-
8/3/2019 Wesley C. Chang et al- In Vivo Use of a Nanoknife for
Axon Microsurgery
1/10
IN VIVO USE OF A NANOKNIFE FORAXON MICROSURGERY
OBJECTIVE: Microfabricated devices with nanoscale features have
been proposed asnew microinstrumentation for cellular and
subcellular surgical procedures, but theireffectiveness in vivo has
yet to be demonstrated. In this study, we examined the in vivouse
of 10 to 100 m-long nanoknives with cutting edges of 20 nm in
radius of curva-ture during peripheral nerve surgery.
METHODS: Peripheral nerves from anesthetized mice were isolated
on a rudimentarymicroplatform with stimulation microelectrodes, and
the nanoknives were positionedby a standard micromanipulator. The
surgical field was viewed through a researchmicroscope system with
brightfield and fluorescence capabilities.
RESULTS: Using this assembly, the nanoknife effectively made
small, 50 to 100 m-long incisions in nerve tissue in vivo. This
microfabricated device was also robust enough
to make repeated incisions to progressively pare down the nerve
as documented visu-ally and by the accompanying incremental
diminution of evoked motor responsesrecorded from target muscle.
Furthermore, this nanoknife also enabled the surgeon toperform
procedures at an unprecedented small scale such as the cutting and
isolationof a small segment from a single constituent axon in a
peripheral nerve in vivo. Lastly,the nanoknife material (silicon
nitride) did not elicit any acute neurotoxicity as evi-denced by
the robust growth of axons and neurons on this material in
vitro.
CONCLUSION:Together, these demonstrations support the concept
that microdevicesdeployed in a neurosurgical environment in vivo
can enable novel procedures at anunprecedented small scale. These
devices are potentially the vanguard of a new fam-ily of microscale
instrumentation that can extend surgical procedures down to the
cel-lular scale and beyond.
KEY WORDS: Axon, Microelectromechanical systems,
Microfabrication, Microsurgery, Nanoknife,Nanoneurosurgery,
Nanotechnology, Subcellular surgery
Neurosurgery 61:683692, 2007 DOI:
10.1227/01.NEU.0000280070.51586.9F www.neurosurgery-online.com
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER2007 | 683
NEW INSTRUMENTATION
Wesley C. Chang, Ph.D.
Departments of Ophthalmologyand Physiology,Neuroscience
Program
and Bioengineering Program,University of California, San
Francisco,San Francisco, California
Elizabeth A. Hawkes, M.S.
Departments of Ophthalmologyand Physiology,Neuroscience
Program
and Bioengineering Program,University of California, San
Francisco,
San Francisco, California
Michel Kliot, M.D.
School of Medicine andDepartment of Neurological Surgery,
University of Washington,Seattle, Washington,and Puget Sound
Veterans
Administration Health Care Center,Seattle, Washington
David W. Sretavan, M.D., Ph.D.
Departments of Ophthalmologyand Physiology,Neuroscience
Programand Bioengineering Program,
University of California, San Francisco,San Francisco,
California
Reprint requests:
Wesley C. Chang, Ph.D.,Departments of Ophthalmologyand
Physiology,
Neuroscience Programand Bioengineering Program,University of
California, San Francisco,
10 Koret Way, K-110,San Francisco, CA 94143.Email:
[email protected]
Received, December 4, 2006.
Accepted, May 17, 2007.
Although axons play a critical role inrelaying information
within the nerv-ous system, there is currently no thera-
peutic intervention that can directly repairthese key neural
processes when severed ordamaged by trauma. Substantial
researchefforts are underway to identify effective ther-apeutic
strategies. Such approaches include
the suppression of growth-inhibitory mole-cules associated with
myelin and scar tissues(8, 18, 19), the harnessing of axon
guidancemolecules that are up-regulated after trauma(8, 12), and
even the application of novel bio-engineered tissue scaffolds to
guide new axonoutgrowth (7). All of these efforts share thegoal of
stimulating the regeneration of injured
adult axons. Recently, we proposed an alterna-tive paradigm in
which transected nerves aredirectly repaired by surgically
reconnectingthe constituent axons to acutely reconstitutenerve
function after damage. To demonstratethe feasibility of this
concept, our researcheffort has presented early demonstrations
ofseveral simple microfabricated devices that
cut, electrostatically translocate, and splicetogether
individual axons in vitro (20).An important aspect of this
microdevice-
based method of axon repair is the effective-ness of such
small-scale instrumentation insurgical environments in vivo.
Current uses ofmicrotechnology in surgical instrumentationinclude
microscale motors, force-generating
-
8/3/2019 Wesley C. Chang et al- In Vivo Use of a Nanoknife for
Axon Microsurgery
2/10
actuators, and catheter-mounted structures for
microsurgicaltissue cutting, ophthalmic procedures, vascular
surgeries, andtargeted drug delivery (1517). However, to operate on
individ-ual cells or on subcellular elements such as axons, new
surgi-cal microdevices are required with characteristic dimensions
atthe micron scale. An important challenge will be to develop
themeans to effectively deploy and manipulate these tiny
devices
in a surgical setting. For instance, surgical microdevices
willhave to be mechanically strong and robust for use in vivo,
andit will be necessary to precisely position and manipulate
thesedevices at scales much smaller than those possible with
manu-ally operated tools. Such devices and capabilities will
allowthe surgeon to perform novel microscale procedures that
arecurrently not possible with existing surgical
instrumentation.
In this study, we have investigated these issues by testing
anaxon nanoknife (6, 20) that can be manipulated as a microde-vice
in a surgical setting. This nanoknife consists of a thin layerof
silicon nitride with a nanometer sharp cutting edge. In thecurrent
demonstration, nanoknives were used to performperipheral nerve
surgery in an anesthetized mouse. By usingthe nanoknife mounted on
a micromanipulator in conjunction
with a simple, custom-assembled microplatform to hold andisolate
an individual nerve, it was possible to precisely manip-ulate this
surgical microdevice in the operating field and tomake targeted,
effective cuts in the sciatic nerve while simulta-neously
monitoring the entire process visually. Furthermore,progressive
cuts to the nerve resulted in an accompanying,incremental reduction
in the evoked electromyography (EMG)signal. Finally, this
custom-assembled surgical suite also
enabled the first targeted cut-ting of a single axon in
ananesthetized animal.
