Embed Size (px)
Citation preview
WHAT IS LARS?
LOW ANTERIORRESECTIONSYNDROME
Sophie Pilkington
Colorectal SurgeonUniversity Hospital Southampton
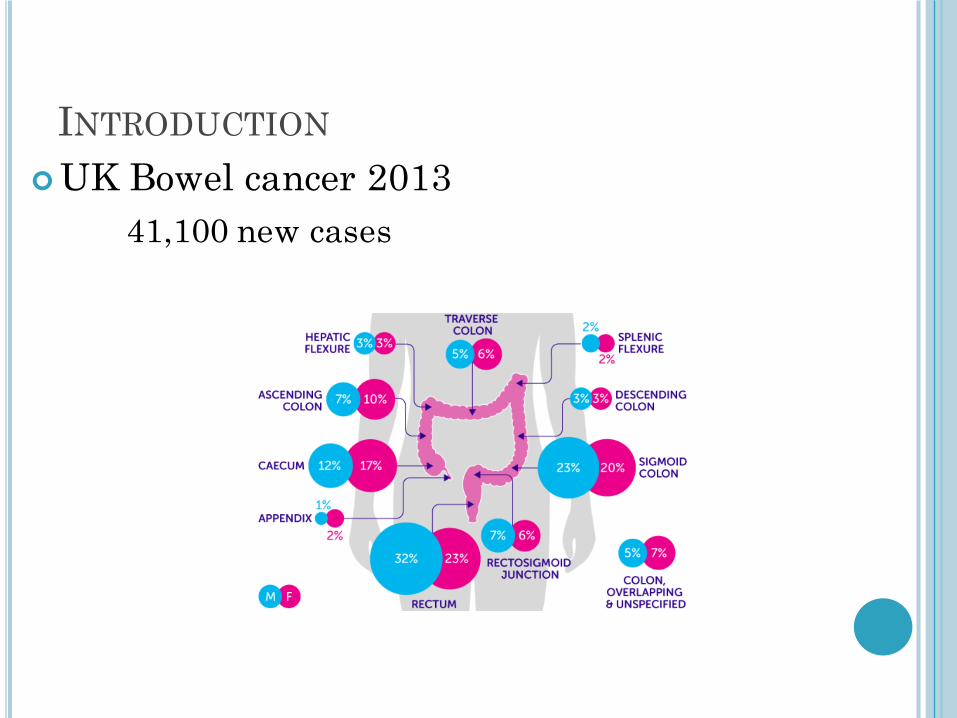
INTRODUCTION¢UK Bowel cancer 2013
41,100 new cases
INTRODUCTION¢UK Bowel cancer 2013
41,100 new cases ¢Major improvements in surgical and
oncological treatment

INTRODUCTION¢UK Bowel cancer 2013
41,100 new cases ¢Major improvements in surgical and
oncological treatment¢ Increased survival rate
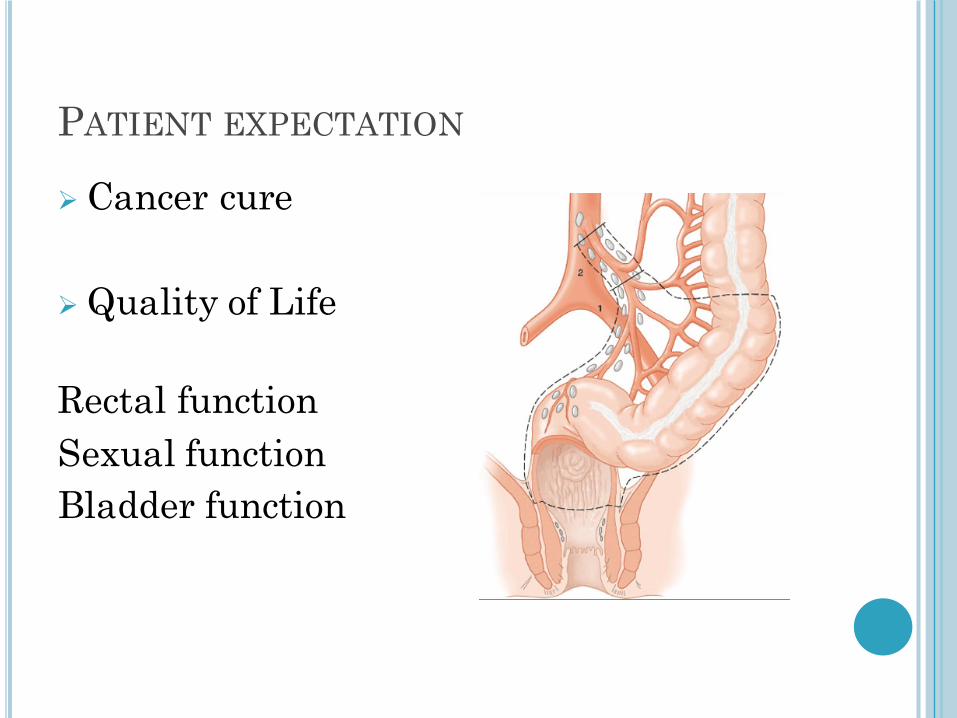
PATIENT EXPECTATION
Ø Cancer cure
Ø Quality of Life
Rectal functionSexual functionBladder function
LOW ANTERIOR RESECTION SYNDROME
¢ Anal incontinence¢ Emptying difficulties¢ Frequency¢ Urgency
Precise definition and incidence?Risk factors?Treatment?
Ø Preoperative or baseline bowel function
WHAT IS LARS?
¢ Sensible questions¢ Published questionnaires¢ Development of specific questionnaire

