Embed Size (px)
Citation preview
23/06/2014
1
What are the Unmet Needs in the
Management of IBD?
Shane Devlin, MD, FRCPCInflammatory Bowel Disease Group
The University of Calgary
Some Real Cases: #1
• 32 yo male with pan UC.• Grumbling phenotype with 8 BM per day with blood
75% of the time, modestly elevated CRP• Poor quality of life• No clinical or endoscopic response to dose
escalated infliximab, weekly adalimumab and now failing golimumab
Some Real Cases: #2
• 42 yo female with ileal and pan colonic CD• Prior ileo-cecal resection in 2009• Induction and maintenance infliximab in 2010• Developed delayed type hypersensitivity reaction
to infliximab in 2012• Switched to adalimumab with incomplete
response, but recently developed severe psoriaform lesions that are not responding to topical or UV therapy
23/06/2014
2
Some Real Cases: #3
• 78 yo male patient• Multiple comorbidities• Newly diagnosed steroid dependent pan ulcerative
colitis, non responsive to 5-ASA
Anti‐TNF in IBD: A Historical Timeline
1995
1997
2002
1999
20041998IFX
2007
2006ADA
2008Topdown
2009 Sonic 2009 COMMIT
2010Postop
2009EXTEND
Anti‐TNF in IBD: A Historical Timeline
1995
1997
2002
1999
20041998IFX
2007
2006ADA
2008Topdown
2009 Sonic 2009 COMMIT
2010Postop
2009EXTEND
Episodic Combination Therapy
23/06/2014
3
Anti‐TNF in IBD: A Historical Timeline
1995
1997
2002
1999
20041998IFX
2007
2006ADA
2008Topdown
2009 Sonic 2009 COMMIT
2010Postop
2009EXTEND
Maintenance Combination Therapy
Anti‐TNF in IBD: A Historical Timeline
1995
1997
2002
1999
20041998IFX
2007
2006ADA
2008Topdown
2009 Sonic 2009 COMMIT
2010Postop
2009EXTEND
Monotherapy? (esp. Humira)
