Embed Size (px)
Citation preview
What is duty/triage? Understanding the role of duty/triage in an area mental health service
Margaret Grigg, Helen Herrman, Carol Harvey
Objective:
To describe the duty/triage system within one urban area mental health servicein Australia and to investigate the factors that affect the decision to organize a comprehensiveassessment.
Method:
Data was collected from 3 months of duty/triage information and key informantinterviews. Policies and procedures related to duty/triage were reviewed. Quantitative andqualitative analyses were conducted.
Results:
Two thousand, six hundred and three contacts with duty/triage occurred over a3-month period. Half of these were related to patients new to the service. Most contacts wereself-referrals or referrals from a carer. Few referrals came through the primary health caresector. New patients were more likely to be assessed if the referral was presented in technicallanguage and if it was initiated by a health professional, particularly a general practitioner,emergency department or other mental health service. Assessment was less likely if thepatient or carer initiated the referral, if the problem was presented in vague or non-technicalterms, if there was a drug or alcohol problem or if the person refused care.
Conclusions:
A substantial number of potential patients contact a duty/triage worker everyday. However, there is little interaction with the primary care sector, limited documentation ofrisk and a lack of consistency in the documented reasons for the service response. Furtherinvestigation is needed of the conditions conducive to consistent quality decision making atthe point of entry to a specialist mental health service.
Key words:
clinical decision-making, mental health assessment, mental health triage,
Australian and New Zealand Journal of Psychiatry 2002; 36:787–791
pathways to care, referral patterns.
While the outcome of a mental illness is affected bythe availability of treatment [1], evidence suggests thatpeople have difficulty gaining access to specialist mental
health services [2,3]. Mental health professionals oftenmake decisions about who will receive available treat-ment. Processes are routinely developed to ensure thatonly those people who need specialist mental health caregain access to the mental health system.
The duty/triage system is the entry point to specialistpublic mental health services in Australia. The cliniciansworking in the duty/triage system make daily decisionsregarding the allocation of resources. Tobin
et al.
[4]identified three functions of an entry system to a well-organized mental health service. They are to:– prioritize referrals based on urgency;– direct resources to manage emergencies quickly; and– reduce unnecessary use of resources by limiting the
inappropriate use of services.
Margaret Grigg, Senior Lecturer (Correspondence)
LaTrobe University, Bendigo and Centre for Rural Mental HealthBendigo Health Care Group, Bendigo, PO Box 126, Bendigo, 3552, Aus-tralia. Email: [email protected]
Helen Herrman, Professor
Department of Psychiatry, University of Melbourne, Melbourne, Aus-tralia
Carol Harvey, Consultant Psychiatrist
North West Area Rehabilitation Services, North Western MentalHealth, Melbourne, Australia
Received 21 March 2002; revised 6 June 2002; accepted 16 July 2002.

788 UNDERSTANDING THE ROLE OF DUTY/TRIAGE
Little attention has been given to the role, functionor effectiveness of duty/triage systems despite theirrole in mediating access to mental health services. Aswell, duty/triage systems are relevant to understandingthe process and barriers to care in any locality and tounderstanding the unmet need for services, even thoughsystem variables do not account for the extent and vari-ation of unmet need in the community [5].
The purposes of this study are (i) to describe the duty/triage system within a public area mental health service(AMHS) in Melbourne, and (ii) to investigate the factorsthat influence the decision to organize a comprehensiveassessment for a person in contact with the duty/triagesystem.
Service description
The AMHS is located in inner Melbourne, and pro-vides specialist adult (i.e. between ages of 18 and 65)mental health services to a population of over 200 000people. The population in the catchment area is diverse.Some localities have significant levels of socioeconomicdisadvantage and high numbers of homeless people whileother areas are relatively affluent. The AMHS providesacute inpatient beds, crisis assessment and treatmentservice (CAT), case management, mobile intensive casemanagement, a long-term community residential rehab-ilitation programme and several specialist statewideservices. These are located and managed by a generalhospital with University affiliations. A single EmergencyDepartment in the general hospital services the area.