MATERIALS ANDMETHODS
Animals
The surgical demonstrationwas performed on adult femaleC57BL/6
mice or transgenic GFPmice (Charles River Laboratories,Inc.,
Wilmington, MA) anes-thetized with a mixture of keta-mine and
xylazine (14). Thesedated animal was placed in aprone position with
its hind legsfully extended. To expose the sci-atic nerve, an
incision was madethrough the skin of the posteriorthigh and
underlying hamstring
muscles. The sciatic nerve splitsinto several major branches
(Fig.1A), the tibial and peroneal nerves,as well as a smaller
branch. Cut-ting by the nanoknife was per-formed on the central
largest
branch (Fig. 1A, arrow), whichinnervates the calf muscles and
which we have identified as the tibial
branch of the sciatic nerve. To access the axons within the
nerve, theensheathing epineurium and perineurium were gently
removedthrough standard microdissection with handheld surgical
forceps whileviewing under a dissection microscope.
Surgical Microplatforms
The isolation and stabilization of the nerve was performed using
aspecial fixture mechanically isolated from the animal (Fig. 1B).
Thisfixture was held and positioned over the animal by a
micromanipula-tor and presented two separate flat platforms (Fig.
1C) for holding thenerve, one for stimulation (Fig. 1C, small
arrow) and the other for nerveor axon cutting (Fig. 1C, arrowhead).
These platforms consisted of twoelongated, rectangular chips of
Pyrex glass (2 mm wide 0.5 mm thick
8 mm long; Corning, Corning, NY) that were arranged in
paralleland held level at a position just a few millimeters above
the hind limbof the animal. During the surgery, the segment of the
sciatic nerve,with axons exposed, was lifted from the leg and
draped over these twoplatforms (Fig. 1, CD). Along one edge of the
proximal platform, a 500m-wide line of gold film was deposited to
provide a conductor fornerve stimulation. This gold trace was
electrically connected to a volt-age pulse generator and delivered
electrical signals to the nerve. Theopposing pole was grounded to
an Ag/AgCl2 electrode placed undera medial flap of skin on the
leg.
The second, more distal platform, dedicated specifically for
nerveand axon cutting, was separated from the stimulating platform
by agap of 2 mm. This separation provided an isolated surface for
themicrocutting of the nerve and also prevented unintended
feed-throughof the electrical stimulation signals generated at the
first platform so thesevered distal segment of nerve on the second
platform could notreceive unintended stimulation.
684 | VOLUME 61 | NUMBER 4 | OCTOBER2007
www.neurosurgery-online.com
CHANG ET AL.
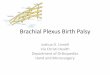
FIGURE 1. A custom surgical suite was assembled to enable
cutting with nanoknives while allowing visual moni-toring through
an overhead microscope. This suite also included the capability for
stimulation of the target nerve andrecording of the resulting EMG.
A, a wide view of the unmounted nerve (arrow) showing its anatomic
position inthe posterior calf along with the target soleus muscle
(asterisk). EMG was recorded from the soleus muscle at a posi-tion
indicated by the asterisk. B, the surgical field showing the tibial
branch of the sciatic nerve (arrow) mountedon the glass
microplatforms. The green board supporting the microplatforms and
facil itating the electrical connection
for stimulation is 2 1.5 cm. C, close-up of the surgical
microplatforms (2-mm wide each) showing the embeddednerve
stimulation electrode (arrow) and the nerve/axon cutting platform
(arrowhead). The nerve is shown drapedon the surgical
microplatforms, which are mechanically isolated from the animal. D,
schematic diagram showing thesurgical field and supporting
equipment, including the stimulation and recording instrumentation
for nerve stimu-lation combined with electromyographic recording
from the soleus muscle. The overhead microscopes objective lensis
positioned just above the nerve straddling the microplatforms.
A
C
B D
-
8/3/2019 Wesley C. Chang et al- In Vivo Use of a Nanoknife for
Axon Microsurgery
3/10
During surgery, the nerve was kept moist by regular irrigation
withphysiologically buffered media. However, it was necessary to
keep the
buffered media within the boundaries of each platform because
themedia itself can serve as a conduit for unintended feed-through
ofelectrical signals.
Electrical Stimulation
The stimulation signal was a single monophasic, rectangular
pulsewith 200-s duration and of varying amplitudes ranging from 100
mVto 2 V delivered at 5 Hz.
Observation
All surgical procedures were monitored in real time using
anupright, boom-mounted microscope (Nikon Erect Image
TrinocularTilting Head and Nosepiece with objective lenses mounted
on SMS 20Diagnostics boom stand and with brightfield and
fluorescence capabil-ities; Nikon Instruments, Garden City, NY),
and surgical manipula-tions were performed directly under long
working distance objectivelenses. Brightfield illumination was
provided from above at obliqueangles to the microscopes optical
axis, whereas fluorescence imagingwas enabled by an on-board
mercury lamp along with appropriate fil-ters. With these
provisions, it was possible to distinguish individual
axons in the mounted nerve. The operating field could be
vieweddirectly by an observer through the microscope eyepieces or
the imagecould be diverted to a mounted digital camera and then
displayed andrecorded on a computer.
Cutting With the Nanoknife
For microcutting of the isolated nerves, a nanoknife
previouslydeveloped for the cutting of individual axons in vitro
was used (6). Thepyramid-shaped nanoknife was fabricated by
conformal molding ofchemical vapor-deposited silicon nitride over
silicon etched preciselyalong specific crystal planes, resulting in
an ultrasharp cutting edge atthe apex (20 nm edge radius of
curvature as determined by scanningelectron microscopy), small
enough to target individual axons. Thisdevice has been used in
vitro to cut both axons from cultured neuronsand from harvested
adult nerves (6). For the surgical procedures in the
present study, the knife was mounted on a supporting rod and
thenpositioned by a commercially available, precision
micromanipulator(MP-285; Sutter Instruments, Novato, CA), which
allowed the nano-knife to be precisely aimed at one or a few axons
at a time. Surgicaldemonstrations were also performed in transgenic
mice expressinggreen fluorescent protein (GFP). Retention of the
cytoplasmically dis-solved GFP after cutting was used to determine
whether or not the sev-ered ends of the axons resealed after
cutting. This analysis of resealingafter single axon cutting has
been previously reported (6).
