Embed Size (px)
Citation preview


What can we learn from the Gold Standard?
“No Place Like Home”
Saraswathi Vedam, RM, MSN, FACNM, SciD (hc)
2011

What is the same & what is different?
• Outcomes • Components of Care • Emotional and physical environments • Locus of control • Impact of provider attitudes, social
norms, and common sense • Evidence Based Practice
Why Home Birth? Woman’s Perspective
(Janssen 2009, Janssen 2006, Hildingsson 2003, Davies 1996, Cunningham 1993)
• Control of environment and process of care
– privacy -cultural congruency – comfort and convenience - spiritual – self-determination - empowerment – low intervention - family involvement – safety - relaxed, peaceful
“Although my previous two hospital deliveries were
very positive they did not compare to the delight of
giving birth at home. It was just so right.”
Mother in Davies study, 1996
Why Learn from Home Birth? Health Policy Perspective
(WHO 2000, APHA 2001)
• Low risk care for low risk women – appropriate use of technology – allocation of resources – cost effectiveness
High Quality Data
• Northern Region Perinatal Mortality Survey • Ackerman-Liebrich et al.,1996 • Wiegers, Keirse, et al., 1996 • Meta-analyses, Olsen, 1997, 2000 • Johnsson and Daviss, 2005 • Janssen, 2002, 2003, 2009 • Jonge et al, 2009 • Hutton E et al, 2009
Mortality and Morbidity • Perinatal mortality
– comparable home birth populations - .6-2.5/1000 – U.S. Birth Centers - 1.3/1000 – Uncomplicated hospital births - 1-2.9/1000
• Maternal and fetal outcomes – less medical interventions
(induction,augmentation, episiotomy, operative vaginal birth, and cesarean)
– better Apgar scores, less severe lacerations – findings supported by clinical trials of elements of
care
BC Outcomes Janssen, et al, CMAJ 2009
• Prospective five-year long cohort study – midwife-attended PHB (2802) – physician attended hospital birth group (N=5985)
– midwife attended hospital birth group (N=5984).
• Similar or reduced rates of adverse outcomes with significantly fewer intrapartum interventions
Framework for Optimal Care
• Screening criteria • Basic skills necessary as attendants • Basic equipment • Continuity of care • Strong provider-patient relationship • Timely access to consultation and/or
referral
What is the same?
Framework for Optimal Care
• Screening criteria • Basic skills necessary as attendants • Basic equipment • Continuity of care • Strong provider-patient relationship • Timely access to consultation and/or
referral


Medical Contraindications (1 of 2)
• Rh incompatibility with a rise in titer • Malnutrition, poor weight gain • Smoking cigarettes • Drug or alcohol addiction • Multiple pregnancy • Polyhydramnios or oligohydramnios • Insulin dependent diabetes • Maternal history of small-for-dates babies • Intrauterine growth retardation • Significant maternal anemia at term
Medical Contraindications (2 of 2)
• History of severe postpartum hemorrhage • Pre-eclampsia • Placenta previa • Prematurity • Abnormal presentation • Primary herpes infection in labor • Positive serology for syphilis • Positive surface antigen for Hepatitis B • Positive HIV • True postmaturity • Unexplained antepartum bleeding (especially after first
trimester)
Basic Skills for Attendants
• Neonatal resuscitation • Ability to monitor maternal and fetal
condition, and assess and treat common ob conditions, with low tech methods
• Ability to screen for complications requiring hospitalization and initiate referral
• Ability to manage complications if delivery is imminent or condition prohibits transfer

Framework for Optimal Care
• Screening criteria • Basic skills necessary as attendants • Basic equipment • Continuity of care • Strong provider/patient relationship • Timely access to expert consultation

What is different?
Are the women different? Macdorman & Declercq 2011, Janssen 2009,Pavlova 2009
• Socioeconomic status • Education • Rural vs. Urban • Race • Occupation • Age and parity • Marital status

How Culture interacts with Birth • Family Roles and organization
• The primary support person(s) • Independence and dependence in
children • Food rules, taboos, and customs • Customs related to dress, modesty,
privacy

Cultural Competency & Birth
• Attitudes and customs related to wellness, illness, birth, and death
• Baby and child care • The place of birth • The type of provider • Naming • Communication • Spirituality

The Labour and Birth Environment
• Tools of the trade • The room set up • Privacy • Space, visuals, colour • Sound • The Players

