Embed Size (px)
Citation preview

Inter-laboratory Analysis of Isavuconazole Plasma Concentration Assays Among
European Laboratories
Federico Pea, MD,* Robert Krause, MD,† Carsten Müller, MD,‡ Benjamin Hennart, PharmD,§
Malcolm Richardson, PhD,¶ Andreas Meinitzer, PhD,† Martin H.J. Wiesen, MD,‡ Tatiana
Wiktorowicz, PhD,ǁ Jochen Spickermann, PhD,ǁ and Anne Santerre Henriksen, PhD,ǁ**
From the *Department of Medicine, University of Udine, and Institute of Clinical
Pharmacology, Santa Maria della Misericordia University Hospital, ASUIUD, Udine, Italy;
† Section of Infectious Diseases and Tropical Medicine, Department of Internal Medicine,
Medical University of Graz, Graz, Austria;
‡Center of Pharmacology, Department of Therapeutic Drug Monitoring, University
Hospital of Cologne, Cologne, Germany;
§Toxicology and Genopathy Unit, CHU Lille, Lille, France;
¶Mycology Reference Centre Manchester, ECMM Excellence Centre of Medical
Mycology, Manchester University NHS Foundation Trust, Manchester, UK;
ǁBasilea Pharmaceutica International Ltd., Basel, Switzerland
**Affiliation at the time of the study
Correspondence: Federico Pea, MD
Address: Piazzale Santa Maria della Misericordia, 3 – 3300 Udine, Italy
Telephone: +39 0432 559833
Fax: +39 0432 559819
(email: [email protected])
(Address for reprints, as above)
Supported by Basilea Pharmaceutica International Ltd.
1

Disclosures
F.P. has received personal fees from Basilea Pharmaceutica, Gilead, MSD, and Pfizer
unrelated to the current study. R.K. has received research grants from Merck and served on
the speakers’ bureau of Pfizer, Gilead, Astellas, Basilea, and Merck. C.M. has received
personal fees from Astellas unrelated to the current study. M.R. has received grants and
personal fees from Basilea related to the current study and personal fees from Gilead
Sciences, Astellas, MSD, and Pfizer unrelated to the current study. T.W. and J.S. are full-
time employees of Basilea Pharmaceutica International Ltd. A. S-H. was a full-time employee
of Basilea Pharmaceutica International Ltd at the time of the study. B.H., A.M., and M.H.J.W.
have nothing to disclose.
2

Abstract
Background: Under certain circumstances, clinicians treating patients with isavuconazole
for invasive aspergillosis or mucormycosis may use therapeutic drug monitoring. However,
the accuracy and reproducibility of the various assays used by different laboratories for the
quantification of isavuconazole plasma concentrations have yet to be determined.
Methods: Human plasma samples spiked with known concentrations of isavuconazole were
provided to European laboratories that took part in a “round-robin” test (an inter-laboratory
test performed independently at least two times; two rounds performed in the current study).
Assay methods included liquid chromatography-tandem mass spectrometry (LC-MS/MS), LC
with ultraviolet detection (LC-UV), LC with fluorescence detection (LC-FL), and bioassay.
The accuracy and reproducibility compared with the known concentrations for each sample
in each round were compared overall, between assays, and between laboratories.
Results: Twenty-seven laboratories participated in the study (LC-MS/MS, n=15; LC-UV; n=9;
LC-FL, n=1; bioassay, n=2). In Round 1, for nominal concentrations of 1000, 1700, 2500,
and 4000 ng/mL, the mean (SD) determined concentrations were 1007 (183), 1710 (323),
2528 (540), and 3898 (842) ng/mL, respectively. In Round 2, for nominal concentrations of
1200, 1800, 2400, and 4000 ng/mL, the mean (SD) determined concentrations were 1411
(303), 2111 (409), 2789 (511), and 4723 (798) ng/mL, respectively. Over both rounds,
determined concentrations were consistently within 15% of the nominal concentrations for 10
laboratories (LC-MS/MS, n=4; LC-UV, n=5; bioassay, n=1) and consistently exceeded the
upper 15% margin for 7 laboratories (LC-MS/MS and LC-UV, n=3 each; LC-FL, n=1).
Conclusions: Alignment of methodologies among laboratories may be warranted to improve
accuracy and reproducibility of therapeutic drug measurements.
Key Words: Bioassay; isavuconazole; LC-FL; LC-MS/MS; LC-UV
3

INTRODUCTION
Triazole antifungal agents are an important class of drugs for the prophylaxis and
treatment of invasive fungal infections (IFIs), which are associated with high morbidity and
mortality in immunocompromised patients.1 However, maintenance of safe and efficacious
plasma or serum concentrations of these drugs can sometimes necessitate therapeutic drug
monitoring (TDM). Factors inherent to a drug that dictate the need for TDM include a high
level of intra- and inter-individual variability of pharmacokinetics (PK), a defined therapeutic
range, and a narrow therapeutic window.2
Isavuconazole is the active moiety of the prodrug isavuconazonium sulfate, the newest
available triazole antifungal agent with demonstrated efficacy and safety for treatment of
adults with IA or mucormycosis.12-14 An early phase study demonstrated good predictability of
the dose-exposure relationship,15 and in a population-PK analysis using data from the phase
III SECURE trial in adult patients with IA and other invasive mold diseases, no relationship of
exposure with either efficacy or elevations/abnormalities in liver enzyme test results was
found.16 This suggests that, in most adults, the clinical dose of isavuconazole results in
exposures that are within the optimal therapeutic window, and so routine TDM of
isavuconazole may not be necessary. Nevertheless, the margins of the therapeutic window
remain to be defined, and it has yet to be determined if and when TDM might be required
during isavuconazole treatment.
Reliable interpretation of the results of TDM requires that the analytical assays are both
accurate and reproducible. Several laboratories have published or presented methods for the
analysis of isavuconazole concentrations using liquid chromatography with tandem mass
spectrometry detection (LC-MS/MS),17-21 ultraviolet detection (LC-UV),22-24 or fluorescence
detection (LC-FL),25 or using bioassay.26 However, it has not been defined how the results of
such analyses compare, both with respect to the different analytical methods used and to the
inter-laboratory differences using the same techniques. Therefore, we conducted a round-
robin exercise (inter-laboratory test performed independently at least two times) at European
4

laboratories to assess the accuracy and reproducibility of measurements of isavuconazole
concentration measurements.
5