Evoked EMG Response
To record the evoked EMG signals triggered by nerve stimulation,
asharp tungsten needle was inserted into the calf soleus muscle.
Theopposite pole was grounded at the same Ag/AgCl2 probe used
withthe stimulating circuit. Signals generated at the tungsten
probe werefed to an AC amplifier (DAM-80; World Precision
Instruments Inc.,Sarasota, FL) and amplified 1000 times. The
amplified signals were inturn read and recorded by an oscilloscope
(TEK 3012B; Tektronix,Beaverton, OR).
For EMG recordings, the amplitude of tibial nerve stimulation
wasfirst varied to find the approximate threshold, below which no
actionpotential and, therefore, no EMG signal could be detected.
Nerve stim-ulation was then elicited using a stimulus fourfold
stronger than the
identified threshold. To capture and display accurate EMG
signals, wesubtracted the background stimulation artifacts, which
were measured
by recording from the muscle in an actual surgical configuration
butwith the sciatic nerve completely severed between the platform
and themuscle while still draped over the platform. (EMGs with this
back-ground subtraction are displayed in all figures.) Although
this proce-dure eliminated signal artifacts substantially, some
remnant of signal
feed-through remained owing to slight variations in the
artifactsbetween recordings.
Evaluation of Biocompatibility
To investigate any potential acute toxicity of silicon nitride,
bothmouse hippocampal neurons and retinal explants were cultured
onflat substrates coated with the same chemical vapor-deposited
siliconnitride used to construct the nanoknives. Briefly,
hippocampal cellswere harvested from the brains of E16 mouse
embryos and plated onsubstrates that were preabsorbed with
poly-L-lysine using standardprotocols (5). Mouse retinal explants
from E14 embryos were plated onlaminin-coated substrates, again
using published protocols (3, 21). Bothcultures were maintained in
37C and 5% CO2/95% air in their respec-tive nutrient media along
with appropriate supplements.
RESULTS
Test Microdevice
The test microdevice is a microscale cutting instrument
withnanoscale features that was originally designed for the
precisesevering of axons under well-controlled research conditions
invitro (6). This pyramid-shaped microdevice consists of
amechanically strong, 1 m-thick shell of silicon nitride (Fig.
2A)and was mounted onto a thin metal rod attached to a
glassmicropipette holder (Fig. 2B). The pipette holder was, in
turn,mounted to a robotic X-Y-Z micromanipulator to move
themicrodevice into position and to deliver the cutting
stroke.Because the nanoknife was used for targeted cutting of
singleaxons in a peripheral nerve, the precise movement provided
bya micromanipulator was necessary. In the current assembly forthis
surgical demonstration, it was possible to station
onemicromanipulator system exclusively to hold the microplat-form
supporting the nerve and then station another microma-nipulator on
the opposite side of the surgical field to presentand manipulate
the nanoknife for nerve cutting. Knife posi-tioning with the
micromanipulator and nerve (or axon) cut-ting using the
microplatform as a cutting board was easy toperform and could be
observed through the microscope.
Deployment in the Surgical Field
The placement of the nerve on the microplatform allowedthe nerve
to be lifted away from the leg musculature and be
mechanically stabilized. When placed on the platform andlifted,
the nerve was put under some tension and was heldstationary and
physically isolated from the animal. Conse-quently, small movements
of the animal resulting from heart-
beat, respiration, and involuntary muscle movements werenot
transmitted to the nerve. The microplatform also allowedthe nerve
to be maintained in an aqueous environment whileeliminating contact
with other tissues, thus ensuring that the
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER2007 | 685
NANOKNIFE FOR AXON SURGERY
-
8/3/2019 Wesley C. Chang et al- In Vivo Use of a Nanoknife for
Axon Microsurgery
4/10
electrical nerve stimulation did not feed through to the
mus-cles through other pathways in the animal. Although mechan-ical
manipulations were required to place the intact nerve onthe
platform and to prepare the exposed axons for cutting,nerve
function itself was not disrupted because nerve stimu-lation using
the built-in electrode on the platform readily trig-gered
observable twitching of the calf muscle and an easilydetectable EMG
signal.
Observation During the Surgical Procedure
Because conventional surgical or tissue dissection micro-scopes
lack the necessary magnification to observe individualaxons, an
upright, boom-mounted research microscopeequipped with 10 eyepieces
was adapted for direct overheadobservation of the surgical field
with both brightfield and flu-orescence imaging. This research
microscope was equippedwith 4 to 20 long working distance objective
lenses that pro-
vided a working distance between the front of the objectiveand
the tissue of 7.4 to 17 mm. Operation of the nanoknife inthe
surgical setting as described required a minimum workingdistance of
approximately 5 mm.
Cutting With the Nanoknife
The exposed tibial branch of the mouse sciatic nerve asviewed
through the microscope during a cutting sequence isshown in Figure
3. In Figure 3A, the black profile is a portion ofthe nanoknife
brought in from above into the surgical field andprepositioned to
the side of the nerve. At this position, thenanoknife is raised
above both the microplatform and thenerve, resulting in the knife
profile being slightly out of focusrelative to the nerve.
To test whether or not this microdevice can be used tomake small
cuts in a living nerve, the nanoknife was broughtover the desired
position and lowered onto the nerve (Fig.3B). The silicon nitride
material is sufficiently optically trans-lucent to allow
visualization of the nerve through the nano-knife itself. This
property of the microdevice was useful in
allowing the operator to roughly judge nanoknife contactwith the
nerve and dimpling of nerve tissue during the cut-ting. The amount
of vertical displacement of the nanoknifeduring cutting could also
be determined more accuratelyfrom the micromanipulator
controller.
The resulting incision from one nerve cutting experiment isshown
in Figure 3C (arrow). The incision measured approxi-mately 100 m in
length, corresponding to the length of the
686 | VOLUME 61 | NUMBER 4 | OCTOBER 2007
www.neurosurgery-online.com
CHANG ET AL.
