Embed Size (px)
Citation preview
What Does MyHeart Scan
Show?Everything you need to know about your heart scan!
William Davis, MD, FACC
What Does My Heart Scan Show?© 2005 William Davis, MD, FACCAll rights reserved.
Published by:Maximillian Publishing2600 N. Mayfair Road, Suite 950Wauwatosa, WI 53226
www.trackyourplaque.com
The information contained in this book is not intended to represent amedical diagnosis, treatment, or medical advice in any way, as it is generalinformation and cannot be relied on without consultation with yourphysician. It is not intended nor is it implied to be a substitute forprofessional medical advice. In fact, taking full advantage of this programwill require that you consult with your physician or a physician willingto work with you. As medical information and your health can changerapidly, we strongly encourage you to discuss all health matters andconcerns with your physician before beginning new diagnostic ortreatment strategies.
The people, incidents, and dialogue discussed in this book are borrowedfrom the author’s collective experience, but do not represent actual peopleor events. Any resemblance to actual persons, living or dead, is entirelycoincidental.
All rights reserved. Printed in the United States. No part of this bookmay be used or reproduced in any form or by any means, or stored in adatabase or retrieval system without the prior written permission of thepublisher, except in the case of brief quotations embodied in criticalarticles or reviews. Making copies of any part of this book for any purposeother than your own personal use is a violation of United States copyrightlaws. Entering any of the contents into a computer for mailing list ordatabase purposes is strictly prohibited unless written authorization isobtained from the publisher.
Table of Contents
Chapter 1................................................................. 13What Exactly Is a Heart Scan?
Chapter 2................................................................. 27The Heart Scan Score: A Glimpse into Your Heart’s Future
Chapter 3................................................................. 47Why Heart Scans Are Better Than Cholesterol
Chapter 4................................................................. 57Does My Testing End Here? Will I Need Other Tests?
Chapter 5................................................................. 73What Should I Do with My Heart Scan Score?
Chapter 6................................................................. 97When Should I Have Another Scan?
Chapter 7................................................................. 105Be a Heart Disease Prevention Success Story!
Appendix................................................................. 109
Index........................................................................ 121

5
What Does My Heart Scan Show?
IntroductionI Just Got My Heart Scan Score.
Now What?!
Nick’s heart scan changed his life.
Before the scan, Nick viewed himself as a healthy,athletic, and successful 49-year-old. He weighed no morethan 10 pounds over his high school wrestling weight, hejogged and played tennis regularly, and just plain felt great.
But the fact that his father had died of a heartattack at age 53 troubled him over the years. How couldhis dad—slender and active, just like Nick—have diedunexpectedly? Nick had spent an entire Sunday with himtwo days before his death, and his dad had been every bitthe vigorous man he’d always been, without a hint of anypain or discomfort. He hadn’t smoked, and he exercisedand even laughed and joked up until the day of his untimelydeath. Was Nick doomed to repeat his father’s fate?
Nick had voiced this concern to his family doctor,who reassured him that his total cholesterol of 154 virtuallyguaranteed a lifetime of safety from heart attack. But thesewords eerily echoed the advice delivered to Nick’s dad
6
Introduction
shortly before his fatal heart attack. To help settle his mind,Nick’s physician had him undergo a stress test, a stressthallium, that proved entirely normal. In fact, according tothe cardiologist performing the stress test, Nick reached alevel ordinarily reserved for competitive athletes.
A nagging suspicion that all was not right led Nickto get a heart scan. The test itself proved no challengewhatsoever. After the obligatory paperwork, the technicianapplied three EKG leads to his chest, he lay down in theCT scanning device, and 30 seconds later the technicianhelped Nick off the imaging table and into a seat besideher to review the scan images.
The initial images left Nick stunned. Within thefirst few “slices” the radiation technologist reviewed, itbecame clear that an extensive quantity of plaque washidden within Nick’s coronary arteries. He left the scancenter following the technologist’s reassurance that theofficial reading by one of the center’s cardiologists wouldfollow.
Two days later, Nick received the official report:his heart scan “score” was 1132, a very high score thatplaced him in the 99th percentile. This meant that his scorewas in the worst 1 percent of men in his age group.
So it was that Nick’s heart scan shattered hisview of himself as a healthy, problem-free 49-year-old. Nick felt as if his future were a void loadedwith danger. Numerous questions raced throughNick’s mind: Now what? Does this mean I’m aboutto drop over from a heart attack? Don’t I needmedication? What about my cholesterol?Shouldn’t I get a stent or bypass surgery?
7
What Does My Heart Scan Show?
What Does My Heart Scan Show? is aguidebook for anyone who has undergone a heartscan, or is contemplating having one, but desiresmore information about what this valuable testmeans to their health. Like Nick, you will havenumerous questions regarding your heart scanscore. Understanding your heart scan score couldmean the difference between a heart attack in thefuture or a lifetime free of heart disease.* It couldmean obtaining heart procedures that could be life-saving, or it could mean avoiding procedures thatcould be unnecessary. All that in just one littlenumber!
The Most Important Health TestYou Can Get!
Mora had a heart scan at age 47, when she finallyacknowledged that her mother’s life had many parallels toher own. She especially feared that she was fated to repeather mom’s run-in with heart attack at age 50. Mora’s heartscan score: 52, in the 90th percentile for females in the 45-50-year age group (i.e., in the worst 10 percent of womenin her age group). Unfortunately, Mora’s doctor wasunfamiliar with the significance of heart scan scores andadvised her that, since she had no symptoms and her
* In this book the phrase “heart disease” will, for simplicity, mean coronary heart disease,and does not include valvular heart disease, condit ions of heart muscle(cardiomyopathies), pericardial diseases, and other systemic disorders that affect theheart.
8
Introduction
cholesterol was only borderline high, she should simplyremain alert for the appearance of chest pain over the years.Perhaps he’d consider a stress test somewhere along theway.
Too often, people undergo a heart scan, get ascore, and then are left in the dark about its sig-nificance. As a result, the score is ignored or for-gotten, and the information is never put to gooduse. That’s a terrible shame, because this simplenumber can be the most important piece of healthinformation you may ever receive.
Your heart scan score contains a world ofinformation. Your score is a measure of the quan-tity of atherosclerotic plaque lining the arteries ofyour heart. It can be compared to other people yoursex and age and thereby provide a gauge of heartattack risk. Your score is the sum total of coro-nary risk factors like cholesterol and high bloodpressure all through your life up until the momentof the scan. Your score can be used to track growthor shrinkage of plaque if you get another scan ayear or more after the first. All this is accomplishedwith ease, safety, and a relatively low cost. Noother test can even come close to the power ofheart scans to yield health-empowering informa-tion!
The sort of advice Mora received is, unfor-tunately, all too common. What’s wrong with wait-
9
What Does My Heart Scan Show?
ing for some tell-tale sign of heart disease? Firstof all, the American Heart Association tabulatesextensive data on heart disease in the U.S., and itis quite clear that the first symptom in 50 percentof heart attacks is also the last (i.e., sudden death).Waiting for symptoms is like waiting for the smellof smoke to prevent fire in your home—if yousmell smoke, it’s already too late. Secondly, stresstesting for asymptomatic people, especiallywomen, is notoriously unreliable, with the vastmajority of future heart attacks occurring in peoplewith normal stress tests. (This is in contrast topeople with symptoms like chest pain, pressure,or breathlessness, where stress testing can be use-ful.) Thirdly, this “watch and wait” approach insomeone like Mora guarantees that coronaryplaque will grow, usually at the rate of 30-35 per-cent per year, since no effort was made to identifythe causes of hidden coronary plaque nor any treat-ment initiated. Mora will suffer a heart attack (ordie or develop unstable symptoms of heart dis-ease) almost certainly by age 55. The opportunityto prevent this dire event was lost with her doctor’sdismissal of her heart scan score. Don’t let thishappen to you.
10
Introduction
When it comes to cardiovascular disease,myths that promote complacency promote disease.
Heart Disease and Stroke StatisticsAmerican Heart Association
Given the fact that nearly 40 percent of uswill die of a heart attack, and that cardiovasculardisease claims more lives each year than the nextfive leading causes of death combined—cancer,chronic respiratory diseases, accidents, diabetes,and influenza and pneumonia—your heart scan isnever a wasted effort.
This Is Your Guide to UnderstandingYour Heart Scan Score.
What Does My Heart Scan Show? is yourguide to understanding precisely what your scoremeans. It should answer all your questions aboutheart attack risk. More importantly, this bookshould galvanize your resolve to begin a preven-tion program that aims to eliminate the risk of heartattack in your lifetime. In other words, if your heartscan can predict for you, with confidence, yourrisk for heart attack and even tell when it mightoccur, you should work hard to alter the future.
11
What Does My Heart Scan Show?
You and your doctor can indeed accomplish this,given proper guidance and commitment.
Millions of people have now undergone heartscans across the U.S., yet too few have been giventhe advantage of a full understanding of this im-portant number. What Does My Heart ScanShow? will fill this information gap for you.

13
What Does My Heart Scan Show?
Chapter 1Chapter 1Chapter 1Chapter 1Chapter 1What Exactly Is a Heart Scan?
Greg, a 51-year-old pharmaceuticalrepresentative, prided himself on his healthy lifestyle. At 5feet 8 inches tall, he weighed a slender 147 pounds, notmuch more than he’d weighed as a champion high schoolwrestler. He felt great and tackled his work and home lifewith enthusiasm and energy. He was also proud of hischolesterol numbers, held in check for the past 10 yearssince he’d worked in the pharmaceutical industry and paidcloser attention to his health. His most recent panel: HDL55 mg/dl, LDL 94 mg/dl, triglycerides 123, all excellentaccording to his family physician. Greg’s mom and dadlived into their early 80s without an encounter with heartdisease, and Greg was confident that he was free of risk.
Unexpectedly, Greg’s older sister informed himthat she’d developed unstable chest pain symptoms recently,
14
Chapter One
Two sample images fromGreg’s heart scan showingextensive plaque.
requiring hospitalization.She’d undergone a heartcatheterization and receivedtwo coronary stents, narrowlyaverting an open heartprocedure. This unsettledGreg’s complacency, and henow became concerned abouthis own health. A heart scansubsequently revealed a scoreof 1387, in the 99th percentilefor men his age. This scoresuggested that, far from beinglow, Greg’s risk was, in fact,an alarming 25 percent peryear for heart attack anddeath.
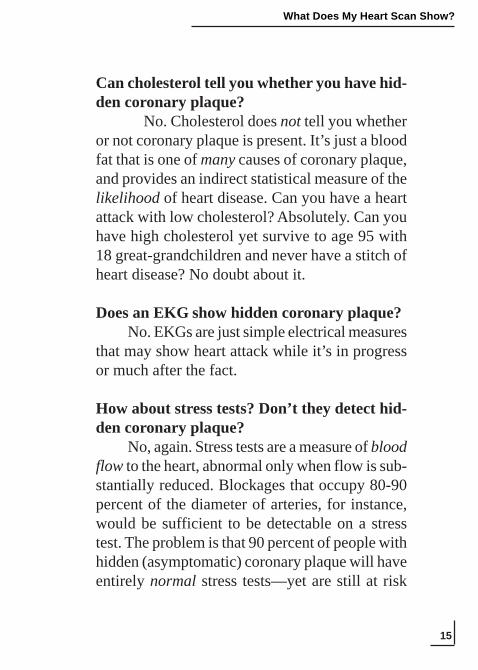
A sample “slice” from the 30–40 total images from a heart scan(generated by an EBT scanner). You’re viewing a cross-section ofthe chest from the feet, looking up. The subject is lying on his backwith his right side to your left, his left side to your right. The spine isthe dense white area toward the bottom of the image. The variousheart structures are located toward the center of the chest.The coronary calcium iscircled in white. This is“scored” (using area and den-sity criteria, or volume crite-ria) and the score of each im-age is added to those of allother images to yield a totalcalcium score.
15
What Does My Heart Scan Show?
Can cholesterol tell you whether you have hid-den coronary plaque?
No. Cholesterol does not tell you whetheror not coronary plaque is present. It’s just a bloodfat that is one of many causes of coronary plaque,and provides an indirect statistical measure of thelikelihood of heart disease. Can you have a heartattack with low cholesterol? Absolutely. Can youhave high cholesterol yet survive to age 95 with18 great-grandchildren and never have a stitch ofheart disease? No doubt about it.
Does an EKG show hidden coronary plaque?No. EKGs are just simple electrical measures
that may show heart attack while it’s in progressor much after the fact.
How about stress tests? Don’t they detect hid-den coronary plaque?
No, again. Stress tests are a measure of bloodflow to the heart, abnormal only when flow is sub-stantially reduced. Blockages that occupy 80-90percent of the diameter of arteries, for instance,would be sufficient to be detectable on a stresstest. The problem is that 90 percent of people withhidden (asymptomatic) coronary plaque will haveentirely normal stress tests—yet are still at risk
16
Chapter One
So how can you detect and measure hiddencoronary plaque?
Remember that we’d like to measure it eas-ily, inexpensively, and safely. We don’t want in-vasive procedures that involve scalpels and cath-eters. We need a test that precisely detects hiddenplaque without pain, with virtually no risk, thatnearly anybody can get.
That’s precisely what a heart scan can do.And it does it better, faster, and easier than anyother test available.
We now know that 95 to 99 percent of heart diseaseoccurs at sites WITHOUT artery narrowing. Thus, the oldtests we perform to detect narrowing and blockages havereally misled us. We miss over 95 percent of the heartdisease that causes heart attacks.
Dr. Steve NissenThe Cleveland Clinic
What Exactly Is a Heart Scan?
If you’ve undergone a heart scan, you alreadyknow that it’s among the easiest and fastest healthtests available: hold your breath for 30 seconds
for heart attack. In fact, most of the people fatedto suffer a heart attack in the next year have nor-mal stress tests.
17
What Does My Heart Scan Show?
and you’re done. It’s about as simple as any testcan get. No poking, prodding, or pushing, no IVs,no pre-medication, no preparation. Most peopleare surprised by how easy it is. The most com-mon comment after the scan is finished is, “Is thatit?” With this small effort, you’ll be provided withthe most powerful piece of information you canget about your heart’s future.
A heart scan is really 30-40 cross-sectionalimages (varying depending on your height) of theheart from top to bottom, all obtained in the fewseconds you hold your breath. (Holding yourbreath eliminates motion of the heart due to ex-pansion of the adjacent lungs.) Within each of the30 or so images, a “slice” of your three coronaryarteries can easily be seen. Because each sliceoverlaps with those above and below it, the scanprovides, in effect, a three-dimensional survey ofthe chest contents.
Each scan is reviewed and a computer ap-plies specific criteria to help decide whether a se-lected area within your coronary arteries is trulycoronary plaque. We then multiply the area (insquare millimeters) by the density of the plaque,and this yields a “score” for this specific plaque.We score all the plaques in every image slice andadd all the scores up. This yields a total score, the
18
Chapter One
one reported to you. You will sometimes hear thetotal score called an “Agatston” score, named af-ter Dr. Arthur Agatston from the University ofMiami, who first developed this method of scor-ing. The Agatston score is now one of the stan-dard calculations performed on all heart scans.(This is the same Dr. Arthur Agatston, by the way,who authored the hugely successful South BeachDiet.)
Some scan centers will also calculate a “volu-metric” score, which is simply a three-dimensionalmeasure of plaque volume. Though the numberprovided for your volumetric score is similar tothe conventional score, the numbers can differsomewhat. Many investigators believe that thevolumetric score is slightly more accurate, and itmay be the preferred number to track if you havetwo or more scans over a several year period.Nonetheless, the standard “Agatston” heart scanscore remains the most commonly used measure.
19
What Does My Heart Scan Show?
Who Should Have a Heart Scan?
If you haven’t yet undergone a heart scan,how do you decide whether you should get one inthe first place? Are there specific criteria you canapply?
Many authorities recommend that men overage 40 and women between ages 45 and 50 bescanned. This is based on the simple observation, intens of thousands of people, that substantial num-bers of men start showing hidden plaque (scoresgreater than zero) at age 40 and older and womenbetween 45 and 50. Prior to these ages, scoresabove zero for either sex are unusual. Women areadvised to get scans later than men because theirdevelopment of plaque lags behind men’s byapproximately 10 years.
