Embed Size (px)
Citation preview

Weight bias reduction in health professionals:a systematic review
A. S. Alberga1, B. J. Pickering1, K. Alix Hayden2, G. D. C. Ball3, A. Edwards4, S. Jelinski5,6, S. Nutter1,S. Oddie7, A. M. Sharma8 and S. Russell-Mayhew1
1Werklund School of Education, University of
Calgary, Calgary, AB, Canada; 2Libraries and
Cultural Resources, University of Calgary,
Calgary, AB, Canada; 3Department of
Pediatrics, University of Alberta, Edmonton,
AB, Canada; 4Cumming School of Medicine,
University of Calgary, Calgary, AB, Canada;5Emergency Strategic Clinical Network,
Alberta Health Services, Edmonton, AB,
Canada; 6Department of Emergency
Medicine, University of Alberta, Edmonton,
AB, Canada; 7Applied Research and
Evaluation Services, Primary Health Care,
Alberta Health Services, Edmonton, AB,
Canada; 8Faculty of Medicine and Dentistry,
University of Alberta, Edmonton, AB, Canada
Received 20 December 2015; revised 7
March 2016; accepted 5 April 2016
Address for correspondence: Shelly Russell-
Mayhew, PhD, Werklund School of Education,
University of Calgary, EDT 634, 2500
University Drive, NW Calgary, Alberta,
Canada T2N 1N4.
E-mail: [email protected]
SummaryInnovative and coordinated strategies to address weight bias among health profes-sionals are urgently needed. We conducted a systematic literature review of empir-ical peer-reviewed published studies to assess the impact of interventions designedto reduce weight bias in students or professionals in a health-related field. Combi-nation sets of keywords based on three themes (1: weight bias/stigma; 2: obesity/overweight; 3: health professional) were searched within nine databases. Oursearch yielded 1447 individual records, of which 17 intervention studies satisfiedthe inclusion criteria. Most studies (n = 15) included medical, dietetic, health pro-motion, psychology and kinesiology students, while the minority included practi-cing health professionals (n = 2). Studies utilized various bias-reduction strategies.Many studies had methodological weaknesses, including short assessment periods,lack of randomization, lack of control group and small sample sizes. Althoughmany studies reported changes in health professionals’ beliefs and knowledgeabout obesity aetiology, evidence of effectiveness is poor, and long-term effects ofintervention strategies on weight bias reduction remain unknown. The findingshighlight the lack of experimental research to reduce weight bias among healthprofessionals. Although changes in practice will likely require multiple strategiesin various sectors, well-designed trials are needed to test the impact of interven-tions to decrease weight bias in healthcare settings.
Keywords: Healthcare, obesity, prejudice, stigma.
Introduction
Despite obesity being classified as a chronic disease by theAmerican Medical Association (1), the Canadian MedicalAssociation (2) and substantial research evidence showingthe genetic basis (3) and complexity of the condition (4),stigmatization of individuals living with obesity hasincreased in frequency and intensity over the last few dec-ades (5). Weight bias, stigma and discrimination, alsoknown as negative attitudes, beliefs and behaviourstowards individuals with obesity, have been observed inhealthcare professionals and student trainees across various
health disciplines, including; physicians and medical resi-dents (6–18), medical and dental students (19–21), nurses(22–24), dieticians (25–27), kinesiologists (28,29), phy-siotherapists (30), health science students (31) and profes-sionals specializing in obesity (32,33). Up to 69% ofwomen with overweight or obesity have reported bias fromhealth providers (34).Weight bias is defined as ‘negative weight-related atti-
tudes, beliefs, assumptions and judgments toward indivi-duals who are overweight and obese (and weight stigma) isthe social sign that is carried by a person who is a victim of
© 2016 World Obesity. clinical obesity 6, 175–188 175
clinical obesity doi: 10.1111/cob.12147

prejudice and weight bias’ ((35), p. 1). Weight bias can fur-thermore be understood as a preconceived adverse judg-ment or opinion targeted at individuals perceived as fat,whereas weight discrimination is the overt behaviouralmanifestation of weight bias (e.g. derogatory humour(19), receiving unsolicited advice and inappropriate com-ments about weight (36)). Stigma can be enacted if theprovider has explicit or implicit negative attitudes aboutpeople with obesity. ‘Explicit attitudes are conscious andreflect a person’s opinions or beliefs about a group’ ((37),p. 320). Medical students’ explicit attitudes or impres-sions of patients with obesity tend to be that they arenon-compliant (20), lazy, sloppy and lacking self-control(38), less adherent to lifestyle recommendations and thatthey are personally responsible for causing their obe-sity (39).Contrary to self-reported explicit attitudes, ‘[…] peo-
ple also possess implicit or unconscious beliefs or biasesthat exist in memory but are often distinct from con-scious values and beliefs’ (40). Unconsciously associating‘fat people’ with negative words like lazy, gluttonous,stupid, undisciplined and worthless are examples ofimplicit biases. A study from a large representative sam-ple showed that both medical doctors and the generalpublic hold strong explicit and implicit weight-biasedattitudes (40).Although perhaps unintentional, there may also be more
structural stigmatizing barriers in healthcare settings, whichcan be embarrassing and increase likelihood of healthcareavoidance for patients with obesity (e.g. small waiting roomchairs and equipment like blood pressure cuffs, examina-tion gowns and weight scales too small to be functional(37) or feeling humiliated about being weighed publicly(41)). Weight bias can affect both verbal and non-verbalcommunication whereby health professionals have reportedless respect for patients living with obesity (14,18). A studythat evaluated 215 patient–physician encounters with30 different physicians in primary care showed that havingless respect for patients could predict less empathetic com-munication and less provision of information to the patients(42). Downstream effects of weight bias among health pro-fessionals include less patient-centred communication andcare such as spending less clinical contact time with them(14) and providing less information (43), which could riskfailing to refer a patient for other diagnostic testing becauseof the focus on the patient’s obesity. The negative physio-logical and psychological implications of patients experien-cing weight bias are widespread and can increase the risk ofengaging in unhealthy behaviours, including increased foodconsumption (44,45) and decreased physical activity(45,46), patient non-adherence, delay in seeking health careor its avoidance (47), feelings of anxiety, depression, lowself-esteem and suicidal thoughts (41).
Given the high prevalence of obesity worldwide andincreasing evidence of weight bias by health professionalsand its detrimental effects on patients, there is an urgentneed to address weight bias among health professionals.The purpose of this paper was to systematically reviewpeer-reviewed published interventions designed to reduceweight bias in health professionals. Other terms such asanti-fat bias, anti-fat stigma and anti-fat prejudice havealso been used synonymously with weight bias. For thepurpose of this paper, weight bias will be used as the all-encompassing term of bias, stigma and prejudice againstindividuals who are overweight or have obesity.
Methods
In conducting our review, we followed the protocol out-lined in the Cochrane Handbook for Systematic Reviews ofInterventions (48). We report our findings in accordancewith the PRISMA (Preferred Reporting Items for System-atic Reviews and Meta-Analyses) statement (49).
Data sources
A health sciences librarian (K.A.H.) developed the searchstrategy and conducted both the preliminary and the finalsearches. The search focused on three main concepts:(i) weight bias/stigma, (ii) obesity/overweight and(iii) health professional. Keywords were generated for eachconcept by reviewing subject indexing and key terms andby reviewing search strategies from similar systematicreviews. The preliminary search strategy was pre-tested toensure that relevant known studies were retrieved. Thefinal search strategy incorporated both keywords and sub-ject headings. Keywords were the same for each database,whereas subject headings were translated for each data-base. The search strategy was limited to the English orFrench language and from the publication date of 1990onwards. Searches were conducted in nine databases(MEDLINE, EMBASE, CINAHL, PsycINFO, SocINDEX,Social Work Abstracts, ERIC, Cochrane Database of Sys-tematic Reviews and Cochrane Central Register of Con-trolled Trials). The search strategy was conducted in earlyApril 2014 and was saved for each database, so it could bere-run to update the search. All searches were updated inearly September 2015 by the same librarian (K.A.H.), andabstracts were reviewed by the same researchers (A.S.A.and B.P.). The updated search identified 225 citationsindexed since April 2014.
Studies published between 1990 and September 2015were included if they met the following criteria:(i) published in English or French, (ii) original primaryempirical research and (iii) where weight bias was the focusof the intervention identified in students or professionals in
© 2016 World Obesity. clinical obesity 6, 175–188
176 Weight bias reduction in health professionals A. S. Alberga et al. clinical obesity

a health-related field. Comments, editorials, letters,abstracts and grey literature were excluded. Reference listsof related publications were also examined for furthersources not identified in online searches.
