Embed Size (px)
Citation preview
Well-Being of the First Responder

Topic Overview
Emotional Aspects of Emergency Care Death and Dying High Stress Situations Stress Management
Critical Incident Stress Debriefing Critical Incident Defusing Debriefing

Topic Overview
Scene Safety Protecting yourself from disease Protecting yourself from injury
Diseases of Concern
Emotional Aspects of Emergency Care Death and Dying
Definitions Clinical Death Biological Death Dead Dead (DRT)
Decapitation Rigor mortis Lividity Decomposition

Emotional Aspects of Emergency Care Death and Dying
Five Emotional Stages Denial
Anger
Bargaining
Depression
Acceptance
Emotional Aspects of Emergency Care Dealing with Dying Patients, Family and Bystanders
To reduce emotional burden Treat with dignity Treat with respect Communicate – help orient to surroundings Allow the to express themselves Listen empathetically Do Not give false reassurances Use a gentle tone of voice Use a reassuring touch Do what you can to provide comfort
Emotional Aspects of Emergency Care High Stress Situations
Multiple casualty incidents Pediatric emergencies Abuse and neglect Injury or death of co-worker Responding or providing emergency care to a relative or
friend Severe traumatic injuries or amputations
Emotional Aspects of Emergency Care
Stress Management Warning Signs
Irritability with coworkers, family & friends Inability to concentrate Difficulty sleeping and nightmares Anxiety Indecisiveness Guilt Loss of appetite Loss of sexual desire or interest Isolation Loss of interest in work
Emotional Aspects of Emergency Care Warning signs – continued
Thinking confusion, inability to make judgments, decisions,
chronic forgetfulness Psychological
depression, excessive anger, negativism, hostility, defensiveness
Physical Persistent headaches, exhaustion, gastrointestinal
distress

Emotional Aspects of Emergency Care Warning signs – continued
Behavioral Overeating, increased drugs / alcohol, hyperactivity
Social Increased interpersonal conflicts, decreased ability to
relate to others
Emotional Aspects of Emergency Care Lifestyle Changes
Diet Exercise Learn to Relax Avoid self medication
Keep balance in your life Make changes in your work environment
Emotional Aspects of Emergency Care Critical Incidents
Defusing Held within 1-4 hours of incident Attended only by those involved Lasts 30-45 minutes Less structured than CISD
Emotional Aspects of Emergency Care Critical Incident Stress Debriefing (CISD)
Not professional counseling Ideally held within 24-72 hour4s Seven phases
Introduction Facts of event Feelings explored Symptoms – self look Teaching using skilled professionals Re-entry – plan of action for returning to work Follow-up several weeks to months later
Scene safety Protecting yourself from disease
Body Substance Isolation 1980’s CDC published guidelines that set a new
standard against infection Assumes that all blood and body fluids are infectious Requires first responders to practice strict infection
control – Body Substance Isolation

