Embed Size (px)
Citation preview

Welcome to this Science-to-Strategy SummitWelcome to this Science-to-Strategy Summit

Critical Challenges and Landmark Critical Challenges and Landmark Advances in Advances in Thrombosis ManagementThrombosis Management
The Evolving and Foundation Role of LMWHs in Cancer and The Evolving and Foundation Role of LMWHs in Cancer and VTE Prophylaxis: Applying Science, Expert Analysis, and VTE Prophylaxis: Applying Science, Expert Analysis, and Landmark Trials to the Front Lines of Oncology PracticeLandmark Trials to the Front Lines of Oncology Practice
Critical Challenges and Landmark Critical Challenges and Landmark Advances in Advances in Thrombosis ManagementThrombosis Management
The Evolving and Foundation Role of LMWHs in Cancer and The Evolving and Foundation Role of LMWHs in Cancer and VTE Prophylaxis: Applying Science, Expert Analysis, and VTE Prophylaxis: Applying Science, Expert Analysis, and Landmark Trials to the Front Lines of Oncology PracticeLandmark Trials to the Front Lines of Oncology Practice
Clotting, Cancer, and ControversiesClotting, Cancer, and Controversies
Program ChairmanProgram ChairmanAjay Kakkar, MBBS, PhD, FRCSAjay Kakkar, MBBS, PhD, FRCSHead of the Centre for Surgical SciencesHead of the Centre for Surgical Sciences
Barts and the London Barts and the London Queen Mary’s School ofQueen Mary’s School ofMedicine and DentistryMedicine and Dentistry
The Thrombosis Research InstituteThe Thrombosis Research InstituteLondon, UKLondon, UK
Program ChairmanProgram ChairmanAjay Kakkar, MBBS, PhD, FRCSAjay Kakkar, MBBS, PhD, FRCSHead of the Centre for Surgical SciencesHead of the Centre for Surgical Sciences
Barts and the London Barts and the London Queen Mary’s School ofQueen Mary’s School ofMedicine and DentistryMedicine and Dentistry
The Thrombosis Research InstituteThe Thrombosis Research InstituteLondon, UKLondon, UK

CME-accredited symposiumCME-accredited symposium jointly sponsored by the jointly sponsored by the Postgraduate Institute of Medicine and CMEducation ResourcesPostgraduate Institute of Medicine and CMEducation Resources
Commercial Support:Commercial Support: Sponsored by an independent educational Sponsored by an independent educational grant from Eisai, Inc.grant from Eisai, Inc.
Mission statement:Mission statement: Improve patient care through evidence-based Improve patient care through evidence-based education, expert analysis, and case study-based managementeducation, expert analysis, and case study-based management
Processes:Processes: Strives for fair balance, clinical relevance, on-label Strives for fair balance, clinical relevance, on-label indications for agents discussed, and emerging evidence and indications for agents discussed, and emerging evidence and information from recent studiesinformation from recent studies
COI:COI: Full faculty disclosures provided in syllabus and at the Full faculty disclosures provided in syllabus and at the beginning of the programbeginning of the program
Welcome and Program OverviewWelcome and Program Overview

Program Educational ObjectivesProgram Educational Objectives
As a result of this session, physicians will be able to:
► Review recent trials, research, and expert analysis of issues focused on thrombosis and cancer.
► Specify strategies for risk-directed prophylaxis against DVT in at risk patients with cancer.
► Explain how to assess and manage special needs of cancer patients at risk for DVT, with a focus on protecting against recurrent DVT.
► Describe how to risk stratify patients undergoing cancer surgery, and implement ACCP-mandated pharmacologic and non-pharmacologic measures aimed at DVT prophylaxis.
► Review landmark clinical trials focusing on DVT prophylaxis in patients with cancer.
► Explain how to appropriately use the range of pharmacologic options available for thrombosis management in patients with malignancy.
As a result of this session, physicians will be able to:
► Review recent trials, research, and expert analysis of issues focused on thrombosis and cancer.
► Specify strategies for risk-directed prophylaxis against DVT in at risk patients with cancer.
► Explain how to assess and manage special needs of cancer patients at risk for DVT, with a focus on protecting against recurrent DVT.
► Describe how to risk stratify patients undergoing cancer surgery, and implement ACCP-mandated pharmacologic and non-pharmacologic measures aimed at DVT prophylaxis.
► Review landmark clinical trials focusing on DVT prophylaxis in patients with cancer.
► Explain how to appropriately use the range of pharmacologic options available for thrombosis management in patients with malignancy.

Program FacultyProgram Faculty
Program ChairmanAjay Kakkar, MBBS, PhD, FRCSHead of the Centre for Surgical SciencesBarts and the LondonQueen Mary’s School of Medicine and DentistryThrombosis Research InstituteLondon, UK
Craig M. Kessler, MDProfessor of Medicine and PathologyGeorgetown University Medical CenterDirector of the Division of CoagulationDepartment of Laboratory MedicineWashington, DC
Program ChairmanAjay Kakkar, MBBS, PhD, FRCSHead of the Centre for Surgical SciencesBarts and the LondonQueen Mary’s School of Medicine and DentistryThrombosis Research InstituteLondon, UK
Craig M. Kessler, MDProfessor of Medicine and PathologyGeorgetown University Medical CenterDirector of the Division of CoagulationDepartment of Laboratory MedicineWashington, DC
Alex C. Spyropoulos, MD, FACP, FCCPChair, Department of Clinical ThrombosisLovelace Medical CenterClinical Associate Professor of MedicineUniversity of New MexicoAlbuquerque, New Mexico
Distinguished Panel Member, Consultant, and Visiting ProfessorSamuel Z. Goldhaber, MDProfessor of Medicine, Cardiovascular Division Harvard Medical SchoolDirector, Venous Thromboembolism Research GroupDirector, Anticoagulation ServiceBrigham and Women’s HospitalBoston, MA
Alex C. Spyropoulos, MD, FACP, FCCPChair, Department of Clinical ThrombosisLovelace Medical CenterClinical Associate Professor of MedicineUniversity of New MexicoAlbuquerque, New Mexico
Distinguished Panel Member, Consultant, and Visiting ProfessorSamuel Z. Goldhaber, MDProfessor of Medicine, Cardiovascular Division Harvard Medical SchoolDirector, Venous Thromboembolism Research GroupDirector, Anticoagulation ServiceBrigham and Women’s HospitalBoston, MA

Faculty COI Financial DisclosuresFaculty COI Financial Disclosures
Ajay Kakkar, MBBS, PhD, FRCSAjay Kakkar, MBBS, PhD, FRCSGrants/research support: sanofi-aventis, AstraZeneca, PfizerGrants/research support: sanofi-aventis, AstraZeneca, PfizerConsultant: Pfizer, sanofi-aventisConsultant: Pfizer, sanofi-aventis
Craig M. Kessler, MDCraig M. Kessler, MDGrants/research support: sanofi-aventis, Eisai, GlaxoSmithKline, Grants/research support: sanofi-aventis, Eisai, GlaxoSmithKline, OctapharmaOctapharmaConsultant: sanofi-aventis, Eisai, NovoNordiskConsultant: sanofi-aventis, Eisai, NovoNordisk
Alex C. Spyropoulos, MD, FACP, FCCAlex C. Spyropoulos, MD, FACP, FCCConsultant: sanofi-aventis, Eisai, Bayer, Boehringer-IngelheimConsultant: sanofi-aventis, Eisai, Bayer, Boehringer-IngelheimSpeaker’s Bureau: sanofi-aventis EisaiSpeaker’s Bureau: sanofi-aventis Eisai
Samuel Z. Goldhaber, MDSamuel Z. Goldhaber, MDGrant/Research Support: sanofi-aventis, GSK, EisaiGrant/Research Support: sanofi-aventis, GSK, EisaiConsultant: sanofi-aventis, BMS, Emisphere, Boehringer-IngelheimConsultant: sanofi-aventis, BMS, Emisphere, Boehringer-Ingelheim
Ajay Kakkar, MBBS, PhD, FRCSAjay Kakkar, MBBS, PhD, FRCSGrants/research support: sanofi-aventis, AstraZeneca, PfizerGrants/research support: sanofi-aventis, AstraZeneca, PfizerConsultant: Pfizer, sanofi-aventisConsultant: Pfizer, sanofi-aventis
Craig M. Kessler, MDCraig M. Kessler, MDGrants/research support: sanofi-aventis, Eisai, GlaxoSmithKline, Grants/research support: sanofi-aventis, Eisai, GlaxoSmithKline, OctapharmaOctapharmaConsultant: sanofi-aventis, Eisai, NovoNordiskConsultant: sanofi-aventis, Eisai, NovoNordisk
Alex C. Spyropoulos, MD, FACP, FCCAlex C. Spyropoulos, MD, FACP, FCCConsultant: sanofi-aventis, Eisai, Bayer, Boehringer-IngelheimConsultant: sanofi-aventis, Eisai, Bayer, Boehringer-IngelheimSpeaker’s Bureau: sanofi-aventis EisaiSpeaker’s Bureau: sanofi-aventis Eisai
Samuel Z. Goldhaber, MDSamuel Z. Goldhaber, MDGrant/Research Support: sanofi-aventis, GSK, EisaiGrant/Research Support: sanofi-aventis, GSK, EisaiConsultant: sanofi-aventis, BMS, Emisphere, Boehringer-IngelheimConsultant: sanofi-aventis, BMS, Emisphere, Boehringer-Ingelheim

Introduction and Chairman’s OverviewIntroduction and Chairman’s Overview
Clotting, Cancer, And Controversies: Clotting, Cancer, And Controversies: What The Cascade Of Evidence And What The Cascade Of Evidence And
Current Thinking Tell UsCurrent Thinking Tell Us
The Evolving Science, Epidemiology, and The Evolving Science, Epidemiology, and Foundation Role of Low Molecular Weight Heparin Foundation Role of Low Molecular Weight Heparin
in the Setting of Cancerin the Setting of Cancer
Program ChairmanProgram ChairmanAjay Kakkar, MBBS, PhD, FRCSAjay Kakkar, MBBS, PhD, FRCSHead of the Centre for Surgical SciencesHead of the Centre for Surgical Sciences
Barts and the London Barts and the London Queen Mary’s School of Medicine and DentistryQueen Mary’s School of Medicine and Dentistry
The Thrombosis Research InstituteThe Thrombosis Research InstituteLondon, UKLondon, UK
Program ChairmanProgram ChairmanAjay Kakkar, MBBS, PhD, FRCSAjay Kakkar, MBBS, PhD, FRCSHead of the Centre for Surgical SciencesHead of the Centre for Surgical Sciences
Barts and the London Barts and the London Queen Mary’s School of Medicine and DentistryQueen Mary’s School of Medicine and Dentistry
The Thrombosis Research InstituteThe Thrombosis Research InstituteLondon, UKLondon, UK

COMORBIDITYCOMORBIDITYCONNECTIONCONNECTION
CAPCAPUTIUTICancerCancerHeart Failure Heart Failure ABE/COPDABE/COPDRespiratory FailureRespiratory Failure Myeloproliferative DisorderMyeloproliferative DisorderThrombophiliaThrombophiliaSurgerySurgeryHistory of DVTHistory of DVTOtherOther
SUBSPECIALISTSUBSPECIALISTSTAKEHOLDERSSTAKEHOLDERS
Infectious diseasesInfectious diseasesOncologyOncologyCardiology Cardiology Pulmonary medicinePulmonary medicineHematologyHematologyOncology/hematologyOncology/hematologyInterventional RadiologyInterventional RadiologyHospitalistHospitalistSurgeonsSurgeonsEMEMPCPPCP
Comorbidity ConnectionComorbidity Connection

Epidemiology of First-Time VTEEpidemiology of First-Time VTE
White R. Circulation. 2003;107:I-4 –I-8.)
Variable Variable FindingFinding
Seasonal Variation Seasonal Variation Possibly more common in winter Possibly more common in winter and less common in summerand less common in summer
Risk Factors Risk Factors 25% to 50% “idiopathic”25% to 50% “idiopathic”15%–25% associated with cancer15%–25% associated with cancer; ; 20% following surgery (3 mo.)20% following surgery (3 mo.)
Recurrent VTE Recurrent VTE 6-month incidence: 7%; 6-month incidence: 7%; higher rate in patients with cancerhigher rate in patients with cancerRecurrent PE more likely after PE Recurrent PE more likely after PE than after DVTthan after DVT
Death After Treated VTE Death After Treated VTE 30 day incidence 6% after 30 day incidence 6% after incident DVTincident DVT30 day incidence 12% after PE30 day incidence 12% after PEDeath strongly associated with Death strongly associated with cancercancer, age, and cardiovascular , age, and cardiovascular diseasedisease

Epidemiology of VTEEpidemiology of VTE
White R. Circulation. 2003;107:I-4 –I-8.)
► One major risk factor for VTE is ethnicity, with a One major risk factor for VTE is ethnicity, with a significantly higher incidence among significantly higher incidence among Caucasians and African Americans than among Caucasians and African Americans than among Hispanic persons and Asian-Pacific Islanders. Hispanic persons and Asian-Pacific Islanders.
► Overall, about 25% to 50% of patient with first-Overall, about 25% to 50% of patient with first-time VTE have an idiopathic condition, without time VTE have an idiopathic condition, without a readily identifiable risk factor. a readily identifiable risk factor.
► Early mortality after VTE is strongly associated Early mortality after VTE is strongly associated with presentation as PE, advanced age, with presentation as PE, advanced age, cancer,cancer, and underlying cardiovascular disease. and underlying cardiovascular disease.

