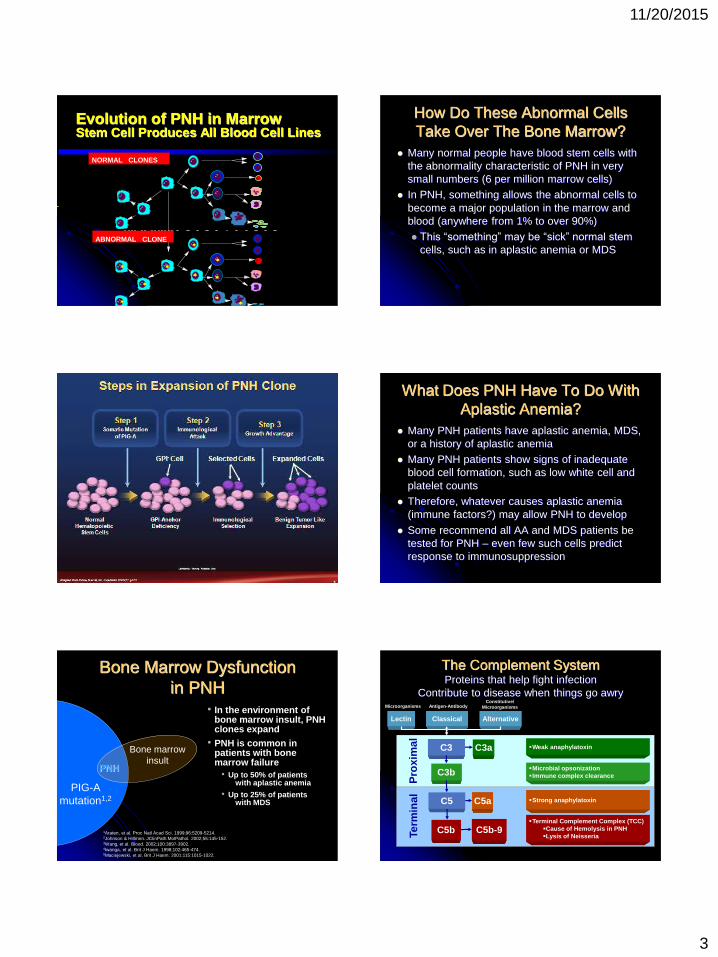
Evolution of PNH in MarrowStem Cell Produces All Blood Cell Lines
ABNORMAL CLONE
NORMAL CLONES
How Do These Abnormal Cells Take Over The Bone Marrow?
Many normal people have blood stem cells with the abnormality characteristic of PNH in very small numbers (6 per million marrow cells)
In PNH, something allows the abnormal cells to become a major population in the marrow and blood (anywhere from 1% to over 90%) This “something” may be “sick” normal stem
cells, such as in aplastic anemia or MDS
What Does PNH Have To Do With Aplastic Anemia?
Many PNH patients have aplastic anemia, MDS, or a history of aplastic anemia
Many PNH patients show signs of inadequate blood cell formation, such as low white cell and platelet counts
Therefore, whatever causes aplastic anemia (immune factors?) may allow PNH to develop
Some recommend all AA and MDS patients be tested for PNH – even few such cells predict response to immunosuppression
Bone Marrow Dysfunction in PNH
PNH
Bone marrowinsult
• In the environment of bone marrow insult, PNH clones expand
• PNH is common in patients with bone marrow failure
• Up to 50% of patients with aplastic anemia
• Up to 25% of patients with MDS
1Araten, et al. Proc Natl Acad Sci. 1999;96:5209-5214.2Johnson & Hillmen. JClinPath:MolPathol. 2002;55:145-152.3Wang, et al. Blood. 2002;100:3897-3902.4Iwanga, et al. Brit J Haem. 1998;102:465-474.5Maciejewski, et al. Brit J Haem. 2001;115:1015-1022.
