Embed Size (px)
Citation preview
Concussion Management Protocol
The following policy will be followed by all schools, leagues, tournaments and events contracted to provide athletic training services. This policy follows guidelines and procedures outlined in consensus statement from 3rd International Conference on Concussion in Sport held in Zurich 2008 and procedures for Impact Concussion testing.
A concussion is defined as a complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces. Several common features that incorporate clinical, pathologic and biomechanical injury constructs that may be utilized in defining the nature of a concussive head injury:
(1) Concussion may be caused by either a direct blow to the head, face, neck or elsewhere on the body with an “impulsive” force transmitted to the head.(2) Concussion typically results in a rapid onset of short-lived impairment of neurological function that resolves spontaneously.(3) Concussion may result in neuropathological changes, but the acute clinical symptoms largely reflect a functional disturbance rather than a structural injury.(4) Concussion results in a graded set of clinical symptoms that may or may not involve loss of consciousness. Resolution of the clinical and cognitive symptoms typically follows a sequential course; however, it is important to note that, in a small percentage of cases, post-concussive symptoms may be prolonged.(5) No abnormality on standard structural neuroimaging studies is seen in concussion.
Any athlete that shows any signs or symptoms of concussion will be removed from play and assessed by healthcare professional. According to the consensus statement of the 2008 Zurich Conference, the suspected diagnosis of a concussion can include one or more of the following clinical domains:
(1) Symptoms: somatic (e.g. headache), cognitive (e.g. feeling like in a fog) and/or emotional symptoms (e.g. lability)
(2) Physical Signs (e.g. loss of consciousness, amnesia)(3) Behavioral changes (e.g. irritability)(4) Cognitive impairment (e.g. slowed reaction times)(5) Sleep disturbance (e.g. drowsiness)
If any one or more of these components is present, a concussion should be suspected and the appropriate management strategy instituted.
Once first aid issues are addressed, an assessment of the concussive injury should be made using the Head Injury Report (Appendix A) or SCAT 2 (Appendix B). The post-injury results will be compared to the baseline SCAT 2, if available. Athletes with a suspected concussion will not be able to return to play that same day. These athletes should not be left alone and will be monitored after 15 and 30 minutes and every 30 minutes thereafter until the end of the event or until EMS are determined to be necessary. EMS should be activated for those athletes who suffer loss of consciousness, have a suspected neck injury or for those athletes whose symptoms worsen over a 15 or 30 minute time frame.
For those athletes not needing immediate referral parent/guardian must be contacted and head injury sheet given. (Appendix C). An athlete with a suspected concussion should not drive home. For those athletes that do not seek treatment at emergency room must be seen by a physician and present documentation to the school nurse.
Concussions will be managed symptomatically and through medical assessment. During the time that an athlete is symptomatic and recovering from injury, it is important to emphasize both physical and cognitive rest as outlined in Appendix C. Activities that require concentration and attention (e.g. scholastic work, video
games, text messaging, etc) may exacerbate symptoms and possibly delay recovery. If necessary, accommodations should be made for student-athletes whose symptoms worsen while in school or become so severe that an athlete is unable to complete studies.
Return to Play Protocol
Once an athlete is asymptomatic for 24 hours and has medical clearance from a physician the athlete may begin Phase 1. The athlete will be seen by the athletic trainer with communication of the Chief School Medical Officer and as authorized by the school policy, the following return to play protocol will be followed. As recommended by the New York State Public High School Athletic Association (NYSPHAA), this progression should be completed over 5-10 days and the athlete must have completed all five phases of the protocol in order to return to normal game play. The athlete must remain asymptomatic to progress to the next level. In the event that symptoms return, the athlete must stop activity. They may return to the previous phase of the protocol when asymptomatic for 24 hours. The athlete should be asymptomatic without the use of pharmacological agents/medications that may affect or modify their symptoms.
Phase 1 - Low impact, non-strenuous, light aerobic activity such as walking or riding a stationary bike at 60-65% of Maximum Heart Rate (MHR). If tolerated without return of symptoms over a 24 hour period proceed to;
Phase 2 - Higher impact, higher exertion, and moderate aerobic activity such as running or jumping rope. No resistance training. Elevate heart rate to 80-85% of MHR. If tolerated without return of symptoms over a 24 hour period proceed to;
Phase 3 - Sport specific non-contact activity. Low resistance weight training with a spotter. Elevate heart rate to 80-85% of MHR. If tolerated without return of symptoms over a 24 hour period proceed to;
Phase 4 - Sport specific activity, non-contact drills. Higher resistance weight training with a spotter. Elevate heart rate to 80-85% of MHR. If tolerated without return of symptoms over a 24 hour period proceed to;
Phase 5 - Full contact training drills and intense aerobic activity. If tolerated without return of symptoms over a 24 hour period proceed to;
Phase 6 - Return to full activities without restrictions.