Results
The search strategy yielded 1447 abstracts of which931 were duplicates. Two authors reviewed (A.S.A. andB.P.) 516 abstracts and discussed to reach consensus ifthere was any discrepancy. We identified 17 interventionstudies (38,50–65) (12 were identified through the databasesearch and five previously identified through personallibraries). Five studies were not identified by databasesearching because (i) there was no indication of an associa-tion with a ‘health’ discipline in indexing and/or in theabstract; (ii) there was no indication that students in a
health discipline were the population under study in index-ing and/or the abstract; and/or (iii) the search would havebeen much to broad to search ‘students’ or ‘undergradu-ates’ without a ‘health’ qualifier.The updated search in September 2015 did not identify
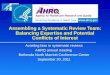
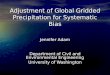
any new studies. Figure 1 represents the PRISMA flow dia-gram. The original detailed MEDLINE search strategy canbe found in Appendix S1.
Data extraction and quality assessment
Two reviewers (A.S.A. and B.P.) independently reviewed(Table 1) and evaluated the 17 extracted studies for meth-odological quality and descriptive purposes using the Qual-ity Assessment Scale (68) (Table 2). Any uncertainties wereresolved through discussion. Higher scores on the scale(range: 0–1) represented higher quality study ratings. The
Figure 1 PRISMA diagram showing selectionof articles.
© 2016 World Obesity. clinical obesity 6, 175–188
clinical obesity Weight bias reduction in health professionals A. S. Alberga et al. 177

Tab
le1
Cha
racteristic
sof
stud
iesthat
met
theinclus
ioncrite
ria
No.
Autho
rsSa
mple
size
Hea
lthprofes
sion
Stud
yde
sign
/interven
tion
Guiding
theo
ryWeigh
tbiasmea
suremen
ttool(s)
Durationof
follow-up
Summaryof
find
ings
1Ciaoan
dLa
tner
2011
(63)
64Und
ergrad
uate
psyc
hology
stud
ents
Ran
domized
controlledtrial,
3grou
ps:
1.Cog
nitivedisson
ance
2.So
cial
cons
ensu
s3.
Con
trol
Social
cons
ensu
stheo
ryan
dco
gnitive
disson
ance
theo
ry
Explicitattitud
es:A
FAT
Others:
Marlowe-Crowne
Social
Des
irabilitySc
ale,
Portrait
Values
Que
stionn
aire,p
ost-
feed
back
ques
tions
1wee
kAtp
ost-interve
ntion,
AFA
Tmea
nsin
cogn
itive
disson
ance
grou
pwerelower
than
control(1.80
vs.2
.01).N
oAFA
Tdiffe
renc
esfoun
dbe
twee
nso
cial
cons
ensu
san
dco
ntrol.Cog
nitive
disson
ance
interven
tions
canch
ange
attitud
esab
outa
ppea
ranc
ean
dattra
ctiven
essof
individu
alswith
obes
ity2
Crand
all
1994
(65)
42Und
ergrad
uatesin
aps
ycho
logy
clas
sAssignm
entto1of
2grou
ps:
1.‘Persu
ade’
cond
ition
.Pa
rticipa
ntswereread
ape
rsua
sive
mes
sage
andgive
nafact
shee
tabo
utthe
unco
ntrollabilityof
weigh
t2.
Con
trolc
onditio
n.Pa
rticipa
nts
wereread
ames
sage
andgive
nafact
shee
tabo
uttherole
ofps
ycho
logica
lstre
sson
illne
ss(unrelated
toweigh
t)
Attribution
theo
ryEx
plicitattitud
es:A
FA,F
earo
fFa
tSca
leOthers:
factua
lque
stions
conc
erning
weigh
t
Immed
iately
after
Participa
ntsin
thepe
rsua
deco
ndition
scored
lower
inwillpo
wer
(4.65vs.5
.57)
anddislike(1.75vs.2
.52)
than
control
cond
ition
,res
pectively.
Nodiffe
renc
eson
theFe
arof
FatS
cale
inpe
rsua
devs.c
ontro
l(6.19
vs.6
.50).P
ersu
ading
stud
ents
ontheun
controllabilityof
weigh
tmay
redu
ceas
sumptions
abou
twillpo
wer
anddisliketo
decrea
sean
ti-fata
ttitude
s
3Cotug
naet
al.
2010
(50)
40Dietetic
andhe
alth
prom
otion/he
alth
beha
viou
rscien
cemajor
stud
ents
enrolledin
anu
tritio
ncu
rriculum
elec
tive
Participa
ntsco
mpleted
theFa
tPh
obia
Scalebe
fore
andaftera
1-wee
kca
lorie
-res
tricted
diet
(120
0ca
lorie
sforw
omen
,150
0ca
lorie
sform
en)
Simulation
theo
ryof
empa
thy
Explicitattitud
es:F
PSOther
:jou
rnal
reflec
tions
1wee
kFa
tpho
biasc
ores
decrea
sedaftera
1-wee
kca
lorie
-res
tricted
diet.M
anyjourna
len
tries
reflec
tedane
wfoun
dresp
ectfor
individu
alsstrugg
lingto
lose
weigh
tand
chan
gein
priorn
egativeattitud
es.
Stud
ents
repo
rtedthat
thisex
perie
nce
wou
ldim
pact
theirfuturede
alings
with
overweigh
t/obe
seclients.
Participa
ntsfelt
that
thisdiet
prov
ided
real
expe
rienc
ean
dhe
lped
them
relate
morean
dbe
moreem
pathetic
toindividu
alstry
ingto
lose
weigh
t4
Diedrichs
etal.
2011
(51)
Initial
n=14
0,fina
ln=85
Und
ergrad
uate
stud
ents
enrolledin
threeps
ycho
logy
course
s
Pre-po
stex
perim
entald
esign,
assign
edto
3grou
ps.
1.Interven
tion=sp
ecially
deve
lope
dlecture
2.Com
paris
on=us
ualc
ourse
lecture
3.Con
trol=
nolecture
Attribution
theo
ryEx
plicitattitud
es:A
FAT(W
eigh
tCon
trol/B
lame,
Una
ttrac
tiven
es,S
ocial
disp
arag
emen
tsub
scales
)
Pre-test
(Tim
e1),
immed
iately
after(Time
2po
st-
interven
tion)
&3wee
ksfollow-up
(Tim
e3)
AtT
ime2Interven
tiongrou
pwereless
likely
tobe
lieve
that
weigh
tisco
ntrollablean
dless
likelyto
hold
anti-fata
ttitude
san
drate
overweigh
tand
obes
epe
ople
asun
attra
ctiveco
mpa
redto
pre-test
atTime
1.Th
eseim
prov
emen
tsweremaintaine
d3wee
kspo
st-in
terven
tionalbe
itwith
noch
ange
sin
social
disp
arag
emen
t.No
chan
gein
theco
mpa
rison
andco
ntrol
grou
psfora
nti-fat
attitud
esor
controllabilityof
weigh
tacros
s3tim
epo
ints
© 2016 World Obesity. clinical obesity 6, 175–188
178 Weight bias reduction in health professionals A. S. Alberga et al. clinical obesity

Tab
le1
Con
tinue
d
No.
Autho
rsSa
mple
size
Hea
lthprofes
sion
Stud
yde
sign
/interven
tion
Guiding
theo
ryWeigh
tbiasmea
suremen
ttool(s)
Durationof
follow-up
Summaryof
find
ings
5Fa
lker
etal.
2011
(52)
30Hea
lthca
reprofes
sion
als
(nurse
s,pa
tient
care
tech
nician
san
dun
itse
cretaries)
Com
pleted
apo
st-surve
yon
attitud
estowards
baria
tric
patie
nts1-mon
thafter
completionof
the44
-pag
ewrittenform
atof
theBariatric
Sens
itivity
Self-Le
arning
Educ
ationa
lMod
ule
Simulation
theo
ryof
empa
thy
Others:
‘The
Careof
theBariatric
Patie
ntNursing
Survey
’
(mea
surin
gstaff’s
know
ledg
ean
dse
nsitivity
towardob
ese
patie
nts)
1mon
thPo
st-surve
yresu
ltsreve
aled
20%
increa
sed
awaren
essthat
theira
ttitude
sca
nim
pact
theca
reprov
ided
toba
riatricpa
tients.
Aba
riatricse
nsitivity
educ
ationa
lmod
ule
decrea
sesstigmatizationof
healthca
reprofes
sion
als
6Gujrale
tal.
2011
(53)
266
Nurse
s2grou
ps:
1.Interven
tionba
riatricse
nsitivity
training(H
ospital1
)2.
