-
8/3/2019 What is Opcab
1/17
What is OPCAB?
The off-pump technique, also known as OPCAB, is very
similar to the conventional Coronary Artery Bypass Grafting
(CABG) procedure. OPCAB still utilizes a medial sternotomy,
however the important difference is that the cardiopulmonary
bypass pump is no longer employed.
Procedure:
OPCAB was developed from the minimally invasive
school of thought, so the basic premise is to reduceincision
sizes. A surgeon will perform median
sternotomy of varying sizes (depending on the
physiology of the patient, the smallest incision will be
made). Arteries or veins can be harvested from the
patients chest wall, arm, and or leg.
To aid the surgeon in operating on the beating
heart, drugs such as Adenosine and Esmolol are
used to slow the heart rate. To allow for access tothe entire
heart, there must be a sufficient amount
of cardiac displacement. This is accomplished by
deep pericardial sutures and the use of specialized
instruments to prop the heart in a position that will
allow the surgeon to access occluded arteries.
Once within the pericardial sac, sponges are used to
reduce free blood in the region being operated on. The
sponges also serve as a way to displace the heart,
allowing a clear view of the region for anastomosis.
With the heart still beating, there is a greater difficulty
in performing a bypass on the posterior and lateral wallsof the
heart. Surgeons have found many ways to
stabilize the heart in order to bypass the necessary
arteries. Along with sponges, some surgeons will use
slings to prop the heart in the necessary positions and
then utilize a stabilizer to focus on a particular occluded
artery. Biotechnical firms have also developed products
such as the Octopus that help to stabilize pertinent
regions of that heart during surgery. Some surgeons will
prepare the patient for attachment to the
cardiopulmonary bypass pump in case of an emergency
or accident that might occur during the operation. This
is precautionary and not all surgeons will choose to doso.
-
8/3/2019 What is Opcab
2/17
The length of the operation depends on a number of variables.
Much like CABG, the number of occlusions can
greatly effect the length of time on the operating table. The
removal of the cardiopulmonary bypass pump does
reduce time since it does not need to be attached and the heart
does not need to be reanimated. However, the beating
heart must be handled with a great amount of care. To reach an
artery on the lateral wall of the heart, the heart must
be propped and stabilized, all of which can add to the length of
the operation.
Techniques and Instrumentation used to Operate on a Beating
Heart
Minimally invasive procedures which are done on a beating heart
and do not use cardiopulmonary bypass (the heart-lung machine),
such
asMIDCABand OPCABoperations, are called off-pump procedures.
These off-pump procedures require special techniques
andinstrumentation in order to perform efficient and reliable
anastomosis on the beating heart. Click on the heading for a page
describing these
techniques and instrumentation.
Surgery Comparisons
Click on the heading for a page with a table comparing the
basics between all minimally invasive surgeries, or continue for
in-
depth analysis of OPCAB vs. CABG and OPCAB vs. MIDCAB.
OPCAB vs. CABG
There are a number of studies being done on all types of
minimally invasive surgeries. The studies in progress offer a
short-term
look at the reliability of minimally invasive procedures.
In a study performed by the Cardiac Surgical Associates, P.A. in
Minneapolis, Minnesota, the comparison of OPCAB to CABG
patients showed that (by percentage) OPCAB had similar or better
results.