Comorbidity ConnectionComorbidity Connection
ComorbidityComorbidityConnectionConnection
Overview Overview

Acute Medical Illness and VTEAcute Medical Illness and VTE
Acute MedicalAcute Medical Relative RiskRelative Risk Illness Illness Risk Risk XX22 PP Value ValueHeart failure Heart failure 1.08 (0.72-1.62) 1.08 (0.72-1.62) 0.05 0.05 .82.82NYHA class III NYHA class III 0.89 (0.55-1.43) 0.89 (0.55-1.43) 0.12 0.12 .72.72NYHA class IV NYHA class IV 1.48 (0.84-2.6) 1.48 (0.84-2.6) 1.23 1.23 .27.27
AcuteAcuterespiratory respiratory disease disease 1.26 (0.85-1.87) 1.26 (0.85-1.87) 1.03 1.03 .31.31
Acute Acute infectious infectious disease disease 1.50 (1.00-2.26) 1.50 (1.00-2.26) 3.54 3.54 .06.06
Acute Acute rheumatic rheumatic disease disease 1.45 (0.84-2.50) 1.45 (0.84-2.50) 1.20 1.20 .27.27
Among Patients Receiving Placebo orAmong Patients Receiving Placebo or Ineffective Antithrombotic TherapyIneffective Antithrombotic Therapy
Alikhan R, Cohen A, et al. Arch Intern Med. 2004;164:963-968

Acute Medical Illness and VTEAcute Medical Illness and VTE
Risk FactorRisk Factor Odds RatioOdds Ratio XX22
(95% CI)(95% CI)
Age >75 y Age >75 y 1.03 (1.00-1.06) 1.03 (1.00-1.06) 0.00010.0001Cancer Cancer 1.62 (0.93-2.75) 1.62 (0.93-2.75) 0.080.08Previous VTE Previous VTE 2.06 (1.10-3.69) 2.06 (1.10-3.69) 0.020.02
Acute Acute infectious infectious disease disease 1.74 (1.12-2.75) 1.74 (1.12-2.75) 0.020.02
Chronic Chronic respiratory respiratory disease disease 0.60 (0.38-0.92) 0.60 (0.38-0.92) 0.020.02
Multivariate Logistic Regression ModelMultivariate Logistic Regression Modelfor Definite Venous Thromboembolism (VTE)for Definite Venous Thromboembolism (VTE)
Alikhan R, Cohen A, et al. Arch Intern Med. 2004;164:963-968

Comorbid Condition and DVT Risk Comorbid Condition and DVT Risk
► Hospitalization for surgery (24%) and for medical illness (22%) Hospitalization for surgery (24%) and for medical illness (22%) accounted for a similar proportion of the cases, while nursing accounted for a similar proportion of the cases, while nursing home residence accounted for 13%.home residence accounted for 13%.
► The individual attributable risk estimates for The individual attributable risk estimates for malignant malignant neoplasmneoplasm, trauma, congestive heart failure, central venous , trauma, congestive heart failure, central venous catheter or pacemaker placement, neurological disease with catheter or pacemaker placement, neurological disease with extremity paresis, and superficial vein thrombosis were extremity paresis, and superficial vein thrombosis were 18%,18%, 12%, 10%, 9%, 7%, and 5%, respectively.12%, 10%, 9%, 7%, and 5%, respectively.
► Together, the 8 risk factors accounted for 74% of disease Together, the 8 risk factors accounted for 74% of disease occurrenceoccurrence
Heit JA, O'Fallon WM, Petterson TM, Lohse CM, Silverstein MD, Mohr DN, Melton LJ 3rd. Heit JA, O'Fallon WM, Petterson TM, Lohse CM, Silverstein MD, Mohr DN, Melton LJ 3rd. Arch Intern MedArch Intern Med. 2002 Jun 10;162(11):1245-8. Relative impact of risk factors for deep vein . 2002 Jun 10;162(11):1245-8. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study thrombosis and pulmonary embolism: a population-based study

VTE RecurrenceVTE Recurrence
BaselineBaseline Hazard RatioHazard RatioCharacteristicCharacteristic (95% CI)(95% CI)
AgeAge 1.17 (1.11-1.24)1.17 (1.11-1.24)
Body Mass IndexBody Mass Index 1.24 (1.04-1.47)1.24 (1.04-1.47)
Neurologic disease withNeurologic disease with 1.87 (1.28-2.73)1.87 (1.28-2.73)extremity paresisextremity paresis
Malignant neoplasmMalignant neoplasm None 1.00None 1.00 With chemotherapyWith chemotherapy 4.24 (2.58-6.95)4.24 (2.58-6.95) Without chemotherapyWithout chemotherapy 2.21 (1.60-3.06)2.21 (1.60-3.06)
Predictors of First Overall VTE RecurrencePredictors of First Overall VTE Recurrence
Heit J, Mohr D, et al. Arch Intern Med. 2000;160:761-768

Cancer Surgery, Thrombosis, and the Cancer Surgery, Thrombosis, and the Biology of MalignancyBiology of Malignancy
A Science-to-Strategy Perspective—The A Science-to-Strategy Perspective—The Foundation Role of LWMH at the Interface of Foundation Role of LWMH at the Interface of
Thrombosis and Cancer Thrombosis and Cancer
Cancer Surgery, Thrombosis, and the Cancer Surgery, Thrombosis, and the Biology of MalignancyBiology of Malignancy
A Science-to-Strategy Perspective—The A Science-to-Strategy Perspective—The Foundation Role of LWMH at the Interface of Foundation Role of LWMH at the Interface of
Thrombosis and Cancer Thrombosis and Cancer
Program ChairmanProgram ChairmanAjay Kakkar, MBBS, PhD, FRCSAjay Kakkar, MBBS, PhD, FRCSHead of the Centre for Surgical SciencesHead of the Centre for Surgical Sciences
Barts and the London Barts and the London Queen Mary’s School ofQueen Mary’s School ofMedicine and DentistryMedicine and Dentistry
The Thrombosis Research InstituteThe Thrombosis Research InstituteLondon, UKLondon, UK
Program ChairmanProgram ChairmanAjay Kakkar, MBBS, PhD, FRCSAjay Kakkar, MBBS, PhD, FRCSHead of the Centre for Surgical SciencesHead of the Centre for Surgical Sciences
Barts and the London Barts and the London Queen Mary’s School ofQueen Mary’s School ofMedicine and DentistryMedicine and Dentistry
The Thrombosis Research InstituteThe Thrombosis Research InstituteLondon, UKLondon, UK
Clotting, Cancer, and ControversiesClotting, Cancer, and Controversies

AuthorAuthor YearYear No. of No. of studiesstudies
Cancer mortalityCancer mortality
UFHUFH LMWHLMWH
GreenGreen 19921992 22 21/67 (31%)21/67 (31%) 7/62 (11%)7/62 (11%)
SiragusaSiragusa 19951995 1313 23/81 (28%)23/81 (28%) 10/74 (14%)10/74 (14%)
Meta-analysis of Meta-analysis of DVT Treatment StudiesDVT Treatment Studies

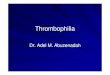
Famous: Trial DesignFamous: Trial Design
Treatment for 1 year or until deathTreatment for 1 year or until death
1º Endpoint: 1 year mortality (50% 1º Endpoint: 1 year mortality (50% 35%) 35%)2º Endpoints: VTE and bleeding2º Endpoints: VTE and bleeding
RRAdvanced solid Advanced solid tumour malignancytumour malignancy
N/Saline placeboN/Saline placebo
Dalteparin Dalteparin 5000 IU od5000 IU od
Kakkar AK, et al. J Clin Oncol. 2004;22:1944-1948.Kakkar AK, et al. J Clin Oncol. 2004;22:1944-1948.

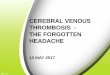
Kaplan–Meier survival curves for all ITT Kaplan–Meier survival curves for all ITT patients in dalteparin and placebo groupspatients in dalteparin and placebo groups
Kap
lan
–Mei
er s
urv
ival
dis
trib
uti
on
K
apla
n–M
eier
su
rviv
al d
istr
ibu
tio
n
fun
ctio
n e
stim
ate
fun
ctio
n e
stim
ate
0 12 24 36 48 60 72 84
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Time from randomisation (months)Time from randomisation (months)
No. at risk:No. at risk:
DalteparinDalteparinPlaceboPlacebo
190190 8585 3030 2222 1212 55 44 DalteparinDalteparin184184 7272 1515 99 88 55 22 PlaceboPlacebo
Kakkar AK, et al. J Clin Oncol. 2004;22:1944-1948.Kakkar AK, et al. J Clin Oncol. 2004;22:1944-1948.

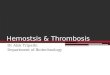
Survival Analysis: Survival Analysis: Good Prognosis PatientsGood Prognosis Patients
Kap
lan
–Mei
er s
urv
ival
dis
trib
uti
on
K
apla
n–M
eier
su
rviv
al d
istr
ibu
tio
n
esti
mat
ees
tim
ate
17 23 29 35 41 47 53 5917 23 29 35 41 47 53 59 65 65 71 77 8371 77 83
1.01.0
0.90.9
0.80.8
0.70.7
0.60.6
0.50.5
0.40.4
0.30.3
0.20.2
0.00.0
4747 17 10 9 917 10 9 9 8 8 5 3 2 8 8 5 3 2 0 0 PlaceboPlacebo55 31 26 22 20 13 8 5 5 555 31 26 22 20 13 8 5 5 5 3 Dalteparin3 Dalteparin
Time from randomisation (months)Time from randomisation (months)
No. at risk:No. at risk:
DalteparinDalteparinPlaceboPlacebo
Kakkar AK, et al. J Clin Oncol. 2004;22:1944-1948.Kakkar AK, et al. J Clin Oncol. 2004;22:1944-1948.

LMWH and Survival: LMWH and Survival: Further Studies (2003)Further Studies (2003)
Solid tumor malignancy and acute VTE
All patients received dalteparin200 IU/kg od 5–7 days
R
Dalteparin1 month 200 IU/kg od5 months 160 IU/kg od
Oral anticoagulant6 months
Small cell lung cancer (SCLC)
Patients with responsive limited disease received thoracic radiotherapy
Chemotherapy plus dalteparin 5000 IU od18 weeks
Chemotherapy (cyclophosphamide, epirubicin, vincristine)18 weeks
Solid tumor malignancy
Nadroparin2 weeks therapeutic dose4 weeks 1/2 therapeutic dose
Placebo6 weeks
CLOT
SCLC study
MALT
R
R
Klerk CPW, et al. Klerk CPW, et al. J Clin OncolJ Clin Oncol. 2005;23:2130-2135.. 2005;23:2130-2135.Altinbas M, et al. Altinbas M, et al. J Thromb HaemostJ Thromb Haemost. 2004;2:1-6.. 2004;2:1-6.
Lee, et.al. Lee, et.al. N Engl J Med, N Engl J Med, 2003;349:1462003;349:146

SCLC Study Survival CurvesSCLC Study Survival Curves
1.0
0.8
0.6
0.4
0.2
0.0
0 5 10 15 20 25 30 35 40
Months after randomization
Pro
bab
ility
of
surv
ival
Good prognosis population
limited disease1.0
0.8
0.6
0.4
0.2
0.0
0 5 10 15 20 25 30 35 40
Months after randomization
Pro
bab
ility
of
surv
ival
Overall population
p=0.01 p=0.007
DalteparinDalteparin
Placebo Placebo
Altinbas M, et al. J Thromb Haemost. 2004;2:1-6.Altinbas M, et al. J Thromb Haemost. 2004;2:1-6.

CLOT Survival CurvesCLOT Survival CurvesP
rob
abili
ty o
f su
rviv
al (
%)
Dalteparin
OAC
Days after randomization
0
10
20
30
40
50
60
70
80
90
100
0 30 60 90 120 150 180 210 240 270 300 330 360 390
OAC
Dalteparin
Pro
bab
ility
of
surv
ival
(%
)
0
10
20
30
40
50
60
70
80
90
100
0 30 60 90 120 150 180 210 240 270 300 330 360 390
Overall population Good prognosis population
without metastases
p=0.62
p=0.03
Days after randomization
Lee, et.al. Lee, et.al. N Engl J Med, N Engl J Med, 2003;349:1462003;349:146

MALT Survival CurvesMALT Survival Curves
Pro
bab
ility
of
Su
rviv
al
1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 36 48 60 72 84 96
Months after randomization
Placebo
Nadroparin
p=0.010
1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 36 48 60 72 84 96
Months after randomization
Pro
bab
ility
of
Su
rviv
al
Placebo
Nadroparin
p=0.021
Overall population Good prognosis population
>6 months survival
Klerk CPW, et al. J Clin Oncol. 2005;23:2130-2135.Klerk CPW, et al. J Clin Oncol. 2005;23:2130-2135.

Mechanistic explanationsMechanistic explanations
VTE Coagulation Protease Direct Heparin OtherVTE Coagulation Protease Direct Heparin Other
LMWH and Prolonged Cancer SurvivalLMWH and Prolonged Cancer Survival

Silver Silver In: In: The Hematologist - modified from Blom et. al. The Hematologist - modified from Blom et. al. JAMAJAMA 2005;293:715 2005;293:715
• Population-based case-control (MEGA) study
• N=3220 consecutive patients with 1st VTE vs. n=2131 control subjects
• CA patients = 7x OR for VTE vs. non-CA patients
Effect of Malignancy on Risk of Effect of Malignancy on Risk of Venous Thromboembolism (VTE)Venous Thromboembolism (VTE)
0
10
20
30
40
50
Hem
ato
log
ical
Lu
ng
Gas
tro
inte
stin
al
Bre
ast
Dis
tan
tm
etas
tase
s
0 to
3 m
on
ths
3 to
12
mo
nth
s
1 to
3 y
ears
5 to
10
year
s
> 1
5 ye
ars
Ad
just
ed o
dd
s ra
tio
Type of cancer Time since cancer diagnosis
2828
22.222.220.320.3
4.94.9
19.819.8
53.553.5
14.314.3
2.62.61.11.13.63.6

Mechanisms of Cancer-Induced Mechanisms of Cancer-Induced Thrombosis: The InterfaceThrombosis: The Interface
1.1. Pathogenesis?Pathogenesis?
2.2. Biological significance?Biological significance?
33. Potential importance for cancer therapy?. Potential importance for cancer therapy?

Fibrinolytic activities:t-PA, u-PA, u-PAR, PAI-1, PAI-2
Procoagulant Activities
FIBRIN
Endothelial cells
IL-1, TNF-VEGF
Tumor cells
Monocyte
PMN leukocyte
Activation of coagulation
Platelets
Angiogenesis,Basement matrix degradation.
Falanga and Rickles, Falanga and Rickles, New Oncology:ThrombosisNew Oncology:Thrombosis, 2005, 2005
Interface of Biology and CancerInterface of Biology and Cancer

Pathogenesis of Thrombosis in Cancer – Pathogenesis of Thrombosis in Cancer – A Modification of Virchow’s TriadA Modification of Virchow’s Triad
1.1. StasisStasis Prolonged bed restProlonged bed rest Extrinsic compression of blood vessels by tumorExtrinsic compression of blood vessels by tumor
2.2. Vascular InjuryVascular Injury Direct invasion by tumorDirect invasion by tumor Prolonged use of central venous cathetersProlonged use of central venous catheters Endothelial damage by chemotherapy drugsEndothelial damage by chemotherapy drugs Effect of tumor cytokines on vascular endotheliumEffect of tumor cytokines on vascular endothelium
3.3. HypercoagulabilityHypercoagulability Tumor-associated procoagulants and cytokines (tissue Tumor-associated procoagulants and cytokines (tissue
factor, CP, TNFfactor, CP, TNF, IL-1, IL-1, VEGF, etc.), VEGF, etc.) Impaired endothelial cell defense mechanisms (APC Impaired endothelial cell defense mechanisms (APC
resistance; deficiencies of AT, Protein C and S) resistance; deficiencies of AT, Protein C and S) Enhanced selectin/integrin-mediated, adhesive interactions Enhanced selectin/integrin-mediated, adhesive interactions
between tumor cells,vascular endothelial cells, platelets and between tumor cells,vascular endothelial cells, platelets and host macrophageshost macrophages

Mechanisms of Cancer-Induced Mechanisms of Cancer-Induced Thrombosis: Clot and Cancer InterfaceThrombosis: Clot and Cancer Interface
► Pathogenesis?Pathogenesis?
► Biological signBiological significanificance?ce?
► Potential importance for cancer therapy?Potential importance for cancer therapy?

