Embed Size (px)
Citation preview

The relationship between vitamin D status and leukocytes in hospitalised cats
Titmarsh, H.F,1 Cartwright J.A1, Kilpatrick, S.1, Gaylor, D1., Milne E 1 Berry, J2., Bommer,
N1., Gunn-Moore, D1., Reed, N1., Handel, I. 1, Mellanby, R.J1. *
1. Royal (Dick) School of Veterinary Studies and The Roslin Institute, The University
of Edinburgh, Roslin, Midlothian, United Kingdom
2. Specialist Assay Laboratory (Vitamin D), Clinical Biochemistry, Manchester Royal
Infirmary, Manchester, United Kingdom
Corresponding author:
Helen Titmarsh BVetMed(Hons)MRCVS
Hospital for Small Animals
Royal (Dick) School of Veterinary Studies
Easter Bush Campus
The University of Edinburgh
Roslin
Midlothian
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18

Email [email protected]
0131 650 7650
Keywords: 25 hydroxyvitamin D, neutrophils, vitamin D, cat
19
20
21
22
23
24
25
26
27
28
29
30
31
32

Abstract
Objectives: Vitamin D deficiency, as assessed by serum 25 hydroxyvitamin D (25(OH)D)
concentrations, has been linked to markers of systemic inflammation in human and canine
medicine. However, the relationship between vitamin D status and inflammation has not
been previously investigated in cats. The aim of this study was to examine the relationship
between serum 25(OH)D concentrations and leukocyte counts in hospitalised sick cats.
Methods: Serum 25(OH)D concentrations, and haematology profiles were measured in 170
consecutive hospitalised sick cats. A binary logistical regression model examined the
relationship between serum 25(OH)D concentration, age, sex, breed and neutrophil,
monocyte, eosinophil and lymphocyte counts.
Results: Cats with a neutrophilia had lower serum 25(OH)D concentrations than cats with
neutrophil concentrations below the upper limit of the reference range. There were no
differences in serum 25(OH)D concentrations in cats with monocyte, lymphocyte or
eosinophil counts above their respective reference interval compared to cats with counts
below the upper limit of the reference interval.
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47

Conclusions and relevance: Hospitalised cats with a neutrophil count above the reference
range had lower vitamin D status. There is a need to establish whether lower vitamin D
status is a cause or consequence of increased neutrophil counts.
Introduction
The actions of vitamin D have been classically understood in terms of its role in regulating
calcium homeostasis and bone metabolism. However, more diverse physiological roles of
vitamin D have been demonstrated in recent years and numerous cell types have been
shown to express the vitamin D receptor.[1, 2] Low serum vitamin D status, most
commonly assessed by measuring serum 25-hydroxvitamin D (25(OH)D) concentrations,
are commonly reported in a number of human and canine diseases including hypertension
[3], diabetes mellitus, [4] cardiovascular disease, [5, 6] cancer [7, 8] autoimmune
conditions [9], chronic enteropathies [10, 11] and infectious diseases.[12-16] In feline
medicine low vitamin D status has been observed in cats with mycobacterial infections [15]
and in cats with inflammatory bowel disease or small cell gastrointestinal lymphoma.[17]
Importantly, serum 25(OH)D concentrations are also predictive of short-term mortality in
hospitalised cats.[18] Similarly, low serum 25(OH)D concentrations have also been found
to be predictive of mortality in people [19] and horses.[20]
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65

Despite the clear association between serum 25(OH)D concentrations and the incidence and
outcome of many diseases, it remains unclear whether vitamin D plays a mechanistic role
in poor health outcomes or is a surrogate marker of ill-health. It has been argued that
vitamin D status may influence health outcomes through its ability to modulate the immune
system. Most leukocytes, including, antigen presenting cells, T-lymphocytes and B-
lymphocytes [21], express the vitamin D receptor (VDR). Vitamin D can promote immune
tolerance by inhibiting pro-inflammatory immune responses and by increasing regulatory T
cell populations.[22-28]
In humans serum 25(OH)D concentrations have been inversely associated with markers of
inflammation including acute phase proteins and, pro-inflammatory cytokines. This has
been demonstrated in a number of diseases including inflammatory polyarthritis,[29]
diabetes mellitus,[30] autoimmune diseases,[31, 32] inflammatory bowel disease [33, 34]
and human immunodeficiency virus.[35] Inflammatory markers are also increased in
elderly and healthy people with low serum concentrations of vitamin D.[36-38] In addition,
low vitamin D status has been associated with markers of inflammation in dogs with
haemoabdomens [8] and dogs with chronic enteropathies.[39]
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83

