Embed Size (px)
Citation preview

Service provision framework: Complex needsIncluding the Multiple and Complex Needs Initiative (MACNI)
and Support for High Risk Tenancies (SfHRT)
March 2020
Service provision framework: Complex Needs August 2019 Page 1

To receive this publication in an accessible format please email Disability and Complex Clients Practice Advice and Support <[email protected]>
Authorised and published by the Victorian Government, 1 Treasury Place, Melbourne.
© State of Victoria, Department of Health and Human Services March 2020.Page 2 Service provision framework: Complex Needs August 2019

Contents
Service provision framework: Complex Needs August 2019 Page 3

Glossary of terms.....................................................................................................................................
1. Audience and purpose.......................................................................................................................
2. Introduction.........................................................................................................................................
3. Complex needs model........................................................................................................................3.1 Complex needs...................................................................................................................................
3.2 Role of Complex Needs Coordinator..................................................................................................
3.3 Service integration and capacity building............................................................................................
3.4 Exclusions to Complex Needs services response..............................................................................
3.5 Transfer of clients between areas.......................................................................................................
4. MACNI legislation...............................................................................................................................4.1 Instrument of delegation.....................................................................................................................
4.2 MACNI eligibility criteria......................................................................................................................
4.2.1 Interpretation of diagnostic criteria...................................................................................................
5. Department of Health and Human Services.....................................................................................5.1 Strategic directions.............................................................................................................................
5.2 Groups and areas...............................................................................................................................
5.3 Governance and responsibilities.........................................................................................................
5.4 Complex Needs Panels......................................................................................................................
6. Multiple and Complex Needs Initiative (MACNI)..............................................................................6.1 Operating model.................................................................................................................................
7. Identification and referral...................................................................................................................7.1 Aboriginal and Torres Strait Islander people.......................................................................................
8. Consultation........................................................................................................................................8.1 Complex Needs Panel involvement....................................................................................................
8.2 Consultation assessment brokerage...................................................................................................
8.3 Consultation closure...........................................................................................................................
9. Pre-MACNI...........................................................................................................................................9.1 Complex Needs Panel involvement....................................................................................................
9.2 Pre-MACNI brokerage........................................................................................................................
9.3 Pre-MACNI closure.............................................................................................................................
10. Formal MACNI services....................................................................................................................10.1 Eligibility............................................................................................................................................
Page 4 Service provision framework: Complex Needs August 2019

10.2 Care plan development.....................................................................................................................
10.3 Care plan coordination......................................................................................................................
10.4 Care plan review...............................................................................................................................
10.5 Care plan progress updates..............................................................................................................
10.6 Suspension of a care plan................................................................................................................
10.7 Transition/exit planning.....................................................................................................................
10.8 Care plan closure..............................................................................................................................
11. Post-MACNI support.........................................................................................................................
12. Support for High Risk Tenancies (SfHRT)......................................................................................12.1 Operating model...............................................................................................................................
12.2 Eligibility............................................................................................................................................
12.3 SfHRT identification and referral.......................................................................................................
12.4 SfHRT consultation...........................................................................................................................
12.5 Case conferencing............................................................................................................................
12.6 Interface with Tenancy Plus..............................................................................................................
12.7 Interface with Indigenous Tenants at Risk (ITAR).............................................................................
12.8 SfHRT consultation closure..............................................................................................................
13. Interface with the NDIS.....................................................................................................................13.1 Transitions Team and Intensive Support Team................................................................................
13.2 Complex Support Needs Pathway....................................................................................................
13.3 NDIS plan and MACNI care plan......................................................................................................
13.4 Public housing and the NDIS............................................................................................................
14. Interface with the Forensic Disability Program..............................................................................
15. Brokerage..........................................................................................................................................15.1 Eligibility for brokerage......................................................................................................................
15.2 Brokerage principles.........................................................................................................................
15.3 Brokerage exclusions........................................................................................................................
15.4 Brokerage approval processes.........................................................................................................
15.5 Brokerage business rules.................................................................................................................
15.6 Brokerage management...................................................................................................................
15.7 Procurement.....................................................................................................................................
15.8 Probity...............................................................................................................................................
15.9 Brokerage transfer to groups............................................................................................................
15.10 Transfer of brokerage between areas.............................................................................................
Service provision framework: Complex Needs August 2019 Page 5

15.11 Acquittal upon closure.....................................................................................................................
15.12 Brokerage recording and reporting in SharePoint and the Complex Support Application...............
16. Quality, safeguards and critical events..........................................................................................16.1 Child safe standards.........................................................................................................................
16.2 Human services standards...............................................................................................................
16.3 Human rights charter........................................................................................................................
16.4 Client refusal.....................................................................................................................................
16.5 Client participation............................................................................................................................
16.6 Privacy and confidentiality................................................................................................................
16.7 Documented consent........................................................................................................................
16.8 Duty of care referrals........................................................................................................................
16.9 Client feedback and complaints........................................................................................................
16.10 Appeal of MACNI service decisions................................................................................................
16.11 Accessing records...........................................................................................................................
16.12 Client Incident Management System (CIMS)..................................................................................
16.13 Quality of support and quality of care review processes.................................................................
16.14 Aboriginal and Torres Strait Islander cultural safety framework......................................................
16.15 The NDIS Quality and Safeguards Commission.............................................................................
16.16 Community services quality governance framework.......................................................................
16.17 Records management.....................................................................................................................
16.18 Escalation to Disability and Complex Clients Practice Advice and Support....................................
17. MACNI quality and performance reporting.....................................................................................17.1 Key performance indicators..............................................................................................................
17.2 Performance targets.........................................................................................................................
17.3 Performance reporting......................................................................................................................
18. SfHRT quality and performance reporting......................................................................................18.1 Performance targets.........................................................................................................................
18.2 Performance reporting......................................................................................................................
19. Complex needs contacts..................................................................................................................
20. Complex needs templates................................................................................................................
21. MACNI booklets................................................................................................................................
Appendix 1 Legislative requirements to be met throughout MACNI service provision...................
Page 6 Service provision framework: Complex Needs August 2019

Service provision framework: Complex Needs August 2019 Page 7

Glossary of terms
Term DefinitionBrokerage agreement
Brokerage agreements provide further detail supplementing the service agreement between the department and the agency in receipt of brokerage. The brokerage agreement complements rather than replaces a service agreement or contract with a service provider.
Capacity-building Capacity-building refers to activities that strengthen and extend the existing care planning and coordination capabilities, skills and knowledge of community service organisations through training, mentoring and secondary consultation.
Care coordination Care coordination is focused on systems collaboration for the client, rather than direct client work. It enables services to remain independent of each other while collaborating to provide an integrated response for clients. It involves the following tasks:
• providing leadership and guidance to the care team• monitoring task completion• promoting integrated service delivery • regular contact with the care team including coordinating and leading care
team meetings.
This practice is provided by Complex Needs Coordinators up to 4 hours each week (per client). Clients requiring more than 4 hours per week should be considered for Pre-MACNI or formal MACNI.
Care plan A plan which documents client needs, goals and makes recommendations about supports and interventions required, taking into account the client’s best interests, goals and working within a strengths-based framework. Care plans may specify the care, treatment, support and housing recommended for the client. These may include welfare services, health services, mental health services, disability services, drug and alcohol treatment services, housing and support services.
Care plan coordination
Care plan coordination is a client-centred, assessment-based, interdisciplinary approach to integrating health care and psychosocial support services in which a comprehensive care plan that addresses the client’s needs, strengths and goals is developed, implemented and monitored. Critical to effective care plan coordination is maintaining regular contact with the care team, including well-structured care team meetings, providing support and guidance at critical points, and monitoring to ensure tasks are completed within agreed timelines.
Typically, care plan coordination is purchased for Pre-MACNI and/or formal MACNI clients and is provided by an external service/agency. However, in some circumstances (e.g. high risk or high profile of client matters), the panel may recommend that care plan coordination remain with the department and is provided by the Complex Needs Coordinator.
Care plan development
It is a requirement that a client determined as eligible for MACNI services under the Human Services (Complex Needs) Act 2009 has a care plan developed within 12 weeks from the date of eligibility. The care plan is based on a
Page 8 Service Provision Framework: Complex Needs March 2020

Term Definitioncomprehensive assessment of the client’s needs.
Case management
Case management refers to work undertaken directly with the client based on the client’s goals and needs and specifically describes the interventions and actions to be developed to achieve the desired personal outcomes for the client. Case management is where a service provider holds responsibility for ensuring the described actions are implemented. The responsibilities of a case manager include assessment, planning, facilitation of referrals and linkages, advocacy, monitoring and review of the progress of the case management plan, and case closure.
Clients with complex needs
A complex needs client is a person who would benefit from enhanced coordination due to the presence of one or more of the following:
• there is a specific client or community safety need for which there is a limited generic service response available
• due to high-risk behaviours, complexity and/or multiplicity of the client’s support needs, additional resourcing, coordination and/or expert input is required to stabilise and continue service provision
• the development of a targeted support response to the client requires shared problem-solving, decision-making, planning and independent expert input.
Generally, clients who fit the above criteria, may not necessarily meet formal legislative eligibility for MACNI or SfHRT, nor have they been formally assessed against the eligibility criteria.
Community housing
Community housing is secure, affordable, long term rental housing managed by not-for-profit organisations for people on low incomes or with special needs. Some specialise in helping specific groups, like people with a disability, women, singles and older people and includes:
• housing associations – own properties or manage some government-owned properties. Like public housing, these organisations manage and maintain the property using their own staff.
• housing providers – primarily manage rental housing portfolios for other parties, such as the Director of Housing. Some housing providers often specialise in particular client groups.
• rooming houses – mainly accommodation for single people. Residents rent a room in the house and share common facilities such as kitchens, bathrooms and laundries.
• cooperatives – governed by voluntary tenant members with support from professional staff.
• Transitional Housing Management (THM) program- provides accommodation for up to 12 months (18 months for young people) to people who are homeless or at risk of homelessness.
• specialist housing providers – focus on particular groups, like the aged, homeless youth or people with disabilities.
Complex Needs Coordinators
The departmental role providing coordination is referred to as Complex Needs Coordinators. For the purpose of this framework, all coordinators providing MACNI, SfHRT and broader complex needs services will be referred to as Complex Needs Coordinators. Complex Needs Coordinators provide assistance to navigate the service system and offer higher-level advocacy and coordination
Service Provision Framework: Complex Needs March 2020 Page 9

Term Definitionas required.
Complex Needs Panel
Area-based panels that provide a formal mechanism for review, consultation and decision making for all clients with complex needs. Complex Needs Panels also assume specific responsibility for clients eligible for the Multiple and Complex Needs Initiative.
Complex Support Application (CSA)
The Complex Support Application (CSA) is a web-based interactive data analysis and reporting tool used by the department to visualise activity for complex needs services. The CSA enables users at a group and area level to monitor and acquit commitments and expenditure, oversee client caseloads, track against targets and undertake trend analysis.
Consultation Consultation services are provided for clients who appear to have complex support needs. The majority of people referred for consultation are supported by a Complex Needs Coordinator. The coordinator’s key tasks at this stage are:
• facilitate assessment• information and practice advice• system navigation and problem-solving• capacity-building• time-limited care coordination (<4 hours per week).
Formal MACNI Once a client is formally determined as eligible for MACNI services, care planning processes are subject to the provisions of the Human Services (Complex Needs) Act 2009. Following eligibility determination, efforts are more intensive and a care plan coordinator is appointed. An eligible client is a person who:
(a) has attained 16 years of age; and
(b) appears to satisfy 2 or more of the following criteria;
i. has mental illness within the meaning of the Mental Health Act 2014
ii. has an acquired brain injury
iii. has an intellectual impairment
iv. has a severe substance dependence within the meaning of section 5 of the Severe Substance Dependence Treatment Act 2010; and
(c) has exhibited violent or dangerous behaviour that caused serious harm to himself or herself or some other person or is exhibiting behaviour which is reasonably likely to place himself or herself or some other person at risk of serious harm, and
(d) is in need of intensive supervision and support and would derive benefit from receiving coordinated services in accordance with a care plan that may include welfare services, health services, mental health services, disability services, drug and alcohol treatment services or housing and support services.
High-risk tenancy A tenancy that is at high-risk of failure (breach or eviction) as a result of the negative impact of the tenant’s social, health and/or welfare circumstances on their ability to responsibly manage the tenancy. Indicators of a tenant’s inability to manage the tenancy include significant and/or unresolvable rent arrears, and
Page 10 Service Provision Framework: Complex Needs March 2020

Term Definitionserious tenancy breaches including anti-social behaviour and/or property damage.
Hoarding Hoarding is recognised as a diagnosable (and treatable) behavioural mental health condition. Hoarding behaviour is the persistent accumulation of, and lack of ability to relinquish, large numbers of objects or living animals, resulting in extreme clutter in or around premises. This behaviour compromises the intended use of premises and threatens the health and safety of people concerned, animals and neighbours.
Housing Integrated Information Program (HiiP)
HiiP is the primary computer system used to managed social housing in Victoria. The HiiP application provides service providers and participating registered agencies with access to the platforms that will allow them to submit and manage their housing applications and offers.
Pre-MACNI Pre-MACNI is indicated where:• a client appears to meet the Human Services (Complex needs) Act 2009
eligibility criteria• the client’s presenting issues were not able to be adequately resolved at the
consultation stage, local problem-solving and collaboration• there is evidence to suggest that a particular intervention is likely to positively
impact on the client’s situation and longer-term outcome and reduce the likelihood of needing to progress to formal MACNI.
Public housing Public housing is a form of long-term rental social housing that is managed by the government. It is for people on low incomes that are most in need, especially those who have recently experienced homelessness, family violence or have other special needs.
Service agreement The service agreement, a form of the Victorian Common Funding Agreement, sets out the key obligations, objectives, rights, and responsibilities of the organisation delivering services and the department providing funding to the organisation.
SharePoint database
The SharePoint database is a web-based Microsoft Office data entry tool used by the department to record all activity for complex needs services including client demographic details and brokerage. This data is then visualised in the Complex Support Application (CSA).
Social housing Social housing is short and long-term rental housing that is owned and run by the government or not-for-profit agencies. Social housing is made up of two types of housing, public housing and community housing. It is for people on low incomes who need housing, especially those who have recently experienced homelessness, family violence or have other special needs.
Support for High Risk Tenancies (SfHRT)
SfHRT provides a continuum of targeted support for people with multiple and complex needs who are at risk of losing their social housing tenancy. This support includes information, consultation, care coordination and/or provision of brokerage to maintain a tenancy. The target group for SfHRT are predominantly public housing tenants, however services are also offered to tenants in community housing (excludes brokerage).
Squalor Squalor describes an unsanitary living environment that has arisen from extreme and/or prolonged neglect and poses substantial health and safety risks to people
Service Provision Framework: Complex Needs March 2020 Page 11

Term Definitionor animals residing in the affected premises, as well as others in the community.
System navigation System navigation refers to tasks that enhance the capacity of the client (and the services and programs supporting them) to access available resources across multiple support systems due to service fragmentation. System navigation helps improve integration by enhancing service knowledge and increasing timely access to support for clients.
Page 12 Service Provision Framework: Complex Needs March 2020

1. Audience and purpose
The Department of Health and Human Services (the department) is responsible for the development and delivery of policies, programs and services that support and enhance the wellbeing of all Victorians. We take a broad view of the causes of ill health, the drivers of good health, the social and economic context in which people live, and of the incidence and experience of vulnerability. This allows us to place people at the heart of policy-making, service design and delivery.
The continuing presence and increase of complexity of needs in clients of the DHHS service system have highlighted the need for flexibility in the consultative role of Complex Needs Coordinators to improve responses to clients. Whilst this inclusion does not impact MACNI or Support for High Risk Tenancies (SfHRT) service responses, in some areas it may broaden the scope of Complex Needs Coordinators and Complex Needs Panels (panels).
This service provision framework: complex needs provides operational guidance to ensure consistent, transparent and high-quality delivery of complex needs services across Victoria, including MACNI and SfHRT. More specifically, the document outlines the service model, including operational processes and decision-making points for the development and implementation of complex needs services, MACNI and SfHRT in Victoria. The intended audience for this document is any person involved in providing a service response for clients with complex needs.
Complex needs services are delivered through the collaboration of government, Aboriginal community-controlled organisations, health and community service organisations to provide services to people with complex support and coordination needs.
This document is subject to ongoing revision in consideration of developments in policy, scope, process and administration.
2. Introduction
The demand to respond proactively and with flexibility to clients with complex needs is growing, reflecting the continuing presence and growing complexity in client presentation, including high-risk behaviours, complex mental health, substance misuse and greater concern for community safety. MACNI and SfHRT form specific elements of this complex needs response and each provides place-based approaches.
MACNI provides targeted, time-limited and flexible interventions to a small number of people aged 16-years and over with combinations of mental illness, substance dependency, intellectual impairment, acquired brain injury, and who pose a risk to themselves and/or others.
MACNI provides individually tailored service responses based on a comprehensive assessment of need, service system capacity and case-by-case considerations.
Focusing on a more effective and coordinated approach to support, MACNI aims to:
• stabilise housing, health, social connection and safety issues• pursue planned and consistent goals for each client• provide a platform for long-term engagement in the service system.
MACNI is funded by the Department of Health and Human Services, the Department of Justice and Community Safety, and the Director of Housing.
Service Provision Framework: Complex Needs March 2020 Page 13

SfHRT is underpinned by holistic, evidence-based approaches that improve the overall coordination of services and connectedness of the client to the support system. It aims to strengthen the service system response to public housing tenants with complex needs through integration and coordination of services to sustain tenancies at risk by:
• improving service responses to high risk tenancies• stabilising housing, health, social connection and safety issues• providing a platform for long-term engagement in the service system• identifying gaps and service development opportunities• developing a greater understanding of the needs of high-risk tenants and service response options to
promote learnings and develop good practice.
SfHRT is solely funded by the Director of Housing.
3. Complex needs model
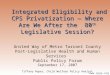
Each of the 17 areas in the department has a dedicated Complex Needs Coordinator which provides a single point of contact for service providers, clinicians or clients seeking general information about complex needs service responses/interventions or wishing to discuss a potential referral. Complex needs service responses/interventions include MACNI, SfHRT and broader complex needs responses. Upon referral, the Complex Needs Coordinator works with the referrer to consider which of the available service responses is most appropriate.
Figure 1 – The complex needs model
Page 14 Service Provision Framework: Complex Needs March 2020

3.1 Complex needsA complex needs client is a person who would benefit from enhanced coordination due to the presence of one or more of the following:
• there is a specific client or community safety need for which there is a limited generic service response available
• due to high-risk behaviours, complexity and/or multiplicity of the client’s support needs, additional resourcing, coordination and/or expert input is required to stabilise and continue service provision
• the development of a targeted support response to the client requires shared problem-solving, decision-making, planning and independent expert input.
Generally, clients who fit the above criteria, may not necessarily meet formal legislative eligibility for MACNI or SfHRT, nor have they been formally assessed against the eligibility criteria. These clients’ cases may be presented at Complex Needs Panels for discussion and allocation of brokerage funding as per Consultation procedures (set out at Section 8.2: Consultation assessment brokerage).
The Complex Needs Coordinator’s key tasks for clients with complex needs are the same as for MACNI and SfHRT consultations (Refer Section 8: Consultation). These are:
• facilitate assessment• information and practice advice• system navigation and problem-solving• capacity-building• time-limited care coordination (<4 hours per week).
Documentation required• complex needs consultation form• consent for complex needs services• complex needs recommendations / closure form.
Coordinator tasks• provide services as specified• enter client referral details into SharePoint client database• complete and provide complex needs recommendations/closure form to the referrer.
3.2 Role of Complex Needs CoordinatorThe role of the Complex Needs Coordinator will involve the following:
• facilitate service planning and coordination for clients with complex support needs, including MACNI and SfHRT clients
• provide a contact point for enquiries, information provision and referral• provide consultation and coordination of services • convene case conferences and attend meetings with other service providers / stakeholders• provide guidance and practice advice for people with multiple and complex support needs including
information on potential referral sources and pathways• partner with service providers to develop integrated responses and promote practice excellence• present client information and advice to panels to assist in decision-making and problem-solving• manage information across areas, groups, funded services, panels and Disability and Complex
Clients Practice Advice and Support unit• manage brokerage processes in line with procurement guidelines, including brokerage agreements
Service Provision Framework: Complex Needs March 2020 Page 15

• negotiate and manages effective communication between panels and care plan coordinators• collate information on systemic issues and barriers identified by panels• implement/support the implementation of the decisions of the panel with care plan coordinators• support the effective operation of each panel meeting• identification of systems gaps, risk factors and training opportunities that will improve service systems
for clients with complex needs• undertake environmental scans of department partnerships and local service innovations to identify
examples of service collaboration for clients displaying complex behaviours• identify and support the implementation of training opportunities that respond to the needs of housing
and homelessness staff working with tenants whose level of complexity places their tenancy at risk• coordinate responses to hoarding and squalor to assist in the sustaining of tenancies and provide
practice advice• update the SharePoint/CSA databases.
3.3 Service integration and capacity buildingComplex Needs Coordinators are required to facilitate relationships between program areas and services, as well as provide capacity building regarding support provision for clients with complex needs. This aims to enhance the service system capacity through cross-program and service partnerships and collaborative practice, thereby ensuring the client is able to receive adequate support from the existing service system. This includes service integration and capacity building activities such as:
• secondary consultation• job shadowing• targeted training or skill development• mentoring• use of brokerage funds to purchase secondary consultation, specific training, specialist clinical staff
support or mentoring in accordance with the care plan and to build service capacity in the longer term.
Capacity building is provided in two forms;• develop a service provider’s capacity/expertise to deliver services for clients with complex needs;
and/or• develop a care team’s skill/expertise to work with a particular complex client presentation.
Capacity building activities are required to be recommended by the Complex Needs Panel and the panel will maintain a level of oversight over these activities. The Disability and Complex Clients Practice Advice and Support unit must also be notified of capacity building activities including service gaps, learnings and examples of best practice.
Coordinator tasks• analyse data on SharePoint/CSA to identify systemic issues and/or service gaps • provide or recommend targeted training in response to systemic issues or service
gaps e.g. hoarding and squalor, implementing behavioural interventions, etc. • ensure capacity building activities are recommended by the Complex Needs Panel• notify the Disability and Complex Clients Practice Advice and Support unit of capacity
building activities
3.4 Exclusions to Complex Needs services responseComplex Needs service responses do not:
Page 16 Service Provision Framework: Complex Needs March 2020