During business hours (Monday to Friday, 09.00 to17.00 hours) a specialist mental health worker (psychi-atric nurse, social worker, psychologist or occupationaltherapist) is available at each of the two communitymental health clinics. This duty worker is rostered torespond to all referrals for a specified time period as acomponent of a broader role as a case manager or crisisteam worker.
Outside normal business hours a specialist mentalhealth triage worker is located in the Emergency Depart-ment of the general hospital. Any contacts with the Emer-gency Department during business hours are referred tothe mental health clinic. Triage workers respond to allreferrals from the Emergency Department and to tele-phone enquiries directed by the hospital switchboard.Triage workers are allocated from clinicians workingwith the crisis team at the two clinics. Secondary consul-tation is available from the on-call psychiatric registrar,consultant psychiatrist or from another clinician withinthe crisis team.
All contacts (either face-to-face or by telephone) witheither the mental health clinic or the triage worker are
recorded in a standard form on an electronic Worddocument. Each weekday morning a review meeting isheld to discuss all contacts from the previous day. Mostclinicians within the clinic including duty workers, teammanagers and medical staff attend the meeting. Eachcontact is discussed and further issues for follow-upidentified.
Methods
The study used a programme evaluation approach and included arange of both quantitative and qualitative data.
Document analysis
Documents that related to the duty/triage system were reviewed.Information on services and the organization of duty/triage systems wasidentified from internal documents describing the system and frominformal discussions with staff. The first author was employed at themental health service during the period of the research.
Content analysis of duty/triage data
1. Quantitative analysis of routinely collected data July, August and September 2000
All patient related contacts with the duty/triage worker during July,August and September 2000 were collated and analysed. Each contactwas recorded in a standard electronic format that included date, time,site, patient details, referrer, nature of inquiry and outcome. These datawere converted to an Excel format and coded by the first author.
2. In depth analysis of data over one week period August 21–27, 2000
One week of data, from the three month sample was subjected to amore detailed analysis. The week chosen was a convenience sample, torepresent a typical week. The week contained no public holidays andwas outside school holiday periods.
The data for this week were compared with the full sample. Gener-ally, the typical week was consistent with the three-month samplealthough more contacts recorded in the typical week had missinginformation on the time of the contact (p < 0.001) and there was ahigher proportion of people contacting for clinical advice as the reasonfor referral (p < 0.05).
A detailed qualitative analysis of the data from the typical week wasconducted. All contacts for new patients who were living in thecatchment area that were referred during the week were reviewed anddivided into three categories, assessment, no assessment and assess-ment not applicable. Themes were developed using the immersion/crystallization (I/C) method. Immersion/crystallization consists of aseries of cycles whereby the researcher is immersed in the text.Reportable interpretations are reached through reflection and intuitiveinterpretation. Immersion/crystallization can be both content andtheory driven [6]. For instance, risk assessment emerged as an impor-tant theme from the literature and the data were explored to identify
M. GRIGG, H. HERRMAN, C. HARVEY 789
how risk was characterized. In contrast, the multiple references to othertreating professionals in the data led to the development of ‘existingtreatment team’ as a theme.
Key informant interviews
Key informant interviews were conducted to provide an overall viewof the role and function of duty/triage from the perspectives of keystakeholders. A key informant from the State Government, generalpractitioners, consumers and carers were interviewed using a semi-structured interview schedule. The consumer and carer informants wereidentified by approaching peak organizations. All interviews were con-fidential and were audiotaped and transcribed.
