Embed Size (px)
Citation preview

What Does the Left Atrial V WaveSignify During Balloon Commissurotomy
of Mitral Stenosis?Andrew Wang, MD, J. Kevin Harrison, MD, Karen S. Pieper, MS,
Katherine B. Kisslo, RDCS, and Thomas M. Bashore, MD
Left atrial v-wave amplitude has been associated withthe presence and severity of chronic mitral regurgitation(MR) but it has not been evaluated for the detection ofacute MR. We evaluated the left atrial v-wave amplitudeof 205 consecutive patients with mitral stenosis immedi-ately before and after stepwise, incremental balloonmitral commissurotomy to determine predictors of largev waves at baseline and an increase in v-wave ampli-tude after balloon commissurotomy. The sensitivity andspecificity of an increase in v-wave amplitude for detect-ing worsening and severe MR were determined. A largev wave was present in 44% of patients before ballooncommissurotomy and was predicted by age, mean leftatrial pressure, mean transmitral gradient, mean pulmo-nary artery pressure, and angiographic severity of MR.There was a strong inverse correlation between v-waveamplitude and calculated left atrial compliance (r 5
20.92). An increase in v-wave amplitude after ballooncommissurotomy was associated with an increasingprobability of worsening or severe MR. This indicatorhad a sensitivity, specificity, and positive and negativepredictive values of 35%, 91%, 64%, 75%, respectively,for detecting any increase in MR. For the detection ofsevere MR, the sensitivity was 79%, specificity 89%,positive predictive value 42%, and negative predictivevalue 98%. Thus, left atrial v-wave amplitude reflects leftatrial compliance and severity of mitral stenosis beforeballoon commissurotomy. An increase in v-wave ampli-tude is an insensitive but very specific indicator of wors-ening or severe MR during stepwise, incremental bal-loon mitral commissurotomy. Q1998 by ExcerptaMedica, Inc.
(Am J Cardiol 1998;82:1388–1393)
The magnitude of the left atrial or pulmonary cap-illary wedge v wave has been associated with the
presence and severity of mitral regurgitation (MR).However, several studies have reported that the vwave does not accurately predict the presence or se-verity of chronic MR.1–4 These studies have beenlimited by the use of pulmonary capillary wedge pres-sure rather than left atrial pressure in evaluating theseverity of MR. Furthermore, the possible relationbetween the v wave and MR has focused on assessingchronic, rather than acute, MR.
Balloon mitral commissurotomy performed via atransseptal approach affords the opportunity to assessthe left atrial pressure waveform directly. During step-wise, incremental balloon commissurotomy using theInoue balloon, multiple inflations with increasing bal-loon diameters are performed until an adequate reduc-tion in the transmitral gradient or an increase in MR isevident. An increase in the left atrial v wave has beenused as a sign of increasing, acute MR and thus mayindicate “when to stop” during incremental, stepwiseballoon commissurotomy. The objectives of this studywere (1) to determine predictors of v-wave amplitudebefore and after balloon mitral commissurotomy, and(2) to determine the sensitivity and specificity of the
left atrial v wave as a marker of acute and increasedMR after the procedure.
METHODSPatients: Clinical, echocardiographic and cardiac
catheterization data were obtained prospectively from205 consecutive patients with symptomatic mitral ste-nosis undergoing balloon commissurotomy with theInoue balloon technique at a single center betweenJanuary 1987 and January 1996. Informed consentwas obtained from all patients in accordance with aprotocol approved by the institutional review board.Patients with Sellers grade$215 MR by left ventric-ular angiography or evidence of left atrial thrombus bytransesophageal echocardiography were excluded.
Balloon mitral commissurotomy: Standard right andleft heart hemodynamic measurements, including si-multaneous measurement of left atrial and left ven-tricular pressures, were obtained before and immedi-ately after balloon commissurotomy using fluid-filledcatheters. Cardiac output was determined by the Fickmethod, and oxygen consumption was measured witha metabolic rate meter (Waters Instruments, Roches-ter, Minnesota). Mitral valve area was calculated us-ing the Gorlin formula, with an empiric constant of40.6 When a left-to-right shunt of.1.3 was observedby oximetric series after the procedure, the calculatedsystemic blood flow was substituted for the cardiacoutput in the Gorlin formula. The average diastolicarea of 3 beats was used for patients in sinus rhythm,whereas the average of 10 beats was used to calculatethe Gorlin valve area for patients in atrial fibrillation.