Evidence Based Practice
Enhancing Physiology Leng 2008, Preng 1979; King 2010; Neumann 2008; Lagercrantz 1986
Emerging science and common sense • Mammals and humans • Fetus to newborn transition • Endurance and prowess • Sphincter law • Sex
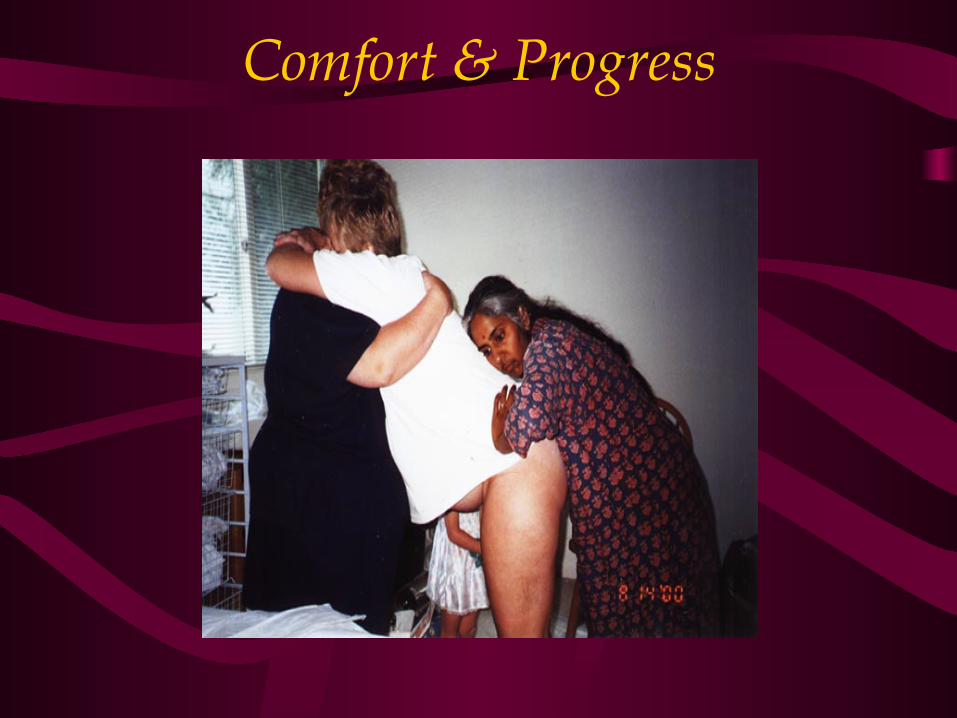
Comfort & Progress
Length of Labor • Friedman:
– Active phase: mean 2.5hrs – 2nd stage: 2.9h in nullips, 50 m multips
• Zhang et. al, 2002: – Active phase: mean 5.5 hrs – 2nd stage: 95%ile = 3h
• Janni et al.: 2nd stage >2h in 20.1% all pts. • O’Connell et al.: 2nd stage > 2h in 48% • Level I, II, and III, Friedman IV • Repeated measures analysis vs plotting 500
individual curves and synthesizing into 1 curve.
Vertical labour Humphrey 1974, Scott 1963, Caldeyro 1960, Mendez-Bauer 1975, Gold 1950, Borel 1957, Russell
1969, Gupta 1991, Lilford 1989, Russell 1982, Gardosi 1989,
• Progress of labour: shorter labour, stronger contractions • Effects of gravity, increased pressure on cervix leading to
dilation • Fewer abnormal fetal heart rate patterns, decreased risk
of aorto-caval compression, 2,3,4 better fetal oxygenation • Stronger and more efficient uterine contractions 5,6 • Improved alignment, rotation, and decent of fetus 7 • Increased anterior-posterior8 and transverse9 diameters
of pelvis in squatting10,11,12 and kneeling12 • Reduced duration of second stage • Reduction in reported pain, episiotomies, augmentation
and assisted deliveries
Eating and drinking in labour
Singata 2010, Maharaj 2009, Beat 2007 • Cochrane review, 5 studies, n=3130: no benefits or
harms from fluids and food in labour, thus no justification for restriction
• Evidence supports fluid intake in labor • Insufficient studies about the relationship between
fasting times and risk of pulmonary aspiration during labor.
• Endurance from caloric intake; compare to athletes
The Nature and Management of Labor Pain
Am J Ob Gyn, 186 (5) suppl, 2002
• Papers presented at invitational symposium sponsored by Maternity Center Association and New York Academy of Medicine
• Evidence-based, rigorous, peer reviewed • Multidisciplinary steering committee:
midwifery, obstetrics, pediatrics, physical therapy, neonatology, nursing, doulas, bioethics, childbirth education, consumer advocacy, epidemiology, public health, anesthesiology.