Results
Summary of data
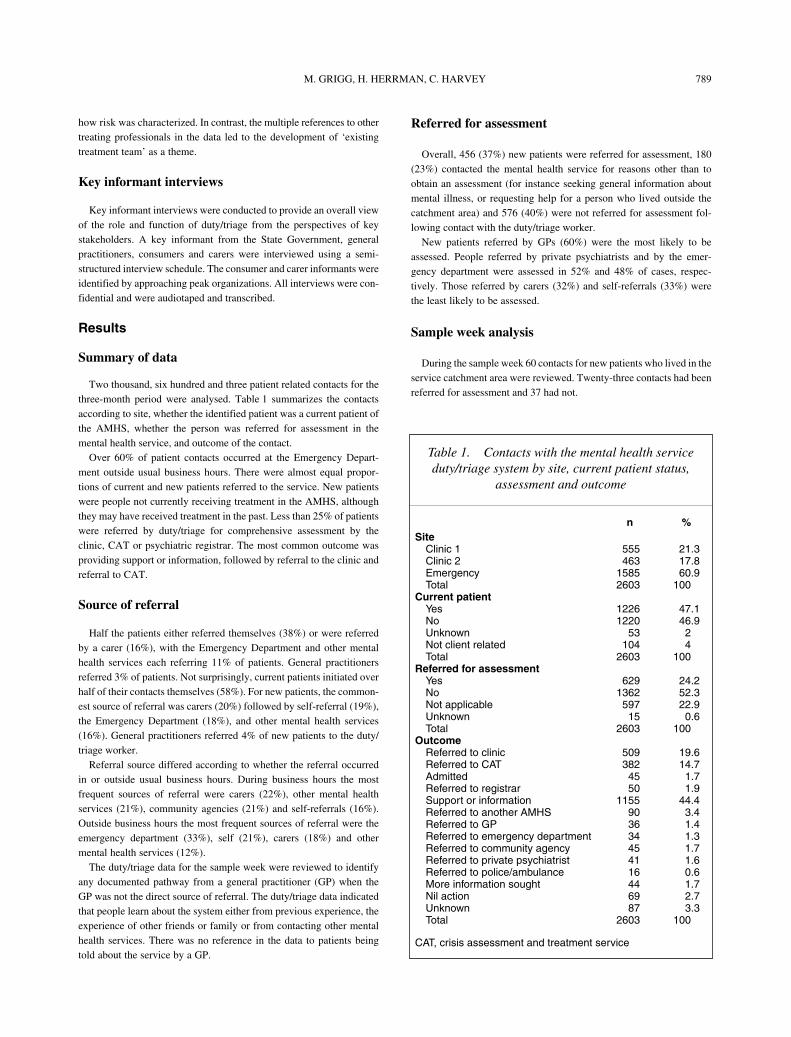
Two thousand, six hundred and three patient related contacts for thethree-month period were analysed. Table 1 summarizes the contactsaccording to site, whether the identified patient was a current patient ofthe AMHS, whether the person was referred for assessment in themental health service, and outcome of the contact.
Over 60% of patient contacts occurred at the Emergency Depart-ment outside usual business hours. There were almost equal propor-tions of current and new patients referred to the service. New patientswere people not currently receiving treatment in the AMHS, althoughthey may have received treatment in the past. Less than 25% of patientswere referred by duty/triage for comprehensive assessment by theclinic, CAT or psychiatric registrar. The most common outcome wasproviding support or information, followed by referral to the clinic andreferral to CAT.
Source of referral
Half the patients either referred themselves (38%) or were referredby a carer (16%), with the Emergency Department and other mentalhealth services each referring 11% of patients. General practitionersreferred 3% of patients. Not surprisingly, current patients initiated overhalf of their contacts themselves (58%). For new patients, the common-est source of referral was carers (20%) followed by self-referral (19%),the Emergency Department (18%), and other mental health services(16%). General practitioners referred 4% of new patients to the duty/triage worker.
Referral source differed according to whether the referral occurredin or outside usual business hours. During business hours the mostfrequent sources of referral were carers (22%), other mental healthservices (21%), community agencies (21%) and self-referrals (16%).Outside business hours the most frequent sources of referral were theemergency department (33%), self (21%), carers (18%) and othermental health services (12%).
The duty/triage data for the sample week were reviewed to identifyany documented pathway from a general practitioner (GP) when theGP was not the direct source of referral. The duty/triage data indicatedthat people learn about the system either from previous experience, theexperience of other friends or family or from contacting other mentalhealth services. There was no reference in the data to patients beingtold about the service by a GP.
Referred for assessment
Overall, 456 (37%) new patients were referred for assessment, 180(23%) contacted the mental health service for reasons other than toobtain an assessment (for instance seeking general information aboutmental illness, or requesting help for a person who lived outside thecatchment area) and 576 (40%) were not referred for assessment fol-lowing contact with the duty/triage worker.