The technique of balloon mitral commissurotomy
From the Division of Cardiology, Department of Medicine, Duke Uni-versity Medical Center, Durham, North Carolina. Manuscript receivedApril 22, 1998; revised manuscript received and accepted June 25,1998.
Address for reprints: Andrew Wang, MD, Box 3428, Duke Uni-versity Medical Center, Durham, North Carolina 27710.
1388 ©1998 by Excerpta Medica, Inc. 0002-9149/98/$19.00All rights reserved. PII S0002-9149(98)00647-X

has previously been described.7,8 Balloon commissur-otomy was performed by the anterograde, transseptalapproach with an Inoue balloon (Toray Industries,Inc., Tokyo, Japan) in all patients. The procedure wasperformed in a stepwise, incremental manner withmeasurement of left atrial pressure and the transmitralgradient between each dilation. Balloon commissurot-omy was stopped when the transmitral gradient wasobserved to decrease adequately (.50% decrease) orthe left atrial v wave was observed to increase (.10mm Hg increase) from their respective baseline levels.Biplane left ventriculography was performed beforeand after completion of balloon mitral commissurot-omy, and MR severity was graded using the Sellersclassification.5 Procedural success was defined aspostprocedural catheterization mitral valve area$1.5cm2 or $50% increase in preprocedural mitral valvearea and the absence of.21 MR after balloon com-missurotomy.
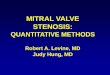
Left atrial v-wave amplitude and compliance: Leftatrial pressure waveforms were recorded immediatelyafter transseptal catheterization, between each ballooninflation, and after the final dilation of the mitral valve(Figure 1). The pre- and postprocedural left atrialv-wave amplitudes were measured at end-expirationby a blinded observer (JKH) after the procedure.
To determine the relation between v-wave ampli-tude and mean left atrial compliance, the baselinepressure waveforms and hemodynamics of patientswho developed 3 or 41 MR after the procedure wereretrospectively reviewed. Mean left atrial compliancewas calculated as previously described by Thomas etal.9 In brief, the “left atrium” was assumed to includethe pulmonary veins and to receive all of the cardiacstroke volume from the right ventricle during systoleand discharge it passively into the left ventricle duringdiastole. Mean left atrial compliance was calculatedby dividing the systolic increase in left atrial pressureinto the stroke volume. Stroke volume was obtainedby dividing Fick cardiac output by heart rate.
Echocardiography: Two-dimensional and Dopplerechocardiographic examinations were performed us-ing a commercially available, phased-array sectorscanner with a 2.5-MHz transducer immediately be-fore cardiac catheterization and the day after balloonmitral commissurotomy. All echocardiographic mea-surements were performed by one of the authors(KK). The echocardiographic score was determinedby the method of Wilkins et al.10 Results for allechocardiographic measures of mitral stenosis sever-ity were derived from the average of 3 beats forpatients in sinus rhythm or 6 beats for patients withatrial fibrillation.
Statistical analysis: Data are reported as medianvalues and interquartile rages (from the 25th to the75th percentile) for continuous variables and by per-centages for discrete variables. V waves were de-scribed as “large” if the v wave equal to or more thanthe mean left atrial pressure110 mm Hg or as “nor-mal” if the v wave was less than mean left atrialpressure110 mm Hg.2,3 Univariable analysis wasperformed to determine differences between patients
with large or normal v waves with regard to baselineclinical, echocardiographic, and catheterization data.Multivariable logistic regression analysis was per-formed to determine factors that were independentlyassociated with baseline v-wave amplitude.
The relation between left atrial v-wave amplitudeand MR was assessed using 3 different criteria for
FIGURE 1. A, left atrial and left ventricular diastolic pressurewaveforms demonstrating a large v wave before balloon mitralcommissurotomy. The electrocardiogram (ECG) is shown above.B, similar waveforms in the same patient after the third incre-mental, stepwise Inoue balloon dilation, demonstrating an acuteincrease in left atrial v-wave amplitude due to severe mitral re-gurgitation.
VALVULAR HEART DISEASE/V WAVE DURING BALLOON MITRAL COMMISSUROTOMY 1389

v-wave amplitude and 2 different end points for MR.The criteria for v wave were (1) the absolute postpro-cedural v-wave amplitude, (2) the difference betweenpre- and postprocedural v-wave amplitude, and (3) theratio of post/pre-v-wave amplitude. MR was evaluatedby 2 definitions: (1) worsening severity from baseline,and (2) presence of 31 or 41 MR after ballooncommissurotomy. Logistic regression modeling tech-niques are used to evaluate the prediction of MRseverity by v-wave amplitude. To check the assump-tion of linearity between the continuous predictor (vwave) and outcome of interest (MR), restricted cubicspline transformations11 of the v-wave amplitudeswere used. Spline transformations sort the v-waveamplitude from lowest to highest values and divide theamplitudes into groups along this ascending contin-uum of amplitudes. This transformed factor is used ina model that predicts MR outcome. The predictedvalues from this model are then plotted to depict therelation that exists between v wave and MR.
