Embed Size (px)
Citation preview
Test inventory.................................................................................................................3Australian Scale for Asperger’s Syndrome................................................................3Achenbach Child Behaviour Checklist......................................................................3Achenbach System of Empirically Based Assessment Ages 6-18.............................4Anxiety Disorders Interview Schedule –Revised (ADIS-R) Child............................4Beck Anxiety Inventory.............................................................................................4Beck Depression Inventory –II..................................................................................5Beck Hopelessness Inventory.....................................................................................7Beck Youth Inventories of Emotional & Social Impairment...................................10Bene Anthony Family Relations Test (Test cupboard).........................................10Benton Controlled Oral Word Association Test......................................................11British Ability Scales...............................................................................................11CAVLT.....................................................................................................................12Child’s Auditory Verbal Learning Test...................................................................13Children’s Apperception Test..................................................................................13Children’s atypical development scale.....................................................................14Children’s Depression Scale....................................................................................15Children’s Memory Scale.........................................................................................15Connor’s rating scales..............................................................................................16Connors’ Continuous Performance Test 2.0............................................................17Coopersmith Self-Esteem Inventory........................................................................17Coping Scale for Adults...........................................................................................18Delis-Kaplan Executive Function System................................................................18Depression Anxiety Stress Scales............................................................................19DES..........................................................................................................................19Eating Disorder Inventory-II....................................................................................19Goldstein-Scheerer Tests of Abstract and Concrete Thinking.................................20Impact of Events Scale (IES)...................................................................................20Kaufman Assessment Battery for Children..............................................................20Key Math Revised....................................................................................................22Millon Clinical Multiaxial Inventory.......................................................................22MMPI-2....................................................................................................................24MMPI-Adolescent....................................................................................................25NART.......................................................................................................................26NEALE.....................................................................................................................26Pain - OMPSQ..........................................................................................................26P-3 & Pain profile....................................................................................................27Padua inventory........................................................................................................27Piers-Harris 2, Piers Harris Children’s Self Concept Scale.....................................27Post-Traumatic Stress Diagnostic Scale...................................................................28Personality Assessment Inventory...........................................................................29Rey Auditory Verbal Learning Test (RAVLT)........................................................30Rey Complex Figure Test........................................................................................31Reynolds Adolescent Depression Scale...................................................................32Reynolds Child Depression Scale............................................................................33RCMAS....................................................................................................................34Rohde Sentence Completion Method.......................................................................34Rorschach Inkblot Test.............................................................................................35SCL-90-R.................................................................................................................35SCOLP.....................................................................................................................37
Self-Directed Search................................................................................................37SIQ...........................................................................................................................38ASIQ.........................................................................................................................39Social Skills Training: Enhancing Social Competence with Children and Adolescents..............................................................................................................39South Australian Spelling Test.................................................................................40STAXI......................................................................................................................40STAXI-2...................................................................................................................42STROOP TEST........................................................................................................43SYMBOL DIGIT MODALITIES TEST (SDMT)...................................................44Thematic Apperception Test....................................................................................45TRAIL MAKING TEST..........................................................................................45TRAUMA SYMPTOM INVENTORY...................................................................46WAIS-R....................................................................................................................47WASI........................................................................................................................49WIAT.......................................................................................................................50Wechsler Memory Scale-Revised............................................................................50WISC-III...................................................................................................................50WISC-IV..................................................................................................................53Wisconsin Card Sort Test.........................................................................................56Woodcock Reading Mastery Tests-Revised............................................................56WPPSI-R..................................................................................................................57WPPSI-III.................................................................................................................59Wide Range Assessment of Memory and Learning.................................................63
Test inventoryAustralian Scale for Asperger’s SyndromeThis questionnaire is designed to identify behaviours and abilities indicative of
Asperger's Syndrome in children during their primary school years. This is the age at
which the unusual pattern of behaviour and abilities is most conspicuous. Each
question or statement has a rating scale with 0 as the ordinary level expected of a
child of that age.
Achenbach Child Behaviour ChecklistPurpose: Designed to assess "social competence" and "behavior problems" in
children. [Parent, teacher, self-report]
Population: Ages 4-18.
Score: Five scale scores.
Authors: Thomas M. Achenbach and Craig Edelbrock.
Publisher: Thomas M. Achenbach.
Description: The Child Behavior Checklist (CBCL) was designed to address the
problem of defining child behavior problems empirically. It is based on a careful
review of the literature and carefully conducted empirical studies. It is designed to
assess in a standardized format the behavioral problems and social competencies of
children as reported by parents.
Scoring: The CBCL can be self-administered or administered by an interviewer. It
consists of 118 items related to behavior problems which are scored on a 3-point scale
ranging from not true to often true of the child. There are also 20 social competency
items used to obtain parents’ reports of the amount and quality of their child’s
participation in sports, hobbies, games, activities, organizations, jobs and chores,
friendships, how well the child gets along with others and plays and works by
him/herself, and school functioning.
Reliability: Individual item intraclass correlations (ICC) of greater than .90 were
obtained "between item scores obtained from mothers filling out the CBCL at 1-week
intervals, mothers and fathers filling out the CBCL on their clinically-referred
children, and three different interviewers obtaining CBCLs from parents of
demographically matched triads of children." Stability of ICCs over a 3-month period
were .84 for behavior problems and .97 for social competencies. Test-retest reliability
of mothers’ ratings were .89. Some differences were found between mothers’ and
fathers’ individual ratings.
Validity: Several studies have supported the construct validity of the instrument.
Tests of criterion-related validity using clinical status as the criterion (referred/non-
referred) also support the validity of the instrument. Importantly, demographic
variables such as race and SES accounted for a relatively small proportion of score
variance.
Norms: Normative data, obtained from parents of 1,300 children, were heterogeneous
with respect to race and socioeconomic status and were proportionate to the
composition of the general U.S. population.
Suggested Uses: It is suggested that the CBCL is a viable tool for assessing a child’s
behaviors, via parent report, in a clinical or research environment.
Achenbach System of Empirically Based Assessment Ages 6-18The Achenbach System of Empirically Based Assessment (ASEBA) includes an
integrated set of rating forms for ages 1.5 to 59:
Ages 1.5-5 Module (Pre-School)
Ages 6-18 Module (School)
new Test Observation Forms for Ages 2-18 (TOF/2-18)
Ages 18-59 Module (Adult)
Ages 60+ Module (Adult) -- Call
ASEBA forms are used and researched worldwide, as reported in some 5,000 studies
across 50 countries.
Features
Multi-informant assessment for ages 1.5-59 with separate forms available for
parents/caregivers, teachers/educators, self-rating
Separate norms by gender and age group for competencies, adaptive functioning,
syndromes, DSM-oriented scales, Internalizing, Externalizing, and Total Problems
Comparable scales across wide age ranges
User-friendly forms for both hand-scoring and key entry (computer-scoring);
scannable forms and direct client entry also available
Specialized Guides illustrate use of the ASEBA in mental health, medical, school, and
child/family service settings
Extensive research on service needs and outcomes; diagnosis; prevalence of problems,
medical conditions, treatment efficacy, genetic and environmental effects,
epidemiology, cross-cultural variatons, child abuse, ADHD, HIV, PTSD
The ASEBA offers a comprehensive approach to assessing adaptive and maladaptive
functioning. ASEBA instruments clearly document clients' functioning in terms of
both quantitative scores and individualized descriptions in respondents' own words.
Descriptions include what concerns respondents most about the clients; the best things
about clients; and details of competencies and problems that are not captured by
quantitative scores alone. The individualized descriptive data, plus competence,
adaptive, and problem scores, facilitate comprehensive, in-depth assessment.
Numerous studies demonstrate significant associations between ASEBA scores and
both diagnostic and special education categories. You can relate ASEBA directly to
DSM-IV diagnostic categories by using the normed DSM-oriented scales that are
available for scoring ASEBA forms.
Ages 1.5-5 Module (Pre-School Age)
Child Behavior Checklist for Ages 1.5-5 (CBCL/1.5-5)
Caregiver-Teacher Report Form (C-TRF/1.5-5)
Ages 6-18 Module (School Age)
Child Behavior Checklist for Ages 6-18 (CBCL/6-18)
Youth Self-Report for Ages 11-18 (YSR/11-18)
Teacher's Report Form for Ages 6-18 (TRF/6-18)
Test Observation Forms for Ages 2-18 (TOF/2-18) NEW
Direct Observation Form for Ages 5-14 (DOF)
Semistructured Clinical Interview for Children & Adolescents (SCICA)
Ages 18-59 Module (Adult Age)
Adult Behavior Checklist for Ages 18-59 (ABCL)
Adult Self-Report for Ages 18-59 (ASR)
Anxiety Disorders Interview Schedule –Revised (ADIS-R) Child(none found yet)
Beck Anxiety InventoryPurpose: Designed to discriminate anxiety from depression in individuals.
Population: Adults.
Score: Yields a total score
Time: (5-10) minutes.
Author: Aaron T. Beck.
Publisher: The Psychological Corporation.
Description: The Beck Anxiety Inventory (BAI) was developed to address the need
for an instrument that would reliably discriminate anxiety from depression while
displaying convergent validity. Such an instrument would offer advantages for clinical
and research purposes over existing self-report measures, which have not been shown
to differentiate anxiety from depression adequately.
Scoring: The scale consists of 21 items, each describing a common symptom of
anxiety. The respondent is asked to rate how much he or she has been bothered by
each symptom over the past week on a 4-point scale ranging from 0 to 3. The items
are summed to obtain a total score that can range from 0 to 63.
Reliability: The scale obtained high internal consistency and item-total correlations
ranging from .30 to .71 (median=.60). A subsample of patients (n=83) completed the
BAI after 1 week, and the correlation between intake and 1-week BAI scores was .75.
Validity: The correlations of the BAI with a set of self-report and clinician-rated
scales were all significant. The correlation of the BAI with the HARS-R and HRSD-R
were .51 and .25, respectively. The correlation of the BAI with the BDI was .48.
Convergent and discriminant validity to discriminate homogeneous and
heterogeneous diagnostic groups were ascertained from three studies. The results
confirm the presence of these validities.
Norms: The three normative samples of psychiatric outpatients were drawn from
consecutive routine evaluations at the Center for Cognitive Therapy in Philadelphia,
Pennsylvania. The total sample size was 1,086. There were 456 men and 630 women.
Suggested Uses: Recommended for use in assessing anxiety in clinical and research
settings
Beck Depression Inventory –IIThe Beck Depression Inventory Second Edition (BDI-II) is a 21-item self-report
instrument intended to assess the existence and severity of symptoms of depression as
listed in the American Psychiatric Association's Diagnostic and Statistical Manual of
Mental Disorders Fourth Edition (DSM-IV; 1994). This new revised edition replaces
the BDI and the BDI-1A, and includes items intending to index symptoms of severe
depression, which would require hospitalization. Items have been changed to indicate
increases or decreases in sleep and appetite, items labeled body image, work
difficulty, weight loss, and somatic preoccupation were replaced with items labeled
agitation, concentration difficulty and loss of energy, and many statements were
reworded resulting in a substantial revision of the original BDI and BDI-1A. When
presented with the BDI-II, a patient is asked to consider each statement as it relates to
the way they have felt for the past two weeks, to more accurately correspond to the
DSM-IV criteria.
Each of the 21 items corresponding to a symptom of depression is summed to give a
single score for the BDI-II. There is a four-point scale for each item ranging from 0 to
3. On two items (16 and 18) there are seven options to indicate either an increase or
decrease of appetite and sleep. Cut score guidelines for the BDI-II are given with the
recommendation that thresholds be adjusted based on the characteristics of the
sample, and the purpose for use of the BDI-II. Total score of 0-13 is considered
minimal range, 14-19 is mild, 20-28 is moderate, and 29-63 is severe.
BDI has been used for 35 years to identify and assess depressive symptoms, and has
been reported to be highly reliable regardless of the population. It has a high
coefficient alpha, (.80) its construct validity has been established, and it is able to
differentiate depressed from non-depressed patients. For the BDI-II the coefficient
alphas (.92 for outpatients and .93 for the college students) were higher than those for
the BDI- 1A (.8 6). The correlations for the corrected item-total were significant at .05
level (with a Bonferroni adjustment), for both the outpatient and the college student
samples. Test-retest reliability was studied using the responses of 26 outpatients who
were tested at first and second therapy sessions one week apart. There was a
correlation of .93, which was significant at p < .001. The mean scores of the first and
second total scores were comparable with a paired t (25)=1.08, which was not
significant.
Validity: One of the main objectives of this new version of the BDI was to have it
conform more closely to the diagnostic criteria for depression, and items were added,
eliminated and reworded to specifically assess the symptoms of depression listed in
the DSM-IV and thus increase the content validity of the measure. With regard to
construct validity, the convergent validity of the BDI-II was assessed by
administration of the BDI-1A and the BDI-II to two sub-samples of outpatients
(N=191). The order of presentation was counterbalanced and at least one other
measure was administered between these two versions of the BDI, yielding a
correlation of .93 (p<.001) and means of 18.92 (SD = 11.32) and 21.888 (SD = 12.69)
the mean BDI-II score being 2.96 points higher than the BDI-1A. A calibration study
of the two scales was also conducted, and these results are available in the BDI-II
manual. Consistent with the comparison of mean differences, the BDI-II scores are 3
points higher than the BDI-1A scores in the middle of the scale. Factorial Validity has
been established by the inter-correlations of the 21 items calculated from the sample
responses.
Beck Hopelessness InventoryDescription: Hopelessness is the experience of despair or extreme pessimism about
the future, and as such, is part of the "cognitive triad" (along with a negative view of
oneself and one's world) described in Beck's (1979) cognitive model of depression.
According to Shneidman (1996), hopelessness-helplessness is the most common
emotion experienced among suicidal persons. The Beck Hopelessness Scale (Beck et
al., 1974; Beck and Steer, 1988; Steer and Beck, 1988) is a 20-item assessment device
designed to measure negative expectations about the future. Individuals completing
the BHS are asked to answer the questionnaire based on their attitudes during the
preceding week. The self-report instrument may be administered in written or oral
form, and each item is scored with a true/false response. Total scores range from 0-20
with higher scores indicating a greater degree of hopelessness. The BHS has been
translated into Dutch (DeWilde et al., 1993) and Hebrew (Pershakovsky, 1985).
Potential Use: Clinical research and assessment.