Activation of Blood Coagulation in CancerActivation of Blood Coagulation in CancerBiological Significance?Biological Significance?
► EpiphenomenonEpiphenomenon? ?
Is this a generic secondary event (as in Is this a generic secondary event (as in inflammation, where clot formation is an inflammation, where clot formation is an incidental finding)incidental finding)
Or, is clotting . . .Or, is clotting . . .
► A Primary Event?A Primary Event?
Linked to malignant transformation Linked to malignant transformation

TF
VEGF
Angiogenesis
Endothelial cellsEndothelial cells
IL-8IL-8
Blood CoagulationActivation
FIBRIN
PAR-2
Angiogenesis
FVII/FVIIaFVII/FVIIa
THROMBINTHROMBIN
Tumor Cell
TF
Falanga and Rickles, New Oncology:Thrombosis, 2005
Interface of Biology and CancerInterface of Biology and Cancer

Coagulation Cascade and TumorsCoagulation Cascade and Tumors
TFTF ThrombinThrombin
Clotting-Clotting-dependentdependent
Clotting-Clotting-dependentdependent
Clotting-Clotting-independentindependent
Clotting-Clotting-dependentdependent
ANGIOGENESISANGIOGENESIS
FibrinFibrin
Clotting-Clotting-independentindependent
PARsPARs
Tumor Growth And MetastasisTumor Growth And Metastasis
Fernandez, Patierno and Rickles. Sem Hem Thromb 2004;30:31

Regulation of Vascular Endothelial Growth Factor Production Regulation of Vascular Endothelial Growth Factor Production and Angiogenesis by the Cytoplasmic Tail of Tissue Factorand Angiogenesis by the Cytoplasmic Tail of Tissue Factor
1.1. TF regulates VEGF expression in human TF regulates VEGF expression in human melanoma cell linesmelanoma cell lines
2.2. Human cancer cells with increased TF are more Human cancer cells with increased TF are more angiogenic (and, therefore, more “metastatic’) angiogenic (and, therefore, more “metastatic’) in vivoin vivo due to high VEGF production due to high VEGF production
Abe et.al. Abe et.al. Proc Nat Acad SciProc Nat Acad Sci 1999;96:8663-8668 1999;96:8663-8668

3.3. The cytoplasmic tail of TF, which contains three The cytoplasmic tail of TF, which contains three serine residues, appears to play a role in serine residues, appears to play a role in regulating VEGF expression in human cancer regulating VEGF expression in human cancer cells, perhaps by mediating signal transductioncells, perhaps by mediating signal transduction
4.4. Data consistent with new mechanism(s) by Data consistent with new mechanism(s) by which TF signals VEGF synthesis in human which TF signals VEGF synthesis in human cancer cells; may provide insight into the cancer cells; may provide insight into the relationship between clotting and cancerrelationship between clotting and cancer
Abe et.al. Abe et.al. Proc Nat Acad SciProc Nat Acad Sci 1999;96:8663-8668 1999;96:8663-8668
Regulation of Vascular Endothelial Growth Factor Production Regulation of Vascular Endothelial Growth Factor Production and Angiogenesis by the Cytoplasmic Tail of Tissue Factorand Angiogenesis by the Cytoplasmic Tail of Tissue Factor

Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation
► Epiphenomenon?Epiphenomenon?
► Linked to malignant transformation?Linked to malignant transformation?
1.1. METMET oncogene induction produces DIC in oncogene induction produces DIC in human liver carcinomahuman liver carcinoma
(Boccaccio et. al. (Boccaccio et. al. NatureNature 2005;434:396-400) 2005;434:396-400)
2.2. PtenPten loss produces TF activation and loss produces TF activation and pseudopalisading necrosis in human pseudopalisading necrosis in human glioblastomaglioblastoma
(Rong et.al. (Rong et.al. Ca ResCa Res 2005;65:1406-1413) 2005;65:1406-1413)
3. 3. K-K-rasras oncogene, p53 inactivation and TF oncogene, p53 inactivation and TF induction in human colorectal carcinomainduction in human colorectal carcinoma
(Yu et.al. (Yu et.al. BloodBlood 2005;105:1734-1741) 2005;105:1734-1741)

► METMET encodes a tyrosine kinase receptor for encodes a tyrosine kinase receptor for hepatocyte growth factor/scatter factor (HGF/SF) hepatocyte growth factor/scatter factor (HGF/SF) Drives physiologicalDrives physiological cellular program of cellular program of
“invasive growth” (tissue morphogenesis, “invasive growth” (tissue morphogenesis, angiogenesis and repair)angiogenesis and repair)
Aberrant execution (e.g. hypoxia-induced Aberrant execution (e.g. hypoxia-induced transcription) is associated with neoplastic transcription) is associated with neoplastic transformation, invasion, and metastasistransformation, invasion, and metastasis
Boccaccio et al Boccaccio et al Nature Nature 2005;434:396-4002005;434:396-400
““1. 1. METMET Oncogene Drives a Genetic Programme Oncogene Drives a Genetic Programme Linking Cancer to Haemostasis”Linking Cancer to Haemostasis”
Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant in Cancer: Malignant TransformationTransformation

► Mouse model of Trousseau’s SyndromeMouse model of Trousseau’s Syndrome
Targeted activated human MET to the mouse Targeted activated human MET to the mouse liver with lentiviral vector and liver-specific liver with lentiviral vector and liver-specific promoter promoter slowly, progressive slowly, progressive hepatocarcinogenesishepatocarcinogenesis
Preceded and accompanied by a Preceded and accompanied by a thrombohemorrhagic syndrome thrombohemorrhagic syndrome Venous thrombosis in tail vein occurred early Venous thrombosis in tail vein occurred early
and was followed by fatal internal hemorrhageand was followed by fatal internal hemorrhage Syndrome characterized by Syndrome characterized by d-dimer and PT d-dimer and PT
and and platelet count (DIC) platelet count (DIC)
““METMET Oncogene Drives a Genetic Programme Oncogene Drives a Genetic Programme Linking Cancer to Haemostasis”Linking Cancer to Haemostasis”
““METMET Oncogene Drives a Genetic Programme Oncogene Drives a Genetic Programme Linking Cancer to Haemostasis”Linking Cancer to Haemostasis”

Blood Coagulation Parameters in Mice Blood Coagulation Parameters in Mice Transduced with the Transduced with the MET MET OncogeneOncogene
TransgeneTransgene ParameterParameter
Time after Transduction (days)Time after Transduction (days)
0 30 900 30 90
GFPGFP
__________________
MET MET
Platelets (x10Platelets (x1033))
D-dimer (D-dimer (µg/ml)µg/ml)
PT (s)PT (s)
________________________________
Platelets (x10Platelets (x1033))
D-dimer (µg/ml)D-dimer (µg/ml)
PT (s)PT (s)
968 656 800 968 656 800
<0.05 <0.05 <0.05<0.05 <0.05 <0.05
12.4 11.6 11.412.4 11.6 11.4
______________________________________________________________
974 350 150974 350 150
<0.05 0.11 0.22<0.05 0.11 0.22
12.9 11.8 25.112.9 11.8 25.1

Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation
2. “2. “PtenPten and Hypoxia Regulate Tissue Factor and Hypoxia Regulate Tissue Factor Expression and Plasma Coagulation By Expression and Plasma Coagulation By
Glioblastoma”Glioblastoma”► PtenPten = tumor suppressor with lipid and protein = tumor suppressor with lipid and protein
phosphatase activityphosphatase activity
► Loss or inactivation of Loss or inactivation of Pten Pten (70-80% of (70-80% of glioblastomas) leads to Akt activation and glioblastomas) leads to Akt activation and upregulation of upregulation of Ras/MEK/ERKRas/MEK/ERK signaling cascade signaling cascade
Rong, Brat et.al. Ca Res 2005;65:1406-1413

► Glioblastomas characterized histologically by Glioblastomas characterized histologically by “pseudopalisading necrosis” “pseudopalisading necrosis”
► Thought to be wave of tumor cells migrating Thought to be wave of tumor cells migrating away from a central hypoxic zone, perhaps away from a central hypoxic zone, perhaps created by thrombosiscreated by thrombosis
► Pseudopalisading cells produce VEGF and IL-8 Pseudopalisading cells produce VEGF and IL-8 and drive angiogenesis and rapid tumor growth and drive angiogenesis and rapid tumor growth
► TF expressed by >90% of grade 3 and 4 TF expressed by >90% of grade 3 and 4 malignant astrocytomas (but only 10% of malignant astrocytomas (but only 10% of grades 1 and 2)grades 1 and 2)
““PtenPten and Hypoxia Regulate Tissue Factor Expression and Hypoxia Regulate Tissue Factor Expression and Plasma Coagulation By Glioblastoma”and Plasma Coagulation By Glioblastoma”

Results:Results:
1.1. Hypoxia and Hypoxia and PTEN PTEN loss loss TF (mRNA, Ag and TF (mRNA, Ag and procoagulant activity); partially reversed with procoagulant activity); partially reversed with induction of induction of PTEN PTEN
2.2. PTEN PTEN effect independent of lipid phosphatase effect independent of lipid phosphatase activity; dependent on protein phosphatase activity; dependent on protein phosphatase
3.3. Both Both AktAkt and and RasRas pathways modulated TF in pathways modulated TF in sequentially transformed astrocytes.sequentially transformed astrocytes.
4.4. Ex vivo Ex vivo data: data: TF by immunohistochemical TF by immunohistochemical staining in pseudopalisades of 7 human staining in pseudopalisades of 7 human glioblastoma specimensglioblastoma specimens
““PtenPten and Hypoxia Regulate Tissue Factor Expression and Hypoxia Regulate Tissue Factor Expression and Plasma Coagulation By Glioblastoma”and Plasma Coagulation By Glioblastoma”

Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation
3. “Oncogenic Events Regulate Tissue Factor 3. “Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells: Implications Expression In Colorectal Cancer Cells: Implications For Tumor Progression And Angiogenesis”For Tumor Progression And Angiogenesis”
► Activation of K-Activation of K-ras ras oncogene and inactivation of oncogene and inactivation of p53 p53 tumor tumor suppressor suppressor TF expression in TF expression in human human colorectal cancer cellscolorectal cancer cells
► Transforming events dependent on MEK/MAPK and PI3KTransforming events dependent on MEK/MAPK and PI3K► Cell-associated and MP-associated TF activity linked to genetic Cell-associated and MP-associated TF activity linked to genetic
status of cancer cellsstatus of cancer cells► TF siRNA reduced cell surface TF expression, tumor growth TF siRNA reduced cell surface TF expression, tumor growth
and angiogenesis and angiogenesis ► TF may be required for K-TF may be required for K-ras-ras-driven phenotypedriven phenotype
Yu, Mackman, Rak et.al. Yu, Mackman, Rak et.al. Blood Blood 2005;105:1734-412005;105:1734-41

““Oncogenic Events Regulate Tissue Factor Expression In Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells: Implications For Tumor Colorectal Cancer Cells: Implications For Tumor
Progression And Angiogenesis”Progression And Angiogenesis”TF expression in cancer cells parallels genetic tumor progression
with an impact of K-ras and p53 status
Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation
Yu, Mackman, Rak et.al. Yu, Mackman, Rak et.al. Blood Blood 2005;105:1734-412005;105:1734-41
0
50
100
150
200
250
300
350
400
450
HKh-2 HCT116 379.2
0
20
40
60
80
100
120
140
160
HKh-2 HCT116 379.2Mea
n C
ha
nn
el T
F F
lou
res
cen
ce
Mea
n C
ha
nn
el T
F F
lou
res
cen
ce
TF
Ac
tiv
ity
(U
/10
TF
Ac
tiv
ity
(U
/1066
cell
s)
cel
ls)
del/+del/+ mut/+mut/+ mut/+mut/++/++/+ +/++/+ del/deldel/del

““Oncogenic Events Regulate Tissue Factor Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells: Expression In Colorectal Cancer Cells:
Implications For Tumor Progression And Implications For Tumor Progression And Angiogenesis”Angiogenesis”
Effect of TF si mRNA on tumor growth in vitro and in vivo
Yu, Mackman, Rak et.al. Yu, Mackman, Rak et.al. Blood Blood 2005;105:1734-412005;105:1734-41
Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation

0
2
4
6
8
10
12
14
HCT116 SI-2 SI-3 MG only
Effect of TF si mRNA on new vessel formation in colon cancerEffect of TF si mRNA on new vessel formation in colon cancer
““Oncogenic Events Regulate Tissue Factor Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells”Expression In Colorectal Cancer Cells”
Yu, Mackman, Rak et.al. Yu, Mackman, Rak et.al. Blood Blood 2005;105:1734-412005;105:1734-41
%V
WF
-Po
siti
ve A
rea
%V
WF
-Po
siti
ve A
rea

““Oncogenic Events Regulate Tissue Factor Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells: Implications Expression In Colorectal Cancer Cells: Implications
For Tumor Progression And Angiogenesis”For Tumor Progression And Angiogenesis”
Matrigel Assay: (D) HCT 116; (E) SI-3 cells – vWF immunohistology
Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation
Yu, Mackman, Rak et.al. Yu, Mackman, Rak et.al. Blood Blood 2005;105:1734-412005;105:1734-41

Mechanisms of Cancer-Induced Mechanisms of Cancer-Induced Thrombosis: ImplicationsThrombosis: Implications
1.1. Pathogenesis?Pathogenesis?
2.2. Biological significance?Biological significance?
3.3. Potential importance for Potential importance for cancer therapy?cancer therapy?

