Embed Size (px)
Citation preview

Welcome! Neonatal Abstinence
Syndrome Project
November Action Period Call
Ohio Perinatal Quality Collaborative November 17, 2016

Welcome to the OPQC NAS November 2016 Action Period Call
Thank you for joining; please sign in the chat box with the names of all webinar participants and hospital affiliation.

The line will be placed on Group Mute
To ask a question:Click on the Raised Hand icon
You can type your question in to the Chat Box
You can use *6 to come off of GROUP MUTE (and *6 to go back on).
3

Time Topic Presenter12:00 pm Welcome & Agenda Review Susan Ford, MSN, RN
12:05 pm Data Overview Rick McClead, MD
12:15 pm Sustainability: do you have a plan??
Presenting your site’s participation in the OPQC NAS Collaborative Project
Susan Ford
12:40 pm Team Discussion All Teams
12:50 pm Next Steps Susan Ford
Agenda
REMEMBER:You can use *6to come off of GROUP MUTE

Key Driver DiagramProject Name: OPQC Neonatal NAS Leader: Walsh
SMART AIM
KEY DRIVERS INTERVENTIONS
By increasing identification of and
compassionate withdrawal treatment for full-term infants born with
Neonatal Abstinence Syndrome (NAS), we will
reduce length of stay by 1 day across participating sites by June 30, 2016.
Improve recognition and non-judgmental support for Narcotic
addicted women and infants
Connect with outpatient support and treatment program prior to
discharge
Standardize NAS Treatment Protocol
Optimize Non-Pharmacologic Rx Bundle
Initiate Rx If NAS score > 8 twice. Stabilization/ Escalation Phase Wean when stable for 48 hrs by 10%
daily.
Swaddling, low stimulation. Encourage kangaroo care Feed on demand- MBM if appropriate
or lactose free, 22 cal formula
All MD and RN staff to view “Nurture the Mother- Nurture the Child”
Monthly education on addiction care
Attain high reliability in NAS scoring by nursing staff
Partner with Families to Establish Safety Plan for Infant
• Fulltime RN staff at Level 2 and 3 to complete D’Apolito NAS scoring training video and achieve 90% reliability.
Establish agreement with outpatient program and/or Mental Health
Utilize Early Intervention Services
Collaborate with DHS/ CPS to ensure infant safety.
Prenatal Identification of MomImplement Optimal Med Rx Program
Engage families in Safety Planning. Partner with other stakeholders to influence policy and primary
prevention. Provide primary prevention materials to sites.
To reduce the number of moms and babies with narcotic exposure, and
reduce the need for treatment of NAS.
GLOBAL AIM












Sustainability
• IHI Getting Started Kit: Sustainability and Spread How-to Guide
• http://www.ihi.org/resources/Pages/Tools/HowtoGuideSustainabilitySpread.aspx

Creating a new system
Improvement
Hold GainsTest Implement
I. During testing
II. During implementation
III. After implementation

What is your team’s status?Are you ready to hold the gains?

What if your entire project team decided to retire by December 31, 2016?
Would the changes you’ve made continue to be used? What could make your organization revert to the old system?

Sliding back to the old systemOld System New System
• “We met our goals”• “We assumed the improvement would hold”• Other priorities took all resources away
(not on senior management’s radar screen)• Did not learn how to hold the gains• Infrastructure not in place

Keys to Holding the Gains
Communication
Infrastructure
Design effective ‘control’ system
Data

Communication
• Make clear to all stakeholders the Aim, successes, learnings, and benefits
• Document what you’ve done
• Keep in contact

Infrastructure• Address training and development of new skills
• Make changes to job descriptions, policies, and procedures
• Assign ownership for improvement and maintenance work of the new process
• Senior leaders held responsible for the efforts to sustain the change and remove inhibitors that might allow slippage back to the old system