Populations Studied: The BHS has been used with high school students and other
non-clinically ascertained populations (DeWilde et al., 1993; Osman et al., 1998),
adolescent psychiatric outpatients (Brent et al., 1997; 1998) and inpatients (Enns et
al., 1997; Goldston et al., 2000; Kashden et al., 1993; Kumar and Steer, 1995; Morano
et al., 1993; Rotheram-Borus and Trautman, 1988; Steer et al., 1993a, 1993b; Topol
and Reznikoff, 1982), and adolescent suicide attempters on a pediatrics unit (Swedo et
al., 1991).
Reliability: Among adolescents who have been psychiatrically hospitalized,
hopelessness as assessed with the BHS seems to be a relatively stable construct
(correlation between serial administrations 6 months apart = .63; Goldston,
unpublished data, January 2000). These data dovetail with data from adult samples
suggesting that hopelessness as assessed with the BHS has some "trait characteristics"
(Young et al., 1996).
Internal Consistency: In adolescent psychiatric inpatients (Steer et al., 1993a), the
BHS has been found to be internally consistent (KR-20 coefficient=.86). Both the
Dutch translation of the scale (in three samples of adolescents) and the Israeli version
of the BHS have been found to be internally consistent (alphas from .68 to .75, and
alpha=.89, respectively).
Concurrent Validity: In a United States adolescent psychiatric inpatient sample, and
in Canadian samples of Aboriginal psychiatric inpatient suicide attempters and non-
Aboriginal psychiatric inpatient suicide attempters, BHS scores were found to
correlate (r=.53, .75, and .82, respectively) with severity of depression as measured
with the BDI (Enns et al., 1997). In nonreferred adolescents, BHS scores were
negatively related (as predicted) with Reasons for Living - Adolescent Version total
scores (r=-.65; Osman et al., 1998). In adolescent psychiatric inpatients, severity of
hopelessness was positively related to suicidal ideation (Steer et al., 1993b). Likewise,
changes in hopelessness over one year among high school students were related to
changes in suicidal ideation over the same period of time, after controlling for
changes in depression (Mazza and Reynolds, 1998).
In both Caucasian and Aboriginal adolescent psychiatric inpatient suicide attempters,
BHS scores were related to suicide intent; the relationship between BHS scores and
suicide intent remained significant for Caucasian but not Aboriginal youths after
controlling for concurrent depression (Enns et al., 1997). BHS scores were not found
to be related to suicidal intent among primarily Hispanic and African-American
adolescent psychiatry inpatient suicide attempters (Rotheram-Borus and Trautman,
1988).
In one study, adolescent suicide attempters reported more hopelessness at psychiatric
hospitalization than did adolescents without a history of attempts (Goldston et al.,
2000). In another study, suicidal adolescents as well as depressed nonsuicidal
adolescents reported more hopelessness than nondepressed, nonsuicidal adolescents
(DeWilde et al., 1993). In this study, depressed adolescents also reported more
hopelessness than suicidal youths, although it is worth noting that some of the suicide
attempters made their suicide attempts as long ago as one year before the study.
Psychiatrically hospitalized adolescent suicide attempters had higher hopelessness
scores than nonattempters, both in samples matched for severity of depression
(Morano et al., 1993) and in samples not matched for depression scores (Kashden et
al., 1993; Topol and Reznikoff, 1982). Hopelessness was one of two variables that
were used to discriminate between (or correctly classify) 76% of suicide attempters
hospitalized on a pediatrics unit, other at-risk youths, and normal controls (Swedo et
al., 1991).
Predictive Validity: Among adults, hopelessness has repeatedly been found to be
associated with eventual suicide (Beck et al., 1985, 1990; Fawcett et al., 1990) and
repeat self-harm behaviors (Scott et al., 1997; Brittlebank et al., 1990) in clinically
referred samples.
Among adolescent psychiatric inpatients with a history of suicide attempts, BHS
scores were predictive of suicide attempts following discharge from the hospital
(Goldston et al., 2000). These predictive effects were not apparent among adolescents
without a history of attempts, and were no longer statistically significant after
controlling for depression (Goldston et al., 2000). In a second study (Hawton et al.,
1999), the BHS failed to differentiate between adolescents who made repeat attempts
and adolescents who did not make repeat attempts in a 1-year follow-up after
hospitalization for self-poisoning. However, this study was limited in power because
of the small number of youths attempting suicide in the follow-up. When Hawton et
al. (1999) combined for statistical analyses the adolescents who presented at
hospitalization with repeat suicide attempts and adolescents who made repeat suicide
attempts over the follow-up, the repeaters did on average have higher BHS scores
than the youths with single overdoses.
Adults who prematurely discontinue cognitive therapy have higher hopelessness
scores than adults who remain in therapy (Dahlsgaard et al., 1998). In a controlled
treatment study, Brent et al. (1997) also found that adolescents who dropped out of
therapy had higher hopelessness scores than adolescents who remained in therapy.
Brent et al. (1998) also found higher BHS scores to be associated with failure to
achieve clinical remission of major depression.
Treatment Studies: A suicide prevention program was found to reduce BHS scores
in some but not all schools (Orbach and Bar-Joseph, 1993); however, BHS scores
were generally low in this high school population even before the intervention.
The BHS has been used in multiple treatment studies with adults (e.g., Rush et al.,
1982), but has not been used as a primary outcomes measure in a controlled treatment
trial with youths.
Summary and Evaluation: The Beck Hopelessness Scale is an excellent scale based
on the cognitive theory of depression that has been widely used with adults, but less
used in studies with adolescents. Among adults, the BHS repeatedly has been found to
be associated with repeat suicide attempts and completed suicide in clinically
ascertained samples. Hopelessness also has been found to predict later suicide
attempts (over 5 years) among psychiatrically hospitalized adolescents with a history
of prior attempts (but not among youths without prior attempts). An important
consideration in treatment studies is that BHS scores have been found to be associated
with treatment dropout in both samples of adults and adolescents.
Beck Youth Inventories of Emotional & Social ImpairmentUsed to assess emotional & social impairment in children ages 7 through 14. The new
Beck Youth Inventories five self-report inventories can be used separately or in
combination to assess symptoms of depression, anxiety, anger, disruptive behavior,
and self-concept.
Five Inventories
The five inventories each contain 20 statements about thoughts, feelings, and
behaviors associated with emotional and social impairment in youth. Children
describe how frequently the statement has been true for them during the past two
weeks, including today. The instruments measure a child's emotional and social
impairment in five specific areas:
Beck Depression Inventory for Youth: In line with the depression criteria of the
Diagnostic and Statistical Manual of Mental Health Disorders–Fourth Edition (DSM–
IV), this inventory allows for early identification of symptoms of depression. It
includes items related to a child's negative thoughts about self, life and the future,
feelings of sadness and guilt, and sleep disturbance.
Beck Anxiety Inventory for Youth: Reflects children's specific worries about school
performance, the future, negative reactions of others, fears including loss of control,
and physiological symptoms associated with anxiety.
Beck Anger Inventory for Youth: Evaluates a child's thoughts of being treated
unfairly by others, feelings of anger and hatred.
Beck Disruptive Behavior Inventory for Youth: Identifies thoughts and behaviors
associated with conduct disorder and oppositional-defiant behavior.
Beck Self-Concept Inventory for Youth: Taps cognitions of competence, potency, and
positive self-worth.
Child-Friendly
Using the same principles as the widely-used Beck Depression Inventory®–II and
other adult Beck Inventories for anxiety, hopelessness and suicide ideation, the Beck
Youth Inventories focus on children's self-perceived behavior, cognitions and
feelings. Each inventory can be completed in just 5 to 10 minutes.
Items are written at a 2nd grade reading level, with language that is easy to understand
for self-reporting; they may also be administered orally to those who have difficulty
reading at this level. Items have been selected from statements made by children seen
in various treatment settings.
Multiple Uses in School and Clinical Settings
Consistent with IDEA legislation requirements, the Beck Youth Inventories are
intended for screening for emotional and social difficulties that may impair a child's
ability to function in school settings. These inventories are useful in planning and
monitoring educational placement as well as in clinical treatment settings.
For children who are classified as emotionally disturbed, or who are emotionally
volatile, the inventories may be used for routine monitoring.
Flexible Scoring and Profiling
Norms allow comparison with responses of children within age and gender groups
that are ethnically and socio-economically representative of the U.S. population.
Scoring and profiling are adaptable to the clinical needs of and time available to the
user, including:
across inventory profiling for a global picture of the child's experience and
possible diagnostic impression;
inventory analysis for specific understanding of a child's experience in one
affective domain; and
single domain scores for expedient progress monitoring.
Cost-Effective for Treatment Decisions
These inventories offer brief, cost-effective methods for assessing both the severity of
a child's symptoms as well as change during the course of treatment. Initially, all
inventories may be administered to assist in treatment planning, with select ones used
in subsequent sessions as needed to target specific areas of treatment. The inventories
can be completed prior to each session without using valuable treatment time; ease
and flexibility of scoring also allows for problem identification and prevention efforts
without extensive training.
Bene Anthony Family Relations Test (Test cupboard)Purpose: The test assesses the feelings and emotions, negative and positive, that a
child has towards their family.
Benefits: Measures outgoing and incoming negative and positive feelings for each
figure, highlighting relationships which you may need to focus on.
Gives you information about a child's view of their family relationships and thoughts
concerning them, to which you can then focus attention.
Contains an easy-to-use scoring procedure which assesses the feelings associated with
maternal and paternal over-protection and over-indulgence and personality strength
and weakness.
Benton Controlled Oral Word Association TestThe Controlled Oral Word Association Test (COWAT) is a measure of a person's
ability to make verbal associations to specified letters (i.e., C, F. and L). This measure
is a useful component of a neuropsychological battery as it is able to detect changes in
word association fluency often found with various disorders.
British Ability ScalesA reliable measure of cognitive functioning over a wide age range, using ability
scales. These are divided into two batteries, available separately or together as a Full
Age Range kit. The assessment enables you to derive a general conceptual ability
score (GCA). Where more specific abilities need investigating, other diagnostic scales
can be used to provide a more detailed profile
Format: Individual
Time: 30-45 mins
Age: 2 years 6 months – 17 years 11 months
Purpose: A cognitive functioning measure that enables you to use scales tailored to a
specific problem.
Benefits: Age-related start points and decision points pinpoint an individual’s ability
range, and terminate the scale as soon as sufficient information is gathered to ensure
manageable testing times and minimise the risk of fatigue.
In addition to presenting profiles and discrepancy scores, it generates two
interpretative narrative reports for you to customise or edit; one for parents/teachers
and a more technical report for psychologists. Microsoft Windows compatible.
Contents
Available in 3 versions:
Full Age Range for 2.6 to 17:11 years
Early Years for 2:6 to 5:11 years
School Age for 5:0 to 17:11 years
Complete Set contains:
Stimulus Items for each scale
Stimulus Booklets
10 Record Forms
10 Assessment Booklets.
CAVLTThe CAVLT-2 measures auditory verbal learning and memory abilities-processes
commonly disrupted in learning disabilities and brain trauma. This test is designed to
be used with children and adolescents ages 6.6-17.11 years as part of a comprehensive
psychoeducational or neuropsychological assessment battery.
The CAVLT-2 is composed of one recognition and two free-recall memory word lists
designed specifically for young people. The first free-recall word list is presented for
five trials. The second free-recall test is presented as an interference list, after which
the individual is asked to recall words from the first list. Following a brief delay,
retention is assessed by a second recall test of the words from the first list. Finally,
words from a new recognition list are presented; the individual must decide whether
each word was included in the original free-recall word list.
The CAVLT-2 yields measures of immediate memory span, level of learning,
immediate recall, delayed recall, recognition accuracy, and total intrusions. The
CAVLT-2 scores for each trial may now be obtained and baserate tables are included
for standard score comparisons. Scores are reported as both percentiles and
normalized standard scores. Performance profiles for both learning trials and CAVLT-
2 summary scores can be plotted on the test booklet.
Normative data are provided for 12 age groups and include learning trial scores.
Results from generalizability and validity studies are contained in the manual. Four
case studies, including a learning-disabled sample, are also presented.
Child’s Auditory Verbal Learning TestType of test: Neuro – Memory / Learning
Ages: 6.5 – 18
Testing time: 45 minutes
Children’s Apperception TestPurpose: Designed as a projective method of describing personality.
Population: Ages 3 to 10 years.
Time: 30 minutes.
Description: The Children’s Apperception Test (CAT-A) is a projective method of
describing personality by studying individual differences in the responses made to
stimuli presented in the form of pictures of animals in selected settings. The 10 items
consist of 10 scenes showing a variety of animal figures, mostly in unmistakably
human social settings. The use of animal rather than human figures was based on the
assumption that children of these ages would identify more readily with appealing
drawings of animals than with drawings of humans. The author discusses
interpretation on the basis of psychoanalytic themes, but there is no compelling reason
that Children’s Apperception Test protocols could not be interpreted from other
theoretical frameworks.
Scoring: This projective technique is not "scored" in a quantitative sense. The gist of
stores is recorded, and the presence or absence of thematic elements is indicated on
the form provided.
Reliability and Validity: No statistical information is provided on the technical
validity and reliability of the CAT.
Norms: Information on norms is not included in the manual.
Suggested Uses: Designed for use in clinical and research settings.
Children’s atypical development scaleJ Abnorm Child Psychol. 1994 Apr;22(2):167-76
Psychometric properties of the children's atypical development scale.
Stein MA, Szumowski E, Sandoval R, Nadelman D, O'Brien T, Krasowski M,
Phillips W.
The Children's Atypical Development Scale (CADS) is a 53-item rating scale
designed to measure unusual behaviors in children. Principal-factor analysis on a
clinic-referred and pediatric sample of 474 children resulted in a four-factor solution:
Communication Deficits, Lability, Social Relatedness Deficits, and Preoccupation.
The CADS is internally consistent and has adequate temporal stability. CADS factor
scores were differentially associated with parent and teacher rating scales, IQ, and
Continuous Performance Test errors. The scale shows promise as a clinical and
research tool for assessing atypical behaviors associated with pervasive
developmental disorder and other neurobehavioral disorders.
Children’s Depression ScaleFirst published in 1978, the CDS is an invaluable tool for identifying depressed
children. Six sub-scales measure affective response, social problems, self-esteem,
pre-occupation with own sickness or death, guilt, pleasure and enjoyment. Children
post responses into one of five boxes: “very right”, “right”, “don’t know / not sure”,
“wrong”, or “very wrong”.