• provide a case management response• offer ongoing direct service engagement to tenants requiring support• offer an emergency or crisis service• offer to pay client debts• replace existing supports.
3.5 Transfer of clients between areasClients may move between areas for a variety of reasons and in making that move, may require support above, below or different to the supports they currently receive. Some moves are temporary, and others are intended to be long-term. The transfer process for clients who move between areas is focused on continued service responsiveness to the client.
Where a client supported by the complex needs team transfers between areas during the period of an approved care plan with the attached brokerage, the funding commitment for the approved period is transferred from the exiting to the receiving area. Any subsequent care plans are subject to the approval processes of the receiving area.
3.5.1 Principles of client transferEffective client transfer relies on the positive interpretation and implementation of the following principles:
• the best interests of the client are the outcome of cooperative, clear and direct inter-area transfer negotiation and agreement
• clients access flexible, personalised and integrated services irrespective of a move between areas• clients’ needs and interests are the primary consideration in negotiating a transfer across areas• communication and planning about the transfer of services involves the client (as possible) to ensure
their input and understanding• the area best able to promote the client’s best interests, continuity and stability is the area to have
lead responsibility, and this is usually the area in which the client resides• the transfer of lead responsibility ensures minimum disruption of service delivery to the client,
including the transfer of all current financial year brokerage commitments for the client to enable service continuity
• transfers occur in a planned way irrespective of whether the client move was planned.
3.5.2 Transient/unsettled clientsIf a client is transient or highly mobile, the Complex Needs Coordinator, with any lead department program staff, considers the following factors to determine which area maintains lead responsibility for complex needs services, the:
• preference of the client• services the client requires• area to which the client frequently returns• location of significant community connections/family members.
When an area becomes aware of a client move, immediate direct communication is commenced between the two area Complex Needs Coordinators.
If it is unclear how long a client will reside in the new area, it is reasonable to deem them as settled after eight weeks and following a stated intention to remain.
In the interim, the Complex Needs Coordinators from the two areas establish transfer meetings within two weeks of the alert date and determines tasks for transfer until the receiving area is on board.
Service Provision Framework: Complex Needs March 2020 Page 17

To allow time for the client to settle into a new area, the transfer of services and lead management by the receiving area is concluded within three months from the initial transfer date.
To support service continuity under the care plan, a transfer between areas is effected with the transfer of funding of the existing care plan for the remaining financial year.
3.5.3 Clients in or to be released from a state-wide facilityWhen a client is in, or to be released from a state-wide facility, the lead area to manage the MACNI services (coordination of care planning) should be the client’s area of origin until a clear plan is developed which includes a medium to long-term placement. Consistent with Section 3.5.2, if it is unclear how long a client will reside in the new area, it is reasonable to deem them as settled after three months and following a stated intention to remain.
Documentation required• all relevant documentation (current and historical) including:
– care plans– assessments– Complex Needs Panel minutes– brokerage history and documentation– care team contact details
• a handover document may be created if requested.
Coordinator tasks• schedule discussion of transfer with Complex Needs Coordinator from the new area.
The handover discussion should focus on:– current and key priorities/critical issues/focus of the care plan– outstanding tasks– recommendations from the Complex Needs Panel– brokerage expenditure to date, including any outstanding payments– transfer of brokerage– meeting schedules
• ensure all appropriate documentation is securely transferred • update the SharePoint client database to reflect the transfer• schedule follow-up discussions with the new area as required• attendance at out-of-area Complex Needs Panels may be required.
4. MACNI legislation
MACNI is underpinned by the Human Services (Complex Needs) Act 2009 (the Act) which establishes the authority for a coordinated approach to planning service delivery for people with multiple and complex needs.
However, while complex needs services do not operate under specific legislation, practice aligns with the provisions for coordination of services consistent with the Human Services (Complex Needs) Act 2009. The Act outlines the following principles with respect to, the determination of eligibility and the development and implementation of a care plan:
Page 18 Service Provision Framework: Complex Needs March 2020

• the wellbeing, health, safety and stable housing of the client are of paramount in the development of a care plan
• the development of a care plan is based on a comprehensive assessment of the client’s needs• the provision of welfare, health, mental health, drug and alcohol treatment and housing and support
services to the client is best achieved when those services are coordinated and when service providers share relevant personal information or health information about the client
• welfare, health, mental health, drug and alcohol treatment and housing and support services provided in accordance with a care plan are delivered by the relevant service providers in a coordinated manner.
For further information on the scope of the Act refer Human Services (Complex Needs) Act 2009 on the Victorian Legislation and Parliamentary Documents website <http://www.legislation.vic.gov.au/>
4.1 Instrument of delegationUnder the Human Services (Complex Needs) Act 2009, the Secretary of the department holds the powers and functions to enact the provisions for the operation of MACNI. To allow for the effective implementation of MACNI, the Act enables the Secretary to delegate any power or function of the Secretary, except for the power of delegation. To give practical effect to the operation of MACNI, an instrument of delegation specifies the delegation of powers and functions to nominated departmental officers.
Refer: Human Services (Complex Needs) Act 2009 on the Delegations Intranet page <https://intranet.dhhs.vic.gov.au/delegations>
4.2 MACNI eligibility criteriaAn eligible client is a person who:
(a) has attained 16 years of age; and
(b) appears to satisfy 2 or more of the following criteria;
i. has mental illness within the meaning of the Mental Health Act 2014
ii. has an acquired brain injury
iii. has an intellectual impairment
iv. has a severe substance dependence within the meaning of section 5 of the Severe Substance Dependence Treatment Act 2010; and
(c) has exhibited violent or dangerous behaviour that caused serious harm to himself or herself or some other person or is exhibiting behaviour which is reasonably likely to place himself or herself or some other person at risk of serious harm, and
(d) is in need of intensive supervision and support and would derive benefit from receiving coordinated services in accordance with a care plan that may include welfare services, health services, mental health services, disability services, drug and alcohol treatment services or housing and support services.
4.2.1 Interpretation of diagnostic criteriaSince the inception of MACNI, it has been recognised that the interpretation of the eligibility criteria relies on an inclusive position with respect to criterion b) (i) (ii) (iii) (iv) to ensure the intent of the legislation and initiative is met. That is, that it is available to those most in need and is used for people where significant effort to assist has been unsuccessfully tried by the current service system. The role of the panel is not to determine eligibility only against formal diagnoses made by a professional.
Service Provision Framework: Complex Needs March 2020 Page 19

Many clients have histories of numerous assessments and associated diagnoses that have remained with them over their life and experience with services. These clients may be presented to MACNI with a clear diagnosis. For these clients, a panel may determine that the diagnostic eligibility criteria are met and further assessments are not needed. In some cases, due to the plethora of assessments (and potentially diagnoses), a panel may determine that a synthesis of existing information for the purpose of developing tailored interventions is required.
For other presenting clients, evidence of prior assessments and diagnoses may not be available, or the available information may contain contradictions that necessitate further integrated assessment. In these scenarios, relying on the words from the legislation - appears to have - enables the use of judgement about the apparent nature of the person's diagnoses which errs on the side of inclusion. At this point, the intent of MACNI is to assist the stabilisation of clients through the coordination of services, and for some clients, this is more likely to be achieved by an integrated comprehensive assessment which has not been previously undertaken. The lack of clarity, despite the appearance of characteristics and behaviours indicating potential diagnoses, is a contributing factor to the lack of coordination for the client.
In further support of the need for less stringent interpretation of eligibility, is the requirement to establish diagnoses consistent with the definitions of `mental illness’ and `severe substance dependence’ in the Mental Health Act 2014 and Severe Substance Dependence Treatment Act 2010.
Both Acts provide definitions with the purpose of narrowly establishing the requirements for the compulsory/mandated treatment of persons. Section 4 of the Mental Health Act 2014 defines mental illness as `…a medical condition that is characterised by a significant disturbance of thought, mood, perception or memory’. The Act establishes a supported decision-making model that will enable and support compulsory patients to make or participate in decisions about their treatment and determine their individual path to recovery. The Severe Substance Dependence Treatment Act 2010 targets a very small group of people affected by the most severe substance dependence who urgently require treatment to save their lives or prevent serious damage to their health. Section 5 of the Act defines that a person has a ‘severe substance dependence’:
(a) if the person has a tolerance to a substance; and
(b) the person shows withdrawal symptoms when they stop using or reduce the level of use of, the substance; and
(c) the person is incapable of making decisions about his or her substance use and personal health, welfare and safety due primarily to the person’s dependence on the substance.
The respective definitions enable an area panel to use its collective professional knowledge and experience to consider the available information about the client and the reliability of the view of the engaged services. The area panel’s role is to establish an `apparent’ presence of diagnostic criteria, even if it to the extent that the panel notes information deficiencies/contradiction that require attention (for clarification) during the development of a care plan.
5. Department of Health and Human Services
The department has responsibility for developing and delivering policies, programs and services that support and enhance the wellbeing of all Victorians.
These activities include housing and community services and programs, public health services, public hospitals, health, mental health and aged care services, and sport and recreation in metropolitan, rural and regional Victoria.
Page 20 Service Provision Framework: Complex Needs March 2020

The department takes a broad view of the causes of ill health, the drivers of good health, the social and economic context in which people live, and the incidence and experience of vulnerability. This places people at the heart of policy-making, service design and delivery.
5.1 Strategic directionsThe department has four strategic directions:
5.1.1 Person-centred services and careMany factors influence a person’s ability to experience a good life – family context, educational outcomes, housing, social support, work opportunities and workplaces, access to transport and recreational opportunities. Person-centred services and care consider all the influences on a client’s health and wellbeing.
The department designs services and funding models around people and their families. This means:
• enabling people to look after themselves better• fostering meaningful relationships that help people improve their health• enabling people to work collaboratively with professionals as equal partners in their care• person-centred care considers the whole client to understand their physical, cultural and social
context.
5.1.2 Local solutions The department involves people and communities in the design and planning of services, and we align service efforts with other community activities. This means:
• taking place-based and community-centred approaches• developing new service models that take into account existing services and infrastructure, cultural
considerations and the long-term implications of investment decisions• engaging collaboratively with evolving local partnerships to build relationships, share knowledge and
data, and jointly plan local and community actions.• local solutions acknowledge that the government alone does not have the answers – we need to work
with others to ensure effective outcomes.
5.1.3 Earlier and more-connected support The department works to prevent health and wellbeing problems before they become too big, and we tailor service responses so they meet the needs of people and their families. This means:
• getting in early to help people build resilience• making services easier to navigate• breaking down the barriers within and across sectors.A key focus of this strategic direction is to support universal services to be more effective in identifying and responding to risk and vulnerability, and more active in linking clients and families to specialist services.
5.1.4 Advancing quality, safety and innovationThe department monitors, and works to improve, the quality and safety of health and community services, and works with partners to build evidence, share knowledge, scale effective practice and support practice development and change.
Under this strategic direction, we are:
Service Provision Framework: Complex Needs March 2020 Page 21

• making sure the people who work in health and human services are qualified and have the right mix of skills
• better measuring and reporting on quality, safety and client/patient experience and outcome data so we can intervene quickly when we identify poor performance
• engaging clinicians and practitioners in the design and implementation of improvement initiatives and building a culture that puts quality and safety first
• seeking improvements and innovations, evaluating what we do, and reducing unacceptable variations in care and outcomes.
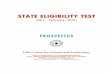
5.2 Groups and areasThe department consists of four groups responsible for oversight and coordination of local areas (see Figure 1). Complex Needs Coordinators seek to support the efforts of local areas to establish innovative, localised and timely responses to people with complex service requirements.
Consistent with localised service delivery principles, people are supported by the group and area they are most connected to. This is typically determined by the client’s residential address and existing support relationships, or at times of itinerancy or custody, the place the client identifies as preferable.
Figure 2 – Department of Health and Human Services group and area structure
5.3 Governance and responsibilitiesAccountabilities and responsibilities that underpin the effective implementation of the complex needs framework are as follows:
Group / Business Area Actions and responsibility
Disability and Complex Clients Practice Advice and Support unit, Office of Professional Practice, Community Services Operations Division, DHHS
• provides oversight, policy direction and guides interdepartmental processes
• provides learning and development initiatives• provides broader sector engagement including facilitating
Statewide forums• responsible for budget allocation and monitoring• monitors adherence to service provision framework:
complex needs• monitoring group and area performance and brokerage
Page 22 Service Provision Framework: Complex Needs March 2020

Group / Business Area Actions and responsibility
expenditure• data collection and analysis• liaison with the Director of Housing and Department of
Justice and Community Safety (DJCS)• policy and procedure development, including updates to the
service provision framework: complex needs• identifying opportunities and implementing strategies to
facilitate interdepartmental and sector collaboration and coordination for integrated service delivery and improved client outcomes
• analyse trends, service system gaps and systemic issues (including those identified by Complex Needs Panels and MACNI closure reports) and escalate to the Client Support and Housing Services Executive Group as required
• providing high-level, strategic advice on systemic issues impacting on client service access and outcomes
• leading and influencing policy, practice and actions to address systemic issues
• improving the planning, delivery and monitoring of services to clients across departments, including review of complex needs data, performance and capacity building activities.
Department of Justice and Community Safety (DJCS)
• provides funds for MACNI service provision• facilitates referrals to MACNI in consultation with DHHS
Complex Client coordinators, build capabilities and collaborative networks with service providers to enable access to local services for MACNI clients.
• attends Panels and provide expert advice on services and supports within the state-wide justice system and collaborate in the development of service system responses to address identified service gaps for dual DJCS and MACNI clients
• facilitates access to service provision where clients with complex needs are engaged in Community Corrections
• ensures that relevant staff with responsibility for policy and operations are engaged in responding to identified systemic issues and service responses to client clients.
Director of Housing • provides funds for MACNI and SfHRT service provision• facilitates early identification of potential clients with complex
needs and their referral• provides advice about local services and supports in the
housing system for clients with complex needs• supports problem-solving for complex needs cohorts
through participation on Panels.
Assistant Director Child Protection, Area Based, DHHS
• facilitates early identification of potential clients with complex needs and their referral
• provides advice about local services and supports in the child protection system for clients with complex needs
Service Provision Framework: Complex Needs March 2020 Page 23

Group / Business Area Actions and responsibility
• supports problem-solving for complex needs cohorts through participation on Panels.
Client Support and Housing Services Executive Group
• consideration of, and advice on issues such as housing reform and initiatives, public housing, funded housing services (i.e. homelessness services, MACNI, SfHRT, reception, client experience, and design and implementation imperatives related to organisation change
• oversight of key projects and initiatives related to the above programs
• provide advice and make recommendations for Divisional Strategic Oversight and Coordination Committee (DSOC) decisions
• oversight and consideration of relevant work and projects within other related state-wide governance groups
• consider how client services and housing initiatives are integrated across the department
• analysis and advice on other issues requested by DSOC, including a regular report back to DSOC
• oversee relevant networks and groups that enable continuous improvement of client support and housing services, including but not limited to:– Housing Operations and Performance and Finance
Reporting Group– Client Support and Housing Services Managers’ State-
wide Group– Tenancy and Property and Housing Advice and
Assistance Team Managers’ Group• liaise with other Executive Groups when required or when
relevant.
Complex Needs Coordinator, Area Based, DHHS
• facilitates service planning and coordination for clients with complex support needs, including MACNI and SfHRT clients
• provides a contact point for enquiries, information provision and referral
• provides consultation and coordination of services • convenes case conferences and attend meetings with other
service providers / stakeholders• provides guidance and practice advice for people with
multiple and complex support needs including information on potential referral sources and pathways
• partners with service providers to develop integrated responses and promote practice excellence
• presents client information and advice to panels to assist in decision-making and problem-solving
• manages information across areas, groups, funded services, panels and central office
• manages brokerage processes in line with procurement
Page 24 Service Provision Framework: Complex Needs March 2020

Group / Business Area Actions and responsibility
guidelines, including brokerage agreements• negotiates and manages effective communication between
panels and care plan coordinators• collates information on systemic issues and barriers
identified by panels• implements/supports the implementation of the decisions of
the panel with care plan coordinators• identification of systems gaps, risk factors and training
opportunities that will improve service systems for clients with complex needs
• supports the effective operation of each panel meeting• undertake environmental scans of department partnerships
and local service innovations to identify examples of service collaboration for clients displaying complex behaviours
• identify and support the implementation of training opportunities that respond to the needs of housing and homelessness staff working with tenants whose level of complexity places their tenancy at risk
• coordinate response to hoarding and squalor to assist in the sustaining of tenancies and provide practice advice
• updates the SharePoint databases fortnightly.
5.4 Complex Needs PanelsEach departmental area operates a Complex Needs Panel (panel) that meets on a regular schedule (monthly/ bi-monthly or quarterly). The panel provides a collaborative forum for the discussion of service delivery options for clients with complex needs. The panel considers and aims to address the needs of clients who pose significant challenges for the service system and community, and who are likely to require an extraordinary response to meet their needs. Panels provide a formal mechanism for review, consultation and decision making for all complex needs clients, including MACNI and SfHRT. Panels assume specific responsibility for clients eligible for the Multiple and Complex Needs Initiative (MACNI) including MACNI consultations, Pre-MACNI and formal MACNI clients.
A panel has both a client and a systems focus. From a client perspective, the role of the panel is to review, question and provide feedback on client care plans and promote opportunities for cross-department/cross-organisation collaborations to achieve client outcomes. From a systems perspective, the panel's role is to provide advice and direction on broader policy or service delivery matters relating to each member's service/program area and to undertake systems and trend analysis to influence strategic thinking regarding clients with complex needs.
The Act does not give panels specific functions or powers. Panels provide authoritative advice, support and recommendations pertaining to client matters to the Area Director who holds delegated functions and powers.
5.4.1 ResponsibilitiesThe key roles and responsibilities of the panel are:
Service Provision Framework: Complex Needs March 2020 Page 25

• evaluate the effectiveness of care plans intended to promote holistic, innovative, flexible, client-centred and value-for-money service responses
• consider eligibility, recommend, vary and terminate care plans for the Multiple & Complex Needs Initiative according to the Act
• consider, recommend and review brokerage for clients with complex needs, including SfHRT consultations (for requests over $25,000 only), MACNI consultations, Pre-MACNI and formal MACNI clients
• consider, recommend and review capacity building activities in the area which are lead by Complex Needs Coordinators
• escalate systemic issues and trend analysis findings to the Disability and Complex Clients Practice Advice and Support unit
• enhance the service system capacity through cross-program and service partnership and collaborative practice
• empower and support practitioners to problem solve client and service system issues through robust discussion and critical reflection.
5.4.2 Membership Panels are typically comprised of the following representation:
• Area Director, DHHS (chair)• Assistant Director Child Protection Operations / Operations Manager, Child Protection / Principal
Practitioner, Child Protection, Area / Group, DHHS• Manager, Disability and Complex Clients Practice Advice and Support, DHHS• Manager, Client Support and Housing Services, Area, DHHS• Senior Advisor/Manager, Population Health & Community Wellbeing, Area, DHHS• Principal Disability Practice Adviser, Area/Group, DHHS• Manager, Agency Performance and System Support, Area, DHHS• Manager, Community Correctional Services, Region/Area, DJCS• senior staff from the Department of Justice and Community Safety and other departments as required• Director / Senior Manager, Area Mental Health Service• Director / Senior Manager, Drug and Alcohol Service• Director / Senior Manager, Youth and/or family Service• 1 - 3 senior representatives of partner sector organisations (examples include the following service
areas; homelessness, community mental health, offender support, neuropsychology, Aboriginal Controlled Community Organisations)
• an Aboriginal advisor should be present when discussing an Aboriginal or Torres Strait Islander clients.
Areas determine their panel membership and choose the breadth and number of representatives. The precise make-up of each panel will depend on the local needs of each area, member availability and interest as well as the need to ensure consistency and place a limit on group numbers.
Panels may also invite independent expert advisers to participate in meetings on a case-by-case basis and as determined necessary according to subject expertise.
Given the nature, membership and role of panel, client/family members/guardian participation is not recommended. Where beneficial, a member of the care team may provide a summary of panel recommendations to the client/family members/guardian.
Page 26 Service Provision Framework: Complex Needs March 2020