A Systematic Overview of VTE A Systematic Overview of VTE Prophylaxis In The Prophylaxis In The Setting of Cancer Setting of Cancer
Linking Science to Clinical PracticeLinking Science to Clinical Practice
A Systematic Overview of VTE A Systematic Overview of VTE Prophylaxis In The Prophylaxis In The Setting of Cancer Setting of Cancer
Linking Science to Clinical PracticeLinking Science to Clinical Practice
Craig M. Kessler, MDCraig M. Kessler, MDProfessor of Medicine and PathologyProfessor of Medicine and Pathology
Georgetown University Medical CenterGeorgetown University Medical CenterDirector of the Division of CoagulationDirector of the Division of Coagulation
Department of Laboratory MedicineDepartment of Laboratory MedicineLombardi Comprehensive Cancer CenterLombardi Comprehensive Cancer Center
Washington, DCWashington, DC
Craig M. Kessler, MDCraig M. Kessler, MDProfessor of Medicine and PathologyProfessor of Medicine and Pathology
Georgetown University Medical CenterGeorgetown University Medical CenterDirector of the Division of CoagulationDirector of the Division of Coagulation
Department of Laboratory MedicineDepartment of Laboratory MedicineLombardi Comprehensive Cancer CenterLombardi Comprehensive Cancer Center
Washington, DCWashington, DC
Clotting, Cancer, and ControversiesClotting, Cancer, and Controversies

VTE and Cancer: EpidemiologyVTE and Cancer: Epidemiology
► Of all cases of VTE:Of all cases of VTE: About 20% occur in cancer patientsAbout 20% occur in cancer patients Annual incidence of VTE in cancer Annual incidence of VTE in cancer
patients ≈ 1/250patients ≈ 1/250
► Of all cancer patients:Of all cancer patients: 15% will have symptomatic VTE15% will have symptomatic VTE As many as 50% have VTE at autopsyAs many as 50% have VTE at autopsy
► Compared to patients without cancer:Compared to patients without cancer: Higher risk of first and recurrent VTEHigher risk of first and recurrent VTE Higher risk of bleeding on anticoagulantsHigher risk of bleeding on anticoagulants Higher risk of dyingHigher risk of dying
Lee AY, Levine MN. Lee AY, Levine MN. CirculationCirculation. 2003;107:23 Suppl 1:I17-I21. 2003;107:23 Suppl 1:I17-I21

1.1. Ambrus JL et al. Ambrus JL et al. J MedJ Med. 1975;6:61-64. 1975;6:61-642.2. Donati MB. Donati MB. HaemostasisHaemostasis. 1994;24:128-131. 1994;24:128-1313.3. Johnson MJ et al. Johnson MJ et al. Clin Lab HaemClin Lab Haem. 1999;21:51-54. 1999;21:51-544.4. Prandoni P et al. Prandoni P et al. Ann Intern MedAnn Intern Med. 1996;125:1-7. 1996;125:1-7
DVT and PE in Cancer DVT and PE in Cancer Facts, Findings, and Natural HistoryFacts, Findings, and Natural History
► VTE is the second leading cause of deathVTE is the second leading cause of death in in hospitalized cancer patientshospitalized cancer patients1,21,2
► The risk of VTE in cancer patients undergoing The risk of VTE in cancer patients undergoing surgery is surgery is 3- to 5-fold higher3- to 5-fold higher than those without than those without cancercancer22
► Up to Up to 50% of cancer patients50% of cancer patients may have may have evidence of evidence of asymptomatic DVT/PEasymptomatic DVT/PE33
► Cancer patients with symptomatic DVT exhibit a Cancer patients with symptomatic DVT exhibit a high risk for recurrent DVT/PE that persists for high risk for recurrent DVT/PE that persists for many yearsmany years44

Clinical Features of VTE in CancerClinical Features of VTE in Cancer
► VTE has significant negative impact on VTE has significant negative impact on quality of lifequality of life
► VTE may be the presenting sign of occult VTE may be the presenting sign of occult malignancymalignancy• 10% with idiopathic VTE develop 10% with idiopathic VTE develop
cancer within 2 yearscancer within 2 years• 20% have recurrent idiopathic VTE20% have recurrent idiopathic VTE• 25% have bilateral DVT25% have bilateral DVT
Bura Bura et. al.,et. al., J Thromb HaemostJ Thromb Haemost 2004;2:445-51 2004;2:445-51

Risk Factors for Cancer-Associated VTERisk Factors for Cancer-Associated VTE
► CancerCancer Type Type
• Men: prostate, colon, brain, lungMen: prostate, colon, brain, lung• Women: breast, ovary, lungWomen: breast, ovary, lung
StageStage
► TreatmentsTreatments SurgerySurgery
• 10-20% proximal DVT10-20% proximal DVT• 4-10% clinically evident PE4-10% clinically evident PE• 0.2-5% fatal PE0.2-5% fatal PE
SystemicSystemic Central venous cathetersCentral venous catheters (~4% generate (~4% generate
clinically relevant VTE)clinically relevant VTE)

Thrombosis and Survival:Thrombosis and Survival:Likelihood of Death After HospitalizationLikelihood of Death After Hospitalization
0 20 40 60 80 100 120140 160 1800.00
0.20
0.40
1.00
0.80
0.60
DVT/PE and Malignant DiseaseDVT/PE and Malignant Disease
Malignant DiseaseMalignant Disease
DVT/PE OnlyDVT/PE Only
Nonmalignant DiseaseNonmalignant Disease
Number of Days
Pro
bab
ilit
y o
f D
eath
Levitan N, et al. Medicine 1999;78:285Levitan N, et al. Medicine 1999;78:285

As Number Of Cancer Survivors As Number Of Cancer Survivors Increases, VTE Rates Increase Increases, VTE Rates Increase
YEARYEAR
0
0.5
1
1.5
2
2.5
3
3.5
4
79 81 83 85 87 89 91 93 95 97 99
VT
E in
Ho
spit
aliz
ed C
ance
rV
TE
in H
osp
ital
ized
Can
cer
An
d N
on
can
cer
Pat
ien
ts (
%)
An
d N
on
can
cer
Pat
ien
ts (
%)
Stein PD, et al. Am J Med 2006; 119: 60-68Stein PD, et al. Am J Med 2006; 119: 60-68
Cancer PatientsCancer Patients
Noncancer PatientsNoncancer Patients

VTE Risk And Cancer Type:VTE Risk And Cancer Type:“Solid And Liquid”“Solid And Liquid”
Stein PD, et al. Am J Med 2006; 119: 60-68Stein PD, et al. Am J Med 2006; 119: 60-68
Rel
ativ
e R
isk
of
VT
E in
Rel
ativ
e R
isk
of
VT
E in
Can
cer
Pat
ien
tsC
ance
r P
atie
nts
Pan
crea
sP
ancr
eas
Bra
inB
rain
Mye
lop
rol
Mye
lop
rol
Sto
mac
hS
tom
ach
Lym
ph
om
aL
ymp
ho
ma
Ute
rus
Ute
rus
Lu
ng
Lu
ng
Eso
ph
agu
sE
sop
hag
us
Pro
stat
eP
rost
ate
Rec
tal
Rec
tal
Kid
ney
Kid
ney
Co
lon
Co
lon
Ova
ryO
vary
Liv
erL
iver
Leu
kem
iaL
euke
mia
Bre
ast
Bre
ast
Cer
vix
Cer
vix
Bla
dd
erB
lad
der
4.54.5
44
3.53.5
33
2.52.5
22
1.51.5
11
0.50.5
Relative Risk of VTE Ranged From 1.02 to 4.34Relative Risk of VTE Ranged From 1.02 to 4.34

Thrombosis Risk In Cancer
Primary Prophylaxis
► SurgerySurgery
► ChemotherapyChemotherapy
► RadiotherapyRadiotherapy
► Central Venous CathetersCentral Venous Catheters
► Acute Illness (immobilization)Acute Illness (immobilization)

Prevention and ManagementPrevention and Managementof VTE in Cancerof VTE in Cancer
► Sparse data specifically related to cancer Sparse data specifically related to cancer patients was available until recentlypatients was available until recently
► Cancer patients are a small subset (< 20%) in Cancer patients are a small subset (< 20%) in most of the largest trials of antithrombotic most of the largest trials of antithrombotic therapytherapy
► Therefore, until the last two or three years, we Therefore, until the last two or three years, we needed to extrapolate from non-cancer needed to extrapolate from non-cancer patients, bearing in mind that cancer patients patients, bearing in mind that cancer patients are in the highest risk groupsare in the highest risk groups

PharmacologicPharmacologic(Prophylaxis & Treatment)(Prophylaxis & Treatment)
Low MolecularLow MolecularWeight HeparinWeight Heparin
(LMWH)(LMWH)
NonpharmacologicNonpharmacologic(Prophylaxis)(Prophylaxis)
UnfractionatedUnfractionatedHeparin (UH)Heparin (UH)
OralOral AnticoagulantsAnticoagulants
ElasticElasticStockingsStockings
InferiorInferiorVena CavaVena Cava
FilterFilter
IntermittentIntermittentPneumaticPneumatic
CompressionCompression
Antithrombotic Therapy: ChoicesAntithrombotic Therapy: Choices
New Agents: e.g. New Agents: e.g. Fondaparinux,Fondaparinux,Direct anti-Xa inhibitors,Direct anti-Xa inhibitors,Direct anti-IIa, etc.?Direct anti-IIa, etc.?

► Cancer patients have Cancer patients have 2-fold risk of post-2-fold risk of post-operative DVT/PE and >3-fold risk of fatal operative DVT/PE and >3-fold risk of fatal PE despite prophylaxisPE despite prophylaxis::
Kakkar AK, et al. Kakkar AK, et al. Thromb HaemostThromb Haemost 2001; 86 (suppl 1): OC1732 2001; 86 (suppl 1): OC1732
Incidence of VTE in Surgical PatientsIncidence of VTE in Surgical Patients
No CancerNo CancerN=16,954N=16,954
CancerCancerN=6124N=6124
P-valueP-value
Post-op VTEPost-op VTE 0.61%0.61% 1.26%1.26% <0.0001<0.0001
Non-fatal PENon-fatal PE 0.27%0.27% 0.54%0.54% <0.0003<0.0003
Autopsy PEAutopsy PE 0.11%0.11% 0.41%0.41% <0.0001<0.0001
DeathDeath 0.71%0.71% 3.14%3.14% <0.0001<0.0001

Natural History of VTE in Cancer Natural History of VTE in Cancer Surgery: Surgery: The @RISTOS RegistryThe @RISTOS Registry
► Web-Based Registry of Cancer SurgeryWeb-Based Registry of Cancer Surgery Tracked 30-day incidence of VTE in 2373 patientsTracked 30-day incidence of VTE in 2373 patients
Type of surgeryType of surgery • • 52% General 52% General • • 29% Urological29% Urological • • 19% Gynecologic19% Gynecologic
82% received in-hospital thromboprophylaxis82% received in-hospital thromboprophylaxis
31% received post-discharge thromboprophylaxis31% received post-discharge thromboprophylaxis
FindingsFindings
► 2.1% incidence of clinically overt VTE (0.8% fatal)2.1% incidence of clinically overt VTE (0.8% fatal)
► Most events occur after hospital discharge Most events occur after hospital discharge
► Most common cause of 30-day post-op deathMost common cause of 30-day post-op death
Agnelli, abstract OC191, ISTH 2003Agnelli, abstract OC191, ISTH 2003

Nilsson: Arch Surg, 142;2007:126–132Nilsson: Arch Surg, 142;2007:126–132
Colorectal Cancer Resection
Association Between Transfusion and Venous Thromboembolism Stratified by Sex Association Between Transfusion and Venous Thromboembolism Stratified by Sex in 14,104 Patients Undergoing Colorectal Cancer Resection in Maryland, 1994-2000in 14,104 Patients Undergoing Colorectal Cancer Resection in Maryland, 1994-2000
VariableVariable Incidence of VTE, %Incidence of VTE, % P ValueP Value Stratified ORStratified OR AdjustedAdjusted(95% CI)*(95% CI)* P ValueP Value
Male SexMale Sex No Transfusion (n = 5683)No Transfusion (n = 5683) 0.70.7 ReferentReferent Transfusion (n = 1156)Transfusion (n = 1156) 0.80.8 .84.84 0.9 (0.5-1.9)0.9 (0.5-1.9) .85.85
Female SexFemale Sex No Transfusion (n = 5565)No Transfusion (n = 5565) 0.90.9 ReferentReferent Transfusion (n = 1610)Transfusion (n = 1610) 2.12.1 <.<.001001 1.8 (1.2-2.6)1.8 (1.2-2.6) .004.004
Overall, 1% incidence of VTE with 3.8 fold mortality
Transfused women 1.8-fold more likely to develop VTE than non-transfused women
Overall, 1% incidence of VTE with 3.8 fold mortality
Transfused women 1.8-fold more likely to develop VTE than non-transfused women

► Age >40 yearsAge >40 years
► Cancer procoagulantsCancer procoagulants
► ThrombophiliasThrombophilias
► Adjuvant chemotherapy or hormonal Adjuvant chemotherapy or hormonal treatmenttreatment
► Complicated, lengthy surgery (tissue Complicated, lengthy surgery (tissue trauma, immobilization)trauma, immobilization)
► Debilitation and slower recoveryDebilitation and slower recovery
► Indwelling venous accessIndwelling venous access
VTE Risk Factors in Surgical VTE Risk Factors in Surgical Oncology PatientsOncology Patients

Clinical thromboembolismClinical thromboembolism CancerCancer
0 1.0 2.0 3.0 4.00 1.0 2.0 3.0 4.0
Major hemorrhageMajor hemorrhage
Asymptomatic DVTAsymptomatic DVT
Clinical PEClinical PE
DeathDeath
Total hemorrhageTotal hemorrhage
Wound hematomaWound hematoma
TransfusionTransfusion
Non-cancerNon-cancer
Mismetti P et al. Br J Surg 2001;88:913–30Mismetti P et al. Br J Surg 2001;88:913–30
Surgical ProphylaxisSurgical Prophylaxis
LMWH betterLMWH better UFH betterUFH better