WHAT IS LARS?
¢ Anorectal physiology¢ Morphological changes
� Defined by endoanal USS, CT, Proctography?

FUNCTIONAL RESULTS AFTER LOWANTERIOR RESECTION
¢ Karanjia, Schache, HealdBJS 1992; 79: 114-116
Personal series 232 anterior resections over 10 yearsCompared stapled anastomosis
at 3cm (n=26) and 6cm (n=42)
Ø Frequency of defaecationØ Differentiating wind and bowel motionØ Hold urge for 15minsØ Soiling
FUNCTIONAL RESULTS AFTER LOWANTERIOR RESECTION
¢ Deterioration in function in both groupsNB retrospective assessment of preoperative function
Preservation distal rectum in 6cm group Improved¢ Ability to defer call to stool¢ Soiling
RECTAL FUNCTION BEFORE ANTERIORRESECTION
¢ UK Department of Health Criteria for high risk of colorectal cancer
Persistent change in bowel habit to looser stools or increased frequency of defaecation in patients older than 60 years

SOUTHAMPTON STUDY
¢ 120 patients undergoing major rectal resection for suspected cancer
¢ Assessment of continence with Cleveland Clinic score
Gender Male 71 (59%)Female 50 (41%)
Radiotherapy None 85 (70%)Short 19 (16%)Long 17 (14%)
Temporary Ileostomy 48 (40%)Age Years 67 yearsIncontinence CCI 4Physiology MRP 60mmHg
MSP 112mmHg
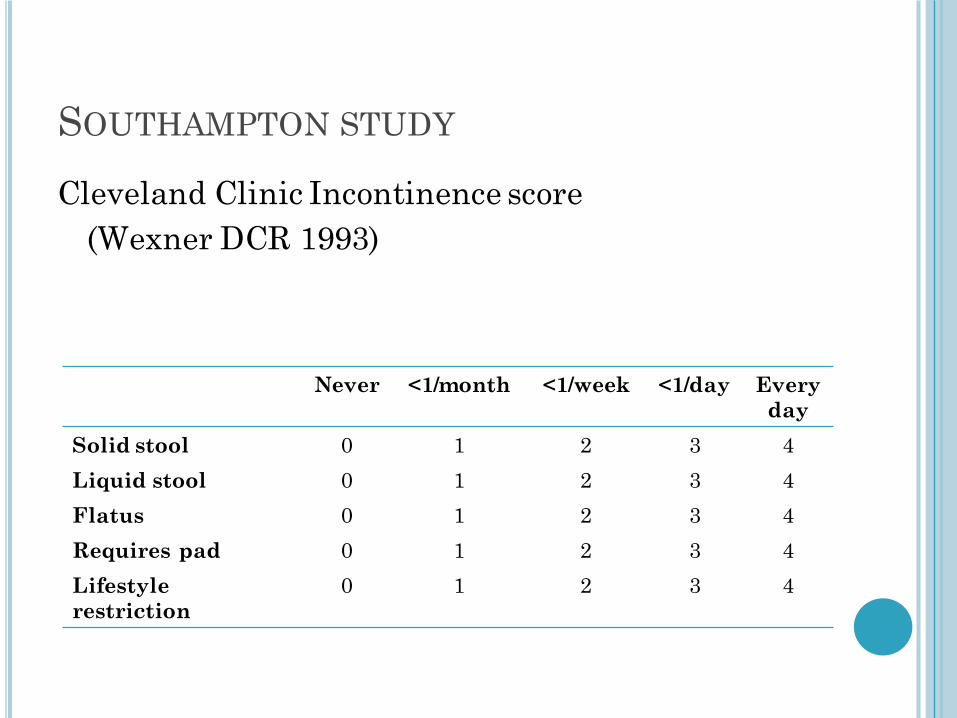
SOUTHAMPTON STUDY
Cleveland Clinic Incontinence score(Wexner DCR 1993)
Never <1/month <1/week <1/day Every day
Solid stool 0 1 2 3 4Liquid stool 0 1 2 3 4Flatus 0 1 2 3 4Requires pad 0 1 2 3 4Lifestyle restriction
0 1 2 3 4
SOUTHAMPTON STUDY
Before surgery 45% no anal incontinence17% severe anal incontinence
Ø Risk factor for 1 year
SOUTHAMPTON STUDY
Before surgery 45% no anal incontinence17% severe anal incontinence
Ø Risk factor for 1 year
Severe anal incontinence over first year27% at 3 months
Ø 59% got betterØ 41% severe anal incontinence at 1 year