5.4.3 Meeting procedures and accountability Each panel has established terms of reference which detail the operation of Complex Needs Panels including dispute resolution, quorum, accountability and reporting procedures.
On quorum, it is anticipated that the quorum determination will use established models of 51 per cent of the membership and be marked by a balance of the panel members.
Panels record each session and document client-related decisions and actions including the allocation of brokerage. The Complex Needs Coordinator reports to the panel with client activity and brokerage budget updates as relevant. Standardised templates for panel reporting are included in the Appendix.
Documentation required
Standing documents
• Complex Needs Panel information pack checklist• Complex Needs Panel manual• Complex Needs Panel terms of reference• Complex Needs Panel member prompt sheet• Complex Needs Panel deed of confidentiality
Before each panel
• Complex Needs Panel agenda• brokerage notification template (optional)• brokerage documentation
Following each panel
• Complex Needs Panel minutes• Complex Needs Panel session report• brokerage documentation• memorandums as required.
Coordinator tasks
Annual tasks
• provide panel members with documents listed on the Complex Needs Panel information pack checklist
• renew panel documentation and membership agreements annually or as required.
Before each panel
• schedule panel dates, sending invitations to panel members and care team members• prepare and circulate the panel agenda (minimum five business days prior)• circulate all documentation to panel members (minimum five business days prior)• assist in the preparation of care plans• prepare brokerage requests and/or notifications• prepare care plan coordinators and care team members to present to Panels• meet with the Area Director to confirm all brokerage requests are within budget• ensure the deed of confidentiality is signed by all attending panel members.
Following each panel
Service Provision Framework: Complex Needs March 2020 Page 27

• prepare and circulate panel minutes and session report to panel members and care teams
• prepare memorandums as required• prepare brokerage agreements as required• update the SharePoint databases with the relevant care plan dates (in client database)
and brokerage• ensure panel recommendations are addressed in care plans.
5.4.4 Out of sessions requestsOut-of-session requests are requests that could not be presented at panel due to being unavailable at the time of the most recent scheduled date. Out of session requests may occur in relation to:
• formal MACNI eligibility consideration requests• the appointment of a care plan development or care plan coordination provider• care plans (new, variations or closures)• brokerage requests.The Complex Needs Coordinator is responsible for circulating the out of session request to all panel members. Queries surrounding the requests can be directed to the Complex Needs Coordinator for a response.
If a unanimous decision cannot be reached, the Chair will make the final decision.
Documentation required• Complex Needs Panel out of session request form• any documentation relevant to the out of session request (e.g. MACNI eligibility
consideration request form, care plans, brokerage request form)
Coordinator tasks• ensure the out of session request form is completed• consult with the Area Director to ensure brokerage requests are within the allocated
area/group complex needs budget• email the complex needs panel members the request, clearly indicating the date
responses are due by• seek Area Director approval as relevant.
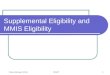
6. Multiple and Complex Needs Initiative (MACNI)6.1 Operating modelMACNI provides a range of targeted supports for people with multiple and complex needs ranging from information, consultation, coordination and referral through to care plan development and coordination for those determined eligible under the Act. Figure 3 illustrates the MACNI service model.
At any stage of MACNI intervention where a critical need arises, the Complex Needs Coordinator will work with the involved services and Panel to determine the most appropriate level of support. Similarly, a case may be closed at any stage or duration of involvement and are not required to progress through stages before closure is recommended.
Page 28 Service Provision Framework: Complex Needs March 2020

The MACNI model is not strictly linear; at any stage, it may become apparent that the client’s needs cannot be effectively met without a higher level of coordination or intervention. At this point, the Complex Needs Coordinator will work with the involved services to determine the next steps of either a referral for:
• Pre-MACNI• MACNI eligibility determination to receive care plan coordination under the Act.
Standardised templates are provided in the appendix to assist Areas implement MACNI at a local level. These templates are to be used by all Complex Needs Coordinators to enhance consistency and promote adherence to legislation and operational guidelines. Where appropriate, templates can be adjusted to each client’s communication capacity and may benefit from pictorial representations and/or translation.
Figure 3: MACNI overview
7. Identification and referral
Service providers may struggle to identify or establish effective supports for a client with complex needs. In these instances, service providers can contact the Complex Needs Coordinator in the relevant department area and request a consultation. Initial contact can occur in a number of ways, but typically the referring agency or program will be asked to complete a consultation form for consideration and review. This enables the coordinator to gain an understanding of the client’s support needs as well as potential service responses or gaps.
Each response to a request for assistance is individually tailored and based on an assessment of client need, care team functionality, risk analysis and other case-by-case considerations. In addition, the
Service Provision Framework: Complex Needs March 2020 Page 29

service system’s capacity to effectively respond to the client’s support needs is a key consideration at this stage and the Complex Needs Coordinator routinely reflects on the progress of tested interventions and service responses.
It is important to note that complex needs intervention is intended as a time-limited response to a client’s high and complex support needs. The focus of the initial consultation is to strengthen and enhance the sustainability of existing service system responses and to reduce the need for over-reliance on time-limited and high-cost support.
The period of time that a Complex Needs Coordinator is engaged with service providers will vary depending on (but is not limited to): the client’s specific circumstances; the level, type and quality of service provider collaboration and agreement; and the availability of suitable supports.
Documentation required
• complex needs consultation form
• consent for complex needs services.
Coordinator tasks• determine which service response is most appropriate (SfHRT, MACNI or broader
Complex Needs response)• reinforce that complex needs interventions are not a crisis response but offer
comprehensive coordination and monitoring when a client’s support needs are high and facilitated multi-service responses are required
• establish whether the client has provided consent for information-sharing • establish the client’s usual or intended place of residence or preference (to ensure the
correct area provides the lead)• determine the service system’s capacity to effectively respond to the client’s support
needs through exploration of available and considered options of support• provide information and advice on support that can be provided, alternate options
and/or next steps.• update the SharePoint client database• provide services as specified.
7.1 Aboriginal and Torres Strait Islander peopleThe department’s Koolin Balit sets out what the department, together with Aboriginal communities, other parts of government and service providers, will do to achieve the government’s commitment to improving Aboriginal health.
Complex needs interventions support the government’s objectives in working to improve access to services and outcomes for Aboriginal people. From consultation to care planning, intervention supports Aboriginal people to strengthen connection to culture and community.
Complex Needs Coordinators work closely with Aboriginal services and communities where a client’s challenging behaviour may have resulted in service or community access barriers, including joint-problem-solving on culturally appropriate interventions and supports. Complex needs intervention actively supports people to access both the mainstream existing service system and Aboriginal-specific services provided by Aboriginal community-controlled organisations, including alcohol and drug treatment services, healing and health services.
Refer Koolin Balit: Victorian Government strategic directions for Aboriginal health 2012-2022 <https://www2.health.vic.gov.au/about/health-strategies/aboriginal-health/koolin-balit>
Page 30 Service Provision Framework: Complex Needs March 2020

Refer: Aboriginal and Torres Strait Islander cultural safety framework <https://dhhs.vic.gov.au/publications/aboriginal-and-torres-strait-islander-cultural-safety-framework>
8. Consultation
Consultation services are provided for clients who appear to have complex support needs or have not yet met eligibility criteria for MACNI or SfHRT. The majority of people referred for consultation are supported by a Complex Needs Coordinator. The coordinator’s key tasks at this stage are:
• facilitate assessment• information and practice advice• system navigation and problem-solving• capacity-building• time-limited care coordination (<4 hours per week).
The Complex Needs Coordinator uses a Consultation form to assist to determine the client’s suitability for support (as at Section 7 – Identification and referral). Once completed by the referrer, the Complex Needs Coordinator will assess and provide confirmation about the support to be provided.
The consultation process is intended to complement and enhance service delivery rather than replace or duplicate available service responses. The primary function of consultation is to improve client outcomes through direct support and guidance to engaged services to maximise flexibility and responsiveness of support options. The focus of the consultation is to strengthen the sustainability of the existing service system. At the consultation stage, support may be provided to seek client diagnostic clarification and/or gain service system access.
During the consultation stage, it may become apparent that the client’s needs cannot be effectively met without a higher level of coordination or intervention. At this point, the Complex Needs Coordinator will work with the involved services and the Panel to determine the next steps of either a referral for:
• Pre-MACNI • MACNI eligibility determination to receive formal care plan coordination under the Act• SfHRT or other service response.
Documentation required• complex needs consultation form• consent for complex needs services• complex needs recommendations / closure form.
Coordinator tasks• update SharePoint client database• provide services as specified • provide complex needs recommendations/closure form to the referrer.
8.1 Complex Needs Panel involvementConsultation clients may be presented to panels by the Complex Needs Coordinator for expert advice on service planning, monitoring and the identification of systemic issues. Not all consultation clients are required to be presented, however, the panel should be consulted where there are:
Service Provision Framework: Complex Needs March 2020 Page 31

• particularly challenging or unusual circumstances• systemic issues• concerns around risk management.
8.2 Consultation assessment brokerageConsultation support includes the capacity to use client-attached assessment brokerage of up to $25,000 in a 12-month period. This brokerage can only be used to purchase specific assessments that are needed to assist with service planning or service system access.
All requests for assessment brokerage must be recorded on a brokerage request form and approved by the appropriate financial delegate. The panel is required to be notified of brokerage requests at the next scheduled meeting.
Documentation required• brokerage request form.
Coordinator tasks• ensure the brokerage request form is prepared• follow appropriate brokerage approval procedure• notify assessment brokerage expenditure to the Complex Needs Panel• update SharePoint brokerage database.
8.3 Consultation closureConsultation services should be considered for closure in the following circumstances:
• the matter is believed to be resolved, and/or• the involved services have not required further consultation support for 3 months• no further tasks have been generated for the Complex Needs Coordinator for 3 months• the client decides to withdraw
The client can be re-referred at a later point in time as the need arises. If the client is re-referred, a new consultation record is opened (ensuring client details are updated), reflecting the current reason/goal of consultation, current service system issues and current service involvement.
Documentation required• complex needs recommendations/closure form.
Coordinator tasks• complete and provide complex needs recommendations/closure form to the referrer • contact referrer to advise of the closure • update the SharePoint client database, ensuring the closure date is recorded.
Page 32 Service Provision Framework: Complex Needs March 2020

9. Pre-MACNI
Pre-MACNI is indicated where:
• a client appears to meet the Human Services (Complex Needs) Act 2009 eligibility criteria (does not require to be confirmed by formal assessment)
• the client’s presenting issues were not able to be adequately resolved through consultation, local problem-solving and collaboration
• the client and care team would benefit from time-limited care coordination (<4 hours per week)• there is evidence to suggest that a particular support intervention is likely to positively impact on the
client’s situation and longer-term outcome and can only be achieved through the use of Pre-MACNI brokerage funding.
Based on the above, a Pre-MACNI response may be considered by the Complex Needs Coordinator.
Documentation required• complex needs consultation form• consent for complex needs services• complex needs recommendations / closure form.
Coordinator tasks• update the SharePoint client database• provide services as specified • provide complex needs recommendations/closure form to the referrer.
9.1 Complex Needs Panel involvementPre-MACNI clients may be presented to the panel by the Complex Needs Coordinator for expert advice on service planning, monitoring and the identification of systemic issues. Not all Pre-MACNI clients are required to be presented, however, the panel should be consulted where there are:
• particularly challenging or unusual circumstances• systemic issues• brokerage expenditure that requires noting• concerns around risk management.
For some people, the use of Pre-MACNI is determined to be an insufficient level of coordination to meet their needs and goals. For some, this will be determined after the approach has been tried; while for others, evidence indicates that a higher level of coordination and care planning is required and a formal referral to MACNI is initiated.
9.2 Pre-MACNI brokeragePre-MACNI support can include the use of client-attached brokerage funding of up to $15,000 in a 12-month period. This brokerage can be used to enhance support by increasing service or assessment options and can enable the development of an intervention/approach that may effectively resolve the matter. The brokerage funding can be used to purchase time-limited care plan coordination and supports to interrupt a significant crisis, trial a new approach or prevent further escalation of need at a local level.
All requests for brokerage must be recorded on a brokerage request form and approved by the appropriate financial delegate. Notification of brokerage expenditure is required to be provided to the
Service Provision Framework: Complex Needs March 2020 Page 33

panel at the next scheduled meeting date. The use of brokerage must be documented within the care plan, including the service provider and dates of service provision. If no suitable care plan (developed by another service provider) exists, Complex Needs Coordinators should ensure a care plan is developed using the Complex Needs Care Plan template.
Documentation required• the care plan must reflect the use of brokerage• brokerage request form• brokerage agreement form (as required).
Coordinator tasks• if no care plan exists, ensure a care plan is developed to reflect the use of brokerage
using the Complex Needs Care Plan template• if a suitable care plan exists, ensure the care plan is updated to reflect the use of
brokerage• ensure the brokerage request form is prepared • follow appropriate brokerage approval procedure• notify the Complex Needs Panel of brokerage expenditure• update the SharePoint brokerage database.
9.3 Pre-MACNI closurePre-MACNI services should be considered for closure in the following circumstances:
• the matter is believed to be resolved, and/or• the involved services have not required further consultation support for 3 months• no further tasks have been generated for the Complex Needs Coordinator for 3 months• the client decides to withdraw
The client can be re-referred at a later point in time as the need arises. If the client is re-referred, a new consultation record is opened (ensuring client details are updated), reflecting the current reason/goal of consultation, current service system issues and current service involvement.
Documentation required• complex needs recommendations/closure form.
Coordinator tasks• contact referral to advise of the closure• update the SharePoint client database, ensuring the closure date is recorded • provide complex needs recommendations/closure form to the referrer.
Page 34 Service Provision Framework: Complex Needs March 2020

10. Formal MACNI services
When a referral to formal MACNI is recommended, care planning and processes are subject to the provisions of the Human Services (Complex Needs) Act 2009.
Documentation required• complex needs consultation form• consent for complex needs services.
Coordinator tasks• update SharePoint client database• provide services as specified.
Figure 4: Key MACNI process considerations
Clients are required to provide consent at each stage of MACNI
Panels make eligibility, care planning and brokerage recommendations
Approval decisions are made consistent with the Instrument of Delegation and Financial Management Act 1994
Eligibility determination outcomes must be provided to clients in writing
Approved care plans must be provided to the clients
Clients to be informed of their right to cease involvement at any time
Clients to be informed of personal information being shared
10.1 EligibilityPrior to being considered for eligibility, there are multiple notification requirements under the Act. A standardised eligibility consideration letter is provided/sent to the client to seek their consent for the consideration of eligibility, including a consent for eligibility determination form. Once the panel considers and recommends (as relevant) the referral, Area Director approval is required. A standardised eligibility outcome letter is then sent to the eligible client.
Documentation required
Prior to Panel
• MACNI eligibility consideration notification – letter to client• consent for MACNI referral and eligibility consideration – client • MACNI eligibility consideration request form
Following Panel
• MACNI eligibility decision notification – letter to client.
Service Provision Framework: Complex Needs March 2020 Page 35

Coordinator tasks• obtain client consent (liaise with the key worker)• complete MACNI eligibility consideration request form• ensure the above eligibility notification requirements are satisfied• prepare notification letters and obtain Area Director signature• update SharePoint client database, ensuring the start date reflects the date eligibility
was recommended at panel and approved by the Area Director.
10.2 Care plan developmentIt is a requirement that a client determined as eligible for services under the Human Services (Complex Needs) Act 2009 has a MACNI care plan developed within 12 weeks from the date of eligibility, based on a comprehensive assessment of the client’s needs. The Instrument of Delegation specifies the roles authorised to make care planning decisions as delegations of the Secretary’s powers and functions under the Act.
The care plan makes recommendations about supports and interventions to address the client’s multiple and complex needs, taking into account their best interests and working within a strengths-based framework. The Human Services (Complex Needs) Act 2009 stipulates care plans should not be longer than 12 months and the total duration of MACNI program involvement must not exceed 36 months. The total duration is calculated from the point of initial care plan approval to the point of MACNI closure, noting any periods of suspension. MACNI care plans are reviewed by the Panel every six months at a minimum.
Core to the establishment of an effective care plan is a strong understanding of the client’s needs and goals. Assessments including clinical assessments and the service interventions that have been attempted or implemented in the past should assist to inform service delivery into the future. Depending on the amount and quality of previous assessments, a brief synthesis or timeline of events/interventions may be sufficient to understand the client’s needs and the systems issues impacting the achievement of desired outcomes. At other times a much more in-depth process of file review and analysis is required.
The service responsible for developing the care plan will be determined based on appropriate matching to the client’s needs as well as the services expertise and capacity to provide care plan development in a timely and effective manner.
10.2.1 ContentA MACNI assessment and care plan development template is provided to a service provider developing a care plan which includes the MACNI information requirements. A service provider may tailor the plan with additional fields as seen relevant.
The initial care plan should include a reference to the following:
• client’s goals and aspirations• description of the client’s needs• reference to assessments and clinical reports completed, and any that may be recommended• summary of personal and family life, including cultural, spiritual, developmental, educational,
occupational and housing milestones/ experiences• summary of physical, cognitive, mental health, substance use, forensic history and issues, and other
key areas of need• description of client strengths, positive attributes and other factors, such as cultural identity and
connectedness, that may contribute to the achievement of change• any risks posed to and by the client as identified in risk assessments
Page 36 Service Provision Framework: Complex Needs March 2020

• identification of any specific behavioural interventions required by the client to support improved service access
• service mapping and gap analysis to establish a profile of the capacities and challenges inherent within the service delivery system, including:– identification of currently engaged services, supports and interventions, including defining role
responsibilities for the services to be provided– identification of services to be engaged/activated for the client against specific goals of the plan– analysis of strengths and barriers to service connectedness between the client and services and
between services themselves– client’s perspective of the service system and the service systems’ experience of the client,
including what has or has not worked to date and why – evaluation of systemic factors arising from the client’s interactions with the service system
• exit/transition planning priorities.
Documentation required• MACNI assessment and care plan development report• MACNI care plan template.
Coordinator tasks• support the care plan developer to access and gather relevant assessments and
documentation as required• provide assessment and MACNI care plan template to the service provider for
completion• ensure 90% of MACNI care plans are recommended by the panel within 12 weeks
from the date of eligibility• ensure MACNI care plans are reviewed and recommended by the panel on a six-
monthly basis• update SharePoint client database, ensuring the initial care plan date is recorded.
10.2.3 DurationThe duration of the MACNI care plan is calculated from the date of the initial care plan approval by the departmental delegate to the date of MACNI closure, less any period of time for which a suspension of the care plan was approved.
10.2.4 Care plan development levelsThe Human Services (Complex Needs) Act 2009 requires MACNI clients to have a care plan. To help target interventions appropriately, MACNI has established a tiered approach to care plan development. The tier levels are based upon the client’s need and the availability and accessibility of required information.
At eligibility determination (or at a later time) panels may make a recommendation on care plan development, including the choice of service provider to engage and the care plan level required. In some cases, a draft care plan is presented to panel at the point of eligibility consideration for its recommendation. If this occurs, the further appointment of a care plan development agency is not required, and service provision can progress to care plan coordination.
The panel reaches a decision about the care plan development level required at a point in time. If the client’s needs or circumstances change, the level can be adjusted outside the panel meeting to ensure a
Service Provision Framework: Complex Needs March 2020 Page 37

timely response. This is initiated through contact with the complex needs coordinator who reviews the request, and if appropriate, seeks approval from a departmental delegate. The decision is reported to panel members at the next scheduled meeting.
Care plan development levels and descriptions
Level Description
Level 1: 20 hours per week for 4 weeks Synthesis and analysis of existing and readily accessible information
Level 2: 20 hours per week for 8 weeks Sourcing and analysis of new or difficult to access information
Level 3: 20 hours per week for 12 weeks Extensive sourcing and analysis of new and difficult to access information
10.2.5 Care plan approvalFollowing the care plan developer’s preparation of a MACNI care plan, the Complex Needs Coordinator ensures the initial care plan is scheduled for an upcoming panel meeting (ensuring that key performance indicators are met (refer Section 17.2 – Performance targets).
The panel considers the initial care plan, the associated brokerage budget and proposed care plan coordination service provider, with a view to making a recommendation to the Area Director for approval.
Coordinator tasks• communicate the outcomes of a panel meeting to the care plan developer, including
feedback and the requirement for any amendment to the plan and/or brokerage request
• update the CSA/SharePoint with the initial care plan approval date (date care plan is approved by the delegate)
• schedule next care plan review date within six months.
10.2.6 Copy of care plan The Act requires that within 14 days after approving a care plan, the department must:
• give a copy of the MACNI care plan to the client• give a copy of the whole or any part of the MACNI care plan to service providers identified in the care
plan if it is in the best interests of the client and assists service providers to give effect to the care plan.
For some clients, panel recommend eligibility and a proposed care plan at the same meeting and a consolidated letter (eligibility outcome and care plan) is sent/given to the client. Typically, the Complex Needs Coordinator will engage with the care plan coordinator to establish the best approach for providing the care plan to the client and other engaged service providers. A standardised care plan letter, with a copy of the care plan, is prepared for the client.
A copy of the whole or part of the care plan is also given to service providers in the plan.
Documentation required• MACNI care plan notification – letter to client• MACNI care plan – to the client (may be modified in accordance with section 20 –
form of notification of the Act)
Page 38 Service Provision Framework: Complex Needs March 2020

