Embed Size (px)
Citation preview

WelcomeWelcomeWelcomeWelcome

DVT Prophylaxis in DVT Prophylaxis in Orthopaedic SurgeryOrthopaedic Surgery
Symposium, American Academy of OrthopedicSymposium, American Academy of OrthopedicSurgeons, Annual Meeting, San Diego, CaliforniaSurgeons, Annual Meeting, San Diego, California
February 14, 2007February 14, 2007

Javad Parvizi, MD, FRCSJavad Parvizi, MD, FRCSAssociate ProfessorAssociate ProfessorDepartment of OrthopedicsDepartment of OrthopedicsThomas Jefferson UniversityThomas Jefferson UniversityRothman InstituteRothman InstitutePhiladelphia, PAPhiladelphia, PA
Peter B. Hanson, MDPeter B. Hanson, MDMedical Director of OrthopedicsMedical Director of OrthopedicsChief of StaffChief of StaffGrossmont HospitalGrossmont HospitalLa Mesa, CALa Mesa, CA
Russell Hull, MBBS, MScRussell Hull, MBBS, MScProfessor of MedicineProfessor of MedicineDirector, Thrombosis Research UnitDirector, Thrombosis Research UnitUniversity of CalgaryUniversity of CalgaryCalgary, AlbertaCalgary, AlbertaCanadaCanada
Program FacultyProgram Faculty
Eugene R Viscusi, MDEugene R Viscusi, MDDirector, Acute Pain ManagementDirector, Acute Pain ManagementAssociate ProfessorAssociate ProfessorDepartment of AnesthesiologyDepartment of AnesthesiologyThomas Jefferson UniversityThomas Jefferson UniversityPhiladelphia, PAPhiladelphia, PA
Paul F. Lachiewicz, MDPaul F. Lachiewicz, MDDepartment of OrthopaedicsDepartment of OrthopaedicsUniversity of North Carolina School of University of North Carolina School of MedicineMedicineChapel Hill, NCChapel Hill, NC

Financial DisclosuresFinancial Disclosures
Javad Parvizi, MD, FRCSJavad Parvizi, MD, FRCSGrant/Research Support: Grant/Research Support: NIH, OREF, NIH, OREF, DOD, Aircast, GSK, Ortho McNeill, DOD, Aircast, GSK, Ortho McNeill, Pfizer, Smith and Nephew, StrykerPfizer, Smith and Nephew, StrykerConsultant: Consultant: Stryker OrthopaedicsStryker OrthopaedicsSpeaker’s Bureau: Speaker’s Bureau: EndoEndo
Peter B. Hanson, MDPeter B. Hanson, MDSpeaker’s Bureau: Speaker’s Bureau: Eisai, sanofi-Eisai, sanofi-aventis, Bristol-Myers Squibbaventis, Bristol-Myers Squibb
Russell Hull, MBBS, MScRussell Hull, MBBS, MScGrant/Research Support: Grant/Research Support: sanofi-sanofi-aventis, Bayeraventis, BayerConsultant: Consultant: sanofi-aventis, Wyeth, sanofi-aventis, Wyeth, GSK, Leo Pharmaceuticals, Pfizer, GSK, Leo Pharmaceuticals, Pfizer, BayerBayer
Eugene R Viscusi, MDEugene R Viscusi, MDResearch Support: Research Support: Ortho-McNeil Ortho-McNeil Pharmaceutical, Inc., Endo Pharmaceutical, Inc., Endo Pharmaceuticals, SkyePharma, Pfizer Pharmaceuticals, SkyePharma, Pfizer Inc, Xsira Pharmaceuticals, Baxter Inc, Xsira Pharmaceuticals, Baxter Pharmaceutical Products, Inc., and Pharmaceutical Products, Inc., and Progenics Pharmaceuticals, Inc.Progenics Pharmaceuticals, Inc. Consultant: Consultant: Ortho-McNeil Ortho-McNeil Pharmaceutical, Inc., Adolor Pharmaceutical, Inc., Adolor Corporation, Endo and SkyePharmaCorporation, Endo and SkyePharma Speaker’s Bureau: Speaker’s Bureau: EndoEndo
Paul F. Lachiewicz, MDPaul F. Lachiewicz, MDConsultant: Consultant: Zimmer, EndoZimmer, EndoResearch Grant: Research Grant: AircastAircast

Educational ObjectivesEducational Objectives
► Learn how to explain current guidelines issued by national Learn how to explain current guidelines issued by national professional organizations and colleges, such as the AAOS, professional organizations and colleges, such as the AAOS, ACCP, and ASA, mandating risk-directed prophylaxis against DVT ACCP, and ASA, mandating risk-directed prophylaxis against DVT in low-to-high risk patients undergoing orthopedic surgery.in low-to-high risk patients undergoing orthopedic surgery.
► Learn how to identify factors to risk stratify orthopedic surgery Learn how to identify factors to risk stratify orthopedic surgery patients undergoing THA, TKA, fracture repair, to assess their patients undergoing THA, TKA, fracture repair, to assess their likelihood for incurring DVT.likelihood for incurring DVT.
► Learn how to describe pharmacologic and/or intermittent Learn how to describe pharmacologic and/or intermittent compression devices as part of a multimodal prophylaxis compression devices as part of a multimodal prophylaxis strategy aimed at the incidence of DVT in the OS patient strategy aimed at the incidence of DVT in the OS patient population.population.
► Learn how to specify pharmacologic agents used for DVT Learn how to specify pharmacologic agents used for DVT prophylaxis based on an analysis of efficacy, safety, and prophylaxis based on an analysis of efficacy, safety, and pharmacoeconomic parameters.pharmacoeconomic parameters.

► Learn to discuss the special anesthesiological needs of Learn to discuss the special anesthesiological needs of OS patients at risk for DVT, with a focus on timing of OS patients at risk for DVT, with a focus on timing of prophylaxis, transitioning agents, and duration of prophylaxis, transitioning agents, and duration of prophylaxis based on the surgical procedure.prophylaxis based on the surgical procedure.
► Describe how to risk stratify patients undergoing Describe how to risk stratify patients undergoing orthopedic surgery, and implement ACCP-mandated orthopedic surgery, and implement ACCP-mandated pharmacologic and non-pharmacologic measures aimed pharmacologic and non-pharmacologic measures aimed at DVT prophylaxis.at DVT prophylaxis.
► Learn how to apply landmark clinical trials focusing on Learn how to apply landmark clinical trials focusing on DVT prevention in OS patients.DVT prevention in OS patients.
Educational ObjectivesEducational Objectives

DVT Prophylaxis After TJADVT Prophylaxis After TJAImportanceImportance
►Catastrophic Catastrophic cardiopulmonary problemcardiopulmonary problem
DeathDeath

► Orthopedic procedures Orthopedic procedures are high riskare high risk
DVT Prophylaxis After TJADVT Prophylaxis After TJAImportanceImportance

► Learn current guidelinesLearn current guidelines(ACCP, AAOS)(ACCP, AAOS)
► Stratify orthopedic surgery Stratify orthopedic surgery patientspatients
► How to apply various modalitiesHow to apply various modalities
DVT Prophylaxis After TJADVT Prophylaxis After TJAObjectivesObjectives

► Pharmacologic agentsPharmacologic agents Unfractionated heparinUnfractionated heparin LMWH LMWH CoumadinCoumadin AspirinAspirin
► Mechanical Mechanical ► MultimodalMultimodal
DVT Prophylaxis After TJADVT Prophylaxis After TJAObjectivesObjectives

► Select pharmacologic agents Select pharmacologic agents based on efficacy, safety, based on efficacy, safety, pharmacoeconomic parameterspharmacoeconomic parameters
► Issues related to Issues related to coadministration of anesthesia coadministration of anesthesia and DVT prophylaxisand DVT prophylaxis
DVT Prophylaxis After TJADVT Prophylaxis After TJAObjectivesObjectives

►Four 20 minutes talkFour 20 minutes talk
►DiscussionDiscussion
DVT Prophylaxis After TJADVT Prophylaxis After TJAFormatFormat

Russell Hull MBBS, MScRussell Hull MBBS, MScProfessor of Medicine, Director,Professor of Medicine, Director,Thrombosis Research Unit,Thrombosis Research Unit,University of CalgaryUniversity of Calgary
► Current guidelines (ACCP)Current guidelines (ACCP)
► Risk stratificationRisk stratification
DVT Prophylaxis After TJADVT Prophylaxis After TJAFirst TalkFirst Talk

Peter Hanson, MDPeter Hanson, MDMedical Director of Orthopedics,Medical Director of Orthopedics,Chief of StaffChief of StaffGrossmont Hospital, La Mesa, CAGrossmont Hospital, La Mesa, CA
► Current controversiesCurrent controversies
► Agent selectionAgent selection
► Duration of prophylaxisDuration of prophylaxis
DVT Prophylaxis After TJADVT Prophylaxis After TJASecond TalkSecond Talk

Paul Lachiewicz MDPaul Lachiewicz MDProfessor of Orthopedic Surgery,Professor of Orthopedic Surgery,University of North Carolina School of University of North Carolina School of Medicine, Chapel Hill, NCMedicine, Chapel Hill, NC
►Multimodal approachMultimodal approach
►Evidence basedEvidence based
►Clinical implications of prophylaxisClinical implications of prophylaxis
DVT Prophylaxis After TJADVT Prophylaxis After TJAThird TalkThird Talk

Eugene Viscusi MDEugene Viscusi MDDirector of Acute Pain,Director of Acute Pain,Department of AnesthesiaDepartment of AnesthesiaThomas Jefferson University,Thomas Jefferson University,Philadelphia, PAPhiladelphia, PA
► Challenges of coadministration of DVT Challenges of coadministration of DVT prophylaxis and anesthesiaprophylaxis and anesthesia
DVT Prophylaxis After TJADVT Prophylaxis After TJAFinal TalkFinal Talk

Applying The Science of DVT Applying The Science of DVT Prophylaxis to Orthopedic SurgeryProphylaxis to Orthopedic Surgery
Javad Parvizi MD, FRCSJavad Parvizi MD, FRCS
Rothman Institute of Orthopedics, Rothman Institute of Orthopedics, Thomas Jefferson University Thomas Jefferson University
Philadelphia, PAPhiladelphia, PA

►Pubmed; MesH heading Pubmed; MesH heading ‘DVT’ and ‘THA’‘DVT’ and ‘THA’
29,714 articles29,714 articles
DVT Prophylaxis After THADVT Prophylaxis After THALiteratureLiterature

►HistoricHistoric 1 - 2%1 - 2%
►CurrentCurrent 0.1 - 0.2%0.1 - 0.2%
Fatal P.E.Fatal P.E.
DVT Prophylaxis After THADVT Prophylaxis After THAImportanceImportance

► In many cases the In many cases the complication is preventablecomplication is preventable
► We (not the internists) are We (not the internists) are responsible for choosing and responsible for choosing and administering prophylaxis administering prophylaxis
DVT Prophylaxis After THADVT Prophylaxis After THAImportanceImportance

► What agent?What agent?
► How longHow long
► ScreeningScreening
DVT Prophylaxis After THADVT Prophylaxis After THAIntroductionIntroduction