SOUTHAMPTON STUDY
Before surgery 45% no anal incontinence17% severe anal incontinence
Ø Risk factor for 1 year
Severe anal incontinence over first year27% at 3 months
Ø 59% got betterØ 41% severe anal incontinence at 1 year
At one year13/89 (15%) severe anal incontinence

DEFINING ANTERIOR RESECTIONSYNDROME
Symptom scoring systems
Quality of life scoring systems
Specific questionnaires

DEFINING ANTERIOR RESECTIONSYNDROME
Symptom scoring systems� Cleveland Clinic Wexner Score (1993)� Fecal Incontinence Severity Index (FISI 2004)� Vaizey Score (1999)
Quality of life scoring systems
Specific questionnaires

DEFINING ANTERIOR RESECTIONSYNDROME
Symptom scoring systems� Cleveland Clinic Score (Wexner 1993)� Fecal Incontinence Severity Index (FISI 2004)� Vaizey Score (1999)
Quality of life scoring systems� SF-36 (Ware 1992) or EQ5D (1990)� EORTC QLQ-CR39 (2009)� FIQL (Rockwood 2000)
Specific questionnaires
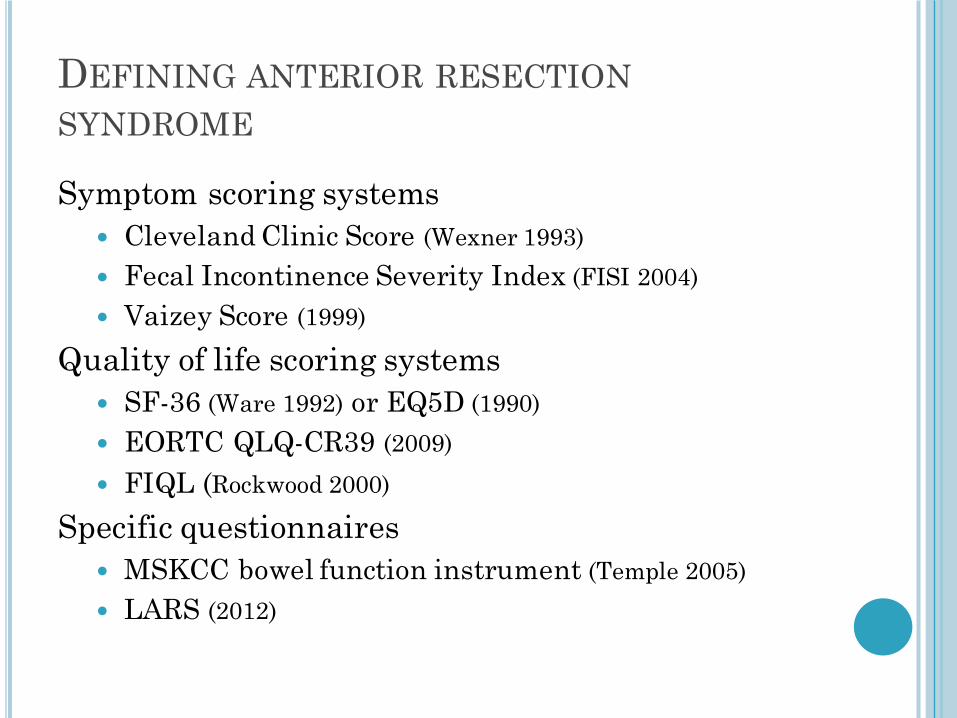
DEFINING ANTERIOR RESECTIONSYNDROME
Symptom scoring systems� Cleveland Clinic Score (Wexner 1993)� Fecal Incontinence Severity Index (FISI 2004)� Vaizey Score (1999)
Quality of life scoring systems� SF-36 (Ware 1992) or EQ5D (1990)� EORTC QLQ-CR39 (2009)� FIQL (Rockwood 2000)
Specific questionnaires� MSKCC bowel function instrument (Temple 2005)� LARS (2012)