• MACNI care plan (whole or part) – to service providers.
Coordinator tasks• ensure adherence to care plan template including details of brokerage expenditure• support the modification of the care plan appropriate to the client’s needs/capacity• prepare care plan notification letter and obtain area director signature• ensure the letter and an appropriate version of the care plan are sent to the client• ensure service providers are provided with a copy of the approved care plan (whole or
part).
10.3 Care plan coordinationThe care plan coordinator continuously collects and analyses information to develop, implement and monitor the progress of a set of tailored service responses and interventions as set out in the client’s care plan. This is achieved through cross-sector collaboration and the documentation of clear actions required to achieve client outcomes.
Critical to effective care plan coordination is maintaining regular contact with the care team, including well-structured care team meetings, providing support and guidance at critical points, and monitoring to ensure tasks are completed within agreed timelines. The care plan coordinator works to assess and document the effectiveness of agreed service responses.
Key responsibilities of the care plan coordinator are to:
• schedule and chair care team meetings, including responsibility for meeting agenda and minutes • monitor the care plan’s implementation and progress of the client• coordinate the services provided to the client as per the care plan• conduct six-monthly reviews of the care plan including funding acquittals• provide a report to the department on client progress when requested• provide a transition/exit plan six months prior to closure• provide a closure report at the point of closure.
The determination of the care plan coordination service is based on the matching of the client’s needs and the service’s expertise and capacity to provide care plan coordination in a timely and effective manner. The Instrument of Delegation specifies the departmental roles authorised to make care planning decisions, including the nomination of the care plan coordination service provider. While a care plan coordinator can be nominated from any service or program, the service provider needs to demonstrate the following:
• a commitment and expertise integrating clients with complex needs into existing service provision• an ability to nominate or recruit an experienced, influential and highly capable person/s to undertake
the care plan coordination role• the capacity to provide appropriate supervision and support to the care plan coordinator• professional values of open communication, effective networking and the capacity to provide
independent and objective care team governance• skill sets in establishing and implementing rigorous accountability frameworks, including the financial
acquittal of brokerage funding.
Coordinator tasks• schedule regular meetings with Care Plan Coordinator to discuss emerging
concerns/trends, risk management, case direction, care team dynamics, processes, brokerage management, etc.
Service Provision Framework: Complex Needs March 2020 Page 39

10.3.1 Care plan coordination levelsA decision is typically made about the level of care plan coordination required for each MACNI client at relevant panel meetings. If circumstances change, the care plan coordination level can be adjusted outside the panel meeting to ensure responsiveness to client need. This is initiated through contact with the complex needs coordinator who reviews the request and if appropriate, seeks approval from a departmental delegate. The decision is also reviewed at the next available panel meeting.
Care plan coordination levels and descriptions
Level Considerations
Level 1:4 hours p/w
Risk is currently managed; the care team is identified as relatively cohesive and high functioning; interventions are not determined especially urgent, and the client is not at a critical transition point.
Level 2:8 hours p/w
Some identified risks have not yet been responded to adequately; the care team is not cohesive and well-functioning; there is some urgency to required interventions, and/or the client is at a critical transition point.
Level 3:12 hours p/w
A high level of risk is identified; the care team is not well developed or dysfunctional; interventions are urgent, and/or the client is at a critical transition point.
Existing Support Coordination provided by the NDISThe amount and level of Support Coordination provided as part of an approved NDIS plan needs to be considered when determining tier level. For example, a client who may be suitable for tier 3 (12 hours per week) may be reduced to tier 2 (8 hours per week) due to a high level of Support Coordination or Specialist Support Coordination funded by an NDIS plan.
Travel requirements
The amount of travel required from the care plan coordinator’s usual place of work to the location of care team meetings, client visits or other relevant meetings needs to be considered when determining tier level.
10.4 Care plan review Once the initial care plan is approved, care plan reviews must occur at a minimum of six-monthly intervals. Preparation for a care plan review enables the care plan coordinator to assess progress in implementing the plan. It also provides an opportunity to consider issues that may be impacting on the implementation of the plan and the outcomes achieved by the client supported.
A review may be requested at any time when there are major changes which occur for the client or when known or emerging significant risks are identified. Any care team member, panel representative or other person listed in the Instrument of Delegation can request a care plan review take place earlier than six-monthly and at any frequency required.
Documentation required• MACNI care plan • MACNI care plan review report
Coordinator tasks• ensure adherence to care plan template including details of brokerage expenditure• ensure MACNI care plans are reviewed and recommended by the panel on a six-
monthly basis
Page 40 Service Provision Framework: Complex Needs March 2020

• update the SharePoint client and brokerage databases as required.
10.5 Care plan progress updatesIn addition to the formal care plan review process, care plan coordinators are required to provide updates regarding formal MACNI clients at each Complex Needs Panel. Progress updates may be provided in two ways:
• brief verbal updates – where there is little or no change to the client’s circumstances • written updates – where there is change to progress/services involved/tasks/status of specific actions
or interventions previously recommended by the panel
Documentation required• MACNI progress update report
Coordinator tasks• provide MACNI progress update report template to Care Plan Coordinator for
completion• ensure MACNI care plan is updated as required • update the SharePoint client and brokerage databases as required.
10.6 Suspension of a care planA change in a MACNI client’s situation may impact the ability to implement the care plan effectively. In these circumstances, it may be appropriate to suspend the care plan until the outcome of the change is known. Suspending the care plan effectively pauses MACNI service provision, preserving it for a point in time where it may be more effective or of greater value to the client.
As a guide, a suspension may be considered when:
• the client is incarcerated or hospitalised (or equivalent), for a period longer than 3 months or unknown, and the care plan is unlikely to be effectively implemented
• a significant crisis or event (e.g. resulting in a move to another location) gives rise to the need for the existing service providers to be engaged about the viability of service continuity.
Alternatively, a care plan may also be varied to change the number and/or type of service providers engaged. This approach would be used when, despite the change in client circumstance, many elements of the care plan can be continued. For example, an incarcerated client may continue to receive MACNI care planning if service provision remains largely unchanged and the goals of the plan can continue to be realized while incarcerated.
The total duration of a MACNI care plan may not exceed 36 months
Panels consider and determine the appropriateness of suspending a care plan. The decision should be made with consideration of the following:
• the client’s perspective • opportunities for the client to access suitable supports within the standard service currently available
to them (i.e. does the hospital/prison provide access to therapeutic supports or assessments?)
Service Provision Framework: Complex Needs March 2020 Page 41

• value of continued service provision in the current circumstances (i.e. is service provision largely unchanged? How effective are services? Are the travel requirements reasonable?)
• the benefit of ‘stopping the clock’ – providing continued MACNI coordination whilst in a restrictive facility vs. longer access to MACNI coordination whilst transitioning / in the community
• the current tier level of care plan coordination (may be reduced if not suspended)• if a suspension is recommended, the panel should establish the circumstances for MACNI service
provision to recommence (i.e. agreed date, when parole or discharge planning commences, etc).
The panel recommendation to suspend a care plan needs to be documented and communicated to the client and engaged services. The Complex Needs Coordinator also needs to notify the Agency Performance and Systems Support (APSS) unit where the funding to a contracted service is to be impacted and/or adjusted in their funding and service agreement.
Where a care plan coordinator is in place and the care plan is suspended, the continued funding for the Care Plan Coordinator may be negotiated by the area in relation to work with other MACNI clients. Alternatively, the Complex Needs Coordinator can vary the service and brokerage agreements and recoup funds accordingly.
Documentation required• MACNI care plan suspension notification – letter to client• MACNI care plan suspension notification – letter to services within the plan.
Coordinator tasks• prepare notification letters and obtain area director signature• communicate the outcomes of a panel meeting to the care team including terms of the
suspension• notify the APSS unit where the funding to a contracted service is to be impacted
and/or adjusted in their funding and service agreement• assume the primary liaison role for the client until formal care plan coordination
recommences• provide the panel with updates as requested• ensure service provider engagement is maintained to enable effective
recommencement of services once the suspension ends.
10.7 Transition/exit planningThroughout the life of the care plan, the care plan coordinator is required to consider options for transition/exit planning. In the last six-months of MACNI service provision, a transition/exit plan should be implemented. The MACNI transition/exit plan facilitates changes in the provision of services as an adjustment to meeting of the needs of the client beyond the life of the MACNI care plan. This planning requires liaison and negotiation with the relevant panel and the services to be involved post-MACNI.
The transition/exit plan is presented as a MACNI care plan, however, demonstrates a transition to sustainable services and supports in the community. For example, the transition/exit plan may include planned reductions in supports funded through the MACNI care plan.
Documentation required• MACNI transition / exit plan (reflecting transition arrangements and supports upon
closure).
Page 42 Service Provision Framework: Complex Needs March 2020

Coordinator tasks• provide guidance and support the care plan coordinator to identify sustainable
supports in the community• ensure all MACNI clients have a transition/exit plan recommended by the Complex
Needs Panel at least six months prior to care plan termination• update SharePoint client database, ensuring the exit/transition plan date is recorded.
10.8 Care plan closureThe panel recommends to the Area Director to close a care plan. There are multiple circumstances in which a care plan is closed:
• at any point in time if requested by the client• when the care plan coordinator, care team and department, in consultation with the client, agree that
the client’s needs/goals have been realised through the care plan• when the care plan’s duration has reached the maximum duration of 36 months.
The care plan coordinator is required to prepare a closure report to assist with the final review of the care plan. The report is provided to the panel at the time the care plan coordinator is recommending that MACNI cease involvement with the client, or when the maximum three-year involvement in MACNI has been reached.
The report reflects on the role MACNI has played in improving the client’s outcomes and enhancing service integration and collaboration. In addition, the closure report forms an assessment and analysis of the formal MACNI service period. There is an important emphasis on the progress of the client throughout the time with MACNI; the learnings gathered; identification of systemic issues; analysis/evaluation of interventions; the client’s perspective on what has been achieved; confirmation of continuing support arrangements (as relevant) and, any other future planning considerations.
Documentation required• MACNI transition/exit plan (reflecting transition arrangements and supports upon
closure)• MACNI care plan closure report, including funding acquittal• MACNI care plan closure notification – letter to client• MACNI care plan closure notification – letter to services within the plan.
Coordinator tasks• ensure all MACNI clients have a transition/exit plan recommended by the Complex
Needs Panel at least six months prior to care plan termination • ensure adherence to the closure report template • ensures all departmental actions are taken in relation to the closure of the care plan:
– funding acquittal– conclusion of funding to the care plan coordination service– completion of data and record management requirements
• prepare and send care plan closure notification letter to the client and services identified in the care plan
• ensure a copy of the closure report is sent to the Manager, Disability and Complex Clients Practice Advice and Support
• update the SharePoint client database, ensuring the closure date is recorded. If required, create a new line reflecting a period of Post-MACNI support (see Section
Service Provision Framework: Complex Needs March 2020 Page 43

11).
11. Post-MACNI supportFor a small number of MACNI clients, the full transition to sustainable engagement with the existing service system is not able to be effected by the closure of the MACNI care plan, particularly where the plan has been in place for the maximum period of 36-months.
The department and services engaged in the care plan will continue to provide coordinated care for an agreed time-limited period (3 months) to ensure the effective integration of the client into the existing service system.
In some cases, the use of approved brokerage may continue for a short period of time post-closure while in transition from MACNI to the standard service system.
Coordinator tasks• continue to monitor and acquit MACNI commitments and expenditure• update the SharePoint client and brokerage databases as required, ensuring all
entries are recorded in the Post-MACNI support type.
12. Support for High Risk Tenancies (SfHRT)
12.1 Operating modelSfHRT provides a continuum of targeted support for people with multiple and complex needs who are at risk of losing their tenancy. This support includes information, consultation, care coordination and/or provision of brokerage to maintain a tenancy. Collaborative practice with departmental property and tenancy staff, Tenancy Plus providers and other housing support services is crucial in the understanding and relationship with the tenant. In addition, SfHRT’s operational model complements the integrated community services system model, family violence initiatives and broader reform agenda.
There are various services that can be accessed for tenancy assistance prior to referral to SfHRT services. It is anticipated that other tenancy management options have been attempted or explored prior to a referral to SfHRT, and the referring program has made an attempt to resolve the tenancy issue through active communication with the relevant support links. The primary provider of support to social housing tenants is the department-funded Tenancy Plus. Support providers offering Tenancy Plus provide early intervention and work in partnership with the department’s housing program, other department program areas, community housing agencies and the general service sector.
SfHRT offers a variety of responses to a referral, these include:
• consultation, information and advice• advocacy or liaison within the department• brokerage to assist in ways that will maintain the tenancy• coordinating care teams to establish supports and/or a care plan.
SfHRT is not a case management or direct service delivery response, it is expected that the lead service provider/key worker will continue to maintain the role as primary contact/liaison for the client throughout the involvement of the coordinator. The Complex Needs Coordinator involvement is only active as long as the referrer or lead support organisation remains in contact.
Page 44 Service Provision Framework: Complex Needs March 2020

Standardised templates are provided in the appendix to assist Areas implement SfHRT at a local level. These templates are to be used by all Complex Needs Coordinators to enhance consistency and promote adherence to legislation and operational guidelines.
Figure 5 illustrates the SfHRT service model.
12.2 EligibilityThe target group for SfHRT are predominantly public housing tenants, however services are also offered to tenants in community housing:
• whose tenancies are at imminent risk of failure• who are not responding to multiple intervention attempts from housing support services or the tenancy
support service provider• whose circumstances make it difficult for them to establish their tenancy and there are no other
service options. These tenants will have complex behaviours that prevent them from engaging with support services
• who have complex support needs including but not limited to mental health, drug and alcohol and behavioural issues that require intensive support from a range of programs and services to assist them to maintain their tenancy.
These tenants may already be receiving support from a range of service providers, however a referral to SfHRT may enable enhanced care coordination and the development of a shared care plan.
Note: Tenants in community housing are offered all SfHRT service responses excluding brokerage.
12.3 SfHRT identification and referralCommon referrals to SfHRT include hoarding, squalor, antisocial behaviour (mental health or substance misuse), environmental neglect and/or family violence. In some cases, the department may have already breached the client or are indicating that legal action is imminent.
SfHRT has the capacity to provide prompt advice and consultation to referrers in time pressured situations via phone, email or in person. This initial contact will determine if the client is eligible for SfHRT and if a more detailed referral form is required. This function aims to support the early identification of tenancies at-risk and focus on prevention, whilst providing capacity building to housing services.
Where it is determined during initial contact that a more intensive advocacy, brokerage or care coordination may be required, a completed Complex Needs consultation form is required. This consultation form also enables requests for brokerage to be documented.
Any contact or correspondence that requires the Complex Needs Coordinator to provide information, practice advice, system navigation, problem solving, referral or coordination is regarded as a consultation.
Documentation required• complex needs consultation form• complex needs recommendations / closure form.
Coordinator tasks• ensure the Complex Needs consultation form is completed• provide referral advice and consultation as required• record the contact under the tenant’s client number in the Housing Integrated
Information Program (HiiP) and note the advice provided
Service Provision Framework: Complex Needs March 2020 Page 45

• update the SharePoint SfHRT client database.
Page 46 Service Provision Framework: Complex Needs March 2020

Figure 5: SfHRT overview
Service Provision Framework: Complex Needs March 2020 Page 47

Page 48 Service Provision Framework: Complex Needs March 2020

12.4 SfHRT consultationWhere the department’s housing staff or community organisations, including the tenancy support service providers, need advice regarding a public housing tenant with complex behaviours/needs, the Complex Needs Coordinator should be consulted.
SfHRT consultation will include advice regarding:
• best practice • care coordination• system navigation• care planning• capacity building.
Coordinator tasks• provide services as specified• convene and chair care team meetings as required• identify staff member / agency to take the lead post SfHRT intervention
12.4.1 Duration of SfHRT consultation / interventionThe duration of a SfHRT consultation is flexible and may vary between referrals. Some consultations may only entail a single interaction, with others requiring longer-term support and oversight. SfHRT interventions are considered short, medium or long-term. Examples of each are below:
Duration Description and examples
Short-termLess than 2 weeks
Referrals for brokerage only (e.g. property clean, rubbish removal, skip hire)
Referrers seeking information, advice or referrals to specialist services.
MediumLess than 3 months
Requirement for multiple case conferences and care coordination
Care team requires support/guidance/leadership to develop and implement a multidisciplinary plan
E.g. clients who reside in a property that requires multiple or staged cleans with or without therapeutic intervention.
Long-termMore than 3 months
Requirement for multiple case conferences and extended care coordination
Client may present with significant hoarding behaviours and require a staged cleaning process supported by therapeutic intervention
May involve a significant transition to social housing (e.g. client with history of arson/fire-setting who is returning to public housing in the community from prison or other secure facility).
12.5 Case conferencingWhere a case conference is considered necessary, it is generally expected that the lead case manager or referring agency is responsible for arranging a suitable time and venue, inviting the appropriate parties and chairing the meeting. Complex Needs Coordinators may assist in organising the meeting wherever necessary and may take notes, prepare and disseminate a list of recommendations and agreed actions.
There will be some instances where it is considered necessary for Complex Needs Coordinators to convene and chair a case conference in order to negotiate the most effective outcome. However, this will be done on a one-off or limited basis to facilitate agreement on an alternative lead service provider or
Service Provision Framework: Complex Needs March 2020 Page 49

create an appropriate care plan. Some examples where Complex Needs Coordinators will coordinate a case conference are if there is:
• no established lead agency• a requirement to secure the involvement of departmental program areas or community service
organisations • no active supports in place• disagreement on an approach to address the tenant’s needs.
Documentation required• departmental meeting agenda and meeting minutes template.
Coordinator tasks• provide support to the lead agency • convene and chair care team meetings as required.
12.6 Interface with Tenancy PlusThe Tenancy Plus support program assists social housing tenants by providing early intervention when a tenancy is at risk to sustain their tenancy and reduce the risk of homelessness. This program offers assertive outreach, case management, local area referral and interim intervention support to assist tenants to maintain housing and prevent homelessness. Tenancy Plus intervention should commence when a housing issue is identified, rather than when the tenancy is at the point of failure.
Tenancy Plus providers will intervene where a social housing tenancy is at risk to identify and assist the tenant to address and resolve the underlying factors that are placing the tenancies at risk. This includes:
• developing a client support plan with the tenant• providing direct support to the tenant• actively engaging with appropriate organisations or department program areas to address the
underlying issues that are causing the tenancy to be at risk• convening a meeting with support providers to determine who will be responsible for actions listed in
the plan• oversight, coordination and implementation of the plan.
Tenancy Plus service locations align with the departments areas and have a close relationship with local housing offices, community housing providers and SfHRT.
At any stage of Tenancy Plus support, it may become apparent that the tenant’s needs cannot be effectively met without a higher level of coordination or intervention; SfHRT provides this escalated service response.
Refer: Tenancy Plus – Tenancy support program operational guidelines <https://providers.dhhs.vic.gov.au/tenancy-plus-tenancy-support-operational-guidelines>
Coordinator tasks• maintain a collaborative relationship with Tenancy Plus, encourage referrals and
provide capacity building as required/requested• support departmental housing staff to engage and collaborate with Tenancy Plus• provide specific advice, referral and care coordination for cases where hoarding and
squalor are prominent/present.
Page 50 Service Provision Framework: Complex Needs March 2020

Figure 6 – The escalation of service response when a tenancy becomes at risk
12.7 Interface with Indigenous Tenants at Risk (ITAR)The Indigenous Tenants At Risk (ITAR) program, also referred to as Aboriginal Tenants at Risk (ATAR), uses an intensive case management and support service model to assist Indigenous people living in mainstream, public housing, community housing or Aboriginal Housing Victoria (AHV) properties whose tenancies are at risk as a result of emerging issues such as financial difficulty, neighbourhood disputes, drug and alcohol and mental health issues. Households are supported to stabilise their housing and retain their tenancies rather than leave the property or risk eviction.
The Support Worker will be required to intervene where a public housing tenancy is breaking down to resolve factors placing the tenancy at risk. It will also involve provision of intensive individual support to tenancies identified at risk and referrals from DHS housing offices, whilst rent arrears are the major factor to contribute to tenancies at risk this initiative will also include other factors such as living skills. It will be expected that where the issues relate to non-housing programs referrals will be made to those programs.
Flexible brokerage is available through this program and its primary uses include:
• household expenses, e.g. electricity, gas and water bills, repairs to whitegoods• counselling services, drug and alcohol counselling, grief and loss counsellors, dealing with stress• life skills e.g. financial services, cooking courses, cleaning skills• recreation activities, sporting and fitness activities, dancing classes, gym membership, join in
community groups, culture events, children holiday clubs, camps, after school activities• education and training, extended learning, language classes, literacy and numeracy, job coaching.• material aid, e.g. food, travel, clothing expenses• medical, doctors, dentist, optometrist, podiatrist• pharmaceutical requirements, glasses, prescriptions, where indicated for use by GP• therapeutic intervention, family counselling, parenting skill courses, anger management, and speech
therapy.
Consistent with SfHRT’s interface with Tenancy Plus, if at any stage of ITAR/ATAR support, it becomes apparent that the tenant’s needs cannot be effectively met without a higher level of coordination or intervention; SfHRT provides this escalated service response.
Refer: Homelessness services guidelines and conditions of funding <https://www.dhhs.vic.gov.au/sites/default/files/documents/201705/Homelessness-Services-Guidelines-and-Conditions-of-Funding-May-2014.pdf>
12.8 SfHRT consultation closureA SfHRT consultation should be considered for closure in the following circumstances:
• the matter is believed to be resolved• the involved services have not required further consultation support for 3 months• no further tasks have been generated for the Complex Needs Coordinator for 3 months• the referring/lead agency has withdrawn• the client decides to withdraw.
Service Provision Framework: Complex Needs March 2020 Page 51