Con
trol(Hos
pital2
)
Non
esp
ecified
orallude
dto
Explicitattitud
es:A
TOP,
BAOP
Interven
tiongrou
pATO
Pweremod
estly
grea
tertha
nthos
eforc
ontro
l(18
.0vs.1
6.1,
P=.03).N
odiffe
renc
esbe
twee
nBAOPsc
ores
forinterve
ntion
vs.c
ontro
l(67
.1vs.6
7.1,
P=.86).A
nnua
lba
riatricse
nsitivity
trainingmight
improv
enu
rsingattitud
estowardob
esepa
tients,
butitd
oesno
timprov
enu
rsingbe
liefs,
rega
rdless
oftheresp
onde
nt’sBMI
7Harris
1991
(64)
244
Und
ergrad
uate
psyc
hology
stud
ents
Ran
domlyas
sign
edto
cond
ition
s.Pa
rticipa
ntsread
andratedon
eof
6interviewsof
a2(exp
ert
interviewor
none
)×3(high
status
,empa
thyor
nomod
el)
factoriald
esign.
Participa
nts
wereprov
ided
(i)factua
linform
ationor
nota
nd(ii)e
xpos
ureto
either
nomod
els,
high
-statusmod
elswith
obes
ityor
mod
elswho
were
similartothepa
rticipa
nts
Attribution
theo
ry12
-item
obes
itykn
owledg
esc
ale,
feelings
abou
tmen
and
wom
enwho
aresu
bstantially
overweigh
t
Immed
iately
after
Participa
ntswho
read
theex
pertinterview
scored
high
eron
thekn
owledg
etest
scores
than
thos
ewho
hadno
t(19
.04
vs.1
6.74
,P<0.00
1).T
here
wereno
effectson
attitud
estowards
men
and
wom
enwho
areov
erweigh
t.While
know
ledg
eab
outo
besity
increa
sed,
there
wereno
chan
gesin
attitud
es
8Kus
hner
etal.
2014
(54)
127
Firsty
earm
edical
stud
ents
Pre-po
stex
perim
entald
esign.
Participa
ntsread
2artic
leson
commun
icationissu
esab
out
weigh
tand
obes
itystigmathen
hadan
8-min
enco
unterw
itha
stan
dardized
patie
ntfollowed
byde
briefing
andfacilitated
reflec
tionan
ddisc
ussion
with
theSP
,other
stud
ents
andthe
facu
ltyprec
eptor.Pa
rticipa
nts
completed
thesu
rvey
onewee
kbe
fore,immed
iately
aftera
nd1-
year
followingtheen
coun
ter
Con
tact
theo
rySe
lected
itemsfro
mex
istin
gqu
estio
nnaireswereus
edto
crea
teane
w16
-item
5-po
int
likerts
cale
ques
tionn
aire
(6,62,66
,67).Q
uestionn
aire
asse
ssed
3sc
ales
:neg
ative
obes
itystereo
type
s,em
pathy
foro
bese
patie
ntsan
dstud
ents’co
nfide
nceon
their
ability
tointeract
with
obes
epa
tients
Immed
iately
afterthe
enco
unter
(pos
t-interven
tion)
and
1follow-up
Sign
ifica
ntim
prov
emen
tsin
stereo
type
s,em
pathyan
dco
nfide
ncepo
st-
interven
tion.
53%
ofstud
ents
indica
ted
less
obes
itystereo
typing
,48.4%
indica
tedmoreem
pathyforo
bese
patie
nts,
and86
.7%
show
edmore
confi
denc
ein
clinical
interactionwith
obes
epa
tientsat
post-in
terven
tion.
At
1ye
ar,h
owev
er,n
egativeob
esity
stereo
typing
regres
sedto
base
lineleve
ls.
Empa
thyan
dco
unse
lling
scores
were
maintaine
dat
1-ye
arfollow-up
© 2016 World Obesity. clinical obesity 6, 175–188
clinical obesity Weight bias reduction in health professionals A. S. Alberga et al. 179

Tab
le1
Con
tinue
d
No.
Autho
rsSa
mple
size
Hea
lthprofes
sion
Stud
yde
sign
/interven
tion
Guiding
theo
ryWeigh
tbiasmea
suremen
ttool(s)
Durationof
follow-up
Summaryof
find
ings
9O’Brie
net
al.
2010
(55)
159
Hea
lthstud
ents
(Hea
lthprom
otion/
public
health
bach
elor
degree
prog
ram)
Ran
domized
controlledtrial,
3grou
ps.
1.Obe
sity
curriculum
onco
ntrollablereas
onsforo
besity
(31-hclas
ses)
2.Prejud
ice-redu
ctionco
ndition
:ob
esity
curriculum
onthe
unco
ntrollablereas
onsfor
obes
ity(3
1-hclas
ses)
3.Con
trolc
urric
ulum
focu
sedon
alco
holu
sein
youn
gpe
ople
(41-hclas
ses)
Elab
oration
Like
lihoo
dMod
el
Explicitattitud
es:A
FAIm
plicitattitud
es:IAT
Beliefs
abou
tobe
sity
&ca
uses
:BAOP,
TheDietin
gBeliefs
Scale
4wee
ksTh
ege
nes/en
vironm
entc
onditio
nsh
owed
a27
%de
crea
sein
theim
plicitgo
od/bad
andade
crea
seof
12%
inthemotivated
/lazy
implicitan
ti-fatp
rejudice
relativeto
othe
rcon
ditio
ns.T
hediet/exe
rcise
cond
ition
show
eda27
%increa
sein
one
mea
sure
ofim
plicitan
ti-fatp
rejudice
(motivated
/lazy).Th
erewereno
sign
ifica
ntgrou
pdiffe
renc
esin
explicit
anti-fatp
rejudice
betwee
nco
ndition
s,ho
wev
er,red
uctio
nsin
Dislikesc
ores
werese
enin
thege
nes/en
vironm
ent
cond
ition
.Nosign
ifica
ntch
ange
sin
beliefs
abou
tobe
sepe
ople
ordieting
controlb
eliefs
werefoun
dac
ross
cond
ition
s.Anti-fat
prejud
iceca
nbe
redu
cedor
exac
erba
tedde
pend
ingon
theca
usal
inform
ationprov
ided
abou
tob
esity
10Pe
rsky
etal.
2011
(56)
110
Third
andfourth
year
med
ical
stud
ents
Con
trolledrand
omized
expe
rimen
tal,2grou
ps:
1.Rea
dab
outg
enetic
orbe
haviou
ralm
echa
nism
sof
obes
ity2.
Rea
dab
outa
controltop
ic.
Stud
ents
then
interacted
with
anob
esevirtu
alpa
tient
inavirtu
alclinic
andco
mpleted
aba
ttery
ofmea
sures
Attribution
theo
ryEx
plicitattitud
es:n
egative
stereo
typing
(OPT
S)Others:
beliefinartic
leprem
ise,
caus
albe
liefs,p
erce
ptions
ofpa
tient’sresp
onsibility,
health
beha
viou
rrec
ommen
datio
ns,
patie
nt’san
ticipated
adhe
renc
e
Immed
iately
after(po
st-
interven
tion)
Rates
ofmos
thea
lthbe
haviou
rscree
ning
reco
mmen
datio
ns(w
eigh
tlos
s,ex
ercise
,an
ddiet
cons
ultatio
ns)werelower
amon
gpa
rticipa
ntsex
pose
dto
gene
ticca
usal
inform
ationthan
control.Th
ege
netic
caus
alinform
ationgrou
pex
hibitedless
nega
tivestereo
typing
ofthepa
tient
than
control,F(1,10
5)=5.00
,P=0.02
8,bu
tdidno
tdiffer
inan
ticipated
patie
ntad
herenc
e,F(1,10
5)=3.18
,P=0.07
711
Poutsc
hiet
al.
2013
(57)
64Con
venien
cesa
mple
ofse
cond
-yea
rmed
ical
stud
ents
attend
inganu
tritio
nco
urse
andthird
-ye
armed
ical
stud
ents
inafamily
med
icineclerkship
Pre-po
stex
perim
entald
esign.
1-h
interven
tionco
nsistedof
watch
inga17
-min
vide
oab
out
weigh
tbias:
Weigh
tBiasin
Hea
lthca
re,a
swella
spo
stvide
odisc
ussion
Attribution
theo
ryEx
plicitattitud
es:B
AOP,
ATO
P,FP
SIm
med
iately
after(po
st-
interven
tion)
Interven
tionincrea
sedthebe
lieftha
tgen
etic
anden
vironm
entalfac
tors
play
anim
porta
ntrole
intheca
useof
obes
ity(BAOPincrea
sedfro
m16
.53to
19.27)
andde
crea
sedne
gativestereo
type
sab
outo
bese
patie
nts(FPS
decrea
sed
from
3.65
to3.45
)
12Pu
hlet
al.
