Embed Size (px)
DESCRIPTION
Welcome Ask The Experts March 24-27, 2007 New Orleans, LA. AntiPlatelet Therapy in ACS and PCI Stephen D. Wiviott, MD Associate Physician, Cardiovascular Division, Brigham and Women's Hospital Investigator, TIMI Study Group Harvard Medical School Boston, MA. - PowerPoint PPT Presentation
Citation preview

Welcome Welcome Ask The ExpertsAsk The Experts
March 24-27, 2007March 24-27, 2007
New Orleans, LANew Orleans, LA

AntiPlatelet Therapy in ACS and PCI
Stephen D. Wiviott, MDAssociate Physician, Cardiovascular
Division, Brigham and Women's Hospital Investigator, TIMI Study Group
Harvard Medical School Boston, MA
Antiplatelet Therapy in ACS and Antiplatelet Therapy in ACS and PCI: Challenges and Future PCI: Challenges and Future
DirectionsDirectionsStephen D. WiviottStephen D. Wiviott
Cardiovascular DivisionCardiovascular DivisionBrigham and Women’s HospitalBrigham and Women’s Hospital
Harvard Medical SchoolHarvard Medical School TIMI Study Group TIMI Study Group

DisclosuresDisclosuresSpeakers Bureau: Pfizer; CME Honoraria: Speakers Bureau: Pfizer; CME Honoraria:
Eli Lilly, Merck, Pfizer, Sankyo; Eli Lilly, Merck, Pfizer, Sankyo; Accumetrics. Consultancies: Amgen, Accumetrics. Consultancies: Amgen,
Transform Pharmaceuticals, Forrest Labs, Transform Pharmaceuticals, Forrest Labs, Biogen-Idec, Sanofi-AventisBiogen-Idec, Sanofi-Aventis
TIMI Study GroupTIMI Study Group Receives Research Receives Research Funding From: Eli Lilly, Sankyo, Merck, Funding From: Eli Lilly, Sankyo, Merck, Schering Plough, Pfizer, Sanofi-Aventis, Schering Plough, Pfizer, Sanofi-Aventis, Astra Zeneca, CV Therapeutics, Corvas, Astra Zeneca, CV Therapeutics, Corvas,
AccumetricsAccumetrics

1 0
1 2
Dual Antiplatelet Rx for PCI Dual Antiplatelet Rx for PCI
8.6
2.7
11
6.2
1.6
5.7
0.5
5.8
0
2
4
6
8
10
12 OAC + ASATiclopidine + ASA
Circ 102: 624,2000
ISAR FANTASTIC STARS MATTIS CLASSICS
% M
AC
E
0.91.5 1.2

CURE
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0.14
Cum
ulat
ive
Haz
ard
Rat
e
Clopidogrel Clopidogrel + ASA*+ ASA*
33 66 99
Placebo Placebo + ASA*+ ASA*
Months of Follow-UpMonths of Follow-Up
11.4%11.4%
9.3%9.3%
20% RRR20% RRRPP < 0.001 < 0.001
N = 12,562N = 12,562
00 1212
* In combination with standard therapy
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Primary End Point - MI/Stroke/CV Primary End Point - MI/Stroke/CV DeathDeath
NSTEACS: Clopidogrel (300/75) vs Placebo

Co
mb
ined
En
dp
oin
t C
om
bin
ed E
nd
po
int
Occ
urr
ence
(%
)O
ccu
rren
ce (
%)
Days From RandomizationDays From Randomization
No-PT - Placebo*No-PT - Placebo*
PT- Clopidogrel*PT- Clopidogrel*
00
55
1010
00 77 1414 2121 2828
PT = Pre-treatmentPT = Pre-treatment
*Plus ASA and other standard therapies*Plus ASA and other standard therapies
Death, MI, UTVR- PP PopulationDeath, MI, UTVR- PP Population
18.5% 18.5% RRRRRR
P=0.23P=0.23
99
88
11
44
33
22
77
66
8.3%8.3%
6.8%6.8%
Steinhubl S, Berger P, Tift Mann III J et al. Steinhubl S, Berger P, Tift Mann III J et al.
JAMAJAMA. 2002;Vol 288,No 19:2411-2420.. 2002;Vol 288,No 19:2411-2420.
Early Effects of Pre-treatment with Early Effects of Pre-treatment with Clopidogrel – 28 Day ResultsClopidogrel – 28 Day Results

- 6
- 5
- 4
- 3
- 2
0 5 10 15 20 25 30
Hours Prior to PCI of Study Drug Loading Dose
Lo
g O
dd
s o
f D
eath
, MI o
r U
TV
R a
t 28
Day
s
Placebo
Clopidogrel
P=0.020for treatment/timing
interaction
CREDO: Clopidogrel Loading Dose Timing and Risk of MACE
Steinhubl, et al

Limitations of Current thienopyridines
Slow onset: requires prolonged pretreatment for PCI efficacy
Bleeding (especially related to CABG)
Modest levels of platelet inhibition
Variability of response