A parent’s questionnaire allows for others to report on the child’s behaviour and
feelings. The questionnaire is intended for use with parents, siblings, teachers and
relatives of the child to provide another index of the child’s depression or well-being.
The CDS is used by clinicians for therapy as well as assessment. In counselling and
psychotherapy the CDS helps children acknowledge their sadness or depression. It is
also used in family therapy to help children and parents talk to each other about their
feelings. The scale has a game-like quality which facilitates the children’s ability to
communicate more fully their experience.
For assessment of depression, the CDS provides an indication of the child’s
depression along two continua: depression and the capacity to enjoy life.
Children’s Memory ScaleCompares memory and learning to ability, attention, and achievement. The Children’s
Memory Scale™ (CMS) fills the need for a comprehensive learning and memory test
for children ages five to 16.
Multiple Uses
• Plays a vital role in assessing learning disabilities and attention deficit disorders
• Helps to plan remediation and intervention strategies for school and clinical settings
As a screener or diagnostic instrument, CMS measures learning in a variety of
memory dimensions:
• Attention and working memory
• Verbal and visual memory
• Short- and long-delay memory
• Recall and recognition
• Learning characteristics.
Serves as a process skills screening instrument
For children with learning disabilities, diagnosed with TBI, ADHD, epilepsy, cancer,
brain tumors
Connor’s rating scalesThe Conners' Rating Scales - Revised (CRS-R) are a result of 30 years of research on
childhood and adolescent psychopathology and problem behavior. The CRS-R assess
for attention-deficit/hyperactivity disorder in children and adolescents (aged 3-17),
and can measure treatment changes and outcome assessment purposes. The CRS-R
are composed of the parent rating scale, teacher rating scale and adolescent self-report
scale, all of which come in a long version, taking 15-20 minutes to complete, and a
short version, taking 5-10 minutes to complete. The information below pertains to the
teacher rating scale.
Number of Versions: 3
Version: Teacher
Author(s): C. Keith Conners, Ph.D.
Date of Publication: 1997
Material(s) Needed for Test: Instrument
Manual: Available
Charge for one form or kit: Yes
Purpose and Nature of Test
Construct(s) Measured:Conduct Problems, Cognitive Problems, Anxiety
Problems, Social Problems.
Population for which
designed:Age Range: 3 through 17 years old
Method of Administration: Individual
Source of Information: Teacher
Subtests and Scores: Oppositional, Social Problems, Cognitive
Problems/Inattention, DSM-IV Symptom Subscales,
Hyperactivity, Conners' ADHD Index, Anxious-Shy,
Conners' Global Index, Perfectionism
Number of Items: 59
Type of Scale: Likert
Connors’ Continuous Performance Test 2.0(nothing located)
Coopersmith Self-Esteem InventoryThe Coopersmith Self-Esteem Inventory was developed through research to assess
attitude toward oneself in general, and in specific contexts: peers, parents, school, and
personal interests. It was originally designed for use with children, drawing on items
from scales that were previously used by Carl Rogers. Respondents state whether a set
of 50 generally favorable or unfavorable aspects of a person are "like me" or "not like
me." There are two forms, a School Form (ages 8-15) and an Adult form (ages 16 and
older) (Anastasi, 1988; Blascovich & Tomaka, 1991; Pervin, 1993). Acceptable
reliability (internal consistency and test-retest) and validity (convergent and
discriminant) information exists for the Self-Esteem Inventory (see Blascovich &
Tomaka, 1991).
Coping Scale for AdultsDesigned as a self-report inventory that examines coping behavior. The test comprises
of an administrator’s manual, four test forms, a scoring sheet and a profile chart. The
manual includes guidance for the administration, scoring and interpretation of the test.
The test forms are made up of two short forms, one for general and the other for
specific concerns, and two long forms, also for general and specific concerns. The
forms contain items which describe a coping strategy; the short forms contain 19
items representing each coping scale; the long version contains between three to seven
items representing each scale, making up 73 items in all. The respondents answer each
item on a five point Likert scale that assesses the degree to which each coping strategy
is used. The scale ranges from ‘Used a great deal’ to ‘Doesn’t apply or don’t do it’.
Each form includes an open question at the end.
The forms appear printed back to back and are appointed by colour; purple for general
and green for specific. Hence, the long forms, for example, will be printed on the
same sheet of paper; one side of this sheet will be purple, the other side green.
Accompanying the long forms is a scoring sheet for manual scoring of both general
and specific versions, and a profile chart, which can provide graphic feedback of
results from both the general and specific forms, and for individual scores or group
scores. The long form may be scored by machine using Optical Mark Recognition
(OMR) Scoring Services. The short form cannot be scored in this manner.
All of the forms are non-reusable. The authors give no indication of the order in
which the forms should be presented.
The respondent will need a pen or pencil and eraser to complete the forms and the
administrator will perhaps need a calculator to score the test, the authors suggest using
different coloured pens to mark out the profile chart in order to distinguish between
the profiles for general and specific concerns.
Delis-Kaplan Executive Function SystemThe Delis-Kaplan Executive Function System (D-KEFS) is the first nationally
standardized set of tests to evaluate higher level cognitive functions in both children
and adults. Assesses key areas of executive function (problem-solving, thinking
flexibility, fluency, planning, deductive reasoning) in both spatial and verbal
modalities, normed for ages 8-89.
With nine stand-alone tests, comprehensively assess the key components of executive
functions believed to be mediated primarily by the frontal lobe.
Engaging Materials: Its game-like format is engaging for examinees, encouraging
optimal performance without providing “right/wrong” feedback that can create
frustration in some children and adults.
Multiple Uses
Assess the integrity of the frontal system of the brain
Determine how deficits in abstract, creative thinking may impact daily life
Plan coping strategies and rehabilitation programs tailored to each patient’s profile of
executive-function strengths and weaknesses..
Depression Anxiety Stress ScalesThe DASS is a 42 item self-report inventory that yields 3 factors: Depression;
Anxiety; and Stress. This measure proposes that physical anxiety (fear
symptomatology) and mental stress (nervous tension and nervous energy) factor-out
as two distinct domains. This screening and outcome measure reflects the past 7 days.
Gamma coefficients that represent the loading of each scale on the overall factor (total
score) are .71 for depression, .86 for anxiety, and .88 for stress. One would expect
anxiety and stress to load higher than depression on the common factor as they are
more highly correlated and, therefore, dominate the definition of this common factor
(Lovibond and Lovibond, 1995). Reliability of the three scales is considered adequate
and test-retest reliability is likewise considered adequate with .71 for depression, .79
for anxiety and .81 for stress (Brown et al., 1997). Exploratory and confirmatory
factor analyses have sustained the proposition of the three factors (p < .05; Brown et
al., 1997). The DASS anxiety scale correlates .81 with the Beck Anxiety Inventory
(BAI), and the DASS Depression scale correlates .74 with the Beck Depression Scale
(BDI).
In the public domain. Can be downloaded for free from the following site
http://www.psy.unsw.edu.au/Groups/Dass/
DESThe Dissociative Experiences Scale (DES) was developed by Eve Bernstein Carlson,
Ph.D. and Frank W. Putnam, M.D. The overall DES score is obtained by adding up
the 28 item scores and dividing by 28: this yields an overall score ranging from 0 to
100. Copies of the DES can be obtained through the Sidran Institute.
The following pages from Dr. Ross's book Dissociative Identity Disorder provide
background information on the DES. The papers by Dr. Ross referenced in the text
are listed elsewhere on this Web site.
The Dissociative Experiences Scale (DES) is a 28-item self-report instrument that can
be completed in 10 minutes, and scored in less than 5 minutes. It is easy to
understand, and the questions are framed in a normative way that does not stigmatize
the respondent for positive responses. A typical DES question is, "Some people have
the experience of finding new things among their belongings that they do not
remember buying. Mark the line to show what percentage of the time this happens to
you." The respondent then slashes the line, which is anchored at 0% on the left and
100% on the right, to show how often he or she has this experience. The DES contains
a variety of dissociative experiences, many of which are normal experiences.
A newer form of the DES has a format in which the responses are made by circling a
percentage ranging from 0% to 100% at 10% intervals. The advantage of the new
form of the DES is that it is easier to score. It appears to have excellent convergent
validity with the original form of the DES, and to be interchangeable with it (Ellason,
Ross, Mayran, & Sainton, 1994).
The DES has very good validity and reliability, and good overall psychometric
properties, as reviewed by its original developers (Carlson, 1994; Carlson &
Armstrong, 1994; Carlson & Putnam, 1993; Carlson et al., 1993). It has excellent
construct validity, which means it is internally consistent and hangs together well, as
reflected in highly significant Spearman correlations of all items with the overall DES
score. The scale is derived from extensive clinical experience with an understanding
of DID. In the initial studies during its development and in all subsequent studies, the
DES has discriminated DID from other diagnostic groups and controls at high levels
of significance, based on either group mean or group median scores. In most samples,
the mean and median DES scores for DID subjects are within 5 points of each other.
As reviewed in Chapter Six, the higher the DES score, the more likely it is that the
person has DID. In a sample of 1,051 clinical subjects, however, only 17% of those
scoring above 30 on the DES actually had DID (Carlson et al., 1993). The DES is not
a diagnostic instrument. It is a screening instrument. High scores on the DES do not
prove that a person has a dissociative disorder, they only suggest that clinical
assessment for dissociation is warranted. This is how we report DES scores in our
consults, as within or not within the range for DID, and as consistent or not consistent
with the clinical and DDIS diagnosis of DID. DID subjects sometimes have low
scores, so a low score does not rule out DID. In fact, given that in most studies the
average DES score for a DID patient is in the 40s, and the standard deviation about
20, roughly about 15% of clinically diagnosed DID patients score below 20 on the
DES.
Eating Disorder Inventory-IIThe EDI-2 is a widely used 91-item self-report measure of symptoms commonly
associated with AN and BN. It provides standardized subscale scores on 11 clinically
relevant dimensions of EDs. Furthermore, it provides normative and reliability data on
11- to 18-year-old females (18).
(18). Shore RA, Porter JE. Normative and reliability data for 11 to 18 year olds on the
eating disorder inventory. Int J Eat Disord 1990;9:201–7.
Goldstein-Scheerer Tests of Abstract and Concrete ThinkingPsychological test inquiring into aptitudes and interests. Reveals weaknesses in
concept formation and abstract thinking, useful in determination between brain
damage and schizophrenia. Hanfmann-Kasanin Test is also used for this same purpose
Impact of Events Scale (IES)
Note: This is The IES not the revised 22 item version (IES-R).
The IES is a 15 item questionnaire evaluating experiences of avoidance and intrusion
which attempts to "reflect the intensity of the post-traumatic phenomena" (McGuire,
1990). Both the intrusion and avoidance scales have displayed acceptable reliability
(alpha of .79 and .82, respectively), and a split-half reliability for the whole scale
of .86 (Horowitz et al., 1979). The IES has also displayed the ability to discriminate a
variety of traumatised groups from non-traumatised groups (see Brier, 1997 for
review).
The IES was developed by Mardi Horowitz, Nancy Wilner, and William Alvarez to
measure current subjective distress related to a specific event (Horowitz, Wilner, &
Alvarez, 1979). Horowitz observed that the most commonly reported responses to
traumatic stressors fell into 2 major response sets: intrusion and avoidance (Horowitz,
et al, 1979; Weiss & Marmar, 1997). Measurements of responses to traumatic events
at the time were confined to physiological measures such as galvanic skin responses
or to self-reports on more general measures of anxiety, neither of which provided a
measure of the current degree of subjective impact experienced following a specific
traumatic event (Weiss & Marmar, 1997). The IES is considered one of the earliest
self-report measures of posttraumatic disturbance ( Briere, 1997).
Type of Instrument: The IES is a broadly applicable self-report measure designed to
assess current subjective distress for any specific life event (Horowitz, et al 1979;
Corcoran & Fischer, 1994). It is an instrument that can be used for repeated
measurement over a period of time. Its sensitivity to change renders it useful for
monitoring the client's progress in therapy (Corcoran & Fischer, 1994).
The IES scale consists of 15 items, 7 of which measure intrusive symptoms (intrusive
thoughts, nightmares, intrusive feelings and imagery), 8 tap avoidance symptoms
(numbing of responsiveness, avoidance of feelings, situations, ideas), and combined,
provide a total subjective stress score. All items of the IES are anchored to a specific
stressor (Horowitz, et al, 1979; Briere, 1997). Respondents are asked to rate the items
on a 4-point scale according to how often each has occurred in the past 7 days. The 4
point on the scale are: 0 (not at all), 1 (rarely), 3 (sometimes), and 5 (often).
Scoring Method: Each item was scored 0, 1, 3 or 5, with the higher scores reflecting
more stressful impact. The scores for the intrusive subscale range from 0 to 35, and is
the sum of the scores for items 1, 4, 5, 6, 0, 11, and 14. The scores for the avoidance
subscale range from 0 to 40, and is the sum of the scores for items 2, 3, 7, 8, 9, 12, 13,
and 15. The sum of the two subscales is the total stress score. It is suggested that the
cut-off point is 26, above which a moderate or severe impact is indicated.
Wayne Corneil, Directory of Employee Assistance for the Department of Health and
Welfare, Canada; Randall Beaton, PhD, Professor of Psychological Nursing at the
University of Washington; and Roger Solomon, PhD, Department Psychologist for
the Washington State Patrol, suggest that the IES can be interpreted according to the
following dimensions:
0 - 8 Subclinical range
9 - 25 Mild range
26 - 43 Moderate range
44 + Severe range
Kaufman Assessment Battery for ChildrenPurpose: Designed for assessing cognitive development in children.
Population: Children, ages 2.5-12.5.
Score: 16 subtests.
Time: (40-85) minutes.
Author(s): Alan Kaufman and Nadeen Kaufman.
Publisher: American Guidance Service.
Description: The Kaufman Assessment Battery for Children (K-ABC) is a clinical
instrument for assessing cognitive development. Its construction incorporates several
recent developments in both psychological theory and statistical methodology. The K-
ABC also gives special attention to certain emerging testing needs, such as use with
handicapped groups, application to problems of learning disabilities, and
appropriateness for cultural and linguistic minorities. The authors rightly caution,
however, that success in meeting these special needs must be judged through practical
use over time. They also point out that the K-ABC should not be regarded as "the
complete test battery"; like any other test, it should be supplemented and corroborated
by other instruments to meet individual needs, such as the Stanford-Binet, Wechsler
scales, McCarthy scales, or neuropsychological tests.