Anti‐TNF in IBD: A Historical Timeline
1995
1997
2002
1999
20041998IFX
2007
2006ADA
2008Topdown
2009 Sonic 2009 COMMIT
2010Postop
2009EXTEND
HSTCL…Monotherapy?
23/06/2014
4
Anti‐TNF in IBD: A Historical Timeline
1995
1997
2002
1999
20041998IFX
2007
2006ADA
2008Topdown
2009 Sonic 2009 COMMIT
2010Postop
2009EXTEND
Earlier Use
Anti‐TNF in IBD: A Historical Timeline
1995
1997
2002
1999
20041998IFX
2007
2006ADA
2008Topdown
2009 Sonic 2009 COMMIT
2010Postop
2009EXTEND
Combo TherapyMucosal HealingAnti TNF for UC
Anti‐TNF in IBD: A Historical Timeline
2014 and Beyond
‐TDM
‐Golimumab and Adalimumab for UC
1995
1997
2002
1999
20041998IFX
2007
2006ADA
2008Topdown
2009 Sonic 2009 COMMIT
2010Postop
2009EXTEND
Combo TherapyMucosal HealingInfliximab for UC
23/06/2014
5
y
Maximize the Use of Anti‐TNF
Therapy
Yet….We have unmet needs
• IBD is a serious, systemic disease• Primary non-response• Inadequate response• Secondary loss of response due to a variety of
mechanisms• Intolerance due to adverse events• Ongoing steroid use
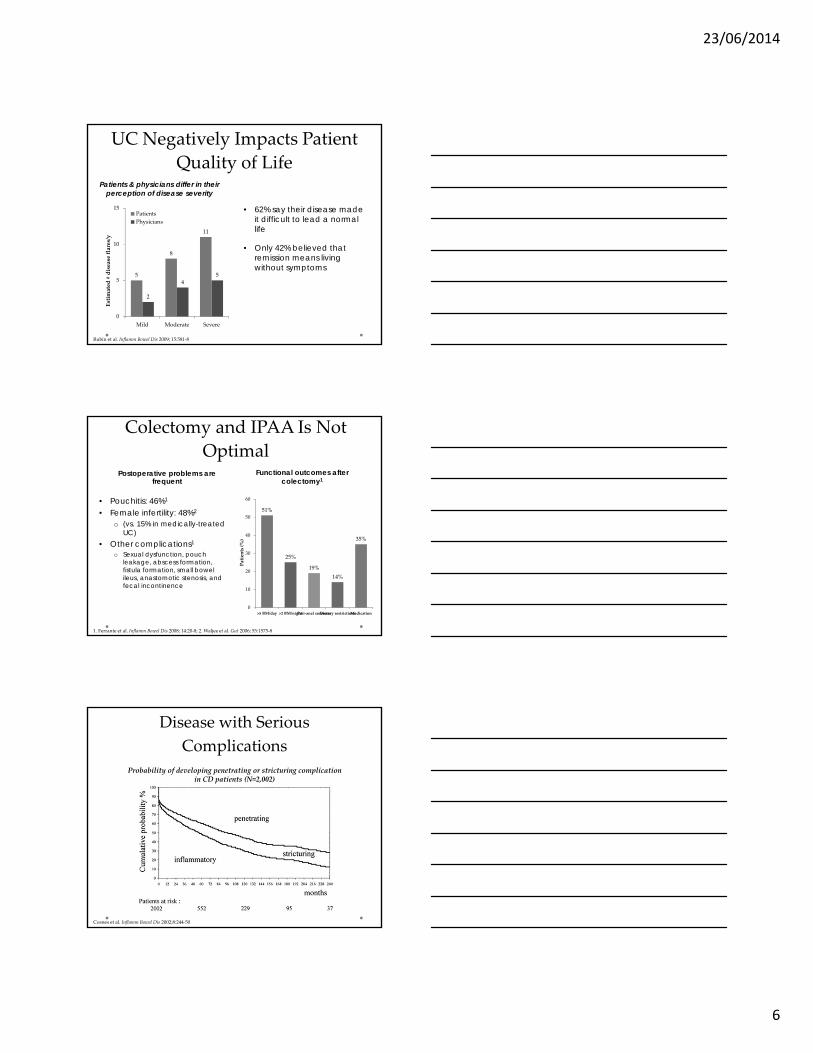
The Requirement for Colectomy in IBD
remains Higher than we’d like
4.9%
11.6%15.6%16.3%
33.3%
46.6%
0
10
20
30
40
50
1‐year 5‐year 10‐year
Colectomy rate
U
C
Colectomy rates in meta‐analysis of 30 population‐based studies
Frolkis et al. Gastroenterology 2013;Online:doi 10.1053/j.gastro.2013.07.041
23/06/2014
6
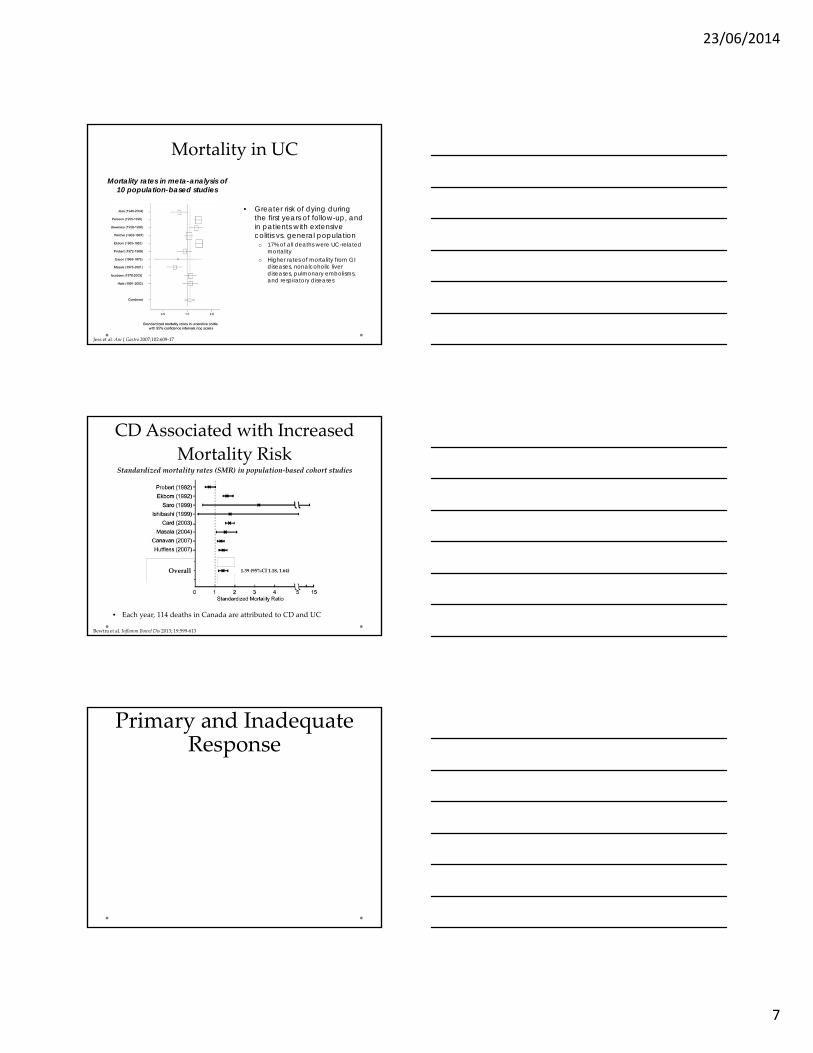
UC Negatively Impacts Patient
Quality of LifePatients & physicians differ in their
perception of disease severity
5
8
11
2
45
0
5
10
15
Mild Moderate Severe
Estimated # disease flares/y
Patients
Physicians
• 62% say their disease made it difficult to lead a normal life