The First Clopidogrel Resistance Study (300 mg):The First Clopidogrel Resistance Study (300 mg): A “Fingerprint” of Clopidogrel Response A “Fingerprint” of Clopidogrel Response Variability
2 Hours 24 Hours
5 Days 30 Days
Aggregation (%)
Resistance = 63% Resistance = 31%Resistance
Resistance = 31%
Resistance
Resistance = 15%
Gurbel PA, et al. Circulation. 2003;107: 2908-2913.
Aggregation (%) Aggregation (%)
Resistance
Pat
ien
ts (
%)
12
24
≤ -30(-30,-20]
(-20,-10](-10,0]
(0,10](10,20]
(20,30](30,40]
(40,50](50,60]
>60
Pat
ien
ts (
%)
11
22
≤ -10 (-10,0] (0,10] (10,20] (20,30] (30,40] (40,50] (50,60] >60
14
28
≤ -30(-30,-20]
(-20,-10](-10,0]
(0,10](10,20]
(20,30](30,40]
(40,50](50,60]
>60
10
20
≤ -30(-30,-20]
(-20,-10](-10,0]
(0,10](10,20]
(20,30](30,40]
(40,50](50,60]
>60
Aggregation (%)
Resistance
Pat
ien
ts (
%)
Pat
ien
ts (
%)

Potential Mechanisms of Response Variability
Extrinsic Mechanisms•Non-compliance
•Under-dosing
•Drug-drug interactions
•Absorption and/or metabolism
•Patient Factors (DM, ACS, etc…)
Intrinsic Mechanisms•P2Y12 receptor affinity (ADP or Drug) or number
•Variable response to agonist:
•Release
•GP IIb/IIIa receptor activationWiviott and Antman Circ 2004

CYP 3A4 Activity* Correlates Inversely with Platelet Aggregation
Following Clopidogrel Loading
*Erythromycin breath test. Lau WC, et al. Circulation. 2004;109:166-171.
Pla
tele
t A
gg
reg
atio
n (
%)
14CO2 Exhaled/Hour (%)
r=–0.6P=0.003
100
90
80
70
60
50
40
30
20
10
00 .5 1 1.5 2 2.5 3 3.5 4

Clinical Importance of Response Variability ?
Failure of Therapy = Drug Resistance
Failure of Therapy Successful Therapy
Lesser Response
Greater Response

0
20
40
60
80
100
120
0
10
20
30
40
5 µM ADP induced plt agg Death/ACS/CVA by 6 m
Days1 2 3 4 5 6
Bas
elin
e (%
)
Quartiles of response
Q1
Q2
Q3
Q4
Clop resist 40
6.7
0 0P
erce
nt
P=0.007
Q1 Q2 Q3 Q4
Matetzky S, et al. Circulation. 2004;109:3171-3175.Wiviott SD, Antman EM. Circulation. 2004 109:3064-3067.
Clopidogrel Resistance andIncreased Risk of Ischemic Events
N = 60 Prim PCI for STEMI
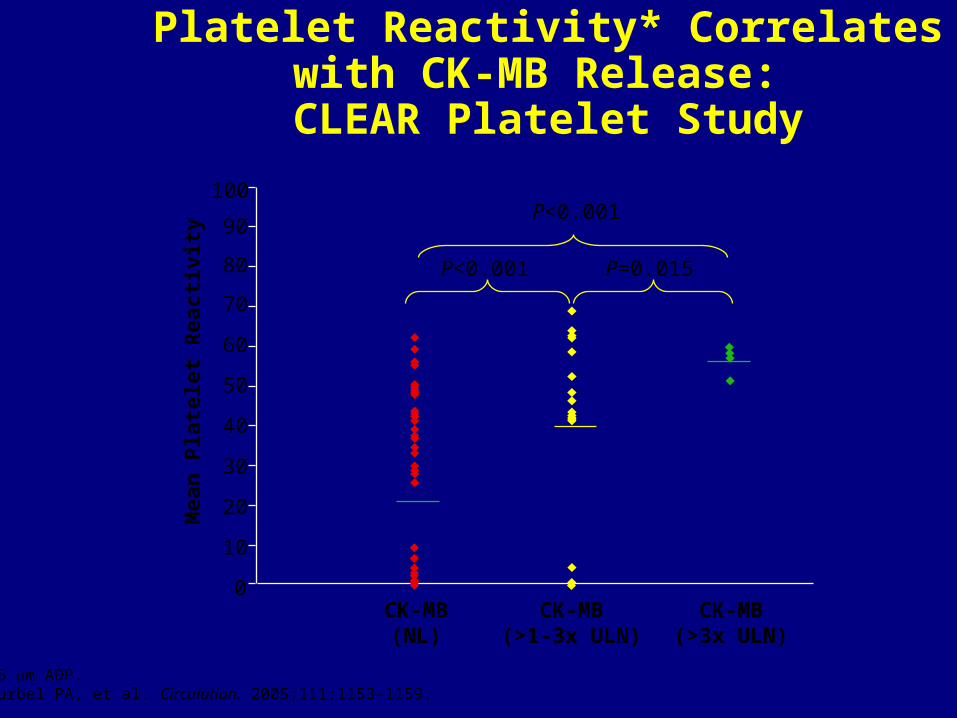
*5 m ADP.Gurbel PA, et al. Circulation. 2005;111:1153-1159.
Platelet Reactivity* Correlateswith CK-MB Release: CLEAR Platelet Study
P<0.001
P<0.001 P=0.015
CK-MB(NL)
CK-MB(>1-3x ULN)
CK-MB(>3x ULN)
100
90
80
70
60
50
40
30
20
10
0
Mea
n P
late
let
Rea
ctiv
ity