Data Difficult to Interpret:Data Difficult to Interpret:► Different methods of diagnosisDifferent methods of diagnosis
clinicalclinical - ultrasound - ultrasound venographyvenography - scans - scans
► Different endpointsDifferent endpoints deathdeath - DVT proximal vs distal - DVT proximal vs distal clinical PE or DVTclinical PE or DVT
► Different definitions of complicationsDifferent definitions of complications bleeding: major, minorbleeding: major, minor post phlebitic syndromepost phlebitic syndrome
DVT Prophylaxis After THADVT Prophylaxis After THAIntroductionIntroduction

DVT Prophylaxis After THADVT Prophylaxis After THAProphylaxis: NoProphylaxis: No
Warwick, JBJS, Br, 1995Warwick, JBJS, Br, 1995► 1162 THA1162 THA► No chemical prophylaxisNo chemical prophylaxis► Fatal PE 0.34%Fatal PE 0.34%
Murray et al, JBJS Br, 1996Murray et al, JBJS Br, 1996► Meta-analysisMeta-analysis► 130,000 THA130,000 THA► Reported fatal PE 0.1 - 0.2%Reported fatal PE 0.1 - 0.2%

““Effective prophylaxis is Effective prophylaxis is necessary in these patients necessary in these patients
[THA, TKA] . . .”[THA, TKA] . . .”► NIH consensus panel, 1986NIH consensus panel, 1986► European consensus European consensus
conference 1992conference 1992
DVT Prophylaxis After THADVT Prophylaxis After THAProphylaxis: YesProphylaxis: Yes

► In 2007 in North America In 2007 in North America we are obligated to do we are obligated to do somethingsomething
King obtains $1.5M settlement for husband and children in pulmonary embolism deathSeptember 14, 2004 | Massachusetts Lawyers Weekly: Verdicts & Settlements
DVT Prophylaxis After THADVT Prophylaxis After THA

DVT Prophylaxis After THADVT Prophylaxis After THAAgents AvailableAgents Available
►Unfractionated heparinUnfractionated heparin►LMWHLMWH►AspirinAspirin►Mechanical prophylaxisMechanical prophylaxis

DVT Prophylaxis After THADVT Prophylaxis After THALMWHLMWH
Advantages:Advantages:► Predictable dose responsePredictable dose response► Proven efficacyProven efficacy
Disadvantages:Disadvantages:► Bleeding complicationsBleeding complications► Injection requiredInjection required

DVT Prophylaxis After THADVT Prophylaxis After THALMWH: ResultsLMWH: Results
►LMWH BIDLMWH BID
►194 THA194 THA
►DVT rate 5%DVT rate 5%
►8 major bleeding episodes8 major bleeding episodes
Colwell et al, JBJS Am, 1994

DVT Prophylaxis After THADVT Prophylaxis After THAWarfarin vs. LMWHWarfarin vs. LMWH
► Prospective, randomizedProspective, randomized► Venography endpointVenography endpoint► LMWH started 2 hrs postopLMWH started 2 hrs postop► Proximal DVT 5% (LMWH) vs 8% Proximal DVT 5% (LMWH) vs 8%
(Warfarin), p = 0.19(Warfarin), p = 0.19► More bleeding in LMWH group More bleeding in LMWH group
(p=0.001)(p=0.001)
Francis, et al: JBJS (A), 1995

DVT Prophylaxis After THADVT Prophylaxis After THALMWHLMWH
► Randomized, double blindRandomized, double blind
► 1472 THA1472 THA
► Dalteparin before or early after vs warfarinDalteparin before or early after vs warfarin
► Venogram detected DVTVenogram detected DVT
► Symptomatic thrombi less frequent in Symptomatic thrombi less frequent in preop dalteparin group (p<0.02)preop dalteparin group (p<0.02)
► Increased bleeding at surgical site for Increased bleeding at surgical site for preop dalteparin grouppreop dalteparin group
► Modified regimen (postoperative) Modified regimen (postoperative)
Hull R et al: Arch Intern Med. 2000

Bottom Line:Bottom Line:►EffectiveEffective►2nd most commonly used 2nd most commonly used
agent in N. Americaagent in N. America►Probably increased bleed Probably increased bleed
risk esp. if given too earlyrisk esp. if given too early
DVT Prophylaxis After THADVT Prophylaxis After THALMWHLMWH

► Coumadin and LMWH equally Coumadin and LMWH equally effective at preventing DVT effective at preventing DVT after THAafter THA
► A slightly higher bleeding rate A slightly higher bleeding rate with LMWHwith LMWH
► Coumadin is harder to use Coumadin is harder to use (outpatient monitoring)(outpatient monitoring)
DVT Prophylaxis After THADVT Prophylaxis After THAResults: SummaryResults: Summary

DVT Prophylaxis After THADVT Prophylaxis After THAPreventative MeasuresPreventative Measures
► Expeditious surgeryExpeditious surgery
► Minimize time vessels kinked in surgeryMinimize time vessels kinked in surgery
► Mobilize promptlyMobilize promptly
► Calf exercises in bedCalf exercises in bed
► Elastic stockings (?)Elastic stockings (?)
► Epidural anesthesiaEpidural anesthesia
Lemos, Clin. Orth. 1992Lemos, Clin. Orth. 1992

DVT Prophylaxis After THADVT Prophylaxis After THAProphylaxis OptionsProphylaxis Options
What is the best What is the best agent for agent for
prophylaxis?prophylaxis?

► 434 surgeons representing 48 434 surgeons representing 48 states and three countries states and three countries (Canada, Egypt, Pakistan)(Canada, Egypt, Pakistan)
► Surgeons have been in Surgeons have been in practice an average of 19 yearspractice an average of 19 years
► >96% prophylax for DVT in >96% prophylax for DVT in their THA and TKA patientstheir THA and TKA patients
OREF SurveyOREF Survey

OREF SurveyOREF Survey

DVT Prophylaxis After THADVT Prophylaxis After THAWhich LMWHWhich LMWH
► Certoparin (18 mg), dalteparin 30 mg, Certoparin (18 mg), dalteparin 30 mg, enoxaparin (24 mg)enoxaparin (24 mg)
► 188 patients undergoing TJA, or spine sx188 patients undergoing TJA, or spine sx► Changes in venous flow pre and postop Changes in venous flow pre and postop
dopplerdoppler► DVT= 1.1%DVT= 1.1%► Bleeding = 11.2% (13 in certoparin, 4 in each)Bleeding = 11.2% (13 in certoparin, 4 in each)► No difference in APTT, TCT, blood countNo difference in APTT, TCT, blood count► All as efficaciousAll as efficacious
Janni W, et al.Janni W, et al.Zentralbl Chir.Zentralbl Chir. 2001 2001

DVT Prophylaxis After THADVT Prophylaxis After THASummarySummary
►Proven efficacyProven efficacy►Works for youWorks for you

DVT Prophylaxis After THADVT Prophylaxis After THADuration of ProphylaxisDuration of Prophylaxis
How long should How long should prophylaxis beprophylaxis be
continued after THA?continued after THA?

►LMWHLMWH Conflicting dataConflicting data
►WarfarinWarfarin Amstutz: 15 days Amstutz: 15 days Colwell: 7 daysColwell: 7 days
DVT Prophylaxis After THADVT Prophylaxis After THADuration of ProphylaxisDuration of Prophylaxis

DVT Prophylaxis After THADVT Prophylaxis After THALMWHLMWH
► Randomized, double blindRandomized, double blind► 569 THA569 THA► dalteparin vs warfarin in hospital and dalteparin vs warfarin in hospital and
placebo out of hospital (35 days)placebo out of hospital (35 days)► Venogram preop and postopVenogram preop and postop► Proximal DVT significantly higher in Proximal DVT significantly higher in
warfarin/placebo group warfarin/placebo group ► No major bleedingNo major bleeding
Hull R et al: Hull R et al: Arch Intern Med.Arch Intern Med. 2000 2000

DVT Prophylaxis After THADVT Prophylaxis After THADuration of ProphylaxisDuration of Prophylaxis
► Markov-based decision analysisMarkov-based decision analysis► Outcome measures: PE prevented, Outcome measures: PE prevented,
hemorrhages induced, overall cost, overall hemorrhages induced, overall cost, overall cost for each PE preventedcost for each PE prevented
► Agents: LMWH, warfarin, ASA, nothingAgents: LMWH, warfarin, ASA, nothing► Extending to 4 weeks was safe for all agentsExtending to 4 weeks was safe for all agents► LMWH-most effectiveLMWH-most effective► ASA-most cost effectiveASA-most cost effective► Conclusion: Safe to extend the prophylaxis to Conclusion: Safe to extend the prophylaxis to
4 but 4 but NOTNOT 6 weeks 6 weeks
Sarasin FP, Bounameaux H.Sarasin FP, Bounameaux H.Thromb HaemostThromb Haemost 2002 2002

►Patients with no specific risk Patients with no specific risk factors (1-3 weeks)factors (1-3 weeks)
►Patients with specific risk Patients with specific risk factor (6 weeks) (like factor (6 weeks) (like previous DVT)previous DVT)
DVT Prophylaxis After THADVT Prophylaxis After THADuration of ProphylaxisDuration of Prophylaxis

DVT Prophylaxis After THADVT Prophylaxis After THAScreeningScreening
► Do patients need Do patients need
routine screening routine screening
for DVT after THA?for DVT after THA?

Advantages:Advantages:► Identify and treat clotsIdentify and treat clots
Disadvantages:Disadvantages:► Accuracy of tests variesAccuracy of tests varies► Problem of treating asymptomatic clotsProblem of treating asymptomatic clots► Unproven advantageUnproven advantage► CostCost
DVT Prophylaxis After THADVT Prophylaxis After THAScreeningScreening

► A large prospective randomized A large prospective randomized trial comparing discharge trial comparing discharge ultrasound with sham ultrasound ultrasound with sham ultrasound showed showed NONO advantage to advantage to screeningscreening
DVT Prophylaxis After THADVT Prophylaxis After THAScreeningScreening
Robinson, KS et al. Robinson, KS et al. Ann Intern MedAnn Intern Med. 1997 Sep 15;127(6):439-45. 1997 Sep 15;127(6):439-45 Robinson, KS et al. Robinson, KS et al. Ann Intern MedAnn Intern Med. 1997 Sep 15;127(6):439-45. 1997 Sep 15;127(6):439-45

►““Good judgment Good judgment comes from experience comes from experience and experience comes and experience comes from bad judgment”from bad judgment”
Winston ChurchillWinston Churchill

Russell D. HullRussell D. HullProfessor of Medicine,Thrombosis Research Unit Professor of Medicine,Thrombosis Research Unit
University of CalgaryUniversity of Calgary
Current Guidelines for DeepCurrent Guidelines for DeepVein Thrombosis Prophylaxis in Vein Thrombosis Prophylaxis in
Orthopedic Surgery: ACCP GuidanceOrthopedic Surgery: ACCP Guidanceand Risk Stratification Strategies – and Risk Stratification Strategies – Matching Intensity of Therapy with Matching Intensity of Therapy with
Patient SubgroupsPatient Subgroups

Diagnosis Of Fatal Pulmonary Embolism In North Diagnosis Of Fatal Pulmonary Embolism In North America Is Problematic Due To The Low Autopsy RateAmerica Is Problematic Due To The Low Autopsy Rate

Evidence-Based Guidelines Evidence-Based Guidelines RecommendationsRecommendations
Two Components:Two Components:
► Benefit/RiskBenefit/Risk
► Methodological Quality of a RecommendationMethodological Quality of a Recommendation
The 7th ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest 2004; 126: 179S-187S.
•Grade 1Grade 1
•Grade AGrade A•Grade BGrade B
•Grade CGrade COrOr
OrOr•Grade 2Grade 2

Methodologic QualityMethodologic Quality
Grade AGrade AConsistentConsistent findings by randomized trials findings by randomized trials
Grade BGrade BRandomized clinical trials with Randomized clinical trials with inconsistentinconsistent resultsresults
Grade CGrade CObservational studiesObservational studies
Chest 2004; 126: 179S-187S.