Beyond age, there are no useful criteria todecide who should and who shouldn’t be scanned.We could, for instance, use LDL cholesterol todecide whom to scan. If we chose anyone with LDLcholesterol greater than 130 mg/dl, we would misshalf the people with heart disease. (In other words,approximately 50 percent of people with measurablecoronary plaque have LDL cholesterols less than130 mg/dl.) Likewise, if low HDL (less than 40) wereour cut-off, we would again miss about half thepeople with heart disease. Similar failures occur forany other screening parameter you can devise.
20
Chapter One
Consider this: Can we screen you for thepresence of heart disease by screening you withanother test first? You may begin to see the absur-dity of this approach. A study by Drs. Arad andGuerci at the St. Francis Medical Center in NewYork, for instance, showed that 67 percent of peopleclassified by the widely-used Framingham riskscoring system (using cholesterol, blood pressure,smoking history, and sex) were mis-classified.People labeled low-risk were actually high-risk;people labeled high-risk were actually low-risk.Another study by Dr. Stephan Achenbach of theMassachusetts General Hospital showed a verypoor 28 percent correlation between risk factorscoring systems, like the Framingham system, andheart scan scores. Most concerning is the fact thatsignificant numbers of people classified as low-riskby the Framingham scoring system had extensivecoronary plaque.
Cholesterol values and conventional riskfactors cannot be reliably used to decide whether ornot to have a scan. We therefore rely on age as aguide.
If there is some high-risk measure in yourlife—parent with heart attack before age 55, diabe-tes, cholesterol greater than 300, smoking—thenyou might consider having your scan five yearsearlier (age 35 for men and 40 for women).
21
What Does My Heart Scan Show?
What’s the best heart scan score? Zero, orno detectable plaque in any of your scan images.What’s terrible? Just like playing golf, the higheryour score, the worse it is. But just like asking,“What’s a terrible golf score?” the answer for whatconstitutes a terrible heart scan score is, “It de-pends!” Certainly, the higher your score, the moreplaque you have in your coronary arteries, andthe greater your heart attack risk. Scores of 1000or greater (that’s a lot of plaque!) carry a risk forheart attack of 25 percent per year (if no preven-tive therapies are initiated), as it did unexpectedlyfor Greg, whom we discussed earlier. Scores be-tween 0 and 1000 are much more common andcarry various degrees of risk in-between. We’lldiscuss this further.
Why Is It Called a “Calcium Score”?
What precisely is measured on your heart scan?Children’s arteries are flexible, thin-walled
tubes, free of plaque, with lining tissue that mea-sures a millimeter or so in thickness. The yearstake their toll, particularly if there are genetic rea-sons or noxious factors like smoking, high cho-lesterol, high-fat meals, high blood sugar, etc.
22
Chapter One
Sample images from a complete heart scanperformed on an EBT scanner. Although only 12 ofthe total 35 images are shown, you can get an ideathat multiple thin “slices” are made through the chestfrom just below chin level to the bottom of yourbreastbone. The amount of calcified plaque is then“scored” on each slice and summed to yield a totalheart scan score.
23
What Does My Heart Scan Show?
The lining tissue of arteries is delicate andeasily injured, and reflects that injury by thicken-ing. Within the thickened lining, fibrous structuralmaterial, calcium (like that in bone), and inflam-matory cells also accumulate. The gruel-like ma-terial that results is called “atherosclerotic plaque.”(Athero is derived from the Greek word for“gruel”; Sclerosis means “hardening.”)
Many plaque components can’t be easilymeasured in a living human being, such as inflam-matory cells or structural tissue. Remember, we’retrying to accurately measure plaque without scal-pels, catheters, or other invasive methods. Cal-cium often collects as tiny pebbles and arcs withinplaque and can be measured accurately and eas-ily. Interestingly, microscopic studies of athero-sclerotic plaque have shown that calcium consis-tently occupies 20 percent of the total volume ofplaque. This proportion remains true for women,men, young, old, and whether or not you’ve al-ready had a heart attack. In other words, calciumprovides an indirect though accurate means tomeasure total plaque volume. If we were to mea-sure two cubic millimeters of plaque, for instance,then we would have a total of 10 cubic millime-ters (2 x 5) of total plaque.
24
Chapter One
The Agatston score and the volumetric scoresare two slightly different methods to measure coro-nary plaque, both using calcium as the measuredparameter to gauge total plaque.
The rule of coronary calcium scoring is easy:the higher your score, the more plaque lines yourcoronary arteries. How your score can be used topredict your risk of heart attack and other troubleis the focus of the discussion in Chapter 2.
25
What Does My Heart Scan Show?
Is It “Hard” or “Soft” Plaque?
A common misconception is that, sincecalcium is a hard substance, the coronary calciumscore obtained on your heart scan provides ameasure of only hard plaque. Not true. Calciummeasured is a reflection of total plaque, both softand hard.
Actually, the great majority of people withcoronary plaque have a mixture of hard and softplaque, and this can change even day to day, weekto week, since plaque is a dynamic, living tissue. Inother words, a soft plaque today can develop hardelements tomorrow, and a hard plaque today canevolve to develop soft parts at any time in the future.Most plaques, in truth, are both. That’s why yourheart scan score is such a great measure of hidden,total, plaque.
26
Chapter One
Selected References
Rationale for coronary calcium measurement asa measure of total coronary plaque
Detrano R, Tang W, Kang X, Mahaisavariya P,McCrae M, Garner D, et al. Accurate coronarycalcium phosphate mass measurements fromelectron beam computed tomograms. Am J CardiacImag 1995; 9:167-173.
Janowitz WR, Agatston AS, Kaplan G, Viamonte J Jr.Differences in prevalence and extent of coronaryartery calcium detected by ultrafast computedtomography in asymptomatic men and women. Am JCardiol 1993; 72:247-254.
Rumberger JA, Simons DB, Fitzpatrick LA, SheedyPF, Schwartz RS. Coronary artery calcium areas byelectron beam computed tomography and coronaryatherosclerotic plaque area: a histopathologiccorrelative study. Circulation 1995;92:2157-2162.
Simons DB, Schwartz RS, Edwards WD, SheedyPF, Breen JF. Noninvasive definition of anatomiccoronary artery disease by ultrafast computedtomographic scanning: a quantitative pathologiccomparison study. J Am Coll Cardiol 1992;20:1118-1126.
27
What Does My Heart Scan Show?
Chapter 2Chapter 2Chapter 2Chapter 2Chapter 2The Heart Scan Score:
A Glimpse into Your Heart’s Future
Wouldn’t you like to see your future?You could find out whether heart attack was
on the horizon, or whether you’ll never have tobe concerned with heart attack, stents, or bypasssurgery. If you knew that you were fated to suffera heart attack at, say, age 53, you’d then knowthat an intensive program of prevention would benecessary to keep this from coming true. On theother hand, if you knew you’d be spared from heartdisease in your lifetime, you could dispense withall the fuss about cholesterol and devote your timeand energy to other pursuits.
Of course, we can’t really see your future ina crystal ball. But the heart scan score is the clos-
28
Chapter Two
est thing we have to foresee your heart’s future—better than EKGs, better than cholesterol, betterthan stress tests, better than relying on howyou feel.
If your heart scan score is zero, your risk forheart attack is very low, or nearly zero. (Nobody’srisk for heart attack is truly zero; there’s alwayssome, even miniscule, risk, even if you’re a strap-ping, healthy 25-year-old.)
If your heart scan score is high, perhaps inthe 90th percentile, then your risk for heart attackis significant. The energy you invest now in yourprevention program will be well worth it. Not asgood as a crystal ball, but darn close.
Aren’t Severe Blockages Required to Have aHeart Attack?
A shocking revelation shook the cardiologyworld in the early 1990s. Up until then, cardiolo-gists believed that coronary plaque grew gradu-ally, got worse and worse until finally one day itbecame a 90 to 99 percent blockage that cut offblood flow to the heart muscle, yielding symp-toms like chest pain. Just a bit more plaque growthand the artery would close and cause heartattack. Numerous studies (based on heart
29
What Does My Heart Scan Show?
catheterizations) have now flatly disproven thiscommonsense theory.
In fact, it is the many “minor” plaques incoronary arteries that can, overnight, cause heartattack. Blockages might be only 10, 20, 30, or 40percent, but “erupt” because of internal plaqueactivity, eroding the thin covering separatingplaque contents from flowing blood. When inter-nal plaque contents succeed in eroding to the sur-face (a common phenomenon), a powerful trig-ger for blood clot formation ensues. A blood clotforms and expands, closing off your coronary ar-tery and resulting in heart attack. In other words,we should try to detect “minor” plaque in a per-son free of symptoms to anticipate the potentialfor future heart attack. Although it might be 10years in the future, the potential is there. Unfortu-nately, old habits die hard, and many physiciansstill focus only on trying to detect severe block-ages and ignore “minor,” though still potentiallyheart attack-causing, plaque.
30
Chapter Two
Learn from Bill Clinton’s Experience.
Former President Bill Clinton underwentstress (thallium) tests every year for five years. Aftercompleting his fifth test, he strode out and declaredto the press corps, “I aced it!” Indeed, Mr. Clintoncontinued his jogging and his cholesterol wasreported to be excellent at 179 mg/dl.
Shortly afterwards, in September 2004, Mr.Clinton developed chest pains and breathlessness.He was promptly admitted to New York-PresbyterianHospital. Extensive blockages of all three coronaryarteries (greater than 90 percent) were diagnosedthrough heart catheterization, and Mr. Clintonunderwent a quadruple coronary bypass operation.
USA Today reported that “Dr. AllanSchwartz, chief of cardiology at the hospital, saidthat given the extent of Clinton’s blockage there wasa ‘substantial likelihood that he would have suffereda substantial heart attack in the near future.’ Doctorsstopped Clinton’s heart for 73 minutes and put himon a heart/lung machine, a common practice inbypass surgery. [Surgeon Craig] Smith said that itwas ‘obvious relatively quickly that what he neededwas an operation.’” After the procedure, the doctorsboasted of their success, calling the procedurelifesaving. Media reports glowed with descriptions ofthe high-tech hospital care Mr. Clinton received.Senator Hilary Rodham Clinton publicly expressedher and her daughter, Chelsea’s, gratitude for thequality care the former President received in thehospital.
31
What Does My Heart Scan Show?
You Mean He Developed HeartDisease Overnight?
Now wait a minute!Before congratulating our medical system,
several questions need to be answered. If coronarydisease takes years to develop, why wasn’t itrecognized earlier, before it threatened his life? Howcould stress test after stress test be normal whenextensive coronary disease was present? How coulddoctors be satisfied with cholesterol values thatpermit life-threatening disease to develop? Theanswers to these questions are already available tous lesser mortals than Mr. Clinton. Had he and hisdoctors been better informed, it is highly likely thathis procedure would not have been necessary.
What Should Have Happened
Had Mr. Clinton’s doctors simply advisedhim, say, in 1996 on assuming the presidency for hissecond term, to take a 30-second heart scan, theywould have been shocked to learn that his scorewas very high, probably over 400, signifying exten-sive hidden coronary plaque. Once Mr. Clinton’shigh score was identified, a search for the causesshould have ensued, followed by correction.With five minutes of Mr. Clinton’s time, a powerfulprevention program could have been devised. Thiskind of information would likely have eliminated Mr.Clinton’s need for bypass surgery.
32
Chapter Two
Stress tests are commonly performed to detecthidden coronary plaque. Unfortunately, stress testsdo not detect hidden coronary plaque. This is pre-cisely why you might have a normal stress test onTuesday but suffer a heart attack on Friday. Stresstests are tests of blood flow, not of coronary plaque.Even if you have extensive coronary plaque butblood flow is maintained—an exceptionally com-mon situation—a stress test will be normal. You’llwalk around with loads of plaque just waiting for atrigger to rupture, but you’ll be unaware of it if youand your doctor relied on stress testing to detect it.
Then why do cardiologists and surgeons stentand bypass only severe blockages? The people whoend up with major heart procedures have, in gen-eral, come to attention because they’ve developedsymptoms of chest pressure or breathlessness thatlead to stress testing, then heart catheterization.These people are suffering symptoms from poor flowthrough their coronary arteries and to the heartmuscle from a plaque that ruptured. Restoring bloodflow through stents or bypass surgery is an effec-tive means to improve blood flow. The plaque thatruptured may have been only a 40 percent blockagethe day before. When a plaque has already ruptured,it is indeed a reasonable approach to bypass or stentthe blocked artery. However, don’t be misled intobelieving that only severe blockages pose risk.
33
What Does My Heart Scan Show?
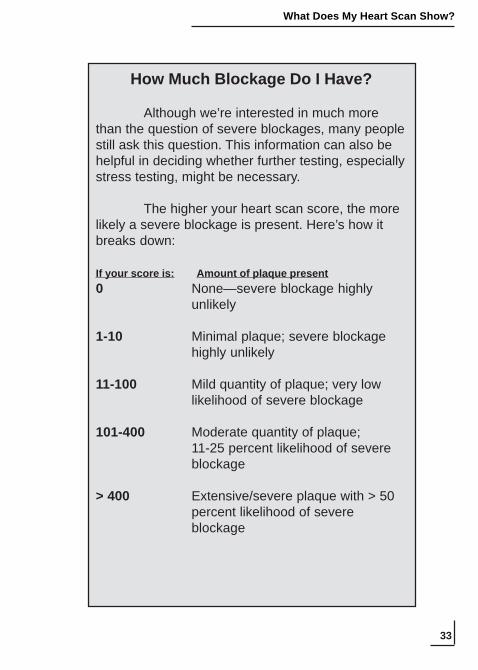
How Much Blockage Do I Have?
Although we’re interested in much morethan the question of severe blockages, many peoplestill ask this question. This information can also behelpful in deciding whether further testing, especiallystress testing, might be necessary.
The higher your heart scan score, the morelikely a severe blockage is present. Here’s how itbreaks down:
If your score is: Amount of plaque present0 None—severe blockage highly
unlikely
1-10 Minimal plaque; severe blockagehighly unlikely
11-100 Mild quantity of plaque; very lowlikelihood of severe blockage
101-400 Moderate quantity of plaque;11-25 percent likelihood of severeblockage
> 400 Extensive/severe plaque with > 50percent likelihood of severeblockage
34
Chapter Two
Find your score in one of the listed ranges,then find the description of the amount of plaquepresent. At a score of 200, for example, there is an11-25 percent chance that a severe blockage ispresent. (A specific calcium score cannot, however,be equated to a specific percent blockage, asplaque accumulates in various patterns along thelengths of arteries, and does not necessarily allaccumulate in one place and thereby create a singlesevere blockage. The calcium score can be associ-ated only with the statistical likelihood of a severeblockage.) Severe blockages can usually be de-tected by stress tests, since they are likely to blockblood flow with exercise.
Remember that any amount of plaque, evenin the absence of severe blockage, can result inheart attack because of plaque “rupture.” The moreplaque you have, the greater the likelihood of plaquerupture leading to heart attack.
35
What Does My Heart Scan Show?
Your Coronary Calcium Score PredictsYour Individual Risk of Heart Attack.
Study after study has shown that the higheryour heart scan score, the greater your risk forheart attack. This is because the more plaque thatlines the length of your coronary arteries, the moreopportunity there is to rupture and cause heart at-tack, even if the plaque is only a 20 percent block-age. This remains true even if you feel great, ifyour cholesterol is low, you’re a long-distancejogger, etc. The score is, by far, the most power-ful means of predicting your heart’s future avail-able. Of course, this does not mean that you can’tchange your future. In fact, that’s exactly whatknowledge of your heart scan should prompt youto do. If you find out that you have a high score,the next step is to begin or further improve yourprevention program. Your goal: to lower your riskfor heart attack to as close to zero as possible. (SeeChapter 4.)