Despite a number of studies having investigated the association between serum 25(OH)D
concentrations and inflammation, surprisingly few studies have looked at the relationship
between serum vitamin D concentrations and leukocyte populations in either human or
veterinary patients.[40] One study which investigated the association between white blood
cell concentrations and serum 25(OH)D found an inverse relationship between these two
parameters in smokers.[40] The lack of studies which have examined the relationship
between leukocytes and vitamin D status in humans resulted in Lee et al (2015) concluding
that ‘evaluation of different forms of inflammatory cells, not just total white blood cell
count, may be a useful method to identify the association of vitamin D and
inflammation’[41].
Despite the growing body of work investigating the relationship between serum 25(OH)D
concentrations and illness in humans and dogs, the association between 25(OH)D and
inflammation has not been previously investigated in cats. Therefore, the objective of this
study was to measure serum concentrations of 25(OH)D, alongside whole blood neutrophil,
lymphocyte, monocyte and eosinophil numbers in a population of hospitalised sick cats.
The hypothesis of the study was that there would be a negative relationship between serum
25(OH)D concentrations and leukocyte counts.
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101

Material and Methods
Cats consecutively examined at the Hospital for Small Animals, Royal Dick School of
Veterinary Studies, were considered for inclusion in the study. Clinical records were
reviewed for each cat enrolled. The age, sex, breed and final diagnosis was recorded for
each cat. In order to be eligible for inclusion the following clinical data needed to be
available; total white blood cell count, segmented and band neutrophil, monocyte,
eosinophil and lymphocyte counts. In addition residual stored serum samples had to be
available for 25(OH)D quantification.
Following handling of blood samples for routine diagnostic procedures on the day of
admission, serum samples were initally stored at -20°C and later moved to -80oC for longer
term storage until 25(OH)D concentrations were measured in batches. Vitamin D is
extremely stable even when stored at -20oC. [42] Serum concentrations of 25(OH)D2 and
25(OH)D3 were determined by liquid chromatography tandem mass spectrophotometry
(LC-MS/MS) using an ABSciex 5500 tandem mass spectrophotometer (Warrington, UK)
and the Chromsystems (Munich, Germany) 25OHD kit for LC-MS/MS following the
manufacturers’ instructions (intra- and inter-assay CV 3.7% and 4.8% respectively). This
Supraregional Assay Service laboratory is accredited by CPA UK (CPA number 0865) and
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119

has been certified as proficient by the international Vitamin D Quality Assurance Scheme
(DEQAS). Total 25(OH)D is defined as the sum of 25(OH)D2 and 25(OH)D3.
Haematology variables were measured on an ADVIA(r) 2120i System with Autoslide
(Siemens Medical Solutions Diagnostics Ltd California, USA). A manual white blood cell
differential count was undertaken on at least 100 leukocytes to establish the concentrations
of neutrophils, monocytes, lymphocytes, eosinophils and basophils. Blood smears from all
cases were evaluated under the direct supervision of a Board-certified veterinary clinical
pathologist. Total calcium concentrations were measured using an ILab650 biochemistry
analyser (Diamond Diagnostics, USA).
The relationship between serum 25(OH)D concentrations and neutrophils, lymphocytes,
monocytes and eosinophils was initially examined using dot plots which plotted leukocyte
counts against serum 25(OH)D concentrations. The relationship between 25(OH)D
concentrations in segmented neutrophils, lymphocytes, monocytes and eosinophils
populations which were above or below the upper limit of the reference interval were
examined using a Mann Whitney U test. In the four leukocyte populations, the relationship
between 25(OH)D concentrations, age, breed and sex was investigated by a binary
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137

logistical regression model. Co-variates were removed from the initial model to minimise
Akaike Information Criterion (AIC), a parameter penalised measure of best fit, to give a
final parsimonious model. The relationship between calcium and serum 25(OH)D
concentrations was assessed by Spearman’s rank correlation test.
The study was approved by the University of Edinburgh’s Veterinary Ethical Review
Committee. Informed consent for the storage and subsequent use of residual clinical blood
samples for research purposes was obtained at admission for each cat enrolled.
138
139
140
141
142
143
144
145
146