MATERIALS AND METHODS
This study commenced September 2016 and completed July 2017.
Preparation of Samples
All samples were prepared by Basilea Pharmaceutica. A 5 mg/mL stock solution was
prepared by dissolving 7.102 mg of isavuconazole in 1.284 mL of dimethyl sulfoxide
(DMSO). The stock solution was then diluted to prepare spiking solutions of 100,000,
170,000, 250,000, 400,000 ng/mL (Round 1) or 120,000, 180,000, 240,000, 400,000 ng/mL
(Round 2) in a 1/1 solution of DMSO/acetonitrile + 0.05% trifluoroacetic acid
(DMSO/ACN/TFA). Samples for the round robin were prepared by addition of 5 μL of the
spiking solutions to 495 μL samples of human plasma containing K3-EDTA as anticoagulant.
Final concentrations of samples used were based on the clinical relevant range of plasma
concentrations for isavuconazole. Concentrations in Round 1 were as follows: Sample 1,
1000 ng/mL; Sample 2, 1700 ng/mL; Sample 3, 2500 ng/mL; and Sample 4, 4000 ng/mL.
Concentrations in Round 2 were as follows: Sample 1, 1200 ng/mL; Sample 2, 1800 ng/mL;
Sample 3, 2400 ng/mL; and Sample 4, 4000 ng/mL. For each round, all plasma samples of a
given concentration were mixed together and re-aliquoted prior to distribution, such that each
laboratory effectively received the same sample.
Laboratories and Testing
European laboratories with the facilities for and expertise in drug-concentration assays
using LC-MS/MS, LC-UV, LC-FL, or bioassays based on diffusion of the drug into inoculated
and incubated media, were identified and invited to participate in the study. All laboratories
included in the study were required to have developed and validated the assays used in this
study prior to inclusion. Participating laboratories, listed in Supplementary Table S1, were
provided with samples in the first and/or second round of the test. Details of some of the
analytical methods used have been published previously17-19,22,24,25; others were adapted from
methods established for detection of other triazole antifungal agents,27-29 or used/adapted a
commercially available assay.30 All samples for each round were also tested by the Basilea
6

Pharmaceutica bioanalytical laboratory using LC-MS/MS. Details of methods used by Basilea
Pharmaceutica and as provided by each laboratory are provided in the Supplementary
Methods. Results from Basilea Pharmaceutica were included in statistical analyses but were
not considered when comparing different methods or laboratories.
Statistics
To determine the accuracy and precision of measurements made in each round, the
mean, standard deviation, and bias (percent deviation from nominal concentration) were
calculated for all samples and for each assay method. The results were assessed with
respect to the European Medicines Agency (EMA)31 and the US Food and Drug
Administration (FDA)32 guideline requirements of accuracy (bias) and precision (relative
standard deviation) within a 15% limit.
7

RESULTS
In total, 34 laboratories in Germany, UK, Netherlands, Italy, France, Austria,
Switzerland, and Denmark were invited to participate in the round-robin test. Of these, 27
laboratories provided results for the determination of isavuconazole concentrations in human
plasma (Supplementary Table S1; Round 1, Laboratories 1–10; Round 2, Laboratories 11–
27). The methods used for the determination were LC-MS/MS (Round 1: Laboratories 1–5;
Round 2: Laboratories 11–20), LC-UV (Round 1: Laboratories 6–8; Round 2: Laboratories
21–26), bioassays (Round 1: Laboratories 9, 10; Round 2, Laboratory 10), and LC-FL
(Round 2: Laboratory 27).
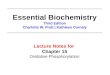
In Round 1, the mean of determined values for the assessments from all laboratories
for each of the samples with nominal concentrations of 1000, 1700, 2500, and 4000 ng/mL
were within the 15% margins, although the standard deviations extended beyond those
margins (Fig. 1). The overall biases at each of these concentrations were 0.7%, 0.6%, 1.1%,
and –2.5%, respectively. Among all 40 samples assessed by the 10 laboratories, 29
determined concentrations were within 15% of the nominal concentrations (acceptance
criterion), 7 were above the upper 15% margin, and 4 were below the lower 15% margin.
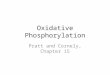
The results were also assessed as a function of the analytic method. For LC-MS/MS
(Laboratories 1–5), the mean of determined values for each nominal concentration was again
within the 15% margins, although the standard deviations exceeded the upper margin at all
tested concentrations (Fig. 2). Determined values from 2 laboratories were consistently
within the 15% margins and those from 1 laboratory consistently exceeded the upper 15%
margin. The overall biases at each of the tested concentrations (1000‒4000 ng/mL) were
4.3%, 7.8%, 9.5%, and 6.9%, respectively. In total, 13/20 determined concentrations were
within the 15% margins. The remaining 7/20 concentrations exceeded the upper 15%
margin, including 1 sample for Laboratory 2, 2 samples for Laboratory 4, and all samples for
Laboratory 5. Determined values from the 3 laboratories that used LC-UV were consistently
within 15% of the nominal concentrations (Fig. 2). The overall biases at each of the tested
concentrations were 7.3%, 3.9%, 7.5%, and 0.2%, respectively. Of the 2 laboratories that
8

used bioassays, all values determined from Laboratory 9 were within 15% of the nominal
concentrations, whereas those from Laboratory 10 were all well below the lower 15% margin
for all samples (overall bias at each concentration, –20%, –26.2%, –33.6%, and –34.5%,
respectively) (Fig. 2).
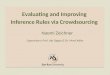
In Round 2, the mean of determined values for the assessments from all laboratories
slightly exceeded the upper 15% margin for each of the samples with nominal concentrations
of 1200, 1800, 2400, and 4000 ng/mL (Fig. 3). The overall biases at each of these
concentrations were considerably larger than those observed in Round 1 (17.6%, 17.3%,
16.2%, and 18.1%, respectively). Among all 72 determined concentrations from the 18
laboratories, 31 were within the 15% margins, 36 exceeded the upper 15% margin, and 5
were below the lower 15% margin.
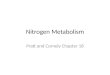
When assessed as a function of the analytic methods, the means of determined values
for those using LC-MS/MS (Laboratories 11–20) were slightly below the upper 15% margin
(Fig. 4). Determined values from 2 laboratories were consistently within the 15% margins and
those from 2 other laboratories consistently exceeded the upper 15% margin. The overall
bias at each nominal concentration was again higher than observed for LC-MS/MS in Round
1 (14.4%, 13.9%, 11.6%, and 12.1%, respectively). In total, 19/40 determined concentrations
were within the 15% margins, 18/40 exceeded the upper 15% margin, and 3/40 were below
the bottom 15% margin. Among laboratories that used LC-UV (Laboratories 21–26), the
means of determined values for all nominal concentrations exceeded the upper 15% margin
(Fig. 4). Two laboratories consistently provided determined values that were within the 15%
of the nominal concentrations and 3 laboratories provided values that all exceeded the upper
15% margin. The overall bias at each nominal concentration was 25.6%, 24.3%, 28.6%, and
30.8%, respectively. Among the 24 total samples, 10 of the determined concentrations were
within the 15% margins and 14 exceeded the upper 15% margin. For LC-FL (Laboratory 27),
determined values for all samples exceeded the upper 15% margin (Fig. 4). For bioassay,
Laboratory 10 was included again after having made technical adjustments. Although
determined values for the 1200 ng/mL and 2400 ng/mL nominal concentrations were each
9

slightly below the lower 15% margin, determined values were with the 15% margins for the
1800 ng/mL and 4000 ng/L nominal concentrations (Fig. 4).
10