• Only 42% believed that remission means living without symptoms
Rubin et al. Inflamm Bowel Dis 2009; 15:581‐8
Colectomy and IPAA Is Not
OptimalPostoperative problems are
frequent
• Pouchitis: 46%1
• Female infertility: 48%2
o (vs. 15% in medically-treated UC)
• Other complications1
o Sexual dysfunction, pouch leakage, abscess formation, fistula formation, small bowel ileus, anastomotic stenosis, and fecal incontinence
Functional outcomes after colectomy1
1. Ferrante et al. Inflamm Bowel Dis 2008; 14:20‐8; 2. Waljee et al. Gut 2006; 55:1575‐8
51%
25%
19%
14%
35%
0
10
20
30
40
50
60
>5 BM/day >2 BM/nightPeri‐anal sorenessDietary restrictionsMedication
Patients (%)
y
Disease with Serious
Complications
Probability of developing penetrating or stricturing complicationin CD patients (N=2,002)
Cosnes et al. Inflamm Bowel Dis 2002;8:244‐50
23/06/2014
7
Mortality in UC
Mortality rates in meta-analysis of 10 population-based studies
• Greater risk of dying during the first years of follow-up, and in patients with extensive colitis vs. general population
o 17% of all deaths were UC-related mortality
o Higher rates of mortality from GI diseases, nonalcoholic liver diseases, pulmonary embolisms, and respiratory diseases
Jess et al. Am J Gastro 2007;102:609‐17
CD Associated with Increased
Mortality Risk
Overall
Bewtra et al. Inflamm Bowel Dis 2013; 19:599‐613
Standardized mortality rates (SMR) in population‐based cohort studies
• Each year, 114 deaths in Canada are attributed to CD and UC
1.39 (95%CI 1.18, 1.64)
Primary and Inadequate Response
23/06/2014
8
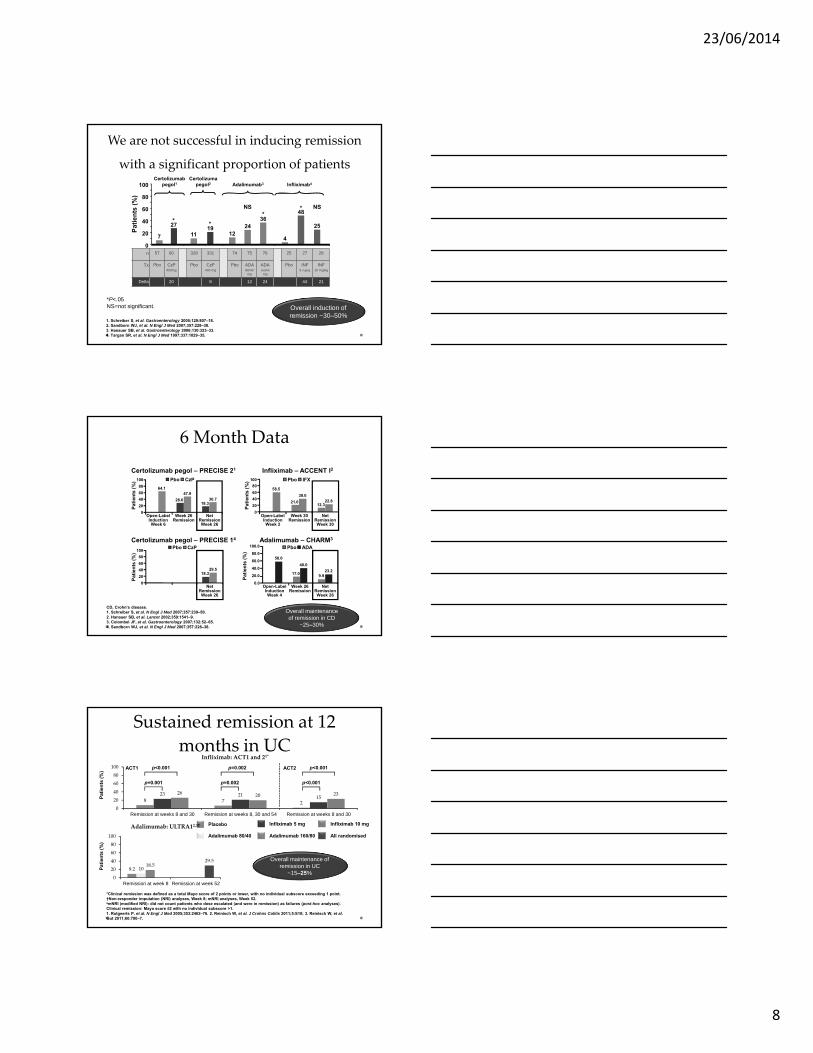
*P<.05NS=not significant.