Univariable analysis of baseline and postproce-dural clinical, echocardiographic, and catheterizationdata was peformed to determine differences betweenpatients in whom v-wave amplitude increased afterballoon mitral commissurotomy versus patients with astable v wave or a decrease in the v wave. Multivari-able logistic regression analysis was performed todetermine those factors that were independently asso-ciated with an increase in v-wave amplitude.
RESULTSBalloon mitral commissurotomy was successful in
140 of 220 patients (79%). The mean mitral valve area
increased from 1.16 0.2 to 1.860.5 cm2 (p ,0.001), and mean mitralvalve gradient decreased from 9.263.9 to 5.86 2.4 mm Hg (p,0.001).Left ventriculography performed be-fore and after the procedure revealedthat the mean grade of angiographicMR increased from 0.56 0.6 to0.9 6 1.0, respectively (p,0.001).MR severity increased in 68 patients(30.9%), remained the same in 144(65%), and decreased in 8 (4%). Se-vere (3 or 41) MR was present in 20of 219 patients (9%) after ballooncommissurotomy, and in these pa-tients, angiographic MR increasedfrom 0.8 6 0.5 to 3.4 6 0.5 (p,0.001). Among patients with se-vere MR, the mean increase in v-wave amplitude was 9.96 16.4 mmHg (38.3 6 8.3 before and 48.3615.9 mm Hg after the procedure),whereas patients with 0.1 or 21 MRafter balloon commissurotomy had ameandecreaseof 9.1 6 9.1 mmHg(32.9 6 9.7 before and 23.86 9.4after the procedure) (p,0.001).
Baseline characteristics for pa-tients with large or normal v wavesare listed in Table I. A large v wave
before balloon commissurotomy was present in 90 of205 patients (44%). These patients differed from thosewith normal v waves with regard to gender, echocar-diographic score, left ventricular systolic and end-diastolic pressures, left atrial pressure, mean pulmo-nary artery pressure, mean transmitral gradient, andcardiac index. When analyzed jointly by multivariablelogistic regression analysis, a large v wave beforeballoon commissurotomy was predicted by age, meanleft atrial pressure, mean transmitral gradient, meanpulmonary artery pressure, and severity of MR (r2 foroverall model5 0.75). Figure 2 depicts the relationbetween mean left atrial compliance and v-wave am-plitude before balloon commissurotomy.
For each definition of v-wave amplitude after theprocedure, the chi-square for detecting 3 to 41 (se-vere) MR was greater than the chi-square for detectingworsening MR. Among the 3 definitions of postpro-cedural v-wave amplitude, the post-preprocedural vwave difference appeared to have a threshold or cutpoint above which the risk of worsening or severe MRincreased significantly. The cubic spline chart of theprobability of severe MR as a function of the differ-ence between pre- and postprocedural v-wave ampli-tude is depicted in Figure 3. The sensitivity, specific-ity, and positive and negative predictive values fordetecting worsening or severe MR after balloon mitralcommissurotomy were then determined for the post-pre-v wave difference. For the cut point of post-pre-v-wave amplitude.0 mm Hg (i.e, any increase in thev-wave amplitude after balloon mitral commissurot-omy) and the detection of worsening MR, the sensi-
TABLE I Baseline Clinical, Echocardiographic, and Catheterization Data
VariableNormal v Wave
(n 5 115)Large v Wave
(n 5 90) p Value
ClinicalAge (yr) 50.0 6 13.3 52.6 6 12.6 0.481Men 21 (18%) 7 (8%) 0.022CHF class
1 1 (,1%) 0 0.2822 24 (21%) 23 (26%)3 80 (70%) 58 (64%)4 9 (8%) 9 (10%)
Atrial fibrillation 37 (32%) 32 (36%) 0.211Echo score 7.6 6 2.2 8.7 6 2.3 0.012Left atrial diameter (cm) 5.3 6 0.9 5.3 6 0.7 0.222Catheterization
LVEF (%) 58.5 6 10.7 59.2 6 9.7 0.789LVSP (mm Hg) 122.8 6 18.2 131.7 6 21.4 0.010LVEDP (mm Hg) 11.9 6 4.6 12.7 6 4.6 ,0.001LA (mm Hg) 22.4 6 5.9 25.7 6 5.7 ,0.001PA (mm Hg) 30.1 6 8.7 35.2 6 11.9 ,0.001Mitral gradient (mm Hg) 11.0 6 4.1 14.0 6 4.4 ,0.001CI (L/min m2) 2.5 6 0.7 2.8 6 0.6 0.008Mitral valve area (cm2) 1.1 6 0.3 1.1 6 0.2 0.590Mitral regurgitation 0.234
0 74 (64%) 46 (51%)1 34 (30%) 37 (41%)2 7 (6%) 7 (8%)
CHF 5 congestive heart failure; CI 5 cardiac index; LA 5 mean left atrial pressure; LVEF 5 leftventricular ejection fraction; LVEDP 5 left ventricular end-diastolic pressure; LVSP 5 left ventricularsystolic pressure; PA 5 mean pulmonary artery pressure.