Stroke
N (%)
New Renal
Failure N (%)
New Atrial
Fib N (%)
Mortality
N (%)
Low Risk On PumpN=2360
30 (1.3) 99 (4.2) 500 (21.2) 27 (1.1)
0-2.59 Off Pump
N=216
2 (0.9) 7 (3.2) 26 (12.0) 3 (1.4)
N=2576 P-value 1.0 0.499 0.001 0.736
MediumRisk
On PumpN=688
29 (4.2) 71 (10.3) 187 (27.2) 45 (6.5)
2.6-9.9 Off Pump
N=95
3 (3.2) 9 (9.5) 17 (17.9) 6 (6.3)
N=783 P-value 0.787 0.799 0.053 0.934
High Risk On PumpN=123
6 (4.9) 26 (21.1) 34 (27.6) 35 (28.5)
>10 Off Pump
N=39
0 (0) 1 (2.6) 7 (17.9) 3 (7.7)
http://biomed.brown.edu/Courses/BI108/BI108_2000_Groups/Heart_Surgery/Instrumentation.htmlhttp://biomed.brown.edu/Courses/BI108/BI108_2000_Groups/Heart_Surgery/MIDCAB.htmlhttp://biomed.brown.edu/Courses/BI108/BI108_2000_Groups/Heart_Surgery/MIDCAB.htmlhttp://biomed.brown.edu/Courses/BI108/BI108_2000_Groups/Heart_Surgery/Comparisons.htmlhttp://biomed.brown.edu/Courses/BI108/BI108_2000_Groups/Heart_Surgery/MIDCAB.htmlhttp://biomed.brown.edu/Courses/BI108/BI108_2000_Groups/Heart_Surgery/Comparisons.htmlhttp://biomed.brown.edu/Courses/BI108/BI108_2000_Groups/Heart_Surgery/Instrumentation.html
-
8/3/2019 What is Opcab
3/17
N=162 P-value 0.337 0.006 0.225 0.008
In another study that was presented at an Annual Meeting of the
Society of Thoracic Surgeons,
the following information was found:
The hypothesis for the study was that off-pump surgery would
reduce some of the side effects of conventional
cardiopulmonary bypass surgery that stops the heart and restarts
it after surgery. There were no hospital deaths in
the off-pump group compared to nine deaths in the CABG group.
Off-pump surgery also reduced the averagepostoperative hospital
stay from 5.5 days to 3.3 days. Perhaps the most significant
statistic was the reduction in the
need for transfusion after the operation. Less than a third of
the off-pump patients (29.6 percent) needed
transfusions compared to more than half (56.5 percent) of the
CABG group.
The problem is that there is, and will not be for a number of
years, any data assessing the outcome of an off pump coronary
artery bypass. The clear problem with the lack of data backing
up the OPCAB procedure is why stray from conventional CABG
that has a 99% success rate, as well as success over time.
OPCAB, it is believed, could be performed in 30-40% of coronary
artery bypass situations (60-70% of the time, the physiology
of the patient does not allow for an off-pump procedure). Many
problems with the procedure have been dealt with over the past
few years of development. For example, there were reports of a
decrease in cardiac output by 33%. This was remedied by
volume loading of the right ventricle. Surgeons have also become
more familiar with the procedure and learned that during
OPCAB, the systolic pressure should not be allowed to fall below
100 mmHg.
However, there are some questions about the safety of the
procedure. Critics of OPCAB have presented several issues that
may
make this new procedure a poor alternative to CABG. The
underlying problem is the lack of data supporting the patients
status
five to ten years down the road following bypass surgery using
OPCAB. Another point being made is the sutures may not hold
given that they were made on a beating heart. This point can not
be contested since there is no long-term postoperative data
that
can show that the sutures held allowing for successful
anastomosis. The major risk in OPCAB is that surgeons may not have
a
great deal of experience with the procedure. This could lead to
poor or even fatal outcomes.
Why Avoid The Heart-Lung Machine?
Since the invention of a crude version of the heart-lung machine
in 1955, it has aided surgeons in performing open-heart and
bypass surgeries. Over time, the machine was refined to its
current form, allowing surgeons to carry out open-heart
procedures
with a success rate of nearly 99%. Though the heart-lung machine
has proven to be a major reason for the success of CABG
procedures, there is some pathology associated with its use
[17].
The surface of the tubes that carry the blood to and from the
heart-lung machine are capable of injuring blood cells
While in the tubes of the machine, the blood is subjected to a
considerable amount of external stress forces
Many substances may be caught in the blood stream such as air,
plastic particles, and small blood clots
All of these factors leads to what some doctors call a "whole
body inflammation". Doctors believe complications will increase
with the amount of time a person is left on the cardiopulmonary
pump. Complications inculde:
Swelling of the brain
Infections
Arrhythmia
Kidney stress
Blood vessel damage
Need for transfusion
Low output syndrome
Weight gain
Difficulty planning out complex actions
Release of cytokines leading to a variety of physiologic
events
Irritability
OPCAB vs. MIDCAB
The main reason why a patient may receive OPCAB as opposed to
MIDCAB is the number of vessels that need to be replaced.