We are not successful in inducing remission
with a significant proportion of patients
n 57 60 328 331 74 75 76 25 27 28
Tx Pbo CzP400mg
Pbo CzP400 mg
Pbo ADA80/40 mg
ADA160/80
mg
Pbo INF5 mg/kg
INF10 mg/kg
Delta 20 8 12 24 44 21
1. Schreiber S, et al. Gastroenterology 2005;129:807–18.2. Sandborn WJ, et al. N Engl J Med 2007;357:228–38.3. Hanauer SB, et al. Gastroenterology 2006;130:323–33.4. Targan SR, et al. N Engl J Med 1997;337:1029–35.
Overall induction of remission ~30–50%
0
20
40
60
80
100
4
25
* NS48
Certolizumabpegol1
7
27*
11
*19
*NS
1224
36
Pa
tie
nts
(%
)
Certolizumapegol2 Adalimumab3 Infliximab4
6 Month Data
CD, Crohn’s disease.1. Schreiber S, et al. N Engl J Med 2007;357:239–50. 2. Hanauer SB, et al. Lancet 2002;359:1541–9. 3. Colombel JF, et al. Gastroenterology 2007;132:52–65. 4. Sandborn WJ, et al. N Engl J Med 2007;357:228–38.
Overall maintenance of remission in CD
~25–30%
Infliximab – ACCENT I2Certolizumab pegol – PRECISE 21
Adalimumab – CHARM3
28.618.3
64.147.9
30.7
0
20
40
60
80
100
Open-LabelInductionWeek 6
Week 26Remission
NetRemissionWeek 26
Pat
ien
ts (
%) Pbo CzP
21.012.3
58.5
39.022.8
0
20
40
60
80
100
Pat
ien
ts (
%) Pbo IFX
17.0 9.9
58.0
40.0
23.2
0.0
20.0
40.0
60.0
80.0
100.0
Pat
ien
ts (
%)
Pbo ADACertolizumab pegol – PRECISE 14
18.329.5
0
20
40
60
80
100
Pat
ien
ts (
%)
Pbo CzP
Open-LabelInductionWeek 2
Week 30Remission
NetRemissionWeek 30
NetRemissionWeek 26
Open-LabelInductionWeek 4
Week 26Remission
NetRemissionWeek 26
Sustained remission at 12
months in UC
8 7 2
23 21 1526 20 23
0
20
40
60
80
100
Remission at weeks 8 and 30 Remission at weeks 8, 30 and 54 Remission at weeks 8 and 30
Infliximab: ACT1 and 21*
Placebo Infliximab 5 mg Infliximab 10 mg
ACT1 ACT2
p=0.001
p<0.001
Pat
ien
ts (
%)
p=0.002
p=0.002
p<0.001
p<0.001
9.2 1018.5
29.5
0
20
40
60
80
100
Remission at week 8 Remission at week 52
Adalimumab: ULTRA12,3†
*Clinical remission was defined as a total Mayo score of 2 points or lower, with no individual subscore exceeding 1 point.†Non-responder imputation (NRI) analyses, Week 8; mNRI analyses, Week 52.amNRI (modified NRI): did not count patients who dose escalated (and were in remission) as failures (post-hoc analyses). Clinical remission: Mayo score ≤2 with no individual subscore >1.1. Rutgeerts P, et al. N Engl J Med 2005;353:2462–76. 2. Reinisch W, et al. J Crohns Colitis 2011;5:S10; 3. Reinisch W, et al. Gut 2011;60:780–7.