Scene Safety Guidelines for BSI precautions
Hand washing Single Most Important Way to Prevent Spread of
Disease Always Wear Personal Protective Equipment
Eye protection Gloves Gowns Masks
Cleaning, disinfecting and sterilizing
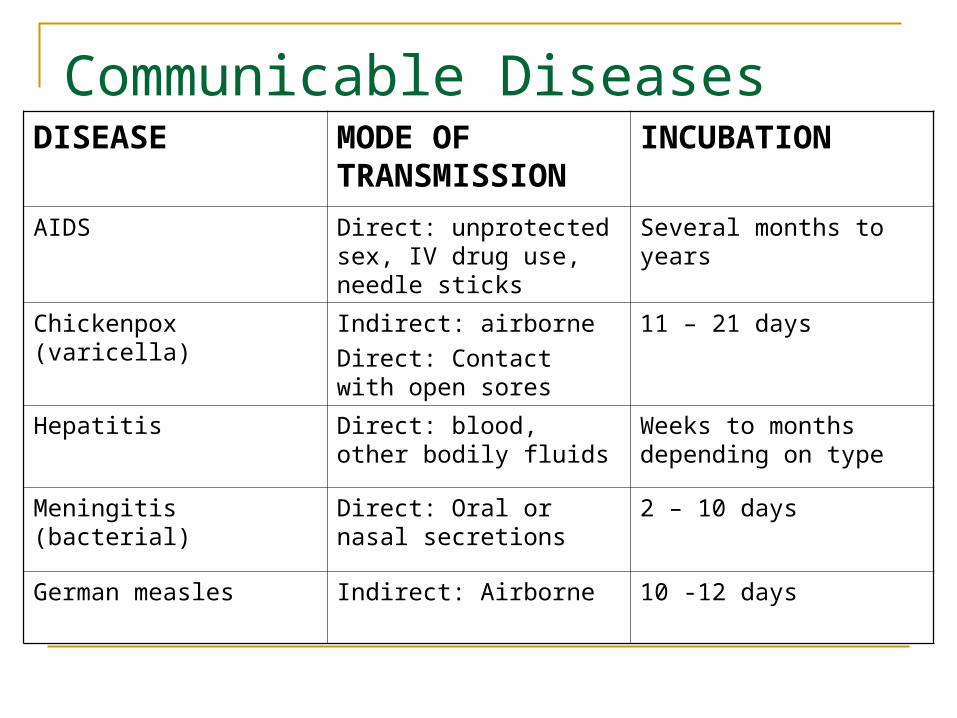
Communicable DiseasesDISEASE MODE OF
TRANSMISSIONINCUBATION
AIDS Direct: unprotected sex, IV drug use, needle sticks
Several months to years
Chickenpox (varicella) Indirect: airborne
Direct: Contact with open sores
11 – 21 days
Hepatitis Direct: blood, other bodily fluids
Weeks to months depending on type
Meningitis (bacterial) Direct: Oral or nasal secretions
2 – 10 days
German measles Indirect: Airborne 10 -12 days
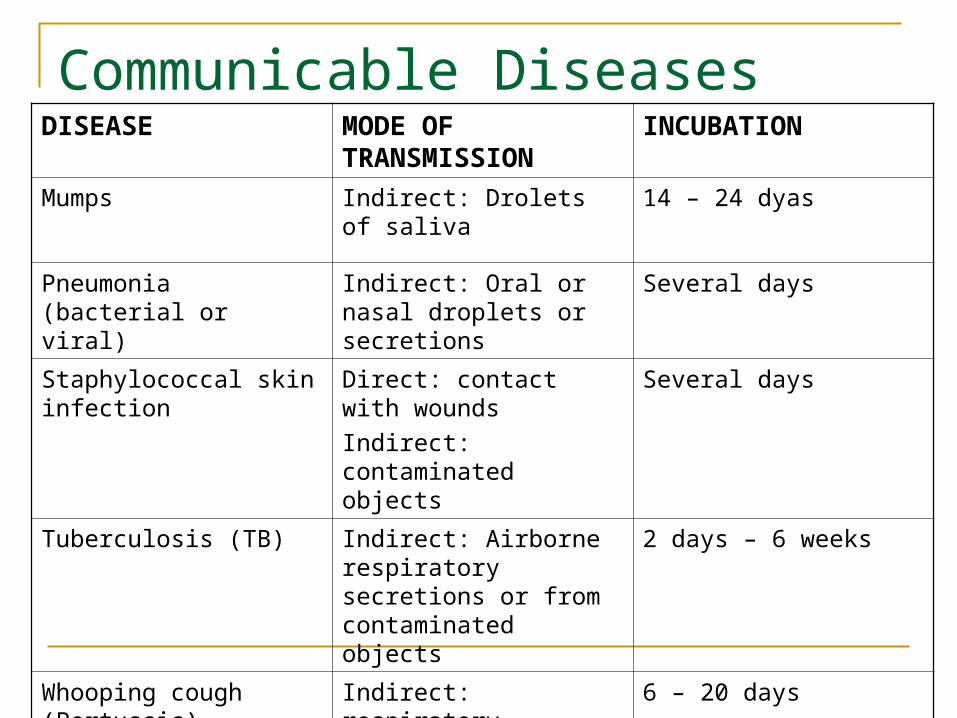
Communicable DiseasesDISEASE MODE OF
TRANSMISSIONINCUBATION
Mumps Indirect: Drolets of saliva 14 – 24 dyas
Pneumonia (bacterial or viral)
Indirect: Oral or nasal droplets or secretions
Several days
Staphylococcal skin infection
Direct: contact with wounds
Indirect: contaminated objects
Several days
Tuberculosis (TB) Indirect: Airborne respiratory secretions or from contaminated objects
2 days – 6 weeks
Whooping cough (Pertussis)
Indirect: respiratory secretions or droplets
6 – 20 days
Scene Safety
Advanced Safety Precautions PPD every year Immunizations
Tetanus (10 years) Hepatitis B Influenza (annually) Polio (if needed) Rubella Measles Mumps