1390 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 82 DECEMBER 1, 1998

tivity, specificity, and positive and negative predictivevalues were 35%, 91%, 64%, and 75%, respectively.For the same cut point and the detection ofsevereMR,the sensitivity, specificity, and positive and negativepredictive values were 79%, 89%, 42%, and 98%,respectively.
After balloon mitral commissurotomy, the percent-
age of patients with large v waves decreased from 90of 205 (44%) to 61 of 201 (30%). An increase inv-wave amplitude from baseline was seen in 36 of 205patients (18%) after the procedure. In univariableanalysis, patients with an increased v wave differedfrom those with a decreased or unchanged v wavewith regard to baseline transmitral gradient, cardiac
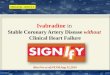
FIGURE 2. Relation between absolute left atrial v-wave amplitude and calculated left atrial compliance among 18 patients with mitralstenosis and insignificant mitral regurgitation (mean grade 5 0.8) before balloon mitral commissurotomy.
FIGURE 3. Cubic spline chart depicting the increasing probability of severe mitral regurgitation (MR) after balloon mitral commissurot-omy (BMC) as a function of the difference in v-wave amplitude (post-pre-balloon mitral commissurotomy v wave).
VALVULAR HEART DISEASE/V WAVE DURING BALLOON MITRAL COMMISSUROTOMY 1391

index, echocardiographic score, and postproceduralleft ventricular end-diastolic, mean left atrial, andmean pulmonary artery pressures, severity of MR, andmitral valve area (Table II). When analyzed by mul-tivariable logistic regression analysis, predictors of anincreased v wave after the procedure included baselinev-wave amplitude, baseline mean left atrial pressure,and postprocedural left atrial pressure. Thus, for anindividual patient, an increase in v-wave amplitudeafter balloon commissurotomy was predicted by lowerv wave and mean left atrial pressure at baseline, andhigher mean left atrial pressure after the procedure.
DISCUSSIONWe assessed the utility of v-wave amplitude after
balloon mitral commissurotomy as an indicator ofacute MR resulting from the procedure. To our knowl-edge, this is the only published study to evaluate thechangein left atrial v-wave amplitude directly as apotential indicator ofacuteMR, as previous studieshave evaluated the association between the pulmonarycapillary wedge v wave and severity of MR.2,3,12
The normal left atrial or pulmo-nary capillary wedge v wave, whichreflects the increase in left atrialpressure during atrial filling, is de-pendent on (1) the volume of bloodentering the left atrium, (2) the posi-tion of the left atrial pressure-volumecurve at the onset of filling, and (3)left atrial compliance.2 A large vwave has been associated with thepresence of severe MR, although itmay be found in other conditionssuch as mitral stenosis, congestiveheart failure, or ventricular septal de-fect.2
In our study, large v waves wereevident in 44% of patients with mi-tral stenosis before balloon commis-surotomy. Whereas the severity ofMR at baseline was found to be anindependent predictor of a large vwave, the other predictors suggestthat v-wave amplitude is largely de-pendent on left atrial compliance andthe severity of mitral stenosis. Thestrong inverse correlation (r520.92) found between left atrialcompliance and baseline v-wave am-plitude supports the significant rela-tion between these variables beforeballoon commissurotomy for mitralstenosis.