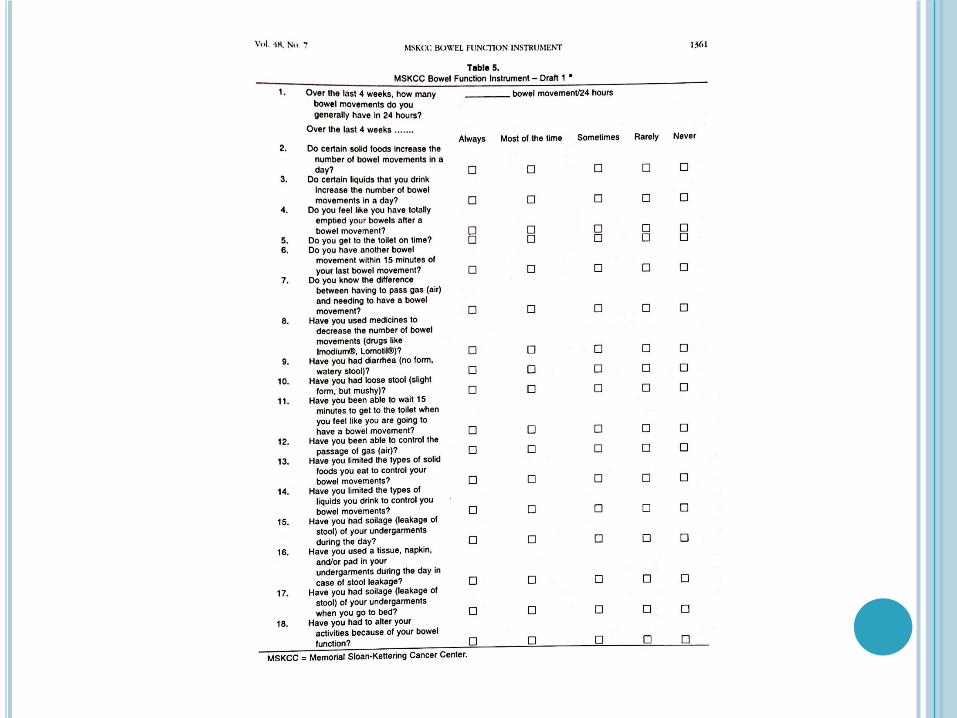
MSKCC BOWEL FUNCTION INSTRUMENT
Temple et al DCR 2005; 48: 1353-1365
18 item questionnaire184 patients sent questionnaire
¢ 70% response rate¢ 129 completed questionnaires
MSKCC BOWEL FUNCTION INSTRUMENT
Temple et al DCR 2005; 48: 1353-1365
5 most common symptoms
¢ Incomplete evacuation¢ Clustering¢ Food affecting frequency¢ Un-formed stool¢ Flatus incontinence
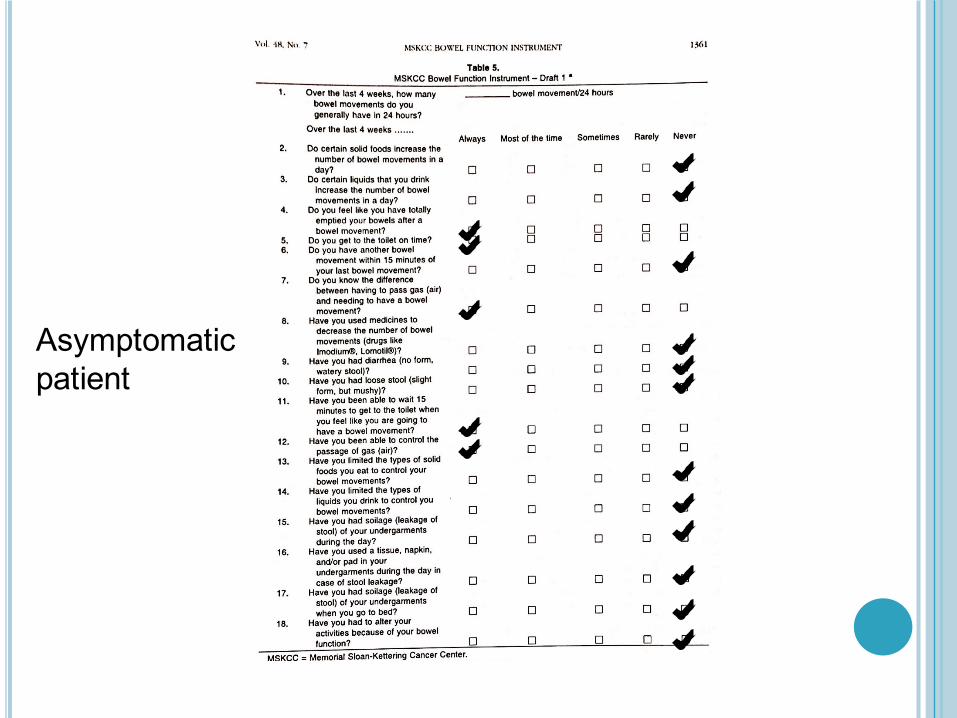
Asymptomatic patient