PIG-Amutation1,2
The Complement SystemProteins that help fight infection
Contribute to disease when things go awry
Lectin Classical Alternative
C3 C3a
C3b
C5 C5a
C5b
Weak anaphylatoxin
Microbial opsonizationImmune complex clearance
Strong anaphylatoxin
Terminal Complement Complex (TCC)Cause of Hemolysis in PNHLysis of Neisseria
Pro
xim
alTe
rmin
al
Microorganisms Antigen-AntibodyConstitutive/
Microorganisms
C5b-9
11/20/2015
4
August_20_2010US
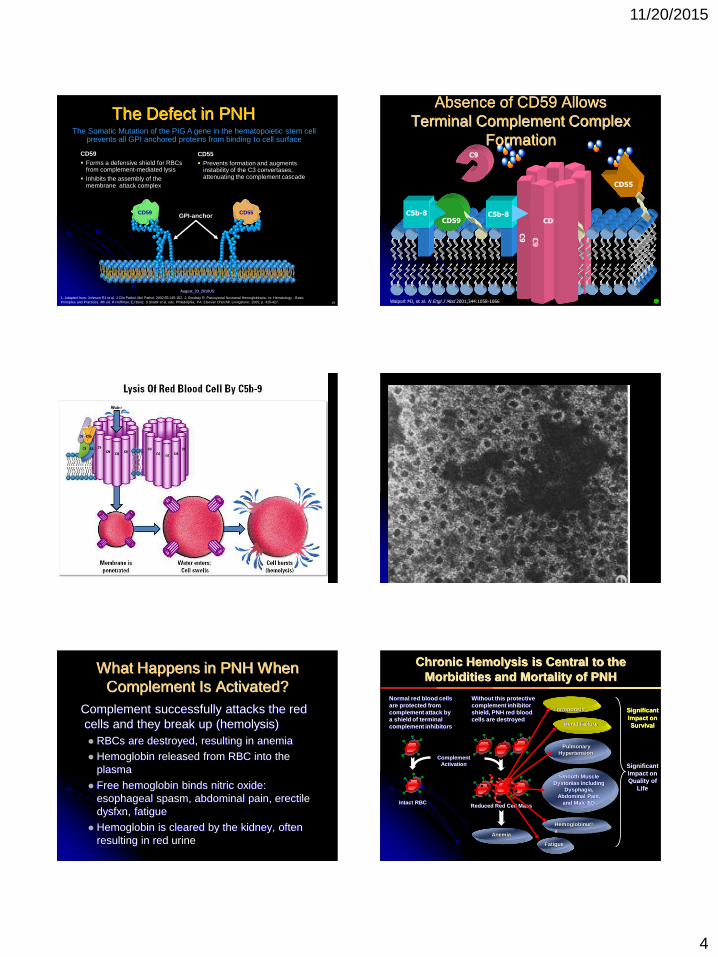
The Defect in PNH
CD55
The Somatic Mutation of the PIG A gene in the hematopoietic stem cell prevents all GPI anchored proteins from binding to cell surface
19
1. Adapted from: Johnson RJ et al. J Clin Pathol: Mol Pathol. 2002;55:145-152. 2. Brodsky R. Paroxysmal Nocturnal Hemoglobinuria. In: Hematology - Basic Principles and Practices. 4th ed. R Hoffman; EJ Benz; S Shattil et al, eds. Philadelphia, PA: Elsevier Churchill Livingstone; 2005; p. 419-427.
CD59 GPI-anchor
CD55 Prevents formation and augments
instability of the C3 convertases, attenuating the complement cascade
CD59 Forms a defensive shield for RBCs
from complement-mediated lysis
Inhibits the assembly of the membrane attack complex
Absence of CD59 Allows Terminal Complement Complex
Formation
C5b-8 C5b-8
CD55
CD59
C9
C9 C
9
CD59
Walport MJ, et al. N Engl J Med 2001;344:1058-1066 +
What Happens in PNH When Complement Is Activated?
Complement successfully attacks the red cells and they break up (hemolysis) RBCs are destroyed, resulting in anemia Hemoglobin released from RBC into the
plasma
Free hemoglobin binds nitric oxide: esophageal spasm, abdominal pain, erectile dysfxn, fatigue
Hemoglobin is cleared by the kidney, often resulting in red urine
Hemoglobinuria
Thrombosis
Fatigue
Renal Failure
Significant Impact on Quality of
Life
Significant Impact on Survival
Smooth Muscle Dystonias including
Dysphagia,Abdominal Pain,
and Male ED
Pulmonary Hypertension
Normal red blood cells are protected from complement attack by a shield of terminal complement inhibitors
Without this protective complement inhibitor shield, PNH red blood cells are destroyed
Intact RBC
ComplementActivation
Reduced Red Cell Mass
Anemia
Chronic Hemolysis is Central to the Morbidities and Mortality of PNH
11/20/2015
5
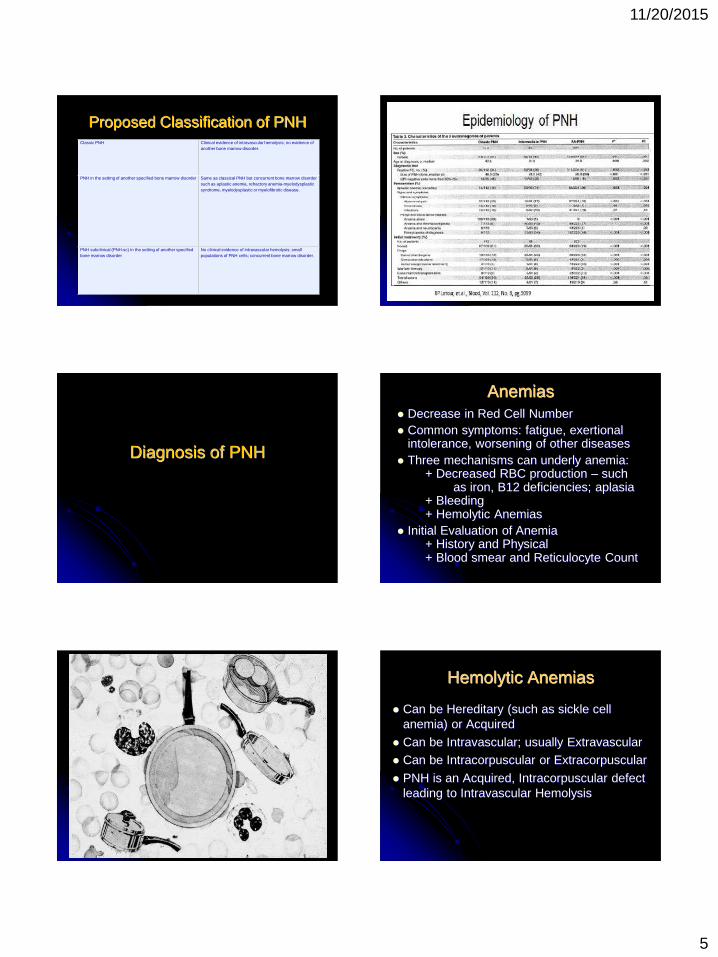
Proposed Classification of PNH Classic PNH Clinical evidence of intravascular hemolysis; no evidence of
another bone marrow disorder.