Use of the left atrial v wave duringballoon commissurotomy: Immedi-ately after balloon mitral commissur-otomy, left atrial compliance in-creases significantly due to a de-crease in left atrial pressure anddownward shift on the left atrialpressure-volume curve.9 Thus, a de-crease in left atrial v-wave amplitude
is expected. However, if acute, severe MR occurs afterthe procedure, the v wave may theoretically rise orremain unchanged as a function of an upward shift onthe left atrial pressure-volume curve.
Left atrial v-wave amplitude was 1 method used todetect the development of acute MR in the multicenterNorth American Inoue Balloon registry,13 yet its sen-sitivity and specificity in this setting have not beenreported. In the present study, the percentage of pa-tients with severe MR after balloon commissurotomyin our cohort (9%) was similar to the North AmericanInoue Balloon registry (7%).13 An increase in the vwave was found to be associated with an increasingprobability of worsening or severe MR. However, thesensitivity for detecting worening MR was poor(35%). This poor sensitivity is likely due to the in-crease in left atrial compliance during the procedure,9
which may negate the increase in left atrial pressurethat accompanies mild or moderate MR. As a sign ofacute,severeMR after balloon mitral commissurot-omy, an increase in the left atrial v-wave amplitude
TABLE II Clinical, Echocardiographic, and Catheterization Data after BalloonMitral Commissurotomy
Variable
Decreased orStable v Wave
(n 5 169)Increased v Wave
(n 5 36) p Value
BaselineAge (yr) 50.4 6 1.34 54.8 6 10.9 0.064Men 24 (14%) 4 (11%) 0.616CHF class
1 1 (1%) 0 0.2372 39 (23%) 8 (22%)3 116 (69%) 22 (61%)4 12 (7%) 6 (17%)
Atrial fibrillation 53 (31%) 16 (44%) 0.138Echo score 7.9 6 2.3 8.8 6 2.4 0.035Left atrial diameter (cm) 5.3 6 0.8 5.4 6 1.1 0.318LVEF (%) 58.8 6 9.5 58.6 6 13.2 0.889LVSP (mm Hg) 127.7 6 20.6 122.4 6 17.3 0.145LVEDP (mm Hg) 12.1 6 4.3 13.0 6 5.8 0.281LA (mm Hg) 24.1 6 5.9 22.5 6 6.4 0.147PA (mm Hg) 32.6 6 10.4 31.1 6 10.7 0.427CI (L/min m2) 2.7 6 0.7 2.4 6 0.4 0.002Mitral gradient (mm Hg) 12.7 6 4.3 10.3 6 4.7 0.013Mitral valve area (cm2) 1.1 6 0.2 1.1 6 0.3 0.862Mitral regurgitation 0.106
0 105 (62%) 15 (42%)1 52 (31%) 219 (53%)2 12 (7%) 2 (5%)
v wave (baseline) (mm Hg) 34.4 6 9.6 31.7 6 9.6 0.127Postballoon commissurotomy
LVEDP (mm Hg) 11.5 6 4.4 17.5 6 7.3 ,0.001LA (mm Hg) 15.8 6 5.4 25.4 6 10.9 ,0.001PA (mm Hg) 28.2 6 9.9 38.2 6 15.2 ,0.001CI (L/min m2) 2.8 6 0.7 2.6 6 0.6 0.153Mitral gradient (mm Hg) 6.5 6 6.1 7.9 6 4.7 0.246Mitral valve area (cm2) 1.9 6 0.5 1.7 6 0.6 0.045Mitral regurgitation ,0.001
0 78 (46%) 8 (22%)1 65 (38%) 8 (22%)2 22 (13%) 5 (14%)3 4 (2%) 8 (22%)4 0 7 (19%)
Abbreviations as in Table I.
1392 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 82 DECEMBER 1, 1998

had a higher sensitivity (79%) with similar specificity(89%) and excellent negative predictive value (98%).Thus, a stable or decreasing v-wave amplitude duringstepwise balloon mitral commissurotomy may be re-assuring that severe MR has not occurred. However,MR severity was not an independent predictor of anincrease in v-wave amplitude in the multivariablemodel.