Adalimumab 80/40 Adalimumab 160/80
Overall maintenance of remission in UC
~15–25%
All randomised
Pat
ien
ts (
%)
23/06/2014
9
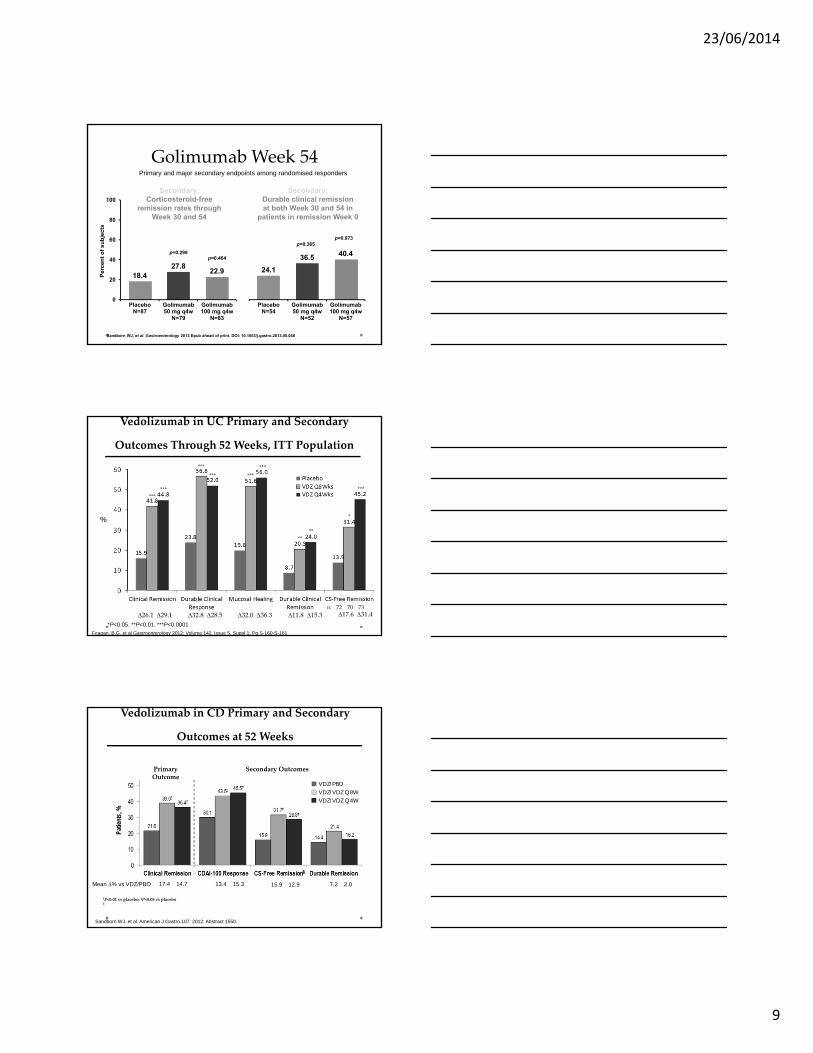
Sandborn WJ, et al. Gastroenterology 2013 Epub ahead of print. DOI: 10.1053/j.gastro.2013.05.048
24.1
36.5 40.4
PlaceboN=54
Golimumab50 mg q4w
N=52
Golimumab100 mg q4w
N=57
18.427.8
22.9
PlaceboN=87
Golimumab50 mg q4w
N=79
Golimumab100 mg q4w
N=83
0
20
40
60
80
100
Per
cen
t o
f su
bje
cts
Secondary:Durable clinical remissionat both Week 30 and 54 in
patients in remission Week 0
Secondary:Corticosteroid-free
remission rates through Week 30 and 54
p=0.073p=0.365
p=0.299p=0.464
GolimumabWeek 54Primary and major secondary endpoints among randomised responders
Vedolizumab in UC Primary and Secondary
Outcomes Through 52 Weeks, ITT Population
%
26.1 29.1 32.8 28.5 32.0 36.3 11.8 15.3 17.6 31.4
******
**
**
***
*** ***
***
*
***
*P<0.05. **P<0.01. ***P<0.0001
n: 72 70 73
Feagan, B.G. et al Gastroenterology 2012; Volume 142, Issue 5, Suppl 1, Pg S-160-S-161
Vedolizumab in CD Primary and Secondary
Outcomes at 52 Weeks
Patie
nts,
%
17.4 14.7 13.4 15.3 7.2 2.015.9 12.9
Primary Outcome
Secondary Outcomes
§
†P<0.01 vs placebo; ‡P<0.05 vs placebo§
Mean % vs VDZ/PBO
VDZ/PBOVDZ/VDZ Q8WVDZ/VDZ Q4W
Sandborn WJ. et al. American J Gastro.107: 2012: Abstract 1550.