Promoting Comfort & Progress Carlsson 2009, Simkin 2002 ,Chang 2010
• Homeopathics, herbals • Nutrition • Hydrotherapy • Nipple Stimulation • Clitoral stimulation • Massage therapy • Acupressure/ acupuncture • Sterile water papules • Optimal fetal positioning and
pelvic manipulation • Continuous loving support
Pain and women’s satisfaction • SR of 137 reports of factors influencing women’s
evaluation of birth experience
• Results: – “4 factors –
• personal expectations, • the amount of support from caregivers • the quality of the caregiver-patient relationship, • and involvement in decision making
appear to be so important that they override the influences of age, socioeconomic status, ethnicity, childbirth preparation, the physical birth environment, pain, immobility, medical interventions, and continuity of care, when women evaluate their…experiences,”
Control Cheyney 2008, Dahlen 2011, Robertson 2011, Symon 2010;Moerman 2002
• Impact of autonomy on woman • Impact of autonomy on provider • Collaborative decision making • Power of Placebo • Desire
Relationship Based Care Clinical benefits • receive more appropriate preventative care • have problems recognized • require fewer diagnostic tests and prescriptions • require fewer hospitalizations • visit the emergency department less frequently • be more likely to be more accurately diagnosed • have lower [per-patient] costs of care
Starfield and Mackinko, 2005
Are women less healthy?
Is the CS rate rising because women are?: too old too fat too hooked on technology too lazy too scared too controlling
What about our own fears?
Perceptions of risk: provider or patient? Bryers 2010
XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
Provider attitudes Vedam 2009, Klein 2009, Klein 2010, Dahlen 2011, Finsen 2008
Providers’ attitudes impact care options & influence women’s choices
Providers may present options that are congruent with their own education, experience, and scope of practice
What shapes provider attitudes?
Science? Exposure? Education? Professional culture? Peer pressure? Regulation? Public Opinion? Media?
Acknowledging Complexity Matthias 2011, WHO 2008
There is no way to take the danger out of human relationships.
Barbara Grizzuti Harrison
Planned home birth
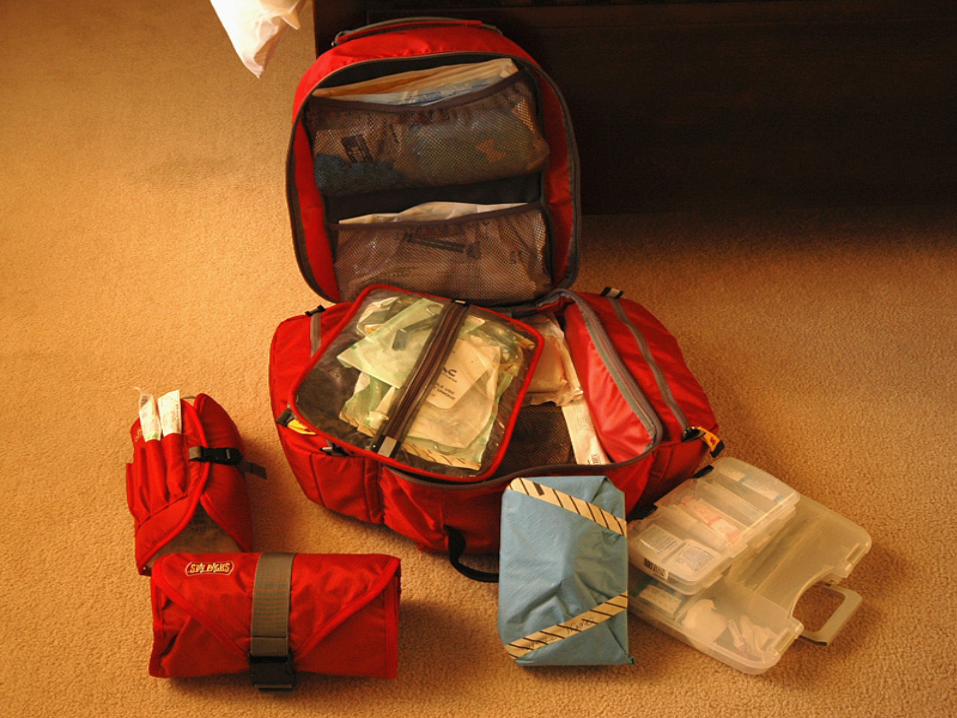
• Anticipatory guidance and preventative care • The Midwife’s Bag of Tricks • Complementary providers • Avoidance of intervention in the absence of
complications • Continuous supportive presence • Collaborative Decision Making • Timely Access to Expert Consultation
Setting the tone
• Trust and communication in home birth practice:
– Shared responsibility for care • Commitment to Time • adequate social support network for the perinatal course • preparation of participants and the birthing environment • open and clear communication with the midwife
– Self-care and physiologic cues – Guest or Host?
• Cultural humility and congruency
What can we learn?
• The physical environment • What does continuous presence mean • Avoidance of intervention in absence of
complications, low tech assessment • Enhancing a conducive emotional state • Understanding healthy physiology • Enlisting the evidence • Consults with experts

RN
RM RM
MD
RM
MD RN
Closing the Theory Practice Gap Vedam 2007, Lange&Kennedy 2006
• Evidence-informed practice • Appropriate use of technology and resources • Education of all providers on physiology • More research needed on factors beyond
mortality and morbidity – effects of birth environment on labour – influences of maternal and provider anxiety – effects of birth experience on long term physical
and psychological well-being