Scoring: The 16 subtests are grouped into a mental processing set and achievement
set, which yield separate global scores. The mental processing set is then grouped into
those requiring primarily sequential processing of information and those requiring
simultaneous processing, with separate global scores for each.
Validity and Reliability: Odd-even reliabilities within one-year age groups averaged
in the .70s and .80s for subtests; for global scores, the averages were in the high .80s
and .90s. Test-retest reliabilities were computed within age groups spanning 3 or 4
years, retested after intervals of 2 to 4 weeks. For subtests, these reliabilities ranged
from .59 to .98, clustering in the .70s and .80s; for global scores, they ranged from .77
to .97. In general, reliabilities were higher for the achievement than for the mental
processing tests. Concurrent and predictive validity (6- to 12 interval) against
standardized achievement tests, were investigated in several small groups of both
normal and exceptional children. The correlations vary widely, but most appear
promising, and the patterns of correlations with subtests tend to fit theoretical
expectations. Analyses by ethnic groups yielded closely similar validities for Blacks,
Hispanics, and Whites.
Norms: Norms for the battery are based on administration of the tests to
representative samples of 100 children at each 6-moth age interval from 2.5 to 12.5, a
total of 2000 individuals. A variety of supplementary norms are provided, some
requiring the testing of additional subjects. Sociocultural norms are provided based on
a cross-tabulation by race (black-white) and by parental education (less than high
school education, high school graduate, and one or more years of college or technical
school).
Suggested Uses: Recommended uses of the K-ABC include integration as a
component of a cognitive assessment battery in clinical situations.
Key Math RevisedThe Revised Key Math is a content-referenced test for children in grades K-9. It can
be used for diagnostic, achievement and curriculum assessment purposes. The 13
domains it measures are: numeration, rational numbers, geometry, addition,
subtraction, multiplication, division, mental computation, measurement, time and
money, estimation, interpreting data, and problem solving. Spring and fall norms are
available for converting raw scores to standard and percentile scores as well as grade
and age equivalents. The test is administered individually and takes between 30 and
50 minutes. The tester, using small flip charts, shows pictures and diagrams to the
examinee and asks progressively harder questions within each domain until three
consecutive errors indicate that a "ceiling level" has been reached. Responses are
recorded by the tester in a score booklet. For the four mathematical operations
sections (addition, subtraction, multiplication, division), and examinee who
progresses beyond the first six basic questions continues within the domain by
working problems by hand at the back of the scoring booklet. Norms for this test were
established on 925 children in 14 states nationwide. Overall alternate-form reliability
averages .90 and split-half reliability is in the high .90s. Cross-validation with the
ITBS yields an overall correlation of .76. Norms are included in the test kit
Millon Clinical Multiaxial InventoryPurpose: Designed as a clinical measure to assist with psychiatric screening and with
clinical diagnosis.
Population: Adult clinical populations.
Score: 10 clinical personality pattern scores.
Time: (25) minutes.
Author: Theodore Millon.
Publisher: National Computer Systems, Inc.
Description: Based on Millon’s theory of personality and psychopathology, the brief
Millon Clinical Multiaxial Inventory-II (MCMI-II) instrument provides a measure of
22 personality disorders and clinical syndromes for adults undergoing psychological
or psychiatric assessment or treatment. Specifically designed to help assess both Axis
I and Axis 11 disorders, the MCMI-II instrument can assist clinicians in psychiatric
diagnosis, developing a treatment approach that takes into account the patient’s
personality style and coping behavior, and guiding treatment decisions based on the
patient’s personality pattern.
Scoring: The MCMI-II consists of 10 clinical personality pattern scales, 3 severe
personality pathology scales, 6 clinical syndrome scales, 3 modifier indices, 1 validity
index.
Reliability: The reliability of the MCMI II generally has been sound, with the Axis II
scales showing the highest stability as predicted by Millon. Normal subjects also had
noticeably higher stability coefficients than clinical subjects. Millon also tested the
stability of high point and double-high-point configurations. He reports that high point
codes are fairly stable over a month, with nearly two thirds of 168 subjects achieving
the same scale high point. For double-high-point configurations, 25% achieve the
same high scores with another 19% achieving the same two scales but in reverse
order. Based on part of his normative sample, Millon reports quite high internal
consistencies. The average of 22 clinical scales is .89, and the range is from .81 to .95.
Validity: Because of extensive item overlap, we cannot be sure of the factor structure
of this instrument. But there are also overlaps based on the overlap of the constructs;
that is, the personality disorders are by no means distinct entities.
Norms: Norms for the MCMI-II instrument are based on a national sample of 1,292
male and female clinical subjects representing a variety of DSM-III and DSM-III-R
diagnoses. The subjects included inpatients and outpatients in clinics, hospitals, and
private practices. The MCMI-II manual describes the distribution of gender, age,
marital status, religion, and other factors within the sample.
Suggested Uses: The MCMI-II is used primarily in clinical settings with individuals
who require mental health services for emotional, social, or interpersonal difficulties.
Qualification Level A
Administer To Individuals 18 years and older
Reading Level 8th grade
Completion Time 25–30 minutes (175 true/false items)
MMPI-2The MMPI-2 test’s contemporary normative sample and extensive research base help
make it the gold standard in assessment for a wide variety of settings. The test can be
used to help:
Assess major symptoms of social and personal maladjustment.
Identify suitable candidates for high-risk public safety positions.
Support classification, treatment, and management decisions in criminal justice and
correctional settings.
Give a strong empirical foundation for a clinician's expert testimony.
Assess medical patients and design effective treatment strategies, including chronic
pain management.
Evaluate participants in substance abuse programs and select appropriate treatment
approaches.
Support college and career counseling recommendations.
Provide valuable insight for marriage and family counseling.
Key Features
Descriptive and diagnostic information relevant to today’s clients.
Tailored reports present interpretive information for specific settings to help meet a
wide range of needs.
Nationally representative normative sample.
Normative sample consists of 1,138 males and 1,462 females between the ages of 18
and 80 from several regions and diverse communities within the U.S.
Flexible administration and scoring.
The test can be administered in several formats: traditional paper-and-pencil,
audiocassette or CD recording, and computer. To help meet the needs of more
individuals, the MMPI-2 test can be administered in English, Spanish, Hmong, and
French for Canada.
Abbreviated format.
The first 370 items of the test can be administered to obtain scores for validity
indicators L, F, and K and the 10 clinical scales. The full MMPI-2 test must be
administered to obtain scores for all the validity indicators, the content scales, and the
supplementary scales.
Quick Facts
Date Published 1989
Qualification Level A
Administer To Individuals 18 years and older
Reading Level 6th grade
Completion Time 60–90 minutes (567 true/false items)
MMPI-AdolescentThe adolescent inventory is shorter than the standard adult version, was developed at
a sixth-grade reading level, and is geared towards adolescent issues and personality
"norms." The MMPI-A has 478 true/false items, or questions, (compared to 567 items
on the MMPI-2) and takes 45 minutes to an hour to complete (compared to 60 to 90
minutes for the MMPI-2). There is also a short form of the test that is comprised of
the first 350 items from the long-form MMPI-A.
The questions asked on the MMPI-A are designed to evaluate the thoughts, emotions,
attitudes, and behavioral traits that comprise personality. The results of the test reflect
an adolescent's personality strengths and weaknesses, and may identify certain
disturbances of personality (psychopathologies) or mental deficits caused by
neurological problems.
There are eight validity scales and ten basic clinical or personality scales scored in the
MMPI-A, and a number of supplementary scales and subscales that may be used with
the test. The validity scales are used to determine whether the test results are actually
valid (i.e., if the test taker was truthful, answered cooperatively and not randomly) and
to assess the test taker's response style (i.e., cooperative, defensive). Each clinical
scale uses a set or subset of MMPI-A questions to evaluate a specific personality trait.
Some were designed to assess potential problems that are associated with
adolescence, such as eating disorders, social problems, family conflicts, and alcohol
or chemical dependency.
NARTTitle: National Adult Reading Test, Second Edition
Author: Nelson, Hazel E.; Willison, Jonathan
Purpose: Developed to estimate "the premorbid intelligence levels of adult patients
suspected of suffering from intellectual deterioration."
NEALEThe Neale Analysis of Reading Ability is an individually administered standardised
diagnostic reading test. It contains a Reader, in book form, comprising six short
graded narratives, each with a limited number of words and having a central theme.
The passages are illustrated.
It consists of four criterion-referenced, supplementary diagnostic tests: Discrimination
of Initial and Final Sounds, Names and Sounds of the Alphabet, Graded Spelling, and
Auditory Discrimination, are provided in the manual, plus Word Lists extracted from
the passages for quick assessment of Accuracy or Word Recognition.
Pain - OMPSQOrebro Musculodkeletal Pain screening questionnaire
Acute pain
Definition: Acute pain is pain that is associated with tissue injury eg, lacerations,
fracture, inflammation, muscle strain.
Analgesics are given to provide pain relief allowing patients to move and function as
normally as possible, particularly as evidence shows that too much rest is detrimental.
Analgesics should be given regularly whilst an injury is still healing; as long as an
injury is present, patients will experience pain.
A sprain may last 2 days while postoperative pain may last up to a week, but patients
often wait until pain becomes intolerable before taking painkillers. This is not
desirable since severe pain is much more difficult to control than moderate pain.
Giving analgesics regularly actually decreases pain before it reaches its peak. For
example, in dysmenorrhea, the pain may be very severe only for the first 2 days.
Therefore, Ponstan® (mefenamic acid, Pfizer), Voltaren® (diclofenac, Novartis) or
other NSAIDs should be taken on a regular basis for 2 days.
Multimodal analgesia describes giving different drugs acting at different levels of the
nociceptive (pain) pathway are used concurrently, using opioids, NSAIDs and local
anesthetics for the same patient. This approach will potentiate the analgesic effects
and allow smaller doses of each drug to be used, thus reducing side effects. [Anesth
Analg 1993; 77:1048-1056]
For example, NSAIDs act peripherally by reducing prostaglandins but opioids act
centrally on opioid receptors. Furthermore, side effects of both drugs are completely
different. Thus NSAIDs and opioids can be given together in the multimodal
approach. Sometimes we may give one drug regularly while the other is given PRN,
eg, regular NSAIDs with prn opioids if the pain is not relieved with NSAIDs alone.
Another important point in treating acute pain is to inform the patient about the
"natural history" of the injury and when he/she can expect the pain to diminish
without analgesics. For example, for muscle strain or sprain, the pain should diminish
after 2 to 3 days; if it does not, the patient should return to the doctor who can then
assess if anything further needs to be done.
Chronic pain
Definition: Although chronic pain is classified as pain that lasts 3 to 6 months, this is
an arbitrary duration. Basically, chronic pain is pain that persists beyond the healing
period (ie, once the tissues have healed). Chronic pain may be nociceptive,
neuropathic, or mixed nociceptive-neuropathic. In many types of chronic pain, it is
not possible to eliminate the pain completely and therefore the approach to this
problem must be to teach the patient to manage the pain rather than to focus on
relieving the pain.
When assessing patients with chronic pain, it is very important to determine the type
of their pain as medications used for nociceptive pain and neuropathic pain are very
different. We also need to assess the impact of pain on the patient's life, as chronic
pain is something that can consume patients and affect not only them but also their
family and friends.
Patient assessment
In assessing patients with chronic pain, history is the most important factor, with
physical examination providing confirmation of the diagnosis; investigations may also
be helpful in eliciting the underlying cause of the pain, eg, diabetes mellitus in a
patient who presents with painful peripheral neuropathy.
Red flags that indicate tumors, infection and neurological deficit, need to be ruled out
and “yellow flags” that indicate psychosocial risk factors should also be looked for. If
any red flags are found, the patient must be referred to the appropriate specialist.
Examples of red flags in patients with low back pain are: age of presentation below 20
years or above 55 years; trauma; constant progressive, non-mechanical pain; previous
history of cancer; steroid use; limited lumbar flexion; weight loss and constitutional
symptoms; widespread neurological deficit; cauda equina syndrome and structural
deformity.
Yellow flags are psychological factors that increase the risk of developing long
term disability. For back pain, yellow flags include the belief that back pain is
harmful and is potentially severely disabling and the fear of becoming paralyzed
in the future. Patients with yellow flags are at higher risk of developing chronic
pain related disability unless these factors are appropriately addressed.
During history taking, a detailed description of the pain will help the doctor to make a
diagnosis. Important questions include asking how the pain started, how long the pain
has lasted, how frequent the episodes of pain are, where the pain is and where it goes,
what the pain feels like ie, pricking, burning, cramping, shooting. Neuropathic pain is
usually burning and shooting or lancinating and nociceptive pain may be cramping,
pricking or sharp.
Patients should be asked to score their pain when they are at rest and during
movement. There are many pain scales available today. A simple scale that can be
used is the Numerical Rating Scale (NRS) where the pain score ranges from 0 (no
pain at all) to 10 (worst pain imaginable). Once patients understand the concept of
pain score, it is easier to assess their level of pain and to monitor their progress after
treatment.
Some doctors use a body chart, which is useful for patients to indicate where they feel
the pain. Sometimes this helps to indicate the level of distress of the patient, for
example if the patient puts crosses or lines all over the body, (“pain all over”) it
usually means that the patient is greatly distressed and that psychosocial factors need
to be addressed as well.
During assessment, the Pain Self Management Checklist devised by Dr. Michael
Nicholas, a clinical psychologist at the Royal North Shore Hospital in Sydney, is
useful. If patients score very high on the questionnaire, they are probably at high risk
of becoming chronic pain sufferers and need help.
Another useful questionnaire is the Orebro Musculoskeletal Pain Screening
Questionnaire (OMPSQ) from Steven Linton in Sweden. This is used to screen
for yellow flags and is reliable. [Clin J Pain 2003; 19:80-86].
P-3 Pain Patient ProfileThe Pain Patient Profile (P-3) assessment, a test from Pearson Assessments, focuses
on the factors most frequently associated with chronic pain. The test can help provide
an objective link between the physician's observations and the possible need for
further psychological assessment.