DISCUSSION
In any instance for which isavuconazole TDM might be considered appropriate, its
usefulness will require accurate measurement with regard to the analytic method used. In
this round-robin exercise of European laboratories, 10 of the 27 laboratories included in both
rounds provided determined plasma concentrations that were consistently within ±15% of the
nominal concentrations. Of all total samples in both rounds, 54% (60/112) determined
concentrations were within ±15% of the nominal concentrations. These data suggest that
there is likely need for refinement and alignment of each of those analytical methods across
the different laboratories.
It may be a concern that determined concentrations were consistently within the 15%
margins stipulated in guidelines from the EMA31 and FDA32 for fewer than half of the
laboratories. Moreover, determined concentrations outside of those margins were far more
likely to be overestimated (43/112) than underestimated (9/112). Overestimation in clinical
practice might result in a decision to reduce the dose and thereby pose a risk for less
efficacious treatment. From a methodological perspective, this suggests that a common
systematic error across a subset of the laboratories is possible. Data regarding the assay
calibrations performed were not available for all laboratories. As isavuconazole is a relatively
new drug, it may be that some have not yet implemented the adjustments necessary to
obtain the desired accuracy. For example, it is unclear whether all laboratories using LC
controlled for possible matrix effects during elution.33 Controls for matrix effects were
reported by 4 of the laboratories in the current study, and among those laboratories,
determined concentrations were consistently within the 15% margin for 3 (LC-MS/MS:
Laboratories 1,17 3,19 and 1818) but consistently exceeded the upper 15% margin for 1 (LC-FL:
Laboratory 2725). Another potentially important source of systemic error is failure to account
for the content of isavuconazole in locally-prepared, concentrated stock solutions for
preparation of calibration/quality control samples. Therefore, it seems likely that there is a
need for standardization of methods, including extraction and dilution of samples, use of
appropriate internal standards, working/stock solutions, and use of solvents. The use of an
11

internal standard would help to enhance the accuracy of the different assays used in this
study to varying degrees. The use of a stable labeled internal standard is best practice for
LC-MS/MS. For a LC-UV approach, an internal standard would need to be
chromatographically separated from all UV peaks of interest. However, for a bioassay
method, an internal standard would not be necessary for concentration determination.
It is noteworthy that the largest overestimations were observed with LC-UV in Round 2
and appeared to be pronounced at higher nominal concentrations. This may involve a
systematic error in purification steps (i.e., steps also used for LC-MS/MS), but that alone may
not account for the greater magnitude of bias. One potential explanation is that uncontrolled
ionization effects, which might have affected LC-MS/MS measurements by some
laboratories, might have an even greater effect on UV absorption. That might also explain the
overestimations observed using LC-FL, although no firm conclusions could be drawn
regarding the overall accuracy and reproducibility of this analytic approach based on results
from 1 laboratory.
As only 2 laboratories in the round-robin test used bioassay, it was also not possible to
draw any firm conclusions from those results. In Round 1, the determined concentrations of
all samples from one of the laboratories were all within the 15% margin; however, the second
laboratory provided values that were underestimated for all samples. In Round 2, after
consultation with the first laboratory and alignment of methodology, the second laboratory
provided results that were all much closer to the nominal concentrations. Nevertheless, 2 of 4
values were still below the lower 15% margin and so it may be that this approach is prone to
inter-user variability.
Although the second laboratory that used bioassay was provided an opportunity to
review and adjust their methodology, other laboratories in this study were not, and so that
might be considered a limitation of this study. In fact, multiple assessments by each
laboratory for each concentration might possibly have resulted in greater consistency.
However, this study was designed to more closely follow normal practice in a clinical setting,
during which replicates are not usually performed. It is also important to note that, although
12

at least one laboratory in this study had possible effects of commonly co-administered
drugs,17 it is not known whether all of the other laboratories had done the same.
CONCLUSION
Taken together, the results of this study suggest that improving the accuracy and
reproducibility of each method is very likely to require standardization of the methodologies
across analytical laboratories. This process would require more open discussion regarding
protocols and might be facilitated by implementing international standards. Ultimately, it
would increase the confidence of clinicians in the event that isavuconazole TDM appears
necessary.
ACKNOWLEDGMENTS
Isavuconazole has been co-developed by Astellas Pharma Global Development Inc.
and Basilea Pharmaceutica International Ltd. The study was funded by Basilea
Pharmaceutica International Ltd, Basel, Switzerland. The authors thank all personnel at the
participating analytical laboratories (see Supplementary Materials). Medical writing support
was provided by Ed Parr, PhD, CMPP, of Envision Scientific Solutions and funded by Basilea
Pharmaceutica International Ltd.
13

REFERENCES
1. Lass-Florl C. Triazole antifungal agents in invasive fungal infections: a comparative
review. Drugs 2011;71:2405-2419.
2. Lewis R, Brüggemann R, Padoin C, et al. Triazole antifungal therapeutic drug
monitoring. Presented at the Sixth European Conference on Infections in Leukaemia;
Sophia Antipolis, France. 2015
3. Luong ML, Al-Dabbagh M, Groll AH, et al. Utility of voriconazole therapeutic drug
monitoring: a meta-analysis. J Antimicrob Chemother 2016;71:1786-1799.
4. Brüggemann RJ, Donnelly JP, Aarnoutse RE, et al. Therapeutic drug monitoring of
voriconazole. Ther Drug Monit 2008;30:403-411.
5. Dolton MJ, McLachlan AJ. Voriconazole pharmacokinetics and exposure-response
relationships: assessing the links between exposure, efficacy and toxicity. Int J
Antimicrob Agents 2014;44:183-193.
6. Walsh TJ, Raad I, Patterson TF, et al. Treatment of invasive aspergillosis with
posaconazole in patients who are refractory to or intolerant of conventional therapy:
an externally controlled trial. Clin Infect Dis 2007;44:2-12.
7. Ashbee HR, Barnes RA, Johnson EM, et al. Therapeutic drug monitoring (TDM) of
antifungal agents: guidelines from the British Society for Medical Mycology. J
Antimicrob Chemother 2014;69:1162-1176.
8. Chau MM, Kong DC, van Hal SJ, et al. Consensus guidelines for optimising antifungal
drug delivery and monitoring to avoid toxicity and improve outcomes in patients with
haematological malignancy, 2014. Intern Med J 2014;44:1364-1388.
9. Hamada Y, Tokimatsu I, Mikamo H, et al. Practice guidelines for therapeutic drug
monitoring of voriconazole: a consensus review of the Japanese Society of
Chemotherapy and the Japanese Society of Therapeutic Drug Monitoring. J Infect
Chemother 2013;19:381-392.
10. Mousset S, Buchheidt D, Heinz W, et al. Treatment of invasive fungal infections in
cancer patients-updated recommendations of the Infectious Diseases Working Party
14