LARS SCORE
Emmertsen and LaurbergAnnals of Surgery 2012Vol 255 (5): 922-928
Draft questionnaireDanish rectal cancer survivors 2009¢ Item selection¢ Validity testing
Final bowel function questionnaire: LARS score
LARS SCORE
Development of basic questionnaire¢ Literature review¢ Draft questionnaire: 27 questions
� Inclusion of published scoring systems� Wexner score, St Marks’ incontinence score,
Cleveland clinic constipation score� Additional relevant questions eg FISI, FIQL
¢ Expert review¢ Pilot testing¢ Test-Retest reliability¢ Semistructured interviews
LARS SCORE
¢ Anchor question
“Overall how much is your quality of life affected by your bowel dysfunction?”
ü Not at allü A littleü Someü A lot

PATIENT CHARACTERISTICS
¢ Participants n = 1143¢ All had undergone low anterior resection 2 to 8
years earlier� 92.8% responded (n = 1061)� 42 had reoperation with permanent colostomy
Total 961 completed draft questionnaire¢ 405 (42%) women¢ Mean age 68.5 (range 36 to 93 years)¢ Mean follow up 55.5 months (range 24 to 96)¢ 573 (60%) underwent TME

LARS SCORE
¢ Anchor question
¢ Item selection and score developed on the basis of questionnaire results from a randomly selected half of the study population
¢ N = 483
LARS SCORE
¢ Anchor question
¢ Item selection and score developed on the basis of questionnaire results from a randomly selected half of the study population
¢ N = 483
¢ Validity¢ Tested on the other half of the study population¢ N = 478
ITEM SELECTION
Development group (n=482)¢ 5 most important items
� Incontinence for flatus� Incontinence for liquid stool� Frequency of bowel motions� Clustering of stools� Urgency
¢ Significant correlation to “impact on quality of life”
¢ Calculated importance & occurrence of each item