In the earlier days of OPCAB, surgeons were only able to reach
blocked arteries on the front wall of the heart. As this
surgical
http://biomed.brown.edu/Courses/BI108/BI108_2000_Groups/Heart_Surgery/MIDCAB.htmlhttp://biomed.brown.edu/Courses/BI108/BI108_2000_Groups/Heart_Surgery/MIDCAB.html
-
8/3/2019 What is Opcab
4/17
method has evolved over the past few years, new devices have
been developed to allow the heart to be displaced from the
protective pericardium. Once exposed, the heart is stabilized
through various methods in various positions. This gives
surgeons
the ability to access arteries on anterior and lateral walls of
the heart. Given this advantage, patients that suffer from
multiple
occlusions may receive OPCAB.
The safety of these two procedures is still in question. OPCAB
and MIDCAB have not been around for more than a few years,
and the long term results are not known. The short-term studies
done on the two procedures have given similar results, both
showing promise of a safe alternative to conventional CABG.
However, the physical condition as well as the number of
occlusions to be removed will be a determinant in choosing OPCAB
over MIDCAB (an over weight patient or a patient with
multiple occlusions would not be eligible for MIDCAB).
Cost:
OPCAB will be a cheaper operation relative to conventional CABG
in several ways. Cost reduction occurs due to:
Cardiopulmonary bypass pump is not used
Shorter postoperative hospital stay due to avoidance of
heart-lung machine
Faster recovery
Note to the Reader
This article is a descriptive summary of anesthetic techniques
for off-pump coronary
artery bypass (OPCAB) surgery. We describe our management
strategies in order to
assist our colleagues who may be encountering OPCAB surgery for
the first time, or
who are interested in different perspectives on management. This
article is not
intended to be a dogmatic approach to the topic, but rather, to
suggest management
strategies in these challenging cases.
Introduction
The anesthetic management for off-pump coronary artery bypass
surgery is
particularly demanding and requires an approach specifically
tailored to the procedure.
OPCAB cases require vigilant anticipation of surgical steps,
skilled hemodynamic
management and close communication with the cardiothoracic
surgeon. Furthermore,
optimal management in OPCAB surgery involves a considerable
learning curve, for the
surgeon, the anesthesiologist and the entire cardiac team. We
present our experience
in the anesthetic management of over 350 cases involving four
different surgeons and
twelve anesthesiologists at our two institutions.
This article will present a brief description of OPCAB surgery
along with some historical
references. Following this is a summary of the advantages of
OPCAB over the
traditional on-pump coronary artery bypass grafting (CABG)
procedure, with pertinent
-
8/3/2019 What is Opcab
5/17
references to the growing literature. Next, the various
anesthetic considerations and
techniques will be described in some detail, with references to
the OPCAB procedure,
as it is relevant. We expect that these particular techniques
will be modified to fit the
experience of individual clinicians, and we anticipate that the
anesthetic management
of these cases will evolve over time.
OPCAB Procedure
Aortocoronary bypass without the use of cardiopulmonary bypass
(CPB) was first
performed by Kolesov (1) in 1964. Others subsequently reported
on the technique,
(2,3,4,5) but it was largely abandoned with the widespread
adoption of cardiopulmonary
bypass (CPB) and cardioplegic arrest. Surgery on the beating
heart re-emerged with
the introduction of so-called minimally invasive procedures.
These surgeries, such as
the minimally invasive direct coronary artery bypass (MIDCAB),
are usually performed
using limited parasternal incisions, special devices to provide
exposure and stabilize
the epicardium, and most often a one or two vessel bypass on a
beating heart, without
the use of CPB. (6,7) However, the use of MIDCAB surgery is
limited because it does not
readily allow for the performance of multiple vessel bypass.