Unlike cholesterol, your score represents thesum total of factors contributing to coronaryplaque growth up until the day of your scan. Let’ssay, for instance, that you spent the years betweenages 30 and 40 overweight, sedentary, smoking,and indulging in unhealthy eating habits. A cho-
36
Chapter Two
lesterol panel during those 12 years may have re-flected your unhealthy lifestyle. But, at age 41,you lose 60 pounds, begin an exercise program,follow a healthy diet, and stop smoking. A cho-lesterol panel after you’ve achieved all this wouldbe much improved—even if you had extensiveplaque in your coronary arteries. A heart scan atthis point, however, would likely reveal a highscore, as it reflects the sum total of influences inyour life. Your score would not falsely reassureyou, as a cholesterol panel would have.
The Percentile Rank—the Best HeartAttack Predictor of All
To some degree, the quantity of plaque con-tained in your coronary arteries is a product of“wear and tear,” the day in, day out stress yourarteries endure. Over age 65, for instance, onlyaround 25 percent of people will have heart scanscores of zero. Therefore, not all scores above zerosignify substantial risk for heart attack. For thisreason, another measure many scan centers reportis called the “percentile rank,” a measure of howyour score compares to other people in your age
37
What Does My Heart Scan Show?
group and sex. This serves to minimize theconfounding effect of wear and tear that may notimpact on heart attack risk.
In most centers, your total calcium score iscompared with a database of 35,000 other peoplewho’ve also been scanned, based on the enormousexperience provided by Dr. George Kondos at theUniversity of Illinois-Chicago. Dr. Kondos’s da-tabase allows us to compare your score with thou-sands of people your age and sex. We report thisas your “percentile rank.” The percentile rank isthe best predictor of heart attack risk, even betterthan your score alone.
For example, a 50-year-old female with ascore of 63 falls into a percentile rank of 90 per-cent. This means that 90 percent of all women herage had lower scores; 10 percent of women herage had higher scores. Although a score of 63 isnot all that high, in a 50-year-old female it stronglypredicts significant heart attack risk and demandspreventive attention. The 90th percentile also tellsus that this woman’s risk for heart attack is 4.5percent per year. (See box entitled “What’s myrisk of heart attack?”)
38
Chapter Two
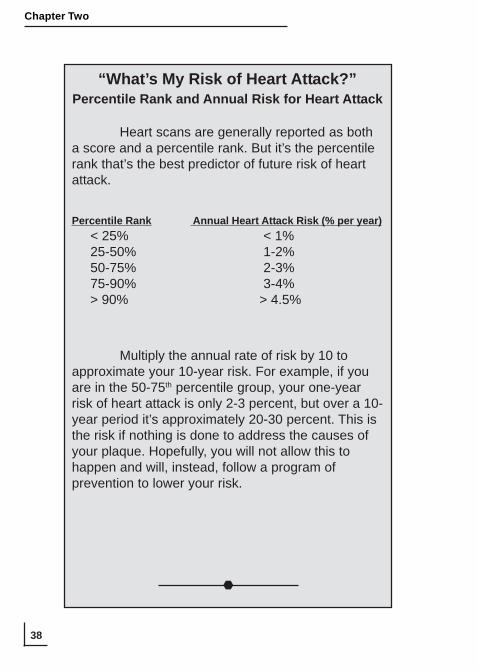
“What’s My Risk of Heart Attack?”Percentile Rank and Annual Risk for Heart Attack
Heart scans are generally reported as botha score and a percentile rank. But it’s the percentilerank that’s the best predictor of future risk of heartattack.
Percentile Rank Annual Heart Attack Risk (% per year) < 25% < 1% 25-50% 1-2% 50-75% 2-3% 75-90% 3-4% > 90% > 4.5%
Multiply the annual rate of risk by 10 toapproximate your 10-year risk. For example, if youare in the 50-75th percentile group, your one-yearrisk of heart attack is only 2-3 percent, but over a 10-year period it’s approximately 20-30 percent. This isthe risk if nothing is done to address the causes ofyour plaque. Hopefully, you will not allow this tohappen and will, instead, follow a program ofprevention to lower your risk.
39
What Does My Heart Scan Show?
For added perspective on percentile rank,let’s compare the same score in several differentpeople. For a 48-year-old man, a heart scan scoreof 100 represents a moderate amount of plaque.This score falls in the 75-90th percentile and re-flects moderately aggressive plaque growth andmoderate risk for heart attack. The identical scoreof 100 in a 65-year-old man represents the exactsame amount of plaque. But this second man’splaque is not as active since it took 65 years toaccumulate, rather than 48. This score falls in the25-50th percentile for men in this age group andposes only a small risk for heart attack. The samescore of 100 in a 48-year-old woman representsthe same amount of plaque but places her score inthe 99th percentile, reflecting aggressive plaquegrowth and high risk for heart attack. The signifi-cance of your heart scan score therefore dependsto a great degree on age and sex, and the best wayto judge this is to look at percentile rank. Mostscan centers will report percentile rank along withyour score. If not, see the table at the end of thischapter to obtain your percentile rank.
40
Chapter Two
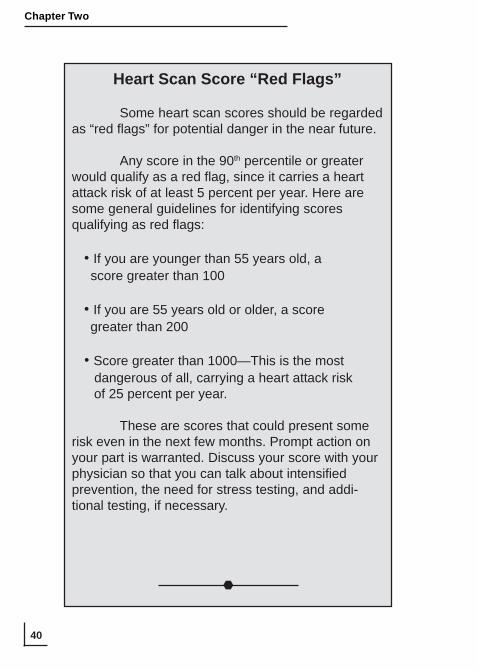
Heart Scan Score “Red Flags”
Some heart scan scores should be regardedas “red flags” for potential danger in the near future.
Any score in the 90th percentile or greaterwould qualify as a red flag, since it carries a heartattack risk of at least 5 percent per year. Here aresome general guidelines for identifying scoresqualifying as red flags:
• If you are younger than 55 years old, a score greater than 100
• If you are 55 years old or older, a score greater than 200
• Score greater than 1000—This is the most dangerous of all, carrying a heart attack risk of 25 percent per year.
These are scores that could present somerisk even in the next few months. Prompt action onyour part is warranted. Discuss your score with yourphysician so that you can talk about intensifiedprevention, the need for stress testing, and addi-tional testing, if necessary.
41
What Does My Heart Scan Show?
Risk for heart attack begins to be a matter totake seriously with scores in the 50th percentileand higher. Scores in the 50th percentile carry aheart attack risk of 1-2 percent per year (roughly10-20 percent over 10 years) and therefore justifya more intensive approach to prevention to loweryour risk. Scores in the 75th percentile, which carrya heart attack risk of 3 percent per year (roughly30 percent over 10 years) are even higher risk andclearly warrant intensification of your preventionprogram. (See Chapter 4.) The higher your per-centile rank, the higher your risk for plaque rup-ture and heart attack, and the more important yourpreventive efforts to reduce heart attack risk be-come.
42
Chapter Two
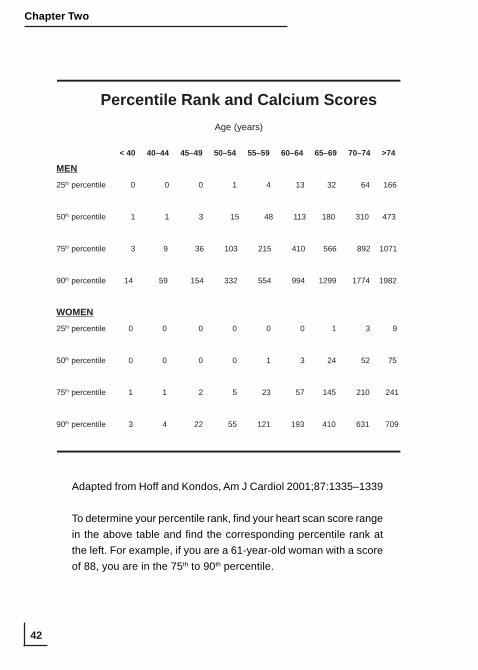
Percentile Rank and Calcium ScoresAge (years)
< 40 40–44 45–49 50–54 55–59 60–64 65–69 70–74 >74
MEN25th percentile 0 0 0 1 4 13 32 64 166
50th percentile 1 1 3 15 48 113 180 310 473
75th percentile 3 9 36 103 215 410 566 892 1071
90th percentile 14 59 154 332 554 994 1299 1774 1982
WOMEN25th percentile 0 0 0 0 0 0 1 3 9
50th percentile 0 0 0 0 1 3 24 52 75
75th percentile 1 1 2 5 23 57 145 210 241
90th percentile 3 4 22 55 121 193 410 631 709
Adapted from Hoff and Kondos, Am J Cardiol 2001;87:1335–1339
To determine your percentile rank, find your heart scan score rangein the above table and find the corresponding percentile rank atthe left. For example, if you are a 61-year-old woman with a scoreof 88, you are in the 75th to 90th percentile.
43
What Does My Heart Scan Show?
Selected References
Heart scans predict risk for heart attack
Arad y, Spadaro LA, Goodman K, Newstein D,Guerci AD. Prediction of coronary events withelectron beam computed tomography. J Am CollCardiol 2000; 36:1253-1260.
Kondos GT, Hoff JA, Sevrukov A, Daviglus ML,Garside DB, et al. Electron-beam tomographycoronary artery calcium and cardiac events: a 37-month follow-up of 5635 initially asymptomatic low-tointermediate-risk adults. Circulation 2003;107:2571-2576.
Wong ND, HSU JC, Detrano RC, Diamond G,Eisenberg H, Gardin JM. Coronary artery calciumevaluation by electron beam computed tomographyand its relation to new cardiovascular events. Am JCardiol 2000;86:495-498.
Wayhs R, Zelinger A, Raggi P. High coronary arterycalcium scores pose an extremely elevated risk forhard
Heart attacks originate from minor plaques
Ambrose JA, Tannenbaum MA, Alexopoulos D,Hjemdahl-Monsen CE, Leavy J, Weiss M, et al.Angiographic progression of coronary artery diseaseand the development of myocardial infarction. J AmColl Cardiol 1988;12:56-62.

44
Chapter Two
Giroud D, Li JM, Urban P, Meier B, Rutishauer W.Relation of the site of acute myocardial infarction tothe most severe coronary arterial stenosis at priorangiography. Am J Caardiol 1992;69:729-732.
Kuller LH, Shemanski L, Psaty BM, Borhani NO,Gardin J, Haan, MN, O’Leary DH, et al. Subclinicaldisease as an independent risk factor for cardiovas-cular disease. Circulation 1995;92:720-726.
Little WC, Constantinescu M, Applegate RJ, KutcherMA, Burrows MT, Kahl FR, et al. Can coronaryangiography predict the site of a subsequent myo-cardial infarction in patients with mild-to-moderatecoronary artery disease? Circulation 1988;78:1157-1166.
45
What Does My Heart Scan Show?
What a heart scan meant to…Martin.
At age 57, Martin felt he had it made. Heheaved a huge sigh of relief as the financial servicecompany he’d started in his mid-30s and built into amulti-million-dollar business was about to be finallypassed on to its new owners.
Over 20 years, Martin had worked 12- (ormore) hour days, six or seven days a week. He andhis wife, Betty, felt that it was time to take a well-deserved retirement. The plan to sell the businessand pass leadership onto another executive teamrequired a full 18 months of toil to bring the succes-sors up to speed. But it was finally done.
As part of their celebration, and beforedeparting for a month-long vacation in the South,Martin’s wife had scheduled Martin for a full check-up with his doctor to be certain he was in goodhealth. Everything checked out, including Martin’scholesterol numbers—LDL cholesterol 119 mg/dl,HDL 43 mg/dl, triglycerides 208 mg/dl. He had anormal blood pressure and even passed a stresstest. But when the doctor heard that Martin’s motherand father had both developed heart disease in theirearly sixties, he suggested a heart scan.
Martin’s heart scan score: 789, a scorehigher than 99 percent of all other men in his age
46
Chapter Two
group. When Martin heard this, tears came to hiseyes. “Twenty years of hard work and now this?”
“Whooooaaa! Hold on, Martin, don’t panic,”the doctor said. “You have no symptoms, youpassed a stress test. Your high score doesn’t meanyou need heart procedures, and it doesn’t meanyou’re going to drop dead tomorrow. It means thatwe’ve got to take your prevention program veryseriously so that a heart attack doesn’t develop. Infact, I think you should make it your goal to notrepeat the history of your mom and dad, and neverhave a heart attack or require a major heart proce-dure.”
Martin and Betty postponed their monthvacation for a few weeks in order to get started onsome of the prevention practices advised by hisdoctor. But Martin left for the South a confident man,feeling great and a lot smarter about his heartdisease risk.
47
What Does My Heart Scan Show?
Chapter 3Chapter 3Chapter 3Chapter 3Chapter 3Why Heart Scans Are Better Than
Cholesterol
Patti is a health-conscious 43-year-old mother ofthree school-aged children. Although the kids’ school andsports activities keep her on the go, she manages to squeezeaerobics and jogging into her schedule four times a week.At 125 pounds, she is proud to be among the thinnest of theother moms of her children’s friends. On the one occasionher cholesterol was checked, her doctor advised her thatthe numbers were spectacular: HDL cholesterol 86 mg/dl,LDL 77 mg/dl.
Despite the appearance of perfect health, herhusband, Eric, just two years older than Patti, suffered amini-stroke at age 45, which prompted an evaluation of hisheart. Extensive coronary disease was identified in Ericand he underwent triple bypass surgery successfully. Pattiwitnessed the emotional and physical roller coaster herhusband endured and couldn’t help but wonder whethersuch a fate was in her future, as well. After several months,
48
Chapter Three
when Eric was finally starting to feel and look his usualself, Patti decided to settle her mind and get a heart scan.Her score: 125, in the 90th percentile. When she relatedthis finding to her family physician, he was dumbfoundedand unable to account for why she had this degree ofcoronary plaque, given her excellent cholesterol levels.
A great cholesterol value is no guarantee ofbeing spared from heart disease, not even close.How can this be? Isn’t high cholesterol the num-ber one cause of heart disease in America?
Contrary to popular opinion, high cholesterolis not the most common cause of heart disease.There are many other causes for heart disease—cholesterol is just one item on the list.
The numbers provided by a cholesterol panelare also not etched in stone, but are likely to changeover time. Anyone who has had his cholesterolchecked more than once quickly recognizes thevariable nature of this test. Differences of 50 ormore points within just a few weeks are not un-common, even if you’ve not made any changes inyour lifestyle. It’s therefore hard, if not impos-sible, to decide from a single cholesterol panelwhether or not you have hidden heart disease.
Conversely, high cholesterol values do notnecessarily ensure a future of heart disease:
49
What Does My Heart Scan Show?
Barbara, a 50-year-old marketing manager, hadstruggled with her weight ever since the delivery of herthird child at age 36, and now tipped the scales at 189pounds at all of 5 feet 2 inches tall. Her doctor had warnedher repeatedly about the need to lose weight, particularlyto control her early diabetes, as well as to reduce LDLcholesterol, most recently 198 mg/dl, and raise HDL, lowat 40 mg/dl. In an effort to twist Barbara’s arm, her doctoradvised her to undergo a heart scan. He reasoned that clear-cut evidence of coronary plaque would finally persuadeBarbara to commit to lifestyle changes. Lo and behold,Barbara’s score: zero—no detectable plaque whatsoever,despite her apparent high-risk features.
The heart scan can swing both ways. It canshow you hidden coronary plaque when risk fac-tors suggest you should not have any, or it canreveal no coronary plaque when risk factors sug-gest that it should be present.