PNH in the setting of another specified bone marrow disorder Same as classical PNH but concurrent bone marrow disorder such as aplastic anemia, refractory anemia-myelodysplastic syndrome, myelodysplastic or myelofibrotic disease.
PNH subclinical (PNH-sc) in the setting of another specified bone marrow disorder
No clinical evidence of intravascular hemolysis; small populations of PNH cells; concurrent bone marrow disorder.
Diagnosis of PNH
Anemias Decrease in Red Cell Number Common symptoms: fatigue, exertional
intolerance, worsening of other diseases Three mechanisms can underly anemia:
+ Decreased RBC production – such as iron, B12 deficiencies; aplasia
+ Bleeding+ Hemolytic Anemias
Initial Evaluation of Anemia+ History and Physical+ Blood smear and Reticulocyte Count
Hemolytic Anemias
Can be Hereditary (such as sickle cell anemia) or Acquired
Can be Intravascular; usually Extravascular Can be Intracorpuscular or Extracorpuscular
PNH is an Acquired, Intracorpuscular defect leading to Intravascular Hemolysis
11/20/2015
6
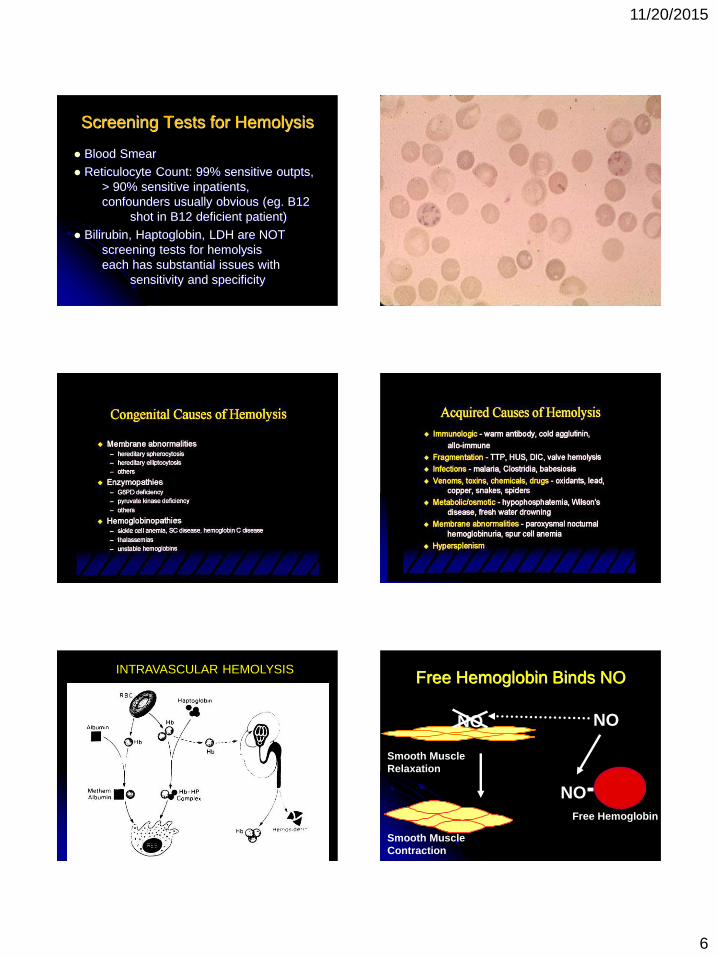
Screening Tests for Hemolysis
Blood Smear
Reticulocyte Count: 99% sensitive outpts,> 90% sensitive inpatients,confounders usually obvious (eg. B12
shot in B12 deficient patient)
Bilirubin, Haptoglobin, LDH are NOT screening tests for hemolysiseach has substantial issues with
sensitivity and specificity
INTRAVASCULAR HEMOLYSIS Free Hemoglobin Binds NO
Smooth MuscleContraction
Smooth MuscleRelaxation
NONO
NOFree Hemoglobin
11/20/2015
7
Which Patients Should Be Screened For PNH?