New patients referred by GPs (60%) were the most likely to beassessed. People referred by private psychiatrists and by the emer-gency department were assessed in 52% and 48% of cases, respec-tively. Those referred by carers (32%) and self-referrals (33%) werethe least likely to be assessed.
Sample week analysis
During the sample week 60 contacts for new patients who lived in theservice catchment area were reviewed. Twenty-three contacts had beenreferred for assessment and 37 had not.
Table 1. Contacts with the mental health service duty/triage system by site, current patient status,
assessment and outcome
n %Site
Clinic 1 555 21.3Clinic 2 463 17.8Emergency 1585 60.9Total 2603 100
Current patient
Yes 1226 47.1No 1220 46.9Unknown 53 2Not client related 104 4Total 2603 100
Referred for assessment
Yes 629 24.2No 1362 52.3Not applicable 597 22.9Unknown 15 0.6Total 2603 100
Outcome
Referred to clinic 509 19.6Referred to CAT 382 14.7Admitted 45 1.7Referred to registrar 50 1.9Support or information 1155 44.4Referred to another AMHS 90 3.4Referred to GP 36 1.4Referred to emergency department 34 1.3Referred to community agency 45 1.7Referred to private psychiatrist 41 1.6Referred to police/ambulance 16 0.6More information sought 44 1.7Nil action 69 2.7Unknown 87 3.3Total 2603 100
CAT, crisis assessment and treatment service

790 UNDERSTANDING THE ROLE OF DUTY/TRIAGE
Description of mental state
The notes on 27 of the contacts, 14 (61%) assessed patients and 13(35%) not assessed patients provided some description of the person’smental state, although in most cases the description was brief. Descrip-tions of mental states for patients who were assessed, generally charac-terized the mental state in technical terms, most commonly describingpsychosis.
There were fewer references to mental state among ‘not assessed’patients, and those references tended to be brief, vague or expressedthe problem in non-technical language. Terms such as ‘counselling’,‘sad and depressed’, and ‘anger issues’ were used to characterize eitherthe person’s mental state or the assistance they required.
Risk assessment
There was minimal documentation of risk for either ‘assessed’ or‘not assessed’ patients. Where risk was documented it was vague andappeared at the end of the entry suggesting that it was the rationale forthe course of action. More frequently risk was mentioned obliquely inthe context of suicide or aggression.
History of mental illness
Half (19) the ‘not assessed’ patients had a reference to the personhaving a history of a mental illness. The most frequently mentionedpast psychiatric history was a history of treatment for psychosis includ-ing schizophrenia (5), followed by depression (3), bipolar disorder (3)and personality disorder (2).
The consumer informant suggested that diagnosis was important inaccessing a mental health assessment. Disorders such as schizophreniaand bipolar disorder were seen as much more likely to result in anassessment than borderline personality disorder or anxiety disorders.
Drug and alcohol use
Twelve of the ‘not assessed’ patient contacts mentioned a drug oralcohol problem while there were only four such references among the‘assessed’ patients. Key informants indicated that mental health assess-ments were more difficult to obtain if the person had a history of drugor alcohol abuse.
Length of time between referral and assessment
For the sample week, all new patients referred for assessment weredivided into two categories. The first category were new patients whohad an assessment within 24 h, the second included people assessedmore than 24 h after contact.
Almost half the new patients assessed (12) had an assessment within24 h. There were few similarities among this group, although in mostcases the referrer had either requested the urgent assessment, or thepatient had presented to the emergency department.
Thirteen of the new patients assessed waited longer than 24 h forassessment, with the length of time between one and 11 days. Many ofthese patients were either transferred from another mental health ser-vice, or the referring person stated that the referral was ‘not urgent’.
However, in some cases the reason for delay was unclear, particularlywhen there appeared to be some risk to the person.
Outcome
The commonest outcome for both current (50%) and new patients(34%) was providing support and information: including advice onaccess to psychiatric crisis services, advice to contact a general prac-titioner or private psychiatrist, and advice about access to private psy-chiatrists (including those who do not require payment beyond thecompulsory insured levels) or other support services. Other outcomesincluded referral to the clinic (20%), crisis team (15%) or psychiatricregistrar (2%) for further assessment.