How to Use This Test
A variety of medical professionals, including anesthesiologists, general practitioners,
rehabilitation specialists, chiropractors, surgeons, neurologists, and nurses can use the
P-3 test to help:
Identify the psychological roadblocks to patient recovery
Assess, document, and justify the need for further psychological evaluation
Facilitate physician-psychologist communication
Evaluate the patient's emotional readiness for surgery
Support evaluations for cases involving vocational readiness; orthopedic,
occupational, and auto injuries; workers' compensation; and long-term
disabilities
Easily and inexpensively measure pre- and post-treatment pain status to
evaluate treatment effectiveness and monitor clinical outcomes
Key Features
The test can help save time and money and reduce frustration for both patient and
medical providers by identifying psychological factors that may be preventing the
patient from reaching a successful medical outcome.
The test report includes an easy-to-understand summary of results to share with
the patient.
Requiring only 12-15 minutes to administer, the test can be easily administered as
part of an initial clinical evaluation.
The test was normed using both pain patients and subjects from the community.
This cross-validating approach helps assure that results are more relevant to pain
patients than more traditional assessments may be.
Quick Facts
Administer To Individuals 17–76 years old
Reading Level 8th grade
Items 44 groups of statements with three statements per group
Formats Paper-and-pencil or computer administration
Report Options Interpretive Report, Progress Report
Scoring Options
Q™ Local Software
Hand Scoring
Mail-in Scoring Service
Fax-in Service
PAD (Patient Assessment Device) Hand-held Electronic Device
Optical Scan Scoring
Scales Somatization, Depression, Anxiety and Validity Index
Norms Pain Patients and Community Samples
Padua inventoryBehav Res Ther. 1990;28(4):341-5.
Obsessions and compulsions: psychometric properties of the Padua Inventory
with an American college population.
Sternberger LG, Burns GL.
The psychometric properties of the Padua inventory, a self-report measure of
obsessive-compulsive behaviors, were examined in a sample of 678 American college
students. Results showed good internal consistency as well as convergent and
divergent validity with the subscales of the Symptom Checklist-90 Revised and the
Maudsley Obsessional-Compulsive Inventory. A principal components analysis
suggested a four factor solution (i.e. 'impaired control of mental activities', 'checking',
'urges and worries of losing control of motor behaviors', and 'being contaminated').
The factor structure was very similar to that found in the original Italian study of the
inventory. Suggestions are made for the use of the Padua Inventory in the study of
obsessions and compulsions in nonclinical samples.
Piers-Harris 2, Piers Harris Children’s Self Concept ScaleThe updated Second Edition of the Piers-Harris Children’s Self-Concept Scale,
one of the most widely used measures of psychological health in children and
adolescents, quickly identifies youngsters who need further testing or treatment.
Comprises a total Score and Six Subscale Scores
Based on the child’s own perceptions rather than the observations of parents or
teachers, the Piers-Harris 2 assesses self-concept in individuals ages 7 to 18. It is
composed of 60 items covering six subscales:
Physical Appearance and Attributes , Intellectual and School Status, Happiness and
satisfaction, Freedom from Anxiety, Behavioral Adjustment, Popularity.
In addition, two validity scales identify biased responding and the tendency to answer
randomly. Test items are simple descriptive statements, written at a second-grade
reading level. Children indicate whether each item applies to them by selecting a yes
or no response. This usually requires just 10 to 15 minutes. (A Spanish Test Booklet is
available for children who read Spanish only.)
The Piers-Harris 2 provides a Total Score that reflects overall self-concept, plus
subscale scores that permit more detailed interpretation. Nationally representative
norms are based on a sample of nearly 1,400 students, ages 7 to 18, recruited from
school districts throughout the U.S. Because the scales remain psychometrically
equivalent to those on the First Edition, results from the Piers-Harris 2 can be
compared, for research or clinical purposes, to those obtained using the original test.
Classroom or Clinical Screening: The Piers-Harris 2 is widely used in both schools
and clinics. It is often administered as routine classroom screening, to identify
children who might benefit from further evaluation. And it is commonly used in
clinical settings to determine specific areas of conflict, typical coping and defense
mechanisms, and appropriate intervention techniques. It is an ideal choice when you
need a quick but comprehensive measure of self-concept in children or adolescents.
Post-Traumatic Stress Diagnostic ScaleThe Posttraumatic Stress Diagnostic Scale (PDS) is a 49 item paper and pencil or on-
line, self-report instrument that is designed to assist with the diagnosis of Post
Traumatic Stress Disorder (PTSD). The PDS is based on the DSM-IV (American
Psychiatric Association, 1994) diagnostic criteria for PTSD. The PDS takes 10-15
minutes to complete and 5 minutes to hand score (Axford, 1999).
The PDS was developed to provide a brief self-report instrument to assist with the
diagnosis of PTSD and it provides a means of quantifying the severity of PTSD
symptoms. It is not intended to replace the structured diagnostic interview (Doll,
1999). The PDS has been validated on a clinical population aged 18 to 65 years.
Nevertheless, clinical judgment may be used in deciding whether to use PDS on
individuals falling outside this age range. However, the PDS is not designed to be
administered to children as the DSM-IV (American Psychiatric Association, 1994)
criteria for PTSD in children are not represented in the PDS. The PDS manual
recommends that the PDS should be used with at least eighth-grade reading level
ability.
The PDS generates judgments on whether the DSM-IV (American Psychiatric
Association, 1994) six diagnostic criteria for PTSD have been met, the level of
impairment and a symptoms severity score.
Personality Assessment InventoryThe PAI is a self-administered, objective inventory of adult personality and
psychopathology. The PAI contains 344 items comprising 22 nonoverlapping full
scales: validity scales, clinical scales, 5 treatment scales and 2 interpersonal scales
(Morey 1991). The PAI has been developed in several computerised forms and can
be used in a shortened form.
The PAI measures manifestation of clinical syndromes which were selected based
upon their historical importance in classification of mental disorder and their
significance in contemporary diagnostic practice (Morey 1991). The PAI provides
information to assist diagnosis, treatment and screening for psychopathology which
parallels DSM-IV categories.
Clinical scales are clustered in Neurotic, Psychotic, Personality Disorders and
Behavioural Disorders. In addition to measurement of clinical constructs,
interpretation of results also provides measures for detecting Malingering; evaluating
potential for Aggression and Suicide; and motivation for Treatment.
The development of the scale used a cluster analysis rather than a two point code type
so that scales would be useful across a number of different applications. Profile
interpretation can be made as a two-point code but the author warns against this
method of assessment, “...the reliability of the small differences that can determine a
two-point code on any psychological instrument is often suspect” (Morey 1996).
The PAI requires a Grade 6 reading level and takes about 40-50 minutes to complete.
The four choice per answer, from False to Very True reduces resistance to forced
choice. Low functioning clients may experience difficulties. It is not designed to
provide a comprehensive assessment of normal personality.
Rey Auditory Verbal Learning Test (RAVLT)
The Auditory Verbal Learning Test was developed by André Rey and first published
in France in the 1960’s. The list learning format that it utilises has become virtually
the standard for verbal learning tests as can be readily seen when examining the
California Verbal Learning Test, WMS-III Word Lists Test, and Hopkins Verbal
Learning Test. With, perhaps, the exception of the Hopkins, the RAVLT probably has
the largest number of published alternate forms (unfortunately there is little to no
normative data for these versions).
The standard administration format of the RAVLT consists of reading a list of 15
words aloud to the client. While a number of variant procedures exist, these tend to
relate to whether or not a delayed recall trial is administered, and the type of
recognition test used. The format presented here will be for the form I have
standardised in Australia and is used in your assignments.
There are 8 recall trials and a recognition test. The first five trials (I through V) are
termed the learning trials and involve the repeated reading of the test list (sometimes
called List A) followed by free recall of this list by the client. This first trial (I) is
often viewed as a measure of immediate memory and some clinicians have proposed
comparing it to other immediate memory tasks such as Digit Span – Forward. This
sort of comparison can certainly be interesting but the differences between RAVLT I
and DS-F are just as great as their similarities. For example, RAVLT I is a supra-span
task (i.e. the number of words is well in excess of the average person’s immediate
memory span) while DS-F is an incremental measure of immediate memory span,
with more than one trial at each span level. Trials II through V are administered in the
same way, first reading the list and then asking the client to recall as many words as
they can in any order. The next trial is commonly referred to as the interference trial
in which a new list (List B) is read aloud to the client and free recall is requested. This
is essentially a poor man’s measure of proactive interference – the degree to which
old learning can interfere with new learning. Trial VI immediately follows in which
the client is asked to recall as many words as they can from the first List (A). This
recall is conducted WITHOUT reading List A again. As with the interfernece taks,
this simulates a retroactive interference situation where new learning interferes with
the recall of old information. The degree to which these constructs (proactive vs.
retroactive interference) are relevant to clinical testing of memory AND the degree to
which these trials are a valid measure of these constructs, is still a matter for debate.
Trial VII is administered in the same way as trial VI (i.e. no reading of List A) but
following a 20-minute delay, which is characteristically not filled with other verbal or
memory tests.
Rey Complex Figure TestPurpose - Measure visuospatial ability and visuospatial memory
Age range – Child, Adolescent, Adult, Elder Adult
Administration – individual
Time – approx 45mins including 30 min delay interval (timed)
Assess - executive functioning
The RCFT standardizes the materials and procedures for administering the Rey
complex figure. The Recognition trial measures recognition memory for the elements
of the Rey complex figure and assesses the respondent's ability to use cues to retrieve
information.
RCFT Materials: The RCFT materials include the 120-page Professional Manual,
Manual Supplement with data for children and adolescents, the laminated RCFT
Stimulus Card, and the 16-page RCFT Test Booklet. A stopwatch is required for
administration.
The manual provides information on the development of the RCFT materials,
administration and scoring procedures with scoring examples, demographically
corrected normative data, guidelines for interpretation with case illustrations, and
reliability and validity data.
The 8.5" x 11" Stimulus Card contains a computer-rendered replica of the original
Rey complex figure. Prior to this publication, Rey's original figure has not been
available commercially.
The Test Booklet provides all forms necessary to administer and score the RCFT.
Pages for the three freehand drawing trials (Copy, Immediate Recall, and Delayed
Recall) and the Recognition trial are perforated for easy detachment.
Scoring and Interpretation: The RCFT provides an objective and standardized
approach to scoring drawings based on the widely used 36-point scoring system. The
same scoring criteria apply to all three drawing trials. Each of the 18 scoring units is
scored based on accuracy and placement criteria. Unit scores range from two
(accurately drawn, correctly placed) to zero (inaccurately drawn, incorrectly placed,
unrecognizable, omitted).
Normative Data: The normative sample included 601 adults ages 18-89 years and
505 children and adolescents ages 6-17 years. Demographically corrected normative
data for the RCFT copy and memory variables are presented to assist in interpretation
as well as in making comparisons among individuals and various patient groups.
Validity: Intercorrelations between the RCFT and other measures, in samples of both
normal and brain-damaged subjects, establish the convergent and discriminant
validity of the RCFT as a measure of visuospatial constructional ability (Copy trial)
and visuospatial memory (Immediate Recall, Delayed Recall, and Recognition trials).
Results of factor analysis suggest the RCFT captures five domains of
neuropsychological functioning: visuospatial recall memory, visuospatial recognition
memory, response bias, processing speed, and visuospatial constructional ability. It
reliably discriminates among brain-damaged, psychiatric, and normal subjects. In
addition, the Recognition trial provides incremental diagnostic power compared to
using recall trials alone
Reynolds Adolescent Depression ScaleThe RADS-2 is a brief, 30-item self-report measure that includes subscales which
evaluate the current level of an adolescent's depressive symptomatology along four
basic dimensions of depression: Dysphoric Mood, Anhedonia/Negative Affect,
Negative Self-Evaluation, and Somatic Complaints. Interpretation of these four
subscales is based on both the nature of the depression domain and the item content of
the subscale.
The RADS-2 standard (T) scores and associated clinical cutoff score provide the
clinician or researcher with an indication of the clinical severity of the individual's
depressive symptoms (normal, mild, moderate, or severe). Scores are plotted on a
Summary/Profile Form, allowing comparison of elevations across subscales.
Examining item endorsement levels within elevated subscales can provide further
information about the nature of an adolescent's reported symptomatology.
In addition to the four subscale scores, the RADS-2 yields a Depression Total score
that represents the overall severity of depressive symptomatology. An empirically
derived clinical cutoff score helps to identify adolescents who may be at risk for a
depressive disorder or a related disorder. Data demonstrate the ability of this cutoff
score to discriminate between adolescents with Major Depressive Disorder and an
age- and gender-matched control group. The six RADS-2 critical items alert clinicians
that an adolescent (with a Depression Total score below the clinical cutoff) may be
experiencing a significant level of depression
Reynolds Child Depression ScalePurpose - Screen for depressive symptoms in children
Age range - Child
Administration – individual or group
Time – 10 mins
The RCDS was developed to screen for depression in children and can be
used in schools or in clinical settings (grades 3-6). It provides school and
mental health professionals with a straightforward, easily administered
measure for the evaluation of the severity of children's depressive symptoms.
The RCDS can also be used in research on depression and related
constructs.
Written at a 2nd-grade level (items are read aloud to assist students in Grades
3 and 4).
30 items are rated on a 4-point scale.
Hand-Scorable for individual or group administration.
Reliability coefficients range from .87-.91.
Total sample alpha reliability of .90 and split-half reliability of .89.
Validity consistently demonstrated in field testing since 1981
RCMAS The RCMAS (“What I Think and Feel” ) is a 37-item self-report inventory used to
measure anxiety in children, for clinical purposes (diagnosis and treatment
evaluation), educational settings, and for research purposes. The RCMAS consists of
28 Anxiety items and 9 Lie (social desirability) items. Each item is purported to
embody a feeling or action that reflects an aspect of anxiety, hence the subtitle, “What
I think and Feel”. It is a relatively brief instrument, which has been subjected to
extensive study to ensure that it is psychometrically sound. However, it is also
advisable that the RCMAS only be used as part of a complete clinical evaluation
when diagnosing and treating a child’s anxiety (Gerard and Reynolds, 1999, p.323).