The Clopidogrel REsistance andStent Thrombosis (CREST) Study
Platelet Reactivity in Patients with SAT(N=20) versus no SAT (N=50)
LTA – 5 M ADP (%) LTA – 20 M ADP (%)
Gurbel PA, et al. J Am Coll Cardiol. 2005 (in press).
49
26
0
10
20
30
40
50
60
70
SAT No SAT
65
46
0
10
20
30
40
50
60
70
SAT No SAT
P<0.001 For Each
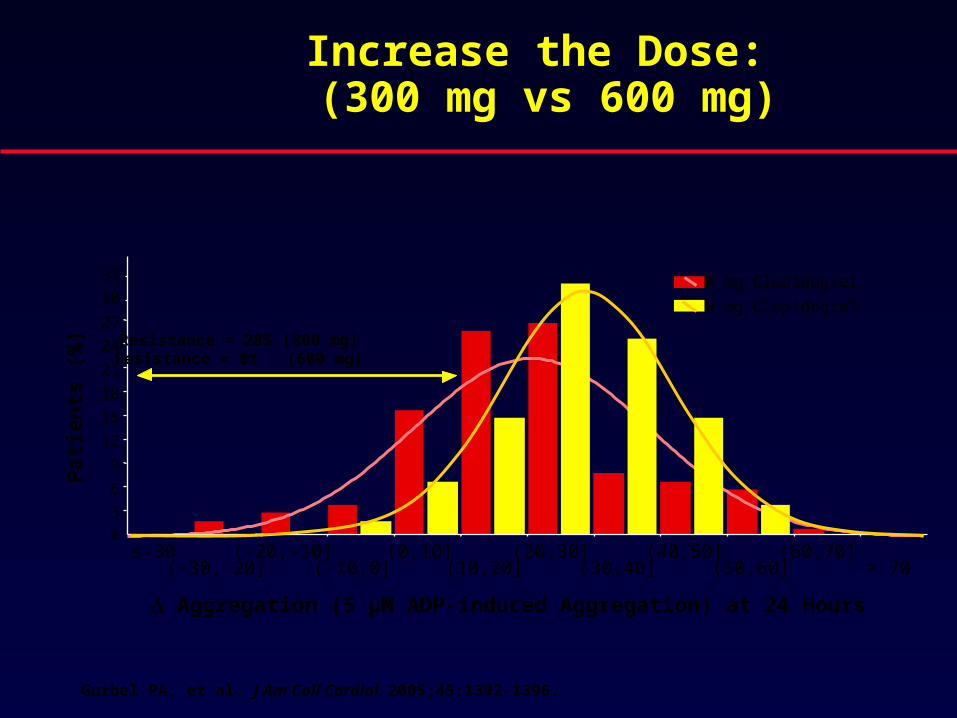
Increase the Dose: (300 mg vs 600 mg)
Gurbel PA, et al. J Am Coll Cardiol. 2005;45:1392-1396.
03
6
9
12
15
18
21
24
27
30
33
≤-30(-30,-20]
(-20,-10](-10,0]
(0,10](10,20]
(20,30](30,40]
(40,50](50,60]
(60,70]> 70
300 mg Clopidogrel
600 mg Clopidogrel
Aggregation (5 µM ADP-induced Aggregation) at 24 Hours
Pat
ien
ts (
%) Resistance = 28% (300 mg)
Resistance = 8% (600 mg)

ISAR - CHOICE
Von Beckenrath et al Circ 2005
Platelet AggregationMetabolite
Concentrations

ARMYDA-2 Trial: Primary endpointARMYDA-2 Trial: Primary endpoint
4%
12%
0%
2%
4%
6%
8%
10%
12%
14%
600 mg 300 mg
4%
12%
0%
2%
4%
6%
8%
10%
12%
14%
600 mg 300 mg
Primary Composite of death, MI, and target vessel revascularization
p = 0.04
Circulation 2005Circulation 2005
255 patients with stable CAD or UA/NSTEMI
4-8 hours prior to PCI
13% received IIb/IIa inhibitors and 20% drug-
eluting stents
255 patients with stable CAD or UA/NSTEMI
4-8 hours prior to PCI
13% received IIb/IIa inhibitors and 20% drug-
eluting stents
Primary Endpoint: Composite of death, MI, or target vessel revascularization (TVR) at 30 days
Primary Endpoint: Composite of death, MI, or target vessel revascularization (TVR) at 30 days