VALIDATION
Validation group (N=478)¢ No impact on quality of life reported (n=121)
� LARS score 13
¢ Minor impact (n=164)� LARS score 23
¢ Some / major impact (n=193)� LARS score 33
Significant difference between all groups (P<0.001)

LARS SCORE QUESTIONNAIRE
¢ Clear instructions
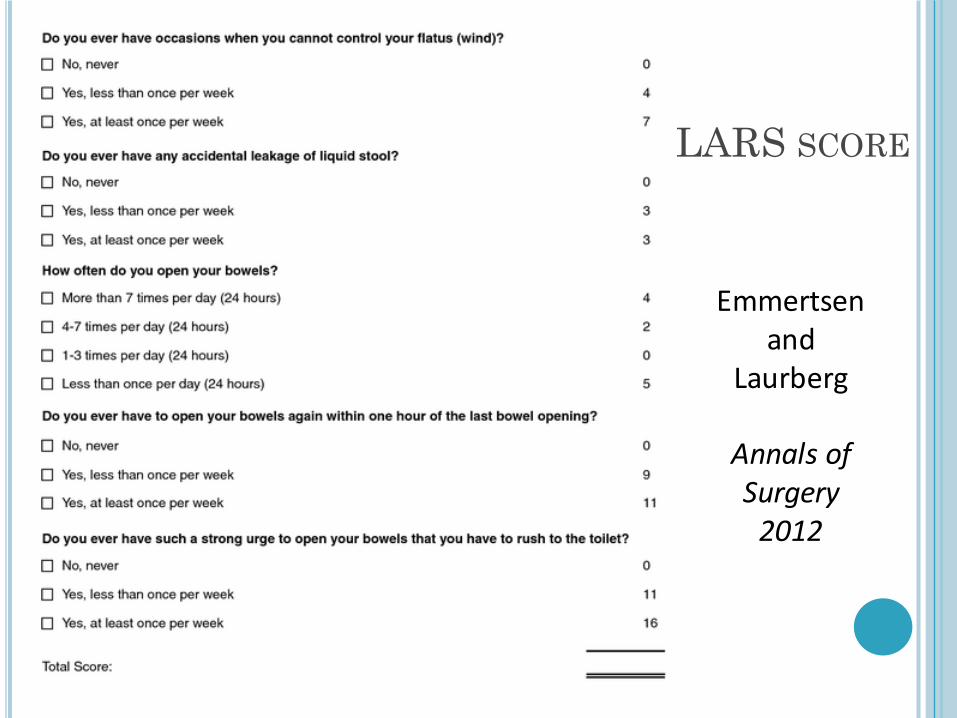
LARS SCORE
Emmertsenand
Laurberg
AnnalsofSurgery2012
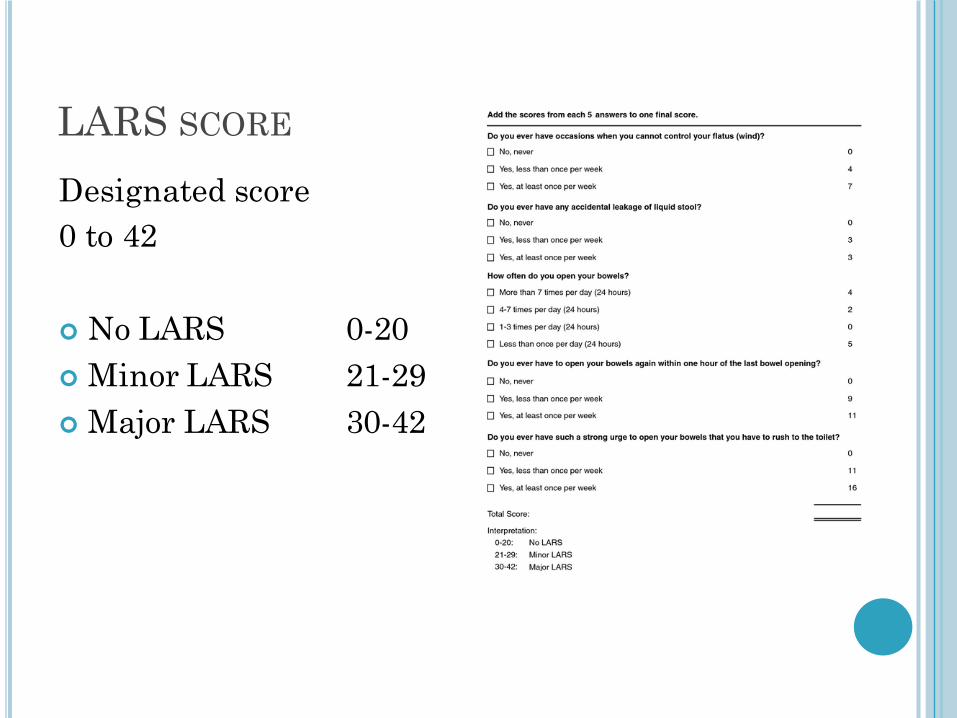
LARS SCORE
Designated score0 to 42
¢ No LARS 0-20¢ Minor LARS 21-29¢ Major LARS 30-42