The client can be re-referred at a later point in time as the need arises. If the client is re-referred, a new consultation record is opened (ensuring client details are updated), reflecting the current reason/goal of consultation, current service system issues and current service involvement.
Documentation required• complex needs recommendations/closure form.
Coordinator tasks• complete and provide complex needs recommendations/closure form to the referrer • update HiiP, uploading the complex needs recommendations/closure form.• update the SharePoint SfHRT client database, ensuring the closure date is recorded.
13. Interface with the NDIS
From 1 July 2019, Victoria reached a full scheme agreement with the National Disability Insurance Scheme (NDIS). Management and funding for disability-specific supports and services have transitioned from State Government (the department) to the National Disability Insurance Agency (NDIA) and all eligible Victorians now have access to the NDIS.
The NDIS Quality and Safeguards Commission (NDIS Commission) provide a nationally consistent system to safeguard the rights of NDIS participants under the NDIS Quality and Safeguarding Framework, taking over Victoria’s previous quality and safeguards arrangements for NDIS participants and services. Further information can be found in Section 16.15.
13.1 Transitions Team and Intensive Support TeamThe department has established NDIS transition teams in each area to support and guide service providers for clients transitioning to the NDIS. The NDIS transition teams have established relationships with NDIA regional offices and provide an important liaison role to resolve transition issues and avoid escalation of clients’ concerns.
Some clients receiving complex needs services have experienced difficulties with their NDIS planning and plan implementation and require additional time-limited intervention to support them to transition. For example, their complex needs or circumstances may lead to significant issues in their NDIS transition, the risk of an adverse outcome for the client is high or the need for intervention is time-critical due to the impact of the issue. In these cases, the assistance of the Intensive Support Team (IST) should be considered.
A key role undertaken by the IST is to assist people who meet eligibility criteria to navigate the NDIS pathway and processes, particularly when they have experienced delays in plan approval or implementation of support or need to seek a plan review. The IST may also work with an NDIS allocated support coordinator or provide capacity building to a service provider in a short-term coordinating capacity where there is no support coordinator involved to improve participant outcomes.
Refer: Intensive Support Team <https://intranet.dhhs.vic.gov.au/ndis-transition-planning#intensive-support-teams>
Page 52 Service Provision Framework: Complex Needs March 2020

Coordinator tasks• identify and refer clients with complex needs who would benefit from support from the
department’s NDIS transitions team and/or Intensive Support Team.
13.2 Complex Support Needs PathwayThe Complex Support Needs Pathway has been established by the NDIA to provide specialised support for participants with a disability who have other challenges impacting their lives such as mental health issues, incarceration or homelessness, and need a higher level of specialised supports in their plan. Involuntary or voluntary involvement with particular government systems such as justice or mental health would also be factors which would necessitate entry to the Complex Support Needs Pathway.
The Complex Support Needs Pathway have dedicated NDIA Complex Support Needs planning teams and a network of specialised planners with strong experience in high-level coordination and/or allied health experience. The Complex Support Needs Pathway includes six key features to deliver better outcomes:
1. pre-access, local engagement and strengthening connections to other servicesStrengthening local engagement and liaison with other government services and community supports with clear pathways and connections into the NDIS to ensure participants experience a joined-up approach to their support.
2. access, detailed handovers and connectionsDetailed handovers from states and territory systems, existing service providers or ‘hard to reach' support workers at the point of access and streamlined access decisions using local NDIA Liaison and Specialised Planner.
3. specialised planners and complex support practice leadPlanning conversations with participants and other stakeholders, led by an NDIA Specialised Planner, focused on ensuring a deep understanding of participant life circumstances.
4. skilled support coordinators and effective plan implementationA stronger focus on maintaining a participants' critical supports, via a skilled Support Coordinator to assist with the development of service plans and agreements, mitigating risks of service failure and coordination with other government services and community support systems.
5. ongoing monitoring and evaluationRegular monitoring and evaluation of the plan, and participant outcomes, with the ability to make minor adjustments to supports and approaches to improve effectiveness.
6. review outcomes and progressPlan reviews measure participant progress toward outcomes, acknowledge achievements and adjust the participant's plan to support their next set of goals and outcomes, including assessing if the participant should remain in the Complex Support Needs Pathway or transition to the general NDIS Pathway.
To find out more about eligibility and referrals to the NDIS Complex Support Needs Pathway contact the NDIA on 1800 800 110 or email NDIS <[email protected]>
13.3 NDIS plan and MACNI care planMany clients receiving MACNI services may also be eligible to receive a service plan from the NDIS. In many instances, the existing MACNI care plan has been provided in pre-planning meetings with the NDIS to demonstrate the level of complex support and coordination required.
Service Provision Framework: Complex Needs March 2020 Page 53

Where a formal MACNI client also has an approved NDIS plan, details regarding NDIS-funded service provision are required to be incorporated in the MACNI care plan, specifying the funding source. No plan takes precedence over another and the two plans exist side-by-side with specific functions.
To avoid duplication of funding, knowledge of what may be funded via the NDIS plan is required before brokerage can be committed. For example, the NDIS plan may include provisions for assessments or direct staff support and should not be requested from MACNI. MACNI does not fund services that would normally be funded by the NDIS, including psychosocial disability support.
Further information regarding brokerage for disability-specific services is in Section 15.2.1.
Coordinator tasks• ensure fund holders (DHHS, NDIA, etc) are clearly indicated within the care plan• obtain consent from the client to have information regarding services in their NDIS
plan released to the Complex Needs Coordinator or Care Plan Coordinator.
13.4 Public housing and the NDISThere are a range of scenarios in which public housing clients will interface with the NDIS, which may impact the SfHRT service response. This includes public housing applicants and tenants who have a disability or are carers of a person with disability, or have a family member with disability, who:
• have transitioned to the NDIS and need to remain connected with the access and planning processes• have not accessed services before or are not yet an NDIS participant and may need assistance to
engage with the NDIS application process• are an NDIS participant but not accessing support, either needing assistance to re-engage with the
NDIS and implement their plan, or to seek a review if their plan is no longer meeting their needs• have an active NDIS plan and are accessing NDIS funded services and may need help coordinating
between NDIS and other mainstream supports (such as health)• are not likely to meet the NDIS access requirements. In this case, a Local Area Coordinator (LAC)
may connect a person to services, supports and activities in the community and other government services.
Departmental staff may use the Public Housing and the National Disability Insurance Scheme: Roles and responsibilities operational guidelines to determine their roles and responsibilities regarding NDIS participants. The purpose of these guidelines is to outline the intent, principles and processes within which the department, on behalf of the Director of Housing, works with people with a disability to address housing needs.
Refer: Public Housing and the National Disability Insurance Scheme: Roles and responsibilities operational guidelines <https://providers.dhhs.vic.gov.au/public-housing-and-national-disability-insurance-scheme-roles-and-responsibilities-operational>
14. Interface with the Forensic Disability Program
Some Complex Needs clients may have had contact with the criminal justice system. The department funds and operates the Forensic Disability Program to respond to people with cognitive impairment involved in the criminal justice system. A forensic disability response refers to the assessment, treatment and support of people with disability who are in contact with or are at significant risk of coming into
Page 54 Service Provision Framework: Complex Needs March 2020

contact with the criminal justice system, with a focus on the impact their disability has on their offending behaviour.
Forensic disability services are a state government responsibility which the Victorian Government will retain following full transition of general disability supports to the NDIS.
The Forensic Disability Program comprises the following services:
• the Forensic Disability State-wide Access Service, which is a state-wide intake and referral service for people seeking access to forensic disability services.
• the Disability Forensic Assessment and Treatment Service (DFATS), including a short-term court-ordered compulsory treatment in a residential treatment facility in Fairfield, community programs, a prison program at Port Philip Prison and a dual disability mental health psychiatric clinic.
• Disability Justice Coordination teams in each of the department’s operational groups to coordinate forensic disability assessments and interventions for people with a cognitive impairment who are subject to a court order or at risk of offending.
• a network of Specialist Forensic Disability Accommodation (SFDA) services consisting of a network of 12 residential staffed houses.
Complex Needs clients who require forensic disability supports can be referred to the Forensic Disability Program through the Forensic Disability State-wide Access Service.
15. Brokerage
The complex needs model allows for the provision of discretionary client-attached brokerage to purchase specialist assessments, services and interventions to support the delivery of the care plan, care plan development and care plan coordination.
• all requests for brokerage must be prepared using a brokerage request form.• all brokerage allocations less than $25,000 are reported as a standard agenda item at Panel
meetings, however, the Complex Needs Panel are required to recommend all brokerage over $25,000.
• it is a requirement for all brokerage allocations to be documented in a care plan.
The authority to approve funding for all departmental programs, including MACNI and SfHRT, is governed by the Financial Management Act 1994. The Secretary’s Financial Authorisation Schedule outlines the delegation levels for all departmental employees. Delegations must be adhered to when seeking approval for allocation of MACNI brokerage funds.
Delegations under the Financial Management Act 1994
Service Provision Framework: Complex Needs March 2020 Page 55
Authorised position Delegation limit per transaction
Complex Needs Coordinator $5,000
Manager, Client Support and Housing Services $50,000
Area Director $500,000

Documentation required• brokerage request form• brokerage notification template – for Complex Needs Panel (optional)• care plan must reflect the use of brokerage.
15.1 Eligibility for brokerage
15.1.1 Eligibility for Complex Needs brokerage Brokerage funding is available for use with clients with complex needs in all stages of support: consultation, assessment, Pre-MACNI and formal MACNI. The amount of brokerage and types of services available for purchase vary depending on the stage of support.
Brokerage allocation for clients with complex needs and the phases of MACNI support
Stage of support Brokerage limit
Purpose of expenditure
Services/items
Consultation and clients with complex needs
Up to $25,000 per 12-month period
Assist with service planning or access
• assessments - for example:– psychiatric– neuro-cognitive– occupational therapy– other allied health– risk assessment
Pre-MACNI Up to $15,000 per 12-month period
Interrupt a significant crisis, trial an intervention and/or prevent further escalation of need at a local level
• accommodation (restrictions apply, see below)
• allied health services (occupational therapy, speech pathology, neuro-cognitive, etc)
• assessments (including allied health)• bridging finance that will have a
significant impact on treatment (e.g. < 8 weeks accommodation)
• care plan development• care plan coordination• direct support provision/worker allocation• other specific items upon approval• psychological/psychiatric assessment and
treatment services• risk assessments• secondary consultation / clinical guidance
/ staff training (capacity building).
Formal MACNI Expendable within area/group budget and in-line with the approved care plan
Support the delivery of the care plan
The primary purpose of SfHRT brokerage is to support public housing tenants with complex behaviours whose tenancies are at risk. For example, to prevent a breach or further commencement of legal proceedings. In some cases, SfHRT brokerage is also used to support individuals who require additional support to establish their tenancy.
Page 56 Service Provision Framework: Complex Needs March 2020

SfHRT brokerage is not available to tenants in community housing.
Brokerage funding is utilised when flexible responses are required that are not available within the existing service system. Consistent with eligibility for SfHRT, it is expected that all other funding options have been explored prior to any requests for SfHRT brokerage funds.
The brokerage request is included on the Complex Needs consultation form and can be completed at the point of referral. It is not expected that every tenant referred to SfHRT will require funding, however, some referrals to SfHRT only require financial intervention (i.e. industrial cleaning, rubbish removal, skip hire, etc).
Stage of support Brokerage limit
Purpose of expenditure
Services/items
Support for High Risk Tenancies
(Public housing tenants only)
Expendable within budget
To maintain or establish at-risk tenancy
Services that support the tenant to maintain or establish a tenancy. For example:
• cleaning services
• specialist services (behavioural intervention)
• capacity building.
Coordinator tasks• ensure other funding options have been explored• consider SfHRT brokerage as a contribution to funds required, rather than funding the
full amount requested.
15.2 Brokerage principles
15.2.1 Complex Needs brokerage principlesThe following principles apply to all brokerage allocations to clients with complex needs:
• client-attached brokerage is available as a last resort when supports or resources in the standard service system are unavailable or are unable to be provided within effective timelines
• the allocation of brokerage is derived from an analysis of the client’s needs and the prior effectiveness of other funding support and takes into account the sustainability of service delivery
• brokerage is strictly for direct purchase of services for the client• brokerage is not an alternative to core funding and cannot be used to duplicate existing services or
cover administrative costs• brokerage is time-limited and non-recurrent and there must be significant effort to integrate the client
back into mainstream service provision• brokerage funds may be used to purchase secondary consultation, training, specialist clinical staff
support or mentoring in accordance with the care plan and to build service capacity in the longer term.
15.2.1 Brokerage for disability-specific servicesMost disability-specific, Victorian government-funded programs have transitioned/are transitioning to the National Disability Insurance Scheme (NDIS).
The Council of Australian Government (COAG) has created a document that delineates the principles that determine the responsibilities of the NDIS vs other service systems such as MACNI and SfHRT. The Victorian Government agrees that the principles outlined in this document will be used to determine the funding and delivery responsibilities of the NDIS.
Service Provision Framework: Complex Needs March 2020 Page 57

The approval of Complex Needs brokerage for all disability-specific services are subject to these principles and must be clarified at Panels to avoid duplication. MACNI care plans are required to clearly indicate which service system (DHHS or NDIS) provides funding for each service.
To avoid duplication of funding, knowledge of what may be funded via the NDIS plan is required before Complex Needs brokerage can be committed. For example, the NDIS plan may include provisions for assessments or direct staff support and should not be requested from MACNI.
Refer: Principles to determine the responsibilities of the NDIS and other service systems <https://www.coag.gov.au/sites/default/files/communique/NDIS-Principles-to-Determine-Responsibilities-NDIS-and-Other-Service.pdf>
Page 58 Service Provision Framework: Complex Needs March 2020

Refer: Public Housing and the National Disability Insurance Scheme: Roles and responsibilities operational guidelines <https://providers.dhhs.vic.gov.au/public-housing-and-national-disability-insurance-scheme-roles-and-responsibilities-operational>
Coordinator tasks• provide Panels with clarification regarding funding responsibilities as required• ensure fund holders (DHHS, NDIA, etc) are clearly indicated within the care plan• obtain consent from the client to have information regarding services in their NDIS
plan released to the Complex Needs Coordinator or Care Plan Coordinator.
15.2.3 SfHRT brokerage principlesThe following principles apply to SfHRT brokerage:
• SfHRT brokerage is only available for tenants in public housing. Tenants in community housing are not eligible for brokerage
• if other funded program areas are involved with the client, it is an expectation that costs will be shared• recurrent requests for similar supports for the same tenant, or to address similar themes regardless of
the amount, will require separate approval from the appropriate financial delegate• quotes from contractors or retailers are required for all brokerage requests and after receipt of
quotations, coordinator will seek approval from a suitable delegate and provide written confirmation of acceptance or rejection of the request (usually via e-mail) to the applicant.
• where the total is going to exceed the original quote, an updated quote must be provided to the Complex Needs Coordinator so that they can seek approval from a suitable delegate for the additional funds. This must occur prior to the service being provided.
15.3 Brokerage exclusionsBrokerage is not to be used for items such as:
• staff phones, fax or computer expenses• purchasing vehicles, vehicle rental, petrol or vehicle maintenance• staff travel expenses• head lease arrangements• office rental, maintenance, utilities or insurance• management/infrastructure fees• standard supervision, training and attendance and conferences (it is the expectation that programs
and organisations offer these provisions).• client debts• landlord related items such as staff travel or associated costs• rent arrears• retrospective funding requests• any items or service that can be funded by the existing service system (for example Housing
Establishment Fund (HEF), etc).
Service Provision Framework: Complex Needs March 2020 Page 59

15.4 Brokerage approval processes
15.4.1 Consultation assessment brokerageConsultation support includes the capacity to use assessment brokerage funding of up to $25,000 in a 12-month period. This brokerage can only be used to purchase specific assessments that are needed to assist with service planning or service system access.
All requests for brokerage must be recorded on a brokerage request form and approved by the appropriate financial delegate. All assessment brokerage allocations are reported as a standard item at Complex Needs Panels.
Consultation assessment brokerage approval requirements
Amount Documentation Role of Panel
Financial delegate Procurement & Probity requirements
Less than $5,000 Brokerage request form
Notify only Complex Needs Coordinator ($5,000)
Minimum of 1 quote
Between $5,000 and $25,000
Brokerage request form
Notify only Manager CSHS ($50,000)
Minimum of 1 quote
Page 60 Service Provision Framework: Complex Needs March 2020

Reminder: Limit up to $25,000 per 12-month period
Documentation required• brokerage request form• brokerage notification template – for Complex Needs Panel (optional).
Coordinator tasks• ensure the brokerage request form is prepared• notify the panel of all assessment brokerage expenditure at the next scheduled panel
date• seek approval for assessment brokerage from the appropriate financial delegate• update the SharePoint brokerage database.
15.4.2 Pre-MACNI brokeragePre-MACNI support includes the capacity to use client-attached brokerage funding of up to $15,000 in a 12-month period. All requests for brokerage must be recorded on a brokerage request form and approved by the appropriate financial delegate. Notification of all brokerage expenditure is required to be provided to the Complex Needs Panel at the next scheduled meeting date. The use of brokerage must be documented within the care plan, including the service provider details and dates of service provision.
Pre-MACNI brokerage approval requirements
Amount Documentation Role of Panel
Financial Delegate Procurement of Probity requirements
Less than $5,000
Brokerage request form
Notify only Complex Needs Coordinator ($5,000)
Minimum of 1 quote
Between $5,000 and $15,000
Brokerage request form
Brokerage agreement form
Notify only Manager CSHS ($50,000)
Minimum of 1 quote
Reminder: Limit of up to $15,000 per 12-month period
Documentation required• brokerage request form• brokerage notification template – for Complex Needs Panel (optional)• MACNI care plan must reflect brokerage expenditure• brokerage agreement form.
Coordinator tasks• ensure the brokerage request form is prepared• notify the panel of all brokerage expenditure at the next scheduled panel date• seek approval for brokerage expenditure from the appropriate financial delegate• prepare brokerage agreement.• update the SharePoint brokerage database.
Service Provision Framework: Complex Needs March 2020 Page 61

15.4.3 Formal MACNI brokerageMACNI brokerage may be allocated to formal MACNI clients to support the delivery of the care plan. The use of brokerage funding with a MACNI care plan is considered and recommended by the Panel at the time of in-principle approval of the care plan, and then approved by the financial delegate. Amounts of less than $25,000 do not require Panel recommendation, however, the Panel must be notified of the expenditure.
Formal MACNI brokerage approval requirements
Amount Documentation Role of Panel
Financial Delegate
Procurement & Probity requirements
Less than $5,000
Brokerage request form Notify only Complex Needs Coordinator ($5,000)
Minimum of 1 quote
Between $5,000 and $25,000
Brokerage request form
Brokerage agreement form^
Notify only Manager CSHS ($50,000)
Minimum of 1 quote
Between $25,000 and $50,000
Brokerage request form
Brokerage agreement form
Service agreement (consult with APSS)
Recommend Manager CSHS ($50,000)
Minimum of 1 quote
Between $50,000 and $100,000
Brokerage request form
Brokerage agreement form
Service agreement (consult with APSS)
Recommend Area Director ($500,000)
Seek a minimum of 3* written quotes (see exceptions below)
Over $100,000
Seek Quote / Tender or as advised by Procurement Services
Brokerage request form
Brokerage agreement form
Service agreement (consult with APSS)
Recommend Area Director ($500,000)
Seek Quote / Tender or as advised by Procurement Services
Page 62 Service Provision Framework: Complex Needs March 2020

^ Unless for assessments.
* In cases where a specialist service is required, this rule does not apply and 1 quote from a provider is acceptable. Brokerage requests must clearly indicate that procurement requirements were waived due to the nature of specialist support provision.
Limit: expendable within area/group budget for the duration of the care plan.
SAMS2 is the preferred method of payment for all formal MACNI services
Documentation required• brokerage request form• brokerage notification template – for Complex Needs Panel (optional)• MACNI care plan must reflect brokerage expenditure• brokerage agreement• SAMS form (as required).
Coordinator tasks• ensure the brokerage request form and table is prepared for the panel• prepare SAMS form (as required)• notify the panel of all brokerage expenditure at the next scheduled panel date• present brokerage requests over $25,000 to the panel for recommendation• seek approval for brokerage expenditure from the appropriate financial delegate• consult with the Area Director prior to the panel to ensure brokerage requests are
within the allocated area/group complex needs budget• prepare brokerage agreements• consult with your local Agency Performance and System Support (APSS) adviser to
determine the status of the provider's service agreement/service plan• update the SharePoint brokerage database.
15.4.4 SfHRT brokerageThe primary purpose of SfHRT brokerage is to support public housing tenants with complex behaviours whose tenancies are at risk and should be prioritised for those who are in the greatest need.
All requests for brokerage must be recorded on a brokerage request form – unless included in the initial Complex Needs consultation form – and approved by the appropriate financial delegate. SfHRT brokerage allocations are reported as a standard item at the Complex Needs panel, however, Complex Needs Coordinators are required to present brokerage requests over $25,000 to the panel for recommendation.
SfHRT brokerage approval requirements
Amount Documentation Role of Panel
Financial delegate Procurement & Probity requirements
Less than $5,000 Brokerage request form
Notify only Complex Needs Coordinator ($5,000)
Minimum of 1 quote
Service Provision Framework: Complex Needs March 2020 Page 63