LMWH vs. UFHLMWH vs. UFH► Abdominal or pelvic surgery for cancer (mostly Abdominal or pelvic surgery for cancer (mostly
colorectal)colorectal)
► LMWH once daily vs. UFH tid for 7–10 days post-opLMWH once daily vs. UFH tid for 7–10 days post-op
► DVT on venography at day 7–10 and symptomatic VTEDVT on venography at day 7–10 and symptomatic VTE
1. ENOXACAN Study Group. 1. ENOXACAN Study Group. Br J SurgBr J Surg 1997;84:1099–103 1997;84:1099–1032. McLeod R, et al. 2. McLeod R, et al. Ann SurgAnn Surg 2001;233:438-444 2001;233:438-444
Prophylaxis in Surgical PatientsProphylaxis in Surgical Patients
StudyStudy NN DesignDesign RegimensRegimens
ENOXACAN ENOXACAN 11 631631 double-blinddouble-blind enoxaparin vs. UFHenoxaparin vs. UFH
Canadian Colorectal Canadian Colorectal DVT Prophylaxis DVT Prophylaxis 22 475475 double-blinddouble-blind enoxaparin vs. UFHenoxaparin vs. UFH

Prophylaxis in Surgical PatientsProphylaxis in Surgical Patients
0%
5%
10%
15%
20%
UFH 5000 U tid
enoxaparin 40 mg
VTE Major Bleeding
In
cid
ence
of
Ou
tco
me
Eve
nt
ENOXACAN ENOXACAN 14.7%14.7%
2.9% 4.1%2.9% 4.1%
18.2%
N=319N=319
N=312N=312
ENOXACAN Study Group. Br J Surg 1997;84:1099–103
P>0.05P>0.05

0%
5%
10%
15%
20%
UFH 5000 U tid
enoxaparin 40 mg
Canadian Canadian Colorectal DVT Colorectal DVT Prophylaxis TrialProphylaxis Trial
13.9%13.9%
1.5% 2.7%1.5% 2.7%
16.9%16.9%
N=234N=234
N=241N=241
McLeod R, et al. McLeod R, et al. Ann SurgAnn Surg 2001;233:438-444 2001;233:438-444
P=0.052P=0.052
In
cid
ence
of
Ou
tco
me
Eve
nt
VTEVTE Major BleedingMajor Bleeding(Cancer) (All)(Cancer) (All)
Prophylaxis in Surgical PatientsProphylaxis in Surgical Patients

Extended prophylaxisExtended prophylaxis► Abdominal or pelvic surgery for cancerAbdominal or pelvic surgery for cancer
► LMWH for ~ 7 days vs. 28 days post-opLMWH for ~ 7 days vs. 28 days post-op
► Routine bilateral venography at ~day 28Routine bilateral venography at ~day 28
1. Bergqvist D, et al. (for the ENOXACAN II investigators) 1. Bergqvist D, et al. (for the ENOXACAN II investigators) N Engl J MedN Engl J Med 2002;346:975-980 2002;346:975-980 2. Rasmussen M, et al (FAME) 2. Rasmussen M, et al (FAME) BloodBlood 2003;102:56a 2003;102:56a
Prophylaxis in Surgical PatientsProphylaxis in Surgical Patients
StudyStudy NN DesignDesign RegimensRegimens
ENOXACAN IIENOXACAN II 332332 Double-blindDouble-blind Enoxaparin vs. placeboEnoxaparin vs. placebo
FAME FAME (subgroup)(subgroup) 198198 Open-labelOpen-label Dalteparin vs. no Dalteparin vs. no
prophylaxisprophylaxis

0%
5%
10%
15%
placebo
enoxaparin 40 mg
VTE Prox Any MajorVTE Prox Any Major DVT Bleeding BleedingDVT Bleeding Bleeding
P=0.02P=0.02
5.1%5.1%
1.8%1.8%
Bergqvist D, et al. (for the ENOXACAN II investigators) Bergqvist D, et al. (for the ENOXACAN II investigators) N Engl J MedN Engl J Med 2002;346:975-980 2002;346:975-980
ENOXACAN IIENOXACAN II
In
cid
ence
of
Ou
tco
me
Eve
nt
Inci
den
ce o
f O
utc
om
e E
ven
t
N=167N=167
N=165N=165
0% 0.4%0% 0.4%
12.0%12.0%
4.8%4.8%
NNT = 14NNT = 140.6%0.6%
3.6%3.6%
Extended Prophylaxis inExtended Prophylaxis inSurgical PatientsSurgical Patients

► A multicenter, prospective, assessor-blinded, open-A multicenter, prospective, assessor-blinded, open-label, randomized trial: label, randomized trial: Dalteparin administered for Dalteparin administered for 28 days after major abdominal surgery28 days after major abdominal surgery compared to compared to 7 days of treatment7 days of treatment
► RESULTS:RESULTS: Cumulative Cumulative incidence of VTE was reduced incidence of VTE was reduced from 16.3% with short-term thromboprophylaxis from 16.3% with short-term thromboprophylaxis (29/178 patients) to 7.3%(29/178 patients) to 7.3% after prolonged after prolonged thromboprophylaxis (12/165) (thromboprophylaxis (12/165) (relative risk reduction relative risk reduction 55%;55%; 95% confidence interval 15-76; P=0.012). 95% confidence interval 15-76; P=0.012).
► CONCLUSIONS:CONCLUSIONS: 4-week administration of dalteparin, 4-week administration of dalteparin, 5000 IU once daily, after major abdominal surgery 5000 IU once daily, after major abdominal surgery significantly reduces the rate of VTEsignificantly reduces the rate of VTE, without , without increasing the risk of bleeding, compared with 1 increasing the risk of bleeding, compared with 1 week of thromboprophylaxis.week of thromboprophylaxis.
Major Abdominal Surgery: FAME Major Abdominal Surgery: FAME Investigators—Dalteparin Extended Investigators—Dalteparin Extended
Rasmussen, J Thromb Haemost. 2006 Nov;4(11):2384-90. Epub 2006 Aug 1.

► Paucity of level I/II studies in this populationPaucity of level I/II studies in this population
► Based on small historical studies:Based on small historical studies: Postoperative risk of DVT/PE varies 12%Postoperative risk of DVT/PE varies 12%––35%35%
LDUH (5000 u bid) ineffectiveLDUH (5000 u bid) ineffective
LDUH 5000 u tid reduces risk by 50%LDUH 5000 u tid reduces risk by 50%––60%60%
Once-daily LMWH comparable to LDUH for efficacy Once-daily LMWH comparable to LDUH for efficacy and safetyand safety
Gynecological Cancer SurgeryGynecological Cancer Surgery

Cochrane Systematic ReviewCochrane Systematic Review
► Meta-analysis of 8 randomized controlled trialsMeta-analysis of 8 randomized controlled trials
► Heparin reduces risk of DVT by 70% (95% CI Heparin reduces risk of DVT by 70% (95% CI 0.10–0.89)0.10–0.89)
► No evidence that anticoagulation reduces risk No evidence that anticoagulation reduces risk of PEof PE
► No statistical difference between LDUH and No statistical difference between LDUH and LMWH in efficacy and bleedingLMWH in efficacy and bleeding
Gynecological SurgeryGynecological Surgery
Oates-Whitehead et al. Oates-Whitehead et al. Cochrane Database Syst RevCochrane Database Syst Rev 2003;4:CD003679 2003;4:CD003679

Urological Cancer SurgeryUrological Cancer Surgery
Poorly studied populationPoorly studied population
Risk of VTE varies with type of surgery and diagnosisRisk of VTE varies with type of surgery and diagnosis
► Small studies have suggested prophylaxis with either LDUH or Small studies have suggested prophylaxis with either LDUH or LMWH is effective and safeLMWH is effective and safe
► Possible increased risk of pelvic hematoma and lymphocele Possible increased risk of pelvic hematoma and lymphocele formationformation
Kibel, Loughlin. Kibel, Loughlin. J UrolJ Urol. 1995;153:1763-1774. 1995;153:1763-1774
DVTDVT PEPE Fatal PEFatal PE
Radical retropubic Radical retropubic prostatectomyprostatectomy 11––3%3% 11––3%3% 0.6%0.6%
CystectomyCystectomy 8%8% 22––4%4% 2%2%
Radiological studiesRadiological studies 51%51% 22%22%

► Majority of patients undergoing Majority of patients undergoing neurosurgery for malignancyneurosurgery for malignancy
► Risk of venographic VTE ~30%-40%Risk of venographic VTE ~30%-40%
► High risk of intracranial or intraspinal High risk of intracranial or intraspinal hemorrhagehemorrhage
► Mechanical prophylaxis preferred methodMechanical prophylaxis preferred method
► Use of anticoagulant prophylaxis remains Use of anticoagulant prophylaxis remains controversial in this settingcontroversial in this setting
Neurosurgery and VTENeurosurgery and VTE
OBSERVATIONSOBSERVATIONS

Meta-analysis of three (3) RCTs evaluating Meta-analysis of three (3) RCTs evaluating LMWH prophylaxisLMWH prophylaxis
► One major bleeding event observed for every 7 proximal One major bleeding event observed for every 7 proximal DVTs prevented with LMWHDVTs prevented with LMWH
ESES LMWHLMWH RRRR NNT/NNHNNT/NNH PP
VTEVTE 28.3%28.3% 17.5%17.5% 0.60.6 99 0.0010.001
Proximal DVTProximal DVT 12.5%12.5% 6.2%6.2% 0.50.5 1616 <0.01<0.01
Total bleedingTotal bleeding 3.0%3.0% 6.1%6.1% 2.02.0 3333 0.020.02
Major bleedingMajor bleeding 1.3%1.3% 2.2%2.2% 1.71.7 115115 0.300.30
Iorio A, AgnellIorio A, Agnelli Gi G. . Arch Intern Med.Arch Intern Med. 2000;160:2327 2000;160:2327--23322332
Neurosurgery and VTE ProphylaxisNeurosurgery and VTE Prophylaxis

77thth ACCP Consensus Guidelines ACCP Consensus Guidelines
GradeGrade Recommendations for Cancer PatientsRecommendations for Cancer Patients
1A1A Patients Patients undergoing surgeryundergoing surgery should receive LDUH 5000 should receive LDUH 5000 U tid or LMWH > 3400 U dailyU tid or LMWH > 3400 U daily
2A2A Patients undergoing surgery Patients undergoing surgery may receive post-hospital may receive post-hospital discharge prophylaxis with LMWHdischarge prophylaxis with LMWH
2A2ANo routine prophylaxis to prevent thrombosis secondary No routine prophylaxis to prevent thrombosis secondary to central venous catheters, including LMWH (2B) and to central venous catheters, including LMWH (2B) and fixed-dose warfarin (1B)fixed-dose warfarin (1B)
1A1A Patients hospitalized with an acute medical illness Patients hospitalized with an acute medical illness should receive LDUH or LMWHshould receive LDUH or LMWH
Geerts W, et al. Geerts W, et al. ChestChest 2004; 126: 338S-400S 2004; 126: 338S-400S

Thrombosis is a potential complication of central Thrombosis is a potential complication of central venous catheters, including these events:venous catheters, including these events:
–Fibrin sheath formationFibrin sheath formation
–Superficial phlebitisSuperficial phlebitis
–Ball-valve clotBall-valve clot
–Deep vein thrombosis (DVT)Deep vein thrombosis (DVT)
• • Incidence up to 60% from historical dataIncidence up to 60% from historical data
• • ACCP guidelines recommended routine prophylaxis ACCP guidelines recommended routine prophylaxis with low dose warfarin or LMWHwith low dose warfarin or LMWH
Central Venous CathetersCentral Venous Catheters
Geerts W, et al. Geerts W, et al. ChestChest 2001;119:132S-175S 2001;119:132S-175S

Placebo-Controlled TrialsPlacebo-Controlled Trials
StudyStudy RegimenRegimen NN CRT (%)CRT (%)
Reichardt* Reichardt* 20022002
Dalteparin 5000 U odDalteparin 5000 U od
placeboplacebo
285285
140140
11 (3.7)11 (3.7)
5 (3.4)5 (3.4)
Couban*Couban*
20022002
Warfarin 1mg odWarfarin 1mg od
placeboplacebo
130130
125125
6 (4.6)6 (4.6)
5 (4.0)5 (4.0)
ETHICSETHICS††
20042004
Enoxaparin 40 mg odEnoxaparin 40 mg od
placeboplacebo
155155
155155
22 (14.2)22 (14.2)
28 (18.1)28 (18.1)
**symptomatic outcomessymptomatic outcomes;; ††routine venography at 6 weeksroutine venography at 6 weeks
Prophylaxis for Venous CathetersProphylaxis for Venous Catheters
Reichardt P, et al. Reichardt P, et al. Proc ASCOProc ASCO 2002;21:369a; Couban S, et al, 2002;21:369a; Couban S, et al, BloodBlood 2002;100:703a; Agnelli 2002;100:703a; Agnelli G, et al. G, et al. Proc ASCOProc ASCO 2004;23:730 2004;23:730

Tolerability of Low-Dose WarfarinTolerability of Low-Dose Warfarin
► 95 cancer patients receiving FU-based infusion 95 cancer patients receiving FU-based infusion chemotherapy and 1 mg warfarin dailychemotherapy and 1 mg warfarin daily
► INR measured at baseline and four time pointsINR measured at baseline and four time points
► 10% of all recorded INRs >1.510% of all recorded INRs >1.5
► Patients with elevated INRPatients with elevated INR2.0–2.92.0–2.9 6% 6%
3.0–4.93.0–4.9 19%19%
>5.0>5.0 7% 7%
Central Venous Catheters: WarfarinCentral Venous Catheters: Warfarin
Masci et al. J Clin Oncol. 2003;21:736-739

SummarySummary► Recent studies demonstrate a low Recent studies demonstrate a low
incidence of symptomatic catheter-incidence of symptomatic catheter-related thrombosis (~4%)related thrombosis (~4%)
► Routine prophylaxis is Routine prophylaxis is not warrantednot warranted to to prevent catheter-related thrombosis, prevent catheter-related thrombosis, but catheter patency rates/infections but catheter patency rates/infections have not been studiedhave not been studied
► Low-dose LMWH and fixed-dose Low-dose LMWH and fixed-dose warfarin have not been shown to be warfarin have not been shown to be effective for preventing symptomatic effective for preventing symptomatic and asymptomatic thrombosisand asymptomatic thrombosis
Prophylaxis for Central Prophylaxis for Central Venous Access DevicesVenous Access Devices

77thth ACCP Consensus Guidelines ACCP Consensus Guidelines
GradeGrade Recommendations for Cancer PatientsRecommendations for Cancer Patients
1A1A Patients undergoing surgery should receive LDUH 5000 U tid Patients undergoing surgery should receive LDUH 5000 U tid or LMWH > 3400 U dailyor LMWH > 3400 U daily
2A2A Patients undergoing surgery may receive post-hospital Patients undergoing surgery may receive post-hospital discharge prophylaxis with LMWHdischarge prophylaxis with LMWH
2A2ANo routine prophylaxis to prevent thrombosis secondary to No routine prophylaxis to prevent thrombosis secondary to central venous catheters, including LMWH (2B) and fixed-central venous catheters, including LMWH (2B) and fixed-dose warfarin (1B)dose warfarin (1B)
1A1A Patients hospitalized with an acute medical illness should Patients hospitalized with an acute medical illness should receive LDUH or LMWHreceive LDUH or LMWH
Geerts W, et al. Geerts W, et al. ChestChest 2004; 126: 338S-400S 2004; 126: 338S-400S

Primary Prophylaxis in Cancer Primary Prophylaxis in Cancer Radiotherapy in the Ambulatory PatientRadiotherapy in the Ambulatory Patient
► No recommendations from ACCPNo recommendations from ACCP
► No data from randomized trials (RCTs)No data from randomized trials (RCTs)
► Weak data from observational studies Weak data from observational studies in high risk tumors (e.g. brain tumors; in high risk tumors (e.g. brain tumors; mucin-secreting adenocarcinomas-mucin-secreting adenocarcinomas-colorectal, pancreatic, lung, renal cell, colorectal, pancreatic, lung, renal cell, ovarian)ovarian)
► Recommendations extrapolated from Recommendations extrapolated from other groups of patients if additional other groups of patients if additional risk factors present (e.g. hemiparesis risk factors present (e.g. hemiparesis in brain tumors, etc.)in brain tumors, etc.)