The OPCAB procedure is a natural extension of the more limited
MIDCAB surgery and is
gaining in popularity with the development of devices to better
stabilize the beating
heart. The key surgical features of OPCAB surgery are the
absence of CPB, operation
on a beating heart, use of an epicardial stabilizer, temporary
interruption of coronary
blood flow during microsurgical anastamosis of distal vessels,
and extubation either in
the operating room or shortly thereafter. Rather than a single
(or at most three) vessel
bypass, which would characterize a MIDCAB, our surgeons have
been bypassing as
many as seven vessels during OPCAB.
Advantages of OPCAB
The key advantage of OPCAB surgery is avoidance of the pump.
This fact alone has
numerous ramifications and has been essential in popularizing
both MIDCAB and
OPCAB procedures.
-
8/3/2019 What is Opcab
6/17
In terms of morbidity and mortality, the clearest advantage of
OPCAB is that the
neuropsychologic impairment associated with CPB may be
significantly reduced.
Numerous recent OPCAB studies report fewer than 1% severe
neurologic deficits, such
as completed strokes and coma. (8,9,10) This compares with
incidences of 2-3% for
CABG surgery, depending on preoperative risk factors. (11,12,13)
In addition, we have
observed a decrease in minor neurologic disturbances, most
notably persistent
confusion, after OPCAB surgery. Most off-pump patients are
clearly more alert, and
many of them are ready to sit up and take liquids a few hours
postoperatively.
While OPCAB involves periods of transient coronary ischemia,
this procedure avoids the
potential global myocardial ischemia that may be associated with
CPB. Studies
measuring troponin I levels, a specific marker of myocardial
damage, report that
OPCAB surgery is associated with significantly less release of
the protein. (14,15,16). We
have found, in agreement with published reports, that fewer
inotropes are needed after
the revascularization, there are fewer dysrhythmias (especially
atrial fibrillation) and
there is less need for post-procedure cardiac pacing. (8,
10,17)
In providing anesthesia for OPCAB, we have experienced far fewer
problems with
hemostasis and perioperative bleeding. Use of a lower dose of
heparin, lack of CPB-
associated hemodilution, and absence of pump-related platelet
dysfunction have a
significant effect on perioperative blood loss. The use of
prophylactic antifibrinolytics,
such as aminocaproic acid and aprotinin, is largely unnecessary.
At our institutions, the
transfusion of heterologous blood has been reduced nearly by
one-half, in agreement
with several published reports. (9, 17,18)
Avoiding extracorporeal circulation confers a number of other
advantages. Respiratory
problems are reduced, and even patients with fairly severe COPD
are being extubated
shortly after the procedure. Renal function is better preserved
with OPCAB, as
demonstrated by fewer instances of postoperative renal
insufficiency. (14, 17)
Pharmacokinetics are more predictable since there is no uptake
of drug from the
pump, and there are fewer metabolic perturbations, especially in
glucose, potassium
and calcium. Lastly, OPCAB avoids complement activation and the
systemic
inflammatory response associated with CPB, (19, 20) which may
facilitate postoperative
analgesia and fluid management.
-
8/3/2019 What is Opcab
7/17
Preoperative Considerations
Since early awakening and extubation is an anesthetic goal in
OPCAB surgery,
preoperative sedation should not be heavy. We use relatively
small doses of
benzodiazepines preoperatively and supplement with intravenous
midazolam and
fentanyl in the operating room and during placement of invasive
lines.
To help maintain normothermia, we assure that our OPCAB patients
are warm
preoperatively, even if active warming is necessary. Once in the
operating room, the
patient is placed on a circulating-water mattress and then
covered with a forced-air
warming blanket (BairHugger, WarmAir). All rapidly infusing
intravenous fluids are
warmed. Using these measures, we have not found it necessary to
raise the ambient
room temperature. This emphasis on maintaining normothermia may
facilitate
hemodynamic management and expedite tracheal extubation shortly
after the case.
(21)
As with all cardiac cases, large-bore intravenous access and
central access to the
circulation is necessary. Because these cases often involve
unstable hemodynamics,
especially during distal anastamoses, ready access to the
central circulation is
essential for both bolus dosing and infusions.