Benefit/RiskBenefit/RiskBenefit/RiskBenefit/Risk
Grade 1Grade 1If we are very certain that the benefits do, or do If we are very certain that the benefits do, or do not, outweigh the risks, burdens, and cost, we not, outweigh the risks, burdens, and cost, we make a strong recommendation (in our make a strong recommendation (in our formulation, formulation, Grade 1Grade 1))
Grade 2Grade 2If we are less certain of the magnitude of the If we are less certain of the magnitude of the benefits and the risks, burdens, and costs, and benefits and the risks, burdens, and costs, and thus of their relative impact, we make a weaker thus of their relative impact, we make a weaker Grade 2Grade 2 recommendations recommendations
Chest 2004; 126: 179S-187S.

Thromboprophylaxis RegimensThromboprophylaxis Regimens
► Mechanical
• Graduated Compression Stockings (GCS)
• Intermittent Pneumatic Compression (IPC)
► Anticoagulants
• Low-Dose Unfractionated Heparin (LDUH)
• Low-Molecular-Weight Heparin (LMWH/fondaparinux)
• Vitamin-K-Antagonists (VKA)
Chest 2004; 126: 179S-187S.

We recommend against the use of We recommend against the use of
ASA alone as prophylaxis ASA alone as prophylaxis againstagainst
VTE for any patient group VTE for any patient group
(Grade 1A)(Grade 1A)
ASAASA
Chest 2004; 126: 179S-187S.

Antiplatelets:Antiplatelets:Antiplatelets:Antiplatelets:
-ASA-ASA-ASA-ASAXX

We recommend against the routine
use of DUS screening at the time of
hospital discharge in asymptomatic
patients following major orthopedic
surgery (Grade 1A)
We recommend against the routine
use of DUS screening at the time of
hospital discharge in asymptomatic
patients following major orthopedic
surgery (Grade 1A)
Screening for DVTScreening for DVT
Chest 2004; 126: 338S-400S.

Levels of Thromboembolism Risk in Surgical Levels of Thromboembolism Risk in Surgical Patients Without ProphylaxisPatients Without Prophylaxis
Patients are stratified as:Patients are stratified as:
► Low RiskLow Risk
► Moderate RiskModerate Risk
► High RiskHigh Risk
► Highest RiskHighest Risk
Risk StratificationRisk Stratification
Chest 2004; 126: 338S-400S.

CalfCalf ProximalProximal
DVT, %DVT, % PE, %PE, %
ClinicalClinical FatalFatal
High RiskHigh Risk
Surgery in patients with multiple risk factors (age >40 yr, cancer prior VTE)
Successful Prevention Strategies:
40-80 10-20 4-10 0.2-5
Hip or knee arthroplasty, HFS
Major trauma; SCI
Chest 2004; 126: 338S-400S.
LMWH (>3,400 U daily), fondaparinux, oral VKAs (INR, 2-3), or IPC/GCS + LDUH/LMWH

Orthopaedic SurgeryOrthopaedic Surgery

Highest riskHighest risk
Elective Hip SurgeryElective Hip Surgery

Elective Hip ArthroplastyElective Hip ArthroplastyElective Hip ArthroplastyElective Hip Arthroplasty
For patients undergoing elective THR, we For patients undergoing elective THR, we recommend the routine use of one of the following recommend the routine use of one of the following three anticoagulants:three anticoagulants:
► LMWH (at a usual high-risk dose, started 12 h before LMWH (at a usual high-risk dose, started 12 h before surgery or 12 to 24 h after surgery, or 4 to 6 h after surgery or 12 to 24 h after surgery, or 4 to 6 h after surgery at half the usual high-risk dose and then surgery at half the usual high-risk dose and then increasing to the usual high-risk dose the following day)increasing to the usual high-risk dose the following day)
► fondaparinux, (2.5 mg started 6 to 8h after surgery)fondaparinux, (2.5 mg started 6 to 8h after surgery)
► Adjusted-dose VKA started preoperatively or the Adjusted-dose VKA started preoperatively or the evening after surgery (INR target, 2.5; INR range, evening after surgery (INR target, 2.5; INR range, 2.0 to 3.0) [all 2.0 to 3.0) [all Grade 1AGrade 1A]]
Chest 2004; 126: 338S-400S.

We recommend We recommend against against the use of:the use of:
As the only method of thromboprophylaxis in these As the only method of thromboprophylaxis in these
patients patients ((Grade 1AGrade 1A))
► ASAASA► DextranDextran► Low-dose unfractionated heparinLow-dose unfractionated heparin► Graduated compression stockingsGraduated compression stockings► Intermittent pneumatic compressionIntermittent pneumatic compression► Venous foot pumpVenous foot pump
Elective Hip ArthroplastyElective Hip ArthroplastyElective Hip ArthroplastyElective Hip Arthroplasty
Chest 2004; 126: 338S-400S.

Underlying values and preferencesUnderlying values and preferences
We have not recommended the use of:We have not recommended the use of:
► fondaparinux over LMWH and VKAfondaparinux over LMWH and VKA► Or the use of LMWH over VKAOr the use of LMWH over VKA
Because we place a relatively Because we place a relatively low value low value on the on the
prevention of venographic thrombosis and a prevention of venographic thrombosis and a
relatively relatively high valuehigh value on minimizing bleeding on minimizing bleeding
complicationscomplications
Elective Hip ArthroplastyElective Hip ArthroplastyElective Hip ArthroplastyElective Hip Arthroplasty
Chest 2004; 126: 338S-400S.

Elective Knee SurgeryElective Knee SurgeryElective Knee SurgeryElective Knee Surgery
Highest riskHighest riskHighest riskHighest risk

For patients undergoing elective TKA, we For patients undergoing elective TKA, we
recommend routine thromboprophylaxis using:recommend routine thromboprophylaxis using:► LMWH (at the usual high-risk dose)LMWH (at the usual high-risk dose)
► FondaparinuxFondaparinux
► Adjusted-dose VKA (target INR, 2.5; INR range,Adjusted-dose VKA (target INR, 2.5; INR range,
2.0 to 3.0) 2.0 to 3.0)
all Grade 1Aall Grade 1A
Elective Knee ArthroplastyElective Knee Arthroplasty
Chest 2004; 126: 338S-400S.

► The optimal use of IPC is an alternative option to The optimal use of IPC is an alternative option to
anticoagulant prophylaxis anticoagulant prophylaxis ((Grade 1BGrade 1B))► We recommend We recommend against against the use of any of the the use of any of the
following as sole methods of thromboprophylaxis:following as sole methods of thromboprophylaxis:• ASA ASA ((Grade 1AGrade 1A) ) • LDUH LDUH ((Grade 1AGrade 1A) ) • Or venous foot pump Or venous foot pump (Grade 1B)(Grade 1B)
Elective Knee ArthroplastyElective Knee Arthroplasty
Chest 2004; 126: 338S-400S.

Underlying values and preferencesUnderlying values and preferences
We have not recommended:We have not recommended:► fondaparinux over LMWH and VKAfondaparinux over LMWH and VKA► Or LMWH over VKAOr LMWH over VKA
Because we place a relatively Because we place a relatively low valuelow value on the on the
prevention of venographic thrombosis and a relatively prevention of venographic thrombosis and a relatively
high valuehigh value on minimizing bleeding complications on minimizing bleeding complications
Elective Knee ArthroplastyElective Knee Arthroplasty
Chest 2004; 126: 338S-400S.

Hip Fracture SurgeryHip Fracture Surgery
Highest riskHighest risk

For patients undergoing hip fracture surgery, we For patients undergoing hip fracture surgery, we
recommend the routine use of:recommend the routine use of:
► fondaparinux fondaparinux (Grade 1A)(Grade 1A)
► LMWH at the usual high-risk dose LMWH at the usual high-risk dose ((Grade 1CGrade 1C))
► Adjusted-dose VKA (target INR, 2.5; INR range,Adjusted-dose VKA (target INR, 2.5; INR range,
2.0 to 3.0) 2.0 to 3.0) (Grade 2B)(Grade 2B)
► Or LDUH Or LDUH (Grade 1B)(Grade 1B)
Hip Fracture SurgeryHip Fracture Surgery
Chest 2004; 126: 338S-400S.

► We recommend We recommend againstagainst the use of ASA the use of ASA alone alone (Grade 1A)(Grade 1A)
► If surgery will likely be delayed, we If surgery will likely be delayed, we recommend that prophylaxis with either recommend that prophylaxis with either LDUH or LMWH be initiated during the LDUH or LMWH be initiated during the time between hospital admission and time between hospital admission and surgery surgery (Grade 1C+)(Grade 1C+)
► We recommend mechanical prophylaxis if We recommend mechanical prophylaxis if anticoagulant prophylaxis is anticoagulant prophylaxis is contraindicated because of a high risk of contraindicated because of a high risk of bleeding bleeding (Grade 1C)(Grade 1C)
Hip Fracture SurgeryHip Fracture Surgery
Chest 2004; 126: 338S-400S.

Distal Fracture ofDistal Fracture ofthe Lower Extremitythe Lower Extremity

We suggest that clinicians We suggest that clinicians notnot use use
thromboprophylaxis routinely in patients with thromboprophylaxis routinely in patients with
isolated lower extremity injuries isolated lower extremity injuries (Grade 2A)(Grade 2A)
Isolated Lower Extremity InjuriesIsolated Lower Extremity Injuries
Chest 2004; 126: 338S-400S.

► Timing of ThromboprophylaxisTiming of Thromboprophylaxis
► Knee arthroscopyKnee arthroscopy
► ThrombocytopeniaThrombocytopenia
Special ConsiderationsSpecial Considerations

Timing of Timing of ThromboprophylaxisThromboprophylaxis

We performed a randomized, double-blind trial
Patients received either:► Just-in-time subcutaneous dalteparin sodium
once daily (initiated immediately pre-operatively
or early post-operatively)► Or warfarin during the acute hospital stay
North American Dalteparin Trial (NAFT)North American Dalteparin Trial (NAFT)
Hull et al. Arch Intern Med 2000; 160: 2199-2207.Hull et al. Arch Intern Med 2000; 160: 2208-2215.

Multicentre: 28 centres in the United States and Canada►Randomized
►Double-blind
NAFTNAFT
Hull et al. Arch Intern Med 2000; 160: 2199-2207.Hull et al. Arch Intern Med 2000; 160: 2208-2215.

Overall Study DesignOverall Study DesignPhase IPhase I Phase IIPhase II
Day 0Day 0 (surgery)(surgery)
Day 6Day 6±2±2
Day 7Day 7±2±2
Day 35Day 35±2±2
Pre-op DalteparinPre-op Dalteparin (2,500 IU)(2,500 IU) DalteparinDalteparin
Post-op DalteparinPost-op Dalteparin (2,500 IU)(2,500 IU) DalteparinDalteparin
WarfarinWarfarin Placebo for Placebo for WarfarinWarfarin
VenographyVenography
VenographyVenography
(5,000 IU)(5,000 IU)
(5,000 IU)(5,000 IU)
NAFTNAFT
Hull et al. Arch Intern Med 2000; 160: 2199-2207.Hull et al. Arch Intern Med 2000; 160: 2208-2215.