Between $5,000 and $25,000
Brokerage request form
Brokerage agreement form
Notify only Manager CSHS ($50,000)
Minimum of 1 quote
Documentation required• Complex Needs consultation form (brokerage request complete) or• brokerage request form • brokerage notification template – for Complex Needs Panel (optional).
Coordinator tasks• ensure the brokerage request is prepared• seek approval for brokerage expenditure from the appropriate financial delegate• notify the panel of all brokerage expenditure at the next scheduled panel date• notify the panel of all brokerage expenditure at the next scheduled panel date• update the SharePoint brokerage database.
15.5 Brokerage business rulesTo ensure all brokerage procedures are consistent and acquitted in a timely manner, the following business rules have been established:
• all services providing care plan coordination are required to have a service agreement and service plan with the department. All payments will be managed via SAMS2 (exclusions apply to rural areas – see 15.7.3 Requirements for brokerage agreements and service agreements)
• where a service agreement exists, payment should only be made through SAMS2• financial acquittals are required to be provided and processed within 30 days of the service being
provided• all services with service agreements will be paid in monthly instalments, regardless of the length of
service provision• all brokerage expenditure is required to be recorded and updated in the SharePoint brokerage
database within 2 weeks • Complex Needs Panels are required to be provided with a transparent budget status by the Area
Director at the commencement of each scheduled meeting. The Area Director will confirm the budget is available to support the requested care plan expenditure.
• financial acquittals are required to be provided and processed within 30 days of the MACNI care plan closure
• care plans that cross financial years, will require the brokerage to be acquitted and processed within the same financial year that the service is provided. This may require ‘in principal’ payments for services provided in May/June.
For example, where a care plan may include services from 1 March - 30 September 2020, those services are required to be acquitted across two financial years;
• Financial Year 2019 / 2020: Service provision from 1 March - 30 June• Financial Year 2020 / 2021: Service provision from 1 July - 30 September.
Page 64 Service Provision Framework: Complex Needs March 2020

Figure 5 – Brokerage approval process
Service Provision Framework: Complex Needs March 2020 Page 65

Reminder: Complex Needs Coordinators are required to consult with the Area Director prior to the panel to ensure brokerage requests are within the allocated group complex needs budget
Page 66 Service Provision Framework: Complex Needs March 2020

15.6 Brokerage managementAt the commencement of each financial year, the Manager, Disability and Complex Clients Practice Advice and Support allocate the complex needs budget to each group. Complex Needs Coordinators record all expenditure approved by the appropriate financial delegates and monitor and acquit the allocation against each client supported.
At mid-year, the Manager, Disability and Complex Clients Practice Advice and Support conduct a review and reconciliation process in which areas are required to report on funds approved and projected for the remainder of the financial year.
Following the review and reconciliation process, allocations for the remainder of the financial year (1 January – 30 June) may be adjusted. Where a group is unable to utilise their funding allocation within the financial year, the funding may be redirected to meet high priority needs of clients supported in other groups. Groups will be engaged and advised throughout this process of any brokerage allocation adjustments.
Each area and group have responsibilities to implement quarterly reviews to ensure that budgets are acquitted correctly and ensure the budget allocation is adhered to. The complex needs budget will be tabled at regular Group Executive meetings to ensure Area Directors are aware of the current budget status.
Roles and responsibilities for the management of complex needs brokerage
Position ResponsibilitiesDisability and Complex Clients Practice Advice and Support unit
• drafting and oversight of compliance to service provision framework: complex needs and departmental procurement policy
• budget allocation to groups• consider requests for additional budget allocation from the groups• transfer of budget allocated following the mid-year review and
reconciliation process• oversight and management of the trust fund.
Finance Manager, Group • oversight of the group budget allocation and area expenditure• regularly monitor brokerage data as reported in the Complex Support
Application• implement practices each quarter to ensure the group budget are
adhered to• implement local area business processes to reconcile brokerage
data between Complex Support Application and DHHS financial records (SAMS2 and Oracle).
Area Director • oversight of area expenditure and processes to reconcile brokerage data
• undertake financial delegate tasks for brokerage expenditure over $50,000 (including the approval of Oracle / SAMS2 payments)
• ensure brokerage requests presented to the Complex Needs Panel are within the allocated area/group complex needs budget
• regularly monitor brokerage data as reported in the Complex Support Application.
Manager Client Support and Housing Services
• ensure that complex needs expenditure is in-line with the service provision framework: complex needs and departmental policies and
Service Provision Framework: Complex Needs March 2020 Page 67

Position Responsibilitiesprocedures
• undertake financial delegate tasks for brokerage expenditure under $50,000 (including the approval of Oracle / SAMS2 payments)
• implement practices each quarter to ensure that budgets are acquitted, and commitments/expenditure are processed using appropriate cost codes
• regularly monitor brokerage data as reported in the Complex Support Application.
Complex Needs Panels • ensure that complex needs expenditure is in-line with the service provision framework: complex needs and departmental policies and procedures
• receive notification of complex needs brokerage expenditure of less than $25,000 and provide comment as appropriate
• review complex needs brokerage requests over $25,000• recommend brokerage requests with consideration of available
area/group budget.
Complex Needs Coordinator
• ensure that complex needs expenditure is in-line with the service provision framework: complex needs and departmental policies and procedures
• meet with the Area Director prior to the panel to confirm all brokerage requests are within budget
• provide Complex Needs Panels with an accurate overview of the current Complex Needs (both MACNI and SfHRT) budget prior to brokerage recommendation
• determine the requirement for a service agreement and/or brokerage agreement
• undertake financial delegate tasks for brokerage expenditure under $5,000
• check the current MACNI unit price on SAMS2 and calculate Care Plan Development and Care Plan Coordination accordingly
• initiate the transfer of approved brokerage funding to contracted service providers via SAMS2
• pay invoices via Oracle• participate in quarterly reviews to ensure that budgets are acquitted,
and commitments/expenditure are processed using appropriate cost codes
• update ALL brokerage allocation and expenditure in the SharePoint brokerage database fortnightly
• undertake local area business processes to reconcile brokerage data as reported in the Complex Support Application and DHHS financial records (SAMS2 and Oracle).
Care Plan Coordinator • seek quotes for service • request quotes and acquittals from service providers.
Services within the care plan
• provide quotes as requested• provide invoices within 30 days of the service being provided• clearly indicate whether GST is applicable
Page 68 Service Provision Framework: Complex Needs March 2020

Position Responsibilities• enter into Brokerage agreements and Service Agreements where
applicable.
15.7 Procurement The Victorian Government Purchasing Board (VGPB) has five policies which cover end-to-end procurement activity, from identifying needs, planning, and market research through to contract management. Each policy is supported by good practice guides, tools and templates to ensure consistency across government.
When applying the policies, the department must ensure that all procurement activity meets the following directives:
• value for money: A balanced judgement of a range of financial and non-financial factors, taking into account the mix of quality, cost and resources; fitness for purpose; total cost of ownership; and risk.
• accountability: The accountable officer (Secretary) has the flexibility to conduct procurement activities using the appropriate capability to provide value-for-money outcomes.
• probity: High standards of behaviour and actions in the conduct of procurement processes. Equity, confidentiality, avoiding conflicts of interest, and consumer/supplier confidence in the integrity of government procurement processes.
• scalability: The relationship between the complexity of a procurement project and the capability of the organisation to conduct it to achieve a good procurement outcome.
The Standing Directions of the Minister for Finance under the Financial Management Act 1994 and the policies of the Victorian Government Purchasing Board require that the department implements and maintains an effective internal control framework over the procurement of goods and/or services. The department’s procurement compliance policy outlines staff responsibilities in relation to a procurement activity that has not complied with the procurement policy.
All staff involved in the funding, purchase or procurement of goods and services must ensure familiarity and compliance with the relevant procurement policies and guidelines as prescribed by the Financial Management Act 1994, the Victorian Government Purchasing Board and the department’s Procurement Committee.
Refer: Procurement policies <https://dhhs.vic.gov.au/procurement-policies>
Refer: Probity <https://intranet.dhhs.vic.gov.au/probity-procurement-and-contract-management>
Refer: Procurement governance <https://intranet.dhhs.vic.gov.au/procurement-governance>
Coordinator tasks• ensure procurement and probity policies are adhered to• utilise the brokerage checklist as a prompt.
15.7.1 Service agreementsThe department works in partnership with a range of community sector organisations who directly provide services to clients, families and communities on behalf of the government. Service agreements are used to manage the funding to community sector organisations. The service agreement sets out the key obligations, objectives, rights and responsibilities of both the organisation delivering services and the department. This contract facilitates a consistent approach to service delivery and accountability and ensures good financial management.
Service Provision Framework: Complex Needs March 2020 Page 69

As such, organisations providing services against the following Complex Needs activity numbers are subject to a service agreement and service plan and must with comply with Volume 3: Human Services Policy and Funding Plan 2015-19, update 2018-19 and all relevant policy and funding guidelines.
• MACNI services against activity ‘17250 Multiple and Complex Needs Imitative’ or• SfHRT services against activity ‘91417 Support for High Risk Tenancies’.
Through this contract relationship, the department monitors and reviews the organisation’s compliance with the service agreement’s requirements, including applicable departmental policies.
Complex Needs (MACNI and SfHRT) services are typically delivered by organisations with experience of delivering services on behalf of the department and have a solid understanding of the service delivery standards and accountability requirements (through a Service Agreement). Where such an organisation is new to delivering services against Complex Needs activity numbers, it is the role of the contracting group, through the Complex Needs Coordinator and the local Agency Performance and System Support (APSS) adviser to ensure the organisation is oriented to the MACNI legislative obligations, service framework, contract and performance requirements. Equally, where a service provider without a Service Agreement is used, the contracting group must ensure the department’s procurement and contract requirements are met.
The service agreement must be referenced in the care plan and linked to the existing service agreement in SAMS2.
While the Disability and Complex Clients Practice Advice and Support unit are responsible for setting the service provision framework: complex needs to support areas to manage the performance of MACNI and SfHRT, it is the responsibility of areas to transfer approved brokerage funding to the contracted service providers through funding and service agreements.
Requirements for brokerage agreements are set out in the table below.
Refer: Department’s funding and service agreements <https://intranet.dhhs.vic.gov.au/service-agreements>
Refer: Service agreement requirements <https://fac.dhhs.vic.gov.au/service-agreement-requirements>
Refer: Service agreement business rules and guidelines <https://intranet.dhhs.vic.gov.au/service-agreement-business-rules-and-guidelines>
Coordinator tasks• consult with your local Agency Performance and System Support (APSS) adviser to
determine the status of the provider's service agreement/service plan• initiate the request for a service agreement as required• ensure the service agreement is referenced in the care plan and linked in SAMS2.
15.7.2 Brokerage agreementsBrokerage agreements provide further detail supplementing the service agreement between the department and the agency in receipt of brokerage against activity 17250 or 91417. The brokerage agreement complements rather than replaces a funding and service agreement or contract with a service provider.
All areas are encouraged to have clear brokerage agreements with any service in receipt of MACNI or SfHRT funds. These agreements should outline the purpose of funds, unit costing, hours of service delivery, timeframes, quality assurance processes, acquittal requirements and parameters for recouping funds if the required tasks are unfulfilled. A standardised template for a brokerage agreement is available.
Page 70 Service Provision Framework: Complex Needs March 2020

All brokerage agreements are required to be submitted to the Complex Needs Panel for review and recommendation in accordance with the service provision framework: complex needs.
Requirements for brokerage agreements are outlined in the table below.
Documentation required• brokerage agreement.
Coordinator tasks• Prepare the brokerage agreement and seek approval from the appropriate financial
delegate.
15.7.3 Requirements for brokerage agreements and service agreementsAll one-off assessments listed below do not require a brokerage agreement if the amount is less than $25,000 per assessment, however, the quote must meet minimum requirements (Refer Section 15.7.4). Examples of assessments:
• independent living skills• neuro-cognitive• occupational therapy• psychological/psychiatric• risk assessments• speech pathology.
Requirements for all other services are subject to the thresholds in the following table.
Requirements for brokerage agreements and service agreements
Service provision funding amount Brokerage agreement required
Service agreement required
Assessments up to $25,000 No No – however, a service agreement may already exist
Care plan development Yes No – however, a service agreement may already exist
Care plan coordination Yes Yes* (exemptions apply)
All other services less than $5,000 No No – however, a service agreement may already exist
All other services between $5,000 and $25,000
Yes Consult with APSS
All other services greater than $25,000
Yes Consult with APSS
* for rural areas where service providers are limited, a service agreement may not be required – though it is preferred. In these instances, the department is responsible to ensure quality and safeguards are in place by confirming the below service provider details:
• details of qualifications, registrations and relevant experience
Service Provision Framework: Complex Needs March 2020 Page 71

• insurance provider• minimum quotation requirements.
15.7.4 Minimum quote requirementsWhen providing quotes for service, agencies are required to include the following information;
• business details – including contact details and ABN• details of qualifications, registrations and relevant experience• insurance provider – including insurance type and amount of cover• schedule for work• payment details, terms and conditions• breakdown of costs – including client items and hourly rates e.g. travel, report writing, etc.• variations• registration for GST• total cost• reference number.
15.7.5 ReimbursementComplex Needs Coordinators are able to use brokerage to reimburse organisations for goods and services that require payment up-front, however approval must be confirmed prior to the goods or services being purchased.
Reimbursements completed via SAMS2 will likely be delayed as SAMS2 variation windows are generally live in the first two weeks of the month. This delay in the reimbursement process should be clearly communicated to the organisation.
Where a service provider without a Service Agreement is used, the contracting group must ensure the department’s procurement and contract requirements are met; invoices may be paid via Oracle or using a departmental credit card. Please check with local administrative and finance services to clarify the preferred method.
15.7.5 Goods and Services Tax (GST)When purchasing services or entering into a Service Agreement with an organisation, Complex Needs Coordinators must check whether GST is payable to an organisation. GST is not payable where:
• the organisation is not registered for GST or does not have an ABN. Organisations are not required to be registered for GST if their annual turnover is below the ATO threshold of $75,000 (for commercial organisations) or $150,000 (for non-profit organisations)
• the Service Agreement is with a government entity (for example, local government, government schools, public hospitals) provided that the non-commerciality test is met by the entity receiving funds
• the services being supplied are not taxable supplies (applies to disability client support funding managed through a financial intermediary arrangement).
To check whether an organisation is registered for GST, you can refer to the Australian Business Register <https://abr.gov.au>
When setting up an organisation in SAMS2, an organisation’s GST status must be recorded, by marking whether the organisation is GST payable. For further information on setting up a new organisation record, you should refer to Chapter 4 Creating a new Service Agreement.
Page 72 Service Provision Framework: Complex Needs March 2020

Coordinator tasks• if unsure, check with the service provider whether GST is payable (some invoices may
be GST-free as they do not meet ATO thresholds)• ensure the correct account strings are used in Oracle to reflect non-GST and GST
applicable services.
15.7.6 Change in GST statusAn organisation’s GST status can change during the period of a service agreement, for example where an organisation becomes registered for GST that has not previously been registered or where an organisation cancels their GST registration.
The Service Agreement Systems and Operations team undertake a comparison between the Australian Business Register and SAMS2 on a regular basis and reports to the lead group/group/region where the status is changed.
When the department is aware of a change, you must record this in the organisation details section in SAMS2. The existing SAMS2 payment schedules will also need to be regenerated by the Service Agreement Systems and Operations team.
Where an organisation’s GST status is updated, and past payments did not have the correct GST amount, the Manager, Service Agreement Systems and Operations unit and the applicable tax manager from the paying department must be notified: The department tax manager will provide advice on whether GST needs to be paid or recouped from the organisation, based on the situation.
15.8 Probity When undertaking funding or procurement activities for or on behalf of the department, staff and contractors who may be assisting with these activities have a core responsibility to maintain and address probity principles at all stages of the funding or procurement cycle from planning through to transitioning in/out, and during contract management.
The Victorian Government Purchasing Board defines probity as:
• high standards of behaviour and actions in the conduct of procurement processes• ensuring equity and confidentiality• avoiding conflicts of interest• maintaining consumer/supplier confidence in the integrity of government procurement processes.Government business must be fair, open and must demonstrate the highest levels of integrity consistent with the public interest.
15.8.1 Key principles of probityKey principles of probity include the following.
• fairness and impartiality - Bidders are to be treated equally and must have the same opportunity to access information and advice. Selection methods including evaluation criteria should not favour particular bidders or particular solutions. The specification should not prefer a particular product or supplier. Personnel involved in the evaluation should be impartial towards all bidders.
• use of open, competitive processes (where possible) - A competitive process should be used as required by government policies.
• consistency and transparency of process:– bids are to be evaluated in a systematic manner against the published evaluation criteria.– records should be kept of all decisions and communications with bidders.
Service Provision Framework: Complex Needs March 2020 Page 73

– communications with bidders should only occur through the nominated contact person.– appropriate behaviour should be observed in all dealings with bidders on matters unrelated to the
procurement process.• security and confidentiality - the processes for receiving, managing and evaluating bids should
ensure their security and confidentiality.• identification and resolution of conflicts of interest - A conflict of interest declaration must be
completed by all staff involved in a procurement assessment process, whether a conflict exists or not. All conflicts, whether actual, potential or perceived, must be identified and registered, and managed and monitored by a senior manager.
The Complex Needs Coordinator has a responsibility to ensure that the development of the care plan, the associated brokerage budget and the review and acquittal of care plan budgets meet the department’s probity, procurement and records management requirements.
Refer: Probity <https://intranet.dhhs.vic.gov.au/probity-procurement-and-contract-management>
Refer: Probity in procurement and contract management <https://intranet.dhhs.vic.gov.au/probity-procurement-and-contract-management>
Refer: Records management requirements <https://intranet.dhhs.vic.gov.au/records>
15.9 Brokerage transfer to groupsAt the commencement of each financial year, the Manager, Disability and Complex Clients Practice Advice and Support arrange the transfer of complex needs brokerage funding to each group.
It is the responsibility of areas to transfer approved brokerage funding to the contracted service providers through funding and service agreements. Where a funding and service agreement is not applicable, a contract consistent with the department’s procurement policy is required. The transfer of brokerage funding includes the transfer of funds for care plan development and coordination services.
Areas are encouraged to have clear brokerage agreements with service providers receiving complex needs funds. These agreements outline the purpose of funds, unit costing, hours of service delivery, timeframes, quality assurance processes, acquittal requirements and parameters for recouping funds if the required tasks are unfulfilled. These agreements are not contracts that replace funding and service agreements, or procurement of services contracts. A standard brokerage agreement form is available which specifies the allocation of funding, the funding period, its purposes and any service providers engaged.
15.10 Transfer of brokerage between areasWhere a client supported by the complex needs team transfers between areas during the period of an approved care plan with attached brokerage, the funding commitment for the approved period is transferred from the exiting to the receiving area. The specific timeframes for transfer should be 6-12 weeks or as agreed between the relevant areas. Any subsequent care plans are subject to the approval processes of the receiving area.
15.11 Acquittal upon closureAt the termination or closure of a MACNI care plan, areas must ensure the care plan is reviewed, including the formal acquittal of allocated brokerage. In some cases, the use of approved brokerage may continue for a short period of time post-closure while in transition from MACNI to the existing service system. It is the responsibility of the Complex Needs Coordinator to continue to monitor and ensure the appropriate acquittal of MACNI commitments and expenditure is performed.
Page 74 Service Provision Framework: Complex Needs March 2020

Coordinator tasks• ensures all departmental actions are taken in relation to the closure of the care plan:
– funding acquittal– conclusion of funding to the care plan coordination service– completion of data and record management requirements.
15.12 Brokerage recording and reporting in SharePoint and the Complex Support ApplicationAreas record brokerage expenditure approved by the Area Director or Group Deputy Secretary and acquit the allocation against each client in the SharePoint brokerage database. This data is then able to be analysed using the CSA provided by the Disability and Complex Clients Practice Advice and Support unit.
The CSA enables groups and areas, to monitor and acquit commitments and expenditure by client within their brokerage budget. Several standardised reports have been developed within the application for ease of access.
Coordinator tasks• use the SharePoint brokerage database to enter all brokerage requests and acquittals• update data fortnightly (at minimum)• regularly review the Complex Support Application to monitor progress against
allocations and group/area budgets.
16. Quality, safeguards and critical events
The department’s standard quality safeguards and critical event instructions apply to the delivery of Complex Needs services.
16.1 Child safe standardsVictorian organisations that provide services or facilities for children, including the department, are required by law to implement and comply with the child safe standards. The standards are designed to:
• drive changes in organisational culture to embed child safety in the everyday thinking and practice of leaders, staff and volunteers
• provide a minimum standard of child safety across all organisations• highlight that we all have a role to keep children safe from abuse, encourage reporting of any harm or
abuse that does occur and improve organisational responses to allegations.
Refer: Child Safe Standards <https://intranet.dhhs.vic.gov.au/child-safe-standards>
16.2 Human services standards Services purchased using complex needs brokerage are typically delivered by community service organisations and Aboriginal community-controlled organisations through a service agreement with the department against activity number `17250’.
Organisations funded to provide services to clients are required through the service agreement to meet the gazetted Department of Health and Human Services Standards (Human services standards) and can be monitored against their compliance with the standards.
Service Provision Framework: Complex Needs March 2020 Page 75