Our use of monitoring for OPCAB cases has evolved over time.
ST-segment analysis
has been particularly useful, especially in assessing the
tolerance of the heart for
coronary occlusion during the distal anastamoses. A non-invasive
BP cuff is used to
back up and verify the arterial tracing. The plethysmograph on
the pulse oximeter isvery helpful in assuring adequate
perfusion.
While a pulmonary artery catheter may not be warranted on the
basis of a patients
cardiac status, we have found that preoperative ventricular
function does not
adequately predict any patients response to heart positioning
and coronary occlusion.
Accordingly, it is our current practice that all OPCAB patients
are monitored with
pulmonary artery catheterization and themodilution cardiac
outputs.
-
8/3/2019 What is Opcab
8/17
The use of transesophageal echocardiography (TEE) is limited in
OPCAB cases by the
difficulty in obtaining useful information while the heart is
retracted for many of the
distal anastamoses. With the use of frequent cardiac output
monitoring, we have found
that the TEE has not changed overall management to any
significant degree.
Induction and Initial Maintenance
Because hemodynamic changes occur rapidly and unexpectedly in
OPCAB surgery, we
routinely have a vasodilator and vasopressor/inotrope ready for
immediate infusion.
The choice of these drugs has evolved over time. While
nitroglycerin is used universally
for vasodilation, the selection of vasopressor remains varied,
the most common
choices being phenylephrine, norepinephrine and dopamine.
Likewise, it is useful to
have a number of vasoactive medications readily available for
bolus administration.
The medications we have found most helpful are ephedrine,
phenylephrine (40-100
mcg/ml), epinephrine (10 & 100 mcg/ml), calcium and
lidocaine.
The induction of anesthesia is determined by the patients status
at the time and the
aim to extubate the trachea at the end of the case. Etomidate or
propofol are most
often used for induction, along with a loading dose of opioid.
For most patients a
fentanyl dose of 7.5 to 10 mcg/kg (or sufentanil 0.5-1.0 mcg/kg)
has been adequate to
help blunt the surgical stimulus of incision and sternotomy, yet
also allow for timely
tracheal extubation. Anesthesia is maintained using a volatile
agent, and occasionally,
a propofol infusion is also used. Any of the intermediate-acting
neuromuscular blockers
adequately provide muscle relaxation, while also being readily
reversible.
The heparin dose we use for OPCAB is 1.5-2 mg/kg, aiming to keep
the activated
clotting time (ACT) greater than 300 seconds during vessel
anastamoses. Reports of
systemic anticoagulation vary considerably in the literature,
with heparin doses varying
between 1 and 3 mg/kg, and ACTs usually targeted in the 200-300
range. (17, 22, 23)
While we initially checked the ACT every 20 minutes, we have
found that less frequent
measurements are reasonable.
We have found it to be advantageous to keep the patient well
hydrated for OPCAB
surgery, a practice differing from that in CPB cases where we
attempt to minimize fluid
-
8/3/2019 What is Opcab
9/17
administration. Generous hydration, guided by the pulmonary
artery catheter, helps
alleviate the reduction in preload that occurs when the heart is
retracted, thereby
aiding hemodynamic management. It may also help reduce oliguria
during this period.
After procurement of saphenous vein and skin closure, we place a
sterile forced-air
warmer at the highest setting over the lower part of the body.
This has made a
significant difference in assuring normothermia during the
remainder of the procedure.
To prevent dysrrhythmias during manipulation of the heart and
coronary occlusion, we
routinely give prophylactic doses of bolus lidocaine (1-1.5
mg/kg) and infused
magnesium (2 gm) prior to the first distal anastamosis. (24) We
have a low threshold for
running a lidocaine infusion (2-3 mg/min) and use it routinely
for right coronary artery
grafting. If nitroglycerin is not already infusing, a
nitroglycerin infusion is usually
started prior to suturing the distal anastamoses and is most
often continued
throughout the procedure. In patients with serum potassium less
than 4.0, we routinely
infuse potassium during this period. (25) Lastly, a pacemaker is
readily available in case
pacing on the field is required, especially to treat
bradyarrhythmias associated with the
right coronary artery anastamosis.