The Revised Children’s Manifest Anxiety Scale was developed by Reynolds and
Richmond (1978) to assess “the degree and quality of anxiety experienced by children
and adolescents” (Gerald and Reynolds, 1999, p. 323). It is based on the Children’s
Manifest Anxiety Scale (CMAS), which was devised by Casteneda, McCandless and
Palermo (1956). The Revised version of the CMAS deletes, adds and reorders items
from the CMAS to meet psychometric standards. Reynolds and Richmond (1978) also
renamed the instrument, “What I Think and Feel”, although subsequent papers
primarily refer to it as the Revised Children’s Manifest Anxiety Scale (RCMAS).
Rohde Sentence Completion Method(nothing found)
Rorschach Inkblot TestThe Rorschach inkblot test is a psychological projective test of personality in which a
subject's interpretations of ten standard abstract designs are analyzed as a measure of
emotional and intellectual functioning and integration. The test is named after
Hermann Rorschach (1884-1922) who developed the inkblots, although he did not use
them for personality analysis.
The test is considered "projective" because the patient is supposed to project his or her
real personality into the inkblot via the interpretation. The inkblots are purportedly
ambiguous, structureless entities which are to be given a clear structure by the
interpreter. Those who believe in the efficacy of such tests think that they are a way of
getting into the deepest recesses of the patient's psyche or subconscious mind. Those
who give such tests believe themselves to be experts at interpreting their patients'
interpretations.
SCL-90-RThe Symptom Checklist-90-R (SCL-90-R) instrument from Pearson Assessments
helps evaluate a broad range of psychological problems and symptoms of
psychopathology. The instrument is also useful in measuring patient progress or
treatment outcomes.
The SCL-90-R instrument is used by clinical psychologists, psychiatrists, and
professionals in mental health, medical, and educational settings as well as for
research purposes. It can be useful in:
Initial evaluation of patients at intake as an objective method for symptom assessment
Measuring patient progress during and after treatment to monitor change
Outcomes measurement for treatment programs and providers through aggregated
patient information
Clinical trials to help measure the changes in symptoms such as depression and
anxiety
Quick Facts
Administer To Individuals 13 years and older
Reading Level 6th grade
Completion
Time12-15 minutes (90 items, 5-point rating scale)
Formats Paper-and-pencil, audiocassette, or computer administration
Report
OptionsInterpretive, Profile, and Progress
Scoring
Options
Q Local™ Software
Mail-in Scoring Service
Hand Scoring
Optical Scan Scoring
Scales9 Primary Symptom Dimensions
3 Global Indices
NormsAdult nonpatients, Adult psychiatric outpatients, Adult psychiatric
inpatients, Adolescent nonpatients
SCOLP
The Speed and Capacity of Language-Processing Test (SCOLP)Alan Baddeley, Ph.D., Hazel Emslie and Ian Nimmo-Smith
Description
This test is sensitive to slowing of
language and cognitive functioning
that often occurs following brain
damage. The SCOLP is composed of
two brief tests, Speed of
Comprehension Test and Spot-the-
Word Vocabulary Test.
The first test asks the client to answer
as many simple true/false questions
about the world as he/she can in a two
minute period. This test is sensitive to the effects of closed head injury, normal
aging, Alzheimer's Disease, schizophrenia and alcohol related disorders.
The second test assesses verbal capacity in order to help interpret results obtained
from the first test. Norms are provided for patients 16 to 65 for both tests.
Test results can help identify the discrepancy between comprehension speed and
vocabulary and the extent of cognitive impairment. Administration time is 6 minutes.
This test is intended for use only by OT, SLP and Psychologists
Self-Directed SearchThe Self-Directed Search (SDS) is the most widely used career interest inventory in
the world, having helped more than 14 million people with career planning decisions.
The SDS is an easy-to-use, self-administered test that helps individuals find
occupations that best suit their interests and skills.
Applications
Assist students and adults with career exploration
Educational and career planning
The SDS was designed to assist students and adults with career exploration and
educational and career planning. Individuals answer questions about their aspirations,
activities, competencies, occupations, and other self-estimates and discover
occupations that best fit their interest skills.
Based upon the Holland "RIASEC" theory that people are most satisfied in work
environments that reinforce their personalities, the SDS categorizes people as one of
six (6) personality types: Realistic, Investigative, Artistic, Social, Enterprising or
Conventional.
SIQPurpose – screen for suicidal ideation in adolescents
Age range – adolescent
Administration – individual or group
Time – 10 mins or less
The Suicidal Ideation Questionnaire assesses the frequency of suicidal thoughts in
adolescents and may be used to evaluate or monitor troubled youths. Because not all
depressed adolescents are suicidal and not all suicidal adolescents are depressed, the
SIQ is a valuable component in a comprehensive assessment of adolescent mental
health.
Items rated on a 7-point scale.
Hand-Scorable for individual or small group administration.
Grades 10-12 (SIQ); Grades 7-9 (SIQ-JR).
Use to evaluate large-scale intervention/prevention programs.
Reliability coefficients are .97 for the SIQ; .93-.94 for the SIQ-JR.
Validity consistently supported in many published content, construct, and clinical
studies
ASIQ
Purpose: Screen for suicidal ideation in college students and adults
Age range: adult, elder adult
Administration: individual / group
Time: 10 mins
The ASIQ can be used during intake interviews or during treatment to reduce liability
and take appropriate preventive action whenever there may be a risk of suicide.
Endorsement of critical items alerts you immediately in case of serious suicidal
ideation.
The ASIQ includes a 25-item self-report; items rated on a 7-point scale; and a built-in
scoring key. Norms are based on 2,000 adults ages 18 years and older, including
psychiatric outpatients, normal adults, and college students.
Internal consistency and test-retest reliability coefficients range from .96-.97
and .85-.95, respectively, in various samples.
The ASIQ yields a total score with a corresponding T score and percentile score.
Comparing the total score to a cutoff allows you to identify individuals in need of
further evaluation for suicide risk.
Results of several research studies support the ASIQ as a valid measure of suicidal
ideation.
Social Skills Training: Enhancing Social Competence with Children and AdolescentsSocial Skills Training is a comprehensive, up-to-date resource that helps you assess
the social competence of young people and design appropriate individual intervention
programmes. The programme aims in particular to change negative thinking patterns
and develop self-esteem.
Purpose
Measures social skills problems and helps design appropriate intervention
programmes to enhance young people’s social competence.
Benefits
Accessible and open, designed to put students and their parents at ease
Versatile – can be used as broad guidelines for practitioners who wish to tailor unique
programmes, or as a 16-session programme in its own right.
Informative – gives a detailed overview of the whole area of social skills.
Contents
Complete Set contains:
User’s Guide
Photocopiable Resource Book
Eight Photo CardsResearch and Technical Supplement.
South Australian Spelling TestThis is a test of real word spelling which has been standardised across the
age range 6-15 years. The revised norms for this simple spelling test provide
estimates of spelling age based on a sample of South Australian students
tested in 1993. This test assesses spelling performance from age 6 to over 15
years. It is popular because it has Australian norms however in some places it
may be over-used and some children are developing familiarity with the test
STAXIThe STAXI was developed with two goals in mind. The first was to develop a
measure of the components of anger in the context of both normal and abnormal
personality. The second goal seems rather more specific to a particular research
orientation - in this case examining the contribution of anger to the development or
exacerbation of medical conditions such as hypertension, coronary heart disease, and
cancer.
There are two fundamental aspects of anger which are addressed - the experience of
anger, and the expression of anger. The experience of anger can be understood in the
context of state - subjective feelings that vary from irritability to intense rage, and trait
anger which refers to a disposition to perceive situations as annoying and to respond
to these situations by more frequent expressions of state anger. Thus state and trait
anger are unlikely to actually be independent characteristics or components of anger.
When expressing anger, it may be focused outward on other people or objects (Anger-
Out), or directed inward (Anger-In). A third component is the degree to which people
attempt to control their expression of anger (Anger Control).
The STAXI is designed to be administered to people aged 13 through adulthood with
a minimum fifth grade reading level. The task of administering the test is
straightforward, essentially self-administered, but interpretation of test scores requires
formal training in assessment. There are no time limits imposed on completing the
STAXI, but it is a brief test and most people complete it within 15 minutes.
STAXI Scales: The STAXI consists of 44 items which are distributed across the five
main scales. Consistent with the conceptualisation of anger above there are three main
aspects to the STAXI scales: State, Trait, and Anger Expression. Trait contains two
subscales that examine different dispositions in trait anger - temperament and
reaction. Anger Expression is actually an experimental composite of the three
expression constructs -In, Out, and Control.
STATE TRAIT ANGER EXPRESSION
(S-Anger) (T-Anger) (AX/EX)
Angry Temperament Anger-In (AX/In)
(T-Anger/T) Anger-Out (AX/Out)
Angry Reaction Anger Control (AX/Con)
(T-Anger/R)
S-Anger - This is a 10-item stand-alone scale which measures the respondent's
current feelings of anger.
T-Anger - This scale also contains 10 items which asks the respondent to answer
questions about his or her disposition towards anger.
T-Anger/T - is a subscale of T-Anger consisting of 4 items that generally
address the disposition to express anger without provocation.
T-Anger/R - is a subscale of T-Anger also consisting of 4 items that ask about
the respondent's disposition to express anger when provoked.
AX/In - this 8 item scale measures the frequency with which the respondent holds in
or suppresses his or her anger.
AX/Out - this 8 item scale measures the frequency with which the respondent
expresses her anger to other people or objects.
AX/Con - another 8 item scale that attempts to measure the degree to which the
respondent attempts to control his or her expression of anger.
AX/EX - this is an experimental composite score that is designed to represent the
combination of AX/In, AX/Out, and AX/Con and essentially examines the overall
frequency of anger expression. AX/EX is computed with the following formula:
AX/EX = AX/Out + AX/In - AX/Con +16.
The addition of 16 at the end may seem unusual but it is designed to ensure that a
negative score cannot be achieved. Since the four possible responses to each item are
assigned a number between 1 and 4 and each of the AX scales has 8 questions, the
minimum total for each scale is 8, and the maximum score is 32. The lowest possible
score would be minimum In and Out and maximum Con which would be 8+8-32 = -
16. Adding 16 to this total would give 0. Similarly if Out and In were at maximum
and Con was at minimum the total would be 32+32-8+16 = 72. For this reason the
raw score range for AX/EX is 0 to 72.
All items are rated on a four-point scale and are assigned a score of between 1 and 4.
Raw score totals are converted to percentile ranks and T-scores using normative
tables. There are separate normative tables for males and female adolescents, adults,
and college students.
STAXI-2The State-Trait Anger Expression Inventory-2 (STAXI-2) is a 57-item inventory
which measures the intensity of anger as an emotional state (State Anger) and the
disposition to experience angry feelings as a personality trait (Trait Anger). The
instrument consists of six scales measuring the intensity of anger and the disposition
to experience angry feelings. Items consist of 4-point scales that assess intensity of
anger at a particular moment and the frequency of anger experience, expression, and
control.
Applications
Assess components of anger in the context of normal personality and
psychopathology.
Evaluate the contributions of the various components of anger to the etiology and
progression of medical conditions, particularly hypertension, coronary heart disease,
and cancer.
The STAXI-2 State Anger scale assesses the intensity of anger as an emotional state
at a particular time. The Trait Anger scale measures how often angry feelings are
experienced over time. The Anger Expression and Anger Control scales assess four
relatively independent anger-related traits:
(a) expression of anger toward other persons or objects in the environment (Anger
Expression-Out);
(b) holding in or suppressing angry feelings (Anger Expression-In);
(c) controlling angry feelings by preventing the expression of anger toward other
persons or objects in the environment (Anger Control-Out);
(d) controlling suppressed angry feelings by calming down or cooling off (Anger
Control-In).
Individuals rate themselves on 4-point scales that assess both the intensity of their
anger at a particular time and the frequency that anger is experienced, expressed, and
controlled
STROOP TESTThe Stroop Task is a psychological test of our mental vitality and flexibility. The task
takes advantage of our ability to read words more quickly and automatically than we
can name colors. If a word is printed or displayed in a color different from the color it
actually names; for example, if the word "green" is written in blue ink (as shown in
the figure to the left) we will say the word "green" more readily than we can name the
color in which it is displayed, which in this case is "blue."
The cognitive mechanism involved in this task is called inhibition, you have to inhibit
or stop one response and say or do something else.
SYMBOL DIGIT MODALITIES TEST (SDMT)PURPOSE: Screen for organic cerebral dysfunction in both children and adults
ADMINISTER TO:
Children 8-17 years;
adults 18-78 years
ADMINISTRATION TIME: 20 minutes (107 items)
Brief and easy to administer, the SDMT has demonstrated remarkable sensitivity in
detecting not only the presence of brain damage, but also changes in cognitive
functioning over time and in response to treatment. It is an economical way to screen
apparently normal children and adults for possible motor, visual, learning, or other
cerebral dysfunction.
The SDMT involves a simple substitution task. Using a reference key, the examinee
has 90 seconds to pair specific numbers with given geometric figures. Because
examinees can give either written or spoken responses, the test is well suited for use
with individuals who have motor disabilities or speech disorders. Because it involves
only geometric figures and numbers, the SDMT is relatively culture free as well and
can be administered to individuals who do not speak English. The SDMT AutoScore
Test Form simplifies scoring
The SDMT is effective in a wide range of clinical applications including
differentiation of brain-damaged from psychotic patients; differentiation of organics
from depressives; early detection of senile dementia and Huntington’s disease;
differential diagnosis of children with learning disorders; early identification of
children likely to have reading problems; assessment of change in cognitive
functioning over time and/or with therapy in individuals who have traumatic vascular,
neoplastic, and other brain insults; and assessment of recovery from closed-head
injury
Thematic Apperception TestThe 31 picture cards included in the TAT are used to stimulate stories or descriptions
about relationships or social situations and can help identify dominant drives,
emotions, sentiments, conflicts and complexes.
Key Features
The test can be administered individually, to groups, or self-administered.
Individuals can respond orally or in writing.
Cards include specific subsets for boys, girls, men, and women.
Quick Facts
Qualification
LevelA
Administer To Individuals 10 years and older
Completion TimeVariable (31 picture cards/2 series of 10 cards for boys, girls,
men and women)
Formats Individuals react (orally or in writing) to a series of picture cards
Scoring Option Hand Scoring
TRAIL MAKING TESTThe test consists of two parts, A and B, and since it is a test of speed, the examiner
should stress the importance of time and efficiency. Part A consists of encircled
numbers from 1 to 25 randomly spread across a sheet of paper. The object of the test
is for the subject to connect the numbers in order, beginning with 1 and ending with
25, in as little time as possible.