2005
(62)
Stud
y1,
N=60
Stud
y2,
N=55
Stud
y3,
N=20
0
Und
ergrad
uate
stud
ents
enrolledin
anintro
ductory
psyc
hology
course
Participa
ntsco
mpleted
self-repo
rtmea
suresof
attitud
estowards
peop
lewith
obes
itypriortoan
dafterm
anipulated
cons
ensu
sfeed
back
depictingattitud
esof
othe
rs
Perceive
dso
cial
cons
ensu
smod
el
Explicitattitud
es:O
PTS,
BAOP
Others:
Marlowe-Crowne
Social
Des
irabilitySc
ale,
Just
World
Scale
1wee
kFa
vourab
leco
nsen
susfeed
back
from
anin-
grou
pha
smoreinflue
nceon
repo
rted
attitud
esthan
whe
nitco
mes
from
anou
t-grou
p.Fa
vourab
leco
nsen
susfeed
back
increa
sedbe
liefs
that
caus
esof
obes
ityareno
tund
erpe
rson
alco
ntrola
nd
© 2016 World Obesity. clinical obesity 6, 175–188
180 Weight bias reduction in health professionals A. S. Alberga et al. clinical obesity

Tab
le1
Con
tinue
d
No.
Autho
rsSa
mple
size
Hea
lthprofes
sion
Stud
yde
sign
/interven
tion
Guiding
theo
ryWeigh
tbiasmea
suremen
ttool(s)
Durationof
follow-up
Summaryof
find
ings
Stud
y1:
Participa
ntsrece
ived
inform
ationab
outo
thers’
stereo
type
dbe
liefs
Stud
y2:
Participa
ntsweregive
nfavo
urab
leco
nsen
susfeed
back
from
anin-group
vs.a
nou
t-grou
pStud
y3:
Participa
ntswere
expo
sedto
oneof
5co
ndition
sto
compa
reco
nsen
sus
inform
ation
show
edmorepo
sitivean
dless
nega
tive
traits
abou
tpeo
plewith
obes
ity.R
eading
abou
tthe
unco
ntrollableca
uses
ofob
esity
decrea
sedbe
liefs
that
obes
ityis
caus
edby
controllablefactors,
redu
ced
nega
tivetra
itsbu
tdid
notimprov
epo
sitivetra
its
13Rob
erts
etal.
2011
(58)
14stud
ents
participa
ted
inthe
elec
tive
principa
lclinical
expe
rienc
eprog
ram
(PCE):
4stud
ents
enrolledin
baria
tric
surgery
long
itudina
lpa
tient
pilot
prog
ram,
9co
ntrols
Third
year
med
ical
stud
ents
Pre-po
stex
perim
entald
esign.
Clinical
clerkstud
ents
paire
dwith
avo
luntee
rpatient
sche
duledto
unde
rgoba
riatricsu
rgeryfor
1ye
ar.L
ongitudina
lbariatric
surgerypa
tient
elec
tive
includ
es:c
urric
ulum
,interdisciplinarypa
tient
visits,
clinical
skillbu
ilding,
long
itudina
lfac
ulty
men
torship
andse
lf-reflec
tion.
Stud
enta
ttitude
sbe
fore
third
year
clerkshipan
dag
ainat
theen
dof
theye
arus
ingbo
thqu
alita
tive&qu
antitative
metho
ds
Non
esp
ecified
orallude
dto
Others:
Attitude
Asses
smen
tSu
rvey
(asu
rvey
ofattitud
esan
dkn
owledg
eof
obes
ity&
baria
tricsu
rgery),refl
ectio
nes
saythem
atic
analysis
1ye
arTh
epilotp
rogram
memay
have
helped
maintainpo
sitiveattitud
estowards
obes
ity.R
eflec
tiones
saythem
atic
analysisreve
aled
that
extend
edlong
itudina
lrelations
hips
(multip
levisits
andwith
multip
lesp
ecialists)w
ithan
individu
alpa
tient
nega
tedprev
ious
lyhe
ldstereo
type
sab
outo
besity
14Ruk
avina
etal.
2008
(59)
69Kines
iology
pre-
profes
sion
alsfro
m4diffe
rent
unde
rgradu
ate
conc
entra
tions
(38clinical
exercise
physiology
,10
fitnes
sman
agem
ent,
13ph
ysical
educ
ationstud
ent
teac
hers
and8sp
ort
commun
ication
majors).T
here
was
Pre-po
stex
perim
entald
esign.
Interven
tioninclud
edbo
tha
clas
sroo
mco
mpo
nent
and
completionof
ase
rvice-learning
projec
t;then
,the
yad
ministered
theFITN
ESSG
RAM
to3–
5clas
sesof
fourth
andfifth
grad
ech
ildren
Attribution
theo
ry,
Expe
riential
learning
theo
ry
Explicitattitud
es:A
FAT,
ERTs
6wee
ksAFA
Tsc
ores
onweigh
tcon
trollability
decrea
sedfollowingtheinterven
tionbu
ttherewereno
diffe
renc
eson
theothe
r2AFA
Tsc
ales
.Interve
ntiondidno
tch
ange
stud
ents’en
dorsem
enttha
tfat
peop
lewerelazy.R
eflec
tivepa
pers
reve
aled
five
them
es:h
ealth
ylifes
tyle
asan
individu
alch
oice
,barrie
rsto
physical
activity,m
ulti-factorialn
atureof
obes
ityan
dprom
otionof
physical
activity
throug
hinform
ationan
den
courag
emen
t
© 2016 World Obesity. clinical obesity 6, 175–188
clinical obesity Weight bias reduction in health professionals A. S. Alberga et al. 181

Tab
le1
Con
tinue
d
No.
Autho
rsSa
mple
size
Hea
lthprofes
sion
Stud
yde
sign
/interven
tion
Guiding
theo
ryWeigh
tbiasmea
suremen
ttool(s)
Durationof
follow-up
Summaryof
find
ings
noco
ntrolg
roup
inthisstud
y15
Ruk
avina
etal.
2010
(60)
Totaln
=78
,ex
perim
ental
n=42
,co
ntrol,
n=36
Kines
iology
pre-
profes
sion
als69
pts
from
4diffe
rent
unde
rgradu
ate
conc
entra
tions
(38clinical
exercise
physiology
,10
fitnes
sman
agem
ent,
13ph
ysical
educ
ationstud
ent
teac
hers
and8sp
ort
commun
ication
majors).T
here
was
noco
ntrolg
roup
inthisstud
y
Pre-po
stex
perim
entald
esign.
Multi-co
mpo
nent
interven
tion
(service
-learning
base
dinterven
tionwhich
includ
eda
clas
sroo
msco
mpo
nent)
cons
istin
gof
attribu
tiontheo
ry(red
ucingpe
rcep
tions
ofco
ntrollabilityto
redu
ceblam
e),
cons
ciou
snes
sraising,
and
evok
ingem
pathythroug
hpe
rspe
ctivetaking
,roleplay
ing
andex
posu
reto
overweigh
tindividu
als.
Ptsco
nduc
teda
FITN
ESS-GRAM
with
scho
olag
edch
ildren(8–10
years)
asthese
rvicelearning
compo
nent.
Similartoea
rlier
2008
stud
ybu
tinclud
edamea
sure
ofim
plicitbias
Attribution
theo
ryEx
plicitattitud
es:A
FAT,
ERTs
Implicitattitud
es:IAT
1mon
thPa
rticipa
tionin
theinterven
tionredu
ced
explicitbias
ontheAFA
Tso
cial
charac
ter
disp
arag
emen
tand
weigh
tcon
trol/b
lame
subs
cales,
butthe
rewereno
sign
ifica
ntch
ange
sin
implicitbias
16Sw
iftet
al.
2013
(61)
n=43
atba
seline,
n=2-
at6wee
kf/u
19dietetic
stud
ents
and24
thrid
-yea
rmed
ical
scienc
estud
ents
PilotR
CT,
2grou
ps.
1.Interven
tion,
n=22
.Pa
rticipa
ntswatch
edtwoan
ti-stigma17
-min
film
s2.