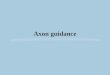
FIGURE 2. A diagram of the axon nanoknife showing device
configura-
tion and the ultrasharp cutting edge (apex of the elongated
pyramidalstructure, green). B, wider view of the mounted knife
(boxed), held by amicropipette holder, which in turn is held in the
micromanipulator.
A
B
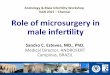
FIGURE 3. Visualization and use of the axon nanoknife for
microscalenerve cutting is demonstrated. A, the intact nerve as
viewed through the
microscope with a total magnification 100. The nanoknife with
a100-m long cutting edge is held above the nerve off to one side at
thebeginning of the procedure (upper right). B, the nanoknife is
brought overthe desired position and lowered to make the cut. C, a
cut approximately100 m long (arrow) is visible in the nerve. D, the
cutting sequence wasrepeated using the same nanoknife to make a
second cut in the nerve(arrow). AD, scale bar, 200 m.
A B
C D
-
8/3/2019 Wesley C. Chang et al- In Vivo Use of a Nanoknife for
Axon Microsurgery
5/10
nanoknife cutting edge of 100 m. The cutting sequence
wasrepeated, and a second incision of approximately the same
sizewas made (Fig. 3D, arrow) next to the original. We estimate
thatin each cut, perhaps 50 to 100 axons are severed, but this
quan-tification remains to be verified objectively.
To assess the physiological state of the cut ends of axons
sev-ered by the nanoknife, this cutting procedure was also
repeatedin a GFP transgenic animal in which all cells contained
freelydissolved cytoplasmic GFP (Fig. 4A). Under fluorescence
imag-ing, it was possible to identify the site of the cut (Fig.
4B,arrow). At this cut site, the severed axons remained
brightlyfluorescent, indicating the retention of cytoplasmic GFP.
Thisability of severed axons to reseal its cut ends has been
previ-
ously demonstrated in vitro (6) and is presumably the result
ofthe preservation of membrane self-repair mechanisms (2).
EMG Recording
When the nerve was stimulated at low frequencies of 5 Hz,the
innervated calf muscles twitched visibly, providing an inde-pendent
visual confirmation that the stimulation worked andwas above
threshold. Concurrently, the recording probe
inserted into the target muscle recorded a signal consisting
ofan artifact coinciding with the stimulating pulse followed by
anEMG waveform beginning approximately 1 ms later. When the
background (control) waveform was subtracted from this
rawrecording, the artifact was largely eliminated, and the
trueshape and duration of the EMG wave could be discerned.Control
waveforms have been subtracted from all EMG record-ings shown in
the figures. Typically, the waveform lasted justover 2 ms (Fig. 5).
By varying the magnitude of the stimulationpulse, it was determined
that, for this system, the threshold forevoking a response in the
muscle was between 300 and 400mV delivered at the platform. Below
this threshold, therecorded muscle signal was nearly identical to
the backgroundcontrol and no muscle twitching was observed.
Repeated Use of the Nanoknife for Targeted Cutting
The precision and durability of the nanoknives was demon-strated
in experiments in which a single nanoknife was usedrepeatedly to
progressively pare down a nerve. For this exer-cise, a shorter
knife with a cutting edge of 10 m was used.From our observations,
we estimate that perhaps only a fewdozen axons are severed with
each cutting stroke. In additionto visual observations of the
cutting sequence and the tissueincisions, the successive removal of
functional axons withinthe nerve was verified simultaneously with
EMG recordingfrom the innervated calf muscle (Fig. 5). The intact
nerve sup-ported by the microplatform at the start of the procedure
isshown in Figure 5A. Figure 5B shows the EMG recording fol-lowing
the delivery of a subthreshold stimulus, whereas Figure5C shows the
EMG waveform recorded after delivery of asupramaximal stimulus.
Figure 5F shows the muscle responseresulting from stimulation of an
intact nerve and after a largenumber of axons had been cut by the
nanoknife (Fig. 5, D andF). We estimate that approximately one-half
to two-thirds of
the nerve had been eliminated at this point. As a result of
thesmall amount of tension on the nerve when it is placed ontothe
microplatform, the ends of severed axons retract from thefield of
view while the remaining uncut axons remain in thesurgical field.
The progressive diminution in the EMG wave-form at various stages
of this cutting procedure is shown inFigure 5, GI. Note that the
EMG recordings in Figure 5, E, F, Hand Iwere obtained using a
fourfold suprathreshold stimulus.Figure 3H shows the EMG
corresponding to the situationshown in Figure 5G, in which only a
few axons are left on themicroplatform. The severing of these
remaining axons withthe nanoknife resulted in the elimination of
detectable EMGsignal (Fig. 5I).
Although we have shown that the EMG signal diminishes
monotonically with the paring down of the nerve, the
exactrelationship between the fraction of the nerve eliminated
andthe diminution of the EMG is undetermined and indeed varies
between different trials. This uncertainty results from the
waythat the EMG signal is constructed, a summation of signalsfrom
the individual innervated muscle cells. The strongest con-tributors
to the composite EMG signal are from the cells clos-est to the
recording probe, whereas more distant muscle cells
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER2007 | 687
NANOKNIFE FOR AXON SURGERY
FIGURE 4. The nerve of a GFP transgenic mouse is demonstrated
beforebeing cut (A) and 3 minutes after being cut (B). The cut is
indicated bythe arrow. The retention of the cytoplasmic GFP
indicated that the cutends readily resealed. Scale bar, 200 m.
A
B
-
8/3/2019 Wesley C. Chang et al- In Vivo Use of a Nanoknife for
Axon Microsurgery
6/10
contribute less. Thus, cutting axons that map to muscle near
theprobe results in a larger diminution of the signal that
wouldoccur when the exact same cut is made in axons mapping
tomuscle cells further away.
With repeated use, the cutting performance of the nanoknifewas
not noticeably diminished. Breakage of the nanoknife itselfduring
cutting was only observed in instances in which opera-tor error led
to the unintended impact of the nanoknife with themicroplatform or
some other nearby surface. The most frequentlimitation to the
lifetimes of the nanoknives was not in fact
breakage of the silicon nitride microdevice, but the breakage
atthe joint where the microdevice is attached to its mounting
rod.