Hemoglobinuria Hemolytic anemia Bone marrow dysfunction
Aplastic anemia (AA) or MDS screened annually Coombs-negative intravascular hemolysis
Elevated serum LDH Unusual or unexplained venous thrombosis
Budd-Chiari syndrome Mesenteric, portal, cerebral, or dermal veins
Unexplained arterial thrombosis Episodic dysphagia or abdominal pain with
evidence of chronic hemolysis.
Red Urine?Me Do Cystoscopy
Who Is Smarter Here?
Joe Urologist
Engelbert Internist
Red Urine can be Hematuria,Hemoglobinuria,
Myoglobinuria, Porphyrins,Dipyrroles, Drugs,
Eating too many beets…
Who Is Smarter Here? Or, Why Don’t More Doctors
Go Into Primary Care?
Internal Med H & P (Intermed) $280
Urology H & P $280-545Cystoscopy, Urologist Fee $1,081
Chronic Hemolysis is Central to the Symptoms and Complications of PNH
1Parker, et al. Blood. 2005;106:3699-3709. 2Brodksy. Paroxysmal Nocturnal Hemoglobinuria. In: Hematology - Basic Principles and Practices. 4th ed. R Hoffman; EJ Benz; S Shattil et al, eds. Philadelphia, PA: Elsevier Churchill Livingstone; 2005; p. 419-427. 3Hillmen, et al. N Engl J Med. 1995;333:1253-1258. 4Rosse, et al. Hematology (Am Soc Hematol Educ Program). 2004:48-62. 5Rother, et al. JAMA. 2005;293:1653-1662. 6Socie, et al. Lancet. 1996;348:573-577. 7SOLIRIS® (eculizumab) [package insert]. Alexion Pharmaceuticals; 2007.
SMOOTH MUSCLEDYSTONIA
Abdominal pain Dysphagia Erectile dysfunction
THROMBOSISVenous:
MI
Cerebral Mesenteric
CVA/TIAArterial:
DVT Liver Dermal
IMPAIRED QoL Disabling fatigue Poor physical functioning Pain Dyspnea
ANEMIA Transfusions Fatigue Dyspnea Angina
END ORGAN DAMAGE Kidney GI Liver Brain
1Hill, et al. Blood. 2006;108:972. 2Moyo, et al. Br J Haematol. 2004;126:133-138.3Socie, et al. Lancet. 1996;348:573-577. 4Nishimura, et al. Medicine. 2004;83:193–
207.5Brodsky. Paroxysmal Nocturnal Hemoglobinuria. In: Hoffman, R et al., eds. Hematology - Basic Principles and Practices. 4th ed. 2005; p. 419-427.
PNH Can Be Disabling and Life-Threatening
An estimated 5,000 affected in US
Median age of diagnosis is early 30’s
Diminished quality of life Anemia, dyspnea, pain, and disabling fatigue
Life-threatening Thrombosis occurs in about 40% of patients
Significant Mortality in PNHHillmen, NEJM, 1995
5 year mortality: 35%
Median time from Dx to death: 10 yrs
100
80
60
40
20
00 5 10 15 20 25
Years After Diagnosis
Pat
ien
ts S
urv
ivin
g (
%)
Age- and Sex-Matched Controls
Patients With PNH
11/20/2015
8
Hillmen et al., NEJM, 1995;333:1253-8. De Latour RP et al., Blood, 2008;112:3099-3106.