The human services policy and funding plan 2015-19 provides funded organisations and departmental staff with information about the department’s policy framework, objectives, budget, service deliverables, desired outcomes, reporting requirements, program guidelines and funding initiatives.
Refer: Service agreement information <http://www.dhs.vic.gov.au/facs/bdb/fmu/service-agreement/contents>
Refer: Human Services Standards https://providers.dhhs.vic.gov.au/human-services-standards
16.2.1 Service provider information packUpon being appointed to deliver formal MACNI services (care plan coordination), service providers are required to be provided with a suite of documents that contain key information, standards, legislation and policy. This service provider information pack is compliant with the Human Services Standards and its content is evidenced on a checklist.
The checklist is to be completed and returned to the DHHS Complex Needs Coordinator 3 months after commencement of service provision. This checklist will be reviewed annually until MACNI closure
Refer: Human Services Standards <https://intranet.dhhs.vic.gov.au/human-services-standards>
Documentation required
• Formal MACNI service provider information checklist and supplementary documentation.
Coordinator tasks• provide a service provider information pack to services offering formal MACNI
services and ensure understanding of its contents and purpose• ensure a representative from the service provider signs the checklist 3 months after
commencement of service provision, and annually thereafter.
16.3 Human rights charterThe Charter of Human Rights and Responsibilities Act 2006 (the Charter) is a Victorian law that sets out the basic rights, freedoms and responsibilities of all people in Victoria. The Charter requires public authorities, such as Victorian state and local government departments and agencies, and people delivering services on behalf of the government, to act consistently with the human rights in the Charter.
Twenty fundamental human rights are protected in the Charter because the Victorian Parliament recognises that we all have basic rights, including the right to be treated equally, to be safe from violence and abuse, to be part of a family and to have our privacy respected. In certain circumstances, some rights may be limited but this must be necessary and reasonable, with clear reasons for the decision.
The delivery of Complex Needs services must be in compliance with the Charter.
Refer: Human Rights Charter <https://intranet.dhhs.vic.gov.au/human-rights-charter>
16.4 Client refusalWhen a referral to MACNI is under consideration, a service provider and/or departmental staff should seek the agreement of the client.
Before a client can be referred to MACNI for determination of eligibility for services under the Act, the client must receive a written notification containing specific information. The client must be advised that they have the option of refusal to have their eligibility considered and that they may refuse to participate in MACNI at any time.
Page 76 Service Provision Framework: Complex Needs March 2020

A refusal can be made to any provider, the care plan coordinator or any delegate of the Secretary. It can be made at any stage of involvement in MACNI, including during the care plan development process or its implementation.
Once a care plan has been developed and/or is being coordinated, and the client communicates a refusal to participate in MACNI, the care plan coordinator or person being advised must determine if the client’s statements of refusal are a true reflection of their wishes. The level of impairment and behavioural profile of some clients suggest that willingness to participate may vary from day to day. Hence, the worker receiving the refusal must form a professional judgement about the intention of the client. A process for checking back with the client about the refusal is recommended before MACNI services are formally ceased.
16.5 Client participation Complex Needs and MACNI processes, including panel deliberations, are designed to assess and review the changing needs and experiences of clients at regular intervals.
Client participation in the identification of priority goals and needs for address through a care plan is initially established by both the referring service and the care plan developer.
Departmental and/or funded community organisation staff meet with the client, their family/carer/guardian and/or the services engaged in the care plan to review the achievement of identified goals. A revised care plan builds on the views, experience and perceived progress of the client (and involved services).
If appropriate, clients and/or their families/guardian may be invited to participate in regular care team meetings (whole or part) and may be provided with a summary of discussion topics if it is in their best interests.
16.5.1 Complex needs client information packUpon being considered for formal MACNI services, clients should be provided with a suite of documents that contain information regarding privacy, information sharing, making a complaint and the department’s client services charter. This client information pack is compliant with the Human Services Standards and ensures information sharing is actively undertaken throughout service provision.
Refer: Human Services Standards <https://intranet.dhhs.vic.gov.au/human-services-standards>
Documentation required
• Formal MACNI client information checklist and supplementary documentation.
Coordinator tasks• provide a client information pack to eligible clients and ensure understanding of its
contents and purpose. This task may be better facilitated by the Care Plan Coordinator or key worker.
16.6 Privacy and confidentialityThe department and funded organisations have access to personal information and health information about clients. The department and funded organisations are obliged to protect the privacy of this personal and health information.
However, sharing information about clients is a legitimate part of providing services and keeping people safe. In sharing information, staff have a responsibility to protect the interests of clients, to respect their privacy and share information appropriately when it is in a client’s best interests. Information may only be shared in accordance with the law.
Service Provision Framework: Complex Needs March 2020 Page 77

Complex Needs service responses operate in accordance with privacy and confidentiality requirements under relevant legislation: Human Services (Complex Needs) Act 2009; Information Privacy Act 2000; Health Records Act 2001; Disability Act 2006; Housing Act 1983, Children, Youth & Families Act 2005; Mental Health Act 2014, Corrections Act 1986 and Severe Substance Dependence Treatment Act 2010.
16.6.1 Human Services (Complex Needs) Act 2009The Human Services (Complex Needs) Act 2009 aims to achieve an appropriate balance between the protection of personal information and the need for disclosure in the best interests of the client. The nature of the MACNI client group means that much of the existing information available about a client may be sensitive.
Under the Act, relevant persons have specific responsibilities and limitations in relation to the sharing of information. The Act defines `relevant persons’ as
• the Secretary (or a delegate)• a person who is or has been engaged or appointed by the Secretary• a service provider to whom a client has been referred for the development of a care plan • any person or organisation that provides or has provided welfare, health, mental health, disability,
drug and alcohol treatment, offender, emergency, or housing and support services to the client• a service provider in a care plan, or a person who is or has been involved in the management of,
engaged or employed at or worked for or at the Public Advocate, the Tribunal or department.
It is an offence for the relevant person to disclose to any other person any personal or health information acquired through their engagement of functions under the Act (except to the extent necessary to carry out functions under this Act or any other Act or regulations made under any other Act).
It is an offence for a relevant person to disclose to another person if a client is:
• or has been an eligible person• being considered for eligibility• a person to whom a care plan relates• a member of any such person’s family.
The Act specifically allows the Secretary and, if there is a service provider contracted by the Secretary, a service provider to seek information about the client from any person or organisation for the limited purpose of developing a care plan. The Act authorises the Secretary, the Public Advocate, the Mental Health Tribunal and any person or organisation providing services to the eligible client to disclose information about this person for the purpose of care plan development.
The Act also allows service providers identified in the care plan to disclose information about a client to another service provider identified in the care plan. This should only occur if the information exchange is in the best interests of the client and the disclosure of the information assists the second service provider to implement the care plan. The Act specifies the limited purpose for which information can be exchanged as when it will assist in giving effect to the care plan. This relates to the development of a care plan and the implementation, monitoring and review of the care plan.
The Act does not compel service providers to exchange information, rather it allows them to make a professional judgement based on what they believe will be in the best interests of the client.
The Privacy and Data Protection Act 2014 and the Health Records Act 2001 provide additional obligations to confidentiality and nothing in this Act affects those obligations.
More broadly, there are a range of policies and resources at the department level to guide practice for appropriate information-sharing and privacy protection.
Page 78 Service Provision Framework: Complex Needs March 2020

Where the request to share or release information with a third party is declined, the Care Plan Coordinator or Complex Needs Coordinator is required to escalate the issue through the relevant service provider (e.g. Hospital, Justice Health, etc).
Refer: Privacy <https://intranet.dhhs.vic.gov.au/privacy>
Refer: Sharing information for better outcomes for children and families https://intranet.dhhs.vic.gov.au/sharing-information-better-outcomes-children-and-families
16.7 Documented consentThe client’s consent is required for each type of Complex Needs service, including at each stage of the MACNI process, from consultation through to formal MACNI. The referrer is responsible for obtaining consent from the client/tenant prior to the referral or consultation, unless duty of care overrides this (see Section 16.8). Consent must also be renewed when the client turns 18.
Prior to a referral for the consideration of a client’s eligibility under the Act, the client receives written notification stating that participation in MACNI is voluntary and that the client can discontinue at any point prior and after a care plan has been developed.
Upon consideration for formal MACNI, a standardised eligibility consideration letter is provided/sent to the client to seek their consent for the consideration of eligibility, including a Consent for eligibility determination form.
The client may at any time refuse to be considered for eligibility or to be the subject of a care plan.
Documentation required• consent for Complex Needs services (to obtain, update or renew consent)• consent for MACNI referral and eligibility consideration.
Coordinator tasks• ensure consent is obtained/renewed:
– upon receiving Complex Needs services – at each stage of the MACNI process– when the client reaches 18 years of age.
16.8 Duty of care referrals Where a staff member or service provider holds considerable concern for the welfare or wellbeing of the client, or member/s of the public, a duty of care referral may be actioned. Duty of care referrals allow for the disclosure of client information pursuant to the department’s privacy policy without prior consent and without breaching the Information Privacy Principles (IPPs).
A duty of care referral is recommended where the organisation reasonably believes that the use or disclosure is necessary to lessen or prevent:
(i) a serious threat to an individual’s life, health, safety or welfare; or
(ii) a serious threat to public health, public safety of public welfare.
Note, if there is an imminent and direct risk of crisis involving the client, these should be directed to the appropriate emergency/ statutory services, such as police, ambulance or child protection.
Refer: Privacy Policy <https://intranet.dhhs.vic.gov.au/search/privacy%20policy>
Service Provision Framework: Complex Needs March 2020 Page 79

Refer: Information Privacy Principles <https://ovic.vic.gov.au/privacy/for-agencies/information-privacy-principles/>
Documentation required• Consent for Duty of Care referral.
Coordinator tasks• upon receiving a duty of care referral, provide the referrer with the additional consent
for duty of care referral form • ensure the duty of care referral is endorsed by:
– Supervisor / Team Leader / Manager of the referrer– Manager Client Support and Housing Services.
16.9 Client feedback and complaintsThe department’s feedback including compliments and complaints management policy and associated procedure provide the overarching framework for how the department manages compliments, complaints and the role and responsibilities in relation to these matters.
All clients receiving service support from the Complex Needs team receive information about how to make a complaint. Specifically, MACNI clients receive information about how to make a complaint to the department in the written notification provided when they are being considered for eligibility and have been determined as eligible for MACNI.
Where a client raises a complaint, they should be supported to seek to resolve the matter directly in the first instance (whether that is to a community organisation or the department).
MACNI clients typically receive care plan coordination through a funded community service organisation. The community service organisation will have a complaint and feedback process in relation to the services it delivers. The care plan coordinator is responsible for ensuring MACNI clients are familiar with processes for making a complaint.
Where the matter is unable to be resolved at this level, the complaint should be referred to the department.
Refer: Making a complaint <https://www.dhhs.vic.gov.au/making-complaint>
Refer: Service feedback <https://intranet.dhhs.vic.gov.au/service-complaints>
16.10 Appeal of MACNI service decisionsMACNI clients may appeal or request a review of actions relating to a departmental action that the client believes has/will adversely and directly affect them. The following events in the MACNI service model may result in an appeal by a client:
• eligibility determination• care plan content and approval• care plan review• care plan suspension• care plan closure.Decisions about these key MACNI interventions are either made or recommended by a panel.
A client may raise a request for appeal via any service provider engaged in the delivery of support, including the care plan coordinator and/or the Complex Needs Coordinator.
Page 80 Service Provision Framework: Complex Needs March 2020

The client’s appeal may be verbal, in writing or another format that is accessible for them. Where an appeal by a client is indicated, the right to appeal should be actively supported for a resolution that is transparent and responsive to the issue raised.
The Complex Needs Coordinator should schedule the appeal for an upcoming panel to consider and resolve through the provision of explanation, revised decision, feedback, rationale for decisions and/or apology.
Where a panel cannot resolve an appeal, the matter will be escalated to the relevant Area Director to assist with resolution.
16.11 Accessing recordsA client can ask for access to their personal, health and sensitive information held by the department by contacting:
• their nominated case manager/worker (including a Complex Needs Coordinator)• the department area that has the information• the Freedom of Information Unit via 1300 650 172 or 03 9096 8449.
Clients receiving services from Aboriginal community-controlled and community service organisations should approach their worker or staff in the organisation to understand the policy and process for accessing their records held by that organisation.
16.12 Client Incident Management System (CIMS)The department’s Client Incident Management System (CIMS) focuses on the safety and wellbeing of clients. The CIMS empowers service providers to effectively respond to and manage client incidents, to be accountable for their actions and to manage the quality of their own services.
CIMS commenced from January 2018 and applies to services delivered by the department and our funded organisations, including children, youth and family services; disability services; health services; housing and community-building services; youth services and National Disability Insurance Scheme providers during transition to full scheme roll-out in 2019. Exempted are the services which report through the Victorian Health Incident Management Systems (VHIMS).
Refer: Client incident management system <https://providers.dhhs.vic.gov.au/cims>
Complex needs services do not have obligations/requirements to report incidents as their role is not direct client work, this responsibility lies with the services that are contained within a care plan. These services should have their own incident management reporting systems. Note, Complex Needs Coordinators and members of the care team may be invited to participate in the incident investigation process.
16.13 Quality of support and quality of care review processes
16.13.1 Guidelines for responding to quality of care concerns in out-of-home careThe guidelines for responding to quality of care concerns in out-of-home care have been developed to ensure that quality of care concerns relating to home-based carers (including lead tenants), residential carers and kinship carers are responded to in a consistent and timely manner. The department wants to be confident that children and young people in care are safe and well cared for, and that carers are supported and treated fairly while quality of care concerns are investigated.
Quality of care concerns refers to any concern that has the potential to compromise a child’s safety, stability and development and may relate to a broad range of issues from minor quality concerns, such as inadequate supervision, through to allegations of possible physical or sexual abuse.
Service Provision Framework: Complex Needs March 2020 Page 81

The guidelines specify that all concerns about possible physical, sexual or emotional abuse, neglect or other quality of care concerns must initially be screened to determine the exact nature of the concern and the most appropriate response.
Refer: Responding to quality of care concerns <http://providers.dhhs.vic.gov.au/responding-quality-care-concerns>
16.14 Aboriginal and Torres Strait Islander cultural safety frameworkThe department believes that everyone has a responsibility for the cultural safety of Aboriginal people in their organisation and how they work with Aboriginal staff, health consumers and clients.
The Aboriginal and Torres Strait Islander cultural safety framework has been developed to help mainstream Victorian health, human and community services and the department to create culturally safe environments, services and workplaces. Cultural safety is about creating an environment that is safe for Aboriginal and Torres Strait Islander people.
The framework provides a continuous quality improvement model to strengthen the cultural safety of individuals and organisations. It aims to help the department and mainstream health, human and community services to strengthen their cultural safety by participating in a process of continuous learning and practice improvement.
The development of the framework is a key commitment in the department's Aboriginal employment strategy 2016–2021 and in Korin Korin Balit-Djak: Aboriginal health, wellbeing and safety strategic plan 2017– 2027. The framework will support Korin Korin Balit-Djak to achieve the Victorian Government's vision of 'self-determining, healthy and safe Aboriginal communities'.
Refer: Aboriginal and Torres Strait Islander cultural safety framework <https://dhhs.vic.gov.au/publications/aboriginal-and-torres-strait-islander-cultural-safety-framework>
16.15 The NDIS Quality and Safeguards CommissionFrom 1 July 2019, the NDIS Commission commenced operating in Victoria. The NDIS Commission is responsible for implementing the NDIS Quality and Safeguarding Framework, taking over Victoria’s existing quality and safeguards arrangements for NDIS participants and services.
Functions transitioning to the NDIS Commission include registration and quality assurance of providers, incident reporting, complaints and oversight of restrictive practices. The Victorian Senior Practitioner continues to have a role in authorising the use of regulated restrictive practices. Victoria also retains responsibility for NDIS Worker Screening.
The NDIS Commission is an independent government body that works to improve the quality and safety of NDIS services and supports, investigates and resolves problems, and strengthens the skills and knowledge of providers and participants.
The NDIS Commission provides a single, national registration and regulatory system for NDIS providers setting a nationally consistent approach to regulation of NDIS supports and services.
The NDIS Commission introduced several changes for Victorian providers. These include a new NDIS Code of Conduct and NDIS Practice Standards, which set out expectations for the quality and safety of the services and supports providers deliver. There have also been changes to provider registration and the way complaints are made, incidents are reported, behaviour support plans are developed and reported, and worker screening is undertaken.
For a limited time (up to 18 months), Victoria will continue operating quality and safeguards for in-kind services and state-funded clients delayed transition into the scheme. The NDIS Commission will work with existing state-based agencies and regulatory bodies to handle complaints and manage reportable incidents from dual regulated providers to ensure quality and safeguards are working as intended.
Page 82 Service Provision Framework: Complex Needs March 2020

Further information and resources for disability service providers, including obligations around quality and safeguards is available on the Victorian Government’s NDIS website:
Refer: NDIS providers in Victoria https://www.vic.gov.au/ndis-providers-victoria
The NDIS Commission’s website also has further information:
Refer: The NDIS Quality and Safeguards Commission <https://www.ndiscommission.gov.au/>
16.16 Community services quality governance frameworkEffective quality governance is fundamental to consistently delivering safe, effective, connected and person-centred community services. Developed by the Community Services Quality and Safety Office, the community services quality governance framework sets the objective of safe, effective, connected and person-centred community services for everybody, every time.
High-quality services and outcomes for every Victorian require everyone at every level in community services to play a role. Everyone from support staff to practice leaders, CEOs and departmental staff should focus on:
• partnering with clients, families and communities• regular reviews, evaluation and identifying areas for improvement• ownership and accountability for the quality of services provided.The framework has been developed to align with and complement existing quality and safety accreditation or frameworks that organisations currently have in place. The service provision framework: complex needs aligns closely with the principles outlined in the community services quality governance framework.
Refer: Community services quality governance framework <https://intranet.dhhs.vic.gov.au/about-us/news-events/news/community-services-quality-governance-framework>
16.17 Records managementThe department’s records management policy is to ensure that comprehensive and accurate records of all activities and decisions of departmental staff are created, managed and kept in accordance with relevant legislation. This requires recordkeeping practices and systems that ensure the creation, maintenance and protection of accurate and reliable records.
Records underpin the department’s transparency and accountability by providing proof of business practices, communications, decisions and actions.
Records are an important information asset of the department and must be managed from the point of creation to their eventual destruction or transfer to the State Archives.
The department also owns all records created by organisations in the delivery of services funded by the department.
Refer: Records <https://intranet.dhhs.vic.gov.au/records>
16.17.1 TRIM / TRIM EDRMTRIM EDRM is the department’s Electronic Document Management and recordkeeping system. TRIM EDRM is an approved storage location which will bring the department into line with the statutory requirements set by the Public Records Act 1973.
It’s a tool that allows staff to create, edit, revise, co-author, share and search for electronic documents more easily across the department. The program is supporting the department by transitioning from hardcopy to electronic documents and records management with TRIM EDRM.
Service Provision Framework: Complex Needs March 2020 Page 83

The use of TRIM EDRM ensures the department’s information is managed in a compliant way; it’s secure and more efficient than working across shared drives and managing hardcopy files.
A record is any information, regardless of the format, that provides evidence of a business activity or decision. All records must be saved in TRIM.
TRIM EDRM is being rolled out across all areas of the department, and at July 2019 some areas are waiting to transition. For those areas, Complex Needs Coordinators are expected to maintain hard copy and soft copy files on their local drives consistent with the TRIM EDRM file structure as set by the Disability and Complex Clients Practice Advice and Support unit. This includes:
• MACNI entry and consultation• assessment reports and plans• client care planning• Complex Needs Panel• brokerage• correspondence.Note: these are the high-level files, sub-headings exist within each file.
Files and documents in TRIM-EDRM should be named consistently, logically and meaningfully, in line with departmental naming conventions available on the Intranet.
Refer: TRIM EDRM <https://intranet.dhhs.vic.gov.au/trim>
16.17.2 Client files and case notesA record of each complex needs referral will be maintained in accordance with departmental policy and procedure for those identifiable clients for whom services are provided.
All MACNI eligible clients are required to have a TRIM file created; hard copy for those areas yet to transition or TRIM EDRM for those areas who have transitioned. The structure of files (TRIM EDRM or hard copy) should be consistent with the TRIM EDRM file structure as set by the Disability and Complex Clients Practice Advice and Support unit (see 15.16.1). Depending on the documentation generated for any Complex Needs referral, a separate client file may be created.
Complex needs consultations may at times be brief and not require the Complex Needs Coordinator to know the identity of the client. In these instances, a record is kept of the event/intervention provided, e.g. secondary consultation, to ensure a record of activity is maintained. In these instances, a separate client file is not practical, and records may be filed together with multiple records contained within one file titled ‘Consultations’.
Complex Needs Coordinators may also maintain case notes for each client, to document actions, key events and outcomes (e.g. Complex Needs Panel or legal process).
Complex Needs Coordinators must ensure that all records are kept secure using locked filing cabinets or password protected/restricted access profiles).
Documentation required• Complex Needs case note• any relevant client documentation
Coordinator tasks• ensure client files are maintained and securely stored in accordance with
departmental policy and procedure
Page 84 Service Provision Framework: Complex Needs March 2020