Discussion
Duty/triage is a complex program. It is provided acrossseveral sites in the mental health service and involves alarge number of clinicians. Documentation of the pre-senting issues and the rationale for decision-making islimited.
The role of duty/triage in the treatment of existingpatients within the mental health service is important.While the focus of this paper is persons who are notcurrently being treated by the mental health service, thereare nevertheless important policy and research issuesassociated with duty/triage systems for existing patients.Which patients use the duty/triage system and whatimpact does it have on their care? How is continuity oftreatment ensured across different service sites, timesand workers? What communication strategies are usedand how effective are these? These are just a few of theissues that require further investigation.
Few patients were referred to duty/triage from primaryhealth care (general practice), with most either referringthemselves or referred by a carer. This suggests that theGP is not actively involved in the referral process for thevast majority of new referrals to the mental health ser-vice. Given that GPs treat the majority of people with amental illness, the finding that they are not a central partof the pathway to specialist treatment raises clinical andpolicy concerns. Further investigation is required toidentify whether this is an anomaly within one mentalhealth service, or whether this is the situation in othermental health services within Australia.
This study illustrates the role that duty/triage playsin allocating resources. Less than half the new patientswho contacted the mental health service were referredon for further assessment. This does not imply that thedecisions were inappropriate, nor that everyone whocontacts duty/triage should be assessed. Rather it illus-trates an internal pathway within mental health ser-vices that acts as a filter and mediates access to a mentalhealth assessment. Further research could usefully

M. GRIGG, H. HERRMAN, C. HARVEY 791
focus on the rationale and processes determining suchdecisions.
A consistent and well-supported entry system formental health services is an important part of reducingthe variance in clinical decision-making [4]. This studysuggests that at the entry point to a mental health service,limited information about the presenting problem andrisk is collected at entry. While there is some informalagreement on how to respond to specific clinical situa-tions, there is also considerable variation in the informa-tion about decisions documented by duty/triage clinicians,and limited opportunity for consultation in the decision-making.
While the study is limited by the reliance on routinelycollected data and the brevity of the documentation, therecording of all contacts with duty/triage with littlemissing data in a standardized electronic format enabledthe analysis of previously collected data.
Conclusion
A substantial number of patients contact the mentalhealth service every day. Most contacts do not result infurther assessment in the service. This study identifiedthat there is little interaction with primary health care atentry to the specialist system, limited documentation of
risk and a lack of consistency in the documented reasonsfor the mental health services’ response to a person witha mental health problem. While these results cannotnecessarily be generalized to other mental health ser-vices, they do illustrate the important role of entrysystems to mental health services and the need to haveconsistent, quality clinical decision-making processes.
References
1. Schaffner K, McGorry P. Preventing severe mental illnesses – new prospects and ethical challenges.
Schizophrenia Research
2001; 5:3–15.2. Henderson S, Andrews G, Hall W. Australia’s mental health:
an overview of the general population survey.
Australian and New Zealand Journal of Psychiatry
2000; 34:197–205.3. National Mental Health Strategy Evaluation Steering Committee
for the Australian Health Ministers Advisory Council.
Evaluation of the National Mental Health Strategy: final report
Canberra: Mental Health Branch, Commonwealth Department of Health and Family Services, 1997.
4. Tobin M, Yeo F, Chen L. The beginning of a structural reform: reorganising the front line of a mental health service.
Australian Health Review
2000; 23:64–76.5. Andrews G, Issakidis C, Carter G. Shortfall in mental health
service utilisation.
British Journal of Psychiatry
2001; 179:417–425.
6. Borkan J. Immersion/Crystallization. In. Crabtree B, Miller W, eds.
Doing qualitative research.
London: Sage, 1999; 179–194.














![Mental Health Triage in CAMHS - STORM...…the initial referral … was querying Asperger's syndrome, but during the triage appointment, the therapist picked up on [childs] lowness](https://img.pdfslide.us/doc/110x75/5e59bcdbd4fb72606319b033/mental-health-triage-in-camhs-the-initial-referral-was-querying-aspergers.jpg)