(AGIHO) of the German Society of Hematology and Oncology (DGHO). Ann Hematol
2014;93:13-32.
11. Tissot F, Agrawal S, Pagano L, et al. ECIL-6 guidelines for the treatment of invasive
candidiasis, aspergillosis and mucormycosis in leukemia and hematopoietic stem cell
transplant patients. Haematologica 2017;102:433-444.
12. Natesan SK, Chandrasekar PH. Isavuconazole for the treatment of invasive
aspergillosis and mucormycosis: current evidence, safety, efficacy, and clinical
recommendations. Infect Drug Resist 2016;9:291-300.
13. Maertens JA, Raad, II, Marr KA, et al. Isavuconazole versus voriconazole for primary
treatment of invasive mould disease caused by Aspergillus and other filamentous
fungi (SECURE): a phase 3, randomised-controlled, non-inferiority trial. Lancet
2016;387:760-769.
14. Marty FM, Ostrosky-Zeichner L, Cornely OA, et al. Isavuconazole treatment for
mucormycosis: a single-arm open-label trial and case-control analysis. Lancet Infect
Dis 2016;16:828-837.
15. Schmitt-Hoffmann A, Roos B, Maares J, et al. Multiple-dose pharmacokinetics and
safety of the new antifungal triazole BAL4815 after intravenous infusion and oral
administration of its prodrug, BAL8557, in healthy volunteers. Antimicrob Agents
Chemother 2006;50:286-293.
16. Desai AV, Kovanda LL, Hope WW, et al. Exposure-response relationships for
isavuconazole in patients with invasive aspergillosis and other filamentous fungi.
Antimicrob Agents Chemother 2017;61.
17. Fatiguso G, Favata F, Zedda I, et al. A simple high performance liquid
chromatography-mass spectrometry method for therapeutic drug monitoring of
isavuconazole and four other antifungal drugs in human plasma samples. J Pharm
Biomed Anal 2017;145:718-724.
18. Müller C, Gehlen D, Blaich C, et al. Reliable and easy-to-use liquid chromatography-
tandem mass spectrometry method for simultaneous snalysis of fluconazole,
15

isavuconazole, itraconazole, hydroxy-itraconazole, posaconazole, and voriconazole
in human plasma and serum. Ther Drug Monit 2017;39:505-513.
19. Toussaint B, Lanternier F, Woloch C, et al. An ultra performance liquid
chromatography-tandem mass spectrometry method for the therapeutic drug
monitoring of isavuconazole and seven other antifungal compounds in plasma
samples. J Chromatogr B Analyt Technol Biomed Life Sci 2017;1046:26-33.
20. Kovanda LL, Petraitiene R, Petraitis V, et al. Pharmacodynamics of isavuconazole in
experimental invasive pulmonary aspergillosis: implications for clinical breakpoints. J
Antimicrob Chemother 2016;71:1885-1891.
21. Farowski F, Cornely OA, Vehreschild JJ, et al. Quantitation of azoles and
echinocandins in compartments of peripheral blood by liquid chromatography-tandem
mass spectrometry. Antimicrob Agents Chemother 2010;54:1815-1819.
22. Wissen CP, Burger DM, Verweij PE, et al. Simultaneous determination of the azoles
voriconazole, posaconazole, isavuconazole, itraconazole and its metabolite hydroxy-
itraconazole in human plasma by reversed phase ultra-performance liquid
chromatography with ultraviolet detection. J Chromatogr B Analyt Technol Biomed
Life Sci 2012;887-888:79-84.
23. Cozzi V, Baldelli S, Castoldi S, et al. Development and validation of a
chromatographic ultraviolet method for the quantification of isavuconazole in human
plasma samples. Ther Drug Monit 2018;40:512-514.
24. Nannetti G, Pagni S, Palu G, et al. A sensitive and validated HPLC-UV method for the
quantitative determination of the new antifungal drug isavuconazole in human
plasma. Biomed Chromatogr 2018:e4333.
25. Jørgensen R, Andersen SR, Astvad KMT, et al. Implementation of isavuconazole in a
fluorescence-based high-performance liquid chromatography kit allowing
simultaneous detection of all four currently licensed mold-active triazoles. mSphere
2017;2.
16

26. Rautemaa-Richardson R, Moore C, Richardson M. Isavuconazole levels in non-
immunocompromised patients treated for chronic pulmonary aspergillosis. Presented
at the 27th European Congress of Clinical Microbiology and Infectious Diseases;
Vienna, Austria. 2017
27. Gordien JB, Pigneux A, Vigouroux S, et al. Simultaneous determination of five
systemic azoles in plasma by high-performance liquid chromatography with ultraviolet
detection. J Pharm Biomed Anal 2009;50:932-938.
28. Jourdil JF, Tonini J, Stanke-Labesque F. Simultaneous quantitation of azole
antifungals, antibiotics, imatinib, and raltegravir in human plasma by two-dimensional
high-performance liquid chromatography-tandem mass spectrometry. J Chromatogr B
Analyt Technol Biomed Life Sci 2013;919-920:1-9.
29. Franceschi L, D’Aronco S, Furlanut M. Development and validation of a liquid
chromatography - tandem mass spectrometry method for the determination of
voriconazole and posaconazole in serum samples from patients with invasive
mycoses. J Bioanal Biomed 2011;3:92-97.
30. Chromsystems Instruments and Chemicals GmbH. TDM of Isavuconazole using
MassTox® TDM Series A Kit. Available at: https://www.chromsystems.com/tdm-of-
isavuconazole. Accessed August 10, 2018.
31. European Medicines Agency. Guideline on bioanalytical method validation. Available
at: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/
2011/08/WC500109686.pdf. Accessed November 2, 2017.
32. US Food and Drug Administration. Guidance for Industry: Bioanalytical method
validation. Available at:
https://www.fda.gov/downloads/Drugs/Guidance/ucm070107.pdf. Accessed
November 2, 2017.
33. Gosetti F, Mazzucco E, Zampieri D, et al. Signal suppression/enhancement in high-
performance liquid chromatography tandem mass spectrometry. J Chromatogr A
2010;1217:3929-3937.
17