23/06/2014
10
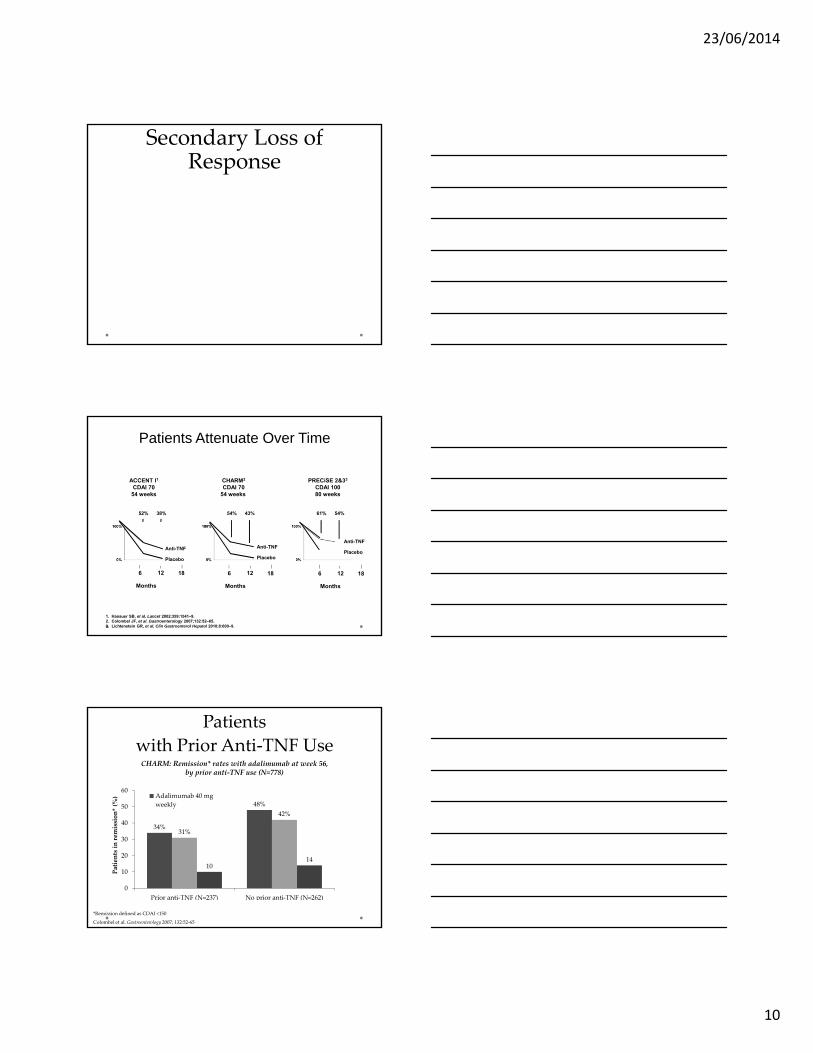
Secondary Loss of Response
1. Hanauer SB, et al. Lancet 2002;359:1541–9.2. Colombel JF, et al. Gastroenterology 2007;132:52–65.3. Lichtenstein GR, et al. Clin Gastroenterol Hepatol 2010;8:600–9.