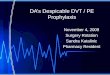
Frequency of DVT: Acute Hospital PhaseFrequency of DVT: Acute Hospital PhaseFrequency of DVT: Acute Hospital PhaseFrequency of DVT: Acute Hospital Phase
00
55
1010
1515
2020
2525
DV
T R
ate
(%
)D
VT
Ra
te (
%)
All DVTAll DVT Proximal DVTProximal DVT
Pre-operative dalteparinPre-operative dalteparin
Post-operative dalteparinPost-operative dalteparin
Combined pre- and post-Combined pre- and post-operative dalteparinoperative dalteparin
WarfarinWarfarin
► Pre-op dalteparin vs warfarin: All DVT 55% (p<0.001); Proximal DVT 72% (p=0.035)Pre-op dalteparin vs warfarin: All DVT 55% (p<0.001); Proximal DVT 72% (p=0.035)► Post-op dalteparin vs warfarin: All DVT 45% (p<0.001); Proximal DVT 72% (p=0.033)Post-op dalteparin vs warfarin: All DVT 45% (p<0.001); Proximal DVT 72% (p=0.033)► Combined pre- and post-op dalteparin vs warfarin: All DVT 50% (p<0.001); Proximal DVT Combined pre- and post-op dalteparin vs warfarin: All DVT 50% (p<0.001); Proximal DVT
72% (p=0.009)72% (p=0.009)
Relative Risk ReductionsRelative Risk Reductions
Hull et al. Arch Intern Med 2000; 160: 2199-2207.Hull et al. Arch Intern Med 2000; 160: 2208-2215.

Low-Molecular-Weight Heparin Prophylaxis Using Low-Molecular-Weight Heparin Prophylaxis Using Dalteparin in Close Proximity to Surgery Vs Warfarin Dalteparin in Close Proximity to Surgery Vs Warfarin
in Hip Arthroplasty Patients in Hip Arthroplasty Patients
► A modified dalteparin regimen in close proximityA modified dalteparin regimen in close proximity to to
surgery resulted in substantive risk reductions for all surgery resulted in substantive risk reductions for all
andand proximal deep vein thrombosis, compared with proximal deep vein thrombosis, compared with
warfarin therapywarfarin therapy
► Such findings have not been observed withSuch findings have not been observed with
low-molecular-weight heparin therapy commenced low-molecular-weight heparin therapy commenced
12 hours preoperatively or 12 to 24 hours 12 hours preoperatively or 12 to 24 hours
postoperatively vs oral anticoagulantspostoperatively vs oral anticoagulants
Hull et al. Arch Intern Med 2000; 160: 2199-2207.

► Increased majorIncreased major but not serious bleeding but not serious bleeding
occurred in patients receiving preoperativeoccurred in patients receiving preoperative
dalteparindalteparin
► Dalteparin therapy initiated postoperatively Dalteparin therapy initiated postoperatively
provided superior efficacy vs warfarin without provided superior efficacy vs warfarin without
significantly increased overt bleedingsignificantly increased overt bleeding
Low-Molecular-Weight Heparin Prophylaxis Low-Molecular-Weight Heparin Prophylaxis Using Dalteparin in Close Proximity to Surgery Using Dalteparin in Close Proximity to Surgery
Vs Warfarin in Hip Arthroplasty Patients Vs Warfarin in Hip Arthroplasty Patients
Hull et al. Arch Intern Med 2000; 160: 2199-2207.

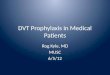
Quadratic Fit For Study Odds Ratio For DVT Vs Number Of Hours From Surgery For The First
Dose Of LMW Heparin
Quadratic Fit For Study Odds Ratio For DVT Vs Number Of Hours From Surgery For The First
Dose Of LMW Heparin
Upper and lower dashed lines indicate the 95% Upper and lower dashed lines indicate the 95% confidence interval for the true odds ratioconfidence interval for the true odds ratio
Hours from SurgeryHours from Surgery
Od
ds
Rat
ioO
dd
s R
atio
Hull et al. Arch Intern Med 2001; 161: 1952-60

Impact of Timing of Prophylaxis: Total DVT Impact of Timing of Prophylaxis: Total DVT in Patients Undergoing Elective Hip in Patients Undergoing Elective Hip
SurgerySurgery
Relative Relative RiskRisk
(95% CI*)(95% CI*)Relative Relative
RiskRiskp p
ValueValue
0.890.89
1.011.01
0.570.57
0.500.50
0.4440.444
0.9840.984
0.0080.008
<0.001<0.001
Favours LMWHFavours LMWH Favours Oral Favours Oral AnticoagulantsAnticoagulants
1.001.00 100.0100.00.100.10 10.010.0
Hull Hull (1993)(1993)
HamulyakHamulyak
FrancisFrancis
Hull Hull (2000)(2000)
StudyStudy Expt n/N (%)Expt n/N (%) Ctrl n/N (%)Ctrl n/N (%)
69/332 (20.8)69/332 (20.8)
27/195 (13.8) 27/195 (13.8)
28/192 (14.6)28/192 (14.6)
80/673 (11.8)80/673 (11.8)
79/340 (23.2)79/340 (23.2)
27/196 (13.8)27/196 (13.8)
49/190 (25.8)49/190 (25.8)
81/338 (24.0)81/338 (24.0)
Time of Time of Initiation Initiation
(hrs)(hrs)
Post:18-24Post:18-24
Pre:12 Pre:12
Pre:Pre: 2 2
Pre:Pre: 2 2Post:4-6Post:4-6
0.010.01
* CI Fixed* CI Fixed
Hull et al. Arch Intern Med 2001; 161: 1952-60

Relative Relative RiskRisk
p p ValueValue
Relative Relative RiskRisk
(95% CI*)(95% CI*)
Hull Hull (1993)(1993)
HamulyakHamulyak
FrancisFrancis
Hull Hull (2000)(2000)
StudyStudy Expt n/N (%)Expt n/N (%) Ctrl n/N (%)Ctrl n/N (%)
Time of Time of Initiation Initiation
(hrs)(hrs)
1.261.26 0.5260.526
1.001.00 100.0100.00.100.10 10.010.0
16/332 (4.8)16/332 (4.8) 13/340 (3.8)13/340 (3.8)Post:18-24Post:18-24
0.010.01
Favours LMWHFavours LMWH Favours Oral Favours Oral AnticoagulantsAnticoagulants
6/712 (0.8)6/712 (0.8)
10/192 (5.2)10/192 (5.2)
12/195 (6.2)12/195 (6.2)
11/363 (3.0)11/363 (3.0)
16/190 (8.4)16/190 (8.4)
9/196 (4.6)9/196 (4.6)
0.0110.011
0.2180.218
0.4950.495
0.280.28
0.620.62
1.341.34
Post:4-6Post:4-6Pre:Pre: 2 2
Pre:Pre: 2 2
Pre:12Pre:12
Impact of Timing of Prophylaxis: Proximal DVT in Patients Undergoing Elective Hip
Surgery
Impact of Timing of Prophylaxis: Proximal DVT in Patients Undergoing Elective Hip
Surgery
Hull et al. Arch Intern Med 2001; 161: 1952-60
* CI Fixed* CI Fixed

Timing of Initial Administration of Low-Molecular-Weight Timing of Initial Administration of Low-Molecular-Weight Heparin Prophylaxis Against Deep Vein Thrombosis in Heparin Prophylaxis Against Deep Vein Thrombosis in
Patients Following Elective Hip Arthroplasty Patients Following Elective Hip Arthroplasty
►The timing of initiating LMWH significantly The timing of initiating LMWH significantly
influences antithrombotic effectivenessinfluences antithrombotic effectiveness
►The practice of delayed initiation of LMWH The practice of delayed initiation of LMWH
prophylaxis results in suboptimal prophylaxis results in suboptimal
antithrombotic effectiveness without a antithrombotic effectiveness without a
substantive safety advantage substantive safety advantage
Hull et al. Arch Intern Med 2001; 161: 1952-60

► For major orthopedic surgical procedures, we For major orthopedic surgical procedures, we
recommend that a decision about the timing of the recommend that a decision about the timing of the
initiation of pharmacologic prophylaxis be based on initiation of pharmacologic prophylaxis be based on
the efficacy-to-bleeding tradeoffs for that particular the efficacy-to-bleeding tradeoffs for that particular
agent agent ((Grade 1AGrade 1A) ) ► For LMWH, there are only small differences between For LMWH, there are only small differences between
starting preoperatively or postoperatively, and both starting preoperatively or postoperatively, and both
options are acceptable options are acceptable ((Grade 1AGrade 1A))
Timing of ProphylaxisTiming of ProphylaxisTiming of ProphylaxisTiming of Prophylaxis
Chest 2004; 126: 338S-400S.

Dosing Options for Patients UndergoingDosing Options for Patients UndergoingHip Replacement SurgeryHip Replacement Surgery
Dosing Options for Patients UndergoingDosing Options for Patients UndergoingHip Replacement SurgeryHip Replacement Surgery
Dose of Dalteparin to be Given SubcutaneouslyDose of Dalteparin to be Given Subcutaneously
Timing of Timing of First Dose of First Dose of DalteparinDalteparin
10-14 hr10-14 hrPre-opPre-op
Within 2 hr Within 2 hr Pre-opPre-op
4-8 hr4-8 hrPost-opPost-op11
Post-op Post-op PeriodPeriod22
Post-op startPost-op start
Pre-op start-day of Pre-op start-day of surgerysurgery
Pre-op start-evening Pre-op start-evening before surgerybefore surgery44
------
------
------
------5000 IU5000 IU
2500 IU2500 IU
2500 IU2500 IU33
2500 IU2500 IU33
5000 IU5000 IU
5000 IU qd5000 IU qd
5000 IU qd5000 IU qd
5000 IU qd5000 IU qd
11 Or later, if hemostasis has not been achieved.Or later, if hemostasis has not been achieved.22 Up to 14 days of treatment was well tolerated in controlled clinical trials, where Up to 14 days of treatment was well tolerated in controlled clinical trials, where
the usual duration of treatment was 5 to 10 days postoperatively.the usual duration of treatment was 5 to 10 days postoperatively.3 3 Allow a minimum of 6 hours between this dose and the dose to be given on Allow a minimum of 6 hours between this dose and the dose to be given on
PostoperativePostoperativeDay 1. Adjust the timing of the dose on Postoperative Day 1 accordingly.Day 1. Adjust the timing of the dose on Postoperative Day 1 accordingly.
44 Allow approximately 24 hours between doses.Allow approximately 24 hours between doses.
www.fda.gov/medwatch/SAFETY/2003/03Feb_PI/Fragmin_pdf

Knee ArthroscopyKnee Arthroscopy

We suggest clinicians do We suggest clinicians do notnot use use
routine thromboprophylaxis in these routine thromboprophylaxis in these
patients, other than early patients, other than early
mobilization mobilization ((Grade 2BGrade 2B))
Knee ArthroscopyKnee Arthroscopy
Chest 2004; 126: 338S-400S.

For patients undergoing arthroscopic knee surgery For patients undergoing arthroscopic knee surgery
who are at a higher than usual risk based on:who are at a higher than usual risk based on:
► Pre existing VTE risk factorsPre existing VTE risk factors
► Or following a prolonged or complicated procedureOr following a prolonged or complicated procedure
We suggest thromboprophylaxis with LMWHWe suggest thromboprophylaxis with LMWH
((Grade 2BGrade 2B))
Knee ArthroscopyKnee Arthroscopy
Chest 2004; 126: 338S-400S.