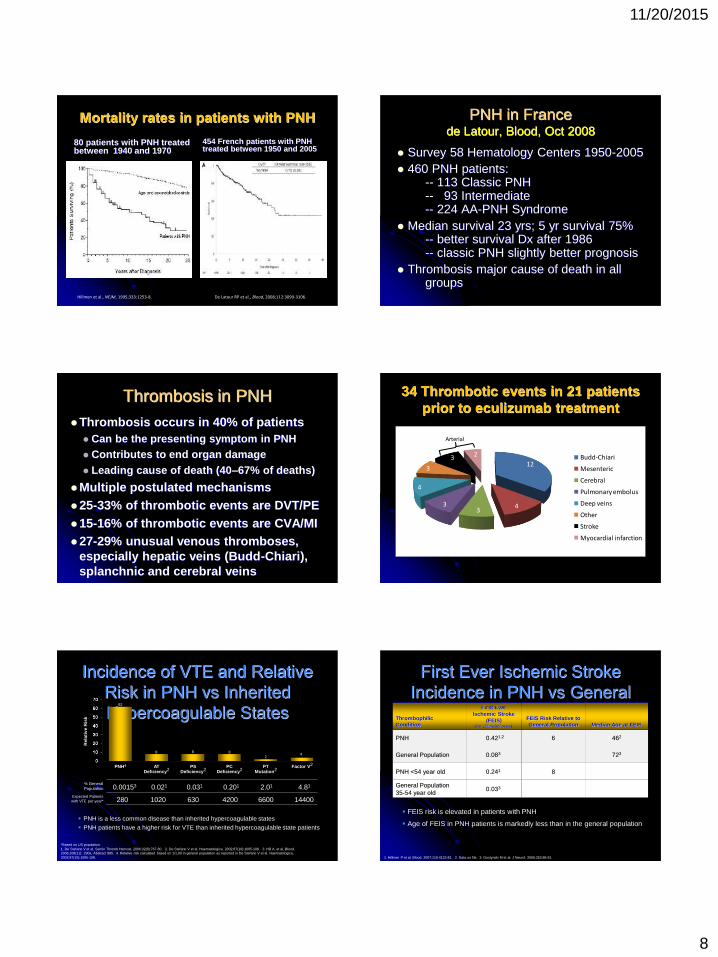
Mortality rates in patients with PNH
80 patients with PNH treated between 1940 and 1970
454 French patients with PNH treated between 1950 and 2005
PNH in Francede Latour, Blood, Oct 2008
Survey 58 Hematology Centers 1950-2005 460 PNH patients:
-- 113 Classic PNH-- 93 Intermediate-- 224 AA-PNH Syndrome
Median survival 23 yrs; 5 yr survival 75%-- better survival Dx after 1986-- classic PNH slightly better prognosis
Thrombosis major cause of death in all groups
Thrombosis in PNHThrombosis occurs in 40% of patients
Can be the presenting symptom in PNH Contributes to end organ damage Leading cause of death (40–67% of deaths)
Multiple postulated mechanisms 25-33% of thrombotic events are DVT/PE15-16% of thrombotic events are CVA/MI27-29% unusual venous thromboses,
especially hepatic veins (Budd-Chiari), splanchnic and cerebral veins
34 Thrombotic events in 21 patients prior to eculizumab treatment
12
43
3
4
3
3 2 Budd-Chiari
Mesenteric
Cerebral
Pulmonary embolus
Deep veins
Other
Stroke
Myocardial infarction
Arterial
Incidence of VTE and Relative Risk in PNH vs Inherited Hypercoagulable States
PNH is a less common disease than inherited hypercoagulable states PNH patients have a higher risk for VTE than inherited hypercoagulable state patients
PNH4 ATDeficiency2
PSDeficiency2
PCDeficiency2
PTMutation2
Factor V2
% GeneralPopulation
Expected Patientswith VTE per year*
Rel
ativ
e R
isk
0.00153 0.021 0.031 0.201 2.01 4.81
280 1020 630 4200 6600 14400
62
8 8 82
4
*Based on US population1. De Stefano V et al. Semin Thromb Hemost. 2006;32(8):767-80. 2. De Stefano V et al. Haematologica. 2002;87(10):1095-108. 3. Hill A, et al. Blood. 2006;108(11): 290a. Abstract 985. 4. Relative risk calculated based on 1/1,00 in general population as reported in De Stefano V et al. Haematologica. 2002;87(10):1095-108.
First Ever Ischemic Stroke Incidence in PNH vs General
Population
1. Hillmen P et al. Blood. 2007;110:4123-81. 2. Data on file. 3. Gostynski M et al. J Neurol. 2006;253:86-91.
FEIS risk is elevated in patients with PNH
Age of FEIS in PNH patients is markedly less than in the general population
Thrombophilic Condition
First Ever Ischemic Stroke
(FEIS) (per 100 patient years)
FEIS Risk Relative to General Population Median Age at FEIS
PNH 0.421,2 6 462
General Population 0.083 723
PNH <54 year old 0.241 8
General Population35-54 year old
0.033
11/20/2015
9
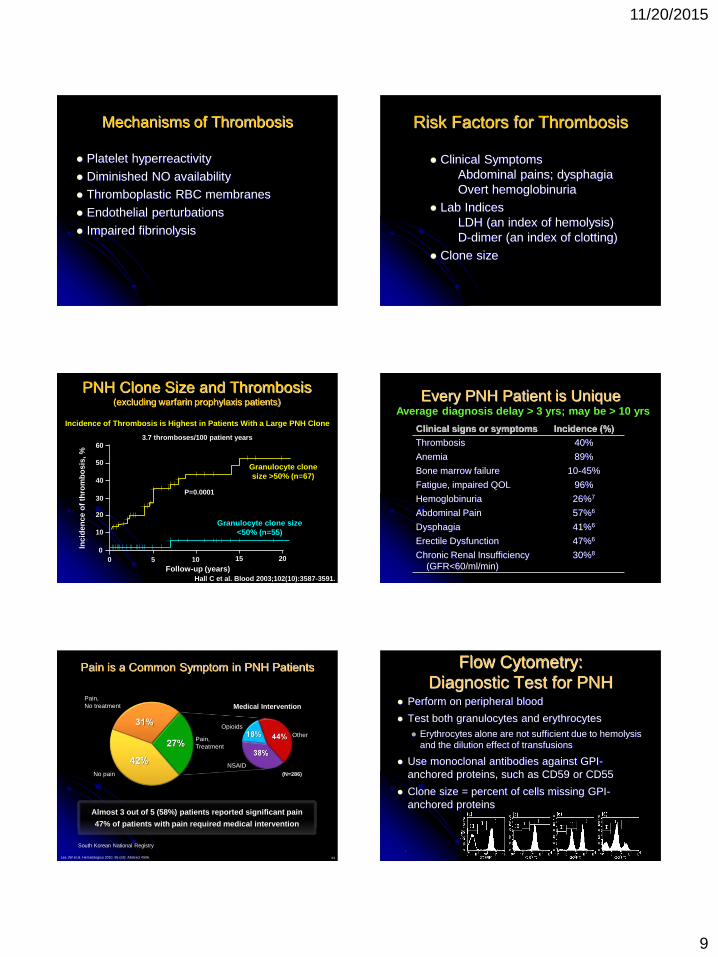
Mechanisms of Thrombosis
Platelet hyperreactivity
Diminished NO availability Thromboplastic RBC membranes
Endothelial perturbations
Impaired fibrinolysis
Risk Factors for Thrombosis
Clinical SymptomsAbdominal pains; dysphagiaOvert hemoglobinuria
Lab Indices LDH (an index of hemolysis)D-dimer (an index of clotting)
Clone size
PNH Clone Size and Thrombosis(excluding warfarin prophylaxis patients)
Hall C et al. Blood 2003;102(10):3587-3591.