Clopidogrel High-Dose GroupClopidogrel High-Dose GroupClopidogrel 600 mg loading dose day 1 followed by Clopidogrel 600 mg loading dose day 1 followed by 150 mg from days 2 to 7; 75 mg from days 8 to 30150 mg from days 2 to 7; 75 mg from days 8 to 30
Clopidogrel Standard-Dose GroupClopidogrel Standard-Dose GroupClopidogrel 300 mg (+ placebo) day 1 followedClopidogrel 300 mg (+ placebo) day 1 followed
by 75 mg (+ placebo) from days 2 to 7;by 75 mg (+ placebo) from days 2 to 7;75 mg from days 8 to 3075 mg from days 8 to 30
Patients with UA/NSTEMI planned for early invasivePatients with UA/NSTEMI planned for early invasiveStrategy; ie, intend for PCI as early as possible within 24 hrsStrategy; ie, intend for PCI as early as possible within 24 hrs
RANDOMIZERANDOMIZE
PCI: Percutaneous coronary interventionUA/NSTEMI: Unstable angina/non-ST-segment elevation myocardial infarction
CClopidogrel optimal loading doselopidogrel optimal loading dose U Usagesage toto R Reduceeduce RRecurrent ecurrent EEveveNTNTs/s/OOptimal ptimal AAntiplateletntiplatelet S Strategytrategy forfor
IInterventionnterventionSS
CURRENT/OASIS 7CURRENT/OASIS 7
RANDOMIZERANDOMIZERANDOMIZERANDOMIZE
ASA low-dose groupASA low-dose groupAt least 300 mg day 1;At least 300 mg day 1;
75–100 mg75–100 mgfrom days 2 to 30from days 2 to 30
ASA high-dose groupASA high-dose groupAt least 300 mg day1;At least 300 mg day1;
300–325 mg300–325 mgfrom days 2 to 30from days 2 to 30
ASA high-dose groupASA high-dose groupAt least 300 mg day 1;At least 300 mg day 1;
300–325 mg300–325 mgfrom days 2 to 30from days 2 to 30
ASA low-dose groupASA low-dose groupAt least 300 mg day 1;At least 300 mg day 1;
75–100 mg75–100 mgfrom days 2 to 30from days 2 to 30

Change the Agent?Change the Agent?Change the Agent?Change the Agent?
PrasugrelPrasugrel
Sankyo Ann Report 51:1,1999
Pro-drugPro-drugPro-drugPro-drug
OxidationOxidation(Cytochrome P450)(Cytochrome P450)
OxidationOxidation(Cytochrome P450)(Cytochrome P450)
HOOCHOOC
* HS* HS
NN
OO
FF
Active MetaboliteActive MetaboliteActive MetaboliteActive Metabolite
NN
SS
OO
FFOO
Sem Vasc Med 3:113, 2003
HydrolysisHydrolysis(Esterases)(Esterases)
HydrolysisHydrolysis(Esterases)(Esterases)
NN
SS
OO
CCHH33
CCOO
FFOONN
SS
OO
ClCl
OO CHCH33CHCH33CCCC
ClopidogrelClopidogrel
85% Inactive 85% Inactive MetabolitesMetabolites
EsterasesEsterases
85% Inactive 85% Inactive MetabolitesMetabolites
EsterasesEsterases
NN
SS
OO
ClCl
OO CHCH33CHCH33CCCC
OONN
SS
OO
ClCl
OO CHCH33CHCH33CCCC
Active MetaboliteActive MetaboliteActive MetaboliteActive Metabolite
HOOCHOOC
* HS* HS
NN
OO
ClCl
OCH3OCH3

Inhibition of Platelet AggregationInhibition of Platelet Aggregation(IPA) at 24 Hours (Healthy Volunteers)(IPA) at 24 Hours (Healthy Volunteers)Inhibition of Platelet AggregationInhibition of Platelet Aggregation(IPA) at 24 Hours (Healthy Volunteers)(IPA) at 24 Hours (Healthy Volunteers)
-20.0-20.0
0.00.0
20.020.0
40.040.0
60.060.0
80.080.0
100.0100.0
Inhi
bitio
n of
Pla
tele
t Agg
rega
tion
(%)
Inhi
bitio
n of
Pla
tele
t Agg
rega
tion
(%)
Response to Response to PrasugrelPrasugrel
Response to Response to ClopidogrelClopidogrel
Clopidogrel ResponderClopidogrel Non-responder
*Responder = *Responder = 25% IPA at 4 and 24 25% IPA at 4 and 24 hh
Inte
rpat
ien
t Va
ria
bilit
y
Interp
atient
Va
riab
ility
Brandt, Payne, Wiviott et al AHJ 2007