Why the discrepancy? First of all, risk fac-tors are just that: measures of risk, not of the dis-ease itself. In the same way, driving too fast onthe freeway is a risk factor for an auto accident,but it is not the same as an accident. Otherwise,most of us would have accidents every day!
Coronary plaque, such as that measured dur-ing a heart scan, is an actual measure of the dis-ease itself, i.e., coronary disease. Just as you canhave car accidents while driving too fast or driv-
50
Chapter Three
ing slowly, you can have coronary plaque regard-less of whether cholesterol is high or low. Thepresence of coronary plaque and cholesterol cor-respond statistically, but often do not agree in aspecific individual.
...plaque imaging is...not to be confused withrisk factors, which merely estimate a probabilityof developing atherosclerosis. Rather, [plaqueimaging] directly measures atherosclerosis, irre-spective of the presence or absence of risk fac-tors; it provides the final common denominatorand is the most powerful predictor of cardiacevents.
Harvey Hecht, MDDirector of Preventive Cardiology
Beth Israel Medical Center Albert Einstein College of Medicine, New York
Another confounding aspect to risk factorslike LDL cholesterol is that they are just snap-shots at a specific point in time. For instance, whatif you spent the first 40 years of your life over-weight, eating badly, and smoking? You turn acorner in your early 40s, lose 30 pounds, eathealthy foods, exercise, and lower your choles-terol. Although the unhealthy period of your life
51
What Does My Heart Scan Show?
caused a lot of plaque to appear and grow, choles-terol values obtained after your transformationwould not reflect this. This is a dramatic examplebut less dramatic situations occur everyday.
Conversely, a heart scan would show coro-nary plaque because it reflects the sum total ofcauses, cholesterol and others, that make plaqueappear and grow. Your heart scan score is muchmore than a simple snapshot in time subject today-to-day change. It reflects the sum total of ef-fects over your entire life up until the day of yourscan. This information is far more powerful andaccurate than fluctuating cholesterol values.
Then What Exactly Is Cholesterol?
What does cholesterol tell you? Cholesterolis a fatty substance carried by various proteins inthe blood that can become deposited within thethin lining of your arteries’ walls, creating plaque.The originators of the concept of cholesterol mea-surement several decades ago acknowledged thatit was an indirect and somewhat flawed index ofrisk for heart disease. As understanding of the di-verse causes of heart disease has evolved, it hasalso become clear that there are many causes ofheart disease that have nothing to do with choles-
52
Chapter Three
terol. Among these causes are inflammation (mostcommonly measured as c-reactive protein, orCRP), lipoprotein(a), homocysteine, fibrinogen,and high insulin levels. These factors can occurwith low cholesterol as easily as they can occurwith high cholesterol.
Nonetheless, cholesterol is indeed statisti-cally related to heart disease. Large studies likethe Framingham study and MRFIT, tracking tensof thousands of apparently normal people, haveconclusively shown that the higher your choles-terol, the more likely you are to have a heart at-tack, up to a maximum risk of three-fold higher.Both studies also showed that the great majority(80 percent) of heart attacks occurred among thegroup of people with average cholesterols, nei-ther high nor low. People in the low cholesterolgroup were not entirely safe, either, as they alsosuffered heart attacks, though at a statisticallylower rate than those with high cholesterol.
The difficulty with cholesterol comes whentrying to apply statistical observations on largegroups of people to a single individual—it all toofrequently breaks down. It’s especially difficultin people with average cholesterol values. Say wehave a 50-year-old woman with a total cholesterolof 200, LDL cholesterol of 135. Can you predict
53
What Does My Heart Scan Show?
whether she’s going to have a heart attack withinthe next ten years? Can you predict that she mightlead a life free of heart disease? No, you cannot,yet this is the question your doctor tries to an-swer.
If we use cholesterol as our initial decision-making point, we will be misled all too often. Youcould also submit to extensive surveys of labora-tory tests in the hopes of identifying some or allof the potential causes of coronary plaque. Or, youcould simply and easily measure the end result ofall risk factors combined and get a heart scan.
Selected References
Achenbach S, Nomayo A, Couturier G, Ropers D,Pohle K, et al. Relation between coronary calciumand 10-year risk scores in primary preventionpatients. Am J Cardiol 2003:92:1471-1475.
Greenland P, Gaziano JM. Selecting asymptomaticpatients for coronary computed tomography orelectrocardiographic exercise testing. N Engl J Med2003;349:465-73.
Grundy SM. Coronary plaque as a replacement forage as a risk factor in global risk assessment. Am JCardiol 2001 Jul 19;88(2A):8E-11E.
54
Chapter Three
Grundy SM. Coronary calcium as a risk factor: rolein global risk assessment: [Comment]. J Am CollCardiol 2001;37:1512-1515.
Hecht HS, Superko R, Smith LK, McColgan BP.Relation of coronary artery calcium identified byelectron beam tomography to serum lipoproteinlevels and implications for treatment. Am J Cardiol2001;87:406-412.
Hoff JA, Chomka EV, Krainik AJ, Daviglus M, Rich S,Kondos GT. Age and gender distributions of coro-nary artery calcium detected by electron beamtomography in 35,246 adults. Am J Cardiol2001;87:1335-1339.
Janowitz WR, Agatston AS, Kaplan G, Viamonte J Jr.Differences in prevalence and extent of coronaryartery calcium detected by ultrafast computedtomography in asymptomatic men and women. Am JCardiol 1993; 72:247-254.
Kondos GT, Hoff JA, Sevrukov A, et al. Electronbeam tomography coronary artery calcium andcardiac events: a 37-month follow-up of 5635 initiallyasymptomatic low- to intermediate-risk adults.Circulation 2003;107:2571-2576.
55
What Does My Heart Scan Show?
What a heart scan meant to…Linda.
Linda prided herself on her high-energypersonality. At age 59, she had more energy thanmany 30-year-olds. Since her oldest child marriedand moved from home, she had plenty of time todevote to healthy eating and exercise. She helddown a full-time job, as well, as a marketing man-ager for a small architectural firm. At 5 foot 2 inchesand 120 pounds, Linda was also quite proud of thefact that she weighed half that of many friends andcoworkers.
The only dark cloud in Linda’s otherwiseterrific life was that her husband, Donald, wasstruggling with heart disease. After a bypass opera-tion at age 54 followed by two catheterizations andthree stents, Linda worried about Donald’s long-termhealth and whether they’d be able to enjoy theretirement they’d planned in three years. Linda reallygave no thought whatsoever to the idea of whetheror not she had heart disease, too. After all, it wascancer that had taken her mother at age 66, and asister had undergone a mastectomy several yearsearlier for early breast cancer. But it was Donald’sconcern for Linda and his wish that she not have tosuffer the hospitalizations and procedures that he’dendured that prompted him to buy a heart scan forhis wife for Mother’s Day.
Linda reluctantly gave in to Donald’s wish,mostly to not seem ungrateful for his concern. Her
56
Chapter Three
score: 168, in the 97th percentile for women in herage group. An unusual quantity of calcified plaquewas also seen in the aorta just above the heart, afinding that the interpreting cardiologist warned wasa risk for future stroke. Linda was stunned. Far frombeing the one spared from heart disease, Linda sawthat her future was going to be just like herhusband’s unless preventive action was taken rightaway.
Thankfully, Linda quickly saw the silverlining in this news: It was a reason to work togetherwith her husband on improving their lifestyles. Sheobtained some insight into what Donald had beenexperiencing, as well, and it actually brought themcloser in their relationship. Having knowledge of herrisk really crystallized Linda’s commitment to herprevention program and she’s proven a source fortremendous support and inspiration to her husband.
57
What Does My Heart Scan Show?
Chapter 4Chapter 4Chapter 4Chapter 4Chapter 4Does My Testing End Here? Will I Need
Other Tests?
Does a heart scan provide all the answers foryour heart?
As powerful as a heart scan can be, it doesn’tprovide all the answers to every heart question.After getting your heart scan, the need for furthertesting is determined by a number of factors, butmostly by how high your total score is and whetheryou have symptoms that could be attributable toyour heart (which should be decided by your doc-tor). Other factors can enter into your doctor’sdecision, such as the appearance of your EKG (ifit’s abnormal, this might tip the scales in favor offurther testing), if there’s anything in your historyto suggest a prior heart attack or other heart-re-
58
Chapter Four
lated event, and other heart-related issues likeblood pressure and the presence of atheroscleroticplaque in other areas of the body, like the carotidsor leg arteries.
Let’s discuss some of the most common ques-tions that arise following a heart scan:
Do I Need a Stress Test?What exactly is a stress test? A stress test is
nothing more than an opportunity to observe howyou and your heart react to exercise, usually on atreadmill, over a few minutes of effort. The exer-cise itself is really no different from what youmight do on your own. After all, you could justwalk on a treadmill at the gym and achieve thesame amount of exertion as most medically-moni-tored stress tests.
Walking on a treadmill is a means of physi-cally challenging the heart, increasing the heartmuscle’s need for blood flow to supply oxygen.For this reason, treadmill tests often incorporateincreasing walking speed as well as incline to in-crementally subject the heart to greater and greaterwork. If you’re unable to walk due to arthritis orother limitations, the treadmill can be replaced byvarious pharmacologic methods of stimulating theheart muscle.
59
What Does My Heart Scan Show?
The stress portion of the test, whether bytreadmill or otherwise, is often combined with oneof several methods to assess the adequacy of bloodflow to the heart. Thallium imaging, a method thatgauges blood flow to the heart muscle, is amongthe most common. Echocardiography is an alter-nate imaging method used to observe the heartmuscle’s ability to meet increased work demandsby observing its contraction pattern.
Stress tests are limited by the fact that, un-less blood flow to the heart is markedly dimin-ished, they will be entirely normal. If your coro-nary arteries are lined with, for example, dozensof 20-40 percent blockages, none of which blockblood flow, your stress test will be entirely nor-mal. You won’t have chest pain with exercise, norwill you be breathless. Your EKG will be normaland the images of your heart (thallium, echo, orother) will show normal blood flow or normalheart function. Your extensive coronary plaquewill not be detected and you’ll likely be told (in-accurately) that your heart is fine. But you are sit-ting on a time bomb made of hidden plaque, justwaiting for that trigger to rupture, since your un-recognized and unmeasured plaque likely will notprompt you or your doctor to take any preventiveaction.
60
Chapter Four
It is clear that stress tests are an ineffectivemeans to screen asymptomatic people for hiddencoronary plaque. These limitations of stress testshave been repeatedly recognized by the Ameri-can Heart Association. Stress tests, however, canbe used effectively in other ways. They can be anespecially useful method for your doctor to sortout the significance of symptoms. If you reportan ache in your chest to your doctor, an EKG anda stress test can help understand whether the chestdiscomfort is an impending heart attack or someother cause. Other causes might include a hiatalhernia (when the upper stomach slides up anddown through a hole in the diaphragm), esoph-agitis (inflammation of the esophagus), gallstones,and other problems, since many disorders causesimilar symptoms. Symptoms that are reproducedwhile walking on a treadmill and that are associ-ated with specific abnormalities on the EKG orimaging portion of the test can more confidentlybe blamed on heart disease.
Stress tests, in their many forms, are, there-fore, tests of coronary blood flow, not of coronaryplaque. Of course, if coronary plaque accumulatesin such a fashion that blood flow is substantiallycut back, then a stress test will show abnormali-ties. You can presume, then, that if your stress test
61
What Does My Heart Scan Show?
is abnormal, there’s a good chance that you haveextensive coronary plaque sufficient to block flow.Further tests such as heart catheterization may thenbe indicated; this should be decided by your doc-tor.
But if you have a normal stress test, you can-not safely assume that no coronary plaque ispresent. Plaque can, in fact, be extensive withoutcutting back on blood flow. That’s precisely whatheart scanning can measure. Unlike stress tests,heart scans are black or white, never murky. Ei-ther you have plaque or you don’t, and when youhave plaque you can be told precisely how muchdown to a cubic millimeter of confidence.
62
Chapter Four
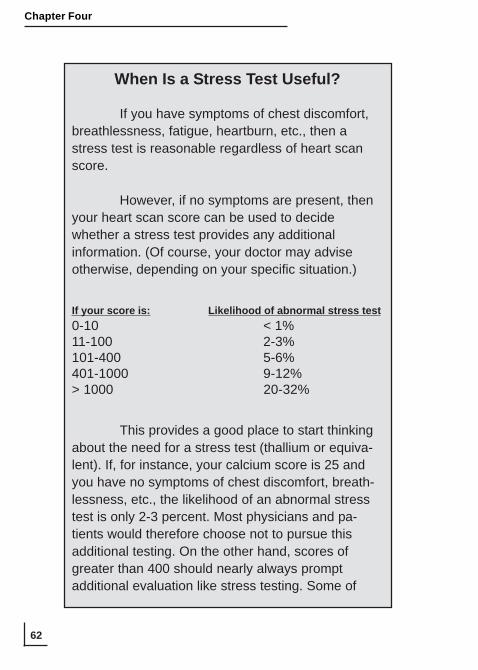
When Is a Stress Test Useful?
If you have symptoms of chest discomfort,breathlessness, fatigue, heartburn, etc., then astress test is reasonable regardless of heart scanscore.
However, if no symptoms are present, thenyour heart scan score can be used to decidewhether a stress test provides any additionalinformation. (Of course, your doctor may adviseotherwise, depending on your specific situation.)
If your score is: Likelihood of abnormal stress test0-10 < 1%11-100 2-3%101-400 5-6%401-1000 9-12%> 1000 20-32%
This provides a good place to start thinkingabout the need for a stress test (thallium or equiva-lent). If, for instance, your calcium score is 25 andyou have no symptoms of chest discomfort, breath-lessness, etc., the likelihood of an abnormal stresstest is only 2-3 percent. Most physicians and pa-tients would therefore choose not to pursue thisadditional testing. On the other hand, scores ofgreater than 400 should nearly always promptadditional evaluation like stress testing. Some of
63
What Does My Heart Scan Show?
these people may require “revascularization,” or aprocedure to restore flow to the involved area, suchas stent placement or bypass surgery.
If some people need to have a stress testanyway, why bother with a heart scan? Because themajority of people (greater than 90 percent) withcoronary plaque will have normal stress tests. Asdiscussed above, any quantity of coronary plaque—whether or not it yields a stress test abnormality—carries risk for heart attack. Even people with ascore of 400—a high score signifying advanced andextensive plaque—have only a 9-12 percent chanceof detecting heart disease by stress testing. Theother 88-91 percent with normal stress tests wouldbe told their coronaries were fine, even thoughthey’re really loaded with plaque.
64
Chapter Four
The majority of people who have heart dis-ease have no symptoms whatsoever and thereforehave “silent” coronary plaque. But as heart scanscores increase, so does the likelihood that plaqueis bulky and large, and that blood flow will bereduced during exercise, thereby yielding an ab-normal stress test. Stress test abnormalities willbe detected in a fairly predictable way judging byyour heart scan scores. If your heart scan score is200, for instance, the likelihood of a stress testabnormality is around 5-6 percent. See the chartto gauge your likelihood of an abnormal stress testbased on your heart scan score. If you undergo astress test because of a high heart scan score andthe stress test proves abnormal, then your doctorwill need to talk to you about further testing (e.g.,heart catheterization). When blood flow is reducedto the heart muscle, the likelihood of dangerousevents (heart attack, unstable heart rhythms, heartfailure) increases.
Will I Need a Heart Catheterization?
If you’ve had your heart scan, will you needheart catheterization?
First of all, if you do not have symptoms suchas chest pain/pressure, breathlessness, or other
65
What Does My Heart Scan Show?
symptoms attributable to your heart (a decisionthat should be made by your doctor), just havingplaque detected by itself is almost never a reasonto have a heart catheterization. In other words, youmight have a relatively high score, say 500, thatat age 53 puts you in the 99th percentile. But ifyou don’t have symptoms, then proceeding di-rectly to invasive procedures is rarely justified.Just having plaque is an insufficient reason toproceed directly to major procedures. It is a rea-son to consider stress testing, however, with thelikelihood of abnormality by stress testing depen-dent on how high your score is. (See page 62.)