Patients Attenuate Over Time
ACCENT I1
CDAI 7054 weeks
CHARM2
CDAI 7054 weeks
PRECiSE 2&33
CDAI 10080 weeks
6 12 18
Months
6 12 18
Months
6 12 18
Months
52% 38% 54% 43% 61% 54%
Anti-TNF
Placebo
Anti-TNF
Placebo
Anti-TNF
Placebo
Patients
with Prior Anti‐TNF Use
34%
48%
31%
42%
1014
0
10
20
30
40
50
60
Prior anti‐TNF (N=237) No prior anti‐TNF (N=262)
Patients in remission* (%) Adalimumab 40 mg
weekly
CHARM: Remission* rates with adalimumab at week 56, by prior anti‐TNF use (N=778)
Colombel et al. Gastroenterology 2007; 132:52‐65
*Remission defined as CDAI <150
23/06/2014
11
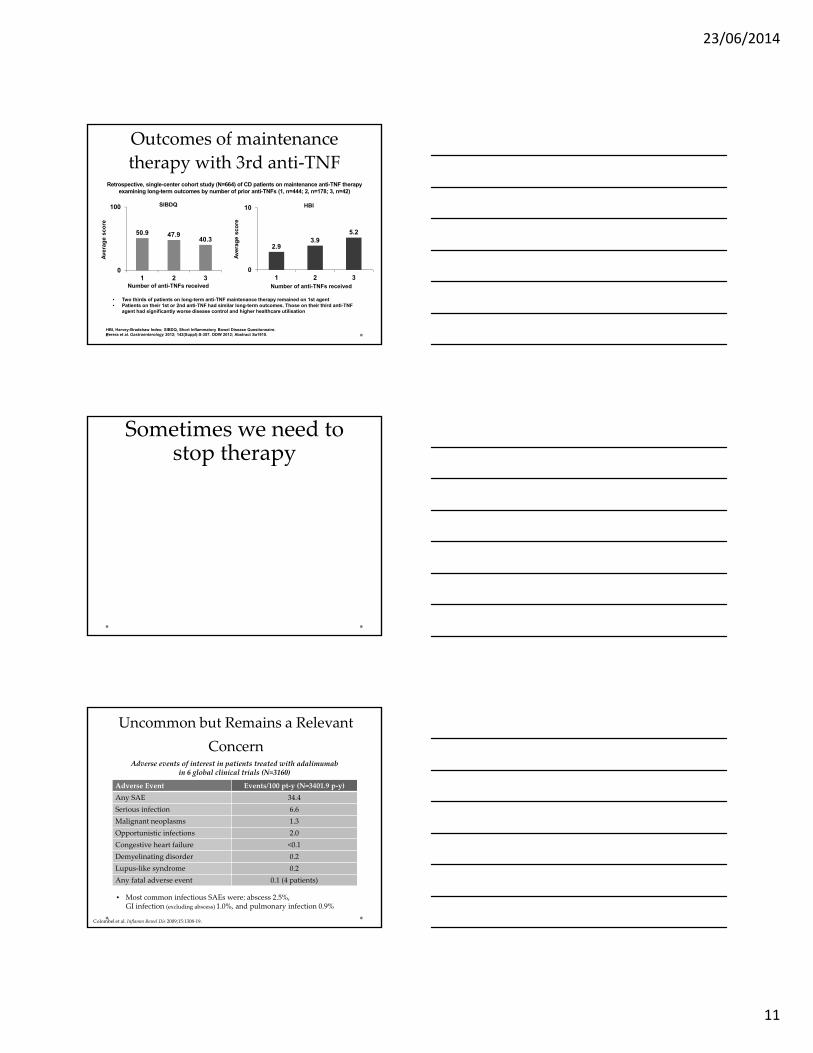
Outcomes of maintenance
therapy with 3rd anti‐TNFRetrospective, single-center cohort study (N=664) of CD patients on maintenance anti-TNF therapy
examining long-term outcomes by number of prior anti-TNFs (1, n=444; 2, n=178; 3, n=42)
• Two thirds of patients on long-term anti-TNF maintenance therapy remained on 1st agent • Patients on their 1st or 2nd anti-TNF had similar long-term outcomes. Those on their third anti-TNF
agent had significantly worse disease control and higher healthcare utilisation
HBI, Harvey-Bradshaw Index; SIBDQ, Short Inflammatory Bowel Disease Questionnaire.Perera et al. Gastroenterology 2012; 142(Suppl):S-357. DDW 2012; Abstract Sa1910.
Ave
rag
e sc
ore
SIBDQ HBI
Number of anti-TNFs receivedNumber of anti-TNFs received
Ave
rag
e sc
ore
2.93.9
5.2
0
10
1 2 3
50.9 47.940.3
0
100
1 2 3
Sometimes we need to stop therapy
y y
Uncommon but Remains a Relevant
Concern
Adverse Event Events/100 pt‐y (N=3401.9 p‐y)
Any SAE 34.4
Serious infection 6.6
Malignant neoplasms 1.3
Opportunistic infections 2.0
Congestive heart failure <0.1
Demyelinating disorder 0.2
Lupus‐like syndrome 0.2
Any fatal adverse event 0.1 (4 patients)
Colombel et al. Inflamm Bowel Dis 2009;15:1308‐19.