LARS SCORE
¢ Quick and easy to use¢ Valid ¢ Specific for population of rectal cancer survivors¢ Includes bowel emptying difficulties and urgency¢ Incorporates bother caused by symptom rather
than just incidence¢ Score is based on calculated importance of each
item and occurrence, rather than a linear scale¢ Rigorous methodology
� Developed in one population, validated on separate similar population
¢ High response rate 93%

LARS SCORE
Daily clinical practiceScientific study
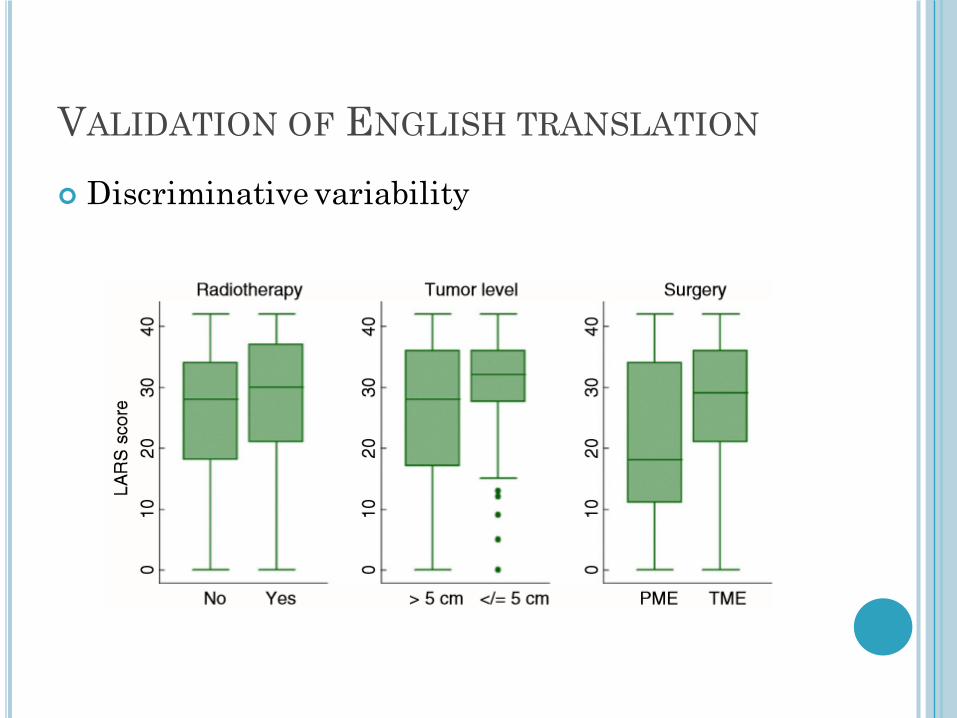
VALIDATION OF ENGLISH TRANSLATION
Juul et alColorectal Disease 201517, 908-916
¢ 12 UK centres¢ Data collection July 2013 to February 2014¢ Participants
� Rectal cancer at 0 to 15cm from anal verge� Surgery with partial or total mesorectal excision� January 2001 to January 2012 and bowel continuity
for at least 12 months
VALIDATION OF ENGLISH TRANSLATION
Postal questionnaire¢ EORTC QLQ-C30¢ LARS score¢ Anchor question for validation: “overall how
much does your bowel function affect your quality of life?
Not at allVery littleSomewhatA lot