ThrombocytopeniaThrombocytopenia
The Harbinger of Doom for Unfractionated Heparin
The Harbinger of Doom for Unfractionated Heparin

Risk for Heparin-Induced Thrombocytopenia with Risk for Heparin-Induced Thrombocytopenia with Unfractionated and Low Molecular-Weight Heparin Unfractionated and Low Molecular-Weight Heparin
Thromboprophylaxis: A Meta-AnalysisThromboprophylaxis: A Meta-Analysis
► Heparin-induced thrombocytopenia (HIT) is an Heparin-induced thrombocytopenia (HIT) is an uncommon but potentially devastating uncommon but potentially devastating complication of anticoagulation with complication of anticoagulation with unfractionated heparin (UFH) or low-molecular-unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH)weight heparin (LMWH)
► The inverse variance–weighted average that The inverse variance–weighted average that determined the absolute risk for HIT with LMWH determined the absolute risk for HIT with LMWH was 0.2%, and with UFH the risk was 2.6%. Most was 0.2%, and with UFH the risk was 2.6%. Most studies were of patients after orthopedic surgery studies were of patients after orthopedic surgery
Martel et al. Blood 2005; 106:2710-15

► VTE is associated with HIT infrequently (<1%) in
LMWH-treated patients, yet often (approximately
one in eight cases) in unfractionated heparin-
treated patients.
► Physicians should suspect the possibility of
HIT if VTE develops during or soon after
unfractionated heparin use; if
thrombocytopenia is present, alternative
anticoagulation should be used until HIT is
excluded.
Levine et al. CHEST 2006; 130(3): 681-687.
How Frequently is VTE in Heparin-Treated Patients Associated with Heparin-Induced Thrombocytopenia (HIT)

Electronic Medical Alerts — So Simple, So Complex
Electronic Medical Alerts — So Simple, So Complex
”One of the most consistent findings in
health research is the gap between
evidence and practice.”
”One of the most consistent findings in
health research is the gap between
evidence and practice.”
Durieux. N Engl J Med 2005: 352: 1034-1036 Durieux. N Engl J Med 2005: 352: 1034-1036


Appendix

ObesityObesity

The Safety of Dosing Dalteparin Based on Actual Body The Safety of Dosing Dalteparin Based on Actual Body Weight for the Treatment of Acute Venous Weight for the Treatment of Acute Venous
Thromboembolism in Obese PatientsThromboembolism in Obese Patients
Our study suggests that it is safe to administer Our study suggests that it is safe to administer dalteparin at or near full dose based on actual dalteparin at or near full dose based on actual body weight for the treatment of acute venous body weight for the treatment of acute venous thromboembolism without an increased risk of thromboembolism without an increased risk of major hemorrhage major hemorrhage
Limiting the dose of dalteparin to 18 000 IU Limiting the dose of dalteparin to 18 000 IU could lead to an increased risk of recurrence could lead to an increased risk of recurrence of venous thromboembolism of venous thromboembolism
Al-Yaseen et al. J Thromb Haemost 2005; 3: 100-102.

Dosing in Heavy-Weight/Obese Patients with the Dosing in Heavy-Weight/Obese Patients with the LMWH, Tinzaparin: A Pharmacodynamic StudyLMWH, Tinzaparin: A Pharmacodynamic Study
Subcutaneous tinzaparin dosing in heavy or Subcutaneous tinzaparin dosing in heavy or
obese patients is appropriate based on body obese patients is appropriate based on body
weight alone; the dose need not be capped weight alone; the dose need not be capped
at a maximal absolute doseat a maximal absolute dose
Hainer J et al. J Thromb Haemost 2002; 87: 817-823.

Renal ImpairmentRenal Impairment

► The use of a 30-mL/min (0.50-mL/s) cutoff is The use of a 30-mL/min (0.50-mL/s) cutoff is
not justified, on the basis of currently available not justified, on the basis of currently available
evidence, to select individuals at increased risk evidence, to select individuals at increased risk
of accumulation when LMW heparin is used of accumulation when LMW heparin is used
► The pharmacokinetic response to impaired The pharmacokinetic response to impaired
renal function may differ among low-molecular-renal function may differ among low-molecular-
weight heparin preparationsweight heparin preparations
Is Is Impaired Renal FunctionImpaired Renal Function a Contraindication a Contraindication to the Use of Low-Molecular-Weight Heparin?to the Use of Low-Molecular-Weight Heparin?
Nagge et al. Arch Intern Med 2002; 162: 2605-2609.

Evidence-Based Guidelines Recommendations
Evidence-Based Guidelines Recommendations
Two Components:Two Components:
►Methodological Quality of a Methodological Quality of a RecommendationRecommendation
●Grade AGrade A
●Grade BGrade B or or
●Grade CGrade C
►Benefit/RiskBenefit/Risk
●Grade AGrade A or or
●Grade BGrade B
The 7th ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004; 126: 179S-187S.

Venous Thromboembolism:Venous Thromboembolism: Recognizing and Treating theRecognizing and Treating the
Patient at RiskPatient at Risk
Peter Hanson, MDPeter Hanson, MDMedical Director of OrthopaedicsMedical Director of Orthopaedics
Chief of Staff Chief of Staff Grossmont Hospital, La Mesa, CAGrossmont Hospital, La Mesa, CA

What Are We Trying To Prevent?What Are We Trying To Prevent?
► Asymptomatic DVT?Asymptomatic DVT?
► Symptomatic DVT?Symptomatic DVT?
► All PE’s?All PE’s?
► Fatal PE’s?Fatal PE’s?
► Post-phlebitic Syndrome?Post-phlebitic Syndrome?

Dear Surgeon………..Dear Surgeon………..
??



VenousVenousStasisStasis
Tourniquet
Immobilization and bed rest
VascularVascularInjuryInjury
Surgical manipulation of the limb
Endothelial injury
HypercoagulabilityHypercoagulability Increase in thromboplastin
agents
Very High Risk
Medium/High Risk
Low/Medium Risk
Virchow’s TriadVirchow’s TriadThrombosis Risk in Orthopedic SurgeryThrombosis Risk in Orthopedic Surgery

0%
10%
20%
30%
40%
50%
60%
70%
80%
Preventive Method
DV
T R
ate
(%
)
IPC
LMWHs
LD heparin
Warfarin
Stockings
Untreated
Aspirin
DVT Prevention in Knee ReplacementDVT Prevention in Knee Replacement(Total DVT by venography)(Total DVT by venography)

Preventing DVT in TKR With AspirinPreventing DVT in TKR With AspirinAspirin Alone Is Not Effective Prophylaxis After TKRAspirin Alone Is Not Effective Prophylaxis After TKR

DVT Prophylaxis in Total Knee DVT Prophylaxis in Total Knee Replacement (TKR) LMWH vs WarfarinReplacement (TKR) LMWH vs Warfarin
Spiro et al. Blood. 1994;84(suppl 1):246a.
Enoxaparin 30 mg sc
twice daily(n=173)
Warfarin dose-adjusted
INR 2-3(n=176)
Total DVT
25.4
45.4
0
10
20
30
40
50
P0.001P<0.001
Proximal DVT
1.7
11.4
0
2
4
6
8
10
12
Enoxaparin 30 mg sc
twice daily(n=173)
Warfarin dose-adjusted
INR 2-3(n=176)
Incidence
%

2.3 3.4
23.3
5.2 6.4
33.5
0
10
20
30
40
Major Bleeding Wound Complications(clinically significant)
Overall Bleeding
Bleeding in Total Knee Replacement Bleeding in Total Knee Replacement (TKR) LMWH vs Warfarin(TKR) LMWH vs Warfarin
Warfarindose-adjustedINR 2-3
Enoxaparin30 mg sc bid
P=0.04
Incidence
%
Spiro et al. Blood. 1994;84(suppl 1):246a.

Enoxaparin vs Warfarin inEnoxaparin vs Warfarin inTotal Knee ReplacementTotal Knee Replacement
Leclerc JR et al. Ann Intern Med. 1996, 124.619-626.

FondaparinuxFondaparinux Targeted Targeted MeMechanism of Actionchanism of Action
IIaII
Fibrinogen Fibrin clot
Extrinsic pathway
Intrinsicpathway
33
ATIII Xa
11
ATIII ATIII
22
Fondaparinux
XaXa
ATIII = antithrombin III
Antithrombin
Adapted with permission from Turpie AGG, et al. N Engl J Med. 2001;344:619-625.

Incidence of patients with VTE up to day 11
27.8
12.5
0
4
8
12
16
20
24
28
32
Fondaparinux2.5 mg QD (n=361)
Enoxaparin30 mg BID(n=363)
n = 45
n = 101
RRR = 55%P = 0.0000003
95% CI 9.2; 16.3 23.3; 32.7
Pat
ien
ts (
%)
TKTKR R Efficacy Efficacy RResults: Primary esults: Primary EEndpointndpoint
Pentamaks

Any DVTP < 0.0001
Proximal DVTP = 0.056
Pat
ien
ts (
%)
12.5
2.4
9.4
27.1
5.4
21.3
0
5
10
15
20
25
30
Distal DVT onlyP = 0.000009
FondaparinuxEnoxaparin
TKR Efficacy TKR Efficacy RResults:esults:Secondary Secondary EEndpointndpoint
Incidence of patients with VTE up to day 11
Pentamaks

PentamaksNS = no statistically significant difference
Fondaparinux2.5 mg QD
Enoxaparin30 mg BID
Fatal bleeding, n
Nonfatal bleeding in critical organ, n
Bleeding leading to reoperation, n (%)
Bleeding with transfusion ≥2 units and/or hg decrease ≥2 g/dL, n (%)
Other bleeding (minor), n (%)
TKR Safety: BleedingTKR Safety: Bleeding
Pvalue
NS
NS
NS
<0.05
NS
From 1st injection to day 11 – all treated patients
0
0
2 (0.4)
9 (1.7)
15 (2.9)
0
0
1 (0.2)
0 (0.0)
21 (4.0)

Incidenceof VTE
(%)
25.7
19.7
0
10
20
30
>7.5 and 9 hrs(n=61)
>9 and 12 hrs
(n=74)
40
30.0
>13 hrs(n=20)
Time to first dalteparin dose
VTE, venous thromboembolism
Thromboprophylaxis for Knee Thromboprophylaxis for Knee ReplacementReplacement
Dalteparin vs Warfarin: Post-Hoc AnalysisDalteparin vs Warfarin: Post-Hoc Analysis
Post-hoc analysis of patients (n=155) who received the 1st dose of dalteparin >7.5 hours postoperatively
Ayers DC et al. Poster presented at: American Academy of Orthopaedic Surgeons 2006 Annual Meeting; March 22, 2006; Chicago, IL.

Rationale for Extended Prophylaxis Rationale for Extended Prophylaxis After THR/TKRAfter THR/TKR
Cumulative Risk of Thromboembolic Events DuringFirst 3 Months Postoperatively
All VTE PE
0
1
2
3
14 28 42 56 70 84
Primary KneePrimary Hip
Days
0
1
2
3
14 28 42 56 70 84Days
Primary KneePrimary Hip
The incidence of thromboembolic events does not stabilize untilapproximately 10 weeks after THR
Incidence
%
White et al. Arch Intern Med. 1998;158:1525-1531.