There are three principal reasons to havea heart catheterization:
• Symptoms—If you have chest pain,breathlessness, or other symptoms that your doc-tor feels are suspicious for heart disease, a cath-eterization might be considered, since the likeli-hood of a severe blockage (from a plaque that hasruptured) and impending heart attack are greater.
• Abnormal stress test—Abnormal find-ings on a stress test indicate poor blood flow tothe heart muscle. This presents dangers that can
66
Chapter Four
make physical exertion and exercise unsafe, andcan raise the near-term risk of heart attack.
• Abnormal heart muscle (left ventricu-lar) function—This is a very serious finding thatsuggests that a heart attack has occurred in thepast or is about to occur.
Most people who’ve undergone a heart scanand have no symptoms should have a stress test priorto any conversation about the need for heart cath-eterization. The need for major cardiac procedureslike heart catheterization, which then often lead tostents, bypass surgery, etc., in asymptomatic peopleshould be based on the finding of “ischemia,” orpoor blood flow to one or more territories of theheart, not simply on the presence of plaque. Thispoint is so important and so often misunderstoodthat it bears repeating: Even though your heart scanscore identifies the presence of plaque, having plaqueby itself is almost never a reason to have heart cath-eterization or other invasive procedures.
If you have no symptoms and your calciumscore is greater than zero, before the need for inva-sive cardiac procedures is decided, you will need astress test. It’s as simple as that.
67
What Does My Heart Scan Show?
What about Stents and Bypass Surgery?
Similar to the decision to proceed with heartcatheterization, the decision to have stents or by-pass surgery should proceed logically and onlywhen properly indicated. It is appropriate, for in-stance, to get to this point if you’ve had a stresstest due to a high heart scan score, the stress testshows abnormalities suggesting poor blood flow,and a heart catheterization shows severe block-ages and/or diminished heart muscle strength.Stents or bypass surgery to restore flow may be alogical solution in this situation.
But just having plaque is still insufficientreason to proceed directly to stents or bypass. Thesame logical sequence that leads to heart catheter-ization should be employed to make the decisionto proceed to stents or bypass, as well.
Is there a role for “prophylactic” stents orbypass? Say you have a high heart scan score like400, have no abnormalities by stress testing, andno symptoms. You therefore probably have manylow-grade, “mild” blockages in the 20-40 percentblockage range. Should you have multiple stentsor bypass grafts put in just to prevent a heart at-tack? Absolutely not. Procedures, even in the besthands, carry risks, and the risk of the procedure
68
Chapter Four
can, in many instances, exceed the dangers of justhaving plaque. Procedures are also not perfect.Stents implanted into arteries provoke a tissuegrowth response and you could conceivably startwith a minor blockage of 20 percent that ends up40 percent six months after your stent is placed!Bypass grafts inserted into arteries with minorblockage often do not “take” because the vigor-ous flow in the artery can cause the graft to close(because of competing sources of flow and col-lapse of the graft). For these reasons, no one ad-vocates stents or bypass surgery as a preventiveprocedure for “mild” blockages.
Does this mean that, if you have plaque anddon’t need a procedure, that you’re simply out ofluck and resigned to a heart attack in your future?No. In fact, this is the best situation of all (be-sides, of course, not having any plaque). It meansthat you’ve had your coronary plaque detectedbefore danger is imminent, allowing you time todevelop a prevention program and shut down yourplaque to prevent a future heart attack. It’s okayto have plaque, but you don’t want active plaque.In the next chapter, we’ll discuss how your heartscan can become the centerpiece of your heartdisease prevention program.
69
What Does My Heart Scan Show?
Selected References
How coronary calcium scores correlate withstress testing
Berman DS, Wong ND, Gransar H, et al. Relation-ship between stress-induced myocardial ischemiaand atherosclerosis measured by coronary calciumtomography. J Am Coll Cardiol 2004;44:923-930.
He Z, Hedrick TD, Pratt CM, Verani MDS, Aquino V,Robert R, Mahmarian JJ. Severity of coronary arterycalcification by electron beam computed tomogra-phy predicts silent myocardial ischemia. Circulation2000;101:244-251.
70
Chapter Four
What a heart scan meant to…Corrine.
“Corrine, it’s really time you started worryingabout your own health,” advised Corrine’s olderbrother, Drew, just after his most recent hospitaliza-tion for his heart. And she knew he was right.
Corrine herself had wondered on manyoccasions whether heart disease was in her future,too. Her concerns were particularly acute duringvisits to Drew in the hospital during his numerousadmissions over the years. Drew was older thanCorrine by only seven years, but by age 65 hadendured a bypass surgery, countless heartcatheterizations, and seven stents.
Heart disease was clearly in the family, astheir dad had suffered a heart attack at the age of51, though had survived another 10 years after-wards, and his father before him shared a similarhistory. Corrine had read that the onset of heartdisease in women tended to occur a decade laterthan men, but that safety cushion had alreadypassed. Drew began his struggle with heart diseaseat age 46, and Corrine was now 58 years old.
After the prodding from her brother, Corrineagreed to have her heart scan. Her score: 217, inthe 99th percentile compared to other women in herage group (heart attack risk 4.5 percent per year).Corrine’s stress test was normal, and she sufferedno symptoms during the test and hadn’t had anychest pain or breathlessness on her own. Her doctor
71
What Does My Heart Scan Show?
therefore helped Corrine develop a preventionprogram that included daily exercise, weight loss of18 pounds, and treatment for her somewhat highLDL cholesterol and low HDL, with the goal ofkeeping Corrine from repeating Drew’s history.

73
What Does My Heart Scan Show?
Chapter 5Chapter 5Chapter 5Chapter 5Chapter 5What Should I Do with My Heart Scan
Score?
You’ve undergone a scan and you’re now theproud owner of your very own heart scan score.What will happen to your score if you sit backand complacently do nothing?
The answer is simple: Your score will in-crease—dramatically.
Elliot is a busy, ambitious real estate broker. At52 years old, he was in good physical shape, playing ballwith his teenage kids on the weekends and singles tennisonce a week, not to mention the walking he did as part ofhis business. Elliot’s wife, Rachel, had undergone a heartscan as soon as it became available in their area, and wasthrilled with her score of zero. But she was concerned aboutElliot, since his mother had died of a heart attack withoutwarning at age 63. When they first talked about it, Elliotpromptly rejected the idea, refusing to believe that he could
74
Chapter Five
have any hidden heart disease since he felt fine, even duringexercise. But Elliot finally caved in after repeated proddingfrom Rachel. His score: 162, in the 75th percentile. Elliotwas a little surprised at first, but lack of time and thedistractions of life and work eventually caused him to forgetabout his scan. Anyway, when he mentioned his heart scanscore to his family doctor, the doctor just shrugged. “Youfeel fine, don’t you? Don’t worry about it.”
Another year passed. Elliot never gave his heartscan another thought, but Rachel did. She remained veryconcerned about Elliot’s score and the lack of directionprovided by his doctor. For his 53rd birthday, Rachel boughtElliot another scan. This time the score was 228, a 40percent increase. This really grabbed Elliot’s attention andhe agreed to seek help to deal with his rapidly growingheart attack risk.
If, like Elliot, nothing is done to address thecauses of your plaque, the score will increase 30percent, 40 percent, or more per year. Once plaquegets a foothold in your coronary arteries, it cangrow at a dizzying pace. Imagine if your invest-ments grew at this pace—you’d be rich in just afew years! Of course, plaque cannot continue togrow at this rate or else you would become onelarge hunk of plaque. Instead, plaque grows andbecomes progressively more unstable until thatday when it erupts, exposing its internal contentsto blood, triggering blood clot formation, and youexperience a heart attack.
75
What Does My Heart Scan Show?
People who allow their plaque to grow at arate greater than 20 percent per year may experi-ence as much as a 20-fold higher risk of heart at-tack compared to someone who keeps his scorestable. By allowing his score to increase 40 per-cent over just a single year, Elliot exposed him-self to a risk 20-fold higher than was necessary.
Let’s agree that we should not allow that tohappen.
Lipids—Tools for Control of Your Score
Once you’ve had a heart scan, you know pre-cisely how much plaque is hidden in your coro-nary arteries. We also know that, if you do noth-ing to correct the causes—which you shouldn’tdo—then your score will increase 30 percent peryear, on average.
Here’s where your cholesterol, or “lipid,”panel comes in. Although lipids have limited use-fulness to uncover hidden coronary plaque, theycan be used as important tools to gain control ofplaque.
The standard lipid panel consists of four ba-sic measures:
• Total cholesterol• LDL cholesterol
76
Chapter Five
• HDL cholesterol• Triglycerides
You and your doctor should review your lip-ids in light of your heart scan score, as your scorewill influence how to approach your lipid patterns.In fact, the treatment for your lipids will dependheavily on your heart scan score.
To illustrate how your heart scan score in-fluences management of your lipid values, let’ssay that your lipids show the following:
Total cholesterol 223 mg/dlLDL cholesterol 138 mg/dlHDL cholesterol 45 mg/dlTriglycerides 199 mg/dl
Your numbers are neither great nor terriblybad. Your LDL cholesterol, for instance, is aroundaverage for American adults (average LDL 131mg/dl; average LDL for people with heart attacks134 mg/dl). Your pattern could be responsible fora fatal heart attack at age 50, or no heart diseaseat all in your lifetime—your lipid panel won’t tellyou which. But, say your heart scan score waszero, meaning no detectable plaque whatsoever.Since your heart attack risk based on a score ofzero is nearly zero for the next three to five years,
77
What Does My Heart Scan Show?
a program of lifestyle changes, like nutritionalstrategies to lower cholesterol (see box on page85), might be all that is necessary. Because yourrisk is extremely low, it can’t be substantially low-ered further by cholesterol medicines or other pre-scription agents. Why go crazy over cholesterolif your risk for heart attack is nearlyunmeasurable? While you and your doctorshouldn’t ignore your lipids, the approach canproceed over an unhurried timeline and the inten-sity of effort will be far less.
What if you have the same lipid numbersabove but your heart scan score is 1200? You haveextensive hidden plaque. Even if you feel greatand your stress test is normal, your risk for heartattack is an alarming 25 percent per year. Giventhe risks identified by your extremely high heartscan score, you and your doctor need to attackyour lipids very seriously. While lifestyle and nu-tritional strategies will be important, you mightmore readily consider medication to bring yourrisk under control. The lipid endpoints achievedthrough your treatment program will also be moredemanding, with a lower LDL and total choles-terol target, higher HDL, and lower triglycerides.In other words, your high risk for heart attack dic-tates a more intensive approach to prevention thanif your score were zero.
78
Chapter Five
The quantity of plaque hidden in your coro-nary arteries therefore determines how to manageyour lipid values. Without knowledge of the ex-tent of your hidden plaque, you’re wandering inthe dark. With this concept in mind, let’s tackleeach of the lipid measures one by one:
LDL Cholesterol
The tools for lowering LDL cholesterol havebecome very powerful since the “statin” choles-terol-lowering drugs entered the arena. There arealso many helpful nutritional strategies you canuse to lower LDL. Lowering LDL cholesterolshould be among your priorities if you have a heartscan score above zero.
How far should LDL be lowered? A goodstarting place is to refer to the Adult TreatmentPanel (ATP) of the National Cholesterol Educa-tion Program. This is a set of guidelines draftedby authorities on cholesterol to provide a refer-ence for your doctor to use in considering treat-ment for cholesterol.
The ATP defines a person as “high-risk” ifthere is probability of heart attack or other car-diac event of 20 percent over a 10-year period. Ifyou’re 50 years old, for instance, your risk of heart
79
What Does My Heart Scan Show?
attack would be 20 percent by age 60. People whoclearly qualify as high-risk include anyone whohas suffered a prior heart attack or had angioplasty,stent, or bypass surgery, and anyone with carotidartery disease, leg artery blockages, abdominalaneurysm, or diabetes. You can also be high-riskwith some combinations of two or more risk fac-tors. (See box on page 80 entitled “How to calcu-late your 10-year risk: The Framingham Risk Cal-culator.”)
From a heart scan viewpoint, a score in the75th percentile or greater should be regarded ashigh-risk, since scores in this range carry a 10-year risk of 20 percent or greater. Any score abovethe 75th percentile clearly qualifies as high-risk,since the 10-year risk is even higher.
Anyone in the high-risk category is advisedto have LDL cholesterol lowered to less than 100mg/dl through lifestyle, diet, and medication, ifnecessary. A recently updated set of guidelinesdrafted by the Adult Treatment Panel (NCEP Re-port, 2004) suggests that targeting 70 mg/dl mightbe considered, but makes this optional. This up-date was based on several recent clinical trials thatproved that lower LDL cholesterol targets trans-lated into less heart attack and death, as well asgreater plaque regression.
80
Chapter Five
How to Calculate Your 10-Year Risk:The Framingham Risk Calculator
The ATP guidelines apply the risk calcula-tions based on the Framingham study. This scoringsystem incorporates the following risk factors:
• Total cholesterol• HDL cholesterol• Smoking• Systolic blood pressure
A 10-year risk for coronary events is thencalculated. To have your 10-year risk calculated, goto the National Heart, Lung, and Blood Institutewebsite (www.nhlbi.nih.gov) and enter “risk calcula-tor” into the search bar. You then enter your per-sonal information on each of the risk factors into theboxes and a 10-year risk will be calculated.
In this approach, high-risk is arbitrarilydefined as risk for heart attack of 20 percent orgreater over 10 years. Intermediate-risk is definedas a risk of 10-20 percent over 10 years. Low-risk isless than 10 percent over 10 years. Keep in mindthat this framework is only a suggested guideline,not a set of rules. You and your doctor may chooseto modify this approach to suit your unique goalsand medical situation. Some people, for instance,because of the murkiness of heart attack prediction,prefer to follow guidelines for the high-risk categoryeven if they are really intermediate-risk. In this way,they may maximize the protection provided by aprevention program.
81
What Does My Heart Scan Show?
The ATP classifies “intermediate-risk” as a10-year risk of heart attack of 10-20 percent.People with combinations of two or more risk fac-tors generally fall into this category. For peoplein the intermediate-risk category, ATP recom-mends lowering LDL cholesterol to less than 130mg/dl. The recent updates make a target LDL of100 mg/dl or less optional. A heart scan score per-centile rank of 50-75 percent would fit into thiscategory.
Lastly, ATP guidelines suggest lowering LDLcholesterol to 160 mg/dl if you fall into the low-risk category with likelihood of heart attack of 10percent or less over the next 10 years. This corre-sponds to a heart scan percentile rank of less thanthe 50th percentile.
Keep in mind that the ATP guidelines are justthat: guidelines. They are not rules. There are nopenalties to pay if you and your doctor choose tofollow a different course. The ATP guidelines areonly advice based on evidence gained throughlarge clinical trials. They represent a consensusviewpoint drafted by committee. You and yourdoctor may choose to modify these guidelines tosuit your particular situation and needs.** In our program of coronary regression, in which we aim to reduce your heart scanscore, we target lipid panel values of 60/60/60, i.e., an LDL cholesterol of 60 mg/dl orless, HDL cholesterol of 60 mg/dl or greater, and triglycerides of 60 mg/dl or less. Thisis detailed in the book Track Your Plaque: The only heart disease prevention programthat shows how to use the new heart scans to detect, track and control coronaryplaque. Please refer to this book if a program of plaque regression, or shrinkage,interests you, or go to www.trackyourplaque.com.
82
Chapter Five
Why Do We Need Heart Scans If We CanCalculate Our Heart Attack Risk?
Some people ask whether heart scans arereally necessary if we can gauge our risk for heartattack by using predictors like the Framingham riskcalculator (see box on page 80).
One of the drawbacks of risk calculators is thatthey are population-based measures. They are helpfulfor predicting risks within large groups of people. Theirgreat weakness is in predicting the risk of a specificindividual.
To illustrate, imagine if you were told thatdriving on the freeway at greater than the speed limit of65 mph carries a three-fold greater risk of dying in acar accident than driving below the speed limit. If youdrive 68 mph, does this mean you will die in a high-speed accident? Does driving 63 mph mean you’llnever die in an accident? Of course not. These aremeasures of relative risks based on the behavior oflarge populations. The same applies to risk calculators.