**The final determination of when an athlete may return to full contact activity (Phase 5) rests with the School Chief Medical Officer.
The consensus panel agreed that a range of “modifying” factors may influence assessment and management of concussions restricting child longer. These factors are:
1. Symptoms – number, duration (> 10 days) and severity of symptoms2. Signs – prolonged LOC (> 1min), amnesia3. Concussive convulsions4. Temporal – frequency (repeated concussions over time), timing (injuries close together over time) and
“recency” of previous concussion5. Threshold – repeated concussions occurring with progressively less impact force or slower recovery
time6. Age – child and adolescent ( < 18 years old)7. Medication – psychoactive drugs, anticoagulants8. Behavior – dangerous style of play9. Sport – high-risk activity, contact and collision sport, high sporting level

10. Gender – no unanimous agreement that female gender be modifier although gender may be a risk factor for injury and/or influence injury severity
The ImPACT Program
The ImPACT Program is a baseline web-based assessment tool that will be implemented to assist in the Return to Play Protocol. This assessment tool can be used in conjunction or in place of the SCAT 2 assessment tool. Student-athletes will be baseline tested prior to the start of their sport season and then retested every two years. The concussion will be managed symptomatically and clinically with consideration of the ImPACT test. The return to play protocol will be initiated and followed as described above. An athlete will be tested on ImPACT once they are asymptomatic for 24 hours and have completed PHASE 4 of the return to play protocol. The ImPACT results will be given to the Chief School Medical Officer as part of their final medical clearance.