We are always prepared to adjust management and maintain
hemodynamics for a
semi-elective or more emergent conversion to CPB. As surgical
experience has grown
with OPCAB, there have been fewer cases where this was
necessary.
Anastamoses
The suturing of the distal anastamoses is by far the most
demanding part of the case.
The anesthesiologist must be continually observing the field,
watching the monitors
and communicating with the surgeon.
Once the surgeon chooses the first vessel for the distal
anastamosis, he places a
silastic tape around it to produce proximal coronary occlusion.
If this is reasonably well
tolerated, he then places the epicardial stabilizing device.
Once this is in position, he
incises the target site and starts the distal anastamosis.
-
8/3/2019 What is Opcab
10/17
During this period of distal anastamosis, there is no turning
back. The consequences
of this temporary coronary occlusion may be relatively
insignificant or may lead to
severe heart failure and ultimately cardiac arrest. It is
helpful to measure serial cardiac
outputs during this period to help determine the need for
resuscitative efforts. In our
experience, cardiac indexes have been as low as 0.7 L/min/m2
during this period. In
addition, the ST segments may become severely elevated or
depressed.
The key to anesthetic management during a distal anastamosis is
to aggressively
maintain hemodynamic stability. In patients where preoperative
cardiac function is
impaired, we often use a background infusion of phenylephrine,
dopamine or
norepinephrine to maintain blood pressure and cardiac output.
Infusion of an inotrope
is also helpful if cardiac output falls significantly after
application of the epicardial
stabilizer. If the cardiac index continues to fall during the
anastamosis (e.g., CI
-
8/3/2019 What is Opcab
11/17
to near baseline levels before the surgeon attempts the next
anastamosis, especially if
it involves displacement of the heart. At times the
anesthesiologist may need to
interrupt the surgeons progress to allow the heart to recover
from a poorly tolerated
period of coronary occlusion.
Subsequent distal anastomoses are carried out in a similar
manner. For certain target
sites, such as the branches of the circumflex artery, deep
pericardial retractors or a
sling may be used to retract the heart into an optimal position
for the surgical
approach. This displacement of the heart, with the apex pointing
anteriorly, causes
right ventricular dysfunction and resultant biventricular pump
failure. This deterioration
in circulatory status is due primarily to a severe reduction in
stroke volume, as the
geometrically distorted right ventricle cannot sufficiently
expand during diastole. (26)
During this retraction phase, the ECG tracing is
characteristically flat and both rhythm
and ST analysis are often indiscernible. If a TEE is being used,
its images of the
retracted heart provide little useful information. Fortunately,
cardiac output
measurements are still possible and plethysmography is often a
reassuring guide of
peripheral perfusion.
To improve the circulatory status during heart displacement, the
patient is placed in
approximately 20-degree Trendelenburg position. As a practical
point, we use special
positioners to keep the patient from shifting on the operating
room table. Steep
Trendelenburg position causes decreases in pulmonary compliance
and functional
residual capacity and may compromise adequate ventilation,
especially in obese
patients.
Once the last distal is in place, the surgeon is ready to apply
a partial cross clamp to
the aorta for placement of the proximal anastamoses. This step
requires a rapid
lowering of blood pressure, usually with volatile agent,
nitroglycerin, or nitroprusside.
The following period of relative calm allows the heart to
recover from the repeated
insults and the anesthesiologist to prepare for closure and
emergence.
Emergence, Extubation, Postop Analgesia
-
8/3/2019 What is Opcab
12/17
Once the heart is reperfused with the multiple bypass grafts, we
administer protamine
to reverse anticoagulation. Heparin reversal is somewhat
controversial and is omitted
in some programs. (23, 27) If the surgeon chooses to perform
parasternal intercostal
nerve blocks, they are done at this point. After the sternum is
reapproximated, the
muscle relaxant is reversed and cell saver blood is
returned.