Inhibition of Platelet Aggregation (Stable Atherosclerosis)
Inhibition of Platelet Aggregation (Stable Atherosclerosis)
Prasugrel (40 mg LD/5 mg MD)
Prasugrel (40 mg LD/7.5 mg MD)
Prasugrel (60 mg LD/10 mg MD)Prasugrel (60 mg LD/15 mg MD)
Clopidogrel(300 mg LD/75 mg MD)
Mea
n I
PA
(%
)
-10
0
10
20
30
40
50
60
70
Day/Hour Post Dosing
1/0 1/2 1/4 1/6 7/1 7/2 28/0 28/2 28/4 28/6
Loading dose (LD) Maintenance dose (MD)
Jernberg, T et al EHJ 2006

In Vitro Antiplatelet Effects of Active In Vitro Antiplatelet Effects of Active Metabolites in PRPMetabolites in PRP
* * PP < 0.05 ** < 0.05 ** PP < 0.01 vs. control < 0.01 vs. control
Prasugrel AMPrasugrel AM(IC(IC5050 = 51 = 51 μμM)M)
Prasugrel AMPrasugrel AM(IC(IC5050 = 26 = 26 μμM)M)
Clopidogrel AMClopidogrel AM(IC(IC5050 = 41 = 41 μμM)M)
(A) Rat(A) Rat (B) Human(B) Human
Concentration (Concentration (μμM)M) Concentration (Concentration (μμM)M)
7070
6060
5050
4040
3030
2020
1010
Pla
tele
t a
gg
reg
ati
on
P
late
let
ag
gre
ga
tio
n
(%)
(%)
001100 100100 100010001010
****
********
****
****
1100 1001001010
****
********
**
Pla
tele
t a
gg
reg
ati
on
P
late
let
ag
gre
ga
tio
n
(%)
(%)
8080
6060
4040
00
2020
10001000
Ogawa, et al ESC 2005.Ogawa, et al ESC 2005.
Clopidogrel AMClopidogrel AM(IC(IC5050 = 21 = 21 μμM)M)
****
****
********

Prasugrel 60 mg
0.1
1
10
100
1000
0 18126 24Time in Hr
Pla
sma
Co
nce
ntr
atio
n
(ng
/ml)
Clopidogrel 300 mg
ISTH 2005 Payne et al, P0952
Insights into Potency : Active Metabolite Insights into Potency : Active Metabolite Levels in Humans (Crossover Study)Levels in Humans (Crossover Study)

STUDY DESIGNSTUDY DESIGNSTUDY DESIGNSTUDY DESIGN
Study Drug in lab; Stratify for GP IIb/IIIa
Maintenance Rx for 30 days
PRASUGREL
LD 40 mg
MD 7.5 mg
N=200
PRASUGREL
LD 60 mg
MD 10 mg
N=200
CLOPIDOGREL
LD 300 mg
MD 75 mg
N=250
1o endpoint: Significant (non-CABG) bleeding through 30 D
2o endpoints: CV MACE through 30 D, Major Bleeding, Component Clinical Endpoints
PRASUGREL
LD 60 mg
MD 15 mg
N=250
PCI with stenting (N=900)
Wiviott et al Circ 2005

110 0 EP: Significant Non-CABG Bleeding 30 DEP: Significant Non-CABG Bleeding 30 D110 0 EP: Significant Non-CABG Bleeding 30 DEP: Significant Non-CABG Bleeding 30 D
1.2%
2.0%1.5%
1.7% 1.6%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
Clop Pras 40/7.5 60/10 60/15
P= NS
3/254 11/650 3/199 4/200 4/251R/N
P = 0.77
Prasugrel LD/MDTreatment Group
Dose RangingClop. vs Prasugrel
Wiviott et al Circ 2005

MI at 30 DMI at 30 DMI at 30 DMI at 30 D
4.0%
5.7%
7.0%6.5%
7.9%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
Clop Pras 40/7.5 60/10 60/15
P= NS
20/254 37/650 14/199 13/200 10/251R/N
RR=0.72 [0.4,1.2]
P = 0.23
Prasugrel LD/MDTreatment Group
Wiviott et al Circ 2005

ImplicationsImplicationsIn patients undergoing PCI, prasugrel:
• Demonstrated a similar safety profile to standard dose clopidogrel
• Resulted in non-significant, but lower rates of ischemic events compared to patients treated with standard doses of clopidogrel
QUESTION: Would prasugrel, with higher and more consistent levels of platelet inhibition, be superior to clopidogrel in reducing ischemic events in a trial powered to detect a clinically significant difference?