ImPact Protocol
Upon implementation of Impact all student-athletes will be baseline tested prior to the start of sport season and then retested every two years. Follow up testing will be completed if an injury occurs. Concussion will be managed symptomatically and utilizing Impact test. An athlete who suffers a concussion will be tested on Impact 24-72 hrs post-injury. Once scores return to where MD and ATC feel the athlete has recovered from concussion s/he may begin functional return to play.
The above policy will be followed by the healthcare professionals that deal with the decision to allow an athlete to return to play and will be followed despite the athlete presenting a prescription note to return to play sooner from their primary care physician or Emergency room. If an athlete presents a prescription from their primary care physician for the appropriate time frame in regards to return to play, then the functional return steps will be followed by the athletic trainer. However, the final determination of when an athlete may return to play rests with the School Chief Medical Officer.
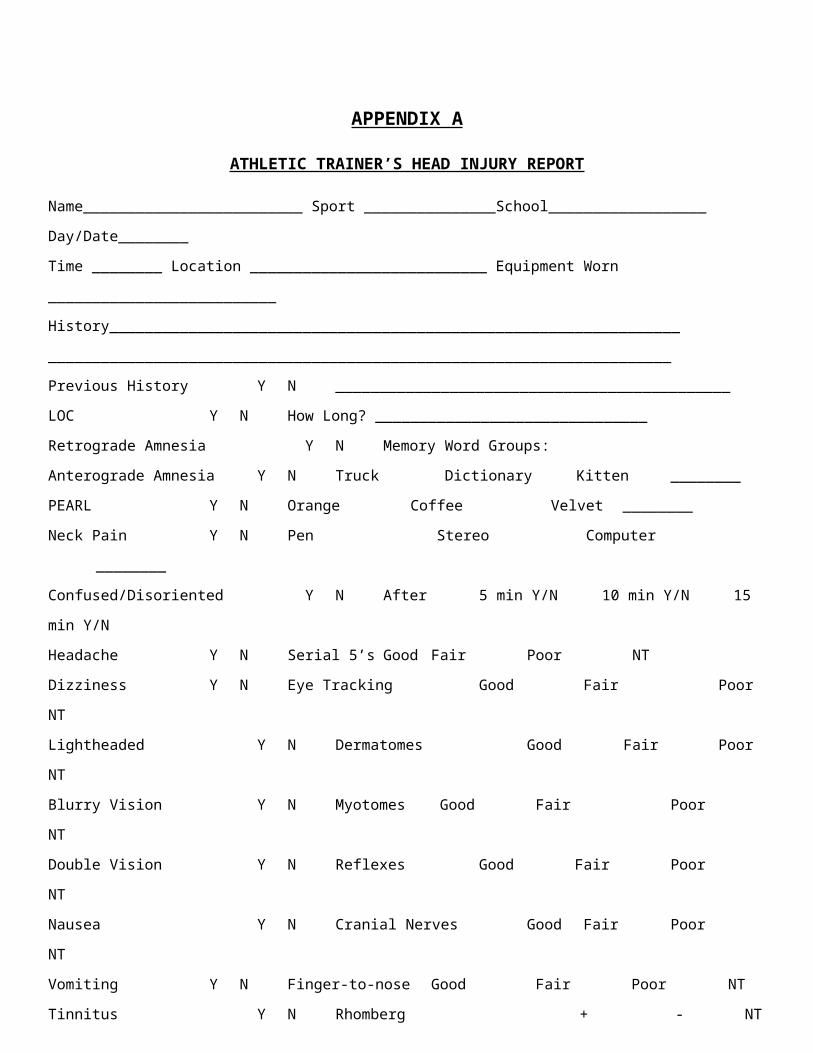
APPENDIX A
ATHLETIC TRAINER’S HEAD INJURY REPORT
Name_________________________ Sport _______________School__________________ Day/Date________
Time ________ Location ___________________________ Equipment Worn __________________________
History_________________________________________________________________
_______________________________________________________________________
Previous History Y N _____________________________________________