18

Figure legends
FIGURE 1. Isavuconazole plasma concentrations determined by Basilea and all laboratories
in Round 1 (Labs 1–10) as a function of the nominal concentrations of 1000, 1700, 2500, and
4000 ng/mL (A, B, C, and D, respectively). Solid lines represent nominal concentrations,
dashed lines represent ±15% margins from nominal concentrations.
FIGURE 2. Isavuconazole plasma concentrations in Round 1 determined using liquid
chromatography-tandem mass spectrometry (LC-MS/MS; Labs 1–5), LC with ultraviolet
detection (LC-UV; Labs 6–8), or Bioassay (Labs 9, 10) as a function of the nominal
concentration of 1000, 1700, 2500, and 4000 ng/mL (A, B, C, and D, respectively). Solid
lines represent nominal concentrations, dashed lines represent ±15% margins from nominal
concentrations.
FIGURE 3. Isavuconazole plasma concentrations determined by Basilea and all laboratories
in Round 2 (Labs 10–27) as a function of the nominal concentrations of 1200, 1800, 2400,
and 4000 ng/mL (A, B, C, and D, respectively). Solid lines represent nominal concentrations,
dashed lines represent ±15% margins from nominal concentrations.
FIGURE 4. Isavuconazole plasma concentrations in Round 2 determined using liquid
chromatography-tandem mass spectrometry (LC-MS/MS; Labs 11–20), LC with ultraviolet
detection (LC-UV; Labs 21–26), LC with fluorescence detection (LC-FL; Lab 27), or Bioassay
(BA; Lab 10) as a function of the nominal concentration of 1200, 1800, 2400, and 4000
ng/mL (A, B, C, and D, respectively). Solid lines represent nominal concentrations, dashed
lines represent ±15% margins from nominal concentrations.
19

FIGURE 1. Isavuconazole plasma concentrations determined by Basilea and all laboratories
in Round 1 (Labs 1–10) as a function of the nominal concentrations of 1000, 1700, 2500, and
4000 ng/mL (A, B, C, and D, respectively). Solid lines represent nominal concentrations,
dashed lines represent ±15% margins from nominal concentrations.
20

FIGURE 2. Isavuconazole plasma concentrations in Round 1 determined using liquid
chromatography-tandem mass spectrometry (LC-MS/MS; Labs 1–5), LC with ultraviolet
detection (LC-UV; Labs 6–8), or Bioassay (Labs 9, 10) as a function of the nominal
concentration of 1000, 1700, 2500, and 4000 ng/mL (A, B, C, and D, respectively). Solid
lines represent nominal concentrations, dashed lines represent ±15% margins from nominal
concentrations.
21

FIGURE 3. Isavuconazole plasma concentrations determined by Basilea and all laboratories
in Round 2 (Labs 10–27) as a function of the nominal concentrations of 1200, 1800, 2400,
and 4000 ng/mL (A, B, C, and D, respectively). Solid lines represent nominal concentrations,
dashed lines represent ±15% margins from nominal concentrations.
22

FIGURE 4. Isavuconazole plasma concentrations in Round 2 determined using liquid
chromatography-tandem mass spectrometry (LC-MS/MS; Labs 11–20), LC with ultraviolet
detection (LC-UV; Labs 21–26), LC with fluorescence detection (LC-FL; Lab 27), or Bioassay
(BA; Lab 10) as a function of the nominal concentration of 1200, 1800, 2400, and 4000
ng/mL (A, B, C, and D, respectively). Solid lines represent nominal concentrations, dashed
lines represent ±15% margins from nominal concentrations.
23

Supplementary materials
TABLE S1. Laboratories Participating in the Round-Robin Test
Laboratory Country Method Round
1 Italy LC-MS/MS 1
2 Italy LC-MS/MS 1
3 France LC-MS/MS 1
4 France LC-MS/MS 1
5 France LC-MS/MS 1
6 Netherlands LC-MS/MS 1
7 Italy LC-UV 1
8 France LC-UV 1
9 United Kingdom Bioassay 1
10 Germany Bioassay 1 and 2
11 Italy LC-MS/MS 2
12 Italy LC-MS/MS 2
13 France LC-MS/MS 2
14 France LC-MS/MS 2
15 France LC-MS/MS 2
16 France LC-MS/MS 2
17 France LC-MS/MS 2
18 Germany LC-MS/MS 2
19 Germany LC-MS/MS 2
20 Austria LC-MS/MS 2
21 Italy LC-UV 2
22 Italy LC-UV 2
23 Italy LC-UV 2
24 France LC-UV 2
25 France LC-UV 2
26 United Kingdom LC-UV 2
27 Denmark LC-FL 2
LC-FL, liquid chromatography with fluorescence detection; LC-MS/MS, liquid
chromatography with tandem mass spectrometry; LC-UV, liquid chromatography with
ultraviolet detection
24

Supplementary Methods
Details of methods as provided by participating laboratories
Details of methods have been published previously for Laboratories 1,17 3,19 6,22 18,18 22,24
and 27.25
Liquid chromatography – tandem mass spectrometry (LC-MS/MS )
Basilea: Spiking solutions were prepared by serial dilution in DMSO and acetonitrile (ACN),
0.05% trifluoracetic acid (TFA) out of a 2 mg/mL stock solution with a range of 0.01–10
µg/mL. Calibration samples were performed by spiking 1 µL of each DMSO/ACN (0.05%
TFA) solution in 99 µL of blank K3-EDTA plasma. Each sample was then quenched with 300
µL of ACN, 0.05% TFA containing 1 µg/mL isavuconazole-d4 as internal standard. After
centrifugation, 10 µL of the supernatant was injected into the LC-MS/MS device. The same
preparation method was performed for the quality control samples. 50 µL of the study
samples were mixed with 150 µL of ACN, 0.05% TFA containing 1 µg/mL isavuconazole-d4
as internal standard and then treated like the calibrators and quality control samples. The
LOQ was 0.01 µg/mL and the linear range of the assay was 0.01–10 µg/mL. The coefficient
of variation ranged from 1.3% to 5.9% in the first round and 1.8% to 2.5% in the second
round of the round-robin test.
Laboratory 2: Working solutions of isavuconazole and IS were prepared by diluting each
analyte in DMSO. Calibrators and quality controls (QCs) were made by spiking analytes from
different batches of working solution into a pool of plasma. An 8-point calibration curve was
prepared by adding isavuconazole to yield concentrations that ranged from 0.08 to 10 mg/L
and included the lower limit of quantification (LLOQ). QC samples were prepared by adding
isavuconazole at the following 4 concentration levels (LLOQ, QClow, QCmedium and QChigh) to a
pool of plasma: 0.08, 0.31, 1.25, 5 ng/mL. A 50 µL aliquot of plasma was spiked with 10 µL of
10 µg/mL IS. Proteins were precipitated by adding 25 µL of extraction buffer and 250 µL of
precipitation reagent, vortexed and centrifuged for 10 minutes at 14,000 rpm. Supernatant
was then diluted 1:10 with methanol and transferred in an autosampler vial. LC-MS/MS
25

