Embed Size (px)
Citation preview
What do we need in order to provide paediatric
palliative care at an intermediate/stepdown care
facility?
Alex Daniels
June 2018
Outline
• Background
• Motivation
• Methodology
• Results
• Evaluation
Background
Impact of life limiting and life threatening conditions on :
• Child - need holistic care
• Caregivers - need to access supportive care
• Health care professionals - require training, mentoring, support
Motivation for study
• NGO (Bigshoes) PPC consultative service - tertiary care
• Community liaison nurse
• DOH - HBC service
• Complex symptom management
• Care of the dying child and family
• Need for respite care
• Gap in service
Opportunities
• CHT - funding
• DOH Western Cape Government - ICPF
• SFCCH -10 bed palliative care unit
Methodology
• Mixed method longitudinal prospective study - 6months
• Multi faceted subject
• Three populations - patients, primary caregivers , health care professionals
• Tools
- Case report form (n=25)
- Primary caregivers questionnaire ( n=25)
- Professional’s demographic sheet (n=15)
- Focus group discussions ( 3)
Patient demographics
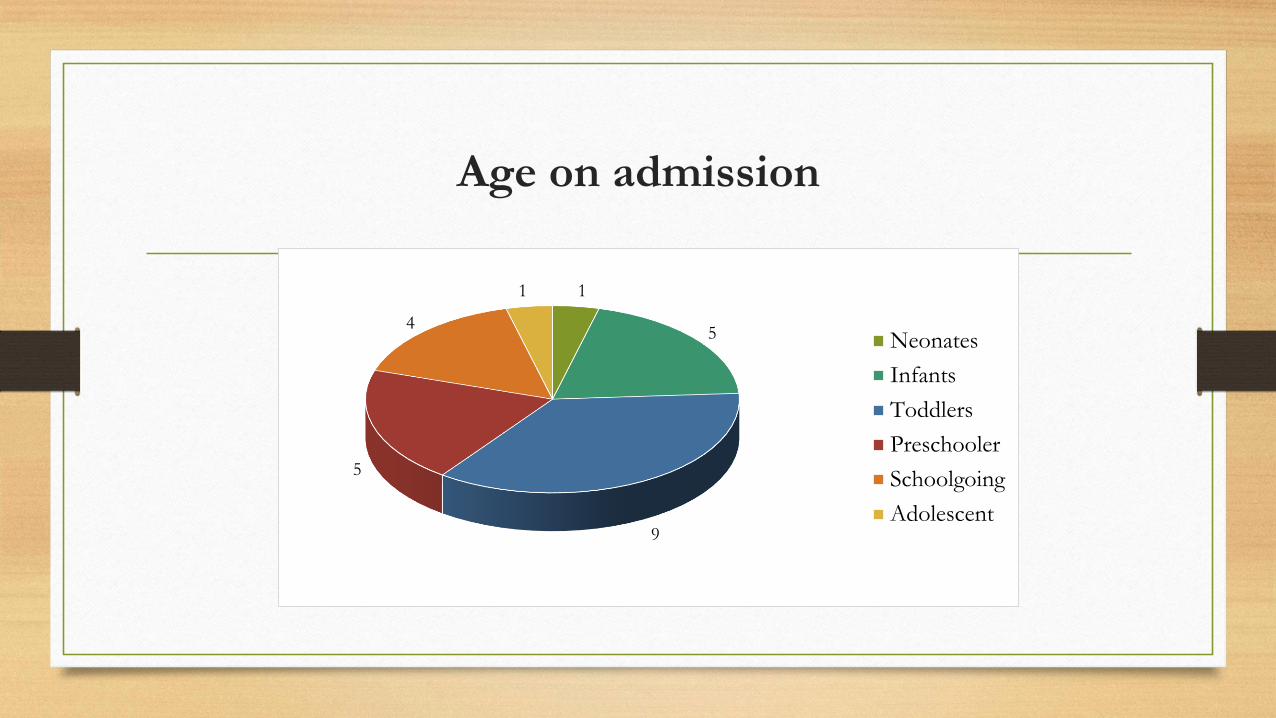
1
5
9
5
4
1
Neonates
Infants
Toddlers
Preschooler
Schoolgoing
Adolescent
Age on admission

Primary diagnosis
0
1
2
3
4
5
6
7
8
9
10
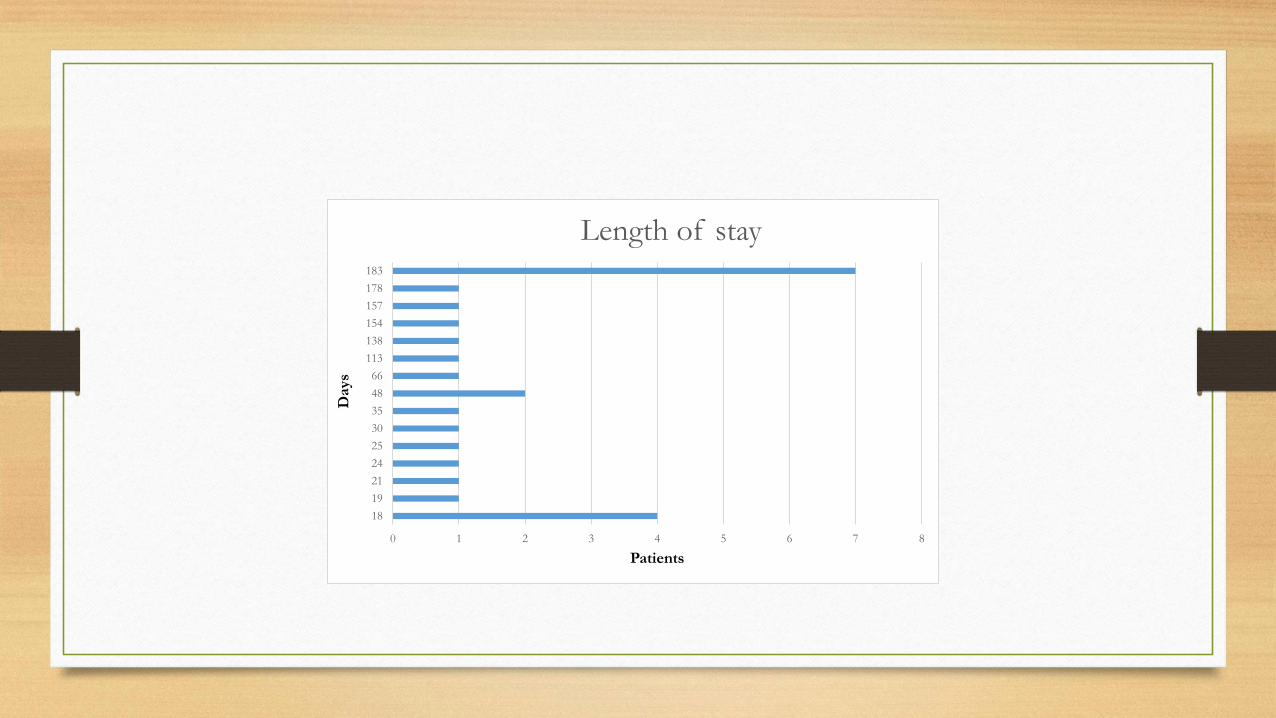
0 1 2 3 4 5 6 7 8
18
19
21
24
25
30
35
48
66
113
138
154
157
178
183
Patients
Days
Length of stay
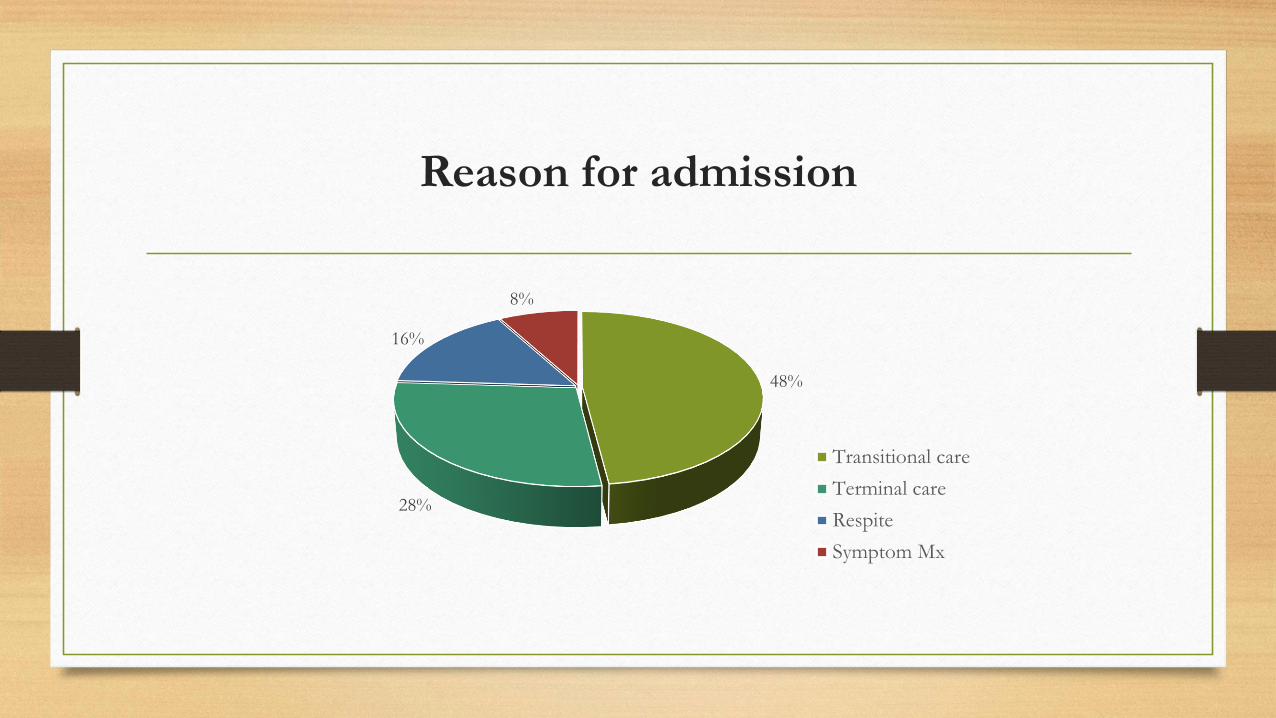
Reason for admission
48%
28%
16%
8%
Transitional care
Terminal care
Respite
Symptom Mx
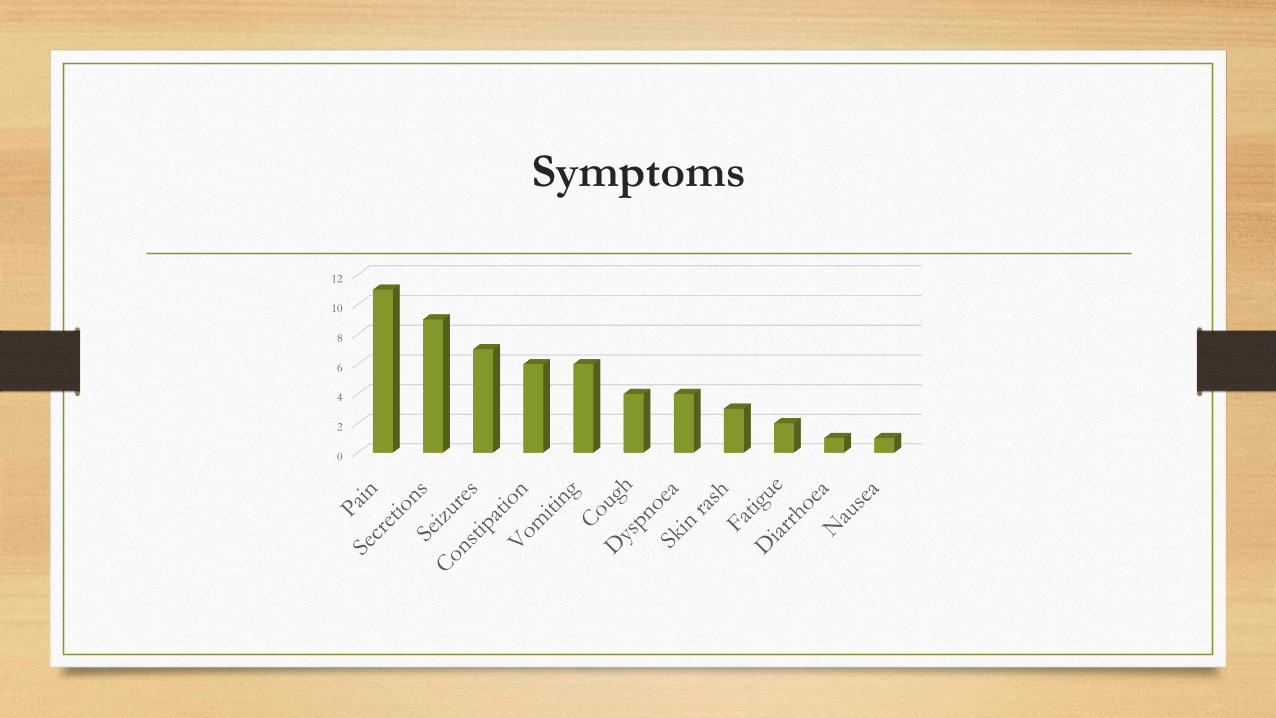
0
2
4
6
8
10
12
Symptoms
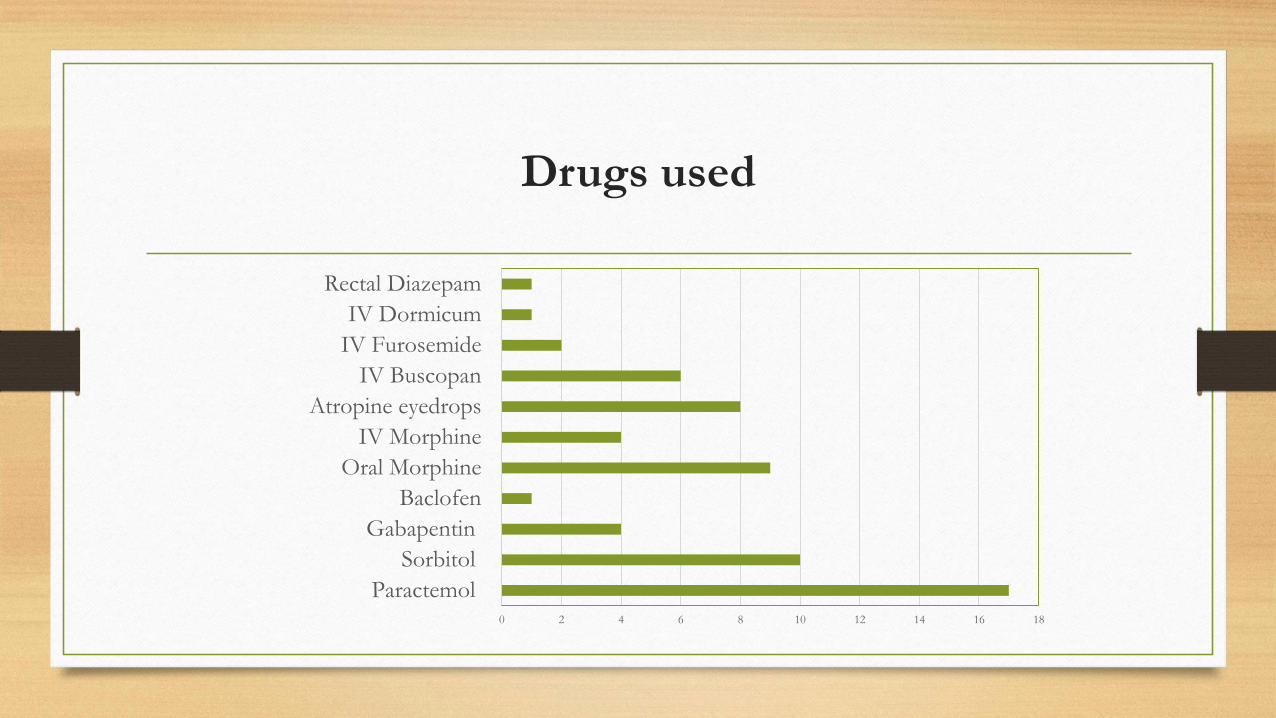
0 2 4 6 8 10 12 14 16 18
Paractemol
Sorbitol
Gabapentin
Baclofen
Oral Morphine
IV Morphine
Atropine eyedrops
IV Buscopan
IV Furosemide
IV Dormicum
Rectal Diazepam
Drugs used
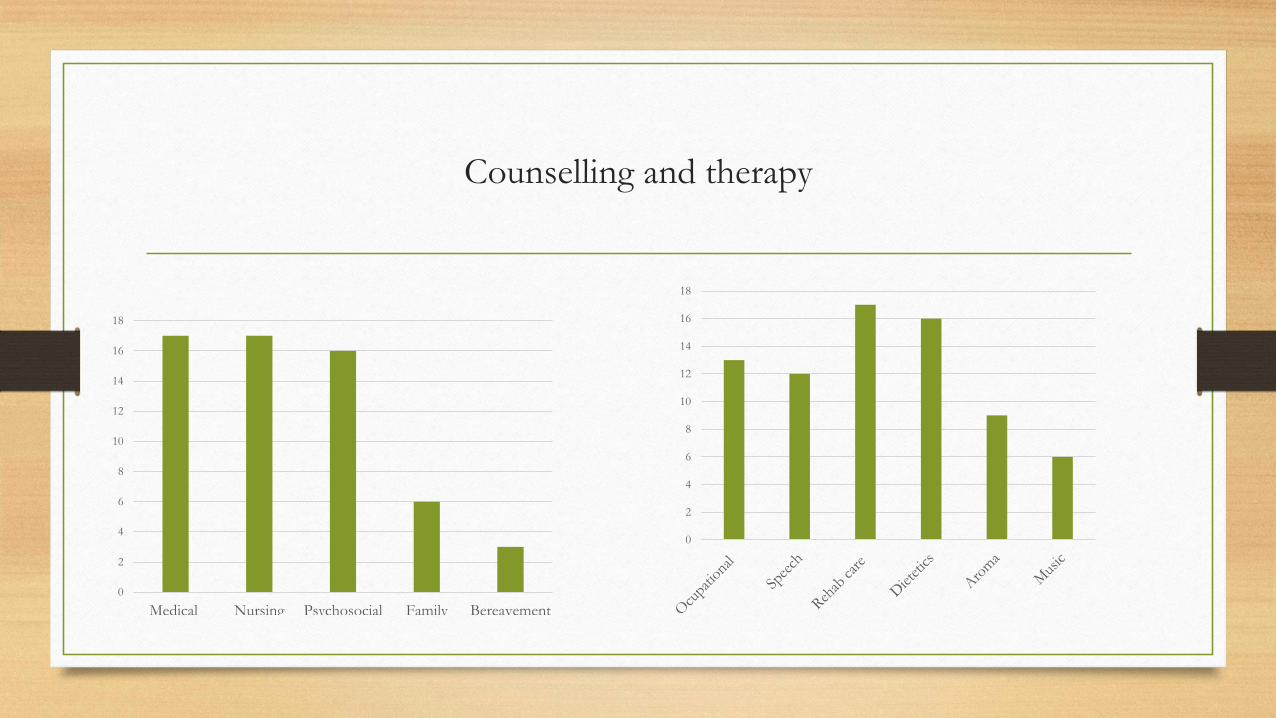
Counselling and therapy
0
2
4
6
8
10
12
14
16
18
Medical Nursing Psychosocial Family Bereavement
0
2
4
6
8
10
12
14
16
18
Primary caregivers
Caring for their child at home
Ten respondents indicated that caring for their child at home was a difficult task