This leads to a phenomenon called “mis-classification of risk.” The risk calculator may, forinstance, suggest a low risk for heart attack of 3percent over 10 years. But your heart scan—a specificgauge of your individual risk—might suggest a risk of20 percent. In this instance, your individual measure,i.e., your heart scan score, is a far more precisereflection of your risk. If you start with a heart scan asthe basis for your prevention program, then riskcalculators like the Framingham scheme simply shedlight on how to best approach treatment to reduce risk,but fall short on determining whether you have heartdisease in the first place.
83
What Does My Heart Scan Show?
There are several approaches to loweringLDL cholesterol:
• Statin agents—These are the cholesterol-lowering drugs Lipitor ™ (atorvastatin), Crestor™(rosuvastatin), Zocor™ (simvastatin),Pravachol™ (pravastatin), and Mevacor™(lovastatin). LDL is lowered from 25 to 60 per-cent on these agents, depending on the one cho-sen and dose.
• Bile acid binding agents—Nowadays, theonly common agent remaining in this class iscolvesevalam (Welchol™). The LDL-loweringpotency is rather modest and this agent is mostcommonly used with the statin drugs to increaseeffectiveness.
• Ezetimibe (Zetia™) is in a class by itself,as it is neither a statin drug nor does it bind cho-lesterol in the intestinal tract, but blocks the ab-sorption of cholesterol across the intestinal lin-ing. It is most commonly used with statin drugs,as it quadruples their potency with no substantialincrease in side effects. It can lower LDL by 18percent when used alone.
84
Chapter Five
There are several specific nutritionalsupplement approaches worth knowing about,as well, that can lower LDL cholesterol 20 to 50points. (See box on page 85.) Any of thenutritional strategies listed can be used safelywith any of the prescription agents describedabove.
HDL Cholesterol
Most people are surprised to learn that themost common reason to have coronary plaque inthe first place is low HDL cholesterol, not highcholesterol. The ATP panel defines low HDL asless than 40 mg/dl, although it may be a risk fac-tor up to a level of 60 mg/dl.
HDL is a protective class of blood particlesresponsible for a process called “reverse choles-terol transport,” or scavenging cholesterol fromplaque. HDL is therefore critically important forregression of plaque.
Of every 100 people with heart disease, atleast 50 have low HDL. It is the cause of heartdisease in many people who’ve been told that ei-ther they have no reason for heart disease, or theyhave a cause that is untreatable. Both statementsare simply untrue.
85
What Does My Heart Scan Show?
Healthy Strategies That Help LowerCholesterol (Total and LDL):
• Raw almonds—Rich in fiber andmonounsaturated fats, a handful (1/4-1/2 cup) of rawalmonds daily lowers cholesterol around 10 percent.Almonds also blunt spikes in blood sugar aftereating and prevent diabetes. They’re tremendouslyfilling, and since almonds take the edge off a sweettooth, are great for sugar addicts who need a snack.
• Soy protein powder—Soy products are a sourceof many fascinating substances, like isoflavones. Butthe protein powder itself (sold in 1 lb. canisters) is atremendous way to reduce cholesterol through soy’stendency to suppress the liver’s production ofcholesterol. Even the FDA, ordinarily charged withreviewing drugs, has endorsed the value of soyprotein powder. Three tablespoons (25 gms) a dayin fruit smoothies, protein shakes, or blended in youryogurt or other foods will lower LDL by around 12percent. Soy protein is also finding its way into avariety of products like low-carb pasta and bread,soy cheese, and soy chips. Just check the label andadd up the protein content, aiming for a total of 25grams of soy protein every day.
• Pectin—Found in apples and the rinds of citrusfruits, pectin is a natural fiber that lowers cholesterol;the same foods also provide flavonoids that yieldbroad health effects. Be extra lazy when you peel
86
Chapter Five
your citrus fruits and leave as much of the white rindon as possible. Pectin is also available as capsules,in which case several grams per day can be used.
• Soluble fibers—Among the best is oat bran.Containing twice the quantity of the healthy fiberbeta-glucan as oatmeal, oat bran is a versatilesource of soluble fiber that can lower cholesterol 10-15 percent while also reducing blood sugar andproviding roughage for bowel health. Starchy beans,like black, pinto, Spanish, red, and kidney, alsoprovide significant soluble fibers that can lower LDL.One-half cup of beans per day can be an easy wayto lower cholesterol. Note that fibers like wheat fiberfound in whole wheat bread and bran cereals donothing for your cholesterol.
• Phytosterols—These soybean oil derivativeslower cholesterol 12-15 percent. Two butter substi-tute products are available on the market containingphytosterols: Take Control and Benecol. Twotablespoons per day is the recommended “dose,”but beware of calories. Minute Maid also producesan orange juice product containing phytosterolscalled Heart Wise. Two glasses (8 oz. each) ofphytosterol-containing orange juice per day lowersLDL cholesterol 12 percent.
87
What Does My Heart Scan Show?
How do you raise HDL? Niacin, or vitaminB3, can significantly raise HDL up to 30 percent.Although it’s a vitamin, hot flushing and other sideeffects make this best taken under medical super-vision. A class of prescription drugs called thefibrates (Lopid™, or gemfibrozil; Tricor™, orfenofibrate) can also raise HDL.
Diet can help a great deal. HDL is very sen-sitive to body weight: gain weight and HDL plum-mets. But a standard low-fat diet does not raiseHDL, and super low-fat diets lower HDL. HDLincreases with losing excess weight. Exerciseraises HDL, and going from a sedentary lifestyleto a moderately active lifestyle (walking thirtyminutes per day five days a week) typically raisestotal HDL two to five points. Most people withlow HDL can raise it about five to ten points witha combination of changes in diet and exercise.Omega-3 fatty acids found in fish oil have a mod-est effect in raising HDL.
Triglycerides
Triglycerides can be a confusing subject.They are not direct causes of coronary plaque. Butthey are a powerful indirect cause.
88
Chapter Five
Low HDL Is Only the Tip of the Iceberg
Low HDL is just the tip of the iceberg.Lurking beneath the surface are several otherclosely related abnormalities that can drive plaquegrowth.
People who have low HDL also commonlyhave a smorgasbord of small LDL particles, hightriglycerides, and abnormal triglyceride-rich lipopro-teins called VLDL (very low density lipoprotein).These abnormalities can occur singly or in variouscombinations.
Low HDL suggests potential for hyperten-sion (high blood pressure), glucose intolerance(“pre-diabetes”), and full-blown diabetes. Thiscombination is often called the Metabolic Syndrome,or Syndrome X. The expression of hypertension anddiabetes are, like HDL, weight-sensitive—the moreoverweight you are, the more likely you’ll developthese patterns.
The lower your HDL below 60 mg/dl, themore likely you are to conceal the entire constella-tion of abnormalities that can occur along with lowHDL. The entire pattern can be assessed with amore extended analysis called lipoprotein testing.(For more information on lipoproteins and how theycan be used to augment your program of prevention,go to www.trackyourplaque.com.)
89
What Does My Heart Scan Show?
Triglycerides are an indirect cause becausethey cause the formation of multiple hidden par-ticles, or lipoproteins, in the blood that can bepotent causes of coronary plaque (especially smallLDL particles and VLDL).
From the standpoint of heart disease, we aremost concerned about triglyceride levels of up to400 mg/dl, as this is the range in which triglycer-ides contribute to growth of coronary plaque.When triglycerides are greater than 400, your doc-tor will need to consider whether other conditionsmight be to blame, such as high blood sugar, un-deractive thyroid, kidney disease, orcertain genetic disorders (e.g., familialhypertriglyceridemia). Levels this high may ormay not contribute to heart disease risk. In therare instances when triglycerides are greater than1000, the pancreas (in your abdomen) can sufferdamage. Levels this high need to be urgently ad-dressed by your doctor.
Triglyceride levels of 100-400 occur com-monly and can contribute significantly to plaquegrowth. What makes triglycerides so evil? Firstof all, triglycerides are present in virtually all hid-den lipoprotein particles to various degrees, suchas VLDL and small LDL. The higher the triglyc-
90
Chapter Five
eride level (up to around 400), the greater the quan-tity of these other particles, all of which are po-tent causes of plaque growth. Only when triglyc-erides are less than 100 do hidden triglyceride-containing particles cease to be a factor. The ATPguidelines target a triglyceride level of less than150 mg/dl.
Replacing carbohydrate calories (from pota-toes, candy, and soft drinks, and flour-containingproducts like breads, bagels, pasta, and cakes) withprotein and healthy fats like the monounsaturatesfrom raw nuts, olive and canola oils, or the omega-3s from fish and flaxseed products, will all helpreduce triglycerides. Avoiding processed foodscontaining high-fructose corn syrup is crucial, asthis ubiquitous additive (in everything from low-fat salad dressings to breads) raises triglyceridessignificantly. Fish oil supplements (but not flax-seed oil) can dramatically lower triglycerides. Pre-scription agents that lower triglycerides includeniacin (doses greater than 500 mg, which shouldbe monitored by your physician), the fibrates likegemfibrozil (Lopid™) and fenofibrate (Tricor™),and the statin agents, especially atorvastatin(Lipitor™) and rosuvastatin (Crestor™).
91
What Does My Heart Scan Show?
Total Cholesterol
Of the four measures on the standard lipidpanel, total cholesterol is the least helpful, as it isa combined measure of LDL, HDL, and triglyc-erides:
Total cholesterol = LDL + HDL + triglycerides/5
This makes total cholesterol a source of con-fusion when there are changes in any of the otherthree measures. For instance, if your LDL goesup and your HDL goes down—both undesirablechanges—you won’t be able to judge this by yourtotal cholesterol because they will cancel eachother out.
The only time total cholesterol might behelpful is when you don’t have the other numbersavailable (e.g., in a cholesterol screening). In thiscase, a total cholesterol score above 200 mg/dl ispotentially concerning and a reason to have thefull lipid panel tested. Unfortunately, many peoplewith total cholesterols in a favorable range (lessthan 200 mg/dl) have been told that they are notat risk for heart disease. The most glaring error inthis advice is that low HDL cholesterol can stilloccur with low total cholesterols.
92
Chapter Five
Your Heart Scan Score—a Reason to Re-think Your Cholesterol
In thinking about your heart’s future, the bestplace to start is with your heart scan score. Thenlook at your cholesterol numbers in light of yourscore. The very same cholesterol numbers in aperson with a heart scan score of zero should beviewed very differently from, say, a person with ascore of 500. These are two different people withvery different risks of heart attack, despite the verysame cholesterol numbers.
Once you’ve had your heart scan, a seriousconversation with your doctor is in order to re-view just what your cholesterol numbers nowmean. Don’t delay! The sooner you begin yourprevention program, the sooner you’ll be on yourway to a life free of heart disease, now armed withthe tremendous insight of your heart scan score.
93
What Does My Heart Scan Show?
Selected References
Calcium scores increase rapidly
Janowitz, WR, Agatston AS, Viamonte M. Compari-son of serial quantitative evaluation of calcifiedcoronary artery plaque by ultrafast computedtomography in persons with and without obstructivecoronary artery disease. Am J Cardiol 1991;68:1-6.
Maher JE, Bielak LF, Raz JA, Sheedy PF, SchwarzRS, Peyser PA. Progression of coronary arterycalcification: a pilot study. Mayo Clin Proc1999;74:347-355.
Budoff MJ, Lane KL, Bakhsheshi H, Mao S,Grassman BO, Friendman BC, Brundage BH. Ratesof progression of coronary calcium by electron beamtomography. Am J Cardiol 2000;86:8-11.
Raggi P, Callister TQ, Lippolis NJ, Russo DJ.Cardiac events in patients with progression ofcoronary calcification on electron beam computedtomography (abstract). Radiology 1999;213:351.
Shah A, Sorochinsky B, Songshou M, Naik TK,Budoff MJ. Cardiac events and progression ofcoronary calcium score using electron beam tomog-raphy (abstract). Circulation 2000;102:II-604.

94
Chapter Five
Relationship of coronary calcium score to lipids
Greenland P, Gaziano JM. Selecting asymptomaticpatients for coronary computed tomography orelectrocardiographic exercise testing. N Engl J Med2003;349:465-73.
Grundy SM. Coronary calcium as a risk factor: rolein global risk assessment: [Comment]. J Am CollCardiol 2001;37:1512-1515.
Grundy SM. Coronary plaque as a replacement forage as a risk factor in global risk assessment. Am JCardiol 2001 Jul 19;88(2A):8E-11E.
Hecht HS, Superko R, Smith LK, McColgan BP.Relation of coronary artery calcium identified byelectron beam tomography to serum lipoproteinlevels and implications for treatment. Am J Cardiol2001;87:406-412.
Wald NJ, Law M, Watt HC, Wu T, Bailey A, JohnsonAM, Craig WY, Ledue TB, Haddow JE.Apolipoproteins and ischaemic heart disease:implications for screening. Lancet 1994;343:75-79.
95
What Does My Heart Scan Show?
What a heart scan meant to…Frank.
At 58, Frank had spent the last 18 years infear of succumbing to heart disease. It all hit himwhen his dad was hospitalized for congestive heartfailure. Frank remembered his dad as an active, vitalman in his late 50s, but saw his health deterioratedramatically as this process unfolded. Witnessinghis dad’s struggle triggered Frank to think seriouslyabout his own health.
Frank started with a conversation with hisdoctor that resulted in a cholesterol panel. Theresults were, in a word, disastrous. Frank remem-bered the initial values well: LDL 218 mg/dl, HDL 34mg/dl, triglycerides 890 mg/dl. Several differentprescription medicines, weight loss of nearly 28pounds, a new exercise program, and counselingfrom a nutritionist all followed. Even then, Frank’scholesterol values, particularly his triglycerides,failed to come under full control. Frank felt doomed.
When his doctor recommended a heartscan, Frank jumped at the idea, though feared theworst. He rationalized that he’d finally get a look atwhat he’d been fearing all those years. His score: abig, fat zero—no detectable plaque whatsoever.Frank was surprised, confused, and elated, all at thesame time. Frank’s doctor, thankfully, was knowl-edgeable about the significance of Frank’s heartscan. He explained to him, “Frank, this is greatnews. Despite your terrible cholesterol numbers
96
Chapter Five
over many years, something has allowed your bodyto not deposit any plaque in your coronaries. Yourheart attack risk is extremely low over the next fiveyears.”
“I don’t get it. If my numbers have been sobad, but no plaque has formed, can’t I just stop allmy treatments and forget about it?”
“I know you’re tempted to do that, Frank. ButI think that, while we don’t have to push your treat-ment program to extremes as we would, say, if yourscore were 500 or 1000, we should still keep you ona health program that keeps your cholesterolnumbers within a reasonable range. But we knowthat we have the luxury of time to do so, and youcan relax knowing that you are unlikely to be in anydanger for a good, long time.” Frank’s doctor alsopointed out that his lipid panel also suggestedpotential for diabetes (low HDL and high triglycer-ides), another reason to maintain a healthy lifestyleand continue treatments.
Heart scans can work both ways. They canshow when coronary plaque is hidden, unsuspected,and far worse than you’d predict from your choles-terol numbers. Or, your heart scan can show thatlittle or no plaque has developed contrary to badcholesterol numbers. Both ways, it can be veryenlightening information in your life.
97
What Does My Heart Scan Show?
Chapter 6Chapter 6Chapter 6Chapter 6Chapter 6When Should I Have Another Scan?
You have your heart scan score. What happensif you just sit back and hope for the best?
If you’ve read the preceding sections, younow know that your heart scan score will increaseat the alarming rate of 30-35 percent per year.Since you’re reading this book, we hope thatyou’re not going to just sit back and do nothing.In fact, we hope that this knowledge spurs you tobegin a new chapter in health to keep your scorefrom increasing.