LOC Y N How Long? _______________________________
Retrograde Amnesia Y N Memory Word Groups:
Anterograde Amnesia Y N Truck Dictionary Kitten ________
PEARL Y N Orange Coffee Velvet ________
Neck Pain Y N Pen Stereo Computer ________
Confused/Disoriented Y N After 5 min Y/N 10 min Y/N 15 min Y/N
Headache Y N Serial 5’s Good Fair Poor NT
Dizziness Y N Eye Tracking Good Fair Poor NT
Lightheaded Y N Dermatomes Good Fair Poor NT
Blurry Vision Y N Myotomes Good Fair Poor NT
Double Vision Y N Reflexes Good Fair Poor NT
Nausea Y N Cranial Nerves Good Fair Poor NT
Vomiting Y N Finger-to-nose Good Fair Poor NT
Tinnitus Y N Rhomberg + - NT
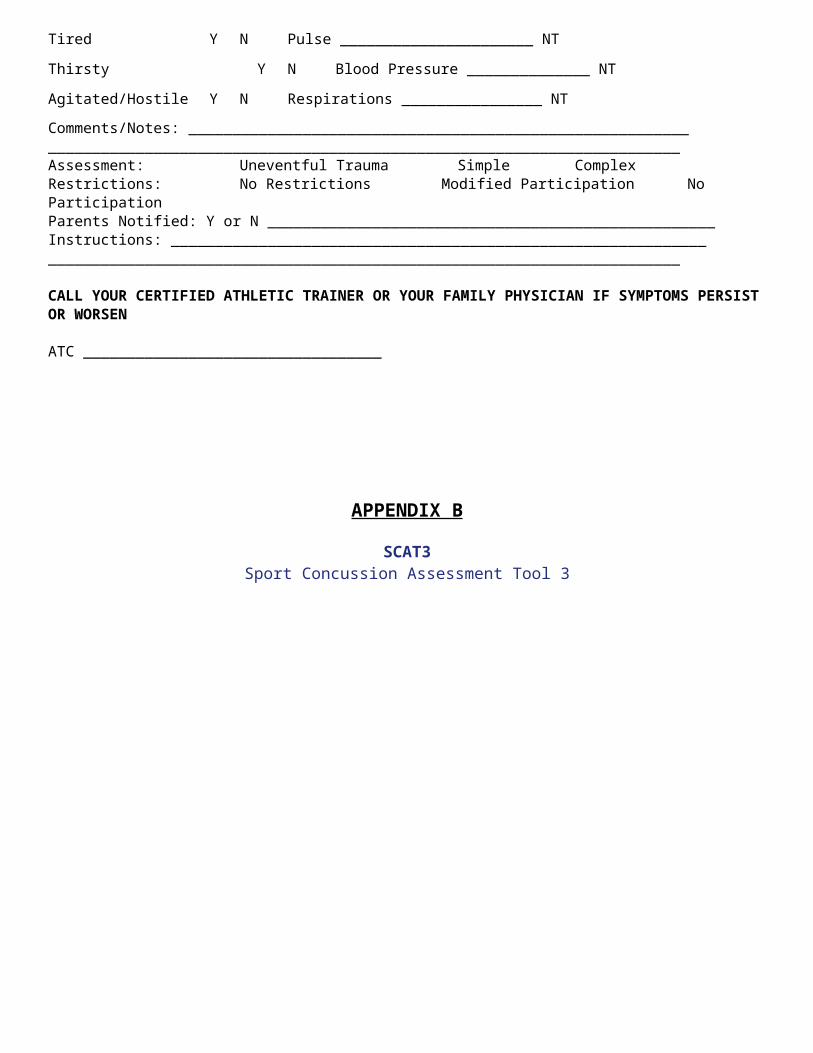
Tired Y N Pulse ______________________ NT
Thirsty Y N Blood Pressure ______________ NT
Agitated/Hostile Y N Respirations ________________ NT
Comments/Notes: _________________________________________________________ ________________________________________________________________________ Assessment: Uneventful Trauma Simple ComplexRestrictions: No Restrictions Modified Participation No ParticipationParents Notified: Y or N ___________________________________________________ Instructions: _____________________________________________________________________________________________________________________________________
CALL YOUR CERTIFIED ATHLETIC TRAINER OR YOUR FAMILY PHYSICIAN IF SYMPTOMS PERSIST OR WORSEN
ATC __________________________________
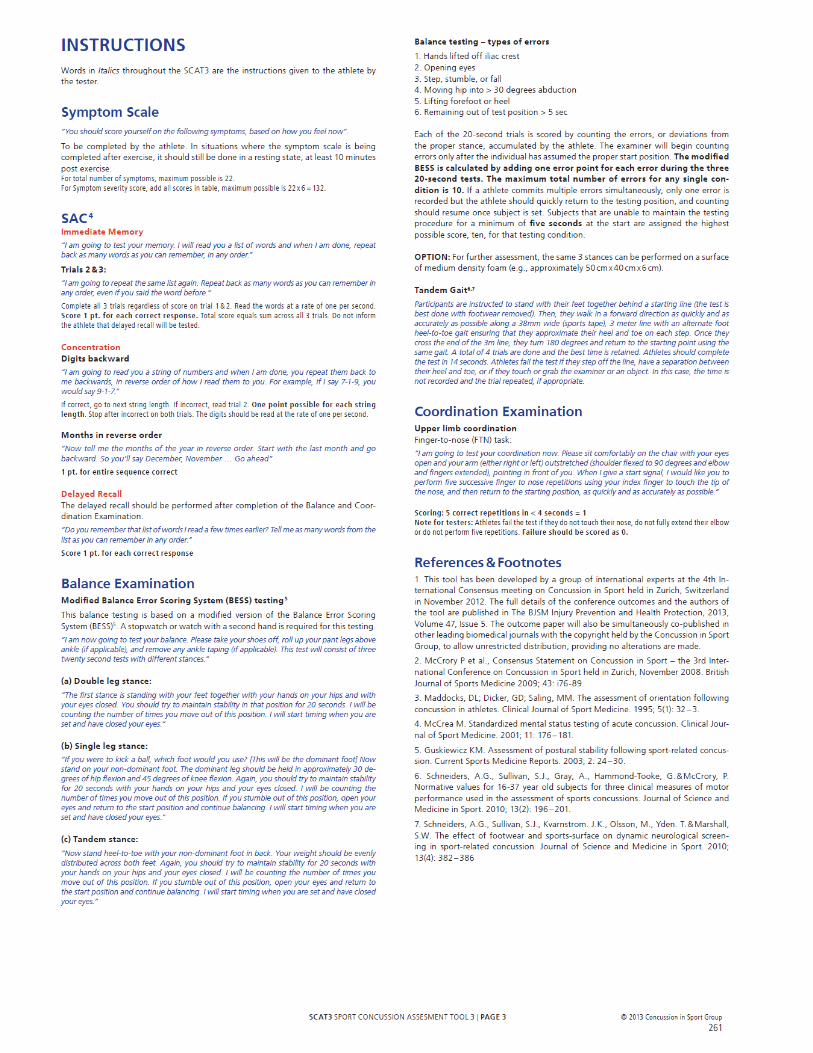
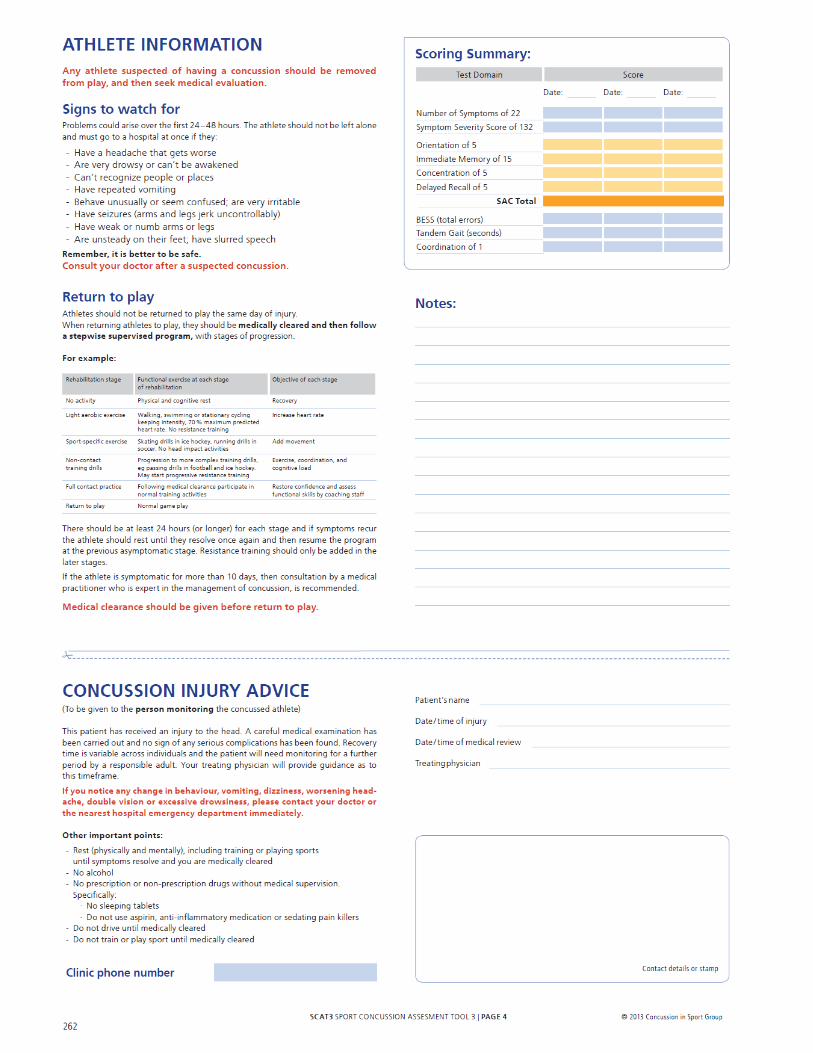
APPENDIX B
SCAT3Sport Concussion Assessment Tool 3


APPENDIX C
HEAD INJURY INSTRUCTIONS