• Standardize crucial steps in the new process
• Clarify individual responsibility/authority
• Design training for new employees
• Define some “simple rules” to guide the practice
• Build in Structures to “Foolproof” Change – In each of the intervention areas, the organization builds structures
(e.g., IT systems, packaged materials that support a given intervention) that make it difficult—if not impossible—for providers of care to revert to old ways of doing things.
– Speaks to our work with High Reliability!
Design an Effective “Control” System

Data• Use periodic self audits to verify practices
are being followed
1.) Ongoing Finnegan Scoring inter-rater reliability
2.) Review/audit of pharmacological bundle compliance (or non-pharmacological bundle compliance)

Are you ready to “Hold the Gains”?• Was your collaborative team successful?
• Is it your team’s intention to hold the gains?
• Is it an organizational priority?
• Is the leadership responsibility clear?
• Is the appropriate infrastructure in place?
• Do you plan to attend to measures?– Will there be ongoing measurement?– Will you ensure reliability by identifying
and understanding ‘failures’?

Follow up survey: IHI Breakthrough Series participants
• Question: Why do you believe you have maintained performance levels?
Top 3 responses:– Ongoing measurement
(keep reviewing your data!!)– Leadership involvement– Continued use of improvement methods
(continuous quality improvement)

IHI Survey of Successful Teams
Question % yesAre you still tracking your performance? 85%
Is there periodic reporting to leadership regarding performance?
88%
Were other residual benefits gained in the improvement process that took hold?
91%
Do you and your colleagues continue to use improvement methodology in your work?
91%

IHI Survey of Successful Teams
Question % yesDid the team begin to plan how to sustain its progress early on in the improvement process?
78%
Did you document the improvement process? 81%
Did you document the process of holding performance at your new level?
66%
Was a financial return on investment tied to the improvement that occurred?
16%
Has the team taken specific action in order to make the improvement process more permanent?
70%

Through collaborative use of improvement science methods, reduce preterm births & improve perinatal and preterm newborn outcomes in Ohio as quickly as possible.
Your Hospital Name here
Ohio Perinatal Quality Collaborative
Neonatal Abstinence Syndrome Project

Neonatal Abstinence Syndrome (NAS)• It is estimated that one infant is born exposed to maternal in-utero narcotic abuse
every hour in the United States. The NAS epidemic is steadily increasing, overwhelming social service systems and public payers.
• Treating newborns impacted by NAS was associated with nearly $100 million in healthcare expenses and almost 25,000 days in Ohio hospitals in 2013, according to data from the Ohio Hospital Association.
• The OPQC NAS initiative was begun to reduce variation in identification and treatment and to optimize the care of infants with NAS across Ohio.
• During the first phase of improvement work (2014-2015), 54 OPQC NAS site teams participated in adapting the Ohio Children’s Hospital Association (OCHA) care bundles, emphasizing compassionate care of infants and mothers, and standardizing both identification of affected infants and use of non-pharmacologic and pharmacologic care practices. In phase-2 of the project (2015-2016) OPQC teams participated in one of four formula groupings to better identify what works
best to improve non-pharmacologic support for infants with antenatal opiate exposure.

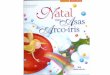
NAS Statewide Rate per 10k
14 19 21 25
3350
70
88
108121
134
0
20
40
60
80
100
120
140
160
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Rat
e pe
r 10,
000
Year
Source: Ohio Hospital Association

