Embed Size (px)
Citation preview
Western Node Collaborative
RIVERVIEW HOSPITAL
Medication Reconciliation ProjectPhase One: Admitting
June 19, 2006
Zaheen Rhemtulla B.Sc. (pharm)
Riverview Hospital (RVH)
As part of British Columbia Mental Health and Addiction Services and governed under the Provincial Health Services Authority, Riverview Hospital provides specialized tertiary mental health services under 3 core programs:
- Adult Tertiary Psychiatric Program (225 inpatient beds + 20 ICU beds)specialized tertiary acute care and rehabilitation services to adults living with a serious mental illness
- Geriatric Psychiatric Program (145 inpatient beds)assessment and treatment services for inpatients as well as outpatient consultation services to patients who often have needs relating to end-stage dementing illness with severe chronic psychiatric and medical conditions
- Neuropsychiatry Program (49 inpatient beds)care to a specialized group of individuals who have cognitive, affective, and psychotic symptoms associated with brain injuries or disease that are beyond the capacity of acute care hospitals and community-based settings
Background Information
Recognizing that Medication Reconciliation is an evidence-based intervention that can prevent a high percentage of medication-related adverse events, Riverview Hospital first convened a MedRec team June 2005 in response to the Safer Healthcare Now Campaign and accreditation requirements.
Having supportive executive sponsorship and leadership buy-in,
the project now has a committed team of over 15 members from various disciplines including physicians, nurse clinicians, unit managers, pharmacists, and administrative staff as well as a new funded project leader. The team meet on a monthly basis to discuss the progress of the project which is being piloted on 5 wards throughout the hospital.
Goal for completion for the admission part of the medication
reconciliation process is October 2006.
Project Charter
Based on studies documenting the high percentage
of adverse events occurring in hospitals due to medication errors, particularly at points of transition, Riverview Hospital is focused on providing the best possible care to the patients it serves by developing and implementing procedures and systems that result in better documentation and eliminate unintentional medication discrepancies at these interfaces of care.
Importance
Efficient transitions in care Better documentation Better communication Better safety Fewer hospitalizations Decreased costs Better patient care
Reason to adopt
To provide the best possible care to a very vulnerable patient population (e.g. pt’s with psychosis/Dementia)
Create standardization with all other health-care providers in order to provide “seamless care”.
Aims
Reduce the mean number of undocumented intentional discrepancies at admission by 90% from baseline by October 2006 on the 5 pilot wards (2 geriatric wards, 2 adult tertiary care wards, 1 ICU)
Reduce the mean number of undocumented unintentional discrepancies at admission by 90% from baseline by October 2006 on the 5 pilot wards
Increase the medication reconciliation rate (success index) by 90% from baseline by October 2006 on the 5 pilot wards
Provide a process to identify high risk patients (> 5 medications, co-existing medical conditions, potentially toxic medications) that may need additional collateral to achieve the Best Possible Medication History (BPMH)
Where are we in the process?