Results
One hundred and seventy cats were included in the study. The median age of the cats was
108 months (2.5-264 months). There were 4 entire males, 102 neutered males, 1 entire
female and 63 neutered female cats. Breeds included in the study were 110 Domestic Short
Hair cats, 15 Domestic Long Hair cats, 8 Maine Coons, 3 Oriental Short Hairs, 8 Burmese,
7 Bengals, 6 Siamese, 2 Ragdolls and one of each of the following breeds; Chinchilla,
Abyssinian, Persian, British Blue, Manx, Siberian, Russian Blue, Egyptian, Norwegian
Forest Cat, Burmilla and Tonkinese. There was a significant positive correlation between
total calcium and 25(OH)D concentration (r=0.21, p<0.01).
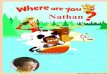
Dot plots of serum 25(OH)D concentrations from cats with haematology parameters above
or below the upper reference interval are shown in figure 1. Serum 25(OH)D
concentrations were significantly lower in cats with a segmented neutrophil count above the
upper reference interval compared to cats with a segmented neutrophil count below the
upper reference range (p=0.04). This significant difference remained even after removal of
the high outlying result in the <12.8x109/l group. Twelve cats had band neutrophils. The
median serum concentration of 25(OH)D from cats with band neutrophils was 59.8nmol/l
compared to cats with band neutrophils was 97.4nmol/l. This difference approached
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164

significance (p=0.06). There was no significant difference in 25(OH)D concentrations in
cats with eosinophil, lymphocyte and monocyte counts above upper reference interval
compared to cats with leukocyte counts below the upper end of the reference interval. The
lower serum 25(OH)D concentrations observed in cats with a segmented neutrophil count
above the upper reference interval was not confounded by age, breed or sex as the final
logistic regression model only included 25(OH)D concentrations as a predictor of increased
neutrophil counts (p=0.021). The odds of having a neutrophil count within the reference
interval increased by 1.32 (1.04-1.72 95% CI) per 25nmol/l increase in serum
concentrations of 25(OH)D.
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180

Discussion
The main finding of this study was that cats with a neutrophilia have lower vitamin D
status than cats with neutrophil counts below the upper reference interval. This observation
is consistent with studies in human and canine patients together with experimental models
of inflammation. For example, a study of over 1300 children found a negative correlation
between neutrophil count and 25(OH)D concentrations.[43] Furthermore, vitamin D
supplementation has been shown to reduce the proportion of neutrophils in a murine model
of allergic airway disease.[44] The finding of a negative relationship between 25(OH)D
concentrations and segmented neutrophils is also consistent with our recent work in dogs
with intestinal inflammation.[39]This study demonstrated that vitamin D status was
negatively correlated with neutrophil counts, together with several other markers of
systemic and intestinal inflammation, in dogs with a chronic enteropathy.
It is presently unclear if low 25(OH)D concentrations are a cause or consequence of
inflammation. It has been hypothesised that serum 25(OH)D may act as a negative acute
phase protein.[45] Evidence in support of this hypothesis include the demonstration that
serum 25(OH)D concentrations decrease alongside parallel increases in inflammatory
markers in patients whom have undergone elective knee surgeries.[46, 47] Decreases in
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198

serum 25(OH)D concentrations have also been reported with spontaneously occurring
inflammatory conditions such as acute pancreatitis.[48] Alterations in vitamin D status may
also occur due the effect of inflammation on vitamin D binding proteins. For example,
serum concentrations of vitamin D binding protein concentration decrease in acute
inflammation.[45] In contrast, other investigators have demonstrated that patients with
lower 25(OH)D concentrations are more likely to develop an inflammatory response
following immune stimulation. For example, the acute phase response following
administration of parenteral bisphosphonates was greater in patients with low vitamin D
status, suggesting that hypovitaminosis D may predispose people to acute inflammatory
reactions.[49] In addition, other studies suggest that vitamin D may not decrease acutely in
all inflammatory conditions. For example, no significant decreases in 25(OH)D
concentrations were reported secondary to myocardial infarction.[50] Similarly, there was
no association between hypovitaminosis D and markers of an acute phase response in
humans with pulmonary tuberculosis.[51]
Investigating the potential relationship between vitamin D and inflammation in a number of
species is important as vitamin D supplementation could be a beneficial treatment for
patients with inflammatory diseases. In experimental animal models, vitamin D and vitamin
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216