Con
trol,n=21
.A34
-min
extra
ctfro
mahistorical
docu
men
tary
serie
sun
relatedto
food
andweigh
t
Attribution
theo
ryEx
plicitattitud
es:F
PS,
BAOP,
AFA
.Im
plicitattitud
es:b
ad/goo
dIAT
andlazy/m
otivated
IAT
6wee
ksTh
einterven
tionsign
ifica
ntlyim
prov
edex
plicitattitud
esan
dbe
liefs
towardob
ese
peop
le.Interve
ntionde
crea
sedF-Sc
ale
from
base
lineto
post-in
terven
tion(3.7
to3.2,
P<0.00
1)vs.n
och
ange
sin
the
controlg
roup
(4.0
to4.0)
Atp
ost-interve
ntion,
BOAPincrea
sedfro
m11
.2to
19.9
at6-wee
kfollow-upin
the
interven
tiongrou
p(P
<0.00
1)vs.n
och
ange
sin
theco
ntrolg
roup
(11.4to
11.7).At6
-wee
kfollow-up,
AFA
Dislike
decrea
sedfro
m1.86
to1.57
(P<0.05
)in
theinterven
tiongrou
p,whe
reas
noch
ange
swereob
served
inco
ntrols(2.39
to2.54
).AFA
Willpo
wer
decrea
sedfro
mba
selineto
post-in
terven
tion(5.42to
3.88
,P<0.01
)vs.
noch
ange
inco
ntrols(5.78
to5.94
).Th
erewereno
chan
gesin
implicitweigh
tbias
© 2016 World Obesity. clinical obesity 6, 175–188
182 Weight bias reduction in health professionals A. S. Alberga et al. clinical obesity

studies assessed ranged from 0.45 to 1.00 (mean: 0.71). All17 studies were included in the narrative analysis regardlessof quality rating.
Interpretation
The results of this systematic review demonstrated a lackof robust interventions that address weight bias reductionamongst students and health professionals. Many includedstudies had methodological weaknesses, including short-term follow-up periods (<6 months); lack of randomizationand control groups; and inconsistency of outcome variablesthat limited comparability. Most studies were conducted inlaboratory settings, limiting their generalizability in naturalsettings, which tend to be more complex. It is essential toalso understand how the context in which interventionswere carried out impacted the results. Overall, there is/areno definitive approach(es) that has/have demonstratedeffectiveness to reduce weight bias among student traineesand health professionals.The studies we reviewed examined the effects of weight
bias reduction interventions, with student trainees pursuinga health-related degree and practicing health professionals.These included students in undergraduate programmes,including dietetics and health promotion (50), dietetics andmedicine (61), health promotion/public health (55), kinesi-ology (59,60), medicine (38,54,56–58), psychology(51,62–65) and health professionals such as nurses (53)and a combination of professionals in a healthcare setting(nurses, patient care technicians and unit secretaries) (52).A literature and environmental scan highlighted four pri-
mary approaches that have been incorporated into inter-ventions designed to reduce weight bias amongst healthprofessionals (69). The first approach emphasized intellec-tual understanding of weight, overweight, obesity andweight-related bias, stigma and discrimination by provid-ing basic information for health professionals. The secondapproach focused on empathy with the lived experience ofpeople who are classified as obese by targeting peoples’emotions. The third approach emphasizes self-awarenessthrough self-reflection and gaining an understanding ofones’ own attitudes and biases. Lastly, the influence ofrespected and trusted leaders or peers who can ‘sway’ peo-ple to think one way or another can be utilized. To date,there is insufficient evidence as to which approach is moresuccessful for reducing weight bias among healthprofessionals.The components and guiding theories of the interven-
tions varied drastically among studies. Some studies uti-lized a single component approach (e.g. being put on a 1-week calorie-restricted diet) (50), receiving a single lecture(51), attending multiple lectures within a course on theuncontrollable causes of obesity (55), completing a self-learning module (52), providing an article on theT
able
1Con
tinue
d
No.
Autho
rsSa
mple
size
Hea
lthprofes
sion
Stud
yde
sign
/interven
tion
Guiding
theo
ryWeigh
tbiasmea
suremen
ttool(s)
Durationof
follow-up
Summaryof
find
ings
17Wiese
etal.
1992
(38)
75Firsty
earm
edstud
ents
Con
trolledde
sign
,2grou
ps.
1.Interven
tion=32
Broad
-ban
dman
ipulation:
expo
sure
toavide
otap
edinterviewwith
apa
tient
expres
sing
difficu
lties
with
dieting,
2role-playex
ercise
san
daradiosp
ecialo
nca
uses
ofob
esity
2.Con
trol=
43
Elab
oration
likelihoo
dmod
el,
attribu
tion
theo
ry,
control
theo
ry
Explicitattitud
es:1
9-ite
mob
esity
attitud
esqu
estio
nnaire
deve
lope
dby
rese
arch
ers
5wee
ksan
d1ye
arAt5
-wee
kas
sessmen
t,interven
tiondiffe
red
controlg
roup
onsixof
eigh
tmea
suresof
attitud
estowardob
esepe
ople..One
year
afterc
ourse,
interven
tiongrou
pwas
sign
ifica
ntlymorelikelyto
rate
gene
ticfactorsas
impo
rtant
inob
esity
andless
likelyto
blam
eob
esepe
ople
forthe
irco
ndition
AFA
,anti-fat
attitud
esqu
estio
nnaire;A
FAT,
anti-fata
ttitude
stest;A
TOP,
attitud
estowardob
esepe
rson
s;BAOP,
beliefs
abou
tobe
sepe
rson
ssc
ale;
ERTs
,exp
licitratin
gstests;
FPS,
fatp
hobiasc
ale(also
know
nas
F-sc
ale);IAT,
implicitas
sociationtest;O
PTS,
obes
epe
rson
stra
itsu
rvey
.
© 2016 World Obesity. clinical obesity 6, 175–188
clinical obesity Weight bias reduction in health professionals A. S. Alberga et al. 183

uncontrollable causes of obesity (56), receiving feedbackabout their level of stigma (cognitive dissonance vs. socialconsensus) (63), training in bariatric sensitivity (53) andviewing videos about weight bias (57,61). Others utilizedmulti-component strategies, including education plus real-world experience in working with a patient with obesity(54,58–60) and education plus another form of self-reflection (38). Although there is insufficient evidence tosuggest one approach and/or a combination of approachesis better for weight bias reduction, results from a previousreview and environmental scan learning from other modelsof discrimination suggested that ‘any approach must bemulti-faceted and multi-level in order to address the manymechanisms that can lead to harm’ ((69), p. 5).Many of the interventions reviewed used attribution
theory to guide the weight bias reduction interventiondesign by providing information about the ‘controllability’ ofweight (62,64,65). In the case of weight bias, attributiontheory posits that the more people believe weight is a function
of personal control and willpower (i.e. ‘controllable’causes such as diet and exercise), the more negative theirattitude will be towards individuals living with obesity.Weight bias interventions based on attribution theory areassumed to work by primarily using education aimed atchanging beliefs and understanding about the controllabil-ity of the stigmatized characteristic (i.e. weight). The abilityto control weight (i.e. believing that people are responsiblefor their weight) is an important contributor to anti-fat atti-tudes (70). Of the studies reviewed, some interventionschanged attitudes about the controllability of weight(38,55,62,65) by presenting facts about the uncontrollable/non-modifiable causes of obesity (i.e. genetics, biology,environment and sociocultural influences). However,interventions designed to change attitudes and beliefsabout people with obesity (i.e. character, attractiveness andnegative stereotypes) have been less successful (64).Information-providing interventions yielded mixed results,with some studies showing improved attitudes (51,62,65)
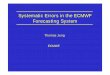
Table 2 Quality assessment of included studies
No. Reference Quality assessment checklist
Summarysc
ore
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Que
stion/ob
jectivesu
fficien
tlyde
scrib
ed
Stud
yde
sign
eviden
tan
dap
prop
riate
Metho
dof
subjec
t/com
paris
ongrou
pse
lectionor
source
ofinform
ation/
inpu
tva
riables
desc
ribed
andap
prop
riate?
Subjec
t(and
compa
rison
grou
p,ifap
plicab
le)ch
arac
teris
ticssu
fficien
tlyde
scrib
ed
Ifinterven
tiona
land
rand
omalloca
tion
was
possible,was
itrepo
rted?
Ifinterven
tionan
dblinding
ofinve
stigatorswas
possible,
was
itrepo
rted?
Ifinterven
tiona
land
blinding
ofsu
bjec
tswas
possible,was
itrepo
rted?
Outco
mean
d(ifap
plicab
le)ex
posu
remea
sure(s)welld
efined
androbu
stto
mea
suremen
t/misclas
sific
ationbias
?Mea
nsof
asse
ssmen
trepo
rted?
Samplesize
approp
riate?
Ana
lytic
metho
dsde
scrib
ed/justified
andap
prop
riate?
Somees
timateof
varia
nceis
repo
rted
forthemainresu
lts?