Collecting baseline data on 5 pilot wards (2 geriatric assessment wards, 2 adult tertiary care wards, ICU). This has already resulted in better documentation and decreased the number of undocumented intentional discrepancies
Starting with the Sunnybrook Hospital Admission Form and testing on a one-patient-one-physician basis, we are trialing the third draft of our own form
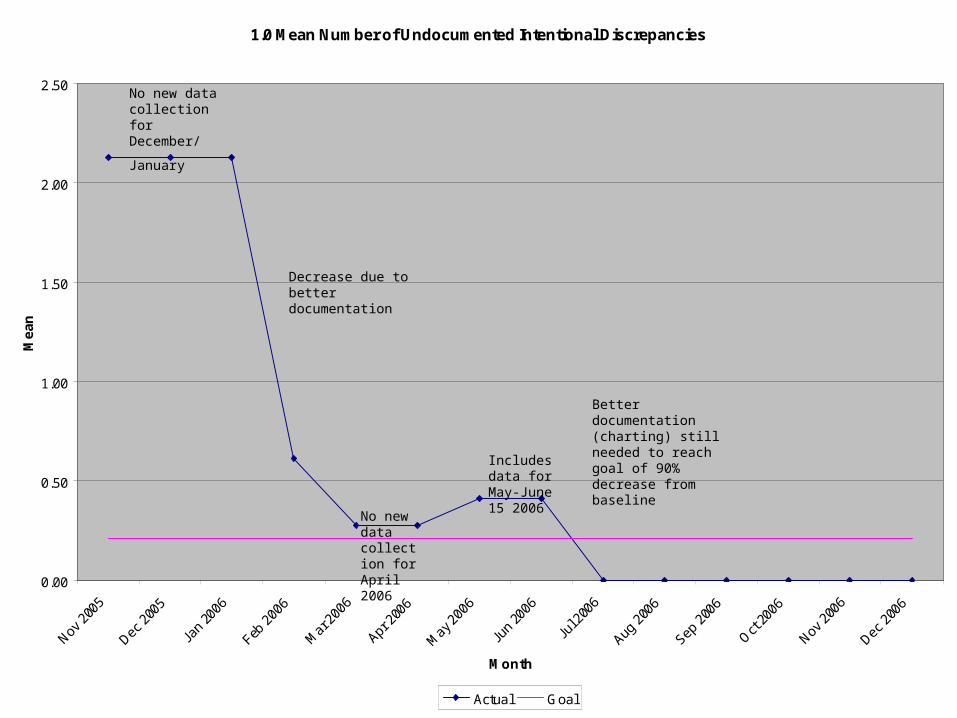
1.0 Mean Number of Undocumented Intentional Discrepancies
0.00
0.50
1.00
1.50
2.00
2.50
Month
Me
an
Actual Goal
No new data collection for December/
January
No new data collection for April 2006
Decrease due to better documentation
Includes data for May-June 15 2006
Better documentation (charting) still needed to reach goal of 90% decrease from baseline
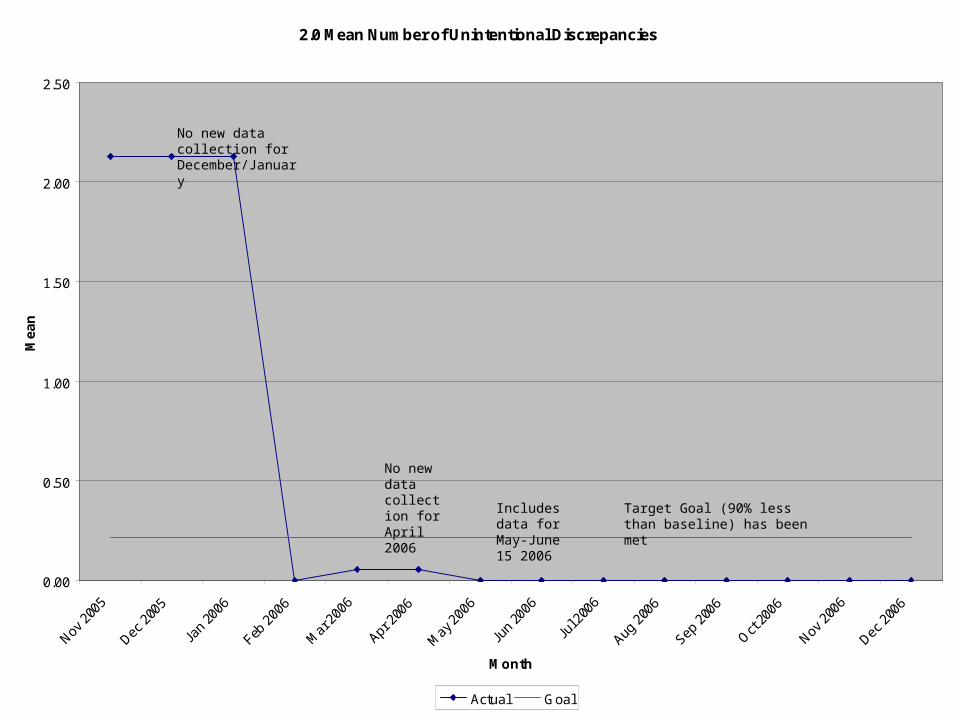
2.0 Mean Number of Unintentional Discrepancies
0.00
0.50
1.00
1.50
2.00
2.50
Month
Me
an
Actual Goal
No new data collection for December/January
No new data collection for April 2006
Includes data for May-June 15 2006
Target Goal (90% less than baseline) has been met
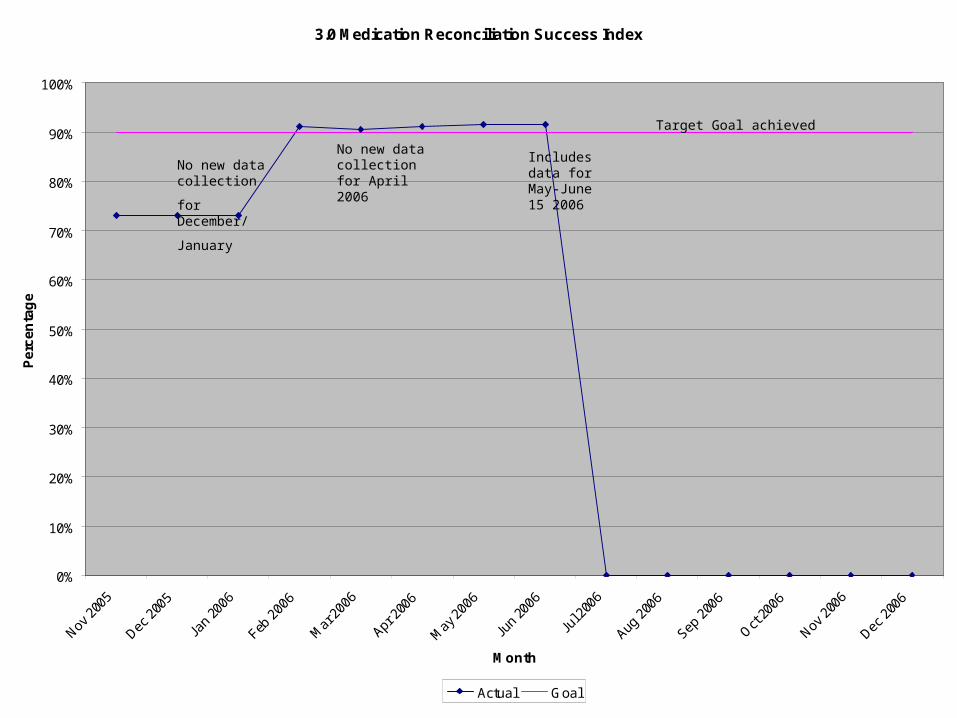
3.0 Medication Reconciliation Success Index
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Month
Pe
rce
nta
ge
Actual Goal
No new data collection
for December/
January
No new data collection for April 2006
Includes data for May-June 15 2006
Target Goal achieved
Keys to Success and Lessons Learned