Part B is more complex than A because it requires the subject to connect numbers and
letters in an alternating pattern (1-A-2-B-3-C, etc.) in as little time as possible.
Because Part B requires more thought processing and attention on behalf of the
subject, it takes longer to complete the test; however, if one works on Part B for more
than two or three minutes, one will become frustrated, and the frustration may
influence performance on other tests (Bradford, 46).
Normally, the entire test can be completed in 5 to 10 minutes. Scores are calculated by
adding the time it takes for the subject to complete Part A with the time it takes to
complete Part B, so it is extremely important for one to understand the directions fully
before the pencil touches the paper and time begins.
If an error is made, the examiner will point it out to the patient for correction and
have them return to and continue from the correct location while the clock remains
running. Errors are recorded and the patient continues with the test. Cutoff scores for
impairment are based on normative data instead of earlier recorded scores suggested
by Matarazzo because there are other factors which may play a role in an individual's
score (ex: age, educational level).
TRAUMA SYMPTOM INVENTORYThe Trauma Symptom Inventory (TSI) is a test containing 100 items claiming to
measure ‘posttraumatic stress and other psychological sequelae of traumatic events’.
It was devised to be used in the assessment of ‘acute and chronic traumatic
symptomatology’, such as rape, physical assault, spouse abuse, major accidents,
combat trauma, natural disasters and the enduring effects of childhood abuse and early
childhood trauma (Briere, 1995).
The TSI has 3 validity scales and 10 clinical scales that assess a broad range of
psychological symptoms including those related to Posttraumatic Stress Disorder
(PTSD) and Acute Stress Disorder (ASD) plus intra and interpersonal difficulties
associated with chronic psychological trauma. The test is self-administered and is
intended for a fifth grade and above reading level (Briere 1995). Items are scored on a
four point scale with 0 = Never through to 3 = Often, and are rated in terms of
frequency of occurrence over the previous six months. Due to this time frame the TSI
was ‘not intended to generate a DSM IV PTSD diagnosis’. The TSI takes
approximately 20 minutes to complete and around 15 minutes to score (Briere and
Elliott, 1997).
Validity scales: Response level (RL); Atypical Response (ATR); Inconsistent
Response (INC)
Clinical Scales: Anxious Arousal (AA); Depression (D); Anger/Irritability (AI);
Intrusive Experiences (IE); Defensive Avoidance (DA); Dissociation (DIS); Sexual
Concerns (SC); Dysfunctional Sexual Behaviour (DSB); Impaired Self-Reference
(ISR); Tension Reduction Behaviour (TRB)
WAIS-RWechsler Adult Intelligence Scale (WAIS) – intelligence test for individuals 16 years
and over
The WAIS(R) was standardised on a sample of 1,800 U.S. subjects, ranging from 16
to 74 years of age. It was a highly stratified sample, broken down into 9 different age
groups. Equal numbers of men and women were used, as were white and nonwhite
subjects, in line with census figures. It was further broken down into four geographic
U.S. regions and six occupational categories. There was also an attempt to balance
urban and rural subjects. The mean I.Q. for each age group on this test is 100, with a
standard deviation of 15. The WAIS scales have impressive reliability and validity.
There are different adaptations of the scale by country. For example, in Australia we
have the Australian adaptation of the WAIS-R (1989). 11 separate subtests, which are
broken into the Verbal scale (6 subtests) and the Performance scale (5 subtests). A
person taking the test receives a full-scale IQ score, a verbal IQ score, a performance
IQ score, as well as scaled scores on each of the subtests.
Verbal WAIS scales
Information: 29 questions - a measure of general knowledge.
Digit Span: Subjects are given sets of digits to repeat initially forwards then
backwards. This is a test of immediate auditory recall and freedom from distraction.
Vocabulary: Define 35 words. A measure of expressive word knowledge. It
correlates very highly with Full Scale IQ
Arithmetic: 14 mental arithmetic brief story type problems. tests distractibility as
well as numerical reasoning.
Comprehension: 16 questions which focus on issues of social awareness.
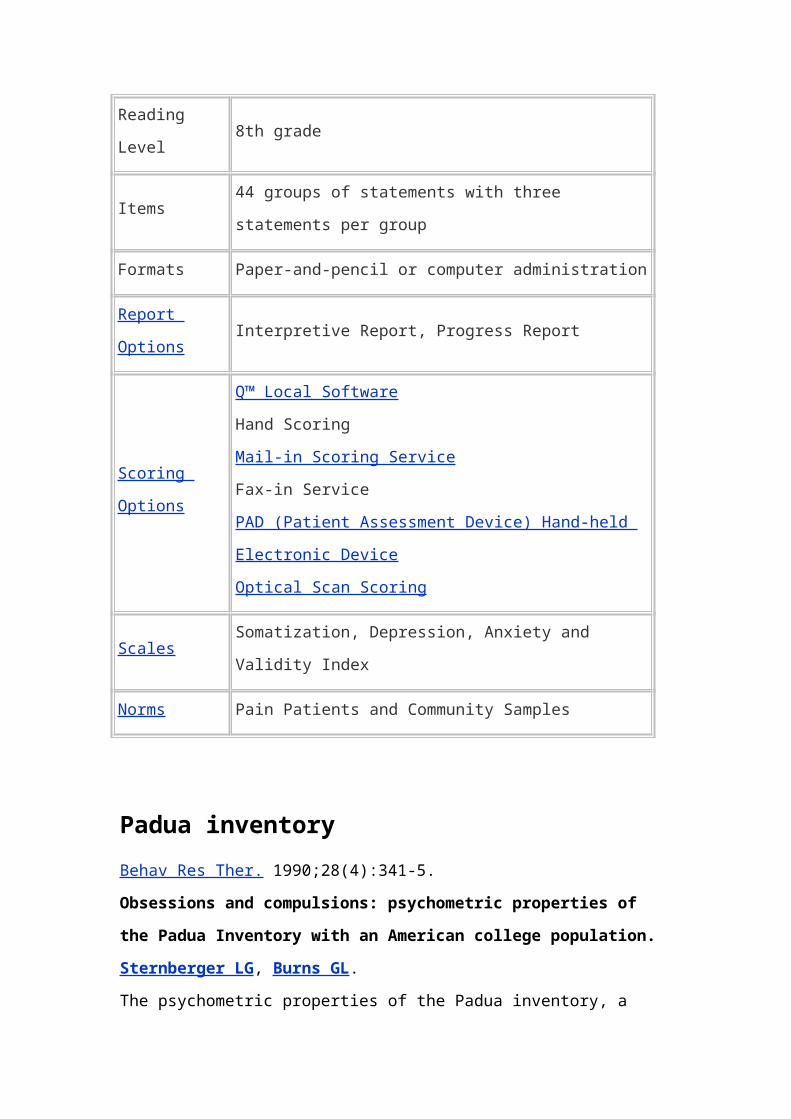
Similarities: A measure of concept formation. Subjects are asked to say how two
seemingly dissimilar items might in fact be similar.
Performance WAIS scales
Picture Completion: 20 small pictures that all have one vital detail missing. A test of
attention to fine detail.
Picture Arrangement: 10 sets of small pictures, where the subject is required to
arrange them into a logical sequence.
Block Design: Involves putting sets of blocks together to match patterns
on cards.
Digit Symbol: Involves copying a coding pattern.
Object Assembly: Four small jig-saw type puzzles.
Three IQ scores are obtained from the WAIS(R):
1. Verbal IQ
2. Performance IQ
3. Full Scale IQ
Interpretation is fairly systematic and can be broken down into a number of discrete
steps:
1. Obtain the 3 IQ scores. What standardized categories do they fall into?
2. Is there a Verbal-Performance discrepancy? Is it significant?
3. Break WAIS scores down into the factorial sub-structure:
(a) Verbal Comprehension
(b) Spatial Perceptual
(c) Freedom from Distraction
Are individual sub-tests very low or very high? Why?
What is the degree of intra-subtest scatter?
The WAIS-R gives a global IQ and also two separate IQ’s for the two scales: verbal
and performance. There are 6 verbal subscales and 5 performance subscales.
Wechsler believes that this test is a good measure of “g”. The two scales can be used
separately to see if a person has particular strengths or weaknesses. Wechsler suggests
that if there is more than 15 IQ points difference between the two main scales then
this might be cause for further investigation. The design of the test, with the two
scales, means that the verbal & performance scales can be used alone. The
Performance section alone can be used with examinees who are unable to properly
comprehend or manage language, or the Verbal scale alone can be used with
examinees who are visually or motor impaired. There is little emphasis on speed in
this test with only some subscales having time limits and some subscales having
bonuses for speed.
WASIWechsler Abbreviated Scale of Intelligence (WASI) – to obtain a reliable brief
measure of intelligence
Age Range: 6 to 89 years
Administration: Individual - Four Subtest Form = 30 minutes; Two Subtest Form =
15 minutes
The WASI meets the demand for a reliable, brief measure of intellectual ability in
clinical, educational and research settings for ages 6 to 89 years.
WIATThis test provides a comprehensive test of reading (word analysis and
comprehension), writing (spelling and written language), language (listening
comprehension and oral expression), and mathematics (numerical operations and
mathematical reasoning).
Wechsler Memory Scale-RevisedThe Wechsler memory test was first developed in 1945 and is the current standard for
memory tests. Scores of four sub-tests were reported in the case study: general
memory, verbal memory, visual memory, and delayed recalled. These scores are
designed to be averaged to obtain a memory quotient (MQ), with scores comparable
to intelligence quotients or lQs. 100 is an average score for both MQ and IQ.
WISC-IIIThe Wechsler Intelligence Scale for Children, often abbreviated as WISC, is an
individually administered measure of intelligence intended for children aged six years
to 16 years and 11 months.
The WISC is designed to measure human intelligence as reflected in both verbal and
nonverbal (performance) abilities. David Wechsler, the author of the test, believed
that intelligence has a global quality that reflects a variety of measurable skills. He
also thought that it should be considered in the context of the person's overall
personality.
The WISC is used in schools as part of placement evaluations for programs for gifted
children and for children who are developmentally disabled.
In addition to its uses in intelligence assessment, the WISC is used in
neuropsychological evaluation, specifically with regard to braindysfunction. Large
differences in verbal and nonverbal intelligence may indicate specific types of brain
damage.
The WISC is also used for other diagnostic purposes. IQ scores reported by the WISC
can be used as part of the diagnostic criteria for mental retardation and specific
learning disabilities. The test may also serve to better evaluate children with attention-
deficit/hyperactivity disorder(ADHD) and other behavior disorders.
Precautions
The Wechsler intelligence scales are not considered adequate measures of extreme
intelligence (IQ scores below 40 and above 160). The scoring process does not allow
for scores outside this range for test takers at particular ages. Wechsler himself was
even more conservative, stressing that his scales were not appropriate for people with
IQs below 70 or above 130. Despite this restriction, many people use the WISC as a
measure of the intelligence of gifted children, who typically score above 130. The age
range for the WISC overlaps with that of the Wechsler Adult Intelligence
Scale(WAIS) for people between 16 and 17 years of age, but experts suggest that the
WISC provides a better measure for people in this age range.
Administration and scoring of the WISC require a competent administrator who must
be able to interact and communicate with children of different ages and must know
test protocol and specifications. WISC administrators must receive training in the
proper use of the instrument and demonstrate awareness of all test guidelines.
Description
The WISC-III consists of 13 subtests and takes between 50 and 75 minutes to
complete. The test is taken individually, with an administrator present to give
instructions. Each subtest is given separately. There is some flexibility in the
administration of the WISC—the administrator may end some subtests early if the test
taker appears to have reached the limit of his or her capacity. Tasks on the WISC
include questions of general knowledge, traditional arithmetic problems, English
vocabulary, completion of mazes, and arrangements of blocks and pictures.
Children who take the WISC are scored by comparing their performance to other test
takers of the same age. The WISC yields three IQ (intelligence quotient) scores, based
on an average of 100, as well as subtest and index scores. WISC subtests measure
specific verbal and performance abilities. The Wecshler scales were originally
developed and later revised using standardization samples. The samples were meant
to be representative of the United States population at the time of standardization.
The WISC is considered to be a valid and reliable measure of general intelligence in
children. It is regularly used by researchers in many areas of psychology and child
development as a general measure of intelligence. It has also been found to be a good
measure of both fluid and crystallized intelligence. Fluid intelligence refers to
inductive and deductive reasoning, skills that are thought to be largely influenced by
neurological and biological factors. Fluid intelligence is measured by the performance
subtests of the WISC. Crystallized intelligence refers to knowledge and skills that are
primarily influenced by environmental and sociocultural factors. It is measured by the
verbal subtests of the WISC. Wechsler himself did not divide overall intelligence into
these two types. The definition of fluid and crystallized intelligence as two major
categories of cognitive ability, however, has been a focus of research for many
intelligence theorists.
Verbal IQ: The child's verbal IQ score is derived from scores on six of the
subtests: information, digit span, vocabulary, arithmetic, comprehension, and
similarities.
The information subtest is a test of general knowledge, including questions about
geography and literature. The digit span subtest requires the child to repeat strings of
digits recited by the examiner. The vocabulary and arithmetic subtests are general
measures of the child's vocabulary and arithmetic skills. The comprehension subtest
asks the child to solve practical problems and explain the meaning of simple proverbs.
The similarities subtest asks the child to describe the similarities between pairs of
items, for example that apples and oranges are both fruits.
Performance IQ: The child's performance IQ is derived from scores on the
remaining seven subtests: picture completion, picture arrangement, block
design, object assembly, coding, mazes, and symbol search.
In the picture completion subtest, the child is asked to complete pictures with missing
elements. The picture arrangement subtest entails arranging pictures in order to tell a
story. The block design subtest requires the child to use blocks to make specific
designs. The object assembly subtest asks the child to put together pieces in such a
way as to construct an entire object. In the coding subtest, the child makes pairs from
a series of shapes or numbers. The mazes subtest asks the child to solve maze puzzles
of increasing difficulty. The symbol search subtest requires the child to match
symbols that appear in different groups. Scores on the performance subtests are based
on both the speed of response and the number of correct answers.
Results: WISC scores yield an overall intelligence quotient, called the full scale IQ,
as well as a verbal IQ and a performance IQ. The three IQ scores are standardized in
such a way that a score of 100 is considered average and serves as a benchmark for
higher and lower scores. Verbal and performance IQ scores are based on scores on the
13 subtests.