Con
trolledforco
nfou
nding?
Res
ults
repo
rtedin
sufficien
tdetail?
Con
clus
ions
supp
ortedby
theresu
lts?
1 Ciao and Latner 2011 (63) 2 2 2 2 2 2 2 2 2 2 2 2 2 2 1.002 Crandall 1994 (65) 2 2 1 1 1 2 1 1 1 1 0 0 0 1 0.503 Cotugna 2010 (50) 2 2 1 0 n/a n/a n/a 1 2 1 0 0 0 1 0.454 Diedrichs 2011 (51) 2 1 1 2 n/a n/a 0 2 1 2 2 0 2 2 0.715 Falker 2011 (52) 2 2 2 2 n/a n/a n/a 1 1 1 0 0 0 0 0.506 Gujral 2011 (53) 2 1 2 1 n/a n/a n/a 2 1 1 1 2 2 1 0.647 Harris 1991 (64) 1 1 1 1 2 0 1 1 2 1 0 0 1 1 0.468 Kushner 2014 (54) 2 2 2 2 n/a n/a n/a 2 2 2 0 0 1 1 0.739 O’Brien 2010 (55) 2 2 2 2 2 2 2 2 2 2 2 2 2 2 1.0010 Persky 2011 (56) 2 2 2 2 2 n/a 1 2 1 2 2 0 2 2 0.8511 Poustchi 2013 (57) 2 2 0 2 n/a n/a n/a 2 1 2 0 0 1 1 0.5912 Puhl et al. 2005 (62) 2 2 2 2 2 1 1 2 2 2 2 1 2 2 0.8913 Roberts 2011 (58) 2 2 2 2 2 2 2 2 2 2 2 2 2 2 0.6414 Rukavina 2008 (59) 2 2 1 2 0 n/a n/a 2 1 2 2 0 2 2 0.7515 Rukavina 2010 (60) 2 2 2 2 1 n/a n/a 2 1 2 2 0 2 2 0.8316 Swift 2013 (61) 2 2 2 2 2 1 2 2 1 2 1 0 2 2 0.8217 Wiese 1992 (38) 2 2 2 1 2 n/a n/a 2 2 2 0 0 2 2 0.79
The scoring rubric for quality assessment was 2 = yes, 1 = partial, 0 = no and n/a = not available. Summary scores were calculated by total sum/totalpossible sum. Total sum = (number of ‘yes’*2) + (number of ‘partials’*1); Total possible sum = 28 − (number of ‘n/a’*2). (68).
© 2016 World Obesity. clinical obesity 6, 175–188
184 Weight bias reduction in health professionals A. S. Alberga et al. clinical obesity

and others no change (56,64). Diedrichs and Barlow(2011) conducted an intervention study with undergradu-ate psychology students and found that participants whoreceived a lecture about the multiple determinants ofweight were less likely to hold negative attitudes towardspeople with overweight and obesity or to rate them asunattractive (51). Other studies have also suggested thatbrief educational interventions show some success in chal-lenging weight controllability beliefs and reducing weightbias in health students (51,62,65). Similarly, a study ofmedical students found that having students read materialshighlighting the genetic contributions to obesity led tosome reduction in weight bias (56); however, this interven-tion also resulted in greater avoidance of discussions withpatients about health behaviours such as diet and exercise.Wiese et al. (1992) evaluated an educational interventionconsisting of a videotaped interview with an individual dis-cussing her history of obesity and experiences with healthprofessionals, reading materials about genetic and environ-mental causes of obesity and role-play, taking on the per-spective of a person living with obesity. This weight biasreduction intervention increased empathy and changedmedical students’ stereotypes about people with obesity,but their willingness to blame people of size for their obe-sity remained unchanged.
O’Brien et al. (2010) used a randomized controlleddesign to evaluate changes in explicit and implicit anti-fatprejudice amongst health students after a series of compul-sory tutorial classes (55). One group received educationabout the uncontrollable causes of obesity; anotherreceived information about the controllable causes, whilethe control group received curriculum on alcohol use inyoung people. Decreases in implicit anti-fat prejudice werefound amongst the uncontrollable causes group, whileincreases in implicit anti-fat prejudice were found amongstthe controllable causes group. They concluded that ‘anti-fat prejudice can be reduced or exacerbated, depending onthe causal information provided about obesity’ (p. 1) andthat ‘health educators should ensure that information ongenetic, social and environmental causes of obesity, andtheir interactions, is delivered in a convincing manneralongside traditional information on causes and treatmentsof obesity, such as diet and exercise’ (p. 6). Phelan et al.(2015) (71) speculate that implicit bias influences subtlenon-verbal communication through changes in spontane-ous behaviour and improvements in patient satisfaction(72,73). It is plausible that more respectful patient-centredcare and improved patient experiences and outcomes mayensue as a result of decreasing implicit weight biases (71).
Despite yielding mixed results, other individual-orientedapproaches have been used in weight bias reduction inter-ventions among health professionals. Ciao and Latner(2011) successfully used a Cognitive Dissonance Theoryintervention (targeting value consistency and self-worth)
and demonstrated decreased negative attitudes about theappearance and attractiveness of people with obesity (63).Another study by Roberts et al. (2011) showed that ongo-ing contact with patients who had undergone bariatric sur-gery led to more positive attitudes (58). Other studiesevoking empathy and/or enhancing personal appreciationof the experience of heavier individuals have shown modesteffects (59,62).There is not enough evidence to suggest that attribution-
based approaches are sufficient to reduce weight bias, add-ing further support to the findings by Danielsdottir et al.(2010) that using one approach, such as manipulatingbeliefs/attributions about the causes and controllability ofobesity, is not sufficient to reduce the implicit attitudes thatcould be robust and durable among health professionals(74). Rukavina et al. (2008) (59) also suggested that inter-ventions will likely have to be multi-faceted and appliedrepeatedly to address both issues of changing controllabil-ity attributions (65) and having trainees reject negativestereotypes (59). The authors also proposed that if studentsare placed with patients who do not exhibit stereotypicalbehaviours, this could potentially help reduce their biases(59). Due to the diversity of the interventions’ theoreticalunderpinnings and approaches, comparison between inter-vention methods could not be assessed. There is a need toevaluate interventions that are based on theoretical frame-works other than attribution theory, and future studiesshould discern differences in effectiveness betweenapproaches to reduce weight bias.Our results show that there is no clear way to decipher
successful strategies to reduce weight bias because of thevariety of approaches used and the lack of high-qualityarticles published to date. Thus, while attributions areimportant, as is sharing information about the uncontrolla-bility of obesity, these approaches are, in and of them-selves, insufficient to change weight bias. It is likely thattrue change requires a change in social norms and theunderlying dominant ideologies about weight (75).Whether that should begin with individuals or broadersocial approaches, or both, is a question worth exploringfurther. Future research needs to assess and compare theeffects of single approaches (i.e. attribution theory basedon the controllability of weight) as well as multiple cumula-tive approaches (i.e. attribution theory, empathy evoking,encounters with standardized patients and peer modelling/shadowing) on weight bias reduction.There is some evidence to suggest that weight bias reduc-
tion interventions may not last over the long term. A studyby Kushner et al. (2014) examined changes in attitudes andbeliefs about obesity and their confidence in communica-tion skills in 127 first-year medical students after an educa-tional intervention, including an encounter with anoverweight standardized patient. Questionnaires wereadministered before, immediately after and one year after
© 2016 World Obesity. clinical obesity 6, 175–188
clinical obesity Weight bias reduction in health professionals A. S. Alberga et al. 185

the clinical encounter. The authors showed that the imme-diate decrease in stereotyping observed following a clinicalencounter with an overweight standardized patient was notsustained at 1-year follow-up (54). However, the authorsdid show that increases in mean empathy and confidence incounselling were maintained at 1-year follow-up. It wasspeculated that perhaps this encounter was not sufficient tooverride other clinical and personal experiences that shapehealth professionals’ attitudes and beliefs about individualsliving with obesity. This study highlights the need to sup-port additional educational experiences relating to obesityin the medical curriculum. There is a strong need to exam-ine the long-term effects of interventions (≥1-year duration)and to understand why stereotypes remain or revert tobaseline levels over time.
Strengths and limitations
To our knowledge, this was the first systematic review tosynthesize the evidence on weight bias reduction interven-tions uniquely in students or professionals in a health-related field. This research should inform the design andmethods of future randomized controlled trials and otherinvestigations to reduce weight bias in trainees or practi-cing health professionals. Due to the low number of studiesthat met our inclusion criteria, our limitations included thelarge variety of samples of health professionals (studenttrainees and practicing clinicians who represented a num-ber of different fields), diversity of intervention designs andapproaches and durations of follow-up assessments. Asthere was a lack of robust trials, transparency of methodsand presence of potential bias and heterogeneity in studydesigns, we could not determine the efficacy of the inter-ventions through a quantitative meta-analysis.