Risk Factors for VTE inRisk Factors for VTE inMedical Oncology PatientsMedical Oncology Patients
► Tumor typeTumor type Ovary, brain, pancreas, lung, colonOvary, brain, pancreas, lung, colon
► Stage, grade, and extent of cancerStage, grade, and extent of cancer Metastatic disease, venous stasis due Metastatic disease, venous stasis due
to bulky diseaseto bulky disease
► Type of antineoplastic treatmentType of antineoplastic treatment Multiagent regimens, hormones,Multiagent regimens, hormones,
anti-VEGF, radiationanti-VEGF, radiation
► Miscellaneous VTE risk factorsMiscellaneous VTE risk factors Previous VTE, Previous VTE, hospitalization, hospitalization,
immobility, infection, thrombophiliaimmobility, infection, thrombophilia

Independent Risk Factors for DVT/PEIndependent Risk Factors for DVT/PE
Risk Factor/CharacteristicRisk Factor/Characteristic O.R.O.R.
Recent surgery w/ institutionalizationRecent surgery w/ institutionalization 21.7221.72
TraumaTrauma 12.6912.69
Institutionalization without recent surgeryInstitutionalization without recent surgery 7.987.98
Malignancy with chemotherapyMalignancy with chemotherapy 6.536.53
Prior CVAD or pacemakerPrior CVAD or pacemaker 5.555.55
Prior superficial vein thrombosisPrior superficial vein thrombosis 4.324.32
Malignancy without chemotherapyMalignancy without chemotherapy 4.054.05
Neurologic disease w/ extremity paresisNeurologic disease w/ extremity paresis 3.043.04
Serious liver diseaseSerious liver disease 0.100.10
Heit JA et al. Heit JA et al. Thromb HaemostThromb Haemost. 2001;86:452-463. 2001;86:452-463

VTE Incidence In Various TumorsVTE Incidence In Various Tumors
47%47%Solid tumors (anti-VEGF + chemo)Solid tumors (anti-VEGF + chemo)
43%43%Renal cell carcinoma Renal cell carcinoma
28%28%Multiple myeloma (thalidomide + chemo)Multiple myeloma (thalidomide + chemo)
9%9%Advanced cancer (1-year survival=12%)Advanced cancer (1-year survival=12%)
6%6%Hodgkin’s disease w/ chemoHodgkin’s disease w/ chemo
3%3%Non-Hodgkin’s lymphomas w/ chemoNon-Hodgkin’s lymphomas w/ chemo
8%8%Breast cancer (Stage IV) w/ chemoBreast cancer (Stage IV) w/ chemo
26%26%High-grade gliomaHigh-grade glioma
2%2%Breast cancer (Stage I & II) w/ chemoBreast cancer (Stage I & II) w/ chemo
0.2%0.2%Breast cancer (Stage I & II) w/o further treatmentBreast cancer (Stage I & II) w/o further treatment
VTE VTE IncidenceIncidenceOncology SettingOncology Setting
Wilms tumor (cavoatrial extension) 4%
Otten, et al. Haemostasis 2000;30:72. Lee & Levine. Circulation 2003;107:I17Otten, et al. Haemostasis 2000;30:72. Lee & Levine. Circulation 2003;107:I17

16% 16% Zangari, 2002Zangari, 2002 (192 pts)(192 pts)
T+dox at T+dox at relapserelapse
17.8%17.8%Baz, Baz, 20042004 (103 pts)(103 pts)
14.7% 14.7% Zangari, 2004Zangari, 2004 (68pts)(68pts)7% 7% Minnema, Minnema, 20042004 (412 pts) (412 pts)
31.4% Z31.4% Zangari, angari, 2004 2004 (35 pts) (35 pts)
34.5% 34.5% Zangari, 2004Zangari, 2004 (87 pts)(87 pts)
T+ dox in T+ dox in newly newly diagnosed diagnosed patientspatients
7% 7% Weber, Weber, 20022002(46 pts)(46 pts)
25% 25% Weber, 2002Weber, 2002 (24 pts) (24 pts)
13% 13% Cavo, 2004Cavo, 2004(52 pts)(52 pts)
26% 26% Cavo, 2002Cavo, 2002 (19 pts)(19 pts)18% 18% Rajkumar, 2004 Rajkumar, 2004 (102 pts)(102 pts)
T+ D in newly T+ D in newly diagnosed diagnosed patientspatients
Aspirin Aspirin (81 (81
mg/d)mg/d)LMWHLMWHWarfarin Warfarin
(INR 2 – 3)(INR 2 – 3)Warfarin Warfarin 1mg/daily1mg/dailyNo prophylaxisNo prophylaxisTherapyTherapy
Strategies for Thromboprophylaxis in Strategies for Thromboprophylaxis in Thalidomide Treated MM PatientsThalidomide Treated MM Patients

DVTDVT
Len + D(%)Len + D(%) D (%) D (%) Len + D(%)Len + D(%) D (%) D (%)
MM-009MM-009 MM-010MM-010
00
22
44
66
88
1010
1212
1414
1616
PEPE
Weber D. ASCO 2005 Annual MeetingWeber D. ASCO 2005 Annual Meeting
MM-009/010: Thromboembolic EventsMM-009/010: Thromboembolic Events

Knight: N Engl J Med.2006,354:2079Knight: N Engl J Med.2006,354:2079
► rEPO used more in USA and Canada
► L+Dex: 23% VTE with EPO vs 5% w/o EPO
► Placebo + Dex: 7% VTE with EPO vs 1% without EPO
Incidence of VTE: USA and Canada Incidence of VTE: USA and Canada >Israel, Australia, and Europe>Israel, Australia, and Europe
Multivariate Analysis of the Risk of Thrombosis Associated Multivariate Analysis of the Risk of Thrombosis Associated with Lenalidomide plus High-Dose Dexamethasone and with Lenalidomide plus High-Dose Dexamethasone and Concomitant Erythropoietin for the Treatment of Multiple Concomitant Erythropoietin for the Treatment of Multiple Myeloma Myeloma
TreatmentTreatment Odds RatioOdds Ratio P ValueP Value(95% CI)(95% CI)
Lenalidomide plusLenalidomide plus 3.51 (1.77-6.97)3.51 (1.77-6.97) <0.001<0.001High-dose dexamethasoneHigh-dose dexamethasone
Concomitant erythropoietin Concomitant erythropoietin 3.21 (1.72-6.01)3.21 (1.72-6.01) <0.001<0.001

Thrombotic Outcomes from rEPO or Thrombotic Outcomes from rEPO or Darbopoietin Use in Cancer PatientsDarbopoietin Use in Cancer Patients
Bohlius: The Cochrane Library, Volume (4).2006
Among 6,769 Among 6,769 pts with cancer, pts with cancer, RR for DVT with RR for DVT with rEPO/Darbepo rEPO/Darbepo was increased was increased by 67%by 67% (RR=1.67; 95% (RR=1.67; 95% CI 1.35 to 2.06)CI 1.35 to 2.06)

Vitamin K antagonist (INR 2.0 - 3.0)Vitamin K antagonist (INR 2.0 - 3.0)
>> 3 months 3 months
LMWH or UFH LMWH or UFH
5 to 7 days5 to 7 daysInitial treatment
Long-term therapy
Standard Treatment of VTEStandard Treatment of VTECan We Do Better Than This?Can We Do Better Than This?

Recurrent VTE in Cancer – Subset Analysis of Recurrent VTE in Cancer – Subset Analysis of the Home Rx Studies (UH/VKA vs. LMWH/VKA)the Home Rx Studies (UH/VKA vs. LMWH/VKA)
Recurrent VTERecurrent VTEEvents per 100 patient yearsEvents per 100 patient years
P valueP valueMalignantMalignant Non- MalignantNon- Malignant
27.127.1 9.09.0 0.0030.003
Hutten et.al. Hutten et.al. J Clin Oncol J Clin Oncol 2000;18:3078 2000;18:3078

Recurrent VTE in Cancer – Subset Recurrent VTE in Cancer – Subset Analysis of the Home Rx StudiesAnalysis of the Home Rx Studies
Major BleedingMajor BleedingEvents per 100 patient yearsEvents per 100 patient years
P-valueP-value
MalignantMalignant Non-Non-malignantmalignant
13.313.3 2.12.1 0.0020.002Hutten et.al. Hutten et.al. J Clin Oncol J Clin Oncol 2000;18:3078 2000;18:3078

Oral Anticoagulant TherapyOral Anticoagulant Therapyin Cancer Patients: Problematicin Cancer Patients: Problematic
► Warfarin (Coumadin®) therapy is Warfarin (Coumadin®) therapy is complicated by:complicated by:
Difficulty maintaining tight therapeutic control, Difficulty maintaining tight therapeutic control, due to anorexia, vomiting, drug interactions, due to anorexia, vomiting, drug interactions, etc. etc.
Frequent interruptions for thrombocytopenia Frequent interruptions for thrombocytopenia and proceduresand procedures
Difficulty in venous access for monitoringDifficulty in venous access for monitoring Increased risk of both recurrence and bleedingIncreased risk of both recurrence and bleeding
► Is it reasonable to substitute long-term Is it reasonable to substitute long-term LMWH for warfarin ? When? How? Why?LMWH for warfarin ? When? How? Why?

CLOT: Landmark Cancer/VTE TrialCLOT: Landmark Cancer/VTE Trial
CANCER PATIENTS WITH CANCER PATIENTS WITH ACUTE DVT or PEACUTE DVT or PE RandomizationRandomization
DalteparinDalteparin
DalteparinDalteparin Oral AnticoagulantOral Anticoagulant
DalteparinDalteparin
[N = 677][N = 677]
► Primary Endpoints:Primary Endpoints: Recurrent VTE and Bleeding Recurrent VTE and Bleeding
► Secondary Endpoint:Secondary Endpoint: Survival Survival
Lee, Levine, Kakkar, Rickles et.al. Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, N Engl J Med, 2003;349:1462003;349:146

Landmark CLOT Cancer TrialLandmark CLOT Cancer TrialReduction in Recurrent VTEReduction in Recurrent VTE
00
55
1010
1515
2020
2525
Days Post RandomizationDays Post Randomization
00 3030 6060 9090 120120 150150 180180 210210
Pro
bab
ility
of R
ecu
rre
nt V
TE
, %P
roba
bili
ty o
f Re
curr
en
t VT
E, %
Risk reduction = Risk reduction = 52%52%
pp-value = 0.0017-value = 0.0017
DalteparinDalteparin
OACOAC
Recurrent VTERecurrent VTE
Lee, Levine, Kakkar, Rickles et.al. Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, N Engl J Med, 2003;349:1462003;349:146

DalteparinDalteparin
N=338N=338
OACOAC
N=335N=335 P-P-
value*value*
Major bleedMajor bleed 19 ( 5.6%) 19 ( 5.6%) 12 ( 3.6%)12 ( 3.6%) 0.270.27
Any bleedAny bleed 46 (13.6%)46 (13.6%) 62 (18.5%)62 (18.5%) 0.0930.093
* Fisher’s exact test* Fisher’s exact test
Bleeding Events in CLOTBleeding Events in CLOT
Lee, Levine, Kakkar, Rickles et.al. Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, N Engl J Med, 2003;349:1462003;349:146

Treatment of Cancer-Associated VTETreatment of Cancer-Associated VTE
StudyStudy DesignDesign Length Length of of
TherapyTherapy
(Months)(Months)
NN Recurrent Recurrent VTEVTE (%) (%)
Major Major BleedingBleeding
(%)(%)
DeathDeath
(%)(%)
CLOT TrialCLOT Trial
(Lee 2003)(Lee 2003)
DalteparinDalteparin
OACOAC
6 6 336336
336336
99
1717
66
44
3939
4141
CANTHENOXCANTHENOX
(Meyer 2002)(Meyer 2002)
EnoxaparinEnoxaparin
OACOAC
33 6767
7171
1111
2121
77
1616
1111
2323
LITELITE
(Hull ISTH 2003)(Hull ISTH 2003)
TinzaparinTinzaparin
OACOAC
33 8080
8787
66
1111
66
88
2323
2222
ONCENOXONCENOX
(Deitcher ISTH (Deitcher ISTH 2003)2003)
Enox (Low)Enox (Low)
Enox (High)Enox (High)
OACOAC
66 3232
3636
3434
3.43.4
3.13.1
6.76.7
NS
NS0.03
NS
NS0.002
NS
NS
NR
0.09 0.030.09

Treatment and 2Treatment and 2° Prevention of VTE ° Prevention of VTE in Cancer – Bottom Linein Cancer – Bottom Line
► New standard of care is LMWH at New standard of care is LMWH at therapeutic doses for a therapeutic doses for a minimum of 3-6 minimum of 3-6 monthsmonths (Grade 1A recommendation—ACCP)(Grade 1A recommendation—ACCP)
► Oral anticoagulant therapy to follow for as Oral anticoagulant therapy to follow for as long as cancer is active (Grade 1C long as cancer is active (Grade 1C recommendation—ACCP)recommendation—ACCP)
Buller et.al. Chest Suppl 2004;126:401S-428SBuller et.al. Chest Suppl 2004;126:401S-428S
New DevelopmentNew Development

