Embed Size (px)
Citation preview

DISEASE MANAGEMENT: A CASE FOR COST EFFECTIVENESS AND QUALITY CARECARE
Presented byRob ParkeLalit BavejaJaiwardhan VijJaiwardhan Vij
F b 12 13 2009February 12-13, 2009

Agendag
India’s Chronic Disease Burden India s Chronic Disease BurdenOverview of Disease Management (DM)O i f DM i I diOverview of DM in IndiaEvolution and current state of DM globallyValue Proposition and actuarial issues in estimating ROIThe outlook for DM in IndiaDiscussion
2 February 12-13, 2009

Lalit Bavejaj
India’s Chronic Disease Burden India s Chronic Disease BurdenOverview of Disease Management (DM)O i f DM i I diOverview of DM in India
3 February 12-13, 2009

India’s Chronic Disease Burden
Over 35 million people with diabetes expected to increaseOver 35 million people with diabetes, expected to increase around 80 million by 2030
50% f th ld’ di ill b f I di b th 50% of the world’s cardiac cases will be from India by the year 2012H t i i t d t t lHypertension cases is expected to see a quantum leap from an estimated 118.2 million in 2000 to 213.5 million in 20252025.
4 February 12-13, 2009

Key Healthcare Issuesy
Rising medical trendRising medical trend• Focus is on the treatment of acute conditions rather than preventive care
No incentives to treat all aspects of chronic conditionsNo incentives to treat all aspects of chronic conditions.Poor quality
• Health care is uncoordinated, wasteful and lacks continuity, y
Declining health Status & poor patient-compliance • More than 50% of the medicines prescribed are not taken at all• Only 4% patients followed dietary advice and • 55% had uncontrolled clinical outcomes
Need to trounce India’s growing chronic disease burden
5 February 12-13, 2009

Overview of Disease Management (DM) g ( )
DM is a process of reducing healthcare costs and/orDM is a process of reducing healthcare costs and/or improving quality of life for individuals by preventing / minimizing the effects of a disease usually a chronicminimizing the effects of a disease, usually a chronic condition, through integrative care.
DM brings two stream together• Managing clinical activitiesg g• Interventions for financial outcomes
6 February 12-13, 2009

The Care Continuum – where it all fits
Wellness Disease Management
Source: Adapted from Healthways Investor report.
7 February 12-13, 2009

Do DM/Wellness Make Sense?
10%1%
Terminally Ill End of Life Care & Case
% of Plan Membership % of Medical CostsType of Intervention
15%
20%10%
At Risk for C
Chronically IllManagement
55%Chronic Illness Disease Management
64%20%
Healthy Lifestyle Programs
15%Wellness & Prevention
Source: Boston Consulting Group and Banc of America Securities LLC estimates.
8 February 12-13, 2009

Course of action of DM
Identify chronically ill populations Identify chronically ill populationsStratify chronics into risk levelsN ll hi h i k h i tNurses call high risk chronics to encourage compliance/adherence with health management protocolsM ili d th t h ti iti t l i k h iMailings and other outreach activities to low risk chronics5 core disease states “common chronic”
CAD CHF COPD th di b t– CAD, CHF, COPD, asthma, diabetes
Other programscancer depression obesity ESRD rare diseases– cancer, depression, obesity, ESRD, rare diseases
9 February 12-13, 2009

Course of action of Wellness
Identify at risk populations (HRAs and biometric testing) Identify at risk populations (HRAs and biometric testing)Assist at risk populations voluntarily change behaviors associated with modifiable risk factorsassociated with modifiable risk factorsOn-line, telephonic and worksite coaching, mailings and other outreach activitiesother outreach activities
10 February 12-13, 2009

Common Wellness ProgramsgSmoking cessationCholesterol managementCholesterol management Hypertension management Exercise/Physical fitnessyNutritionWeight controlCancer detection/preventionBack care
S b t b tiSubstance abuse preventionStress management Jobs hazards/injury prevention Jobs hazards/injury prevention Flu shots
11 February 12-13, 2009

Benefits to Stakeholders
Individual Government Health Providers PharmaIndividual Government Health Plans and
Payers
Providers PharmaCompanies
Improved Healthier Competitive Improved Increased Improved quality of life
Convenience
Healthier more productive population
Competitive differentiator
Reduced
Improved compliance with best practice
Increased sales
Public e.g. services at home
Reduced
p p
Reduced spending on healthcare
costsp
relations
Reduced costs from unwarranted use of acute
healthcare
services
12 February 12-13, 2009

Status of DM in India
DM at a nascent stageDM at a nascent stageLess than 10% of population covered by some form of health insurancehealth insuranceProducts to cover chronic conditions are yet to fully developN ti l P b th tNational Programs by the government
13 February 12-13, 2009

Status of DM in India ………………………………continued
Pharma Sponsored DMPharma Sponsored DMSpecialist Diabetes CentersI C Di b t C Insurance Company Diabetes CareStand alone DMOGuidelines and treatment protocolsDisease Management Association of India
14 February 12-13, 2009

Rob Parke
Evolution and current state of DM globallyEvolution and current state of DM globallyTrends Driving the demand for DM/WellnessM j Th t t DMOMajor Threats to DMOs
15 February 12-13, 2009