Successes: Leadership buy-in, team commitment, funding for project leader, funding for event attendance
Barriers: Time constraints, individual preferences of methods for documentation, established ward admission procedures, varying needs on individual wards
Lessons Learned: Do as many; Plan, Do, Study, Act (PDSA) cycles as possible to work out “wrinkles”
Next Steps
Design a flowchart to capture “high need” patients requiring more collateral for BPMH
Do more PDSA cycles to fine tune Admissions Form Trial form, to determine if it is universal for all
patients admitted to RVH. Educate staff how to use to utilize form Implement form on all wards Collect data to see results
Medication Reconciliation Team Contact Information
Riverview Hospital2601 Lougeed Highway
Coquitlam, BC(604) 524-7000
Project Leader: Zaheen Rhemtulla [email protected] Leadership: Marilyn Macdougall [email protected] Francis Hu [email protected] Management: Peter Owen [email protected]
Clinical Support: Jane Dumontet Pharm.D. [email protected] Dr. Heather Cherneski [email protected] Dr. Meagan O’Keefe [email protected]
Riola Crawford [email protected] Ancill [email protected] Bushell [email protected] Sanassy [email protected]
Program Support: Ruby Virani [email protected] Tin Au [email protected] Eggen [email protected] Edwards [email protected]
Forensic Representatives Ellen Haworth [email protected] Wharton [email protected]