Let’s say that you have a heart scan at age 45and your score is 200. This concerns you and yourdoctor. The cholesterol numbers that were previ-ously viewed as satisfactory are now viewed in anew light, and your doctor recommends that yourLDL cholesterol of 145 should now be reduced to
98
Chapter Six
100 mg/dl, maybe even 70, your HDL of 38 mg/dl should be increased to at least 45 mg/dl, andyour triglycerides of 199 mg/dl should be reducedto 150 mg/dl. Your doctor recommends a diet lowin saturated fat, replacing refined carbohydrateswith unrefined, using healthy oils like olive andcanola, eliminating soft drinks and processedsnacks, and that you cut back on the beers you’dhave several times a week. You add a walking pro-gram four days a week. Over a year’s effort, youfeel great and you’re proud of the 12 poundsyou’ve lost.
You ask your doctor, “I think I’ve done agreat job of turning my life around. I eat better,exercise, and my cholesterol numbers are whereyou recommended. Has it worked?”
Good question. Just how do you knowwhether your program has worked? Does surviv-ing to your next birthday without heart attackqualify as a satisfactory answer? Is remaining freeof chest pain or other symptoms good enough?
For most people, just feeling good and con-tinuing life tells you nothing about whether yourprevention program has been effective. Yourplaque may have stopped growing, it could haveshrunk, or it could have doubled—you’d feel thesame regardless.
99
What Does My Heart Scan Show?
Does a stress test prove that you’re safe onyour prevention program? Most people understandthat stress tests are flawed measures of heart dis-ease. Just remember former President BillClinton’s story. Stress tests every year for fiveyears failed to identify the unstable, extensivecoronary plaque he had prompting bypass surgery.Stress tests do not effectively uncover nor mea-sure hidden coronary plaque in the great majorityof people. Then how can we expect a stress test todetermine whether your coronary plaque has re-sponded to your treatment program? Stress testsare essentially useless for this purpose.
Then how do you gauge what’s happened toyour coronary plaque?
Easy—just have another heart scan. Thinkabout it and it makes perfect sense. If you startwith a scan that precisely quantifies the amountof plaque concealed in your coronary arteries, whynot measure your coronary plaque again, afteryou’ve engaged in a program to gain control ofyour heart disease risk? It’s as easy as that.
You should consider undergoing a secondscan no sooner than one year after the first. Sinceit takes most people several months to reach theircholesterol goals alone, don’t consider a second
100
Chapter Six
scan until prevention program goals have beenachieved and maintained for a year. This way,you’ll have a score that reflects a full year of ef-fort. You and your doctor will be able to calculateyour percent per year increase or decrease in score.(Many scan centers will calculate this for you,even if the interval between scans is not an exactyear. In this case, you’ll be provided an annual-ized rate of increase or decrease.)
Can’t I Just Assume My Plaque Hasn’t GrownIf I Stick to My Program?
Many people ask: Doesn’t having a “perfect”cholesterol value with treatment (e.g., a statindrug) guarantee that your heart scan score doesn’tincrease? How about a perfect lifestyle—strictadherence to diet, vigorous exercise, etc.?
Unfortunately, with our present knowledge,nothing absolutely guarantees that your scorewon’t increase. However, healthy strategies canindeed slow plaque growth substantially and will,in many, completely halt it, or even shrink plaquein some. But you cannot assume that plaque hasstopped growing just by following your program.Lowering cholesterol, eating healthy, etc. are un-questionably helpful and enhance the likelihood
101
What Does My Heart Scan Show?
of improving your score, but no specific measureguarantees it. (For a more detailed discussion ofstrategies to lower your score, read Track YourPlaque: The only heart disease prevention pro-gram that shows how to use the new heart scansto detect, track and control coronary plaque.Available through Amazon.com, bookstores, orthrough www.trackyourplaque.com.)
The only way to assess results in a specificindividual is to remeasure the quantity of plaquepresent—get another scan. Another scan no soonerthan a full year after your first scan, and afteryou’ve achieved your prevention program goals,will provide you with important feedback on theeffects of your efforts over this time period. De-pending on the results of your repeat scan, youand your doctor can adjust your health programaccordingly.
102
Chapter Six
Jim—the Value of a Second Scan
Jim’s first heart scan was an eye-opener forhim. At 40, Jim knew that his lifestyle was notexactly perfect, but not that bad either. He was 5 feet11 inches tall, weighed 225 pounds, and wore muchof his excess weight around his middle. His initialcholesterol numbers were LDL 153 mg/dl, HDL 35mg/dl, and triglycerides 211 mg/dl—neither terriblenor cause for celebration. Jim’s heart scan scorewas 34 (75th percentile, 3 percent per year risk forheart attack, 30 percent over 10 years), suggestingthat his lifestyle and cholesterol numbers werepermitting more plaque growth than might havebeen predicted simply by looking at LDL, etc.,despite his relatively young age.
This knowledge prompted Jim to follow adiet low in saturated fat, include three times morevegetables and fruits in his diet than before, slashhis intake of cookies, bagels, chips, and otherrefined starches, and—reluctantly—add dailywalking to his schedule.
After this great start, Jim’s motivationflagged over the next two-and-a-half years, espe-cially as work pressures piled up and some homestruggles with a teenager demanded his attention.Hospitalization of a close colleague with a heartattack refocused Jim’s attention on his own health,
103
What Does My Heart Scan Show?
and he decided to review his heart’s status withanother scan. The repeat score: 48, representing a14.8 percent annual rate of increase. Though notperfect (e.g., no change or even a negative rate ofgrowth or plaque shrinkage), it was a good dealbetter than the expected rate of increase of 30-35percent per year.
This news reinvigorated Jim’s motivation toimprove on his program. After a discussion with hisdoctor, Jim was determined to lose an additional 15pounds, raise HDL, increase the dose of fish oil he’dbeen taking to further reduce triglycerides, andaccept an increase in his statin medication. His goalin two years: no plaque growth, no increase in hisscore.
104
Chapter Six
Selected References
Effects of lipid treatment on coronaryplaque and calcium scores
Calllister TQ, Raggi P, Cooil B, Lippolis NJ, RussoDJ. Effect of HMG-CoA reductase inhibitors oncoronary artery disease as assessed by electronbeam computed tomography. N Engl J Med1998;339:1972-1978.
Achenbach S, Ropers D, Pohle K, Leber A, et al.Influence of lipid-lowering therapy on the progres-sion of coronary artery calcification: a prospectiveevaluation. Circulation 2002;106:1077-1082.
Brown BG, Zhao X-Q, Chait A, Fisher LD, CheungMC, Morse JS, Dowdy AA< Marino EK, et al.Simvastatin and niacin, antioxidant vitamins, or thecombination for the prevention of coronary disease.N Engl J Med 2001;345:1582-1592.
105
What Does My Heart Scan Show?
Chapter 7Chapter 7Chapter 7Chapter 7Chapter 7Be a Heart Disease Prevention
Success Story!
Back in 1980, doctors could hazard only acrude guess as to whether someone had hiddenheart disease. Even if you could detect silent heartdisease, there wasn’t much you could do about itshort of major procedures. Our parents and grand-parents really had no choice but to wait for a ca-tastrophe like heart attack to strike to find outwhether they had hidden heart disease.
Thankfully, times have changed. We now livein a new age of heart disease prevention. CT heartscans represent a method of measuring hiddencoronary plaque available to nearly everyone inthe U.S. We can detect the potential for heart at-tack 10 years before it becomes reality. We do sowith ease and precision, without discomfort, inabout 30 seconds.
106
Chapter Seven
Early detection can mean complete elimina-tion or dramatic reduction of risk. If you under-stand precisely how much plaque you have, youcan focus more effectively on a program to gaincontrol of it. You won’t have to rely solely onmurky cholesterol numbers that may or may notcause heart attack. Instead, you can rely on a mea-sure of the disease itself—your heart scan score.
Don’t be satisfied simply with detection ofyour coronary plaque. Don’t let it end there. Toolsto keep plaque from growing and substantiallyreducing risk for heart attack are worlds bettertoday. You require specific answers to the ques-tion, “Why do I have plaque in the first place?”The better you and your doctor understand howyou developed plaque, the more powerful yourprevention program will be in turning off heartattack risk.
And don’t let your heart disease preventionprogram end with you. Pass the word on! Educateyour family and friends. Tell them that heart dis-ease should not be a surprise. Forty percent of thepeople around you will die of heart disease, yetthose people likely have no inkling whatsoever.Measure it, understand it, and control it, with thegoal of complete elimination of danger of heartattack and the need for procedures.

107
What Does My Heart Scan Show?
For more information on how to gain controlover your heart’s future by using heart scans, read TrackYour Plaque: The only heart disease preventionprogram that shows how to use the new heart scans todetect, track and control coronary plaque, available atAmazon.com, BarnesandNoble.com, bookstores, orthrough www.trackyourplaque.com.

109
What Does My Heart Scan Show?
AppendixIncidental Findings on Heart Scans and
What They Mean
Obviously, heart scans are meant to uncoverthe presence of hidden coronary plaque. The scan-ners capable of such detailed imaging of minutecalcified plaque are very powerful machines thatprovide images of many other structures in thechest adjacent to the heart. This means that, alongwith images of your coronaries, a heart scan yieldsloads of information on other hidden processes.
In this section, we list a variety of commonfindings on heart scans that, though they may havenothing to do with coronary plaque and heart at-tack risk, can still have important implications foryour health.
110
Appendix
Enlarged Aorta and Calcium in the Aorta
The aorta is the major artery of the body. Itemerges from the top of the heart and branchesinto all other arteries like the carotid arteries, thearteries to the arms and legs, abdominal organs,etc. Heart scans provide images of the aorta emerg-ing upward from the heart, called the ascendingaorta, and the portion that curves and then headsdownward through the chest towards the abdo-men, called the transverse and descending thoracicaorta. (Because heart scans image the chest only,the abdominal aorta is not imaged. Many centerscan image this for you if you or your doctor de-sire and specifically request it.) Being the firstvessel receiving blood ejected from the heart, theaorta is also the most likely to become enlargedwhen blood is ejected at high pressure. High pres-sure is, of course, measured as high blood pres-sure.
High blood pressure must be present for yearsbefore the aorta becomes enlarged. The normalaorta measures no more than 4.0 cm in an adult(external diameter). Diameters greater than 4.0 cmsuggest that forces to cause it to enlarge have beenat work for several years.
111
What Does My Heart Scan Show?
Other causes of an enlarged aorta are factorsthat weaken the lining of its wall and make plaquegrow, just like the plaque in your coronary arter-ies. Just as plaque in the coronaries is accompa-nied by calcium, so too is plaque in the aorta. Therisk factors that create coronary plaque are there-fore the same ones that create aortic plaque, likehigh LDL cholesterol, low HDL cholesterol,smoking, and diabetes. The calcium in the aortais not generally quantified but is instead describedas mild, moderate, or severe.
Occasionally, the aorta may enlarge due tospecific congenital disorders that weaken thestructural tissues of arteries (e.g., Marfan’s syn-drome).
An enlarged aorta presents two concerningconsequences: development of an aortic aneurysmand stroke. Once the aorta enlarges to a diametergreater than 4.5 cm, it is officially classified as ananeurysm. Surgical replacement is often recom-mended when the aorta reaches 5.5 cm, since thelikelihood of rupture increases dramatically at thisdiameter. Enlarged aortas frequently are lined withatherosclerotic plaque. Like the coronary arteries,where plaque can rupture and cause heart attack,aortic plaque can also rupture. However, becauseof the greater diameter of the aorta, ruptured aor-
112
Appendix
tic plaque does not close off the aorta, but smallfragments of both plaque and any overlying bloodclot that has formed can break off and travel toother parts of the body. Most commonly, thesefragments go to the arteries of the brain and causestroke.
Should your heart scan report mention thatyour aorta is enlarged, discuss this with your doc-tor with the goal of preventing it from getting anylarger, reducing your risk of stroke, and avoidinga major operation. Likewise, if your aorta con-tains calcified plaque, discuss with your doctorhow this finding will impact on your preventionprogram. Many authorities suggest that calcifiedplaque in the aorta be tackled just like calcifiedplaque in coronary arteries and that lipid issuesneed to be intensified to prevent further plaquegrowth and perhaps diminish risk for stroke.
Aortic Valve Calcium
Controlling the flow of blood ejected fromthe heart and into the aorta is an ingenious pieceof natural engineering called the aortic valve. Justlike any valve in the plumbing of our home or car,
113
What Does My Heart Scan Show?
the aortic valve serves a similar function: to al-low the flow of blood in one direction and pre-vent it from flowing backward into the heart.Viewed end-on, the aortic valve looks like a piecut in three pieces. The three slices, or leaflets,are anchored to the aorta, allowing each leaflet toopen and close with each beat of the heart.
Unfortunately, the aortic valve is subject towear and tear, just like brake pads in your car andthe cartilage in your knees. It’s also only recentlybeen appreciated that the same factors that createplaque in your coronaries and aorta can also do soin the aortic valve. As plaque material accumu-lates along the aortic valve leaflets, they becomestiff. Part of the plaque accumulation, wear andtear, and stiffness is calcium deposition, the samerock-like substance that accumulates in your coro-naries.
If your heart scan showed aortic valve cal-cium, this alerts you to the fact that aortic valvedisease may be in your future. (Please note thataortic valve calcium is distinct from aortic cal-cium.) Although calcium in the aortic valve usu-ally develops alongside calcium in the coronar-ies, they occasionally occur independently with-out the other. But just as coronary calcium shouldtrigger a re-evaluation of your prevention program,so too should aortic valve calcium.
114
Appendix
Most of the time, the finding of aortic valvecalcium is described as mild, moderate, or severe.Moderate and severe levels may lead to a needfor echocardiography, an easy, sound-based testthat can more precisely quantify the severity ofvalve dysfunction. Echocardiograms are better atthis since they can assess valve leaflet mobilityand measure velocity of blood flow across thevalve, which can be used to calculate the severityof valve stiffness or dysfunction.
Pericardial Thickeningand Pericardial Fluid
Did you ever wonder how the heart managesto beat 60 times a minute, 24 hours a day, all whilenestled right in between the two lungs, also in-flating and deflating with their own rhythm out ofsync with the beating heart? It does so largely dueto the insulating effect of a tough sac encasing theheart called the pericardium. The pericardial saccontains around 50 cc of a lubricating fluid thatallows the heart to do its work with as little fric-tion as possible.
115
What Does My Heart Scan Show?
Just as the adjacent lungs are prone to infec-tion, particularly with viruses and resulting inpneumonia, so too can viruses infect the pericar-dium. Most of the time, you’re not even aware ofit. Occasionally, pericardial infection with a virusyields sufficient inflammation, or pericarditis, tocause a characteristic sharp pain in the chest. Ofcourse, we are all exposed to numerous virusesthroughout our lives and more than one bout ofpericarditis can occur over your lifetime.
Each bout of pericardial inflammation leavesits scar by causing thickening of the pericardium.After several bouts, some people are left with avisibly thickened (defined as greater than 1 cm inthickness) pericardium. Rarely, a very thickenedpericardium can actually squeeze the heart, dis-rupting its function and resulting in breathless-ness and leg swelling. This is called pericardialconstriction.
Should your pericardium be thickened onyour heart scan, discuss this with your doctor todecide whether your pericardium is thickenedwithout consequence, or whether it could accountfor symptoms and warrants further evaluation.
Sometimes inflammation can also cause ex-cess lubricating fluid, or an effusion, to develop.This can also be uncovered on your heart scan. If
116
Appendix
you’ve recovered from a viral illness within thelast four or so weeks, your effusion might simplybe a consequence of your infection and will likelyand gradually get resorbed. However, if the effu-sion is substantial in size or if there is no recenthistory of a viral infection, further evaluationmight be necessary. At the very least, many phy-sicians will recommend another evaluation to re-assess how much fluid remains after several weeksto see whether the fluid has been resorbed. Rarely,for large or persistent fluid collections, additionalevaluation might be necessary to discover a causesuch as hidden cancers or inflammatory diseaseslike lupus.