Surgical Cutting of Single Axons
A major goal of this study was to determine whether or
notnanoknife use could enable novel cellular or
subcellular-scalesurgical procedures that are not currently
feasible using exist-ing instrumentation. We tested the precision
and cutting per-formance of the nanoknife on individual axons in an
in vivosurgical environment. A sequence of images illustrating the
useof a nanoknife on a single axon is shown in Figure 6. In
thisexample, the nanoknife was operated in the same manner as
described previously for mak-ing incisions in whole
nerves.Figure 6, B and C, shows thenanoknife moved into posi-tion
for axon cutting, whereasFigure 6D shows the resultingcut (arrow)
in the targetedaxon. Asecond cut was subse-quently made in the
sameaxon resulting in the isolationof a short 30-m segment (Fig.6E,
arrow). This axon segmentwas moved away from theparent axon to aid
in visuali-zation (Fig. 6F, arrow).
Biocompatibility ofSilicon Nitride forNeurons
During the course of ourexperimentation, we did notencounter
instances of appar-ent acute deleterious effects ofsilicon nitride
on nerves orsurrounding tissues. To exam-ine this issue of
biocompatibil-ity in more detail, we placedactual nanoknives in
tissueculture dishes and seededmouse retinal explant tissue
orhippocampal neurons directlyonto silicon nitride knives
todetermine whether this mate-rial was suitable as a neuronal
growth substrate. The results showed that after 2 days in
culturedirectly on silicon nitride, hippocampal neurons that
wereseeded as isolated neurons exhibited significant process
out-growth (Fig. 7A). Likewise, a fairly dense network of
axongrowth could be observed from the explanted retinal tissue
(Fig.7B). The appearance of the retinal axons and hippocampal
neu-rons were very similar to what has been reported when they
aregrown on tissue culture glass (3, 5, 21).
DISCUSSION
In this study, we subjected silicon nitride nanoknives to
test-ing under the operative conditions of peripheral nerve
surgeryin a living anesthetized mouse. The main objectives of
this
work were to examine whether or not this new type ofmicroscale
neurosurgical instrumentation could be used effec-tively in vivo
and to verify the ability of these microdevices todeliver surgical
precision at unprecedented cellular and subcel-lular length scales.
The results demonstrated that by using arudimentary microplatform
and off-the-shelf components suchas micromanipulators and research
microscopes, nanoknivescan be deployed and used effectively for
microscale peripheral
688 | VOLUME 61 | NUMBER 4 | OCTOBER 2007
www.neurosurgery-online.com
CHANG ET AL.
FIGURE 5. Nerve images and EMG recordings showing the
progressive loss of evoked muscle response signal dur-ing nerve
section using an axon nanoknife. A, image showing the intact tibial
branch of the sciatic nerve supportedon the microplatform. B,
application of a subthreshold stimulus (200 mV) resulted in no
detectable EMG signal. C,the resulting EMG signal after application
of a suprathreshold stimulus (500 mV) is shown. D, view of the
nerve aftermost of its axons have been pared away using the
nanoknife is demonstrated. E, the EMG waveform recorded in
thesoleus muscle after stimulation of the intact nerve is shown
with a stimulus fourfold above threshold. F, the EMGwaveform was
recorded from the remaining axons shown in D. This waveform is
reduced in amplitude compared withthat obtained from the intact
nerve. G, continued axon cutting using the same nanoknife left just
a few axons remain-ing on the microplatform. H, the EMG waveform
was recorded from stimulation of the axons remaining in G. I,
noapparent EMG signal is observed after all of the axons have been
cut using the nanoknife.
-
8/3/2019 Wesley C. Chang et al- In Vivo Use of a Nanoknife for
Axon Microsurgery
7/10
nerve surgery. In addition to precise 50 to 100 m incisions ina
peripheral nerve, and the incremental paring down of a sin-gle
nerves muscle response, novel subcellular-scale neurosur-gical
procedures enabled by this novel surgical instrumentationincluded
the precise targeted cutting and isolation of a seg-ment from a
single axon in vivo. All procedures could beobserved and monitored
in real-time, allowing user feedback,image capture, and EMG
recording.
Microdevice Robustness
For use in microsurgery, microdevices must be mechanicallystrong
to permit repeated use. The robust performance of thenanoknife is
attributable in part to the material properties of sil-icon nitride
(ultimate strength, 28 GPa), which is actuallystronger than bulk
steel (ultimate strength, 0.5 GPa).Moreover, silicon nitride is not
subject to plastic deformation(4), which would tend to dull cutting
edges after repeated use.
A single device has been used previously to cut more than
200axons in vitro (6).
Microinstrumentation Use in Vivo
A fundamental question concerning the surgical use
ofmicrodevices that have characteristic sizes of only several
tensor hundreds of microns is whether or not such small
instru-mentation can be deployed satisfactorily and used
efficiently
in an operative field. For the current study, we have chosen
toaddress this question using the relatively accessible tibial
branch of the mouse sciatic nerve in a demonstration ofmicroscale
nerve and single axon cutting. The key to deploy-ment of the
nanoknife in this instance was the use of a rudi-mentary
microplatform that provided support for the nerveand allowed the
nerve to be mechanically isolated. Themicroplatform also served as
an axon microcutting surface,
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER 2007 | 689
NANOKNIFE FOR AXON SURGERY
FIGURE 6. Precise targeted cutting of a single axon is performed
usingthe nanoknife. A, view of an axon (center bottom) isolated
from the tib-ial branch of the sciatic nerve and resting on the
microplatform is shown.B, the nanoknife (upper right) is elevated
above the axon off to one sideat the beginning of the procedure. C,
the nanoknife is lowered to make a
precise cut in the axon of interest. D, the axon is severed at
the locationindicated by the arrow. The nanoknife has been removed
from the surgi-
cal field. E, the cutting sequence was repeated using the same
nanoknife tomake a second cut in the axon (arrow). F, the small
segment in betweenthe two incisions made in D and E was moved aside
and is indicated bythe arrow. AF, scale bar, 200 m.