Rationale for Extended ProphylaxisRationale for Extended Prophylaxis
White et al. Arch Intern Med. 1998;158:1525-1531.
1.1%
0.8%
0
0.5
1.0
Total HipArthroplasty
n = 19,000
Total KneeArthroplasty
n = 24,000
% o
f p
atie
nts
wit
h P
EIncidence of PE within 3 months post-surgery

76
47
0
20
40
60
80
Total HipReplacement
Total KneeReplacement
% DVT Diagnosis Made Post-Discharge
n=19,000 n=24,000
Rationale for Extended ProphylaxisRationale for Extended Prophylaxis
White et al. Arch Intern Med. 1998;158:1525-1531.

Total KneeArthroplasty
Total HipArthroplasty
Median Time of DVT Diagnosis After Surgery (Days)
0 5 10 15 20
17 Days17 Days
7 Days7 Days
n=19,000
n=24,000
Rationale for Extended ProphylaxisRationale for Extended Prophylaxis
White et al. Arch Intern Med. 1998;158:1525-1531.

NAFT Study DesignNAFT Study Design
visit
Screening
Day 35
Dalteparin (post-op) Dalteparin
Dalteparin (pre-op) Dalteparin
Warfarin
Venography
Switched to Placebo
Acute Phase Extended PhaseDay 0(surgery)
Day 6 Day 7
Venography

*RR=combined risk reduction vs. warfarin/placebo group†P=0.023‡ P<0.001§ P=0.007¥P=0.003
NAFT ResultsNAFT Results
Treatment Group Proximal DVT RR* Total DVT RR*(%) (%) (%) (%)
Pre-op dalteparinPre-op dalteparin 3.13.1 6767†† 17.217.2 5555‡‡
Post-op dalteparinPost-op dalteparin 2.02.0 7979§§ 22.222.2 4141¥¥
Warfarin/placeboWarfarin/placebo 9.2 (5 de novo)9.2 (5 de novo) 36.736.7
Extended Outpatient Phase (Day 35 ± 2)Extended Outpatient Phase (Day 35 ± 2)(Patients with negative bilateral venograms at day 6±2)(Patients with negative bilateral venograms at day 6±2)
Hull RD, et al. Arch Intern Med. 2000;160:2199-2207.

MajorMajorTreatment Group Bleeding (%) Wound Hematoma (%)Treatment Group Bleeding (%) Wound Hematoma (%)
Complicated Complicated Uncomplicated Uncomplicated
Pre-op dalteparinPre-op dalteparin 00 0.5 0.5 2.5 2.5
Post-op dalteparinPost-op dalteparin 00 0.5 0.5 2.1 2.1
WarfarinWarfarin 00 1.1 1.1 2.8 2.8
NAFT ResultsNAFT Results
Extended Outpatient Phase (Day 35 ± 2)Extended Outpatient Phase (Day 35 ± 2)(Patients with negative bilateral venograms at day 6±2)(Patients with negative bilateral venograms at day 6±2)
Hull RD, et al. Arch Intern Med. 2000;160:2199-2207.

Enoxaparin: Extended ProphylaxisEnoxaparin: Extended Prophylaxis
► Comp et al 2001 JBJS: Comp et al 2001 JBJS:
Enoxaparin 7-10 days vs 4 wks, Enoxaparin 7-10 days vs 4 wks, TKA’s and THA’s TKA’s and THA’s
Extended dosing in THA’s Extended dosing in THA’s significantly decreased DVT’s, no significantly decreased DVT’s, no difference in TKA’s difference in TKA’s
No added bleeding riskNo added bleeding risk

Recent Studies: Extended ProphylaxisRecent Studies: Extended Prophylaxis
► Eikelboom et al 2001 Lancet:Eikelboom et al 2001 Lancet: Meta-analysis of Meta-analysis of 3999 patients3999 patients, THA and , THA and
TKA, extended prophylaxis vs TKA, extended prophylaxis vs placebo/no tx placebo/no tx
DecreasedDecreased Sx’ic DVT in hips (not knees) Sx’ic DVT in hips (not knees) DecreasedDecreased Asx’ic DVT in hips Asx’ic DVT in hips
(not knees)(not knees) 20 sx’ic DVT/1000 pts, 1death/1000 pts 20 sx’ic DVT/1000 pts, 1death/1000 pts
preventedprevented $4-7 / day in UK, $24-28 / day in US$4-7 / day in UK, $24-28 / day in US No warfarin studies availableNo warfarin studies available

Extended Prophylaxis: Extended Prophylaxis: PENTPENTasaccharide in asaccharide in HHip-ip-FRAFRActure Surgery (PENTHIFRA Plus) Resultscture Surgery (PENTHIFRA Plus) Results
Incidence (%) of EventsIncidence (%) of Events
PlaceboPlacebo FondaparinuxFondaparinux RRR %RRR %
VTE*VTE* 3535 1.41.4 95.995.9
DVT*DVT* 33.933.9 1.41.4 95.895.8
Proximal DVT*Proximal DVT* 15.815.8 0.90.9 94.394.3
Major BleedingMajor Bleeding†† 0.60.6 2.42.4
Minor BleedingMinor Bleeding†† 0.60.6 1.51.5
Eriksson BI et al. Arch Intern Med. 2003;163:1337-1342.
* p < 0.001†no significant difference between treatment groups

Extended Prophylaxis with Fondaparinux: Extended Prophylaxis with Fondaparinux: Hip Fracture RepairHip Fracture Repair
35.0%35.0%
1.4%1.4%
00
55
1010
1515
2020
2525
3030
3535
FondaparinuxFondaparinux(n=208)(n=208)
PlaceboPlacebo(n=220) (n=220)
n = 3
n = 77n = 77
RRR = 96%RRR = 96%
Pa
tie
nts
(%
)P
ati
en
ts (
%)
Eriksson BI et al. Arch Intern Med. 2003;163:1337-1342.

Guidelines for Prevention of VTE:Guidelines for Prevention of VTE:Are They Relevant?Are They Relevant?
Current Findings: Applications for Thromboprophylaxis in Orthopaedic Surgery
The Four Seasons Hotel, San Francisco
March 10, 2004

Definition of Practice GuidelinesDefinition of Practice Guidelines
Practice guidelines are Practice guidelines are
systematically developedsystematically developed
statements to statements to assistassist
practitioner and patient practitioner and patient
decisionsdecisions about about appropriate appropriate
health carehealth care for specific for specific
clinical circumstances.clinical circumstances.

Seventh ACCP RecommendationsSeventh ACCP Recommendations

Seventh ACCP RecommendationsSeventh ACCP Recommendations

Seventh ACCP RecommendationsSeventh ACCP Recommendations

Duration Of Treatment (ACCP)Duration Of Treatment (ACCP)
► Optimal duration of Optimal duration of prophylaxis after THR or TKR prophylaxis after THR or TKR - at least 7-10 days - at least 7-10 days
► Extended prophylaxis with Extended prophylaxis with LMWH recommended at least LMWH recommended at least for “high risk” patientsfor “high risk” patients

Multimodal Approach to VTED Multimodal Approach to VTED Prophylaxis for THA and TKAProphylaxis for THA and TKA
Paul F. Lachiewicz, M.D.Paul F. Lachiewicz, M.D.
Department of OrthopaedicsDepartment of Orthopaedics
University of North Carolina - Chapel HillUniversity of North Carolina - Chapel Hill
ACCP Orthopaedists

THA TechniquesTHA Techniques
ThenThen Now Now
Bed restBed rest ≥1 week≥1 week <1 day<1 day
Hospital stayHospital stay 2-3 weeks2-3 weeks 2-4 days2-4 days
EBL EBL (mean)(mean) 1650 ml1650 ml 300-600 ml300-600 ml
BloodBlood HomologousHomologous AutologousAutologous
Transfusion Transfusion (mean)(mean) 1144 ml1144 ml 0-500 ml0-500 ml
AnesthesiaAnesthesia GeneralGeneral RegionalRegional

These major changes in THA These major changes in THA techniques suggest that our older techniques suggest that our older
ideas about chemoprophylaxis ideas about chemoprophylaxis should be reconsidered in 2007should be reconsidered in 2007

PreoperativePreoperative
IntraoperativeIntraoperative
Postoperative Postoperative
Multimodal ProphylaxisMultimodal ProphylaxisMultimodal ProphylaxisMultimodal Prophylaxis

Preoperative Risk Factors VTEDPreoperative Risk Factors VTED
► Genetic predispositionGenetic predisposition► Hypercoaguable statesHypercoaguable states► Prior history PEPrior history PE► Oral contraceptives (?)Oral contraceptives (?)
► Classic risk factors have notClassic risk factors have notcorrelated with VTED in elective correlated with VTED in elective THA patients THA patients

PreoperativePreoperativeAutologous DonationAutologous Donation
► Retrospective study: 2043 patientsRetrospective study: 2043 patients
► Donation 1037; not 1006Donation 1037; not 1006
► DVT DVT Donation 9.0% Donation 9.0% (p=0.003)(p=0.003)
(venogram) (venogram) NotNot 13.5%13.5%
► P.E.P.E. Donation 0.3% Donation 0.3% (ns)(ns)
(clinical)(clinical) NotNot 0.7% 0.7%
Bae et al. JBJS (B) 2001

Thromboembolism THRThromboembolism THRAnesthesiaAnesthesia
► Spinal or epidural anesthesia Spinal or epidural anesthesia reduces risk by 40-50%reduces risk by 40-50%
► Regional anesthesia increased Regional anesthesia increased blood flow in lower extremities blood flow in lower extremities during and after the procedureduring and after the procedure
► Lower blood loss, ? quicker Lower blood loss, ? quicker surgerysurgery

Mechanical Prophylaxis THAMechanical Prophylaxis THA
Intraoperative use does Intraoperative use does notnot interfere interfere with positioning, exposure, with positioning, exposure,
placement of implantsplacement of implants

Intraop and postop IPC is specific Intraop and postop IPC is specific localized prophylaxis: localized prophylaxis:
► Decreased venous stasis Decreased venous stasis increase venous velocityincrease venous velocity
increase venous volumeincrease venous volume► Inhibits coagulation cascadeInhibits coagulation cascade
tissue factor pathway inhibitortissue factor pathway inhibitor
factor VIIafactor VIIa
NO and endogenousNO and endogenous NO synthase NO synthase
Mechanical Prophylaxis THAMechanical Prophylaxis THA

► Wide variety of devicesWide variety of devices foot pumpfoot pump calfcalf thigh-calfthigh-calf
► Each device has its own mechanics with Each device has its own mechanics with resultant change in peak venous resultant change in peak venous velocity and venous volumevelocity and venous volume
► For THA, optimal characteristics of For THA, optimal characteristics of pneumatic compression are not knownpneumatic compression are not known
Mechanical Prophylaxis THAMechanical Prophylaxis THA

Venous Hemodynamics After THAVenous Hemodynamics After THA
► Devices with rapid inflation time Devices with rapid inflation time Produced the greatest increase Produced the greatest increase
in peak venous velocityin peak venous velocity
► Devices that compress calfDevices that compress calfand thighand thigh Produced the greatest increase Produced the greatest increase
in venous volumein venous volume