Your son/daughter has suffered a head injury. Head injuries vary in severity from mild to severe concussions, to skull fractures. Though most severe head injuries can be recognized at the time of injury, the signs and symptoms of others may not develop until later. Therefore it is extremely important that any athlete who has sustained even a minor head injury be monitored for at least 24 hours.
1. If any of the following conditions occur or current symptoms worsen, you should immediately contact your physician or go to the emergency room:
Headache continues or more importantly worsens, especially deep throbbing ones Nausea and or vomiting Unusual drowsiness, lethargic, or difficult to arouse Ringing in the ears Blurred or double vision Pupils are unequal in size or become dilated Confused or inability to concentrate Convulsions or seizures Blood or clear fluid draining from the ears or nose
2. Do not give any pain medication, sedatives or allow the consumption of alcoholic beverages.
3. Avoid strenuous activity for at least 24 hours. Do not participate in any form of physical activity until all symptoms (i.e. headache, dizziness) are gone.
4. If you have any doubts call your physician or take your son/daughter to the emergency room.
The protocol for any athlete suspected of suffering a concussion is that they must see a physician and provide the school nurse and athletic trainer with a note from that physician. The concussion management policy states that an athlete will not be allowed to return to play until asymptomatic and he or she must complete the return to play protocol conducted by the athletic trainer.
Athletic Trainer: ________________________________________________
Parent/Guardian: _______________________________________________