STUDY DESIGNSTUDY DESIGNSTUDY DESIGNSTUDY DESIGN
Double-blindDouble-blind
ACS (STEMI or UA/NSTEMI) & Planned PCIACS (STEMI or UA/NSTEMI) & Planned PCI
ASAASA
PRASUGRELPRASUGREL60 mg LD/ 10 mg MD60 mg LD/ 10 mg MD
PRASUGRELPRASUGREL60 mg LD/ 10 mg MD60 mg LD/ 10 mg MD
CLOPIDOGRELCLOPIDOGREL300 mg LD/ 75 mg MD
CLOPIDOGRELCLOPIDOGREL300 mg LD/ 75 mg MD
11oo endpoint: endpoint: CV death, MI, StrokeCV death, MI, Stroke22oo endpoints: endpoints: CV death, MI, Stroke, Rehosp-Rec IschCV death, MI, Stroke, Rehosp-Rec Isch
CV death, MI, UTVRCV death, MI, UTVR
Median duration of therapy - 12 monthsMedian duration of therapy - 12 months
N= 13,000N= 13,000
Wiviott et al, AHJ 2006
Enrollment CompleteEnrollment Complete January 2007January 2007

ImplicationsImplications
•Establish the safety and efficacy of prasugrel compared to clopidogrel in patients with ACS undergoing PCI in this registry pathway trial
•Proof of Concept:
Does an agent that has higher inhibition of platelet aggregation and less “thienopyridine resistance” result in improved clinical outcomes in an adequately powered clinical trial?
Wiviott et al, AHJ 2006
TIMI 38 C R Hypotheses
1.Patients withdrawn from thienopyridine at study completion will have a higher rate of stent thrombosis than those continuing therapy in the registry follow up period
2.Patients treated with DES will have higher rates of stent thrombosis than those treated with BMS over the entire treatment period (trial plus registry)
In the follow up phase, beyond completion of TRITON – TIMI 38*:
*Analyses adjusted for baseline, procedural features, and propensity for clopidogrel use

TIMI 38 C R
DES
BMS
TRITON – TIMI 38
Clinical Trial
Prasugrel vs Clopidogrel
Open LabelThienopyridine
Continue
Discontinue
Continue
Discontinue
24 M Following LPV in TRITON – TIMI 38
30 - 54 Months
Registry + Trial Duration
Registry Duration
Summary of Analytical Groups and Trial/ Registry Timing
6-15 Months
Trial Duration

Prasugrel 10 mg MD vs. Clopidogrel 75 mg MD: Higher IPA During Maintenance Dosing
mean ± SEM 20 μM ADP
Inh
ibit
ion
of
Pla
tele
t A
gg
reg
ati
on
(%
)
0
20
40
60
80
100
Loading Dose Maintenance Doses
Time Hours Days
0.25 0.5 1 2 4 6 24 3 4 5 6 7 8 90
Clop 300 mg
Clop 75 mg
††
!
!
† §
†p<0.001 vs. Clop 300!
p<0.05 vs. Clop 300§p<0.05 vs Clop 300/75
Clop 600 mg
Clop 75 mg
*
*
** * *
* * * * * * *
*p<0.001 vs. Clop 300 mg or 600 mg LD
Pras 60 mg
Pras 10 mg

Planned Elective PCIAggregometry*and Biomarkers√
ASA
CLOPIDOGREL Naive
ClopidogrelClopidogrel600 mg600 mg
Prasugrel Prasugrel 60 mg60 mg
0.5, hour post-LD Aggregometry* and Biomarkers√
Diagnostic Catheterization Anatomy Suitable for PCI
Post Cath† aggregometry
Planned GP IIb/IIIa Prohibited
N < 180
N = 100 PCI
6, 18-24 h, Aggregometry*, biomarkers
†Or 2 h whichever is sooner
Primary Endpoint: Mean IPA (6h) in all treated subjects
PHASE I
Protocol DesignPRINCIPLE – TIMI 44 (PCI Subjects Only) – Phase I