Multimodal ProphylaxisMultimodal Prophylaxis
► June 1991 – May 2005June 1991 – May 2005► Single surgeonSingle surgeon► 1042 consecutive THA1042 consecutive THA
(388 in previous study)(388 in previous study)
► 10 exclusions10 exclusions (5 hemophilia, 5 other)(5 hemophilia, 5 other)
Lachiewicz, Soileau. Clin Orthop 2006

Study GroupStudy Group
► 1032 hip procedures1032 hip procedures► 422 male, 610 female422 male, 610 female► Mean age 64 (22-95)Mean age 64 (22-95)► Primary 680Primary 680
Revision 352Revision 352
*Patients with prior history of TED or on warfarin for *Patients with prior history of TED or on warfarin for cardiac conditions cardiac conditions notnot excluded excluded

Materials & MethodsMaterials & Methods
► AnesthesiaAnesthesia
RegionalRegional 95%95%
General only 5%General only 5%► Intraoperative mechanicalIntraoperative mechanical
bilateral, thigh-highbilateral, thigh-high sterile sleeve-operative limbsterile sleeve-operative limb single manufacturersingle manufacturer
► Recovery room + until dischargeRecovery room + until discharge► Duplex ultrasound prior to discharge Duplex ultrasound prior to discharge
(day 3-8)(day 3-8)

Results - MortalityResults - Mortality
► 1 fatal pulmonary embolism (0.09%)1 fatal pulmonary embolism (0.09%)
24 days postop-autopsy24 days postop-autopsy
patient in long-leg bracepatient in long-leg brace
minimal ambulationminimal ambulation► 1 cerebrovascular accident1 cerebrovascular accident► 1 unknown; abdominal pain & cardiac arrest1 unknown; abdominal pain & cardiac arrest
? M.I. vs P.E.? M.I. vs P.E.
30 day mortality30 day mortality
3 of 1032 (0.3%)3 of 1032 (0.3%)
30 day mortality30 day mortality
3 of 1032 (0.3%)3 of 1032 (0.3%)

Pulmonary EmbolismPulmonary Embolism
Symptomatic 7Symptomatic 7 (0.7%) (0.7%)
4 early 4 early (POD #4-7)(POD #4-7)
3 late3 late
POD # 23POD # 2324 24 (fatal)(fatal)
3737Only 1 of 7 also had DVT or Only 1 of 7 also had DVT or DuplexDuplex

Mechanical Prophylaxis withMechanical Prophylaxis withAspirin vs Aspirin AloneAspirin vs Aspirin Alone
► Prospective, randomizedProspective, randomized► 100 hips - MR venography100 hips - MR venography
► Rapid inflation device (VenaflowRapid inflation device (Venaflow®)®) applied in recovery roomapplied in recovery room epidural hypotensive anesthesiaepidural hypotensive anesthesia aspirin 325 mg BIDaspirin 325 mg BID
► Mechanical + aspirin 8% prox. DVTMechanical + aspirin 8% prox. DVT aspirin alone 22% prox. DVT (p<.05)aspirin alone 22% prox. DVT (p<.05)
Ryan et al. JBJS 2002

Multimodal Prophylaxis THAMultimodal Prophylaxis THA
► Calf-thigh compression begun Calf-thigh compression begun intraoperatively is effective and intraoperatively is effective and acceptable for 99% THA patientsacceptable for 99% THA patients
► 1032 hips1032 hips► Fatal PE 0.09%Fatal PE 0.09%► Total DVT-PE 4.6%Total DVT-PE 4.6%► Pulmonary embolism 0.7%Pulmonary embolism 0.7%

VTED After TKAVTED After TKA Orthopaedic Perspective Orthopaedic Perspective
► Different “disease” than after THADifferent “disease” than after THA
► Most thrombi occur in calf onlyMost thrombi occur in calf only
► Extension to proximal veins Extension to proximal veins occurs infrequentlyoccurs infrequently
► Pulmonary embolism rare Pulmonary embolism rare

Orthopaedist’s ConcernsOrthopaedist’s Concerns
Prevention ofPrevention of
► Fatal PEFatal PE► Symptomatic PESymptomatic PE► Symptomatic DVTSymptomatic DVT► Knee bleedingKnee bleeding
How important is it to prevent asymptomatic venogram or Duplex scan-detected thrombi?

Orthopaedist’s ConcernsOrthopaedist’s Concerns Anticoagulation TKA Anticoagulation TKA
► Increased risk of major bleeding into Increased risk of major bleeding into knee and wound complications knee and wound complications (0.9 – 5.2%)(0.9 – 5.2%)
► True risk of bleeding and outcome not True risk of bleeding and outcome not established for all TKA patients established for all TKA patients
► Bleeding into TKA associated with Bleeding into TKA associated with hematomas, drainage, infection and hematomas, drainage, infection and poorer outcomespoorer outcomes

Mechanical Prophylaxis TKAMechanical Prophylaxis TKA
► Wide variety of devicesWide variety of devices thigh-calfthigh-calf calf onlycalf only foot pumpfoot pump
► Each device has its own mechanics with Each device has its own mechanics with different changes in peak venous different changes in peak venous velocity and volumevelocity and volume
► Optimal characteristics for devices?Optimal characteristics for devices?

Venous Hemodynamics After TKAVenous Hemodynamics After TKA
Westrich et al. JBJS (B) 1998
Flowtron DVTVenaFlowPlexiPulsefoot-calf
PlexiPulsefoot
A-V impulsesystem
DPF Jobstathrombic
pump
SCD system
Calf-thighCalfFoot calfFoot
Incr
ease
in
ver
iou
s ve
loci
ty (
%)

Mechanical Prophylaxis TKAMechanical Prophylaxis TKA
► Devices with rapid inflation time Devices with rapid inflation time produced the greatest increase in produced the greatest increase in peak venous velocitypeak venous velocity
► Devices that compress calf and Devices that compress calf and thigh produced the greatest thigh produced the greatest increase in venous volumeincrease in venous volume
► What matters most –What matters most –velocity or volume?velocity or volume?

Two Mechanical Devices for Prophylaxis Two Mechanical Devices for Prophylaxis of Thromboembolism After TKAof Thromboembolism After TKA
Lachiewicz et al. JBJS (B), Nov 2004. University of North Carolina-Chapel Hill
Prospective, randomized studyProspective, randomized studyProspective, randomized studyProspective, randomized study

Patient PopulationPatient Population
► 423 patients, 472 knees423 patients, 472 knees
► Mean age 66.8 yrs (23-94)Mean age 66.8 yrs (23-94)
► Mean wt 87.3 kg (45-148)Mean wt 87.3 kg (45-148)
► DiagnosisDiagnosis DJDDJD 307 307
RA 25RA 25
Rev.Rev. 64 64
Other 27Other 27

ResultsResults
AsymmetricalAsymmetrical CircumferentialCircumferential CompressionCompression CompressionCompression
PatientsPatients 206 206 217217
KneesKnees 232 232 240240
MortalityMortality 0 0 1 1 (.46%)(.46%)
Pulm. EmbolismPulm. Embolism 00 1 1 (.46%)(.46%)
ThrombiThrombi 16 16 (6.9%)(6.9%) 36 36 (15%) p = .007(15%) p = .007
CalfCalf 15 15 3030ProximalProximal 1 1 66

ThromboembolismThromboembolismKnee ProcedureKnee Procedure
AsymmetricalAsymmetrical CircumferentialCircumferential CompressionCompression Compression Compression
Unilateral, primaryUnilateral, primary
KneesKnees 155 155 158 158 ThrombiThrombi 13 13 (8.4%)(8.4%) 26 26 (15.8%)(15.8%) p = 0.03p = 0.03
Bilateral, primaryBilateral, primary
Patients (knees)Patients (knees) 25 25 (50)(50) 22 22 (44)(44)
Patients-thrombiPatients-thrombi 1 1 (4%)(4%) 55 (22.7%)(22.7%) p = 0.09p = 0.09
Limbs-thrombiLimbs-thrombi 2 2 (4%)(4%) 77 (15.9%)(15.9%) p = 0.05p = 0.05

Personal TKA Series Personal TKA Series Calf IPC Plus AspirinCalf IPC Plus Aspirin
856 TKAs856 TKAs
Mortality (MI)Mortality (MI) 1 1 (0.12%)(0.12%)
Symptomatic PESymptomatic PE 3 3 (0.35%)(0.35%)
DVT DVT (Duplex)(Duplex) 6666 (7.7%)(7.7%)
(56 pts)(56 pts)
1991 - present1991 - present1991 - present1991 - present

Multimodal Prophylaxis TKAMultimodal Prophylaxis TKAVenaflowVenaflow®® + LMWH vs. Venaflow + LMWH vs. Venaflow®® + Aspirin + Aspirin
► Prospective, randomizedProspective, randomized
► 275 unilateral TKAs275 unilateral TKAs
► Duplex scan 3-5 days; 4-6 weeksDuplex scan 3-5 days; 4-6 weeks
► DVT 14.1% vs 17.8% DVT 14.1% vs 17.8% (p = 0.27)(p = 0.27)
► No difference between groups!No difference between groups!
Westrich et al. J. Arthroplasty 2006

VTED Prophylaxis TKAVTED Prophylaxis TKAWhat is Acceptable in 2007What is Acceptable in 2007
► Mechanical prophylaxis plus aspirin is Mechanical prophylaxis plus aspirin is safe and effective for most TKA patients safe and effective for most TKA patients
► Recommend rapid-inflation, asymmetric Recommend rapid-inflation, asymmetric calf compression devicecalf compression device
► Anticoagulation for patients allergic to Anticoagulation for patients allergic to aspirin or with heritable coagulopathyaspirin or with heritable coagulopathy
► Multimodal prophylaxis is an acceptable Multimodal prophylaxis is an acceptable alternative to ACCP Guidelinesalternative to ACCP Guidelines

Anticoagulation andAnticoagulation andthe Orthopedic Patient:the Orthopedic Patient:
the Anesthesiologist’s Perspectivethe Anesthesiologist’s Perspective
Eugene R Viscusi, MDEugene R Viscusi, MDDirector, Acute Pain ManagementDirector, Acute Pain Management
Associate ProfessorAssociate Professor
Department of AnesthesiologyDepartment of Anesthesiology
Thomas Jefferson University, Philadelphia, PAThomas Jefferson University, Philadelphia, PA

OverviewOverview
► Venous thromboembolism (VTE), DVT Venous thromboembolism (VTE), DVT and PE are real and significant threats to and PE are real and significant threats to the orthopedic patientthe orthopedic patient
► The anesthesia and analgesia plan must The anesthesia and analgesia plan must accommodate treatment of VTEaccommodate treatment of VTE
► Anesthesia and pain management can be Anesthesia and pain management can be challenging and pose risks to the patient challenging and pose risks to the patient in the absence of communication and in the absence of communication and cooperation between care teamscooperation between care teams

► The 2004 ACCP recommendations further The 2004 ACCP recommendations further increased the level and duration of increased the level and duration of thromboprophylasis. Despite the thromboprophylasis. Despite the reduction of asymptomatic reduction of asymptomatic thromboembolic events, an actual thromboembolic events, an actual reduction of clinically relevant events has reduction of clinically relevant events has been difficult to demonstrate been difficult to demonstrate 1,21,2
► These changes create new challenges for These changes create new challenges for managing neuraxial and invasive non-managing neuraxial and invasive non-compressible peripheral blockadecompressible peripheral blockade
1. Murray DW, et al. J Bone Joint Surg. 1996;78:863-870.2. Mantilla CB, et al. Anesthesiology. 2002;96:1140-1146.
OverviewOverview