Promedica Toledo Children’s & ProMedica
Toledo - Normal Newborn
Miami Valley
Mercy Anderson
Aultman
Mt. Carmel EastOSU
UH Rainbow Babies & Children’s
Bethesda North Hospital
Nationwide Dublin Methodist
Akron Children’s Summa
Cincinnati Children’s
Hillcrest HospitalFairview Hospital
ClevelandClinic
Dayton Children’s
NationwideRiverside Methodist
Nationwide Grant
Nationwide Mt. Carmel St. Ann’s
UH Cincinnati
Good Samaritan Hospital
MetroHealth
Mt. Carmel WestNationwide Doctor’s
Akron Children’s
NationwideChildren’s
Mercy Children’s Hospital
Atrium Medical CenterFort Hamilton
Mercy Hospital Fairfield
Mercy Medical Center Canton
The Christ Hospital
St. Rita’sMedical Center
Southview Medical Center
Good Samaritan Hospital Dayton
Kettering
Mercy Health West
Southern Ohio Medical Center
Genesis Healthcare System
Marion General
Elyria Medical Center -UH
Mercy Regional Medical Center Lorain
ProMedica Bay Park
Lima Memorial Health System
Springfield RegionalMedical Center
Adena Regional
Medical Center
Soin Medical Center
Upper Valley Medical Center
Licking Memorial Health System
NAS Participating Sites
1/2014 start Level 3 and Level 2 teams
Akron Children’s St. Elizabeth
Health Center/Mahoning
Valley
Trumbull Memorial
4/2014 start Level 2 teams
Move circle over your hospital

Improve recognition and non-judgmental support for narcotic-addicted women and infants
Attitude Measures Survey:• To what extent are adverse life circumstances likely to be responsible for a person's
problematic drug use?
• To what extent is an individual personally responsible for their problematic drug use?
• To what extent do you feel angry towards people using drugs?
• To what extent do you feel disappointed towards people using drugs?
• To what extent do you feel sympathetic towards people using drugs?
• To what extent do you feel concerned towards people using drugs?
• To what extent do people who use drugs deserve the same level of medical care as people who don't use drugs?

Improve recognition and non-judgmental support for narcotic-addicted women and infants
Your Hospital Name

Optimize non-pharmacologic prescription bundle
Aggregate: 40% breast fed Your Hospital Name: %
• Add your site specific graph here.
• https://portal.opqc.net/NAS/SitePages/Home.aspx

Standardize NAS treatment protocol:% of infants that receive pharm tx
Aggregate: median 40.8% Your Hospital Name: %
• Add your site specific graph here.
• https://portal.opqc.net/NAS/SitePages/Home.aspx

Standardize NAS treatment protocol:length of treatment (LOT)
Aggregate: median 14.8 days Your Hospital Name: %
• Add your site specific graph here.
• https://portal.opqc.net/NAS/SitePages/Home.aspx

Standardize NAS treatment protocol:Length of Stay (LOS)
Aggregate: median 19.5 days Your Hospital Name
• Add your site specific graph here.
• https://portal.opqc.net/NAS/SitePages/Home.aspx

Connect with outpatient support and treatment program prior to discharge
Highlight your work/outreach to regional outpatient support agency. This was included in the January 2105 Learning Session Storyboard.

Your Site NamePDSA Ramp
Hunches Theories
Ideas
Changes That Result in
Improvement
A PS D
A PS D
Very Small Scale Test
Follow-up Tests
Wide-Scale Tests of Change
Implementation of Change
Detail your team’s PDSAs



Next Steps
• Please continue to submit all NAS Data using the current Data Collection Form for all babies (non pharm & pharm tx) thru December 31, 2106.
• There will be a new Data Collection Form for NAS Sustain Phase (starts 1/1/17). This will be reviewed on December’s Action Period Calls.
• December Action Period Calls: – Tuesday, December 13th from 3pm -4pm– Thursday, December 15th from 12N-1pm

The OPQC NAS Project is funded by The Ohio
Department of Medicaid

















![Untitled-2 [contents.iptime.co.kr]contents.iptime.co.kr/~contents/link/NAS-II.pdf · 2018-10-01 · Windows 192.1680250 admin ipTIME NAS NAS ëë..l admin ipTIME NAS](https://img.pdfslide.us/doc/110x75/5ec53605e2d46f7ca85b5c6b/untitled-2-contentslinknas-iipdf-2018-10-01-windows-1921680250-admin.jpg)