Scene Safety
Reporting Exposure State laws vary Prompt reporting
Protecting yourself from accidental injury
OSHA
Occupational Safety and Health Administration Regulations
Issues regulations to reduce or remove hazards of bloodborne pathogens in the workplace.
Regulations apply to employers whose employees have potential exposure risk.
OSHA Requirements Exposure Control Plans
Exposure Determination Communications Schedules and methods for implementing elements of the
OSHA standard Procedures for evaluating exposure incidents
Engineering Controls Cleaning Schedule
Workplace Practices Universal Precautions, PPE
METHODS OF COMPLIANCE
Exposure Control Plan
Needle acupuncture
Nose bleed First Aid (CPR) Electrotherapy
pads Patients with
open wounds or sores
Venipuncture Vomitus Lab Samples Contaminated
laundry Accidental puncture
using a pinwheel
Potential Risks in a Chiropractic Practice
Exposure Control Plan
COMMUNICATION Signs & Labels
- Biohazard Sign - Warning Labels - MSDS
EATING, DRINKING, SMOKING, APPLYING COSMETICS OR LIP BALM AND HANDLING CONTACT LENSES IS PROHIBITED IN WORK AREAS WHERE
THERE IS POTENTIAL FOR BLOOD BORNE EXPOSURE
Exposure Control Plan
PREVENTION Immunizations
OSHA REQUIRES that employers make the hepatitis B vaccination series
available to employees whose have an exposure risk. If an employee refuses the hepatitis B series a
signature is required on a refusal form.
Infectious Disease Prevention Preventive vaccines Immune status verification (titer) Testing (Tuberculin - PPD)