Conclusion and future directions
Our systematic review showed that there is no clearlydefined approach to reduce weight bias among studentsand professionals in a health discipline. The findings high-light the need to conduct randomized controlled trials todevelop evidence-informed, effective weight bias reductionpractices in healthcare settings. Health professionals mustbe aware of their own attitudes and behaviours towardspatients living with obesity and how negative stereotypescan impact patient care and engagement in the healthcaresystem. We argue that as students training to becomehealth professionals are still learning and forming attitudes,pre-professional education is a valued target for weightbias reduction, and health professional curriculum revi-sions are warranted. Phelan et al. (2015) (71) suggestedthat the medical school curricula about disparities and stig-matized populations should include discussion about
caring for patients with obesity. The authors also suggestincorporating positive experiences of medical studentswhen placed in contact with a patient living with obesity(known as contact theory). It has also been suggested thatsharing positive experiences and hearing from role modelswho treat patients with obesity with respect and dignitycould be influential for medical students in training.Addressing these factors could be important avenues toconsider when designing future weight bias reduction inter-ventions among health professionals.
Promoting positive attitudes, beliefs, skills and compe-tencies regarding obesity during student training mayincrease preparedness of future health professionals andoptimize the quality of care of individuals with obesityentering the healthcare system. However, there is a need tomove beyond awareness and information provision to raiseskills and competencies in health professionals regardingweight, obesity and weight bias. Furthermore, differenthealth professionals are grounded in different philosophicalmodels; interventions that work for one group might needto be modified to be effective for another. It would beimportant to investigate weight bias reduction in the con-text of the unique and diverse professional and healthcarecultures. Future research and evaluations should also assesschanges in behaviour and practices, which often stem fromresponses to changes in beliefs and attitudes. Long-termfollow-up is needed to evaluate whether changes in knowl-edge and attitudes will translate into changes in practicewhen treating patients with large bodies without stigma.As the education and training of health professionals areembedded in a society often fraught with weight bias, chan-ging the larger, systemic, social norms may be necessary tomake meaningful inroads into its reduction.
Conflict of Interest Statement
No conflict of interest was declared.
Acknowledgements
This work was funded by a Canadian Institutes of HealthResearch (CIHR) Partnerships for Health System Improve-ment (PHSI) Grant (201302MHS-302821) under PrincipalInvestigator Dr. Shelly Russell-Mayhew. Dr. AngelaS. Alberga currently holds a Banting CIHR PostdoctoralFellowship (BPF-139175) and was previously funded by anEyes High Postdoctoral Fellowship from the University ofCalgary. We gratefully acknowledge Gail MacKean andKathy GermAnn for their helpful guidance throughout thesystematic review process and for their insight and advicewhile reviewing and editing this manuscript.
© 2016 World Obesity. clinical obesity 6, 175–188
186 Weight bias reduction in health professionals A. S. Alberga et al. clinical obesity

References
1. Pollack A. A.M.A. recognizes obesity as a disease, 2015.[WWW document] URL http://wwwmedscapecom/viewarticle/806566 (accessed March 2016).2. Rich P. CMA recognizes obesity as a disease, 2015. [WWWdocument] URL https://wwwcmaca/En/Pages/cma-recognizes-obesity-as-a-diseaseaspx (accessed March 2016).3. Sumithran P, Proietto J. The defence of body weight: a physio-logical basis for weight regain after weight loss. Clin Sci (Lond)2013; 124: 231–241.4. Frood S, Johnston LM, Matteson CL, Finegood DT. Obesity,complexity, and the role of the health system. Curr Obes Rep2013; 2: 320–326.5. Andreyeva T, Puhl RM, Brownell KD. Changes in perceivedweight discrimination among Americans, 1995–1996 through2004–2006. Obesity (Silver Spring) 2008; 16: 1129–1134.6. Foster GD, Wadden TA, Makris AP et al. Primary care physi-cians’ attitudes about obesity and its treatment. Obes Res 2003;11: 1168–1177.7. Harvey EL, Hill AJ. Health professionals’ views of overweightpeople and smokers. Int J Obes Relat Metab Disord 2001; 25:1253–1261.8. Bocquier A, Verger P, Basdevant A et al. Overweight and obe-sity: knowledge, attitudes, and practices of general practitioners infrance. Obes Res 2005; 13: 787–795.9. Thuan JF, Avignon A. Obesity management: attitudes and prac-tices of French general practitioners in a region of France. Int JObes (Lond) 2005; 29: 1100–1106.10. Campbell K, Engel H, Timperio A, Cooper C, Crawford D.Obesity management: Australian general practitioners’ attitudesand practices. Obes Res 2000; 8: 459–466.11. Fogelman Y, Vinker S, Lachter J et al. Managing obesity: asurvey of attitudes and practices among Israeli primary care physi-cians. Int J Obes Relat Metab Disord 2002; 26: 1393–1397.12. Epstein L, Ogden J. A qualitative study of GPs’ views of treat-ing obesity. Br J Gen Pract 2005; 55: 750–754.13. Loomis GA, Connolly KP, Clinch CR, Djuric DA. Attitudesand practices of military family physicians regarding obesity. MilMed 2001; 166: 121–125.14. Hebl MR, Xu J. Weighing the care: physicians’ reactions tothe size of a patient. Int J Obes Relat Metab Disord 2001; 25:1246–1252.15. Ogden J, Bandara I, Cohen H et al. General practitioners’ andpatients’ models of obesity: whose problem is it? Patient EducCouns 2001; 44: 227–233.16. Block JP, DeSalvo KB, Fisher WP. Are physicians equipped toaddress the obesity epidemic? Knowledge and attitudes of internalmedicine residents. Prev Med 2003; 36: 669–675.17. Brandsma LL. Physician and patient attitudes toward obesity.Eat Disord 2005; 13: 201–211.18. Huizinga MM, Cooper LA, Bleich SN, Clark JM, Beach MC.Physician respect for patients with obesity. J Gen Intern Med2009; 24: 1236–1239.19. Wear D, Aultman JM, Varley JD, Zarconi J. Making fun ofpatients: medical students’ perceptions and use of derogatory andcynical humor in clinical settings. Acad Med 2006; 81: 454–462.20. Wigton RS, McGaghie WC. The effect of obesity on medicalstudents’ approach to patients with abdominal pain. J Gen InternMed 2001; 16: 262–265.21. Magliocca KR, Jabero MF, Alto DL, Magliocca JF. Knowl-edge, beliefs, and attitudes of dental and dental hygiene studentstoward obesity. J Dent Educ 2005; 69: 1332–1339.