CLOT 12-month MortalityAll Patients
0
10
20
30
40
50
60
70
80
90
100
0 30 60 90 120 180 240 300 360
DalteparinDalteparin
OACOAC
HR 0.94 P-value = 0.40
Days Post Randomization
Pro
bab
ility
of S
urv
iva
l, %
Lee A, et al. ASCO. 2003

0
10
20
30
40
50
60
70
80
90
100
Days Post Randomization
0 30 60 90 120 150 180 240 300 360
Pro
bab
ility
of S
urv
iva
l, %
OAC
Dalteparin
HR = 0.50 P-value = 0.03
Anti-Tumor Effects of LMWH CLOT 12-month Mortality
Lee A, et al. ASCO. 2003
Patients Without Metastases (N=150)

► 84 patients randomized: CEV +/- LMWH (18 weeks)84 patients randomized: CEV +/- LMWH (18 weeks)
► Patients balanced for age, gender, stage, smoking Patients balanced for age, gender, stage, smoking history, ECOG performance statushistory, ECOG performance status
LMWH for Small Cell Lung CancerLMWH for Small Cell Lung CancerTurkish Study Turkish Study
Altinbas et al. J Thromb Haemost 2004;2:1266.Altinbas et al. J Thromb Haemost 2004;2:1266.
Chemo + Chemo + DalteparinDalteparin Chemo aloneChemo alone P-valueP-value
1-y overall survival, %1-y overall survival, % 51.351.3 29.529.5 0.010.01
2-y overall survival, %2-y overall survival, % 17.217.2 0.00.0 0.010.01
Median survival, mMedian survival, m 13.013.0 8.08.0 0.010.01
CEV = cyclophosphamide, epirubicin, vincristine; LMWH = Dalteparin, 5000 units daily

VTE Prophylaxis Is Underused VTE Prophylaxis Is Underused in Patients With Cancer in Patients With Cancer
5
89
3833
42
52
0
10
20
30
40
50
60
70
80
90
100
FRONTLINESurgical
FRONTLINE:Medical
Stratton Bratzler Rahim DVT FREE
1. Kakkar AK et al. Oncologist. 2003;8:381-3882. Stratton MA et al. Arch Intern Med. 2000;160:334-3403. Bratzler DW et al. Arch Intern Med. 1998;158:1909-1912
Cancer:FRONTLINE Survey1— 3891 Clinician Respondents
Rat
e o
f A
pp
rop
riat
e P
rop
hyl
axis
, %
Major Surgery2
Major Abdominothoracic Surgery (Elderly)3 Medical
Inpatients4
Confirmed DVT (Inpatients)5
Cancer: Surgical
Cancer: Medical
4. Rahim SA et al. Thromb Res. 2003;111:215-2195. Goldhaber SZ et al. Am J Cardiol. 2004;93:259-262

Venous Thromboembolism (VTE) Venous Thromboembolism (VTE) Prophylaxis in the Cancer PatientProphylaxis in the Cancer Patient
Guidelines and Implications for Guidelines and Implications for Clinical PracticeClinical Practice
Venous Thromboembolism (VTE) Venous Thromboembolism (VTE) Prophylaxis in the Cancer PatientProphylaxis in the Cancer Patient
Guidelines and Implications for Guidelines and Implications for Clinical PracticeClinical Practice
Alex C Spyropoulos, MD, FACP, FCCPAlex C Spyropoulos, MD, FACP, FCCPChair, Department of Clinical ThrombosisChair, Department of Clinical Thrombosis
Lovelace Medical CenterLovelace Medical CenterClinical Associate Professor of MedicineClinical Associate Professor of Medicine
Associate Professor of PharmacyAssociate Professor of PharmacyUniversity of New Mexico Health Sciences CenterUniversity of New Mexico Health Sciences Center
Albuquerque, NM, USAAlbuquerque, NM, USA
Alex C Spyropoulos, MD, FACP, FCCPAlex C Spyropoulos, MD, FACP, FCCPChair, Department of Clinical ThrombosisChair, Department of Clinical Thrombosis
Lovelace Medical CenterLovelace Medical CenterClinical Associate Professor of MedicineClinical Associate Professor of Medicine
Associate Professor of PharmacyAssociate Professor of PharmacyUniversity of New Mexico Health Sciences CenterUniversity of New Mexico Health Sciences Center
Albuquerque, NM, USAAlbuquerque, NM, USA
Clotting, Cancer, and ControversiesClotting, Cancer, and Controversies

Outline of PresentationOutline of Presentation
► VTE prophylaxis in cancerVTE prophylaxis in cancer Surgical, CVC, medicalSurgical, CVC, medical
► Guidelines for VTE prophylaxis Guidelines for VTE prophylaxis in the cancer patientin the cancer patient ACCP, NCCNACCP, NCCN
► Performance to datePerformance to date
► Opportunities for improvementOpportunities for improvement

Thromboprophylaxis in Cancer vs Non-Thromboprophylaxis in Cancer vs Non-Cancer Surgical patientsCancer Surgical patients
Non-Cancer (%)N=16,954
Cancer (%)N=6124
P
Post-op VTEPost-op VTE 0.610.61 1.261.26 <0.0001<0.0001
Non-fatal PENon-fatal PE 0.270.27 0.540.54 <0.0003<0.0003
Autopsy PEAutopsy PE 0.110.11 0.410.41 0.00010.0001
DeathDeath 0.710.71 3.143.14 0.00010.0001
Cancer patients have a 2-fold increased riskCancer patients have a 2-fold increased riskOf VTE and 3-fold increased risk of fatal PEOf VTE and 3-fold increased risk of fatal PEdespite prophylaxisdespite prophylaxis
Haas S et al Thromb Haemost 2005;94:814-819Haas S et al Thromb Haemost 2005;94:814-819
Kakkar AJ et al Thromb Haemost 2005;94:867-71Kakkar AJ et al Thromb Haemost 2005;94:867-71

Thromboprophylaxis in Surgical PatientsThromboprophylaxis in Surgical Patients
► ARISTOSARISTOS Prospective cohort of 2373 patientsProspective cohort of 2373 patients
► Overall symptomatic VTE 2.1% and Overall symptomatic VTE 2.1% and death 1.7%death 1.7%
► Advanced tumorAdvanced tumor OR 4.4 (95% CI 1.4 – 5.2)OR 4.4 (95% CI 1.4 – 5.2)
Agnelli G Ann Surg 2006; 243:85-89Agnelli G Ann Surg 2006; 243:85-89

In-hospital Thromboprophylaxis in In-hospital Thromboprophylaxis in Cancer SurgeryCancer Surgery
ENOXACANENOXACAN Canadian Colorectal StudyCanadian Colorectal Study
P=NSP=NS
NNT=29NNT=29
P=0.05P=0.05
NNT=33NNT=33
ENOXACAN Study Group Br J Surg 1997;84:1099-1103ENOXACAN Study Group Br J Surg 1997;84:1099-1103
Mcleod R et al Ann Surg 2001;233:436-44Mcleod R et al Ann Surg 2001;233:436-44
0
2
4
6
8
10
12
14
VTE MajorBleed
VTE MajorBleed
UFH 5000 Enox 40 mg

Extended Thromboprophylaxis in Extended Thromboprophylaxis in Cancer SurgeryCancer Surgery
ENOXACAN IIENOXACAN II FAMEFAME
P= 0.02P= 0.02
NNT=14NNT=14
P<0.03P<0.03
NNT= 9NNT= 9
Berquvist D et al NEJM 2002;346:975-80Berquvist D et al NEJM 2002;346:975-80
Rasmusan M et al Blood 2003;102;52aRasmusan M et al Blood 2003;102;52a
0
5
10
15
20
25
30
35
40
VTE Prox DVT VTE Prox DVT
Placebo Enox 40 mg Placebo 2 Dalteparin

Systematic Review of DVT Prophylaxis of Systematic Review of DVT Prophylaxis of Surgical Cancer PatientsSurgical Cancer Patients
► 26 RCTs of 7,639 patients26 RCTs of 7,639 patients
Overall DVT of pharmacological Px Overall DVT of pharmacological Px vs controls - 12.7% vs 35.2%vs controls - 12.7% vs 35.2%
High dose vs Low dose LMWH for High dose vs Low dose LMWH for DVT 7.9% vs 14.5% (p<0.01)DVT 7.9% vs 14.5% (p<0.01)
No differences in LMWH vs UFH in No differences in LMWH vs UFH in efficacy, DVT location, or bleedingefficacy, DVT location, or bleeding
Overall bleeding complications 3%Overall bleeding complications 3%
Leonardi MJ et al Ann Surg Oncol 2007;14(2):929-36

Thromboprophylaxis for CVCThromboprophylaxis for CVC
► Prior studies with ~ 5% incidence of Prior studies with ~ 5% incidence of symptomatic catheter-related thrombosissymptomatic catheter-related thrombosis
RegimenRegimen NN Cath Cath Thrombosis (%)Thrombosis (%)
Kathaus Kathaus 20062006
dalteparin 5000U qddalteparin 5000U qdplaceboplacebo
285285140140
11 (3.7)11 (3.7)5 (3.4)5 (3.4)
Couban Couban 20052005
warfarin 1mg QDwarfarin 1mg QDPlaceboPlacebo
130130125125
6 (4.6)6 (4.6)5 (4.0)5 (4.0)
Verso 2005Verso 2005 enoxaparin 40mg qdenoxaparin 40mg qdplaceboplacebo
155155155155
22 (14.2)22 (14.2)28 (18.1)28 (18.1)
Karthaus et al Oncol 2006;17:286-296Karthaus et al Oncol 2006;17:286-296
Couban et al JCO 2006: 23:4063-8Couban et al JCO 2006: 23:4063-8
Verso et al JCO 2006;23:4057-62Verso et al JCO 2006;23:4057-62

Thromboprophylaxis in Hospitalized Thromboprophylaxis in Hospitalized Medical Cancer PatientsMedical Cancer Patients
► There are no randomized trials in hospitalzed medical There are no randomized trials in hospitalzed medical oncology patientsoncology patients
► Randomized, placebo controlled trials in acutely ill Randomized, placebo controlled trials in acutely ill hospitalized medical patients (of which cancer patients hospitalized medical patients (of which cancer patients
area percentagearea percentage))
0
2
4
6
8
10
12
14
16
ME DE NOX P R E VE NT AR T E MIS
E nox aparin 40mg
P lac ebo
Dalteparin 5000IU
P lac ebo2
F onda 2.5mg QD
P lac ebo3
Pt noPt no 866866 29912991 644644
Cancer (%)Cancer (%) 1414 55 55

Dentali, F. et. al. Ann Intern Med 2007;146:278-288Dentali, F. et. al. Ann Intern Med 2007;146:278-288
Fatal Pulmonary Embolism During Fatal Pulmonary Embolism During Anticoagulant ProphylaxisAnticoagulant Prophylaxis
0.001 0.01 0.1 1.0 10 100 1000Favors Treatment Favors Placebo
Study,
Year (Reference)
Prophylaxis
n/n
Placebo
n/n
RR Fixed
(95% CI)
RR Fixed
(95% CI)
Dahan et al, 1986 (41) 1/132 3/131 0.33 (0.03 to 3.14)
Garlund at al, 1996 (35) 3/5776 12/5917 0.26 (0.07 to 0.91)
Leizorovic et al, 2004 (23) 0/1829 2/1807 0.20 (0.01 to 4.11)
Mahe et al, 2005 (22) 10/1230 17/1244 0.59 (0.27 to 1.29)
Cohen at, 2006 (42) 0/321 5/323 0.09 (0.01 to 1.65)
Total (95% CI) 0.38 (0.21 to 0.69)
Total events 14 39

Unfractionated Heparin Prophylaxis:Unfractionated Heparin Prophylaxis:BID vs TID—What Works, What Doesn’t?BID vs TID—What Works, What Doesn’t?
Meta-analysis: 12 Meta-analysis: 12 RCTsRCTs
► DVT, PE, all VTE events, BleedingDVT, PE, all VTE events, Bleeding
► Proximal DVT plus PEProximal DVT plus PE BID VTE event rate: BID VTE event rate:
2.34 events per 1,0002.34 events per 1,000patient dayspatient days
TID event rate: TID event rate:
0.86 events per 1,0000.86 events per 1,000patient dayspatient days
P=0.05P=0.05
► NNTNNT 676 hospital prophylaxis days 676 hospital prophylaxis days
with UFH TID to preventwith UFH TID to prevent 1 major bleed with 1,649 1 major bleed with 1,649
hospital prophylaxis days of hospital prophylaxis days of TID dosingTID dosing
King CS et al. CHEST 2007;131:507-516King CS et al. CHEST 2007;131:507-516

15,231
56,364
0
10,000
20,000
30,000
40,000
50,000
60,000
With HIT Without HIT
Co
st
of
adm
iss
ion
($
)
Incidence and Economic Incidence and Economic Implications of HITImplications of HIT
0.084
0.51
0
0.1
0.2
0.3
0.4
0.5
0.6
UFH LWMH
Inci
den
ce o
f H
IT (
%)
Creekmore FM, et al. Creekmore FM, et al. Pharmacotherapy.Pharmacotherapy. 2006;26:1438-1445 2006;26:1438-1445..
N = 10,121N = 10,121
PP = 0.037 = 0.037 PP < 0.001 < 0.001

2004 ACCP Recommendations2004 ACCP Recommendations
Cancer patients undergoing surgical procedures receive prophylaxis that is Cancer patients undergoing surgical procedures receive prophylaxis that is appropriate for their current risk state (Grade 1A)appropriate for their current risk state (Grade 1A)
General, Gynecologic, Urologic SurgeryGeneral, Gynecologic, Urologic Surgery• Low Dose Unfractionated Heparin 5,000 units TIDLow Dose Unfractionated Heparin 5,000 units TID• LMWH > 3,400 units DailyLMWH > 3,400 units Daily
– Dalteparin 5,000 units Dalteparin 5,000 units – Enoxaparin 40 mg Enoxaparin 40 mg – Tinzaparin 4,500 unitsTinzaparin 4,500 units
• GCS and/or IPCGCS and/or IPC
Surgical patients may receive post-discharge prophylaxis with LMWH (Grade 2A)Surgical patients may receive post-discharge prophylaxis with LMWH (Grade 2A)
No routine prophylaxis for central venous catheters, including LMWH (Grade 2B) No routine prophylaxis for central venous catheters, including LMWH (Grade 2B) and fixed-dose warfarin (Grade 1B)and fixed-dose warfarin (Grade 1B)
Cancer patients with an acute medical illness receive prophylaxisCancer patients with an acute medical illness receive prophylaxisthat is appropriate for their current risk state (Grade 1A)that is appropriate for their current risk state (Grade 1A)
• Low Dose Unfractionated HeparinLow Dose Unfractionated Heparin• LMWHLMWH
Contraindication to anticoagulant prophylaxis (Grade 1C+)Contraindication to anticoagulant prophylaxis (Grade 1C+)• GCS or IPCGCS or IPC
Geerts WH et al. Chest. 2004;126(suppl):338S-400S