D analogues have demonstrated anti-inflammatory properties in a number of conditions
including cerebral malaria [52], experimental models of colitis [53], models of cognitive
dysfunction [54], acute kidney injury [55] and interstitial cystitis [56]. There is evidence
that supplementing vitamin D can reduce inflammatory markers in systemic lupus
erythematosus, [57] cystic fibrosis [58] and patients with type II diabetes.[59] However,
vitamin D supplementation does not universally reduce markers of inflammation.[60, 61]
Therefore, the role of vitamin D in the initiation, perpetuation and resolution of
inflammation is worthy of further investigation
Our study also demonstrated a significant correlation between total calcium and 25(OH)D.
This is consistent with our findings in dogs with a CE [11] and in humans. [62] Our finding
of an association between total calcium and 25(OH)D is consistent with the known effects
of vitamin D, which includes increasing serum calcium concentrations by increasing dietary
calcium absorption in the intestines, and acting in the kidney to promote calcium
reabsorption and promote calcium resorption from bone. [63]
There are some limitations with this study. Firstly, leukocyte numbers can be altered by
processes other than inflammation. For example, neutrophil numbers will transiently
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234

increase due to the release of adrenaline in response to stressful stimuli such as
hospitalisation or blood sampling. Other limitations of this study include that cats come
from a referral population. This makes it difficult to fully assess a number of confounding
variables that could affect both serum vitamin D concentrations and leukocyte numbers.
For example, the cats involved in this study may have been treated with a number of
medications prior to admission to the hospital, which may have influenced haematological
values. It is not known if medications influence serum 25(OH)D concentrations in cats.
Although glucocorticoids may influence vitamin D concentrations in people, short term,
anti-inflammatory doses of glucocorticoids do not significantly alter vitamin D metabolism
in dogs.[64] As information regarding the influence of drugs on vitamin D homeostasis in
cats is lacking, no cases were excluded based on previous medical therapy. However, it
must be acknowledged that pre-treatment with drugs may have influenced the results of this
study and future work investigating the effect of drugs such as steroids on serum 25(OH)D
concentrations of cats would be valuable. Diet could also influence serum 25(OH)D in cats
and a further limitation of this study is that the cats didn’t receive the same diets. However,
it is standard practice in our hospital to record the diets fed to cats at the time of admission.
All but one cat in this study was fed commercial cat food. As commercial cat foods are
standardly supplemented with vitamin D within recommended limits,[65] variation in
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252

vitamin D content of the diets consumed by cats enrolled in the study was unlikely to have
been a significant confounding variable
In conclusion, the study has demonstrated that cats with a neutrophilia have lower vitamin
D status than cats with a neutrophil count below the upper limit of the reference range. This
study demonstrates the need to further clarify the relationship between inflammation and
vitamin D status in cats.
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267

References
1. The Nonskeletal Effects of Vitamin D: An Endocrine Society Scientific Statement. Endocrine Reviews, 2012. 33(3): p. 456-492.
2. Christakos, S., et al., New insights into the mechanisms of vitamin D action. Journal of Cellular Biochemistry, 2003. 88(4): p. 695-705.
3. Tamez, H. and R.I. Thadhani, Vitamin D and hypertension: an update and review. Current Opinion in Nephrology and Hypertension, 2012. 21(5): p. 492-499.
4. Feng, R., et al., Lower serum 25 (OH) D concentrations in type 1 diabetes: A meta-analysis. Diabetes Res Clin Pract, 2015. 108(3): p. e71-5.
5. Grandi, N.C., L.P. Breitling, and H. Brenner, Vitamin D and cardiovascular disease: systematic review and meta-analysis of prospective studies. Preventive medicine, 2010. 51(3): p. 228-233.
6. Kraus, M.S., et al., Relation of Vitamin D Status to Congestive Heart Failure and Cardiovascular Events in Dogs. Journal of Veterinary Internal Medicine, 2014. 28(1): p. 109-115.
7. Churilla, T.M., et al., Vitamin D deficiency is widespread in cancer patients and correlates with advanced stage disease: a community oncology experience. Nutr Cancer, 2012. 64(4): p. 521-5.
8. Selting, K.A., et al., Serum 25-hydroxyvitamin D concentrations in dogs – correlation with health and cancer risk. Veterinary and Comparative Oncology, 2014: p. n/a-n/a.
9. Kriegel, M.A., J.E. Manson, and K.H. Costenbader. Does vitamin D affect risk of developing autoimmune disease?: a systematic review. in Seminars in arthritis and rheumatism. 2011. Elsevier.
10. Mellanby, R., et al., Hypocalcaemia associated with low serum vitamin D metabolite concentrations in two dogs with protein losing enteropathies.‐ Journal of Small Animal Practice, 2005. 46(7): p. 345-351.
11. Gow, A.G., et al., Hypovitaminosis D in dogs with inflammatory bowel disease and hypoalbuminaemia. Journal of Small Animal Practice, 2011. 52(8): p. 411-8.
12. Mehta, S., et al., Vitamin D status of HIV-infected women and its association with HIV disease progression, anemia, and mortality. PLoS One, 2010. 5(1): p. e8770.
13. Berry, D.J., et al., Vitamin D status has a linear association with seasonal infections and lung function in British adults. British Journal of Nutrition, 2011. 106(09): p. 1433-1440.
14. Quraishi, S.A., et al., Association between prehospital vitamin D status and hospital-acquired bloodstream infections. The American Journal of Clinical Nutrition, 2013. 98(4): p. 952-959.
268
269270271272273274275276277278279280281282283284285286287288289290291292293294295296297298299300301302