A B
C D
E F
FIGURE 7. Fluorescent images showing hippocampal neurons (A)
andneurite outgrowth (B) from embryonic retinal explants cultured
on siliconnitride substrates. The neurons used in these experiments
express a solu-ble cytoplasmic GFP protein and are fluorescent. AB,
scale bar, 100 m.
A
B
-
8/3/2019 Wesley C. Chang et al- In Vivo Use of a Nanoknife for
Axon Microsurgery
8/10
allowing the nerve to remain moist while isolated from
othertissues. The spatial stability of the resulting operative
fieldduplicated the well-controlled in vitro environment in whichwe
have previously used similar cutting microdevices suc-cessfully (6,
20). Lastly, the microplatform also contained anembedded electrode
for nerve stimulation. Although thismicroplatform strategy was
designed for microdevice use inperipheral nerve surgery, a similar
strategy can also be triedfor the more challenging use of surgical
microdevices in cen-tral nervous system regions such as the spinal
cord.
Improvements to Off-the-shelf Components
Except for the nanoknife and the microplatform, all
otherinstrumentation used in this study is commercially
available.Although they serve the needs of this initial study,
morerefined equipment could be developed specifically to enablethe
efficient use of surgical microdevices. One area of need isthe
development of miniaturized micromanipulators to econ-omize on
space utilization around the operative field. Anotherarea of
critical need is the development of surgical micro-scopes with
sufficient magnification to visualize axons andthat provide
sufficient working distances between the opticalelements and the
tissue, similar to the boom-mounted micro-scope used in this study
but more specifically designed formicrosurgery. The design of
future surgical microscopes forcellular-scale neurosurgery should
also include on-boardlighting and likely also incorporate
fluorescence imaging,which provides more contrast and far better
signal-to-noiseratios over brightfield imaging. Another useful
feature would
be a mechanism to coordinate the spatial positioning andmovement
of the surgical field (animal), the operatingmicrodevices, and the
field of view of the surgical microscope.Finally, ease of use by
the operator and other ergonomicissues must be considered and
incorporated into more refined
systems compatible with clinical use.Issues of
Biocompatibility
An obvious concern of any prospective medical device is
thesuitability of the constituent materials for the target
tissue.Evaluations of biocompatibility include identifying any
acutetoxins that have an immediate, detrimental effect on the
hosttissue as well as longer-term responses of the host tissue
result-ing from the prolonged presence of the materials. For
siliconnitride, an essential material in many microdevices,
biocompat-ibility has been demonstrated both in vitro with tissue
slicesand in vivo (9, 10, 22). In our own tests, we demonstrated
thatindividual neurons grow and extend neurites directly on
siliconnitride-coated substrates with outgrowths and neuronal
sur-
vival comparable to those on standard culture glass,
indicatingthe absence of any acute toxicity. Furthermore, extensive
stud-ies of silicon nitride with implantable microdevices such
asminiature electrode and neurorecording arrays (10) haveshown that
this material can be implanted in an animal and leftfor many weeks
without eliciting adverse responses from hosttissues. One study (9)
explicitly evaluated silicon nitride, alongwith other materials,
against a battery of standard biocompat-
ibility tests and considered the material as a nonirritant.Taken
together, these findings establish silicon nitride as suit-able for
use with neural tissues, especially in cases requiringonly brief
contact with tissues.
Cellular and Subcellular-scale Surgery
In this study, we performed what we believe is the first
sub-cellular-scale surgery on a single axon in a living
anesthetizedanimal. Although the simple cutting of single axons in
itself haslimited clinical applications, the development of
microdevicesfor precise axon cutting is the first part of a
long-term researchprogram that examines the feasibility of
conducting the surgi-cal repair of individual damaged or severed
axons as a meansof achieving functional recovery after nervous
system injuryindependent of axonal regeneration (20). We have
previouslyproposed that axon cutting would be followed by the
align-ment of severed axon ends and subsequent axon splicing
byelectrofusion to reconstitute functional axons. Although
pre-liminary proof of principle has been obtained for these
lattersteps, the execution of an entire axon repair sequence in
vivowill require much future research and development. However,it
is worthwhile to consider that new microscale surgical
instru-mentation can extend surgical therapy beyond the
currentorgan and tissue levels into the realm of cells or even
subcellu-lar components. This cell level surgical capability may
invari-ably have other uses in clinical neurosurgery and in
basicresearch where the isolation or manipulation of specific parts
ofa neuron may have substantial scientific interest.
Micro- and Nanotechnology in Neurosurgery
It is increasingly recognized that not only will micro-
andnanotechnology greatly impact the current practice of medi-cine
in both diagnosis and therapy, these emerging disciplinescan also
potentially enable new neurosurgical procedures at
unprecedented small scales (1, 1113, 17). Currently,
optimaltreatment is not possible in many cases as a result of a
mis-match between tissue size and surgical instrumentation.
Newmicrofabricated surgical instruments with nanoscale featuresthat
can overcome these limitations will allow a new level ofaccess at
the cell and tissue level that is not possible with cur-rent
technology. Microdevices fabricated using methodsadapted from the
semiconductor industry are already used incommon everyday products
such as automobile airbag sen-sors, inkjet printer heads, and
micromirror arrays in digitallight processing projectors. As a
result of their inherent smallmass and robust mechanical
properties, such micromachinescan be operated at extremely high
speeds and have proven to
be very durable and reliable. However, the use of
microdevices
as cellular or subcellular-scale operative instruments
bringsabout a different set of challenges. Although the
manufactureof miniature-scaled neurosurgical devices is based on
well-developed and reasonably mature fabrication technology,
theactual performance of such microinstrumentation in vivo andtheir
potential use in cellular and subcellular-scale neurosurgi-cal
procedures have yet to be optimized and should representan
important new direction in microsurgery.
690 | VOLUME 61 | NUMBER 4 | OCTOBER2007
www.neurosurgery-online.com
CHANG ET AL.