analysis was performed on a TSQ Quantum Access Max™ Triple Quadrupole coupled to an
Accela 1250 UHPLC system (ThermoFisher Scientific, Milan, Italy). Gradient separation
chromatography was carried out using a Accucore Polar premium analytical column 50 mm x
2,1 i.d. x 2.6 µm particle size (ThermoFisher Scientific, Milan, Italy) with mobile phase 1 and
2. The percentage of mobile phase 2 started at 20%, then programmed to reach 100% in 1.5
minutes and kept for 1 minute at flow rate of 600 µL/min, then the column was reconditioned
at 20% B for 2.5 minutes for a total run time of 5 minutes. The column temperature was
maintained at 40°C and injection volume was 2 µL. Ionization was achieved using HESI in
the positive ion mode with 3500 V. Nitrogen was used as the nebulizer and auxiliary gas, set
at 60 and 20 arbitrary units, respectively. Vaporizer and ion transfer tube temperature
settings were 350°C and 400°C. For collision-induced dissociation, high purity argon was
used at a pressure of 1.5 mTorr. Analytes were detected using selective reaction monitoring
(SRM) of the specific transitions for isavuconazole 438.2->127; 215; 224; 369 and its IS
442.2-> 127; 219; 224; 373 m/z.
Laboratory 4: Briefly, protein precipitation was achieved with the addition of 100 μL of
precipitation reagent [methanol/0.2 M zinc sulfate (80/20, v/v)] including 1 mg/L deuterated
isavuconazole (internal standard) in a 1.5 mL conical plastic Eppendorf test tube. Samples
were immediately vortexed and then centrifuged at 13,000 × g for 15 minutes at +4 °C. Then,
100 μL of supernatant was transferred into a sample vial and 10 μL was injected into the
chromatographic system. The chromatographic system consisted of Agilent (Palo Alto, CA,
USA) 1200 Series components including a binary pump, isocratic pump, column oven, 2 ten-
port switching valves and an autosampler. The hardware configuration included an Applied
Biosystems (Foster City, CA, USA) API 3200 equipped with a TurboIonSpray source. On-line
extraction was performed using a perfusion column (POROS R1/20, 2.1 mm × 30 mm,
Applied Biosystems, Foster City, CA, USA). The HPLC column was a short phenyl-hexyl
column (Phenomenex Luna 5 μm Phenyl-Hexyl, 2 mm × 50 mm, Aschaffenburg, Germany).
Data analysis was performed using the Analyst 1.4.2 software package (Applied Biosystems,
Foster City, CA, USA).
26

Laboratory 5: An LC-MS/MS method was developed and validated according to the
guidelines on bioanalytical method validation from the European Medicines Agency (2012)
for 6 azole analytes: fluconazole, voriconazole, posaconazole, isavuconazole, itraconazole,
and its active metabolite hydroxyl-itraconazole.
Laboratory 11: The LC-MS/MS method was adapted from a previously published approach
for detection of triazole antifungal agents.29
Laboratory 12: The LC-MS/MS method was based on a commercially-available approach
from Chromsystems.30 Sample preparation and subsequent analysis in LC-MS/MS were
performed using Chromsystems' parameter set Antimycotic drugs on Waters TQD
instrument. The Internal Standard Mix (800 μL) was added to 12 mL Precipitation Reagent to
form mixture A. A 50 μL sample/calibrator/MassCheck® control was pipetted into a 1.5 mL
reaction vial, to which 25 μL Extraction Buffer was added, mixed, and incubated for 2
minutes at ambient temperature (without centrifuging). 250 μL of mixture A was added and
mixed (vortex) for 30 seconds minimum before centrifuging 5 minutes at 15,000 x g. The
supernatant was diluted with Dilution Buffer prior to injection depending on the instrument
sensitivity. 0.2–50 μL was injected into the LC-MS/MS device (electrospray ionization;
multiple reaction monitoring mode; gradients, 0.00–0.50 min 30% mobile phase 2, 0.51–2.80
min 100% mobile phase 2, 2.81–3.20 min 30% mobile phase 2). The limit of quantification
ranged from 0.01 to 2.00 mg/L (linearity up to 250 mg/L; recovery of 95–111%; intra-assay
coefficient of variation [CV], 1.7–4.9%; inter-assay CV, 3.6–5.3%).
Laboratory 13: The LC-MS/MS method was based on a commercially-available approach
from Chromsystems.30
Laboratory 14: The LC-MS/MS method was adapted from a commercially-available
approach from Chromsystems.30 For the working solution of the internal standard, its
concentration was fixed at a concentration of 10 mg/L and 35 µL of the internal standard
working solution was added to a volume of 50 µL of sample. Sample preparation was
27

performed according to the protocol provided by Chromsystems and using extraction buffer
and precipitation reagent commercialized by Chromsystems.
Laboratory 15: The LC-MS/MS method was adapted from a previously published approach
to analysis of other triazole antifungal agents.28
Laboratory 16: LC-MS/MS was performed with deuterated internal standard extraction by
precipitation home-made standard curve.
Laboratory 17: The method was LC-MS/MS (HPLC- Quattro™ micro API detector, Waters,
MA, USA) with ESI positive mode. Samples were extracted with SPE MCX µElution
cartridge. The linearity was 0.2–8 µg/mL.
Laboratory 19: Extraction was from 200 µL serum/plasma, diluted with 200 µL 0.1 M
phosphate buffer pH 9.5, extracted with 1 mL chlorbutane/ether (1:1). Measurement was
performed with Agilent LC-TOF MS, internal standard Diazepam-d5. Calibration 2.5–25
mg/L.
Laboratory 20: Isavuconazole was measured with electrospray ionization tandem mass
spectrometry on a Voyager TSQ Quantum triple quadrupole instrument equipped with an
UltiMate 3000 chromatography system (Thermo Instruments, San Jose, CA, USA).
Chromeleon Xpress software for device management and LCQuanTM 2.7 for data
processing were used. Isavuconazole and its deuterated isotope were kindly provided by
Basilea (Basel, Switzerland). Calibrators and controls were prepared by spiking drug free
plasma from healthy donors with stock solutions. In brief, 20 µL serum samples (calibrators
or controls) were deproteinized by addition of ice cold 100 µL of methanol containing the
internal standard (isavuconazole-d4, 1000 ng/mL). After vortexing and centrifugation at
24,000 g (5 min), the clear supernatant was 10-fold diluted with 5% ACN. 10 µL were loaded
on a trapping column (POROS™ R1 20, 2.1 x 30 mm, Thermo Fisher) with mobile phase 1
(5:95 v/v ACN/water). After a short washing period the analytes were transferred and
separated on a Luna 5 μm Phenyl-Hexyl column 100A 50 x 2.1 mm (Phenomenex™
Aschaffenburg, Germany) with a linear gradient of mobile phase 2 (0.1% formic acid in MS
28