Adverse events of interest in patients treated with adalimumab in 6 global clinical trials (N=3160)
• Most common infectious SAEs were: abscess 2.5%, GI infection (excluding abscess) 1.0%, and pulmonary infection 0.9%
23/06/2014
12
Infection and TNF Antagonists
• TREAT registry n > 6,000, f/u > 5yrs
• Factors independently associated with serious infections (Descending order of risk) : • Disease activity mod‐severe (HR = 2.24, 95% CI = 1.57, 3.19; P < 0.001),
• Narcotic analgesic treatment (HR = 1.98, 95% CI = 1.44, 2.73; P < 0.001)
• Prednisone therapy (HR = 1.57, 95% CI = 1.17, 2.10; P = 0.002)
• Infliximab treatment (HR = 1.43, 95% CI = 1.11, 1.84; P =
0.006).
Lichtenstein GR. Am J Gastroenterol. 2012 Sep;107(9):1409‐22.
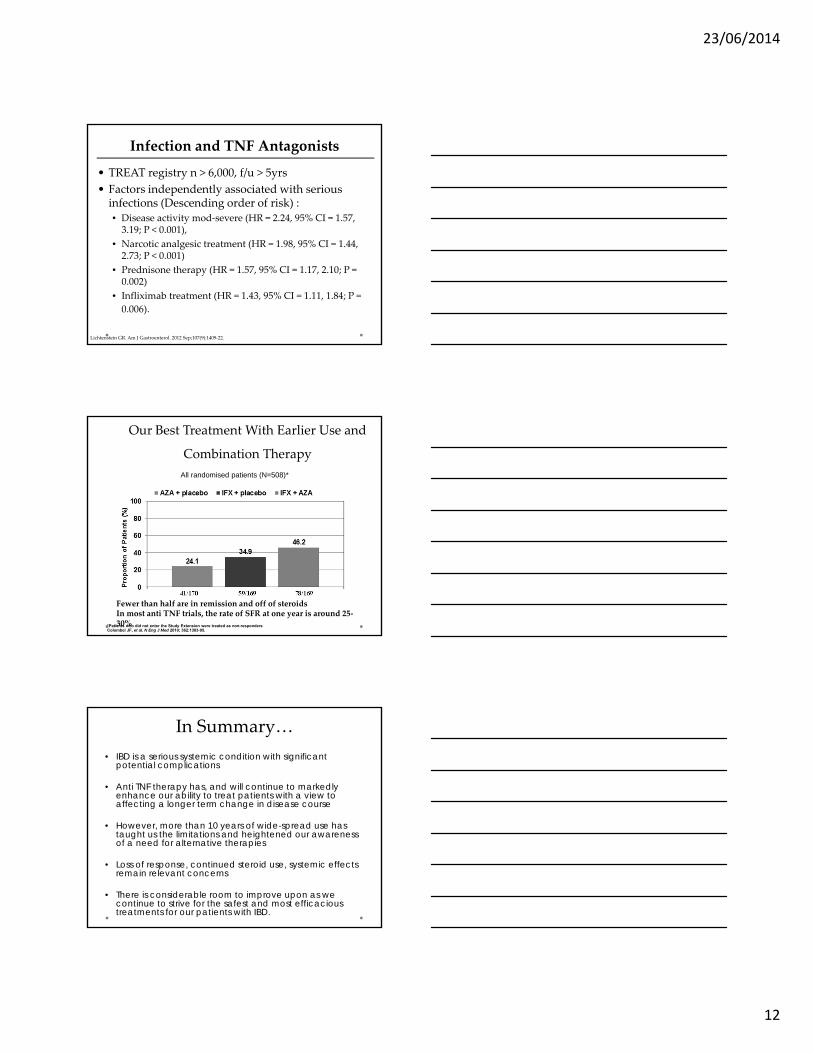
Our Best Treatment With Earlier Use and
Combination Therapy
All randomised patients (N=508)*
p<0.001
p=0.028 p=0.035
41/170 59/169 78/169
*Patients who did not enter the Study Extension were treated as non-respondersColombel JF, et al. N Eng J Med 2010; 362:1383-95.
Fewer than half are in remission and off of steroidsIn most anti TNF trials, the rate of SFR at one year is around 25‐30%
In Summary…
• IBD is a serious systemic condition with significant potential complications
• Anti TNF therapy has, and will continue to markedly enhance our ability to treat patients with a view to affecting a longer term change in disease course
• However, more than 10 years of wide-spread use has taught us the limitations and heightened our awareness of a need for alternative therapies
• Loss of response, continued steroid use, systemic effects remain relevant concerns
• There is considerable room to improve upon as we continue to strive for the safest and most efficacious treatments for our patients with IBD.