15. Lalor, S.M., et al., Domesticated cats with active mycobacteria infections have low serum vitamin D (25(OH)D) concentrations. Transboundary and Emerging Diseases, 2012. 59(3): p. 279-81.
16. Rosa, C.T., et al., Hypovitaminosis D in Dogs with Spirocercosis. Journal of Veterinary Internal Medicine, 2013. 27(5): p. 1159-1164.
17. Lalor, S., et al., Cats with Inflammatory Bowel Disease and Intestinal Small Cell Lymphoma Have Low Serum Concentrations of 25-Hydroxyvitamin D. Journal of Veterinary Internal Medicine, 2014. 28(2): p. 351-355.
18. Titmarsh, H., et al., Vitamin D Status Predicts 30 Day Mortality in Hospitalised Cats. PLoS ONE, 2015. 10(5): p. e0125997.
19. Melamed, M.L., et al., 25-hydroxyvitamin D levels and the risk of mortality in the general population. Arch Intern Med, 2008. 168(15): p. 1629-37.
20. Kamr, A.M., et al., Vitamin D Metabolites and Their Association with Calcium, Phosphorus, and PTH Concentrations, Severity of Illness, and Mortality in Hospitalized Equine Neonates. PLoS ONE, 2015. 10(6): p. e0127684.
21. Prietl, B., et al., Vitamin D and immune function. Nutrients, 2013. 5(7): p. 2502-21.22. Chambers, E.S., et al., 1alpha,25-dihydroxyvitamin D3 in combination with transforming
growth factor-beta increases the frequency of Foxp3(+) regulatory T cells through preferential expansion and usage of interleukin-2. Immunology, 2014. 143(1): p. 52-60.
23. Khoo, A.-L., et al., Vitamin D3 down-regulates proinflammatory cytokine response to Mycobacterium tuberculosis through pattern recognition receptors while inducing protective cathelicidin production. Cytokine, 2011. 55(2): p. 294-300.
24. Boonstra, A., et al., 1α,25-Dihydroxyvitamin D3 Has a Direct Effect on Naive CD4+ T Cells to Enhance the Development of Th2 Cells. The Journal of Immunology, 2001. 167(9): p. 4974-4980.
25. Martineau, A.R., et al., IFN-γ- and TNF-Independent Vitamin D-Inducible Human Suppression of Mycobacteria: The Role of Cathelicidin LL-37. The Journal of Immunology, 2007. 178(11): p. 7190-7198.
26. Harishankar, M., et al., 1,25-Dihydroxy vitamin D3 downregulates pro-inflammatory cytokine response in pulmonary tuberculosis. Int Immunopharmacol, 2014. 23(1): p. 148-52.
27. Jeong, M.S., et al., Calcitriol May Down-Regulate mRNA Over-Expression of Toll-Like Receptor-2 and -4, LL-37 and Proinflammatory Cytokines in Cultured Human Keratinocytes. Ann Dermatol, 2014. 26(3): p. 296-302.
28. Nissou, M.F., et al., Additional clues for a protective role of vitamin D in neurodegenerative diseases: 1,25-dihydroxyvitamin D3 triggers an anti-inflammatory response in brain pericytes. J Alzheimers Dis, 2014. 42(3): p. 789-99.
303304305306307308309310311312313314315316317318319320321322323324325326327328329330331332333334335336337338339