Exposure Control Plan
Post Exposure Personal hygiene practices
Immediately & thoroughly wash affected area Immediate verbal notification of exposure Follow-up measures within 24 hours
ENGINEERING CONTROLS Gloves, Gowns, Masks, Eye
Protection Hand washing Facilities Self Sheathing Needles Sharps Containers Specimen Containers N95 Particulate TB Masks
Engineering Controls
CLEANING SCHEDULE Equipment that contacts mucous membranes: 10:1 Bleach
Solution with warm water, then EPA Registered Sterilant Equipment with VISIBLE Blood or Body Fluids: 10:1 Bleach
solution, then EPA Registered Germicide with Tuberculocidal Properties
Surface or Equipment without Visible blood or fluids: 1/4 cup bleach to 1 gallon of water
Laundry In house of Out of house
Body Substance Isolation
Protects the First Responder and Patient Assumes all body substances are infectious Procedures set by OSHA and local policy
Body Substance Isolation
Wash hands thoroughly, even if gloves were used.
Body Substance Isolation Wear latex, vinyl or synthetic gloves Use Protective eyewear Gowns protect clothing from fluid splatter Mask / eye shield combination offers
protection from fluid splatter
Body Substance Isolation NIOSH-approved respirators designed to
protect caregivers against air-borne pathogens
Workplace Practices
UNIVERSAL PRECAUTIONS Treat all human body fluids as if they are known to be
infectious Assume that all patients have disease Use Standard Precautions (Body Substance Isolation)
Workplace Practices
Hand washing Cleaning &
Decontamination of Spills
Cleaning & Disinfecting of Equipment & Surfaces
Infectious Waste Clothing PPE Needles & Sharps
Containers
Workplace Practices
Wash hands and any exposed skin with regular soap and Hot H20 ASAP after removal of PPE or following any contact of body areas with blood or other infectious materials
Flush Mucous Membranes with H20
Never bend or recap Contaminated Needles
Workplace Practices
Gloves Gowns Masks Pocket Masks Face Protection
Personal Protective Equipment
Scene Safety
Scene Size Up Five (5) Key Points
Scene Safety Location Mechanism of Injury / Nature of Illness. Number of Victims / Bystanders Resources Available
Scene Safety
Scene Size-up An ongoing process A very fluid process Approach with CAUTION
Scene Safety
IS IT SAFE TO APPROACH THE PATIENT? Motor Vehicle Accidents (MVAs) Hazardous materials Unstable Structures or Surfaces Traffic / Vehicles Violence / Crime Scene Environmental Considerations Bystander Behavior
Scene Safety Establishing a Danger Zone
No apparent hazards 50 feet in all directions
Spilled fuel Minimum 100 feet in all directions
Collision vehicle on fire At least 100 feet in all directions
Hazardous materials 50 – 2,000 feet Uphill / upwind