0 5 10 15 200
10
20
30
40
50
60
Inci
den
ce o
f th
rom
bo
sis,
%
Granulocyte clone size >50% (n=67)
Granulocyte clone size<50% (n=55)
P=0.0001
Follow-up (years)
3.7 thromboses/100 patient years
Incidence of Thrombosis is Highest in Patients With a Large PNH Clone
Every PNH Patient is UniqueAverage diagnosis delay > 3 yrs; may be > 10 yrs
Clinical signs or symptoms Incidence (%)
Thrombosis 40%
Anemia 89%
Bone marrow failure 10-45%
Fatigue, impaired QOL 96%
Hemoglobinuria 26%7
Abdominal Pain 57%6
Dysphagia 41%6
Erectile Dysfunction 47%6
Chronic Renal Insufficiency (GFR<60/ml/min)
30%8
53
Pain is a Common Symptom in PNH Patients
Almost 3 out of 5 (58%) patients reported significant pain
47% of patients with pain required medical intervention
Lee JW et al. Hematologica 2010. 95 (s2): Abstract #506.
No pain
Pain, No treatment
Pain, Treatment
NSAID
OtherOpioids
Medical Intervention
(N=286)
South Korean National Registry
Flow Cytometry: Diagnostic Test for PNH
Perform on peripheral blood
Test both granulocytes and erythrocytes Erythrocytes alone are not sufficient due to hemolysis
and the dilution effect of transfusions
Use monoclonal antibodies against GPI-anchored proteins, such as CD59 or CD55
Clone size = percent of cells missing GPI-anchored proteins
.
11/20/2015
10
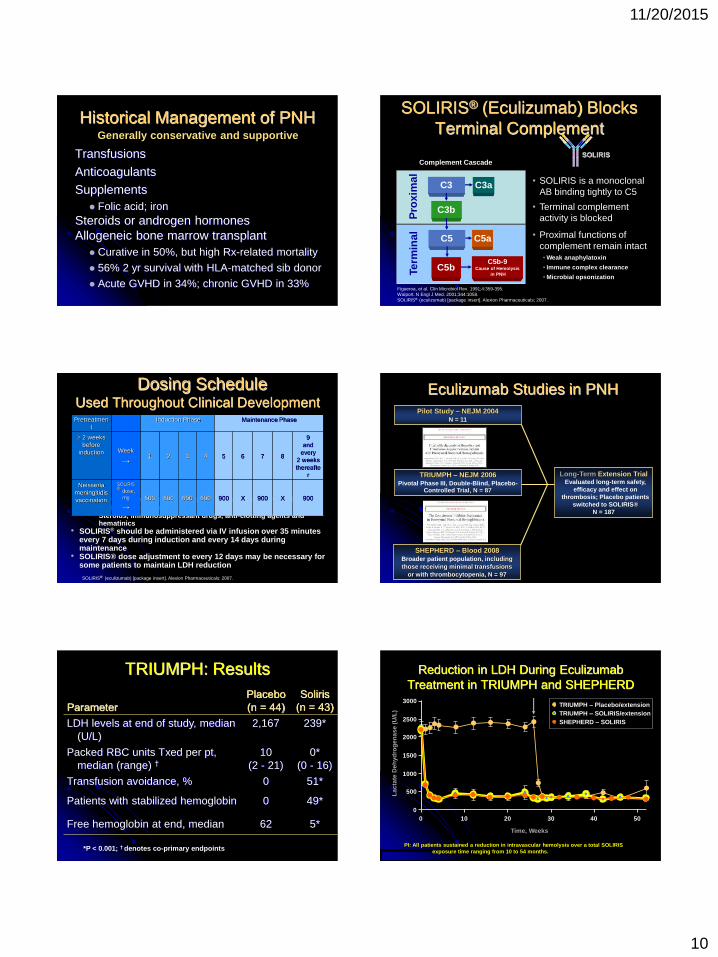
Historical Management of PNH
Transfusions
AnticoagulantsSupplements
Folic acid; ironSteroids or androgen hormones Allogeneic bone marrow transplant
Curative in 50%, but high Rx-related mortality
56% 2 yr survival with HLA-matched sib donor
Acute GVHD in 34%; chronic GVHD in 33%
Generally conservative and supportive
SOLIRIS® (Eculizumab) Blocks Terminal Complement
C3 C3a
C3b
C5
Pro
xim
alTe
rmin
al
Figueroa, et al. Clin Microbiol Rev. 1991;4:359-395.Walport. N Engl J Med. 2001;344:1058.SOLIRIS® (eculizumab) [package insert]. Alexion Pharmaceuticals; 2007.