Protocol Design
√ Biomarkers (VASP, CD40L, P-selectin, LPA, Tn, CK-MB, CRP, MPO)
*Aggregometry: Primary (20 uM ADP), secondary (5 uM ADP), Accumetrics
PrasugrelPrasugrel10 mg x 14d10 mg x 14d
14 d clinical events, biomarkers
√, aggregometry*, CROSSOVER
PRINCIPLE – TIMI 44 (PCI Subjects Only) – Phase II
Clopidogrel Clopidogrel 150 mg 150 mg
x14dx14d
PrasugrelPrasugrel10 mg x 14 10 mg x 14
dd
Clopidogrel Clopidogrel 150 mg 150 mg
x14dx14d30 d clinical events,biomarkers
√, aggregometry*
Confidential
Primary Endpoint: Mean IPA (14d&30d) in all treated subjects
PHASE II PCI
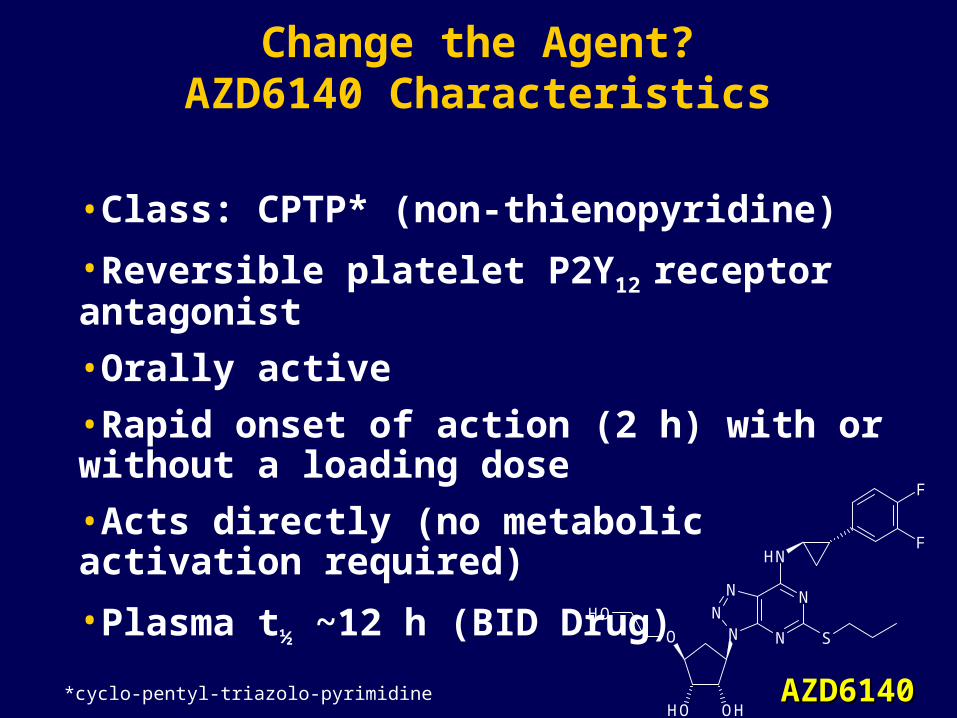
Change the Agent?AZD6140 Characteristics
*cyclo-pentyl-triazolo-pyrimidine
•Class: CPTP* (non-thienopyridine)
•Reversible platelet P2Y12 receptor antagonist
•Orally active
•Rapid onset of action (2 h) with or without a loading dose
•Acts directly (no metabolic activation required)
•Plasma t½ ~12 h (BID Drug)
OH OH
N
N
NN
NH
SNO
F
F
OH
AZD6140AZD6140

Maximal and Final IPA on Day 1 Clopidogrel Naive Patients
AZD6140 90 mg AZD6140 180 mg AZD6140 270 mg CLOP 300 mg
0
25
50
75
100
IPA
(%
)M
ea
n ±
SE
M
0
25
50
75
100
0 2 4 8 12
Time, h0 2 4 8 12
Time, h
Maximal Extent Final Extent
P<0.0176 for all AZD6140 groups vsclopidogrel at 4 h
P<0.0002 for all AZD6140 groups vs clopidogrel at 4 h




UA/NSTEMI (mod-high risk)
STEMI (if primary PCI)All Receiving ASA
Clopidogrel Treated or Naïve
ClopidogrelIf pretreated, no additional load;if naïve, standard 300 mg load,
then 75 mg od maintenance(additional 300 mg allowed pre-PCI)
Primary Endpoint: CV Death/MI/StrokeSecondary EP: CV Death/MI/Stroke/Revascularization with PCI;
CV Death/MI/Stroke; Severe Recurrent Ischemia
12 month maximum exposure12 month maximum exposure(Min=6 mo, max=12 mo, mean=11 mo)(Min=6 mo, max=12 mo, mean=11 mo)
n=18,000 ptsn=18,000 pts
AZD6140180 mg load, then
90 mg bid maintenance(additional 90 mg pre-PCI)
ClinicalTrials.gov Identifier: NCT00391872