22. Brown I, Stride C, Psarou A, Brewins L, Thompson J. Man-agement of obesity in primary care: nurses’ practices, beliefs andattitudes. J Adv Nurs 2007; 59: 329–341.23. Brown I, Thompson J. Primary care nurses’ attitudes, beliefsand own body size in relation to obesity management. J Adv Nurs2007; 60: 535–543.24. Zuzelo PR, Seminara P. Influence of registered nurses’ atti-tudes toward bariatric patients on educational programming effec-tiveness. J Contin Educ Nurs 2006; 37: 65–73.25. Berryman DE, Dubale GM, Manchester DS, Mittelstaedt R.Dietetics students possess negative attitudes toward obesity similarto nondietetics students. J Am Diet Assoc 2006; 106: 1678–1682.26. Harvey EL, Summerbell CD, Kirk SF, Hill AJ. Dietitians’views of overweight and obese people and reported managementpractices. J Hum Nutr Diet 2002; 15: 331–347.27. Campbell K, Crawford D. Management of obesity: attitudesand practices of Australian dietitians. Int J Obes Relat Metab Dis-ord 2000; 24: 701–710.28. Chambliss HO, Finley CE, Blair SN. Attitudes toward obeseindividuals among exercise science students. Med Sci Sports Exerc2004; 36: 468–474.29. Hare SW, Price JH, Flynn MG, King KA. Attitudes and per-ceptions of fitness professionals regarding obesity. J CommunityHealth 2000; 25: 5–21.30. Setchell J, Watson B, Jones L, Gard M, Briffa K. Physiothera-pists demonstrate weight stigma: a cross-sectional survey ofAustralian physiotherapists. J Physiother 2014; 60: 157–162.31. Robinson EL, Ball LE, Leveritt MD. Obesity bias amonghealth and non-health students attending an Australian universityand their perceived obesity education. J Nutr Educ Behav 2014;46: 390–395.32. Schwartz MB, Chambliss HO, Brownell KD, Blair SN,Billington C. Weight bias among health professionals specializingin obesity. Obes Res 2003; 11: 1033–1039.33. Teachman BA, Brownell KD. Implicit anti-fat bias amonghealth professionals: is anyone immune? Int J Obes Relat MetabDisord 2001; 25: 1525–1531.34. Puhl RM, Brownell KD. Confronting and coping with weightstigma: an investigation of overweight and obese adults. Obesity(Silver Spring) 2006; 14: 1802–1815.35. Washington RL. Childhood obesity: issues of weight bias.Prev Chronic Dis 2011; 8(5): A94.36. O’Brien KS, Latner JD, Ebneter D, Hunter JA. Obesity dis-crimination: the role of physical appearance, personal ideology,and anti-fat prejudice. Int J Obes (Lond) 2013; 37: 455–460.37. Phelan SM, Burgess DJ, Yeazel MW et al. Impact of weightbias and stigma on quality of care and outcomes for patients withobesity. Obes Rev 2015; 16: 319–326.38. Wiese HJ, Wilson JF, Jones RA, Neises M. Obesity stigmareduction in medical students. Int J Obes Relat Metab Disord1992; 16: 859–868.39. Persky S, Eccleston CP. Medical student bias and care recom-mendations for an obese versus non-obese virtual patient. Int JObes (Lond) 2011; 35: 728–735.40. Sabin JA, Marini M, Nosek BA. Implicit and explicit anti-fatbias among a large sample of medical doctors by BMI, race/ethnic-ity and gender. PLoS One 2012; 7: e48448.41. Puhl RM, Heuer CA. The stigma of obesity: a review andupdate. Obesity (Silver Spring) 2009; 17: 941–964.42. Beach MC, Roter DL, Wang NY, Duggan PS, Cooper LA. Arephysicians’ attitudes of respect accurately perceived by patientsand associated with more positive communication behaviors?Patient Educ Couns 2006; 62: 347–354.
© 2016 World Obesity. clinical obesity 6, 175–188
clinical obesity Weight bias reduction in health professionals A. S. Alberga et al. 187

43. Bertakis KD, Azari R. The impact of obesity on primary carevisits. Obes Res 2005; 13: 1615–1623.44. Schvey NA, Puhl RM, Brownell KD. The impact of weightstigma on caloric consumption. Obesity (Silver Spring) 2011; 19:1957–1962.45. Puhl RM, Luedicke J. Weight-based victimization among ado-lescents in the school setting: emotional reactions and coping beha-viors. J Youth Adolesc 2012; 41: 27–40.46. Vartanian LR, Novak SA. Internalized societal attitudes mod-erate the impact of weight stigma on avoidance of exercise. Obe-sity (Silver Spring) 2011; 40: 757–762.47. Drury CA, Louis M. Exploring the association between bodyweight, stigma of obesity, and health care avoidance. J Am AcadNurse Pract 2002; 14: 554–561.48. Higgins JPT, Green S. Cochrane Handbook for SystematicReviews of Interventions Version 5.1.0 (updated March 2011).The Cochrane Collaboration, 2011. Available from http://handbook.cochrane.org.49. Liberati A, Altman DG, Tetzlaff J et al. The PRISMA state-ment for reporting systematic reviews and meta-analyses of studiesthat evaluate health care interventions: explanation and elabora-tion. J Clin Epidemiol 2009; 62: e1–e34.50. Cotugna N, Mallick A. Following a calorie-restricted diet mayhelp in reducing healthcare students’ fat-phobia. J CommunityHealth 2010; 35: 321–324.51. Diedrichs PC, Barlow FK. How to lose weight bias fast! Evalu-ating a brief anti-weight bias intervention. Br J Health Psychol2011; 16: 846–861.52. Falker A, Sledge J. Utilizing a bariatric sensitivity educationalmodule to decrease bariatric stigmatization by healthcare profes-sionals. Bariatr Nurs Surg Patient Care 2011; 6: 73–78.53. Gujral H, Tea C, Sheridan M. Evaluation of nurse’s attitudestoward adult patients of size. Surg Obes Relat Dis 2011; 7:536–540.54. Kushner RF, Zeiss DM, Feinglass JM, Yelen M. An obesityeducational intervention for medical students addressing weightbias and communication skills using standardized patients. BMCMed Educ 2014; 14: 53.55. O’Brien KS, Puhl RM, Latner JD, Mir AS, Hunter JA. Redu-cing anti-fat prejudice in preservice health students: a randomizedtrial. Obesity (Silver Spring) 2010; 18: 2138–2144.56. Persky S, Eccleston CP. Impact of genetic causal informationon medical students’ clinical encounters with an obese virtualpatient: health promotion and social stigma. Ann Behav Med2011; 41: 363–372.57. Poustchi Y, Saks NS, Piasecki AK, Hahn KA, Ferrante JM.Brief intervention effective in reducing weight bias in medical stu-dents. Fam Med 2013; 45: 345–348.58. Roberts DH, Kane EM, Jones DB et al. Teaching medical stu-dents about obesity: a pilot program to address an unmet needthrough longitudinal relationships with bariatric surgery patients.Surg Innov 2011; 18: 176–183.59. Rukavina PB, Li W, Rowerll MB. A service learning basedintervention to change attitudes toward obese individuals inkinesiology pre-professionals. Soc Psychol Educ 2008; 11:95–112.
60. Rukavina PB, Li W, Shen B, Sun H. A service learning basedproject to change implicit and explicit bias toward obese indivi-duals in kinesiology pre-professionals. Obes Facts 2010; 3:117–126.61. Swift JA, Tischler V, Markham S et al. Are anti-stigma films auseful strategy for reducing weight bias among trainee healthcareprofessionals? Results of a pilot randomized control trial. ObesFacts 2013; 6: 91–102.62. Puhl RM, Schwartz MB, Brownell KD. Impact of perceivedconsensus on stereotypes about obese people: a new approach forreducing bias. Health Psychol 2005; 24: 517–525.63. Ciao AC, Latner JD. Reducing obesity stigma: the effective-ness of cognitive dissonance and social consensus interventions.Obesity (Silver Spring) 2011; 19: 1768–1774.64. Harris MB, Walters LC, Waschull S. Altering attitudes andknowledge about obesity. J Soc Psychol 1991; 131: 881–884.65. Crandall CS. Prejudice against fat people: ideology and self-interest. J Pers Soc Psychol 1994; 66: 882–894.66. Allison DB, Basile V, Yuker H. The measurement of attitudestoward and beliefs about obese persons. Int J Eat Disord 1991;10: 599–607.67. Bacon JG, Scheltema KE, Robinson BE. Fat phobia scale revis-ited: the short form. Int J Obes Relat Metab Disord 2001; 25:252–257.68. Kmet LM, Lee RC, Cook LS. Standard Quality AssessmentCriteria for Evaluating Primary Research Papers from a Variety ofFields. Alberta Heritage Foundation for Medical Research:Edmonton, 2004 HTA Initiative #13.69. MacKean G, GermAnn K. Reducing Weight Bias and Stigmain the BC Healthcare System, British Columbia: Provincial HealthServices Authority, 2013. Available from: http://cfe.keltyeatingdisorders.ca/sites/default/files/resource/Reducing%20Weight%20Bias%20%20Stigma_ExSum_May%202013_FINAL_0.pdf.70. DeJong W. The stigma of obesity: the consequences of naiveassumptions concerning the causes of physical deviance. J HealthSoc Behav 1980; 21: 75–87.71. Phelan SM, Puhl RM, Burke SE et al. The mixed impact ofmedical school on medical students’ implicit and explicit weightbias. Med Educ 2015; 49: 983–992.72. Dovidio JF. On the nature of prejudice: automatic and con-trolled processes. J Exp Soc Psychol 1997; 33: 510–540.73. Penner LA, Dovidio JF, West TV et al. Aversive racism andmedical interactions with black patients: a field study. J Exp SocPsychol 2010; 46: 436–440.74. Danielsdottir S, O’Brien KS, Ciao A. Anti-fat prejudice reduc-tion: a review of published studies. Obes Facts 2010; 3: 47–58.75. Link BG, Phelan JC. Conceptualizing stigma. Annu Rev Sociol2001; 27: 363–385.
Supporting Information
Additional Supporting Information may be found in theonline version of this article at the publisher’s web-site:
Appendix S1. Detailed MEDLINE search strategy
© 2016 World Obesity. clinical obesity 6, 175–188
188 Weight bias reduction in health professionals A. S. Alberga et al. clinical obesity