C5b-9Cause of Hemolysis
in PNH
C5a
C5b
SOLIRIS
• Proximal functions of complement remain intact
• Weak anaphylatoxin
• Immune complex clearance
• Microbial opsonization
• Terminal complement activity is blocked
• SOLIRIS is a monoclonal AB binding tightly to C5
Complement Cascade
Dosing Schedule Used Throughout Clinical Development
• All patients were vaccinated against Neisseria meningitidis• Concomitant medications allowed:
• Steroids, immunosuppressant drugs, anti-clotting agents and hematinics
• SOLIRIS® should be administered via IV infusion over 35 minutes every 7 days during induction and every 14 days during maintenance
• SOLIRIS® dose adjustment to every 12 days may be necessary for some patients to maintain LDH reduction
Pretreatment
Induction Phase Maintenance Phase
2 weeks before
induction Week
→1 2 3 4 5 6 7 8
9and
every2 weeks thereafte
r
Neisseria meningitidisvaccination
SOLIRIS ® dose,
mg
→
600 600 600 600 900 X 900 X 900
SOLIRIS® (eculizumab) [package insert]. Alexion Pharmaceuticals; 2007.
Long-Term Extension Trial Evaluated long-term safety,
efficacy and effect on thrombosis; Placebo patients
switched to SOLIRIS®N = 187
Pilot Study – NEJM 2004N = 11
TRIUMPH – NEJM 2006 Pivotal Phase III, Double-Blind, Placebo-
Controlled Trial, N = 87
SHEPHERD – Blood 2008Broader patient population, includingthose receiving minimal transfusions
or with thrombocytopenia, N = 97
Eculizumab Studies in PNH
TRIUMPH: Results
ParameterPlacebo(n = 44)
Soliris(n = 43)
LDH levels at end of study, median (U/L)
2,167 239*
Packed RBC units Txed per pt,median (range) †
10(2 - 21)
0*(0 - 16)
Transfusion avoidance, % 0 51*
Patients with stabilized hemoglobin 0 49*
Free hemoglobin at end, median 62 5*
*P < 0.001; † denotes co-primary endpoints
Reduction in LDH During Eculizumab Treatment in TRIUMPH and SHEPHERD
Time, Weeks
Lac
tate
Deh
ydro
gen
ase
(U/L
)
0
500
1000
1500
2000
2500
3000
0 10 20 30 40 50
TRIUMPH – Placebo/extensionTRIUMPH – SOLIRIS/extensionSHEPHERD – SOLIRIS
PI: All patients sustained a reduction in intravascular hemolysis over a total SOLIRIS exposure time ranging from 10 to 54 months.