Lung Nodules
With the ability to see detail down to a milli-meter, heart scans commonly uncover a myriadof findings in the lungs. Remember that flu youhad last winter? It may have left some streaky linesas a souvenir of the virus infecting your lungs (vi-ral pneumonitis). How about the 20 years of smok-ing before you quit at age 40? That left hundredsof little blank spaces—holes—in your lungs (em-physematous “blebs”), even though your smoker’scough has long since dried up.
117
What Does My Heart Scan Show?
But the finding that is most common, andrepresents a potentially dreaded cancer, is that oflung nodules. As the term suggests, lung nodulesare little pebbles or balls of tissue, generallygreater than 1.0 cm in diameter. A nodule can be aremnant of some long-ago infection, or it can be amalignant tumor that originated in the lung tissueor metastasized there from another source, likethe colon or liver. For radiologists, distinguishingthe two varieties of nodules is a daily exercise,and they will point out that nodules with abun-dant calcium are almost always benign and leftfrom some prior infection. The problem lies withuncalcified or mildly calcified nodules—theycould be benign or malignant. Thankfully, onlyaround 5 percent of all incidentally discoverednodules are malignant.
If your heart scan uncovered one or more lungnodules, it often comes with advice to repeat thelung portion of the scan in several months (usu-ally three to six months) as a means of gaugingwhether it is stable in size (benign) or is growing(malignant). Although this is not a very satisfac-tory approach because it leaves you sweating theissue for the months while you’re waiting for thenext scan, it may spare you from a biopsy. Some-times a repeat scan, but with administration of x-
118
Appendix
ray dye, is advised to provide more detail of thenodule itself, as well as the surrounding lung tis-sue. Other times, consultation with apulmonologist or thoracic surgeon is advised sothat the nodule can be directly studied under amicroscope, i.e, a biopsy is performed. PET scan-ning is also emerging as a helpful tool to charac-terize nodules that is being used in some centers.
Should you have a lung nodule identified onyour heart scan, don’t panic! Discuss the findingwith your doctor to decide the best means to evalu-ate it further. Lung nodules are, unfortunately,quite common and only a small minority trulyprove to be cancerous.


121
What Does My Heart Scan Show?
IndexAabdomen, 110abdominal aneurysm, 79abdominal organs, 110abnormal heart muscle, 66accidents, 10, 49, 82Achenbach, Dr. Stephan, 20Adult Treatment Panel, 78-81, 84, 90aerobics, 47Agatston score. See heart scan score.Agatston, Dr. Arthur, 18age, 19-20, 35-37, 102
relation to percentile rank, 39, 42Albert Einstein College of Medicine, 50almonds, 85Amazon.com, 100American Heart Association, 9-10, 60angioplasty, 79aorta
ascending, 110calcium in the, 110-112
122
Index
enlarged, 110-112thoracic, 110
aortic valve, 112-114apples, 85Arad, Dr., 20arthritis, 58asymptomatic, 9, 29, 66atherosclerosis. See coronary plaque.atherosclerotic plaque. See coronary plaque.atorvastatin. See Lipitor.ATP. See Adult Treatment Panel.
Bbagels, 90, 102beans, 86beer, 98Benecol, 86Beskind, Dr. Daniel, 121beta-glucan, 86Beth Israel Medical Center, 50bile acid binding agents, 83biopsy, 117-118blockage, 28-29, 32, 35, 59, 65, 68
how much do you have, 33-34leg artery, 79
blood clot, 29, 74, 112blood flow to the heart, 15, 32, 58-61, 64-65, 67blood pressure, 20, 45
high, 8, 88, 110systolic, 80
blood sugar, 21, 85high, 89
123
What Does My Heart Scan Show?
body weight, 35, 49-50, 88bookstores, 100brain, 112bran cereals, 86bread, 85-86, 90break pads, 113breast cancer, 55breathlessness, 9, 30, 32, 62, 64-65, 115butter, 86bypass. See coronary bypass.
Ccake, 90calcium. See coronary calcium.calories, 90cancer, 10, 55, 116-118candy, 90canola oil, 90, 98car, 112-113carbohydrates, 90, 98cardiologists, 28, 32cardiology, 28cardiomyopathies, 7carotid arteries, 58carotid artery disease,79cheese, 85chest pain, 9, 13, 28, 30, 59, 64-65, 115chest pressure, 9, 32, 64children, 21cholesterol, 8, 13, 19-20, 28, 35-36, 47-48, 50-53,
71, 75-80, 91, 97-100absorption of, 83
124
Index
change over time, 35-36definition of, 51guidelines, 78-79HDL, 13, 19, 45, 47, 49, 71, 76-77, 80-81,87-88, 91, 95, 98, 102-103, 111heart disease and, 48, 52, 84heart scan score and, 92LDL, 13, 19, 45, 47, 49-50, 52, 71, 75-79,81, 83-86, 91, 95, 97, 102, 111lowering total and LDL, 85-86medication, 77, 95of William Jefferson Clinton, 30raising HDL, 87relation to plaque, 15statistical observations of, 52total, 91VLDL, 88-89
chronic respiratory diseases, 10citrus, 85-86Cleveland Clinic, 16clinical trial, 81Clinton, Chelsea, 30Clinton, Hillary Rodham, 30Clinton, William Jefferson, 30-31, 99colvesevalam. See Welchol.complacency, 10congestive heart failure, 95cookies, 102coronary arteries, 15, 17, 21, 28-30, 32, 59, 74, 76,
111-112lining tissue of, 21-23narrowing, 16
125
What Does My Heart Scan Show?
coronary bypass, 30-32, 47, 55, 63, 66-68, 70, 79,99as preventive procedure, 67-68
coronary calcium, 14, 21, 23, 26in the aorta, 111in the aortic valve, 112-114percent of total plaque, 23score and scoring, 23-24, 37, 42, 66
coronary heart disease. See heart disease.coronary plaque, 8-9, 14-15, 18, 20-21, 35-36,
38-41, 49-51, 56, 59-61, 67-68, 96, 99,105-106, 109, 113active, 68area of, 17density of, 17development of, 19, 28growth of, 9, 74-75, 88-90, 98, 100, 103, 111hard, 25heart catheterization and, 65-66hidden, 32indirect cause of, 87, 89in men vs. women, 19lipid values and, 75-77minor, 29percent calcium, 23regression, 79, 84relation to blockage, 33-34risk based on, 21silent, 64soft, 24stress test and, 63
coronary stents, 14, 32, 55, 63, 66-68, 70, 79as preventive procedure, 67-68
126
Index
c-reactive protein, 52Crestor, 83, 90
Ddiabetes, 10, 20, 49, 79, 88, 111
pre-, 88diaphragm, 60diet, 87, 98, 100, 102
unhealthy, 35, 50driving, 49-50, 82
Eeating. See diet.EBT scanner, 14, 21EKG, 15, 28, 57, 59-60, 114esophagitis, 60esophagus, 60exercise, 58-59, 64, 66, 71, 74, 87, 100ezetimibe. See Zetia.
Ffamilial hypertriglyceridemia, 89family history, 20, 57, 70fat, 90
high-fat meals, 21low-fat diet, 87saturated, 98, 102
fatigue, 62FDA. See Food and Drug Administration.fenofibrate. See Tricor.fiber, 86
127
What Does My Heart Scan Show?
fibrates, 87, 90fibrinogen, 52fish, 90, 103flavonoids, 85-86flaxseed, 90flour, 90flu. See influenza.Food and Drug Administration, 85food. See diet.Framingham study and risk scoring system, 20, 52,80, 82freeway, 49, 82fruit, 102fruit smoothies, 85
Ggallstones, 60gemfibrozil. See Lopid.genetic disorders, 89glucose intolerance, 88golf, 21Guerci, Dr., 20
HHDL. See cholesterol.healthy fats, 90heart
motion of, 17heart attack, 35, 64-66, 98, 102
10-year risk of, 38, 78-80, 82, 105causes, 29, 74
128
Index
cholesterol and, 52EKGs and, 15first symptom, 9high risk of, 78-79intermediate risk of, 81prevention. See prevention.prior, 79risk of, 35, 38-41, 52, 63, 66, 75-80, 82, 96,106, 109
heart catheterization, 14, 29-30, 32, 55, 61, 67reasons for, 65-66, 70will you need, 64-66
heart disease, 55, 64, 82, 84, 89, 91, 95, 99, 106artery narrowing and, 16causes of, 48, 51-52definition of, 7likelihood, 15number one cause of, 48prevention. See prevention.symptoms, 60, 64-65
heart scanas predictor of cardiac events, 50cost of, 16definition of, 16-17follow-up, 97-103, 117incidental findings of, 109-118need for, 82questions following 58-68relation to blockage, 33-34reporting, 38sample images, 14, 22, 71scope of, 57second, 97-103
129
What Does My Heart Scan Show?
speed of, 16value of, 16, 82who should have a, 19-20volumetric, 18
heart scan score, 22, 35, 42, 57-58, 64, 81-82,100, 106age and, 40as measure of disease, 49best, 21cholesterol and, 92definition of, 8doing nothing with your, 73formula, 17-18greater than 100, 40greater than 200, 40greater than 400, 62-63greater than 1000, 40, 77high risk, 79increase of, 75, 97, 100likelihood of abnormal stress test and, 62lipid values and, 76-77red flags, 40reduction of, 81
heartburn, 62Hecht, Dr. Harvey, 50hiatal hernia, 60high blood pressure. See blood pressure.high blood sugar. See blood sugar.high-fructose corn syrup, 90holding your breath, 16-17homocysteine, 52hypertension. See blood pressure.
130
Index
Iinfection, 115-117inflammation, 52, 115inflammatory diseases, 116influenza, 10, 116insulin, 52intestinal tract, 83invasive procedures, 16, 23, 65, 67ischemia, 67isoflavones, 85
Jjogging, 47kidney disease, 89
KKondos, Dr. George, 37
LLDL. See cholesterol.leading causes of death, 10leg arteries, 58leg swelling, 115lifestyle, 77, 79, 87, 96, 100, 102lipid, 75-78, 81, 91, 96, 112. See also cholesterol.
standard panel, 75-76Lipitor, 83, 90lipoprotein, 52, 88-89. See also cholesterol.liver, 85
131
What Does My Heart Scan Show?
Lopid, 87, 90lovastatin. See Mevacorlow-fat diet, 87lung, 114-115
nodules, 116-118lupus, 116
MMassachusetts General Hospital, 20mastectomy, 55men
aged 35, 20aged 40 and older, 19aged 48, 39aged 65, 39percentile rank and calcium scores, 42
metabolic syndrome, 88Mevacor, 83microscope, 118Minute Maid, 86misclassification of risk, 82monounsaturates, 90Mother’s Day, 55motivation, 102-103MRFIT, 52
NNational Cholesterol Education Program, 78National Heart, Lung, and Blood Institute, 80New York, 20, 50New York-Presbyterian Hospital, 30
132
Index
niacin, 87, 90Nissen, Dr. Steve, 16nutrition, 77, 84
to lower cholesterol, 85nutritionist, 95nuts, 90
Ooat bran, 86olive oil, 90, 98omega-3 fatty acids, 87, 90open heart surgery, 14orange juice, 86overweight. See body weight.
Ppasta, 85, 90pectin, 85-86percent of deaths, 10percentile rank of heart scan score, 36-41, 81
calcium scores and, 42heart attack risk and, 38
pericardial fluid, 114-116pericardial thickening, 114-116pericarditis, 115pericardium, 114-116PET scan, 118phytosterols, 86plaque. See coronary plaque.pneumonia, 10potatoes, 90
133
What Does My Heart Scan Show?
Pravachol, 83pre-diabetes, 88prevention 10, 27, 35, 41, 46, 56, 68, 71, 77, 80, 92,
100, 105-107, 112success of, 98-99
processed foods, 90, 98protein, 90
powder, 85shakes, 85
pulmonologist, 118
Rradiologist, 117red flags, 40relative risks, 82revascularization, 63reverse cholesterol transport, 84risk calculators, 80, 82risk factors, 8, 20, 49-50, 53, 79, 84rosuvastatin. See Crestor.rupture, 34-35, 111-112
Ssalad dressing, 90Schwartz, Dr. Allan, 30sedentary, 35, 87September 2004, 30sex, 20, 36simvastatin. See Pravachol.Smith, Dr. Craig, 30smoker’s cough, 116smoking, 20-21, 35, 50, 80, 111, 116
134
Index
soft drinks, 90, 98soluble fibers, 86South Beach Diet, 18soy, 85spine, 14St. Francis Medical Center, 20starches, 102statin agents, 78, 83, 90, 103stents. See coronary stents.stomach, 60stress test, 9, 15-16, 28, 30-33, 45, 58-61, 67, 70,
77, 99abnormal, 65-67definition, 58do you need a, 58-61likelihood of abnormal, 62normal, 61, 63reason for, 65relation to heart scan score, 62usefulness of, 62-63
stroke, 47, 112sudden death, 9sugar addicts, 85surgeons, 32sweet tooth, 85syndrome X, 88
TTake Control, 86tennis, 73thallium imaging, 59, 62thoracic surgeon, 118
135
What Does My Heart Scan Show?
Track Your Plaque, 81, 101, 107, 121-122treadmill, 58-60Tricor, 87, 90triglyceride, 13, 45, 76-77, 87-90, 95-96, 102-103
levels, 89-90tumor, 117
Uunderactive thyroid, 89United States, 11, 48University of Arizona, 121University of Illinois—Chicago, 37University of Miami, 18USA Today, 30
Vvalvular heart disease, 7vegetables, 102virus, 115-116vitamin B3, 87VLDL. See cholesterol.volumetric score, 18
Wwalking, 58, 87, 98, 102watch and wait approach, 9weight loss, 71Welchol, 83wheat fiber, 86women
136
Index
aged 40, 20aged 45 to 50, 7, 19aged 48, 39aged 50, 37aged 65, 39percentile rank and calcium scores, 42
work pressure, 102
Xx-ray dye, 117-118
Yyogurt, 85
ZZetia, 83Zocor, 83


Special offer to readers . . .Take your heart disease prevention program tothe next level!
If you’ve had a heart scan and want to develop themost powerful prevention program available, con-sider reading Track Your Plaque: The only heartdisease prevention program that shows how touse the new heart scans to detect, track andcontrol coronary plaque.
Track Your Plaque helps you understand preciselywhy you have hidden coronary plaque. More impor-tantly, you need to know what to do about it! TrackYour Plaque is a complete guidebook that showsyou how to:
1) Identify the causes of your coronary plaquewith methods that go far beyond simple-mindedcholesterol measures, and
2) Effectively treat the causes and gain controlof your plaque.
“This is the best book I have read for preventing heartdisease disasters. It is well written, comprehensive, andgives you an easy, life-long method to keep your hearthealthy, so you never have to have a heart attack.I read a lot of books on this subject, and this is the best byfar.”
Dr. Daniel BeskindClinical Assistant Professor of Emergency Medicine,
University of Arizona
“Track Your Plaque shatters many of the myths associatedwith heart disease and answers several questions that havebothered me for years: How can you pass a stress test andthen die from a heart attack? How can your cholesterol benormal or ‘under control’ but you can still have a heartattack? Do I have to suffer the same fate as my father?This book is packed with information regarding the earlydetection of heart disease and its hidden causes. This bookwas written for patients, but should be required reading fordoctors.”
Steve B.Waterford, WI
Track Your Plaque is available on Amazon.com andBarnesandNoble.com for $19.95. Track Your Plaqueis also available from the www.trackyourplaque.comwebsite. Please go to the www.trackyourplaque.comwebsite for more information on becoming a memberof the Track Your Plaque program and to find outmore about our interactive counseling programs, ourTrack Your Plaque video seminar, new discussionsfrom world experts, and other exciting contentall devoted to controlling and conqueringcoronary plaque. Become a member and the book,Track Your Plaque, is included at no extra cost!



![[PPT]No Slide Titleadoboli/355/class_9.ppt · Web viewDocument presentation format: On-screen Show Company: UC Berkeley ... Scan-Path Register Scan-based Test —Operation Scan-Path](https://img.pdfslide.us/doc/110x75/5aee5f607f8b9ac62b8bfc34/pptno-slide-adoboli355class9pptweb-viewdocument-presentation-format-on-screen.jpg)