The full scale IQ is derived from the child's scores on all of the subtests. It reflects
both verbal IQ and performance IQ and is considered the single most reliable and
valid score obtained by the WISC. When a child's verbal and performance IQ scores
are far apart, however, the full scale IQ should be interpreted cautiously.
WISC-IV
It is an individually administered clinical instrument for assessing the cognitive ability
of children
aged 6 years through 16 years 11 months.
WISC IV has 4 composite scores (instead of the 2 we had with the WISC III).
Full Scale IQ (FSIQ) is comprises of the four composite scores.
Verbal Comprehension
Index (VCI)
Perceptual Reasoning Index
(PRI)
Working Memory Index (WMI)
Processing Speed Index (PSI)
List of the Subtest under each of the four Indexes:
(key= "( )" indicated that the subtest is not included in the index total score.)
Verbal Comprehension Index (VCI):
Similarities
Vocabulary
Comprehension
(Information)
(Word Reasoning)
Perceptual Reasoning Index (PRI):
Block Design
Picture Concepts
Matrix Reasoning
(Picture Completion)
Working Memory Index (WMI):
Digit Span
Letter-Number Sequencing
(Arithmetic)
Processing Speed Index (PSI):
Coding
Symbol Search
(Cancellation)
The WISC-IV has a total of 15 subtests, 10 are retained from the WISC-III
These are the five new subtests:
Word Reasoning
Matrix Reasoning
Letter-Name Sequencing
Symbol Search
Cancellation
Object Assembly subtest from the WISC III is gone.
On the WISC III there was Picture Arrangement, now on the WISC IV there is
Picture Concepts, under Perceptual Reasoning Index. (Not sure if it is testing the
same type of information or not. Not to be confused with the Picture Completion is
on both versions of the WISC).
Scoring: Current reports show that most students re-tested with the WISC-IV will
have approximately a 5 point discrepancy, lower (to the negative) because of this
newer version of WISC, its novelty and its increased difficulty.
The good news is that the WISC IV has been normed on normal peers and for special
education populations:
Mental Retardation (MR), Attention-Deficit / Hyperactivity Disorder (AD/HD),
Learning Disabilities (LD), both AD/HD and LD, Traumatic Brain Injury (TBI), etc.
With 4 composite scores (vs. 2 as is the case with the WISC III), there is no standard
discrepancy formula, it now all has to be evaluated in terms of the child's ability, test
results, current educational functioning, achievement test expectations based on
ability, evaluation of the subtests as well as evaluation of the composite sets.
Some evaluators have suggested that a 19 point discrepancy in the VCI/PRI
composites may warrant further investigation.
Standard deviation is 15 points, it is not clear that these score will tell enough about
the child's areas of weakness.
Wisconsin Card Sort Test
A test measurement that can be used to measure the level of dopamine activation in
the pre-frontal cortex. The individual is asked to decipher rules, such as shape,
concerning the arrangement of cards, and then must sort the cards according to these
rules. Once they have seen the pattern or rule, the arrangement changes and the
individual must then sort the cards according to the new rule
Woodcock Reading Mastery Tests-RevisedAge Range: Grades K-16, ages 5-0 through 75+
Administration Time: 10-30 minutes for each cluster of tests
Scores/Interpretation: Age- and grade-based percentile ranks, standard scores (M =
100 SD = 15), and NCEs (for Chapter I ), age and grade equivalents.
Benefits
Provides thorough coverage of reading readiness, basic skills, and comprehension
Two forms make it easy to test and retest
Wide age range allows you to test young children to older adults
More diagnostic power with a wide array of scores
The Woodcock Reading Mastery Test-Revised-Normative Update provide an
expanded interpretive system and age range to help you assess reading skills of
children and adults. Two forms, G and H, make it easy to test and retest, or you can
combine the results of both forms for a more comprehensive assessment.
Form G
Two readiness tests and four tests of reading achievement:
Visual-Auditory Learning
Letter Identification (and a Supplementary Letter Checklist)
Word Identification
Word Attack
Word Comprehension (Antonyms, Synonyms, Analogies)
Passage Comprehension
Form H
Four tests of reading achievement with parallel test items to Form G:
Word Identification
Word Attack
Word Comprehension (Antonyms, Synonyms, Analogies)
Passage Comprehension
Vocabulary measured in content areas
Reading vocabulary, measured by the Word Comprehension test, may be evaluated in
four areas: General Reading, Science-Mathematics, Social Studies, and Humanities.
WRMT-R includes practice items and training procedures to help you administer the
test to younger children.
The complete kit also includes an audiocassette with pronunciation guides for Word
Attack and Word Identification items in each form.
WPPSI-RThe Wechsler Preschool and Primary Scale of Intelligence-Revised (WPPSI-R) is a
battery of tests for 3-7 year olds that assesses intellectual functioning. Administration
time is approximately 50-75 minutes.
The WPPSI-R has two parts, the Verbal Scale and the Performance Scale. Each of
these scales has several subtests.
The Verbal Scale measures language expression, comprehension, listening, and the
ability to apply these skills to solving problems. The examiner gives the questions
orally, and the child gives a spoken response. The Performance Scale assesses
nonverbal problem solving, perceptual organisation, speed, and visual-motor
proficiency. Included are tasks like puzzles, analysis of pictures, imitating designs
with blocks, and copying.
Scales Percentile Age
Equivalent
Description of subtest
Performance
Subtests
Object Assembly Visual analysis, object construction
Geometric Design Fine motor co-ordination, copying,
drawing
Block Design Visual motor problem solving,
spatial relationships
Mazes Fine motor co-ordination, planning,
following directions
Picture
Completion
Visual discrimination, alertness to
detail
(Animal Pegs) Visual-motor co-ordination, speed,
concentration
Verbal Subtests
Information Factual knowledge, long term
memory, recall
Comprehension Social and practical judgement,
common sense
Arithmetic numerical reasoning, concentration,
attention
Vocabulary Language development, word
knowledge, verbal fluency
Similarities Abstract reasoning, verbal categories
and concepts
(Sentences) short-term auditory memory,
attention
A Percentile rank expresses the relative position of a score. Additional scores, like
quotients based on groups of selected subtests, can be calculated. These scores can
suggest additional hypotheses about factors underlying the young child's performance
on the WPPSI-R.
A percentile rank of 98 means that a child has scored as well as or better than 98% of
students of the same age on that subtest. The confidence interval indicates the
probable range of scores which can be expected when this individual is retested.
IQ Scale IQ Scale
Score
Percentile Confidence
Interval
Classification
Performance
IQ
Verbal IQ
Full Scale IQ
Conceptual
Index
Spatial Index
Sequential
Index
Intelligence tests like this one are samples of problem solving abilities and learned
facts, and are good predictors of future learning and academic success. However,
there are several factors that the tests do not measure. For instance, they cannot
determine motivation, curiosity, or creative talent. At an early age, they are also
limited by the child's experiences and opportunities for formal and informal learning.
WPPSI-IIIWPPSI™-III features shorter, more game-like activities that hold the attention of
children as young as 2-1/2 years. Simplified instructions and scoring procedures
enhance the ease of administration for examiners.
WPPSI™-III has undergone substantial revision to increase the scale's age
appropriate properties. Age range has been lowered to 2 years 6 months, allowing
for earlier testing of children who could benefit from earlier intervention with special
services Scale has been divided into two age bands, 2:6-3:11 years and 4:0-7:3 years.
Younger children take fewer subtests that are designed to measure verbal
comprehension and perceptual organization abilities. Older children take a greater
number of subtests designed to measure verbal comprehension, perceptual
organization, and processing speed abilities
Less emphasis on acquired knowledge
Instructions to children have been simplified
Elimination of time bonuses due to the normal lags in motor skill development
relative to cognitive skills
Use of queries and prompts is generally unrestricted
All stimulus booklet art has been redrawn to be more colorful and more closely
resemble illustrations found in materials familiar to children
WPPSI™-III test materials have been modified to make administration of the scale
as user friendly as possible.
Instructions to the examiner and scoring procedures have been simplified
New stimulus booklet page layout provides greater comfort and efficiency
throughout testing
Elimination of Object Assembly shield makes presentation of puzzle pieces less
difficult and time-consuming
All subtests now feature teaching and practice items
Overall testing time for core subtests has been reduced, especially for children in
the younger age group, with 25-35 minutes required for them and 40-50 minutes
required for the older children
The scale's psychometric properties have significantly improved.
New items have been added to ensure that all existing subtests have adequate
floors, ceilings, and difficulty-level gradients
All items have been reviewed for ethnic, gender, regional, and socio-economic bias
Seven new subtests were developed to enhance the scale's measurement capabilities
of fluid reasoning, receptive and expressive vocabulary, and processing speed
Significantly improved reliability and validity
Norms include Subtest Scaled Score and Composite Scores (e.g. FSIQ, VIQ, PIQ,
PSQ)
Wide Range Assessment of Memory and LearningPurpose: Designed to evaluate a child's ability for learning and memorizing
information.
Population: Ages 5 through 17
Scales: Verbal Memory Index, Visual Memory Index, Learning Index, General
Memory Index
Time: 45-60 minutes for Core Battery; 83-102 minutes for Expanded Battery.
Authors: David Sheslow & Wayne Adams
Publisher: Jastak Associates Inc
Description: The Wide Range Assessment of Memory and Learning (WRAML) is
designed to assess memory and learning functions across the school years.
Scoring: There are nine subtests each yielding a norm-referenced score. Scores on
three subtests are combined to give a Verbal Memory Index, a Visual Memory Index,
and a Learning Index. The scaled scores for these three indexes are then summed to
yield a General Memory Index. Four of the nine subtests (Verbal Learning, Story
Memory, Sound Symbol, and Visual Learning) ask for both immediate and delayed
recall. Interpretations are provided, based on the age of the child tested, of the
difference between the immediate and delayed score. Thus, the nine subtests of the
WRAML yield a total of 18 scores. The GMI and Verbal, Visual, and Learning
Indexes can be computed in percentiles and standard scores. Individual subtests yield
scaled scores.
Reliability: For the nine subtests, the reliability coefficients are usually between .80
and .85. When subtests are combined, reliabilities range from approximately .90
to .96. Test reliability is as high for younger as for older children.
Validity: Construct validity, used in Rasch measurement, indicates excellent item
definitions of variables measured and internal consistency Comparisons with the
WMS-R for adolescents (16-17 year). The WRAML appears superior to the WMS-R
for use with adolescents. The WRAML is well validated, and is widely used in
research. Information is also included concerning the standard error of measurement
for each subtest and index for each age group, along with correlations between scores
on the WRAML and other standardized instruments such as the McCarthy Memory
Index, Stanford Binet Short-Term Memory, and the Wechsler Memory Scale.
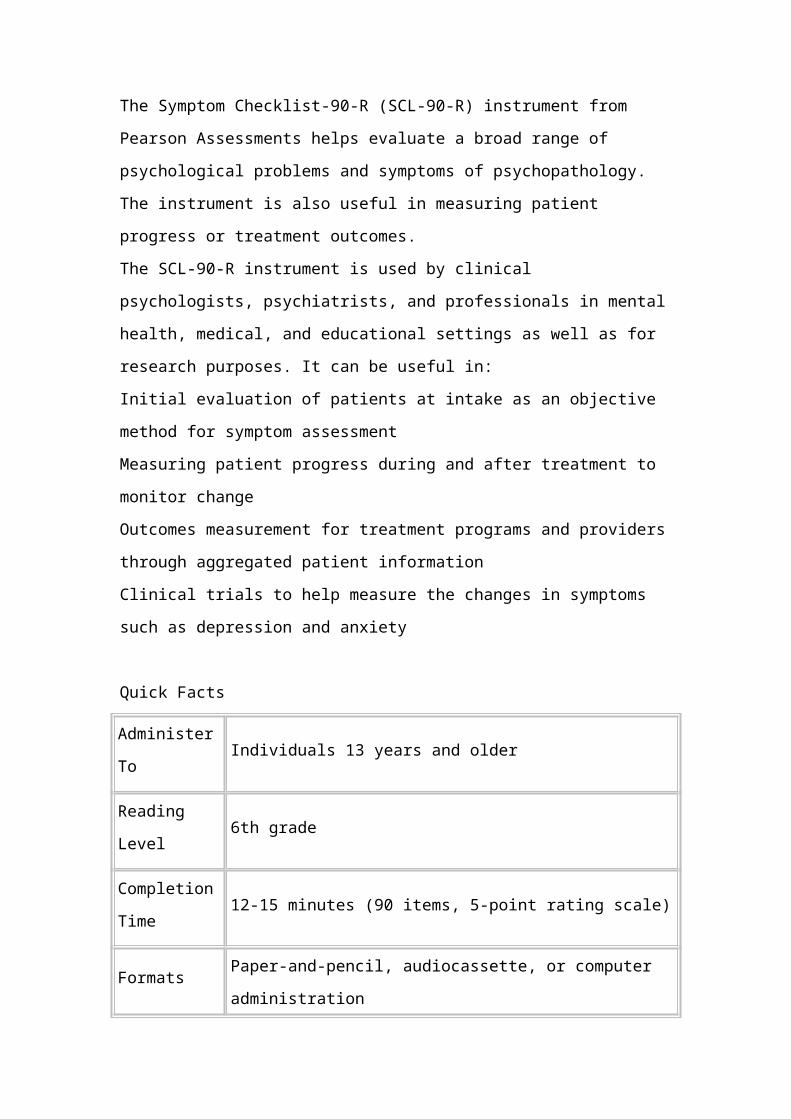
Norms: The test was normed and standardized based on samples of children from 5
to 16 years of age. There were approximately 112 children in each subgroup (half-
year intervals). The total norming group consisted of 2,363 individuals. The norming
samples are representative of the US population with regard to gender, geographic
region, and parental occupation.
Suggested use: The major use for the WRAML is clinical in terms of providing
incremental information in making an individual diagnosis. The WRAML is used to
evaluate learning and school–related problems. It is helpful in evaluating the effects
of a language disability or problems with verbal memory retrieval, in identifying the
inefficient or disorganized memory strategies of a bright but under-achieving student,
and in pointing to the functional inefficiency of memory in a child with attention
deficit. It can be used to assess memory following head injury.





