Evolution and current state of DM globallyg y
DM began in the USA in the early 1980sDM began in the USA in the early 1980sSoon after HMO staff/ group model embraced the conceptPh ti l i id tifi d it t tPharmaceutical companies identified it as a way to promote and sell drugs.S l t t d i th id 1990 t d lSeveral entrepreneurs stepped in the mid-1990s to develop independent Disease Management Organizations (DMOs) Industry has since grown to $2 billion a year Industry has since grown to $2 billion a year.
Th l ti t t d f t ti i l diThe evolution started from targeting single disease transformed to cover numerous diseases and co-morbidities and most recently wellness programs
16
morbidities and most recently wellness programs. February 12-13, 2009

The Market for DM
Estimated Annual Disease Management RevenuesEstimated Annual Disease Management Revenues (Estimates for 2007)
$2,000.0 100%95%
$1,400.0
$1,600.0
$1,800.0
$2,000.0
70%
80%
90%
100%
60%
41%$800.0
$1,000.0
$1,200.0
$ , 00 0
Rev
enue
(in
Mill
ions
)
40%
50%
60%
0%
nnua
l Gro
wth
34%28% 26% 28% 28% 29%
15%$200.0
$400.0
$600.0
$(
10%
20%
30%
An
$-1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
0%
17 February 12-13, 2009

Trends Driving the demand for DM/Wellness g
ConsumerismConsumerismPreventive care/wellness Information technology Information technologyQuality initiatives
18 February 12-13, 2009

Major Threats to DMOsj
DM/Wellness Value PropositionDM/Wellness Value Proposition• Lack of empirical support• Financial ROI methodological flaws• Purchasers expectations
Health Plan In-sourcingE il li t d i h• Easily replicated in house
• Care Management
Alternative Model of DM/Wellness like servicesAlternative Model of DM/Wellness like services• Online• Patient centered medical home by Physicians
19 February 12-13, 2009

Jaiwardhan Vijj
Value Proposition and actuarial issues in estimating ROIValue Proposition and actuarial issues in estimating ROIThe outlook for DM in India
20 February 12-13, 2009

Estimation of ROI
Three methods of calculationsThree methods of calculations
C i f t d t d iComparison of requested to approved services– May Overstate savings
Comparison of Medical expenses between control and intervention group
– Theoretically desirable but hard to achieve in practice
Comparison of pre-enrollment to post-enrollment medicalComparison of pre enrollment to post enrollment medical expenses
– Most often used
21 February 12-13, 2009

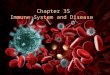
Issues in Estimating ROIgRegression to the Mean
Q1: $17,982
20,000
Commercial Diabetes Average Claim Cost
Q $ ,
16,000
Q1: $10,137 Q1 - Q4: $9,533
8 000
12,000
Cla
ims
($) 0 - 18 Years
19 + YearsWeighted Average 0 - 18Weighted Average 19 +
Q5 - Q16: $3,022
Q5 - Q16: $4,759
Q-3 - Q0: $2,995 Q1 - Q4: $4,706
4,000
8,000
Q-3 - Q0: $1,402
0 Q-3 Q-1 Q1 Q3 Q5 Q7 Q9 Q11 Q13 Q15
Quarters
22 February 12-13, 2009

Issues in Estimating ROI ………continuedg
23 February 12-13, 2009

Issues in Estimating ROI …………………continuedg
DataData– Inadequate to identify DM participant– Faulty Coding in data records leads to false positives or negativesy g p g– Difficulty getting data into decision support system
Statistical Credibility– High-cost, high-variance population is small in number
F rther attempting to adj st for pop lation differences– Further attempting to adjust for population differences
24 February 12-13, 2009

Issues in Estimating ROI …………………continuedg
TrendTrendBenefit DesignCl i Adj di tiClaim Adjudication Incurred or Paid claimsSeverityChanges in health care delivery infrastructure
25 February 12-13, 2009

Outlook for DM in India
The rising healthcare costs tied with a huge populationThe rising healthcare costs tied with a huge population Increasing incidence of Non Communicable DiseasesI d H lth di b th t & Increased Healthcare spending by the government & private sector
S d f DM i I di i tSo, need for DM in India is apparent
26 February 12-13, 2009

Outlook for DM in India …………………..continued
Alternative health insurance products coveringAlternative health insurance products covering• Chronic conditions• Outpatient care
Data quality, completeness and consistencyEncouraging collaboration among providersBehavior modification programsAppropriate use of Information Technology
27 February 12-13, 2009

DM Model
G tGovernment Is there an Actuary in the room?
DM Ins rersDMOs
IndustryInsurersDMOs
ProvidersProviders
28 February 12-13, 2009

Role of the Government
Policy maker Provider and the PayerPolicy maker, Provider and the PayerSelecting key clinicians champions as leadersFi i l i ti f id t t h i DMFinancial incentive for providers to support chronic DM Introducing appropriate clinical outcomes measuresDevelop disease registries and data collation to identify at risk population
29 February 12-13, 2009

Role of Insurers
Increase promotion of stand alone products Increase promotion of stand alone products Include DM in generic productsS t DM il tSupport DM pilot programsWork in collaboration with DMOs and providers to evaluate ththe
30 February 12-13, 2009

Role Providers
Collaborate in developing chronic DM protocolsCollaborate in developing chronic DM protocolsAdvocate the benefits of DM programs
31 February 12-13, 2009

Role of DMOs
Involve physicians and providers as key stakeholders Involve physicians and providers as key stakeholders.Establish strategic networks of providers, pharmaceuticals, diagnostics and informaticsdiagnostics and informatics.Develop new delivery strategiesD l i bl l iti th t d t t b thDevelop a viable value proposition that demonstrates both clinical improvements and financial benefits.
32 February 12-13, 2009

Discussion