To be eligible for extubation in the OR, the patient must be
awake, normothermic, non-
acidotic and adequately ventilating. If the patient is not ready
to be extubated in the
OR, he may usually be extubated a short time later in the
intensive care unit.
A key to success here is adequate analgesia. Unless
contraindicated, we routinely give
ketorolac (Toradol) to OPCAB patients prior to extubation.
Additionally, intravenous
opioids are titrated to effect. We have also used
patient-controlled analgesia with
considerable acceptance.
At one of our institutions, intrathecal morphine has been used
for postoperative
analgesia. For patients without coagulation abnormalities,
preservative-free morphine
(0.2-0.4 mg) is instilled into the subarachnoid space at the
lumbar level. This is usually
done in the operating room just prior to placement of invasive
lines, but it has also
been done during the postoperative period. Despite reports of
prolonged ventilatory
depression and inadequate analgesia in CABG patients, (28) in
our situation intrathecal
morphine has been well accepted, safe and effective, with
minimal side effects.
Our experience with recovering OPCAB patients in the ICU has
been one of slow, but
gradual acceptance by both nurses and respiratory therapists.
While our ICU nurses
have been accustomed to receiving anesthetized, intubated
cardiac patients, OPCAB
patients often arrive extubated and may be restless and
complaining of pain. Nurses
caring for these patients must be skilled in pain management as
well as in handling
various airway problems. For them, management of inotropic
support and
measurement of chest tube output has been replaced with
placement of
nasopharygeal airways, titration of morphine and reassurance of
the temporarily
disoriented patient.
-
8/3/2019 What is Opcab
13/17
Similarly, respiratory therapists accustomed to ventilator
management are most often
called upon to provide enriched oxygenation, bronchodilator
treatment and early chest
physiotherapy. With experience, we have eliminated routine
ventilator set-up but we
still insist on having a respiratory therapist readily
available.
Conclusion
OPCAB surgery is a significant advance in the operative
treatment of coronary artery
disease and presents significant challenges for the
anesthesiologist. A number of
aspects such as careful preparation, appropriate monitoring,
maintenance of
normothermia, specifically tailored drug management, maintenance
of hemodynamic
stability, provision of good operating conditions and a goal of
early extubation are
important in the management of these cases. As both surgical and
anesthetic expertise
with OPCAB surgery grows, we will make further progress toward
anesthetic
management that provides the optimum of safety and comfort to
our patients.
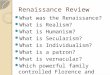
AccuMist Blower/Mister
Precise coronary suturing requires a clear, bloodless field. The
AccuMist device offers advanced fluid/gas mixing
technology, setting a new standard in creating a consistent,
predictable blood clearing mist.
The AccuMist Blower/Mister features:
On/off control in hand-piece
Easy-to-hold design
Malleable shaft
Specialized nozzle, utilizing a micro-orifice for fluid delivery
and a separate orifice for gas delivery
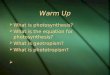
ClearView Intracoronary Shunt
For a Bloodless Anastomotic Site and Distal Blood Flow
-
8/3/2019 What is Opcab
14/17
As beating heart surgery techniques continue to evolve,
Medtronic continues to innovate. One such innovationfrom Medtronic
is the ClearView Intracoronary Shunt.
The ClearView Shunt is designed to help you perform quality
anastomosis on a beating heart.
The ClearView Shunt improves visualization by providing a
bloodless field for anastomotic suturing, while at thesame time
providing flow through the anastomotic site to the myocardium. With
the introduction of the ClearViewshunt, Medtronic is proud to offer
further innovation the first 1 mm intracoronary shunt.