29. Patel, S., et al., Association between serum vitamin D metabolite levels and disease activity in patients with early inflammatory polyarthritis. Arthritis and Rheumatology, 2007. 56(7): p. 2143-9.
30. Shih, E.M., et al., Effects of vitamin D repletion on glycemic control and inflammatory cytokines in adolescents with type 1 diabetes. Pediatric Diabetes, 2014.
31. de Souza, V.A., et al., Association of hypovitaminosis D with Systemic Lupus Erythematosus and inflammation. Jornal Brasileiro de Nefrologia, 2014. 36(4): p. 430-6.
32. Robinson, A.B., et al., Vitamin D deficiency is common and associated with increased C-reactive protein in children and young adults with lupus: an Atherosclerosis Prevention in Pediatric Lupus Erythematosus substudy. Lupus Science and Medicine, 2014. 1(1): p. e000011.
33. Raftery, T., et al., Vitamin D Status Is Associated with Intestinal Inflammation as Measured by Fecal Calprotectin in Crohn's Disease in Clinical Remission. Digestive Diseases and Sciences, 2015.
34. Garg, M., et al., Association of Circulating Vitamin D Concentrations with Intestinal but Not Systemic Inflammation in Inflammatory Bowel Disease. Inflammatory Bowel Diseases, 2013. 19(12): p. 2634-2643.
35. Poudel-Tandukar, K., et al., Serum 25-hydroxyvitamin d levels and C-reactive protein in persons with human immunodeficiency virus infection. AIDS Research And Human Retroviruses, 2013. 29(3): p. 528-34.
36. De Vita, F., et al., Relationship between vitamin D and inflammatory markers in older individuals. Age (Dordr), 2014. 36(4): p. 9694.
37. Laird, E., et al., Vitamin D deficiency is associated with inflammation in older Irish adults. The Journal of Clinical Endocrinology and Metabolism
2014. 99(5): p. 1807-15.38. Peterson, C.A. and M.E. Heffernan, Serum tumor necrosis factor-alpha concentrations are
negatively correlated with serum 25(OH)D concentrations in healthy women. Journal of Inflammation 2008. 5: p. 10.
39. Titmarsh, H.F., et al., Low Vitamin D Status Is Associated with Systemic and Gastrointestinal Inflammation in Dogs with a Chronic Enteropathy. PLoS ONE, 2015. 10(9): p. e0137377.
40. Mellenthin, L., et al., Association between serum vitamin D concentrations and inflammatory markers in the general adult population. Metabolism, 2014. 63(8): p. 1056-1062.
41. Lee, H., et al., Interaction of Vitamin D and Smoking on Inflammatory Markers in the Urban Elderly. J Prev Med Public Health, 2015. 48(5): p. 249-56.
340341342343344345346347348349350351352353354355356357358359360361362363
364365366367368369370371372373374375