Based on these results, echocardiography betweensuccessive balloon dilations is now used to detectworsening MR during procedures performed at ourinstitution. However, studies that have evaluated themechanism of severe MR as a complication of thisprocedure suggest that it is not a gradual process (i.e,moderate MR does not typically precede severe MR)but rather may be an “all-or-none” phenomenon.13–15
Study limitations: Our study involved patients withmitral stenosis undergoing balloon mitral commissur-otomy. It is not known whether left atrial hemody-namic measurements are similar in other causes ofacute MR. Semiquantitation of MR severity was basedon left ventriculography performed before the first andafter the final dilation. Ventriculography was not per-formed between successive inflations. In addition, an-giographic MR severity may not correlate with regur-gitant volume in the setting of changing left atrialcompliance. Left atrial pressure waveforms weremonitored between each dilation, but only the finalleft atrial pressure waveforms (at the end of the pro-cedure) were available for determination of v-waveamplitude.
Conclusions: Left atrial v-wave amplitude beforeballoon mitral commissurotomy reflects left atrialcompliance and the severity of mitral stenosis. Anincrease in the v-wave amplitude during stepwise,incremental balloon commissurotomy is associatedwith a higher probability of worsening or severe MR.
An increase in v-wave amplitude is an insensitive butvery specific indicator of worsening or severe, acute MR.
1. Braunwald E, Awe WC. The syndrome of severe mitral regurgitation withnormal left atrial pressure.Circulation 1963;27:29–35.2. Fuchs RM, Heuser RR, Yin FCP, Brinker JA. Limitations of pulmonary wedgev waves in diagnosing mitral regurgitation.Am J Cardiol1982;49:849–854.3. Pichard AD, Kay R, Smith H, Rentrop P, Holt J, Gorlin R. Large v waves inthe pulmonary wedge pressure tracing in the absence of mitral regurgitation.Am JCardiol 1982;50:1044–1050.4. Risk SC, D’Ambra MN, Griffin B, Fine R, O’Shea JP. Left atrial v wavesfollowing mitral valve replacement are not specific for significant mitral regur-gitation.J Cardiothorac Vasc Anesth1992;6:3–7.5. Sellers RD, Levy MJ, Amplatz K, Lillehei CW. Left retrograde cardioangiog-raphy in acquired cardiac disease.Am J Cardiol1964;14:437–447.6. Hammermeister KE, Murray JA, Blackmon JR. Revision of Gorlin constant forcalculation of mitral valve area from left heart pressure.Br Heart J 1973;35:392–396.7. Inoue K, Onaki T, Nakamura F, Miynmoto N. Clinical applications oftransvenous mitral commissurotomy by a new balloon catheter.J Thorac Car-diovasc Surg1984;87:394–402.8. Zaibag M, Al Kasab S, Riberio PD, Al Fugih M. Percutaneous double balloonmitral valvotomy for rheumatic mitral valve stenosis.Lancet1986;1:753–761.9. Thomas JD, Wilkins GT, Choong CYP, Abascal VM, Palacios IF, Block PC,Weyman AE. Inaccuracy of mitral pressure half-time immediately after percuta-neous mitral valvotomy dependence on transmitral gradient and left atrial andventricular compliance.Circulation 1988;78:980–993.10. Wilkins GT, Weyman AE, Abascal AM, Block PC, Palacios IF. Percutaneousballoon dilatation of the mitral valve: an analysis of echocardiographic variablesrelated to outcome and the mechanism of dilatation. Br Heart J 1988;60:299–308.11. Stone CJ, Koo CY. Additive splines in statistics.Proc Stat Comput SectionASA1985:45–48..12. Snyder RW, Glamann B, Lange RA, Willard JE, Landau C, Negus BH, HillisLD. Predictive value of prominent pulmonary arterial wedge v waves in assessingthe presence and severity of mitral regurgitation.Am J Cardiol1994;73:568–570.13. Hermann HC, Lima JA, Feldman T, Chisholm R, Isner J, O’Neill W,Ramaswamy K. Mechanisms and outcome of severe mitral regurgitation afterInoue balloon valvuloplasty.J Am Coll Cardiol1993;22:783–789.14. Hernandez R, Macaya C, Banuelos C, Alfonso F, Goicolea J, Iniguez A,Fernandez-Ortiz A, Castillo J, Aragoncillo P, Aguado MG, Zarco P. Predictors,mechanisms and outcome of severe mitral regurgitation complicating percutane-ous mitral valvotomy with the Inoue balloon.Am J Cardiol1992;70:1169–1174.15. Essop MR, Wisenbaugh T, Skoularigis J, Middlemost S, Sareli P. Mitralregurgitation following mitral balloon valvotomy. Differing mechanisms forsevere versus mild-to-moderate lesions.Circulation 1991;84:1669–1679.
VALVULAR HEART DISEASE/V WAVE DURING BALLOON MITRAL COMMISSUROTOMY 1393