11/20/2015
11
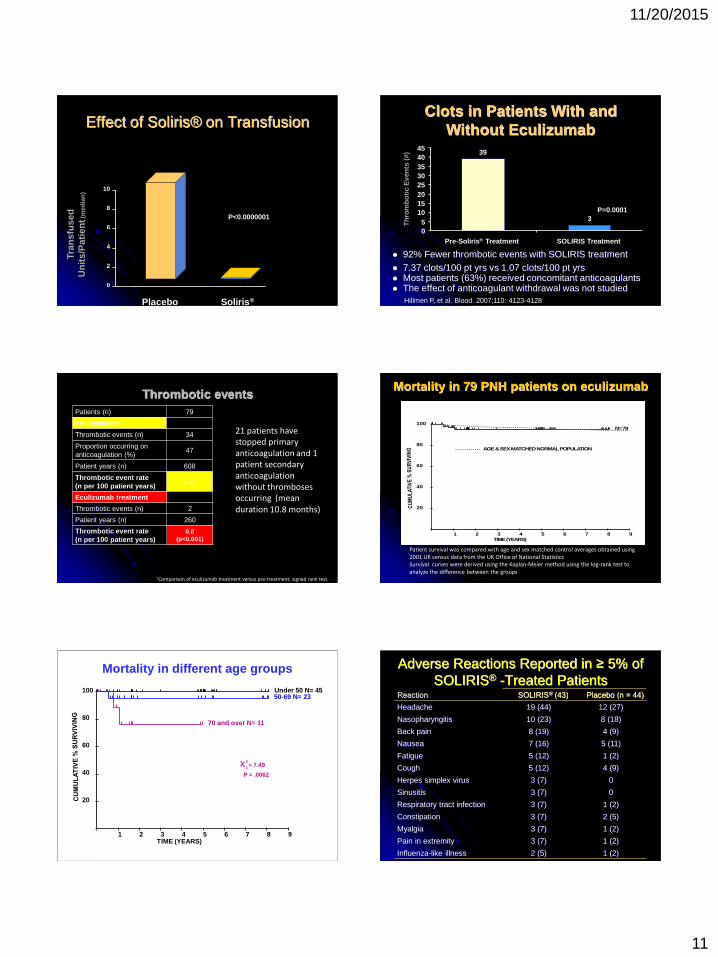
Effect of Soliris® on Transfusion
P<0.0000001
Tran
sfu
sed
Un
its/
Pat
ien
t(m
edia
n)
Soliris®Placebo
0
2
4
6
8
10
Clots in Patients With and Without Eculizumab
92% Fewer thrombotic events with SOLIRIS treatment 7.37 clots/100 pt yrs vs 1.07 clots/100 pt yrs Most patients (63%) received concomitant anticoagulants The effect of anticoagulant withdrawal was not studied
Hillmen P, et al. Blood. 2007;110: 4123-4128
39
3
05
1015202530354045
Pre-Soliris® Treatment SOLIRIS Treatment
Th
rom
bo
tic
Eve
nts
(#)
P=0.0001
Thrombotic eventsPatients (n) 79
Pre-treatment
Thrombotic events (n) 34
Proportion occurring on anticoagulation (%)
47
Patient years (n) 608
Thrombotic event rate (n per 100 patient years)
5.60
Eculizumab treatment
Thrombotic events (n) 2
Patient years (n) 260
Thrombotic event rate (n per 100 patient years)
0.8(p<0.001)
1Comparison of eculizumab treatment versus pre-treatment; signed rank test.
21 patients have stopped primary anticoagulation and 1 patient secondary anticoagulation without thromboses occurring (mean duration 10.8 months)
1 2 3 4 5 6 7 8 9
20
40
60
80
100
TIME (YEARS)
N= 79
AGE & SEX MATCHED NORMAL POPULATION
Mortality in 79 PNH patients on eculizumab
Patient survival was compared with age and sex matched control averages obtained using 2001 UK census data from the UK Office of National StatisticsSurvival curves were derived using the Kaplan-Meier method using the log-rank test to analyze the difference between the groups
P=0.46
1 2 3 4 5 6 7 8 9
20
40
60
80
100
TIME (YEARS)
Under 50 N= 4550-69 N= 23
70 and over N= 11
2
1 = 7.49
P = .0062
Mortality in different age groups Adverse Reactions Reported in ≥ 5% of SOLIRIS® -Treated Patients
Reaction SOLIRIS® (43) Placebo (n = 44)
Headache 19 (44) 12 (27)
Nasopharyngitis 10 (23) 8 (18)
Back pain 8 (19) 4 (9)
Nausea 7 (16) 5 (11)
Fatigue 5 (12) 1 (2)
Cough 5 (12) 4 (9)
Herpes simplex virus 3 (7) 0
Sinusitis 3 (7) 0
Respiratory tract infection 3 (7) 1 (2)
Constipation 3 (7) 2 (5)
Myalgia 3 (7) 1 (2)
Pain in extremity 3 (7) 1 (2)
Influenza-like illness 2 (5) 1 (2)
11/20/2015
12
What Does Soliris® Do?
Quickly and markedly reduces hemolysisImproves anemia (may not be normal)Markedly reduces transfusion needs
Reduces symptoms assoc. with hemolysis fatigue, esophageal spasm, abdominal pain, erectile dysfxn
Appears to reduce thrombosisMay change role of blood thinners
What is Eculizumab NOT expected to Do?
Does not improve genetic defect
Does not improve impaired hematopoiesis(bone marrow dysfunction) Low white count or low platelet count persist
Some shortcomings of Eculizumab
Does not address genetic defect Does not address underlying marrow dysfunction
Extravascular hemolysis (C3-mediated) may continue
Risk of Hemolytic Crisis with sudden withdrawal
Susceptibility to meningococcemia/ meningitis More rapid metabolism in some patients
Very rare genetic resistance (C5 mutation)
Cost Inconvenience (IV infusion every 12-14 days)
PNH Summary
A rare but fascinating blood disorder Incredibly well-understood down to genetic
and molecular levels Myriad manifestations, most importantly:
+ intravascular hemolytic anemia+ clotting tendency, including unusual
sites Scientific understanding increasing rapidly Targeted therapy now available; more
options on the horizon
Wonderful…Just Wonderful! So much
for instilling them with a sense of awe…