► The ACCP guidelines and the ASRA The ACCP guidelines and the ASRA consensus statement on neuraxial consensus statement on neuraxial techniques often leave the clinician in the techniques often leave the clinician in the zone of discomfort:zone of discomfort: Both statements provide important Both statements provide important
clinical information but don’t address clinical information but don’t address all situationsall situations
ASRA guidelines are based on ASRA guidelines are based on knowledge of the agents and past knowledge of the agents and past adverse events rather than large adverse events rather than large studies. (Difficult to provide the studies. (Difficult to provide the denominator)denominator)
The ChallengeThe Challenge

2004 ACCP Recommendations2004 ACCP Recommendations
► Unfractionated heparin every 8 hoursUnfractionated heparin every 8 hours No data documenting safety of No data documenting safety of
neuraxial catheters; complicates neuraxial catheters; complicates catheter removalcatheter removal
► Fondaparinux following major Fondaparinux following major orthopedic surgeryorthopedic surgery ASRA recommends againstASRA recommends against
epidural catheterepidural catheter
► Warfarin; target INR for TJA is 2.5Warfarin; target INR for TJA is 2.5 If achieved would precludeIf achieved would preclude
epidural cathetersepidural cathetersChest. Sept 2004, supp

2004 ACCP Recommendations2004 ACCP Recommendations
► Dosing of LMWH early in the Dosing of LMWH early in the postoperative period was associated postoperative period was associated with an increased risk of neuraxial with an increased risk of neuraxial bleedingbleeding
► Anticoagulate a minimum of 10 days; Anticoagulate a minimum of 10 days; 28-35 for total hip28-35 for total hip Interaction of prolonged Interaction of prolonged
thromboprophylaxis, neuraxial thromboprophylaxis, neuraxial instrumentation, difficult or instrumentation, difficult or traumatic needle insertion is traumatic needle insertion is UNKNOWNUNKNOWN

1,260,000 spinals; 450,000 epidurals1,260,000 spinals; 450,000 epidurals
► 33 spinal hematomas33 spinal hematomas 24 in females, 25 with epidural24 in females, 25 with epidural Coagulopathy in 11Coagulopathy in 11
► Time of occurrence: 24 hours (6H-14D)Time of occurrence: 24 hours (6H-14D)
► 5 of 33 recovered (delay in treatment)5 of 33 recovered (delay in treatment)
► 4 patients with indwelling epidural 4 patients with indwelling epidural catheters received 5,000 U heparin catheters received 5,000 U heparin during surgeryduring surgery
Moen V, et al. Anesthesiology. 2004;101:950-959

► Authors calculated risk for females Authors calculated risk for females undergoing TKA 1:3,600! (female, age, undergoing TKA 1:3,600! (female, age, spinal canal pathology, duration of spinal canal pathology, duration of catheter, thromboprophylaxis)catheter, thromboprophylaxis)
► One–third of all spinal hematomas One–third of all spinal hematomas occurred in patients receiving occurred in patients receiving thromboprophylaxis in accordance thromboprophylaxis in accordance with current guidelineswith current guidelines
Moen V, et al. Anesthesiology. 2004;101:950-959

Spinal HematomaSpinal Hematoma
► May occur in the absence of May occur in the absence of identifiable risk factorsidentifiable risk factors
► Neurological monitoring is critical for Neurological monitoring is critical for early interventionearly intervention Early recognition and treatment is Early recognition and treatment is
key to improved outcome key to improved outcome (laminectomy within 8 hours) (laminectomy within 8 hours) 11
► Focus not only on prevention but also Focus not only on prevention but also improving neurological outcome improving neurological outcome
Vandermeulen ER, et al. Anesth Analg 1994:79:1165-77

WarfarinWarfarin
► INR of less than 1.5 is recommended INR of less than 1.5 is recommended for removal of epidural cathetersfor removal of epidural catheters11
► Check INR: Check INR: Every day with an indwelling Every day with an indwelling
epidural catheter epidural catheter Prior to needle insertion if given Prior to needle insertion if given
more than 36 hours priormore than 36 hours prior
1. 2nd ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation.Reg Anesth Pain Med. 2003;28:172-197.

Can Epidural Anesthesia andCan Epidural Anesthesia andWarfarin be Coadministered?Warfarin be Coadministered?11
► Prudence must be exercised when Prudence must be exercised when enforcing these guidelines, both in the enforcing these guidelines, both in the upper INR limit as well as potential upper INR limit as well as potential reversal of anticoagulationreversal of anticoagulation11
11,235 patients: no detectable 11,235 patients: no detectable hematomas hematomas • 1030 randomly reviewed charts: 1030 randomly reviewed charts:
398 patients had INR greater than 398 patients had INR greater than 1.5 (1.54 mean, range 0.93-4.25)1.5 (1.54 mean, range 0.93-4.25)
1. Parvizi J, Viscusi ER. CORR, 2007( in press)

► If the INR is “elevated”, should If the INR is “elevated”, should anticoagulation be reversed?anticoagulation be reversed? Pulmonary embolism is aPulmonary embolism is a
serious riskserious risk FFP is not without risk in itselfFFP is not without risk in itself
► Decision should be taken case by Decision should be taken case by case and the thought process fully case and the thought process fully documented!documented!
Can Epidural Anesthesia andCan Epidural Anesthesia andWarfarin be Coadministered?Warfarin be Coadministered?11
1. Parvizi J, Viscusi ER. CORR, 2007( in press)

Standard (Unfractionated) HeparinStandard (Unfractionated) Heparin
► BID dosing is theoretically safe if BID dosing is theoretically safe if catheter removal is timed with catheter removal is timed with trough levelstrough levels
► TID dosing: no data exists but PTT TID dosing: no data exists but PTT (anecdotally) may remain elevated(anecdotally) may remain elevated
► Heparin induced thrombocytopena Heparin induced thrombocytopena (HIT) is a real concern(HIT) is a real concern Platelet count is indicated after 5 Platelet count is indicated after 5
days of unfractionated heparindays of unfractionated heparin

Standard Heparin andStandard Heparin andRegional AnesthesiaRegional Anesthesia
► No contraindication following subcutaneous No contraindication following subcutaneous injection prior to spinal/epidural needle injection prior to spinal/epidural needle insertioninsertion
► Delay administration for one hour following Delay administration for one hour following needle placementneedle placement
► Remove indwelling catheter at trough level Remove indwelling catheter at trough level or one hour prior to next doseor one hour prior to next dose
► Prolonged therapy is linked to increase in Prolonged therapy is linked to increase in spinal hematomaspinal hematoma
► Traumatic needle insertion may increase Traumatic needle insertion may increase risk of spinal hematomarisk of spinal hematoma
ASRA consensus guidelines

LMWHLMWH
► Restrict to once daily dosing regimen Restrict to once daily dosing regimen with epidural catheterwith epidural catheter
► LMWH dosing minimum of 2 hours after LMWH dosing minimum of 2 hours after catheter removalcatheter removal
► Spinal hematomas have been reported Spinal hematomas have been reported with this regimen; (The last chapter with this regimen; (The last chapter hasn’t been written)hasn’t been written)
ASRA consensus guidelines

► Consider the risk/benefit ratio of Consider the risk/benefit ratio of thromboembolic event vs. spinal thromboembolic event vs. spinal hematomahematoma
► Timing: With once daily dosing, time Timing: With once daily dosing, time epidural catheter removal in a safe epidural catheter removal in a safe window window beforebefore next dose next dose Minimize delay of next doseMinimize delay of next dose
► Renal function affects metabolism of Renal function affects metabolism of LMWH (and other drugs). Elderly at LMWH (and other drugs). Elderly at particular risk. Dose accordingly particular risk. Dose accordingly 11
D’Sousa G, Viscusi ER. ASA 2006 (abstract)
LMWHLMWH

Antiplatelet MedicationsAntiplatelet Medications
► Uncommon as primary agents for Uncommon as primary agents for thromboprophylaxis but may be used thromboprophylaxis but may be used chronically by orthopedic patientschronically by orthopedic patients11
A number of large studies A number of large studies demonstrated relative safetydemonstrated relative safety
However, if this is combined with However, if this is combined with heparin there may be increased heparin there may be increased (but unquantified) risk(but unquantified) risk
Horlocker T, Wedel D. Anesth Analg 1995;80:303-309

Platelet Aggregation InhibitorsPlatelet Aggregation Inhibitors
► Interfere with platelet-fibrinogen binding Interfere with platelet-fibrinogen binding and platelet-platelet interaction and platelet-platelet interaction Ticlopidine: stop 14 daysTiclopidine: stop 14 days Clopidogrel: stop 7 daysClopidogrel: stop 7 days
► Platelet glycoprotein IIb/IIIa receptor Platelet glycoprotein IIb/IIIa receptor antagonistsantagonists 48 hours: abciximab48 hours: abciximab 8 hours eptifibatide, tirofiban8 hours eptifibatide, tirofiban
ASRA consensus guidelines

FondaparinuxFondaparinux
► Factor Xa inhibitor with half-life ofFactor Xa inhibitor with half-life of21 hours21 hours11
► Clinical trials:Clinical trials: Atraumatic epidural needle Atraumatic epidural needle
placementplacement Epidural catheter removed 2 hours Epidural catheter removed 2 hours
prior to dosingprior to dosing► Avoid indwelling epidural catheters with Avoid indwelling epidural catheters with
this drugthis drug
Turpie AG et al.[Letter]NEJM. 2001; 345:292

Recommendations for Safety with Recommendations for Safety with Neuraxial TechniquesNeuraxial Techniques
► Know the ASRA guidelinesKnow the ASRA guidelines► Employ single agent anticoagulationEmploy single agent anticoagulation► Understand risks of each individual agentUnderstand risks of each individual agent► Follow developments with peripheral Follow developments with peripheral
nerve blocksnerve blocks► Careful monitoring of dose timing, Careful monitoring of dose timing,
coagulation studies and neurologic coagulation studies and neurologic function are criticalfunction are critical
► Atraumatic needle placement if possibleAtraumatic needle placement if possible

Analgesic Techniques: HipAnalgesic Techniques: Hip
► Intrathecal MorphineIntrathecal Morphine
► Lumbar Plexus BlockLumbar Plexus Block Single injection or continuous catheterSingle injection or continuous catheter
► Epidural AnalgesiaEpidural Analgesia Single injection, standard morphineSingle injection, standard morphine Extended-release Epidural MorphineExtended-release Epidural Morphine Indwelling epidural catheterIndwelling epidural catheter

► Femoral BlockFemoral Block Single injection or catheterSingle injection or catheter
► Lumbar plexus (posterior approach)Lumbar plexus (posterior approach) Single injection or continuous catheterSingle injection or continuous catheter
► Epidural analgesiaEpidural analgesia Indwelling continuous catheterIndwelling continuous catheter Extended-release Epidural Morphine Extended-release Epidural Morphine Single injection standard morphineSingle injection standard morphine
Analgesic Techniques: KneeAnalgesic Techniques: Knee

SummarySummary
► Safe and effective anesthesia and Safe and effective anesthesia and pain management for the orthopedic pain management for the orthopedic patient can be achieved in the patient can be achieved in the presence of VTE prophylaxis when presence of VTE prophylaxis when the entire care team (orthopedics, the entire care team (orthopedics, anesthesiology, nursing) understands anesthesiology, nursing) understands the limitations, risks and works the limitations, risks and works togethertogether