grade water) and mobile phase 3 (0.1% formic acid in MS grade ACN). Isavuconazole and
internal standard were monitored in positive multiple reaction monitoring mode using
characteristic precursor–product ion transitions: m/z 438.1→214.9 and m/z 442.1→218.9,
respectively. Within-day CVs were 2.9% (2900 ng/mL) and 1.5% (6600 ng/mL), and
between-day CVs were 3.1% (2900 ng/mL) and 1.8 % (6600 ng/mL). On the lower limit of
quantification (100 ng/mL) the coefficient of variation (CV) was <10%.
Liquid chromatography – ultraviolet detection (LC-UV)
Laboratory 7: Samples were prepared containing 0.25 mL plasma, 0.05 mL IS (6,7-
dimethylquinoxaline, 1 mg/L), 0.4 mL ACN, vortexed, then after 10 minutes they were
centrifuged at 17,000 rpm for 10 minutes and the supernatant transferred for drying under
nitrogen flow. Samples were reconstituted with mobile phase (0.2 mL; A: 50% monobasic
ammonium phosphate [NH4H2PO4] 0.04 M, pH=6; B: 50% ACN [CH3CN]) and 0.05 mL was
injected. UV detection was performed at 270 nm (linearity: 100–8000 ng/mL [calibration
curve with 7 not-zero points] plus 3 QC [320, 3200, 6000 ng/mL]).
Laboratory 8: This approach used LC with diode array detection. Plasma (200 µL), or
control, or calibrant, was mixed and centrifuged (10,000 g, 4°C, 10 minutes) after addition of
400 µL ACN for protein precipitation and containing 1.35 mg/L methyl-clonazepam (Sigma
Aldrich) as an internal standard. Supernatant (400 µL) was dried under nitrogen stream and
150 µL of a mix of ACN and phosphate buffer (pH 3.6) was added. Seventy microliters was
injected onto an UPLC-UV system (Acquity, Waters, Milford, MA) equipped with a
SYMMETRY 18 column (5 µM, 4.6 mm x 250 mm) at 30°C. Isavuconazole was detected at
284 nm and IS at 310 nm.
Laboratory 21: Briefly, 0.8 mL of ACN was added to 0.5 mL plasma samples. After protein
precipitation, the supernatant was dried; the residue was reconstituted in mobile phase and
injected into the HPLC device. Chromatographic separation was performed with a
SymmetryShield RP8 (3.9 mm × 150 mm, particle size 3.5 µm; Waters, Milan, Italy) column
29

under gradient conditions. The total chromatographic run time was 10 minutes per samples.
The method was linear in the range of 0.15–10 mg/L isavuconazole concentrations. The
lowest limit of quantification was set at 0.15 mg/L.
Laboratory 23: In a sensitive, selective high-performance liquid chromatographic (HPLC)
method with UV detection developed and validated for the determination of isavuconazole,
an aliquot (0.5 mL) of plasma or standard was pipetted into a 5 mL polypropylene tube
(Sarstedt, Leicester, UK) and ACN, 1.0 mL, added. The mixture was vortexed and the
mixture was centrifuged at 1200×g for 10 minutes. The organic layer was evaporated to
dryness and the residue was reconstituted with 500 μL of mobile phase and 180 μL injected
in the chromatographic system. The compounds were separated on a C18 5μm 150 × 4.6
mm (Restek) column using sodium potassium phosphate buffer (0.04 M): ACN ultrapure
(50/50 v/v) as mobile phase. The compounds were detected at a wavelength of 270 nm. The
assay was linear and validated over the range 0.25–8.0 mg/L. The mean recovery was 98%.
Assay reproducibility was: intraday <6%; interday <10%.
Laboratory 24: The LC-UV method was adapted from a previously published approach to
analysis of other triazole antifungal agents.27
Laboratory 25: The protocol used a liquid chromatographic method coupled with a photo
array diode for the detection. The calibration was made by standard from 0.25 to 10 mg/L.
We had 3 internal controls (1.5, 3.5 and 7.5 mg/L). The first step of the method consisted of
an extraction. 200 µL of sample added to 70 µL of Internal Standard (ketoconazole at 1
mg/L), 250 µL of ammonium acetate at 200 mM (pH9). After 10 seconds of mixing, 3.5 mL of
ethyl acetate/diethyl ether (50/50) was added, vortexed for 5 minutes, and the supernatant
was transferred and evaporated under nitrogen flux at 45°C. The dry extract was then
solubilized in 100 µL of a mixture of ACN/water (85/15). The chromatography system was a
UFLC-XR Shimadzu. A Kinetex C8 column (100 × 3 mm, 2.6 µm). 10 µL was injected in the
system. The chromatograms were extracted at 260 nm.
30

Laboratory 26: The LC was performed with a Gilson System (Autosampler, 231XL; Sample
Dilutor, 402; Pump, 307; Detector, 155 UV/VIS; System Interface 506C) with analytical
column (ThermoScientific, Accucore XL C18, 4 µm, 100 × 4.6 mm; mobile phase - ACN/0.2%
acetic acid 60/40). A 15 µL injection volume was used (ambient temperature for both the
sample and column) and detection was performed at 262 nm. Extraction was performed
using 250 µL serum + 50 µL internal standard (itraconazole) + 2 mL heptane/isoamyl alcohol
(98.5/1.5), rotated for 20 minutes, centrifuged for 5 minutes, supernatant removed, and then
concentrated under nitrogen for about 10 minutes until the tubes were dry before re-
dissolving in mobile phase.
Bioassay
Laboratory 9: Quality control samples with known amounts of isavuconazole were placed on
each bioassay plate, prepared as follows: A 1000 mg/L standard (A) was used as a drug
stock solution. This stock was diluted 1:10 (100 µL drug stock and 900 µL plasma) to give a
100 mg/L solution (B). For the 2 mg/L internal standard, stock solution B was further diluted
1:50 (150 µL drug stock and 7.35 mL plasma). For the 0.75 mg/L internal standard, stock
solution B was diluted 1:10 (100 µL drug stock and 900 µL plasma) to give a 10 mg/L stock
solution, which was then further diluted 1:13.3 (500 µL drug stock and 6.167 mL plasma).
Both sets of internal standards were then stored in 200 µL amounts in Z5 bottles at –80º C
for up to 3 months.
In the isavuconazole bioassay procedure, a 1000 mg/L stock solution of isavuconazole in
dimethyl sulfoxide (1000 mg/L) was prepared and dispensed into twelve 250 µL aliquots. A
hot plate was used to melt 90 mL of base agar before allowing it to cool to 56 ± 2°C in a
warm water bath. A solution of yeast nitrogen base with glucose and tri-sodium citrate
(YNBG + citrate) was also warmed to the same temperature in the bath. A suspension of
Candida kefyr (San Antonio strain) was prepared in 7 mL of sterile distilled water equal to 5
McFarland standard. The optical density of the suspension was determined at a wavelength
31