NCCN Practice Guidelines in VTE NCCN Practice Guidelines in VTE DiseaseDisease
At Risk Population Initial ProphylaxisAt Risk Population Initial Prophylaxis
http://www.nccn.org/professionals/physician_gls/PDF/vte.pdf
► Adult patientAdult patient► Diagnosis or Diagnosis or
clinical clinical suspicion of suspicion of cancercancer
► InpatientInpatient
Relative contra-Relative contra-indication to indication to anticoagulation anticoagulation treatmenttreatment
Prophylactic anticoagulation Prophylactic anticoagulation therapy (category 1) therapy (category 1) ++ sequential sequential compression device (SCD)compression device (SCD)
Mechanical prophylaxis (options)Mechanical prophylaxis (options)- SCD- SCD- Graduated compression stockings- Graduated compression stockings
NONO
YESYES
RISK FACTOR ASSESSMENTRISK FACTOR ASSESSMENT► AgeAge► Prior VTEPrior VTE► Familial thrombophiliaFamilial thrombophilia► Active cancerActive cancer► TraumaTrauma► Major surgical proceduresMajor surgical procedures► Acute or chronic medical illness requiring Acute or chronic medical illness requiring
hospitalization or prolonged bed resthospitalization or prolonged bed rest► Central venous catheter/IV catheterCentral venous catheter/IV catheter► Congestive heart failureCongestive heart failure► PregnancyPregnancy► Regional bulky lymphadenopathy with Regional bulky lymphadenopathy with
extrinsic vascular compressionextrinsic vascular compression
AGENTS ASSOCIATED AGENTS ASSOCIATED WITH INCREASED RISKWITH INCREASED RISK
► ChemotherapyChemotherapy► Exogenous estrogen Exogenous estrogen
compoundscompounds- HRT- HRT- Oral contraceptives- Oral contraceptives- Tamoxifen/Raloxifene- Tamoxifen/Raloxifene- Diethystilbestrol- Diethystilbestrol
► Thalidomide/lenalidomideThalidomide/lenalidomide
Modifiable risk factors: Lifestyle, Modifiable risk factors: Lifestyle, smoking, tobacco, obesity, smoking, tobacco, obesity, activity level/exerciseactivity level/exercise

http://www.nccn.org/professionals/physician_gls/PDF/vte.pdfhttp://www.nccn.org/professionals/physician_gls/PDF/vte.pdf
NCCN Practice Guidelines NCCN Practice Guidelines in VTE Diseasein VTE Disease
Inpatient Prophylactic Anticoagulation TherapyInpatient Prophylactic Anticoagulation Therapy
► LMWHLMWH- Dalteparin 5,000 units subcutaneous daily- Dalteparin 5,000 units subcutaneous daily- Enoxaparin 40 mg subcutaneous daily- Enoxaparin 40 mg subcutaneous daily- Tinzaparin 4,500 units (fixed dose) subcutaneous daily or - Tinzaparin 4,500 units (fixed dose) subcutaneous daily or
75 75 units/kg cubcutaneous daily units/kg cubcutaneous daily
► PentasaccharidePentasaccharide- Fondaparinux 2.5 mg subcutaneous daily- Fondaparinux 2.5 mg subcutaneous daily
► Unfractioned heparin 5,000 units subcutaneous 3 times dailyUnfractioned heparin 5,000 units subcutaneous 3 times daily

http://www.nccn.org/professionals/physician_gls/PDF/vte.pdfhttp://www.nccn.org/professionals/physician_gls/PDF/vte.pdf
NCCN Practice Guidelines NCCN Practice Guidelines in VTE Diseasein VTE Disease
Relative Contraindications to Prophylactic or Relative Contraindications to Prophylactic or Therapeutic AnticoagulationTherapeutic Anticoagulation
► Recent CNS bleed, intracranial or spinal lesion at high risk for Recent CNS bleed, intracranial or spinal lesion at high risk for bleedingbleeding
► Active bleeding (major): more than 2 units transfused in 24 hoursActive bleeding (major): more than 2 units transfused in 24 hours► Chronic, clinically significant measurable bleeding > 48 hoursChronic, clinically significant measurable bleeding > 48 hours► Thrombocytopenia (platelets < 50,000/mcL)Thrombocytopenia (platelets < 50,000/mcL)► Severe platelet dysfunction (uremia, medications, dysplastic Severe platelet dysfunction (uremia, medications, dysplastic
hematopoiesis)hematopoiesis)► Recent major operation at high risk for bleedingRecent major operation at high risk for bleeding► Underlying coagulopathyUnderlying coagulopathy► Clotting factor abnormalitiesClotting factor abnormalities
- Elevated PT or aPTT (excluding lupus inhibitors)- Elevated PT or aPTT (excluding lupus inhibitors)- Spinal anesthesia/lumbar puncture- Spinal anesthesia/lumbar puncture
► High risk for fallsHigh risk for falls

Compliance With ACCP VTE Compliance With ACCP VTE Prophylaxis Guidelines Is PoorProphylaxis Guidelines Is Poor
9.9% 6.7%
35,124
62,012
0
5,000
10,000
70,000
Nu
mb
er
of
pa
tie
nts
At risk for DVT/PE
Received compliant care
15.3% 12.7%52.4%
2324
9175
1388
OrthopedicSurgery
At-risk Medical Conditions
General Surgery
UrologicSurgery
Gynecologic Surgery
Data collected January 2001 to March 2005; 123,340 hospital admissions. Compliance assessment was based on the 6th American College of Chest Physicians (ACCP) guidelines.
HT Yu et al. Am J Health-Syst Pharm 2007; 64:69-76
Compliance With VTE Prophylaxis Guidelines in Hospitals by Patient GroupCompliance With VTE Prophylaxis Guidelines in Hospitals by Patient Group

In-Hospital Prophylaxis by Medical Condition – In-Hospital Prophylaxis by Medical Condition – IMPROVE RegistryIMPROVE Registry
57%
45%
49%
63%
60%
55%
59%
55%
49%
64%
0% 20% 40% 60% 80% 100%
Malignancy
Other disease
Renal failure
Diabetes
Severe Infection
Hypertension
Ischemic heart disease
COPD or Resp. failure
Stroke
Heart failure (CHF)
Tapson V et al Chest 2007 (in press)Tapson V et al Chest 2007 (in press)

Odds Ratio
Malignancy 0.40
Others 0.58
Infection 0.83
Bleeding Risk 0.91
Gender 0.92
Hospital Size 0.93
Age 1.00
LOS 1.05
Cardiovascular Disease 1.06
Internal Medicine 1.33
Respiratory 1.35
AMC 1.46
Duration of Immobility 1.60
VTE Risk Factors 1.78
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0
Effect Odds Ratio (95% CI)
Predictors of the Use of Predictors of the Use of ThromboprophylaxisThromboprophylaxis
Kahn SR et Al. Thromb Res 2007; 119:145-155Kahn SR et Al. Thromb Res 2007; 119:145-155

Independent factors present at admission for in-hospital Independent factors present at admission for in-hospital bleeding – multivariate analysis (IMPROVE Registry)bleeding – multivariate analysis (IMPROVE Registry)
Adjusted Odds Ratio Adjusted Odds Ratio (95% CI) (95% CI)
Bleeding disorderBleeding disorder 5.11 5.11 (2.38, 10.98)(2.38, 10.98)
Active G-duodenal ulcer Active G-duodenal ulcer 4.934.93 (2.86, 8.50)(2.86, 8.50)
Adm platelets<50 x 10Adm platelets<50 x 1099 3.003.00 (1.67, 5.41)(1.67, 5.41)
Hepatic failureHepatic failure 2.792.79 (1.57, 4.95)(1.57, 4.95)
ICU/CCU stayICU/CCU stay 2.412.41 (1.60, 3.63) (1.60, 3.63)
Current cancerCurrent cancer 1.991.99 (1.39, 2.85)(1.39, 2.85)
Central venous catheterCentral venous catheter 1.981.98 (1.33, 2.95)(1.33, 2.95)
Age Age 85 years85 years 1.911.91 (1.29, 2.85)(1.29, 2.85)
S. creatinine S. creatinine ≥2.5 mg/dL≥2.5 mg/dL 1.881.88 (1.26, 2.79)(1.26, 2.79)
Decousus H et al Blood 2005

Computer Reminder SystemComputer Reminder System
► Computer program linked to patient database to identify Computer program linked to patient database to identify consecutive hospitalized patients at risk for VTEconsecutive hospitalized patients at risk for VTE
► Patients randomized to intervention group or control groupPatients randomized to intervention group or control group
► In the intervention group the physicians were alerted to the In the intervention group the physicians were alerted to the VTE risk and offered the option to order VTE prophylaxisVTE risk and offered the option to order VTE prophylaxis
► Point scale for VTE riskPoint scale for VTE risk Major riskMajor risk: : CancerCancer, prior VTE, hypercoagulability, prior VTE, hypercoagulability
(3 points)(3 points) Intermediate riskIntermediate risk: Major surgery (2 points): Major surgery (2 points) Minor riskMinor risk: Advanced age, obesity, bedrest, HRT,: Advanced age, obesity, bedrest, HRT,
use of oral contraceptives (1 point)use of oral contraceptives (1 point)
► VTE prophylaxis (VTE prophylaxis (graduated elastic stockingsgraduated elastic stockings, IPC, UFH, , IPC, UFH, LMWH, warfarin)LMWH, warfarin)
Kucher N, et al. N Engl J Med. 2005;352:969-77Kucher N, et al. N Engl J Med. 2005;352:969-77

Electronic Alerts to Prevent VTEElectronic Alerts to Prevent VTE
88
90
92
94
96
98
100
0 30 60 90
Fre
edo
m f
rom
D
VT
or
PE
(%
)
Number at riskIntervention group 1,255 977 900 853Control group 1,251 876 893 839
Control group
Intervention group
P<0.001
Time (days)
Kucher N, et al. N Engl J Med. 2005;352:969-77

Cohen A et al Thromb Haemost 2005;94(4):750-9
VTE Risk Assessment for VTE Risk Assessment for Hospitalized Medical PatientsHospitalized Medical Patients
All medical patients All medical patients should be routinely should be routinely
assessedassessedand considered for and considered for
thromboprophylaxisthromboprophylaxis
Is the patient > 40 years Is the patient > 40 years old with acute medical old with acute medical
illness and reduced illness and reduced mobility?mobility?
Does the patient have one of the following Does the patient have one of the following acute medical illnesses/conditions?acute medical illnesses/conditions?
Evidence-based:
■ Acute MIAcute MI■ Acute heart failure—NYHA III/IVAcute heart failure—NYHA III/IV■ Active cancer requiring therapyActive cancer requiring therapy■ Severe infection/sepsisSevere infection/sepsis■ Respiratory disease (respiratory failure Respiratory disease (respiratory failure
with/without mechanical ventilation, with/without mechanical ventilation, exacerbations of chronic respiratory exacerbations of chronic respiratory disease)disease)
■ Rheumatic disease (including acute Rheumatic disease (including acute arthritis of lower extremities and vertebral arthritis of lower extremities and vertebral compression)compression)
■ Ischemic strokeIschemic stroke■ ParaplegiaParaplegia
Consensus view only:
■ Inflammatory disorder with immobilityInflammatory disorder with immobility■ Inflammatory bowel diseaseInflammatory bowel disease
YESYES
Does the patient have one of the following Does the patient have one of the following risk factors?risk factors?
Evidence-based in acutely ill medical patients:
■ History of VTEHistory of VTE■ History of malignancyHistory of malignancy■ Concurrent acute infectious diseaseConcurrent acute infectious disease■ Age > 75 yearsAge > 75 years
Consensus view only:
■ Prolonged immobilityProlonged immobility■ Age > 60 yearsAge > 60 years■ Varicose veinsVaricose veins■ ObesityObesity■ Hormone therapyHormone therapy■ Pregnancy/postpartumPregnancy/postpartum■ Nephrotic syndromeNephrotic syndrome■ DehydrationDehydration■ ThrombopiliaThrombopilia■ ThrombocytosisThrombocytosis

Cohen A et al Thromb Haemost 2005;94(4):750-9.
VTE Risk Assessment for VTE Risk Assessment for Hospitalized Medical PatientsHospitalized Medical Patients
Is pharmacological Is pharmacological thromboprophylaxis thromboprophylaxis
contraindicated?contraindicated?
YESYES
Mechanical Mechanical thromboprophylaxis with thromboprophylaxis with graduated compression graduated compression stockings or intermittent stockings or intermittent
pneumatic compression is pneumatic compression is recommendedrecommended
YESYES
LMWH (enoxaparin 40 mg o.d. or LMWH (enoxaparin 40 mg o.d. or dalteparin 5000 IU o.d.) or dalteparin 5000 IU o.d.) or
UFH (5000 IU t.i.d.) UFH (5000 IU t.i.d.) (LMWH preferred due to (LMWH preferred due to
better safety profile)better safety profile)
NONO
No evidence for the benefits of No evidence for the benefits of thromboprophylaxis. However, thromboprophylaxis. However,
patients should be considered for patients should be considered for thromboprophylaxis on a case-by-thromboprophylaxis on a case-by-
case basiscase basis
NONO

ConclusionsConclusions
Current practices of VTE prophylaxis in the Current practices of VTE prophylaxis in the cancer patcancer patientient
► Cancer surgical patients have an increased risk of Cancer surgical patients have an increased risk of VTE and fatal PE despite prophylaxisVTE and fatal PE despite prophylaxis
► Prophylaxis with LMWH or UFH reduces Prophylaxis with LMWH or UFH reduces venographic VTE but not CVC-related thrombosisvenographic VTE but not CVC-related thrombosis
► Out-of-hospital prophylaxis with LMWH is Out-of-hospital prophylaxis with LMWH is warranted in specific surgical cancer populationswarranted in specific surgical cancer populations
► Prophylaxis in hospitalized non-surgical cancer Prophylaxis in hospitalized non-surgical cancer patients is suboptimalpatients is suboptimal
► Compliance with ACCP and NCCN guidelines is Compliance with ACCP and NCCN guidelines is poorpoor