VALIDATION OF ENGLISH TRANSLATION
¢ Response rate 463 / 579 (80%)
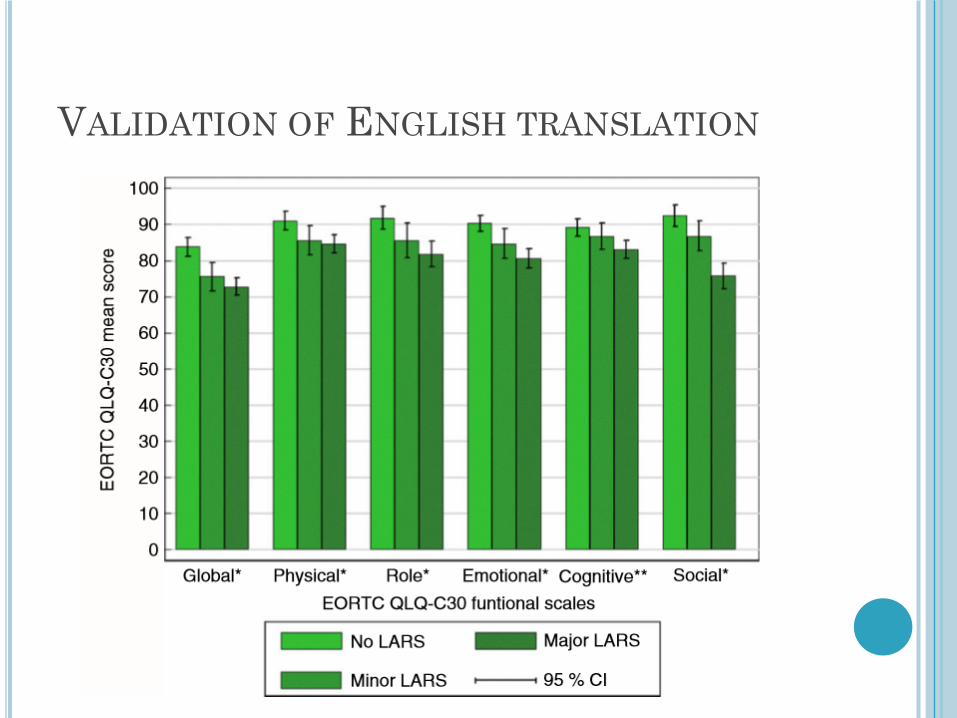
VALIDATION OF ENGLISH TRANSLATION
VALIDATION OF ENGLISH TRANSLATION
¢ Discriminative variability
LARS BOWEL DYSFUNCTION
Bregendahl et al CRD 2013: 15, 1130-1139Danish rectal cancer registry¢ Major LARS 41%
Associated with� Neoadjuvant therapy (independent of preoperative
radiotherapy regime)� Total mesorectal excision� Anastomotic leakage� Age <= 64 years� Female gender
¢ 64% minor LARS¢ 3% no LARS
LARS BOWEL DYSFUNCTION
But¢ No baseline scores: LARS score in preoperative
patients is unknown¢ Emphasis on flatus incontinence¢ Anchor question
ACPGBI 2016 ORAL PRESENTATION
Lynes, ThahaMulticentre study Response rate 53%
1093 patientsØ 41% Major LARSØ 22% Minor LARSØ 37% No LARS
Risk factors� Neoadjuvant chemotherapy� Female gender� Open surgery
LOW ANTERIOR RESECTION SYNDROME
LARS score assessment of bowel dysfunction¢ Daily clinical practice¢ Scientific study
LOW ANTERIOR RESECTION SYNDROME
LARS score assessment of bowel dysfunction¢ Daily clinical practice¢ Scientific study
But¢ No baseline scores: LARS score in preoperative
patients is unknown¢ Emphasis on flatus incontinence¢ Anchor question¢ Anorectal physiology¢ Other tests: endoanal USS, CT or proctography
LOW ANTERIOR RESECTION SYNDROME
Persistent problems with anal incontinence, urgency and frequency of defaecation (fragmented) following anterior resection
Negative impact on quality of life for rectal cancer survivors
LARS score: symptom-based scoring system correlated with quality of life





