-
8/3/2019 Wesley C. Chang et al- In Vivo Use of a Nanoknife for
Axon Microsurgery
9/10
Disclosure
David W. Sretavan, M.D., Ph.D., is a founder with a financial
inter-est in a biotechnology company developing microdevices for
applica-tions in microsurgery.
REFERENCES
1. Apuzzo ML, Liu CY: 2001: Things to come. Neurosurgery
49:765778, 2001.2. Bement WM, Yu HY, Burkel BM, Vaughan EM, Clark
AG: Rehabilitation and
the single cell. Curr Opin Cell Biol 19:95100, 2007.
3. Birgbauer E, Oster SF, Severin CG, Sretavan DW: Retinal axon
growth conesrespond to EphB extracellular domains as inhibitory
axon guidance cues.
Development 128:30413048, 2001.
4. Bostock R, Collier J, Jansen R-JE, Jones R, Moore D, Townsend
J: Siliconnitride microclips for the kinematic location of optic
fibres in silicon V-shapedgrooves.J Micromech Microeng 8:343360,
1998.
5. Brewer GJ, Torricelli JR, Evege EK, Price PJ: Optimized
survival of hippocam-pal neurons in B27-supplemented Neurobasal, a
new serum-free mediumcombination.J Neurosci Res 35:567576,
1993.
6. Chang WC, Keller CG, Sretavan DW: Isolation of neuronal
substructures andprecise neural microdissection using a nanocutting
device. J Neurosci
Methods 152:8390, 2006.
7. Ellis-Behnke RG, Liang YX, You SW, Tay DK, Zhang S, So KF,
Schneider GE:Nano neuro knitting: Peptide nanofiber scaffold for
brain repair and axon
regeneration with functional return of vision. Proc Natl Acad
Sci U S A103:50545059, 2006.
8. Goldshmit Y, Galea MP, Wise G, Bartlett PF, Turnley AM:
Axonal regenerationand lack of astrocytic gliosis in
EphA4-deficient mice. J Neurosci24:10,06410,073, 2004.
9. Kotzar G, Freas M, Abel P, Fleischman A, Roy S, Zorman C,
Moran JM,Melzak J: Evaluation of MEMS materials of construction for
implantable
medical devices. Biomaterials 23:27372750, 2002.10. Kristensen
BW, Noraberg J, Thibaud P, Koudelka-Hep M, Zimmer J:
Biocompatibility of silicon-based arrays of electrodes coupled
to organotypic
hippocampal brain slice cultures. Brain Res 896:117, 2001.11.
Leary SP, Liu CY, Apuzzo ML: Toward the emergence of
nanoneurosurgery:
Part IInanomedicine: Diagnostics and imaging at the nanoscale
level.
Neurosurgery 58:805823, 2006.12. Leary SP, Liu CY, Apuzzo ML:
Toward the emergence of nanoneurosurgery:
Part IIInanomedicine: Targeted nanotherapy, nanosurgery, and
progresstoward the realization of nanoneurosurgery. Neurosurgery
58:10091026,
2006.13. Leary SP, Liu CY, Yu C, Apuzzo ML: Toward the emergence
of nanoneuro-
surgery: Part Iprogress in nanoscience, nanotechnology, and the
comprehen-
sion of events in the mesoscale realm. Neurosurgery 57:606634,
2005.14. Okabe M, Ikawa M, Kominami K, Nakanishi T, Nishimune Y:
Green mice as
a source of ubiquitous green cells. FEBS Lett 407:313319,
1997.
15. Polla DL, Erdman AG, Robbins WP, Markus DT, Diaz-Diaz J,
Rizq R, Nam Y,Brickner HT, Wang A, Krulevitch P: Microdevices in
medicine. Annu Rev
Biomed Eng 2:551576, 2000.
16. Rebello KJ: Applications of MEMS in surgery. Proceedings of
the IEEE92:4355, 2004.
17. Roy S, Ferrara LA, Fleischman AJ, Benzel EC:
Microelectromechanical sys-
tems and neurosurgery: A new era in a new millennium.
Neurosurgery49:779798, 2001.
18. Schwab ME: Repairing the injured spinal cord. Science
295:10291031, 2002.
19. Silver J, Miller JH: Regeneration beyond the glial scar. Nat
Rev Neurosci5:146156, 2004.
20. Sretavan DW, Chang W, Hawkes E, Keller C, Kliot M:
Microscale surgery onsingle axons. Neurosurgery 57:635646,
2005.
21. Suh LH, Oster SF, Soehrman SS, Grenningloh G, Sretavan DW:
L1/Lamininmodulation of growth cone response to EphB triggers
growth pauses and reg-
ulates the microtubule destabilizing protein SCG10.J Neurosci
24:19761986,2004.
22. Voskerician G, Shive MS, Shawgo RS, von Recum H, Anderson
JM, Cima MJ,
Langer R: Biocompatibility and biofouling of MEMS drug delivery
devices.Biomaterials 24:19591967, 2003.
AcknowledgmentsThis research was supported by the Sandler Family
Supporting Foundation
and the That Man May See Foundation. David W. Sretavan, M.D.,
Ph.D., is arecipient of Research to Prevent Blindness Lew R.
Wasserman Merit Award.Additional support to the Sretavan Laboratory
from the National Eye Institute
and the Research to Prevent Blindness Foundation is gratefully
acknowledged.All devices were fabricated at the University of
California Berkeley Micro-fabrication Laboratory.
COMMENTS
Chang et al. have eloquently presented their work in a most
excitingarea of medicine, the micro- and nanoworld as it pertains
tomanipulation and alteration of neural structures. They have
demon-strated that axon surgery is indeed possible. This seems
farfetched butso have many advances in neurosurgery during their
early formativeyears. The major obstacles to the advancement of
this field will berelated to the development of surgical platforms
and the performanceof multiple microtasks in rapid succession or
simultaneously. The lat-ter is required to accomplish clinically
relevant surgical procedures inmultiple axons in a timely manner.
The work of Chang et al., however,suggests that such further
refinements are not all that far off. Theauthors are to be
commended for their vision, their forward-thinkingefforts, and
their creativity.