Off-center lineplacement allowsfor easy removal
Clear shaftallows for a clear
view of flowthrough the
anastomotic site
Beveled tip allowsfor atraumaticinsertion and
removal
Ordering Information
Catalog Code Bulb Size Length Between Bulbs
31100 1.00 mm 14 mm
31125 1.25 mm 14 mm
31150 1.50 mm 14 mm
31175 1.75 mm 14 mm
31200 2.00 mm 14 mm
31225 2.25 mm 14 mm
31250 2.50 mm 14 mm
31275 2.75 mm 14 mm
31300 3.00 mm 14 mm
New: Octopus System II:
Octopus4 Tissue Stabilizer and Starfish2 Heart Positioner
Medtronic, the leader in suction stabilization, has improved
upon what is already the market-leading stabilization systemfor
beating heart surgery. The new Octopus System II (Octopus4 and
Starfish2) features significant innovations inease of use and
performance that make it the obvious choice for access to, and
stabilization of, all vessels -- even thetough-to-reach OMs.
FREE VIDEO:Click here to registerto receive a copy of our new
video Octopus System II: Complete MultivesselRevascularization.
Octopus4 Innovations
The Octopus4 retains the clear, malleable, spreading pods
surgeons have become accustomed to, combined with new
enhancements:
http://www.medtronic.com/cardsurgery/products/octosystem_reg.htmlhttp://www.medtronic.com/cardsurgery/products/octosystem_reg.htmlhttp://www.medtronic.com/cardsurgery/products/octosystem_reg.html
-
8/3/2019 What is Opcab
15/17
Starfish2 Innovations
The Starfish2 continues to simplify cardiac positioning and
minimize hemodynamic deterioration.1
Octopus System Positioning Options
Simplified Positioning, Enhanced Access, Superior
Stabilization
The Medtronic Octopus System is designed to maximize access and
stabilization of coronary arteries for off-pump grafting. The
OctoBase retractor allows for the highest performance of both the
Starfish and Octopusby making multiple mounting options
available.
The following graphic illustrations represent suggested mounting
and positioning options for the MedtronicOctopus System. They are
provided solely as guidelines and are not to be interpreted as
directions for use.
Proper surgical techniques and procedures are the responsibility
of the medical professional.
Introducing the Starfish Heart Positioner
Two attachment options enhance lateralwall exposure.
Integrated Bellows Suspension allows fornatural heart movement
throughout thecardiac cycle.
Three-appendage silicone head designallows for multiple
attachment options tooptimize placement on the epicardium.
Attachment procedure:
1. Place the Starfish head on the epicardium prior to turning on
the vacuum.
2. Turn on the vacuum and position the heart after the vacuum
has reached (-)400mm Hg.
3. Avoid placing the device over an epicardial sulcus or crevice
to prevent loss of vacuum seal.
4. Orient the bellows perpendicular to the weight and force of
the heart.
The Octopus 3-0 Tissue Stabilizer
The pioneering and market-leadingsuction stabilzer.
Malleable stabilizer pods can beformed to the unique contours of
thepatient's anatomy.
A unique tissue-spreading mechanismenhanced stabilization of
theanastomotic site and presentation ofthe coronary.
-
8/3/2019 What is Opcab
16/17
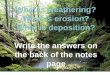
Lateral Wall Positioning Options
[ Click to Enlarge ]
[ Click to Enlarge ]
Apex Under Right Hemisternum
Starfish attached to the left ventricle, immediately lateral to
apex.
Even modest rightward movement of apex greatly enhances exposure
of proximal OMs and lowers the profile of the device.
Posterior Wall PositioningOptions
Anterior Wall PositioningOptions
[Click to Enlarge] [ Click to Enlarge ]
http://www.medtronic.com/cardsurgery/products/octo_pos.html#lateralhttp://www.medtronic.com/cardsurgery/products/octo_pos.html#apexhttp://www.medtronic.com/cardsurgery/products/octo_pos.html#posthttp://www.medtronic.com/cardsurgery/products/octo_pos.html#posthttp://www.medtronic.com/cardsurgery/products/octo_pos.html#posthttp://www.medtronic.com/cardsurgery/products/octo_pos.html#posthttp://www.medtronic.com/cardsurgery/products/octo_pos.html#lateralhttp://www.medtronic.com/cardsurgery/products/octo_pos.html#apexhttp://www.medtronic.com/cardsurgery/products/octo_pos.html#posthttp://www.medtronic.com/cardsurgery/products/octo_pos.html#post
-
8/3/2019 What is Opcab
17/17