of 490 nm on a spectrophotometer in triplicate; the average optical density was calculated,
adjusted to an OD of 0.1, and the suspension was vortexed before removing 5 mL to a new
sterile universal to be used as the bioassay inoculum. When the agar had cooled to 56 ± 2°C
(approximately 30 minutes), the 10 mL aliquot of concentrated YNBG + citrate solution and
the 5 mL Candida kefyr suspension were vortexed thoroughly and added. The agar, YNBG +
citrate and Candida kefyr suspension was mixed before pouring it in to a labeled bioassay
plate ensuring no bubbles were present and left to solidify for at least 30 minutes. To
construct a standard curve, a set of standards of isavuconazole stock solution diluted in
plasma were prepared (0.125, 0.25, 0.5, 1.25, 2.5, 5, and 7.5 mg/L). When the agar had
solidified, cut 36 wells of 8 mm in diameter with sterile cork borer No. 3 were cut (6 rows of 6)
using a template as a guide. The plate was dried at 37°C, inverted with the lid open, for
approximately 1 hour. Using the template, 40 µL of standard, internal control or specimen
were placed into the appropriate wells (at room temperature). The drug was allowed to pre-
diffuse until all the wells appear completely dry and the plate was incubated at 37ºC
overnight (approximately 18 hours). The diameters of the zones of inhibition around each
well were measured using calipers (to the nearest 0.01 mm) and recorded on the results
template. Concentrations in samples were determined by placement on the standard curve
graph.
Laboratory 10: The approach was adapted from Steinmann, et al. (Mycoses. 2011;54:e421-
8). Briefly, commercially available isavuconazole 200 mg (Basilea, Basel, Switzerland) was
reconstituted in 20 mL of dimethyl sulfoxide (Roth, Karlsruhe, Germany). From this, further
dilutions were made in bovine serum (Oxoid, Wesel, Germany) to get a stock solution
containing 10 mg l-1 isavuconazole. Immediately after reconstitution, routine daily calibration
standard samples containing 0.5, 1.0, 2.0, 4.0 or 8.0 mg/L isavuconazole were prepared by
diluting the stock solution in bovine serum. The samples were stored in small portions at
–20°C. The biological activity of isavuconazole in serum samples was measured by a disc
diffusion assay. The agar medium contained 7 g yeast nitrogen base (Difco; Becton
Dickinson, Heidelberg, Germany), 7 g tryptic peptone (Merck KGaA, Darmstadt, Germany),
32

15 g glucose and 20 g agar-agar (Merck) and phosphate buffer. For phosphate buffer
production, 1.43 g KH2PO2, 10 g Na2HPO4 and 2 H2O were dissolved in 1000 mL Aqua dem.
with a final pH of 7.5. The ingredients were dispersed in the buffer and autoclaved for 15
minutes at 121°C. After being cooled to 50°C, 70 mL of the agar was dispensed into sterile
150 × 200 mm Petri dishes which were stored in plastic bags at 4°C for as long as 7 days. An
isavuconazole-hypersusceptible Candida kefyr strain (internal identifier number R34) served
as the test organism. Subcultures were performed weekly on Sabouraud dextrose agar
plates (Becton Dickinson, Franklin Lakes, NJ, USA). One colony forming unit of the
subcultured test organism was tipped and suspended in 5 mL of sterile 0.85% sodium
chloride solution; the turbidity was adjusted to a McFarland standard of 1.0. Then 200 µL of
this suspension was spread on the surface of the test plate. Paper discs (Becton Dickinson)
6 mm in diameter were impregnated with 40 µL of a standard sample, a blank control
sample, or patient sera. The loaded samples were allowed to prediffuse for 20–30 minutes at
room temperature. Zones of inhibited growth were measured after the plates had been
incubated at 35°C for 18–20 hours. The vertical and horizontal inhibition zones were
measured using an electronic vernier caliper (0–150 mm/0–6”, Insize, Zamudio [Bizkaia],
Spain). The diameter of zones of inhibited growth was plotted on a semilogarithmic graph
and the isavuconazole concentrations were placed on the logarithmic abscissa. The graph
was interpreted by estimating the isavuconazole concentration in the patient specimen and in
the internal standard sample. All test runs were performed in duplicate and for each sample,
one standard curve was prepared.
33

List of participating investigators (alphabetical by country and last name)
Austria: Robert Krause, Andreas Meinitzer (Graz)
Denmark: Rene Jörgensen (Copenhagen)
France: Delphine Allorge (Lille); Youssef Bennis (Amiens); Guillaume Deslandes (Nantes);
Marie-Claude Gagnieu (Lyon); Nicolas Gambier (Nancy); Benjamin Hennart (Lille);
Vincent Jullien (Paris); Veronique Kemmel (Strasbourg); Castaing Nadège (Bordeaux);
Damien Richard (Clermont-Ferrand); Julien Scala-Bertola (Nancy); Françoise Stanke
(Grenoble); Nicolas Venisse (Poitiers)
Germany: Carsten Müller (Cologne); Jörg Steinmann (Essen); Stefan Tönnes (Frankfurt);
Martin Wiesen (Cologne)
Italy: Jessica Biasizzo (Udine); Giuliana Congemi (Genova); Antonio D’Avolio (Torino);
Antonello Di Paolo (Pisa); Elisa Furfaro (Genova); Arianna Loregian (Padova);
Mariadelfina Molinario (Pavia); Andrea Novelli (Firenze); Federico Pea (Udine); Tanja
Zamparo (Udine)
Netherlands: Roger Brüggeman (Nijmegen)
United Kingdom: Debbie Oliver (Bristol); Caroline Moore, Malcolm Richardson, Cheryl
Wilkinson (Manchester)
34