• P06:“It was very difficult, she didn’t sleep at all, always crying she did not want to sleep because of her head, only ‘Panado’ for pain but that did not work, it was difficult to look after her at home”.
• P07:“It was difficult, he needs special attention because of the way he is. There is nothing he can do or say, when you look at him you must decide what he needs or requires, not always easy”.
Health care professionals
On the death of a childP3: “For example when patient XX died, I hated seeing her suffering, when she passed on I was happy cos they in a
better place….also feel somewhat guilty because I feel so relieved that they were not suffering anymore….. different
reactions to different deaths …… I think for anyone working with a child it is a constant struggle…..feeling too much
or too little… you want to be in the middle”.
P15: “Emotionally draining to see children who you learn to love, deteriorate and pass away. They slowly
deteriorate and they don’t pass away I feel , some of the kids they fluctuate, look like they going to die, you say your
goodbyes and you cry, two days later she’s fine, then three weeks later she terminal, she’s fine again cycle
continues…”
P11: “Taxing in a way, I am young, feeling a little worn down emotionally…”
P2: “The debriefing helped us a lot….space to cry and say what you want to say, after that you feel relief in your heart
and can move on”.
Value of team
P4: “Seeing the diff that’s it made with a team approach that includes families and patient, commitment from them (staff) andenthusiasm, hunger and getting to grips with working with the big challenge of working with a PC approach and delivering very good PC….…which is often instinctive or intuitive in people but to see it overtly practised”.
P3: “Will not have coped if I had not been a part of an experienced team”.
P4: “Pro: Strong team in place, mutual respect in that unit, sense I get doesn’t matter who you are, what is your role is, you will be afforded respect for what you doing”.
P1:” Pro: especially recently there is a big team, all this big organism, with the aim to settle the child and to provide support and kind of a container for them …..I can’t be doing this in isolation”.
HCP reflections on service provision
• P6: “It’s kind of sad: I don’t know whether it is the DOH or management is not acknowledging PC…it’s kind of sad not a common practice, it is so rare to find one (PPC IPU) I am feeling sad we do not have much support for that…”
• P15: “Any place has ups and downs, politics get in the way, perhaps there is a lot of reluctance from management to come on board with PC….because whether it is financial burden that PC places on the SF budget or fact that management does not understand PC, seems like a lot of blocking.”
• P14: “People have remained positive there are good staff that have stayed there - it is a difficult place to work. People should be encouraged to practice their passion you can’t keep them in their place. We have accomplished so much despite what has been thrown in front of us, sad for what could have been…..”
Lessons learnt
• Gap in policy
• Importance of buy in from management
• Inadequate staffing ratios
• ALOS - 42days
• Time - nature of intervention
• Drug access
Acknowledgments
• Children and families of SFCCH
• Staff of SFCCH
• Supervisors : Dr Michelle Meiring and Ms Linda Ganca