42. Wielders, J.P.M. and F.A. Wijnberg, Preanalytical Stability of 25(OH)–Vitamin D3 in Human Blood or Serum at Room Temperature: Solid as a Rock. Clinical Chemistry, 2009. 55(8): p. 1584-1585.
43. Hollams, E.M., et al., Vitamin D and atopy and asthma phenotypes in children: a longitudinal cohort study. European Respiratory Journal, 2011. 38(6): p. 1320-1327.
44. Gorman, S., et al., Reversible Control by Vitamin D of Granulocytes and Bacteria in the Lungs of Mice: An Ovalbumin-Induced Model of Allergic Airway Disease. PLoS ONE, 2013. 8(6): p. e67823.
45. Waldron, J.L., et al., Vitamin D: a negative acute phase reactant. Journal of Clinical Pathology, 2013. 66(7): p. 620-2.
46. Reid, D., et al., The relation between acute changes in the systemic inflammatory response and plasma 25-hydroxyvitamin D concentrations after elective knee arthroplasty. The American Journal of Clinical Nutrition, 2011. 93(5): p. 1006-11.
47. Henriksen, V.T., et al., Pro-inflammatory cytokines mediate the decrease in serum 25(OH)D concentrations after total knee arthroplasty? Medical Hypotheses, 2014. 82(2): p. 134-7.
48. Bang, U.C., et al., Variations in Serum 25-Hydroxyvitamin D during Acute Pancreatitis: An Exploratory Longitudinal Study. Endocrine Research, 2011. 36(4): p. 135-141.
49. Bertoldo, F., et al., Serum 25-hydroxyvitamin D levels modulate the acute-phase response associated with the first nitrogen-containing bisphosphonate infusion. Journal of Bone and Mineral Research, 2010. 25(3): p. 447-454.
50. Barth, J.H., et al., Serum 25 hydroxy-vitamin D does not exhibit an acute phase reaction after acute myocardial infarction. Annals of Clinical Biochemistry, 2012. 49(4): p. 399-401.
51. Friis, H., et al., Hypovitaminosis D is common among pulmonary tuberculosis patients in Tanzania but is not explained by the acute phase response. Journal of Nutrition, 2008. 138(12): p. 2474-80.
52. He, X., et al., Vitamin D inhibits the occurrence of experimental cerebral malaria in mice by suppressing the host inflammatory response. The Journal of Immunology, 2014. 193(3): p. 1314-23.
53. Laverny, G., et al., Efficacy of a potent and safe vitamin D receptor agonist for the treatment of inflammatory bowel disease. Immunology Letters, 2010. 131(1): p. 49-58.
54. Briones, T.L. and H. Darwish, Vitamin D mitigates age-related cognitive decline through the modulation of pro-inflammatory state and decrease in amyloid burden. Journal of Neuroinflammation, 2012. 9: p. 244.
55. Lee, J.W., et al., Renoprotective effect of paricalcitol via a modulation of the TLR4-NF-kappaB pathway in ischemia/reperfusion-induced acute kidney injury. Biochemical and Biophysical Research Communications 2014. 444(2): p. 121-7.
376377378379380381382383384385386387388389390391392393394395396397398399400401402403404405406407408409410411

56. Benigni, F., et al., Oral treatment with a vitamin D3 analogue (BXL628) has anti-inflammatory effects in rodent model of interstitial cystitis. BJU International, 2006. 97(3): p. 617-24.
57. Abou-Raya, A., S. Abou-Raya, and M. Helmii, The effect of vitamin D supplementation on inflammatory and hemostatic markers and disease activity in patients with systemic lupus erythematosus: a randomized placebo-controlled trial. The Journal of rheumatology, 2013. 40(3): p. 265-72.
58. Grossmann, R.E., et al., Impact of vitamin D supplementation on markers of inflammation in adults with cystic fibrosis hospitalized for a pulmonary exacerbation. European Journal of Clinical Nutrition
2012. 66(9): p. 1072-4.59. Shab-Bidar, S., et al., Improvement of vitamin D status resulted in amelioration of
biomarkers of systemic inflammation in the subjects with type 2 diabetes. Diabetes/metabolism research and reviews, 2012. 28(5): p. 424-30.
60. Jorde, R., et al., No effect of supplementation with cholecalciferol on cytokines and markers of inflammation in overweight and obese subjects. Cytokine, 2010. 50(2): p. 175-180.
61. Carlson, N., et al., Hypovitaminosis D correction and high-sensitivity C-reactive protein levels in hypertensive adults. The Permanente Journal, 2013. 17(4): p. 19-21.
62. Harris, S.S., et al., Vitamin D Insufficiency and Hyperparathyroidism in a Low Income, Multiracial, Elderly Population. The Journal of Clinical Endocrinology & Metabolism, 2000. 85(11): p. 4125-4130.
63. Gallieni, M., et al., Vitamin D: physiology and pathophysiology. Int J Artif Organs, 2009. 32(2): p. 87-94.
64. Kovalik, M., et al., Short-term prednisolone therapy has minimal impact on calcium metabolism in dogs with atopic dermatitis. The Veterinary Journal, 2012. 193(2): p. 439-442.
65. Federation, F.E.P.F.I., Nutritional Guidelines For Complete and Complementary Pet Food for Cats and Dogs, F.E.P.F.I. Federation, Editor. 2014: www.fediaf.org.
412413414415416417418419420421
422423424425426427428429430431432433434435436437438439440
441
442
443

Figures
Figure 1: Graphs showing 25(OH)D concentrations between cats with leukocytes numbers
above and below upper limits of reference intervals
444
445
446
447
448
449
450