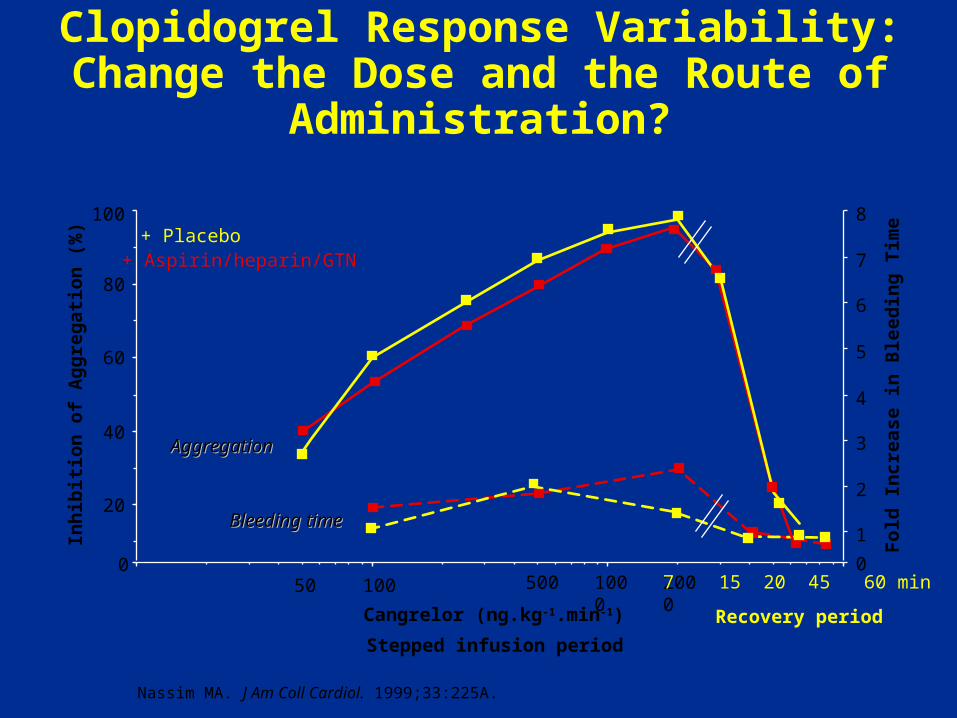
Change The Agent and the Route: Cangrelor?
Low volume of distribution, extensively protein bound
Short half-life (3-5 min), full recovery 20 min
Unlike thienopyridines, direct P2Y12 inhibition, independent of CYP 3A4 metabolism
? Competitive inhibition of clopidogrel
Fo
ld I
nc
rea
se i
n B
leed
ing
Tim
e
Stepped infusion period
Inh
ibit
ion
of
Ag
gre
gat
ion
(%
)
0
20
40
60
80
100
0
1
2
3
4
5
6
7
8
50 100 500 1000 2000
AggregationAggregation
Bleeding timeBleeding time
+ Aspirin/heparin/GTN+ Placebo
Cangrelor (ng.kg-1.min-1) Recovery period
7 15 20 45 60 min
Clopidogrel Response Variability: Change the Dose and the Route of Administration?
Nassim MA. J Am Coll Cardiol. 1999;33:225A.
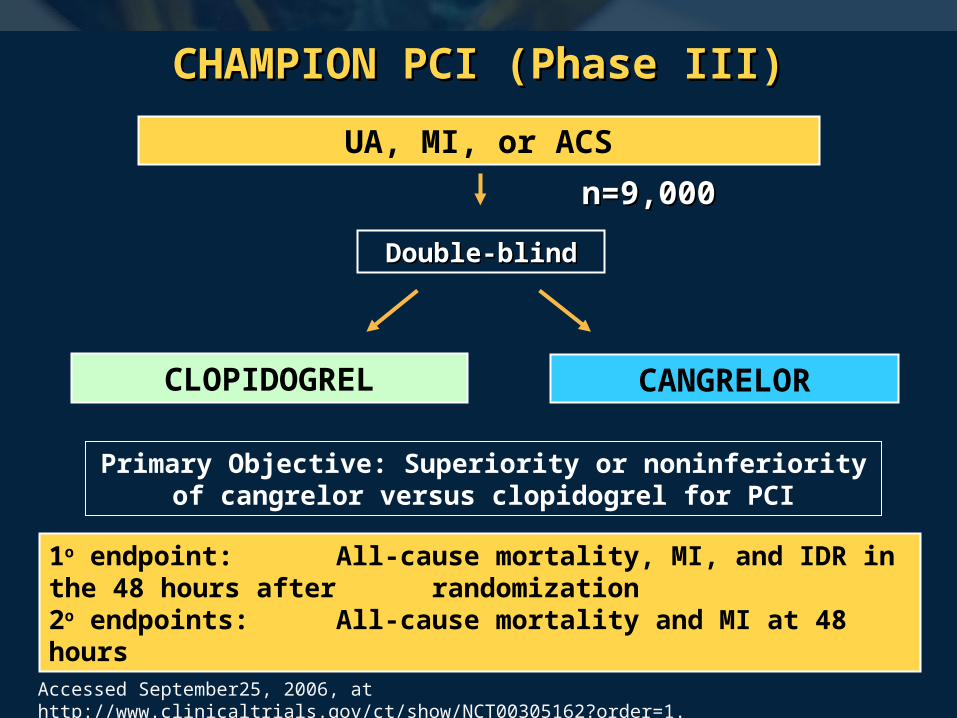
CHAMPION PCI (Phase III)CHAMPION PCI (Phase III)
Double-blindDouble-blind
UA, MI, or ACS
CANGRELORCLOPIDOGREL
1o endpoint: All-cause mortality, MI, and IDR in the 48 hours after randomization 2o endpoints: All-cause mortality and MI at 48 hours
n=9,000n=9,000
Accessed September25, 2006, at http://www.clinicaltrials.gov/ct/show/NCT00305162?order=1.
Primary Objective: Superiority or noninferiority of cangrelor versus clopidogrel for PCI

Summary
1. ADP induced platelet activation plays a central role in ACS and PCI complications
2. Thienopyridines have become a key component of therapy
3. Current thienopyridines have important limitations including response variability
4. Agents in development offer improved pharmacological profiles, and results of ongoing trials will determine clinical efficacy

Question Question
&&
AnswerAnswer

Thank You!Thank You!
Please make sure to hand in your evaluation and pick up a
ClinicalTrialResults.org flash drive





