Edward C. BenzelCleveland, Ohio
In this report, the authors describe the use of a
microfabricatednanoknife with a cutting edge measuring 20
nanometers for use invivo. Previous work from the same group has
reported the use of thesame nanoknife as applied in vitro for
single axon surgery. This rep-resents an extension of the work to
the in vivo environment forperipheral nerve surgery in a mouse
model. The authors were able toconstruct a surgical setup such that
the operative substrate wasimmobilized from the normal respiration
and movements of themouse. The nanoknife was used to make
progressive cuts in the sci-atic nerve, with electrophysiological
recordings demonstrating the
progress dimunition of motor responses from the target muscle.
Inaddition, single axon surgery was demonstrated in vivo. Finally,
bio-compatibility of the device was also demonstrated by cell
cultureexperiments. This is a highly important report in that it
represents thefirst demonstration of subcellular surgery in vivo.
Although it is notquite surgery on the nanoscale, this
demonstration represents a majorreduction in the scale of surgery
in a living animal. I look forward tofuture work from the authors
with demonstration of the sequentialsteps of single axon
repair.
Charles Y. LiuLos Angeles, California
This project uses a nanoblade to cut nervous tissue and axons.
Theirdevice appears similar to single-cell extraction techniques
inwhich a micropipette tip controlled by a robotic micromanipulator
is
used to selectively aspirate axons, dendrites, or cell bodies
from neu-rons in culture. As with previously published in vitro
experiments (1),once an axon has been isolated, it can be precisely
transected. Usinga mouse sciatic nerve, the authors had to first
separate an axon fromthe nerve before cutting it on the platform.
Therefore, in situ singleaxon transection has not been demonstrated
thus far. Limitationsinclude a wide nanoblade and, perhaps,
difficulty differentiating indi-vidual axons.
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER2007 | 691
NANOKNIFE FOR AXON SURGERY
-
8/3/2019 Wesley C. Chang et al- In Vivo Use of a Nanoknife for
Axon Microsurgery
10/10
The authors ultimate goal is to use this device to directly
repairaxons. However, the current clinical applications of direct
axon repairappear quite limited. For example, what is the time
window for axonrepair before Wallerian degeneration? Additional
pathophysiologicalstudies are needed to answer questions such as
these. Regardingperipheral nerve repair, alignment of the basal
lamina delineating theendoneurial tubes may be an alternative
application that is more read-
ily applicable to current practice.Despite these concerns, the
authors are commended for their for-ward-thinking concept. As their
technology advances parallel to simul-taneous discoveries in
neuronal protection, intraoperative imaging,and device production,
potential nanotechnology applications in neu-rosurgery will surely
appear over time.
Stephen M. RussellNew York, New York
1. Sretavan DW, Chang W, Hawkes E, Keller C, Kliot M: Microscale
surgery on
single axons. Neurosurgery 57:635646, 2005.
W
ith the advent of the operating microscope and
microsurgicaltechniques, Millesi (4) and Millesi et al. (5)
improved clinical
results and popularized the use of nerve grafts for nerve
repair. Todate, surgical techniques for nerve repair have been at
the tissue orcable level. Even in a fascicular nerve repair, there
are literally severalhundred to a few thousand axons in the
proximal stump and a simi-lar number of endoneurial pathways in the
distal stump (3). With themost meticulous repairs, the endoneurial
tubes can never be reap-proximated exactly, and this results in
mismatching of regeneratingaxons at the site of suture, or within
the graft, leading to inappropri-ate (non-specific) and incomplete
reinnervation and subsequent poorrecovery in function (1).
Misdirection at the repair site is common,and precise reinnervation
is only possible in clean and focal crushinjuries rather than ones
in which the nerve is severed and thenrepaired with a suture
(6).
Techniques to match regenerating axons with reciprocal and
appro-priate targets in the distal nerve stump are currently only
partially
possible with experimental techniques that maximize
topographic
alignment (2). Further technological advances will require
micro-surgery to be performed at a cellular level.
It is in this context that the current report by Chang et al. is
relevant.They illustrate the in vivo use of a microfabricated
nanoknife to per-form nerve and axon microsurgery. Essentially, the
data demonstratethat precise and targeted severance of a portion of
a mouse tibial nerveand individual axons from the same tibial nerve
can be achieved using
the prototype device. It is notable that a significant
engineering aspectis the development of the entire assembly for the
micromanipulation,a microplatform in which the nerve is positioned,
followed by theactual use of this cutting device. Each of these is
a fundamental engi-neering issue that the investigators have solved
admirably. Yet, thetranslation of this device from the type of
proof of principle demon-strated herein to a practical tool for
human nerve surgery remains chal-lenging.
A major shortcoming with even the most microscopic form of
nerverepair is the biological constraint of cellular misalignment,
which can-not be easily overcome by further progress in
microsurgical techniques.The authors have provided the first
glimpse of the technologies thatmay enable more precise surgery at
the nanoscale level. I look forwardto further studies by these
investigators as they endeavor to advancenerve repair into the
cellular domain.
Rajiv MidhaCalgary, Canada
1. Brushart TM: The mechanical and humoral control of
specificity in nerverepair, in Gelberman RH (ed): Operative Nerve
Repair and Reconstruction.
Philadelphia, J.B. Lippincott, 1991, pp 215230.2. de Medinaceli
L, Rawlings RR: Is it possible to predict the outcome of
periph-
eral nerve injuries? A probability model based on prosoects for
regenerating
neurites. Biosystems 20:243258, 1987.3. Matsuyama T, Mackay M,
Midha R: Peripheral nerve repair and grafting tech-
niques: A review. Neurol Med Chir (Tokyo) 40:187199, 2000.
4. Millesi H: Brachial plexus injuries. Nerve grafting. Clin
Orthop Relat Res237:3642, 1988.
5. Millesi H, Meissl G, Berger A: The interfascicular
nerve-grafting of the median
and ulnar nerves.J Bone Joint Surg Am 54:727750, 1972.6. Nguyen
QT, Sanes JR, Lichtman JW: Pre-existing pathways promote
precise
projection patterns. Nat Neurosci 5:861867, 2002.
692 | VOLUME 61 | NUMBER 4 | OCTOBER 2007
www.neurosurgery-online.com
CHANG ET AL.