Scene Safety
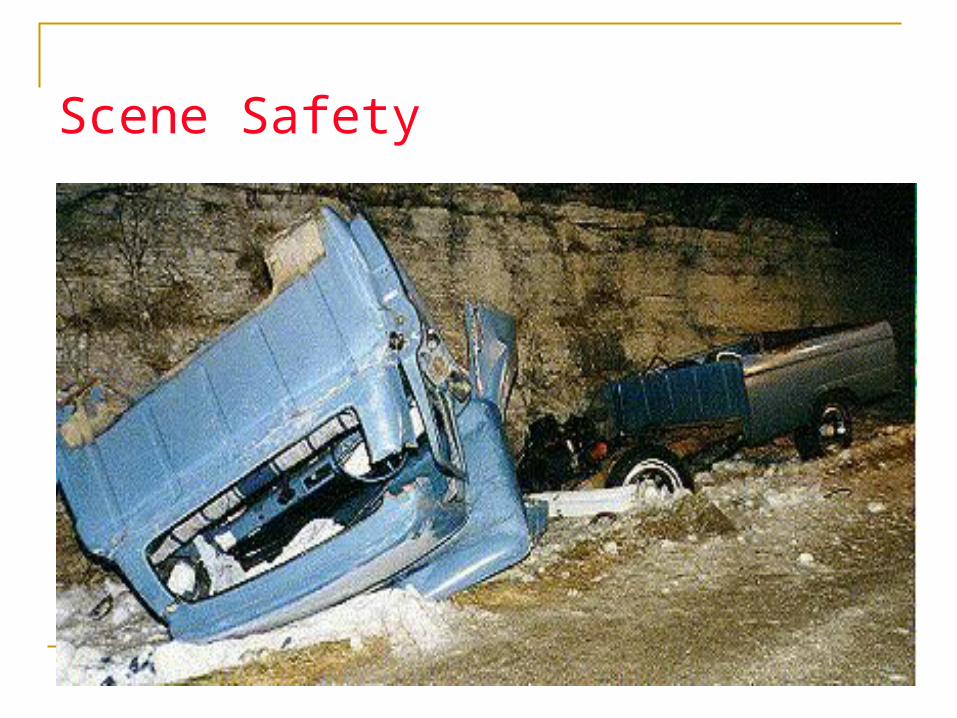
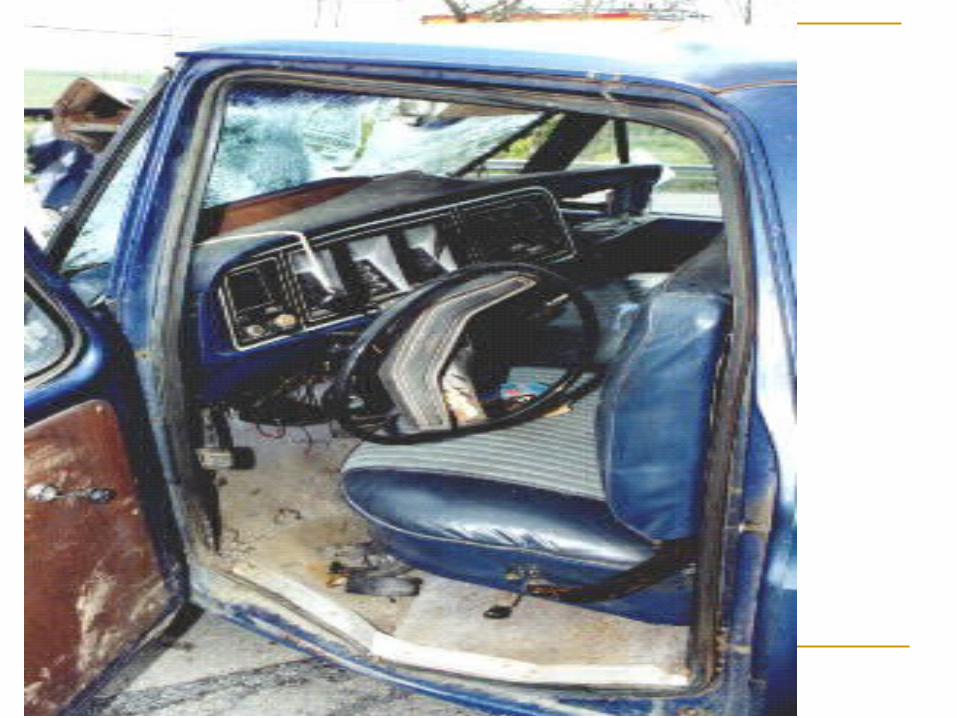
Motor Vehicle Accidents (MVAs) Identify Threats
Electricity Fire, Gas, Smoke Explosion Hazardous Materials (Placards) Traffic Unstable Vehicle
Scene Safety
Scene Safety
Hazardous materials Is Identification of Hazard Possible? Dos and Don’ts
Up Wind / Up Hill Don’t rely on Placards
Only enter scene SAFE Placards

Scene Assessment
Scene Assessment

Scene Safety
Unstable Structures or Surfaces Debris Falling glass Slick surfaces Power (electric / gas) Structural stability itself Blocked Passageways

Scene Safety
Traffic / Vehicles Speed Traffic volume Airbag Fuel
Scene Safety
Violence / Crime Scenes Don’t enter if
Fighting or loud voices Signs of alcohol or drug abuse Knowledge of prior violence
Always let law enforcement control violent and potential violent scenes
If scene is safe Do Not disturb anything Maintain a chain of evidence
Hazards – people, guns, knives, broken bottles
Scene Safety
Environmental Considerations Fire Animals
Dogs, Snakes Water Ice Wind Lightning
Scene Safety
Bystander Behavior Body language Language
Multiple Victims
Scene Safety
Personal Safety GET HELP Take Time to Evaluate the Scene Wear Appropriate PPE Take BSI precautions DO NOT attempt to do anything you are not
trained to do

Scene Safety
Scenes are dynamic and every changing Be aware of your surroundings Never let your means of egress be blocked Watch people If a scene becomes hostile or unsafe
LEAVE
Always, Always Remember -
What you don’t see can hurt you, the patient, or the
bystanders.
Starts With YouBe Aware of Your Scene At All Times
Scene Safety
Scene Safety
Scene Size Up Five (5) Key Points
Scene Safety Location Mechanism of Injury / Nature of Illness. Number of Victims / Bystanders Resources Available