16.18 Escalation to Disability and Complex Clients Practice Advice and SupportThere are a number of instances where consultation with the Disability and Complex Clients Practice Advice and Support unit is required. This includes any action that is non-compliant with the service provision framework: complex needs. The Manager, Disability and Complex Clients Practice Advice and Support is required to be contacted:
• where clarification is required regarding the service provision framework: complex needs or supporting documentation (e.g. the Act)
• requests to vary a standard procedure outlined in the Service provision framework: Complex needs• any proposal to exceed set brokerage limits (e.g. more than $15,000 for a Pre-MACNI client)• brokerage requests for items not included in the service provision framework: complex needs• brokerage funding where the expenditure would result in an area/group overspending its allocated
brokerage budget• requests to remunerate an expert adviser to participate in a Complex Needs Panel if unavailable from
the standard service system.
Coordinator tasks• Seek policy advice and direction to the Disability and Complex Clients Practice Advice
and Support unit as appropriate.
17. MACNI quality and performance reporting
Areas maintain data in the SharePoint databases. This data is able to be analysed via the Complex Support Application (CSA) which is reviewed regularly by the Disability and Complex Clients Practice Advice and Support unit.
Coordinator tasks• update the SharePoint databases with relevant client, care plan and brokerage data
on a fortnightly basis (minimum)• utilise report functions in the CSA to view and monitor client, area and group-specific
information.
17.1 Key performance indicatorsKey performance indicators were introduced for MACNI effective 1 July 2015. The performance indicators are to be adhered to by all funded services providing MACNI care plan development and coordination against activity ‘17250’.
The indicators are:
• the client has an assessment and recommended care plan within 12 weeks of eligibility• the client has a recommended transition plan at least six months prior to the planned MACNI care
plan termination.
Complex Needs Coordinators are expected to monitor organisation adherence and consider the indicators when developing panel schedules.
Service Provision Framework: Complex Needs March 2020 Page 85

Funded care plan development and coordination services may reasonably request Complex Needs Coordinators to consider panel rescheduling if key performance indicator achievement is likely to be negatively impacted by maintaining the schedule already in place.
It is the responsibility of Complex Needs Coordinators and funded services to manage panel demands effectively in line with the key performance indicators. Achievement of key performance indicators is based on the dates on which a panel consideration occurs, not the date a service submits the care planning documents to the Complex Needs Coordinators.
17.2 Performance targetsThe following are MACNI targets:
• 90% of care plans are recommended by the Panel within 12 weeks from the date of eligibility• 100% of clients have an exit transition plan recommended at least six months prior to care plan
termination.
17.3 Performance reporting The areas are required to collect and maintain data on:
• performance targets• referral targets (contacts)• client demographics• activity across consultation, Pre-MACNI and MACNI eligible client services.
The above information can be entered and edited in SharePoint. The SharePoint database was launched on 1 November 2019 and replaces the previous Excel-based data entry system. Complex Needs Coordinators are able to record data which is then collated and analysed for reporting purposes.
The CSA is an interactive data analysis and reporting tool for MACNI and replaces the previous Excel-based quarterly data collection system. The CSA is built on the QlikView Business Discovery Platform and is a data visualisation tool which provides the following capabilities:
• data analysis through the use of graphs, tables and charts• workload oversight and management • budget oversight and management • target monitoring• reporting to meet the needs of multiple audiences.
The CSA was launched 1 April 2019 and is anticipated to improve the quality of data analysis for Complex Needs service responses. It will inform the department’s knowledge of, and responses to complex clients and the identification of trends across cohorts and department areas.
17.3.1 What is a Complex Needs / MACNI contact?For data recording purposes and to ensure consistency, a contact is defined as:
"a period of service (consultation / Pre-MACNI / Formal MACNI / Post-MACNI) in which there is regular contact and consultation with the DHHS Complex Needs Coordinator. This contact is confined by a start and end date.”
The contact may involve the DHHS Complex Needs Coordinator undertaking a variety of tasks including:
• facilitate assessment• information and practice advice• system navigation and problem-solving
Page 86 Service Provision Framework: Complex Needs March 2020

• capacity-building• time-limited care coordination
A new contact is counted when:
• any period of service commences • a client transitions from one support level to another (e.g. Consultation to Formal MACNI, Pre-MACNI
to Formal MACNI, etc.)
If the circumstances meet requirements for closure, a closure/recommendations form is completed, and the end date is recorded in the CSA/SharePoint. If the client is re-referred some weeks/months/years later, a new line of data is created, with the new commencement date entered. That is, each contact is a new line of data, even if it is for the same client within the same financial year.
One client may have numerous contacts over a financial year. For example, initially a contact for 2-months, then a second contact for 4-months, then a third contact for 1-month consultation.
Alternatively, a Formal MACNI client will have 1 consultation over a number of months / years, up to 3 months in total. This may be recorded as 1 contact each financial year.
What does not constitute a contact?
• quick, one-off questions regarding service provision• brief conversations held in passing• client details / information exchange that is insufficient to populate a client registration form.
17.3.2 Data sources• The SharePoint database – recorded by Complex Needs Coordinators
– client databases (MACNI and SfHRT)– brokerage database
• Complex Support Application (CSA) • reporting as agreed with funded service agencies.
17.3.3 Data analysis for service planningAreas maintain data via SharePoint which is then analysed in the CSA. The Disability and Complex Clients Practice Advice and Support unit regularly review the CSA to identify:
• trends in client demographics/service profile • service access barriers• area and group performance against the MACNI key performance indicators• the use of brokerage funding, including expenditure/equity/accountability and implications for
resourcing requirements.
An annual complex needs report is compiled which details the achievement of key performance indicators and targets and provides a view of MACNI clients at the state-wide, group and area level.
The annual report is available to MACNI stakeholders which includes but is not limited to: areas; groups; engaged community service organisations; the Director of Housing; and the Department of Justice and Community Safety.
Service Provision Framework: Complex Needs March 2020 Page 87

18. SfHRT quality and performance reporting
18.1 Performance targetsSfHRT referral targets are set by the Disability and Complex Clients Practice Advice and Support unit each year. They are allocated at a group level and are based on previous year targets.
Information regarding how the client and service providers are supported (including hours per week) is recorded on HiiP and the SharePoint database.
There are no Key Performance Indicators.
18.2 Performance reportingComplex Needs Coordinators are required to collect and report on:
• referral targets (contacts)• client demographics• brokerage expenditure• activity across consultation and SfHRT eligible client services.
The above information is recorded and analysed in two systems; SharePoint and the CSA. The Housing Integrated Information Program (HiiP) also provides a platform to document activity which can be readily accessed by housing staff.
18.2.1 What is a SfHRT contact?For data recording purposes and to ensure consistency, a contact is defined as:
"a period of SfHRT service response in which there is contact and consultation with the DHHS Complex Needs Coordinator. This contact is confined by a start and end date.”
The contact may involve the DHHS Complex Needs Coordinator undertaking a variety of tasks including:
• facilitate assessment• information and practice advice• system navigation and problem-solving• capacity-building• time-limited care coordination• providing brokerage
A new contact is counted when:
• any period of service commences (including those that only request brokerage) • a client transitions from one support to another (e.g. SfHRT to Pre-MACNI etc.)
If the circumstances meet requirements for closure, a closure/recommendations form is completed, and the end date is recorded in the CSA/SharePoint. If the client is re-referred some weeks/months/years later, a new line of data is created, with the new commencement date entered. That is, each contact is a new line of data, even if it is for the same client within the same financial year.
One client may have numerous SfHRT contacts over a financial year. For example, initially a contact for brokerage assistance only, then a second contact for 3-months, then a third contact for 1-month consultation.
What does not constitute a contact?
Page 88 Service Provision Framework: Complex Needs March 2020

• quick, one-off questions regarding service provision• brief conversations held in passing• client details / information exchange that is insufficient to populate a client registration form.
18.2.2 Data sourcesRelevant qualitative data should be included in case file notes in HiiP and SharePoint.
Housing Integrated Information Program (HiiP)
Complex Needs Coordinators will record the actions taken under the tenant’s client number in HiiP.
SharePoint
The SharePoint databases are used to record data for client demographics and brokerage. For each referral, a record should be kept regarding consultation dates, intervention or services provided, support hours and brokerage allocation.
Complex Support Application (CSA)
The CSA is used to analyse data for client demographics and brokerage.
Coordinator tasks• update HiiP with relevant data, including qualitative content where appropriate• ensure SfHRT referral box is selected in HiiP• record client demographics and brokerage using SharePoint databases• utilise report functions to view and monitor group, client and area-specific information.
18.2.3 Data analysis for service planningThe Disability and Complex Clients Practice Advice and Support unit reviews the SfHRT data to identify:
• trends in client demographics/service profile• systemic issues e.g. barriers to service access• performance against the set key performance indicators• the use of brokerage funding.
Service Provision Framework: Complex Needs March 2020 Page 89

19. Complex needs contacts
There are seventeen areas across four groups of the department. Each area has a Complex Needs Coordinator, who is the first point of contact for MACNI, SfHRT and complex needs queries.
North Group
Area Office location Contact
North East Melbourne Preston 1300 664 977
Hume Moreland Broadmeadows 03 9309 1511
Loddon Bendigo 03 5434 5555
Mallee Mildura 03 5022 3111
East Group
Area Office location Contact
Inner Eastern Melbourne Box Hill 03 9843 6000
Outer Eastern Melbourne Ringwood 03 9871 5199
Goulburn Shepparton 03 5832 1500
Ovens Murray Wangaratta 03 5722 0555
South Group
Area Office location Contact
Southern Melbourne Dandenong 03 8765 7629
Bayside Peninsula Dandenong 03 8765 7341
Inner Gippsland Morwell 1800 650 813
Outer Gippsland Sale 03 5144 9100
West Group
Area Office location Contact
Western Metropolitan(Western Melbourne & Brimbank Melton)
Footscray 1300 360 462
Sunshine 03 9229 4100
Central Highlands Ballarat 03 5333 6726
Barwon Geelong 03 5226 4540
Wimmera South West Warrnambool 03 5561 9444
Page 90 Service Provision Framework: Complex Needs March 2020

20. Complex needs templates
The following templates are available from the Complex Needs Coordinators for areas and groups to support the delivery of services consistent with this framework:
1 Complex Needs consultation form
1a Complex Needs care plan
1b Complex Needs recommendations and closure form
1c Complex Needs case note
2 MACNI assessment and care plan development report
3 MACNI care plan
4 MACNI transition/exit plan
5a Consent for Complex Needs services
5b Consent for MACNI referral and eligibility consideration
5c Consent for Duty of Care referral
6a Complex Needs Panel information pack checklist
6b Complex Needs Panel manual
6c Complex Needs Panel Terms of Reference
6d Complex Needs Panel member prompt sheet
6e Complex Needs Panel Deed of Confidentiality
6f Complex Needs Panel agenda
6g Complex Needs Panel minutes – to panel members
6h Complex Needs Panel session report – to a specific care team
6i MACNI eligibility consideration request form
6j MACNI care plan review report
6k MACNI progress update report
6l MACNI care plan closure report
6m Complex Needs Panel out of session request form
7a Brokerage checklist
Service Provision Framework: Complex Needs March 2020 Page 91

7b Brokerage request form
7c Brokerage agreement
7d Brokerage notification template – for Complex Needs Panel
8a MACNI eligibility consideration notification – letter to client, parent/guardian
8b MACNI eligibility decision notification – letter to client, parent/guardian
8c MACNI care plan notification – letter to client, parent/guardian with care plan (or a version of) attached
8d MACNI care plan suspension notification – letter to client, parent/guardian
8e MACNI care plan suspension notification – letter to services within the care plan
8f MACNI care plan closure notification – letter to client, parent/guardian
8g MACNI care plan closure notification – letter to services within the care plan
9 Formal MACNI client information checklist
10 Formal MACNI service provider checklist
11 New staff orientation checklist
21. MACNI booklets
In addition to the service provision framework: complex needs, three booklets have also been developed. These target specific audiences external to the department:
• Getting it together: Multiple and Complex Needs Initiative (for service providers and/or carers)• Care Plan Coordination: A guide for service providers on the Multiple and Complex Needs Initiative
(for care plan coordinators)• Support for you: How the Multiple and Complex Needs Initiative can assist you (for clients).
Page 92 Service Provision Framework: Complex Needs March 2020

Appendix 1 Legislative requirements to be met throughout MACNI service provision
MACNI ServiceHuman Services (Complex Needs) Act 2009 Section
Legislative requirement
Eligibility 9 Notice to be given to persons before determination is made
The Act requires that a person is not considered for the determination of eligibility if the person refuses to be considered and that the person may at any time refuse to be considered for eligibility or to be the subject of a care plan.The Act requires that before a person can be considered, the department must notify the person in writing that the department:• may consider whether the person appears to be eligible unless the person refuses to be considered for
eligibility• will ensure a care plan is developed if eligible unless the person refuses to be the subject of a care plan
• may seek to obtain from any person or organisation health and/or personal information about the person for the purpose of considering whether the person is eligible or developing them a care plan
• may disclose health and/or personal information about the person to a service provider identified their care plan if the department is satisfied that the disclosure is in the best interests of the person and would assist the service provider in giving effect to the care plan, and of how to contact the relevant department contact.
At the same time, the person is notified that a care plan coordinator:• may seek to obtain from any person or organisation health and/or personal information about the person for
the purpose of developing their care plan• may disclose personal information or health information about the person to another service provider
identified in the care plan if the first-mentioned service provider is satisfied that the disclosure is in the best interests of the person and would assist the second-mentioned service provider in giving effect to the care plan.
Service Provision Framework: Complex Needs March 2020 Page 93

MACNI ServiceHuman Services (Complex Needs) Act 2009 Section
Legislative requirement
Eligibility 10 Secretary to notify person of determination of eligibility
The department must notify in writing a person whose eligibility has been considered whether or not the department has determined that the person is eligible.The Complex Needs Coordinator ensures that the above notification requirements are satisfied. A standardised Eligibility consideration letter is provided/sent to the person to seek their consent for the consideration of eligibility, including a Consent for eligibility determination form.The Complex Needs Coordinator then schedules the referral consideration for a Panel meeting, providing the panel with the Request for eligibility determination to panel form. The panel may also provide advice on service responses and identify systemic issues to be addressed through service planning. In particular, the Panel ensures that Aboriginal community-controlled organisations have been engaged for Aboriginal clients.The panel considers and recommends (as relevant) the referral which requires Area Director approval. A standardised Eligibility outcome letter is then sent to the eligible client.
Care plans 11 - 18 In summary, the Act requires the:• department to ensure that a care plan is developed, based on a comprehensive assessment of the person’s
needs after a person has been determined as eligible• care plan to specify the care, treatment and support strategies recommended for the person taking into
account their best interests• care plan is initially not for longer than 12 months but thereafter may be extended with the total duration of a
care plan not exceeding 36 months.
Care plan development
13 What does development of a care plan involve?
The Act requires that the department or an appointed care plan development service provider must ensure that:• the client is consulted in person and if deemed necessary and the client agrees, their family and carers are
consulted• the persons and organisations currently providing welfare, health, mental health, disability, drug and alcohol
treatment, offender or housing and support services to the client are consulted• a comprehensive assessment of the person’s needs is carried out
• relevant health/personal information in relation to the client is obtained and considered.Following the determination of a client’s eligibility, a care plan developer is appointed by a Panel to assess the client’s needs and develop the care plan. The Panel ensures a care plan is developed as a partnership between a range of services, the client, family members and significant others.
Care plan 14 Seeking and The Act enables the department and a service provider appointed by the department for the development of
Page 94 Service Provision Framework: Complex Needs March 2020

MACNI ServiceHuman Services (Complex Needs) Act 2009 Section
Legislative requirement
development disclosing information for purposes of developing a care plan
the care plan, to seek to obtain health/personal information about the client from any person or organisation for the purposes of developing a care plan that relates to the client.The Act also indicates that the following are authorised to disclose health/personal information about the client to the department or a service provider developing a care plan, the:• department, in the case of a service provider requesting information
• Public Advocate
• Mental Health Tribunal
• any person or organisation that provides or has provided welfare, health, mental health, disability, drug and alcohol treatment, offender, emergency, or housing and support services to the client.
Copy of care plan
15 Copy of care plan and notice to be given to eligible persons
The Act requires that within 14 days after approving a care plan, the department must:• give a copy of the care plan to the person
• give a copy of the whole or any part of the care plan to service providers identified in the care plan if it is in the best interests of the client and assists service providers to give effect to the care plan.
The department must notify the person in writing:• that a care plan has been approved
• that the department, the care plan coordinator and service providers identified in the care plan may share and use health and/or personal information about the client if in the best interests of the client and would assist service providers to give effect to the care plan
• of how to contact the department representative
• that the person may at any time refuse to be the subject of the care plan
• that the person may request the department to vary or terminate the care plan.Typically, the Complex Needs Coordinator will engage with the care plan coordinator to establish the best approach for providing the care plan to the client and other engaged service providers. A standardised Care plan letter, with a copy of the care plan, is given/sent to the client. A standardised Care plan letter (services) or email is also sent to the services engaged in the care plan, including the whole or relevant part of the care plan.For some clients, a Panel approves eligibility and a proposed care plan at the same meeting and a consolidated letter (eligibility outcome and care plan) is sent/given to the client. A copy of the whole or part of the care plan is also given to service providers in the plan.
Service Provision Framework: Complex Needs March 2020 Page 95

MACNI ServiceHuman Services (Complex Needs) Act 2009 Section
Legislative requirement
Care plan coordination
16 Care plan coordinator
The Act requires the department to appoint a care coordinator for a person eligible under the Act to:• monitor the care plan implementation and progress of the client
• coordinate the services provided to the client as per the care plan
• provide a report to the department on client progress when requested.The determination of the care plan coordination service is based on the matching of the person’s needs and the service’s expertise and capacity to provide care plan coordination in a timely and effective manner. As indicated, the care plan coordination service provider is typically recommended in the care plan approved by the department.While a care plan coordinator can be nominated from any service or program, the service provider needs to demonstrate the following:• a commitment and expertise integrating clients with complex needs into existing service provision
• experience in advocating for service options that best meet clients’ needs
• an ability to nominate or recruit experienced, influential and highly capable person/s to undertake the care plan coordination role
• the capacity to provide appropriate supervision and support to the care plan coordinator
• professional values of open communication, effective networking and the capacity to provide independent and objective care team governance
• skill sets in establishing and implementing rigorous accountability frameworks, including the financial acquittal of brokerage funding.
The care plan coordinator continuously collects and analyses information to develop and implement a set of service responses and interventions. This is achieved through cross-sector collaboration and the documentation of clear actions required to achieve client outcomes. Critical to effective care plan coordination is maintaining regular contact with the care team, including well-structured care team meetings, providing support and guidance at critical points and monitoring to ensure tasks are completed within agreed timelines. The care plan coordinator works to assess and document the effectiveness of agreed service responses.
Care plan coordination
17 Service providers may share personal
The Act authorises a service provider identified in a care plan to disclose personal information or health information about the eligible person to another service provider in the care plan if the first service provider is
Page 96 Service Provision Framework: Complex Needs March 2020

MACNI ServiceHuman Services (Complex Needs) Act 2009 Section
Legislative requirement
and health information to give effect to care plan
satisfied that the disclosure of the information• is in the best interests of the person to whom the information relates
• would assist the second service provider in giving effect to the care plan.The Act authorises a service provider identified in a care plan to use personal information or health information about the person to whom the care plan relates that is obtained from another service provider identified in the care plan if the use of the information—• is in the best interests of the person to whom the information relates; and
• would assist the first-mentioned service provider in giving effect to the care plan.The Act specifies the limited purpose for which information can be exchanged as when it will assist in giving effect to the care plan. This relates to the development of a care plan and the implementation, monitoring and review of the care plan.The Act does not compel service providers to exchange information, rather it allows them to make a professional judgement based on what they believe will be in the best interests of the client.
Care plan review
16 Care plan coordinator
In summary, the Act requires the care plan coordinator to:• monitor the care plan implementation and progress of the client
• coordinate the services provided to the client as per the care plan
• provide a report to the department on client progress when requested.To achieve this, the care plan coordinator may seek health and/or personal information from the department or any provider in the care plan.
Care plan variation
18 Variation and termination of care plan
The Act allows the department to vary a care plan, including the extension of a care plan (to a maximum of 36 months).Following a review, the Panel’s recommended adjustments are made to the care plan and the plan is approved by the Area Director.
Care plan closure
18 Variation and termination of care plan
The Act allows the Secretary (or delegate) to terminate a care plan. If a care plan is terminated, the person and any service provider under the care plan must be notified by the Secretary (or delegate) in writing.The Panel recommends to the Area Director to close a care plan. The care plan is closed:
Service Provision Framework: Complex Needs March 2020 Page 97

MACNI ServiceHuman Services (Complex Needs) Act 2009 Section
Legislative requirement
• at any point in time if requested by the client
• when the care plan coordinator, care team and department, in consultation with the client, agree that the client’s needs/goals have been realised through the care plan
• when the care plan’s duration has reached the maximum duration of 36 months.A Panel may request the care plan coordinator to prepare a closure report to assist with the final review of the care plan. The report is provided to the panel at the time the care plan coordinator is recommending that MACNI cease involvement with the client, or when the maximum three-year involvement in MACNI has been reached.The report reflects on the role MACNI has played in improving the client’s outcomes and enhancing service integration and collaboration. There is an important emphasis on the progress of the client throughout the time with MACNI; the learnings gathered; the client’s perspective on what has been achieved; confirmation of continuing support arrangements (as relevant) and, any other future planning considerations.The Complex Needs Coordinator ensures a letter is provided to the client and services identified in the care plan which explains that the MACNI care plan has ended, identifying any continuing supports and a contact person for questions and the continuing supports. Further, the coordinator ensures all departmental actions are taken in relation to the closure of the care plan, including:• funding acquittal
• conclusion of funding to the care plan coordination service
• completion of data and record management requirements.A standard Care plan closure notification - letter to person, parent/guardian and a Care plan closure notification - letter to care plan coordination service is sent by the Complex Needs Coordinator.
Page 98 Service Provision Framework: Complex Needs March 2020